Salivary Gland Surgery
Overview of Salivary Glands1
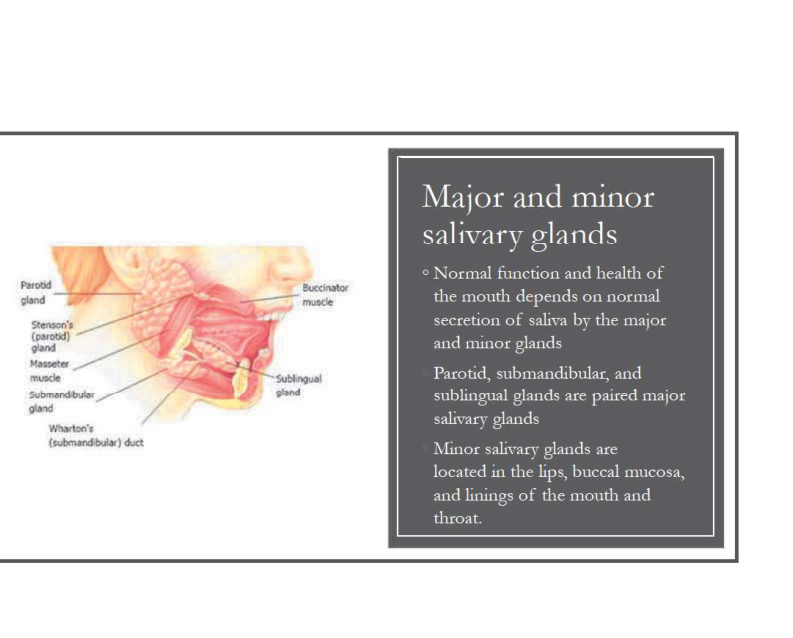
Normal function and health of the mouth depends on the normal secretion of saliva by both major and minor glands.
- Major Salivary Glands: These consist of the paired parotid, submandibular, and sublingual glands.
- Minor Salivary Glands: These are distributed throughout the lips, buccal mucosa, and the linings of the mouth and throat.
 |  |
Anatomy and Physiology of Salivary Glands
Common Obstructive Conditions
Salivary gland dysfunction often involves obstructive pathologies, including:
- Salivary calculi: The formation of stones within the gland or duct system.
- Duct strictures: Narrowing of the salivary ducts that impedes flow.
- Mucocele: Mucous extravasation or retention phenomena typically affecting minor glands.
Obstructive Salivary Gland Disorders
Sialolithiasis and Duct Strictures
Pathophysiology and Characteristics2
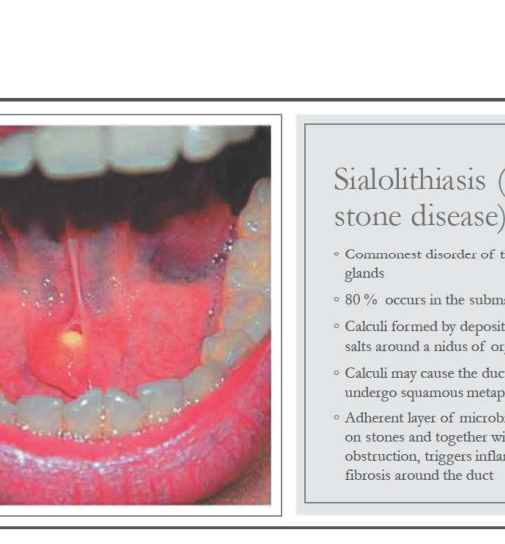
- Commonest disorder of the salivary glands
- 80% occurs in the submandibular gland
- Calculi formed by deposition of calcium salts around a nidus of organic material
- Calculi may cause the duct lining to undergo squamous metaplasia
- Adherent layer of microbial flora grows on stones and together with obstruction, triggers inflammation and fibrosis around the duct
 |  |
 |
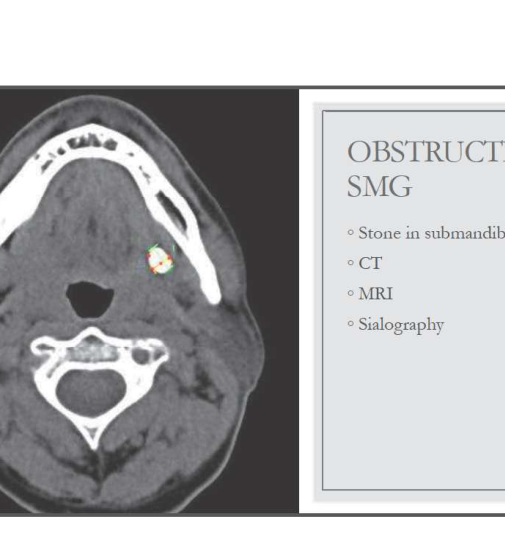
Diagnostic Imaging for Submandibular Obstruction
- CT
- MRI
- Sialography
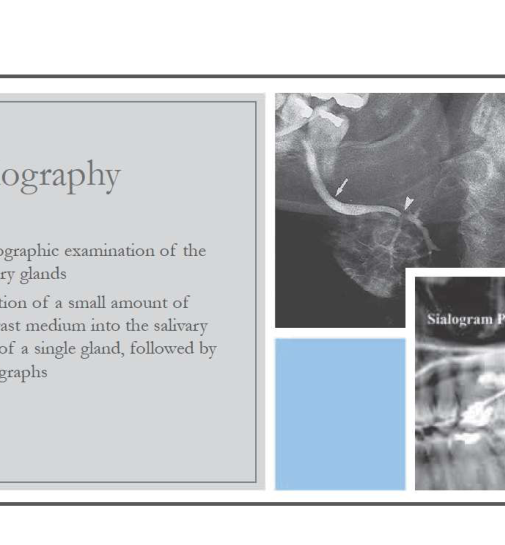
Sialography Overview
- Radiographic examination of the salivary glands
- Injection of a small amount of contrast medium into the salivary duct of a single gland, followed by radiographs
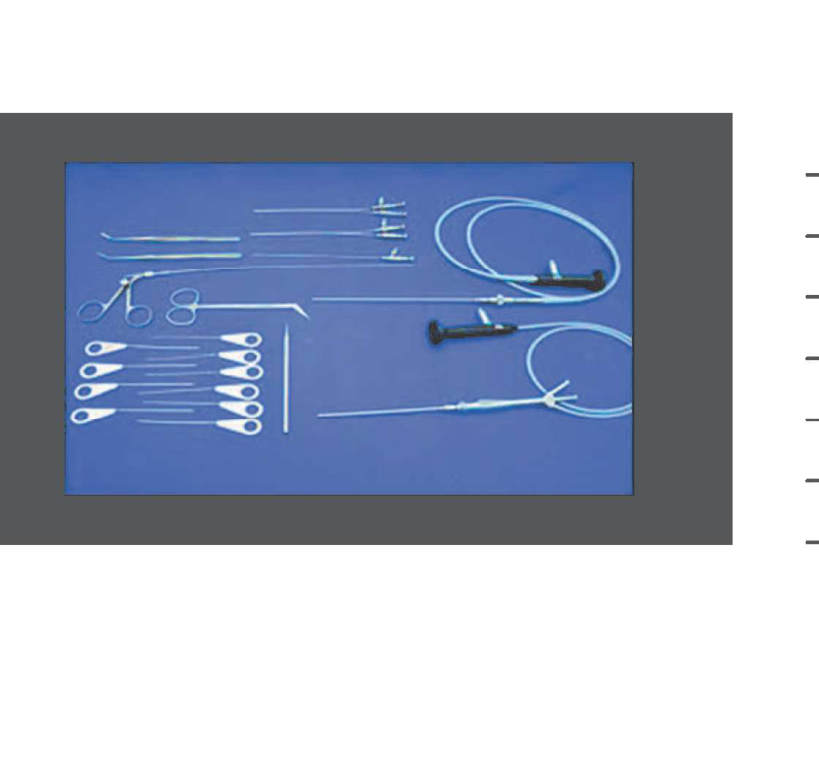
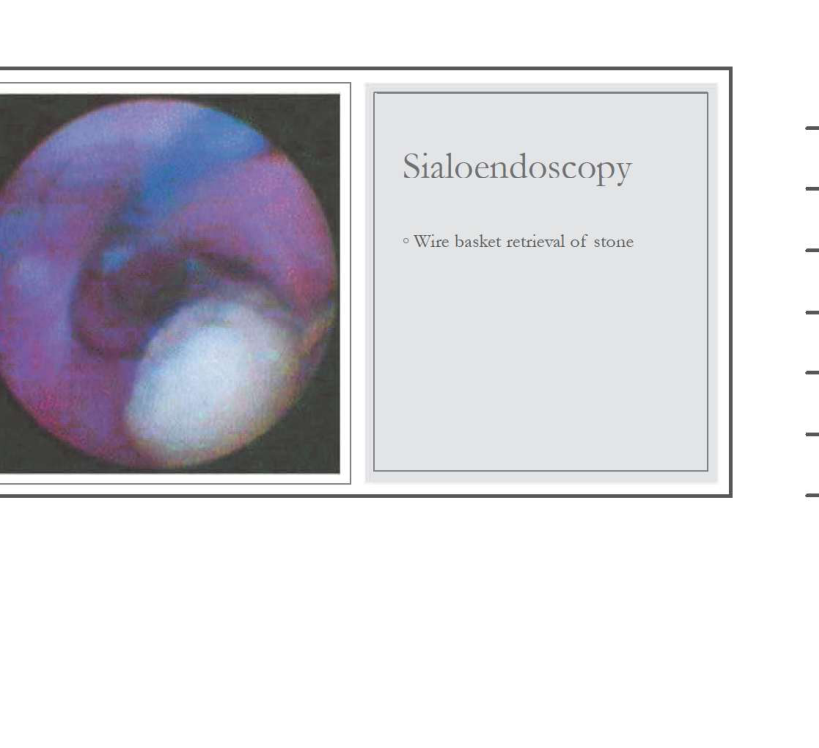
Sialoendoscopy and Stone Retrieval
Sialoendoscopy Techniques3
- Wire basket retrieval of stone
 |  |
 |
Mucocoele and Ranula
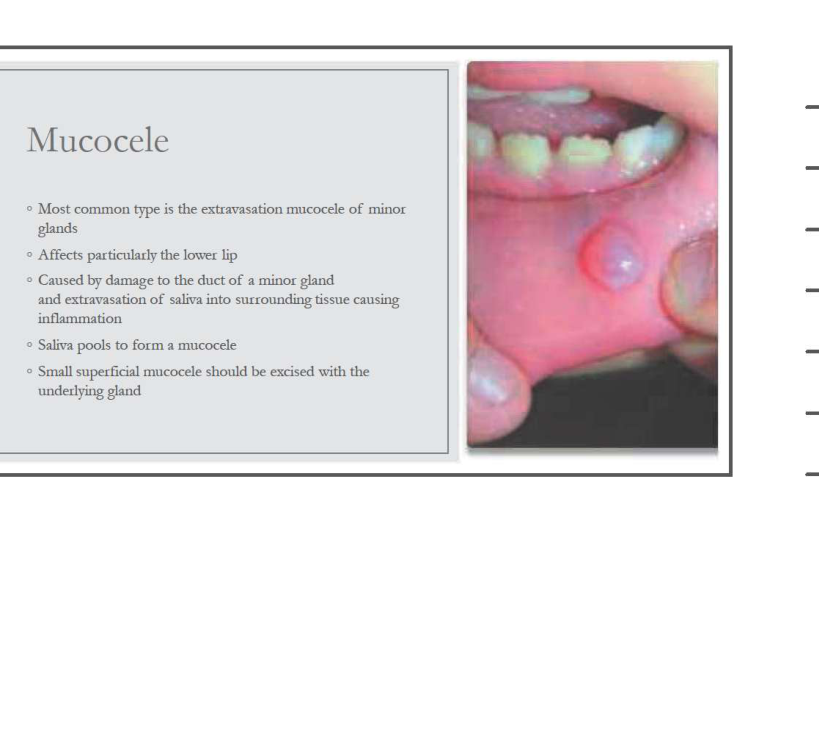
Mucocoele Characteristics
- Most common type is the extravasation mucocele of minor glands
- Affects particularly the lower lip
- Caused by damage to the duct of a minor gland and extravasation of saliva into surrounding tissue causing inflammation
- Saliva pools to form a mucocoele
- Small superficial mucocele should be excised with the underlying gland
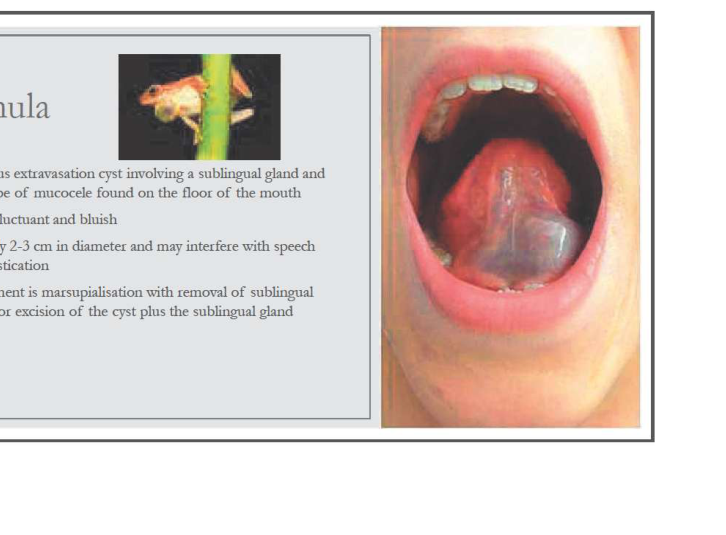
Ranula Clinical Presentation4
- Mucous extravasation cyst involving a sublingual gland and is a type of mucocele found on the floor of the mouth
- Soft, fluctuant and bluish
- Usually 2-3 cm in diameter and may interfere with speech or mastication
 |  |
 |
Management
- Treatment is marsupialisation with removal of sublingual gland or excision of the cyst plus the sublingual gland
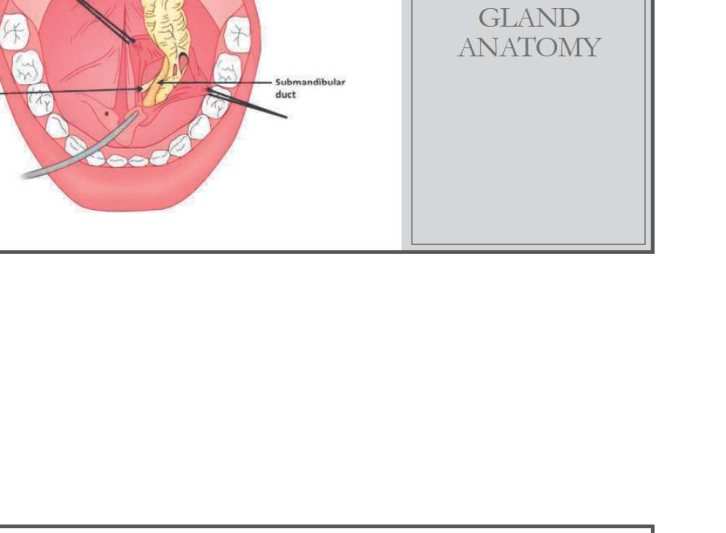
Anatomy
- Floor of mouth
- Sublingual gland anatomy
Submandibular Gland Surgery
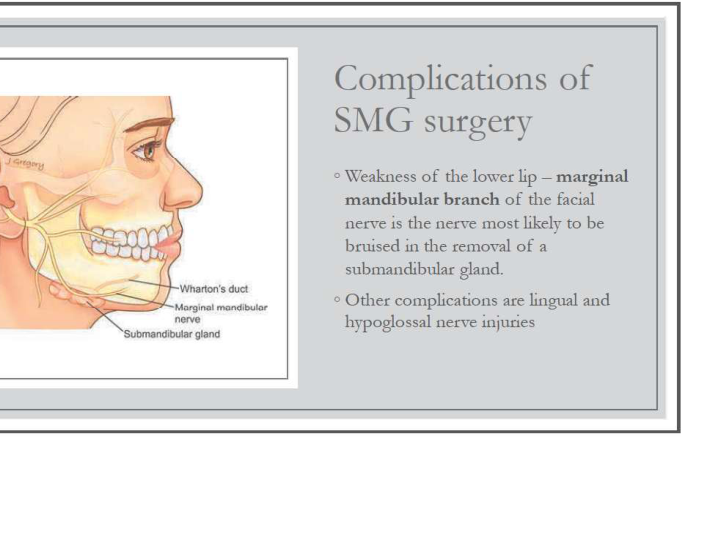
Complications of Submandibular Gland Excision
Nerve Injuries
- Weakness of the lower lip – marginal mandibular branch of the facial nerve is the nerve most likely to be bruised in the removal of a submandibular gland.
- Other complications are lingual and hypoglossal nerve injuries
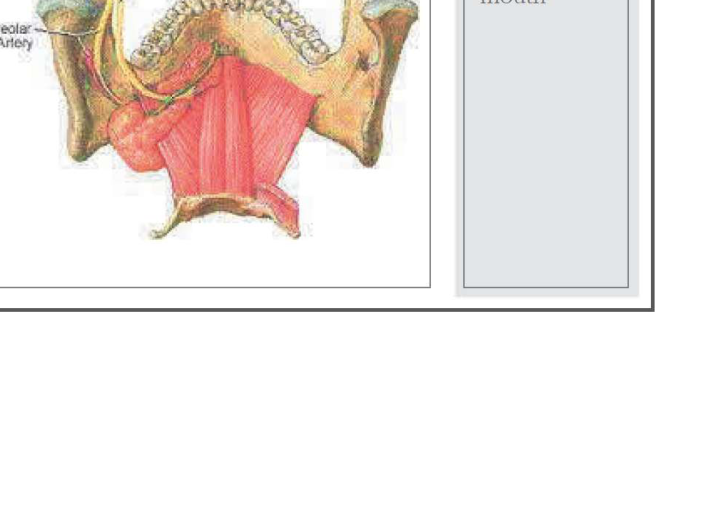
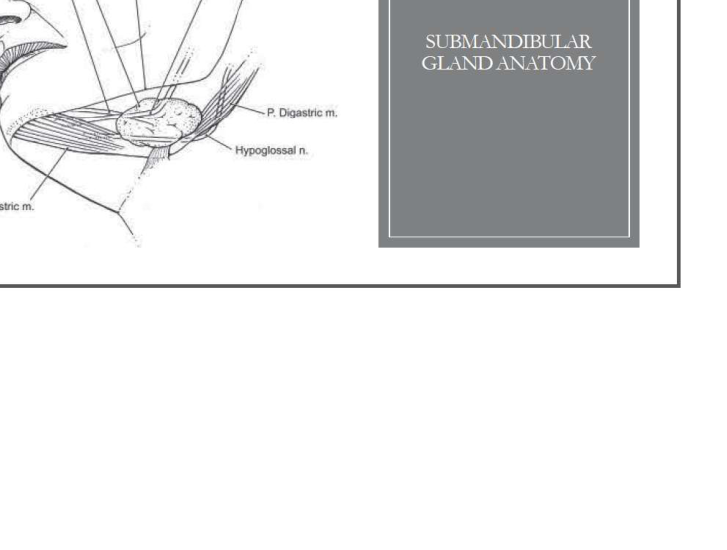
Surgical Anatomy of the Submandibular Triangle
Anatomical Structures5
- Submandibular gland
- Edge of mandible
- Lingual nerve
- Hypoglossal nerve
- Digastric muscle (Anterior and Posterior)
- Wharton’s duct
 |  |
Management of Salivary Gland Obstruction
- Antibiotics for underlying salivary gland infections
- Lithotripsy +/- sialoendoscopy to retrieve calculi
- Excision of calculi from Wharton’s duct (sialolithotomy)
- Excision of the gland (submandibular gland or superficial parotidectomy)
Non-Neoplastic Cysts and Conditions
Lymphoepithelial Cysts6
- Slow growing unilocular or multilocular lesions, predominantly in the parotid glands
- Obstruction of salivary ducts by diffuse lymphoid infiltrate
- Seen in patients with HIV infection as part of diffuse infiltrative lymphocytosis syndrome
- In non-HIV individuals with autoimmune disease (e.g., Sjogren syndrome), lymphocytes infiltrate the gland and choose around ducts, resulting in destruction of acini and replacement of the gland by dense lymphocytic infiltrate
Bilateral Parotid Enlargement
Salivary Gland Tumours Overview
- Global annual incidence of 0.4-13.5 cases per 100,000
- Commonly appear in sixth decade of life
- Malignant lesions typically present after age 60 years
- Benign lesions usually present between 40-60 years
- Malignant tumours distributed equally between the sexes
- Incidence of salivary gland cancers in Australia is 1.2 per 100,000 and mortality is 0.3 per 100,000
- Accounts for 5-6% of head and neck cancers, and 0.3-1% of all sites of malignancy
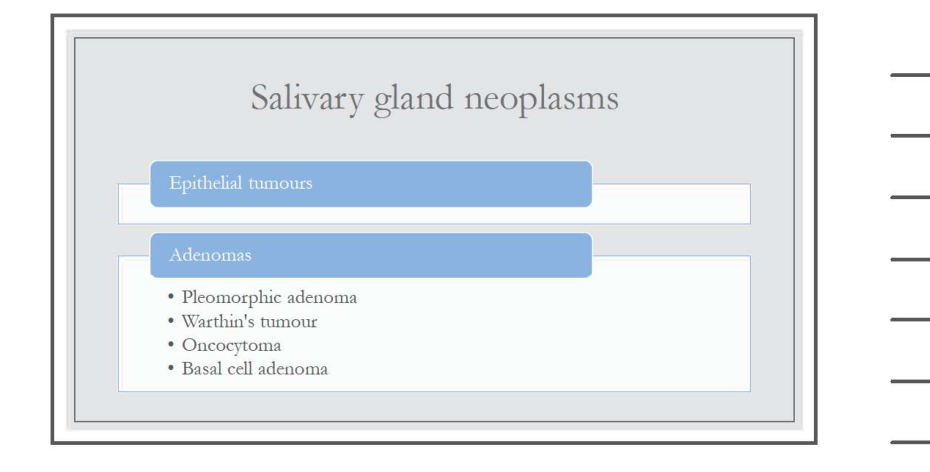
Salivary Gland Neoplasms
Epidemiology and Distribution
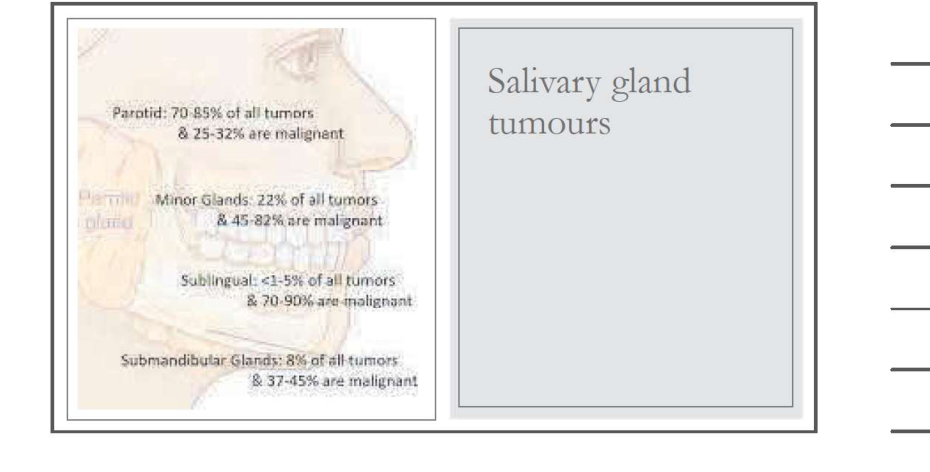
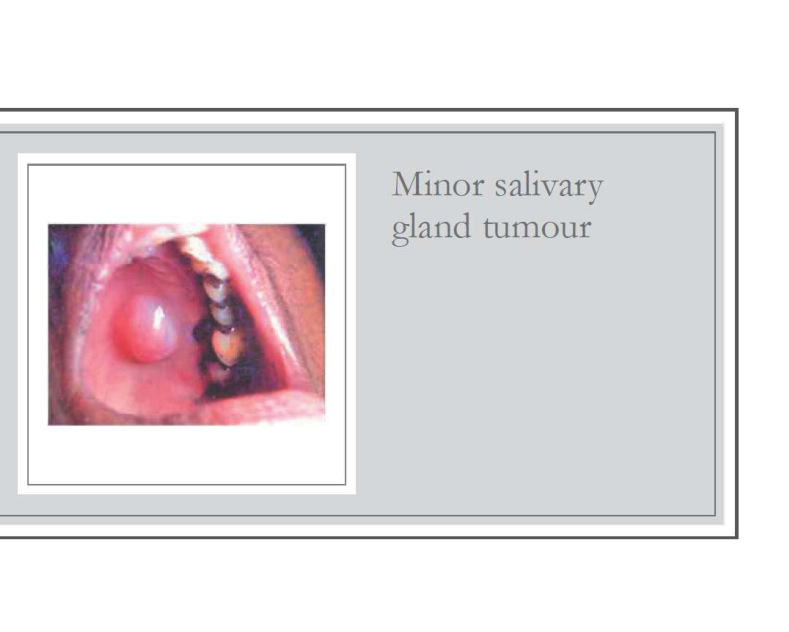
Tumor Distribution by Gland Site7
- Parotid: 70-85% of all tumors; 25-32% are malignant
- Minor Glands: 22% of all tumors; 45-82% are malignant
- Sublingual: <1-5% of all tumors; 70-90% are malignant
- Submandibular Glands: 8% of all tumors; 37-45% are malignant
 |  |
 |
Classification of Epithelial Tumours
Adenomas
- Pleomorphic adenoma
- Warthin’s tumour
- Oncocytoma
- Basal cell adenoma
Carcinomas
- Mucoepidermoid carcinoma
- Acinic cell carcinoma
- Adenoid cystic carcinoma
- Polymorphous low-grade adenocarcinoma
- Salivary duct carcinoma
- Epithelial-myoepithelial carcinoma
- Adenocarcinoma
- Undifferentiated carcinoma
- Carcinoma ex pleomorphic adenoma
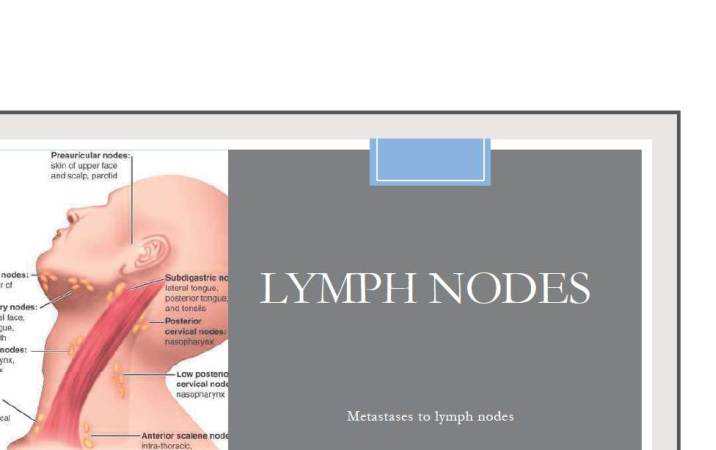
Non-Epithelial Tumours and Metastases
Types and Lymph Node Involvement8
- Lymphomas
- Metastases to parotid lymph nodes and submandibular lymph nodes
 |  |
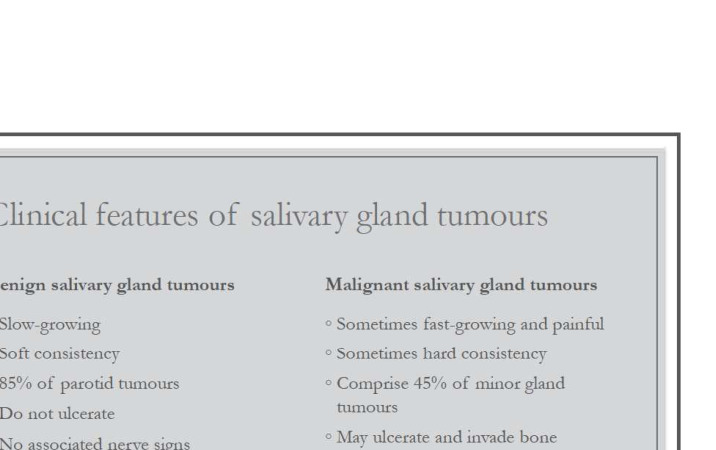 |
Clinical Presentation and Diagnosis
Comparison of Benign vs. Malignant Tumours
| Benign salivary gland tumours | Malignant salivary gland tumours |
|---|---|
| • Slow-growing | • Sometimes fast-growing and painful |
| • Soft consistency | • Sometimes hard consistency |
| • 85% of parotid tumours | • Comprise 45% of minor gland tumours |
| • Do not ulcerate | • May ulcerate and invade bone |
| • No associated nerve signs | • May cause cranial nerve palsies |
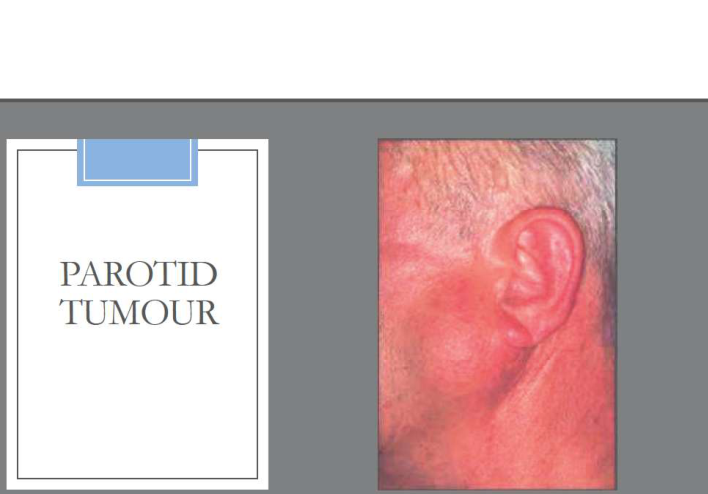
Malignant Parotid Tumour Symptoms9
- Hard fixed lump
- Numbness
- Muscle weakness
- Difficulty swallowing
- Trismus
- Lymph node metastasis
Diagnostic Imaging
- Sialography: useful for inflammatory disease
- CT, US, and MRI: for suspected neoplasm
- MRI: often superior to CT in demonstrating interface of tumour and surrounding tissue to predict possible malignancy
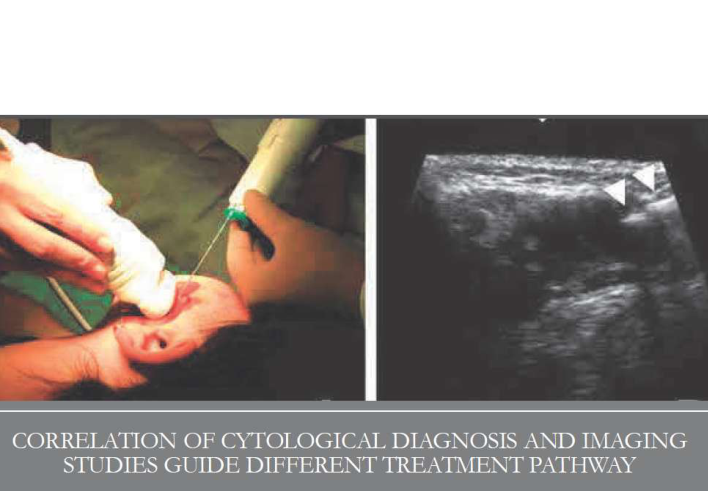
Fine Needle Aspiration Cytology (FNAC)
- Evaluation of head and neck tumours
- Provides distinction between benign and malignant tumours
- Inexpensive, easy to perform, relatively painless, and well tolerated
- Correctly establishing diagnosis as benign or malignant in 81.98% of cases
- False positive and false negative rates: 1-14%
- Specific diagnosis in 60-75%
- Accuracy varies depending on the precision and experience of the pathologist
Management of Parotid Gland Tumours
Surgical Considerations and Facial Nerve Anatomy
Parotid Tumour and Facial Nerve Anatomy10
 |  |
Malignancy Management and Adjuvant Therapy
Management of Parotid Gland Malignancy11
- Parotid gland malignancies with clinically evident regional nodal metastasis should undergo a formal neck dissection, followed by appropriate adjuvant therapy (e.g., radiotherapy).
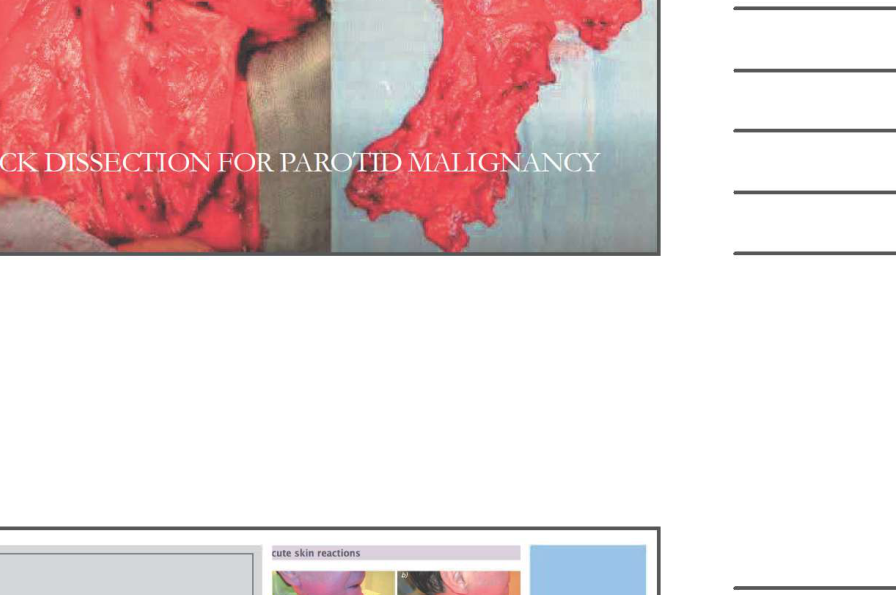
Adjuvant Therapy
- Radiotherapy
Post-Surgical Rehabilitation and Prosthetics12
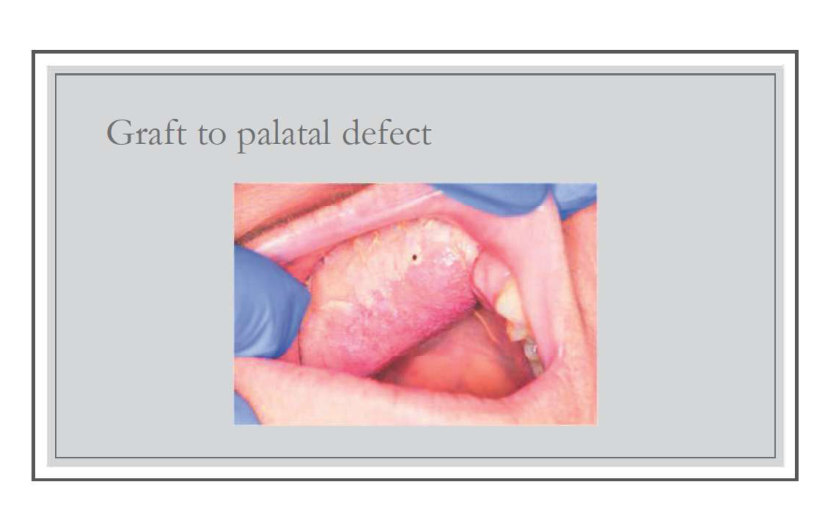
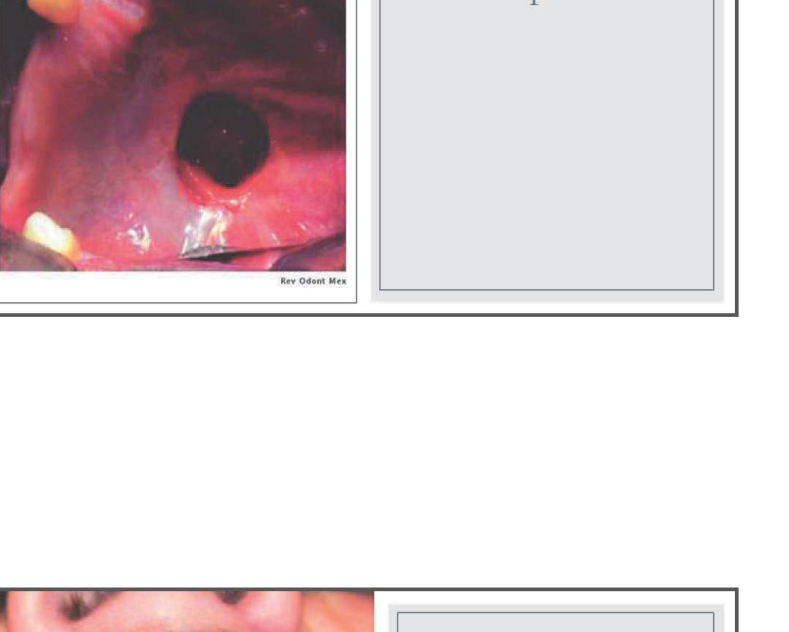
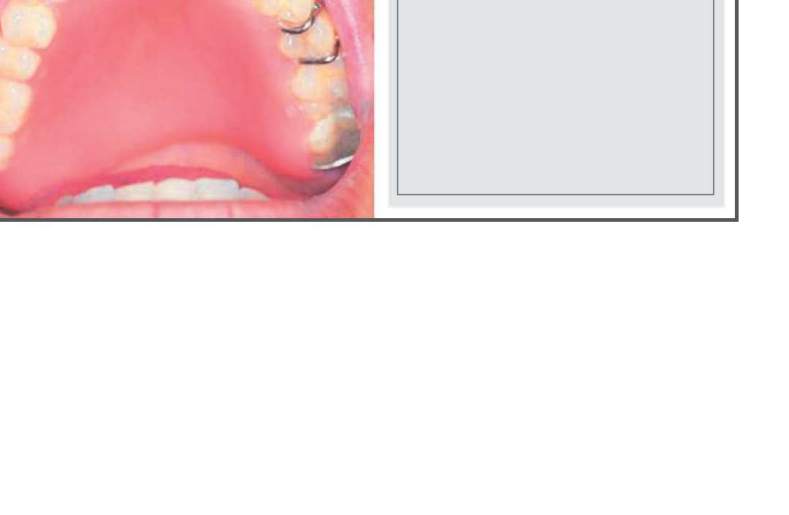
Palatal Defects13
- Hole in palate
- Obturator
 |  |
 |
Footnotes
-
Original PDF page 1: W3.1 Salivary gland surgery, p.1 ↩
-
Original PDF page 2: W3.1 Salivary gland surgery, p.2 ↩
-
Original PDF page 3: W3.1 Salivary gland surgery, p.3 ↩
-
Original PDF page 4: W3.1 Salivary gland surgery, p.4 ↩
-
Original PDF page 5: W3.1 Salivary gland surgery, p.5 ↩
-
Original PDF page 6: W3.1 Salivary gland surgery, p.6 ↩
-
Original PDF page 7: W3.1 Salivary gland surgery, p.7 ↩
-
Original PDF page 8: W3.1 Salivary gland surgery, p.8 ↩
-
Original PDF page 9: W3.1 Salivary gland surgery, p.9 ↩
-
Original PDF page 10: W3.1 Salivary gland surgery, p.10 ↩
-
Original PDF page 11: W3.1 Salivary gland surgery, p.11 ↩
-
Original PDF page 13: W3.1 Salivary gland surgery, p.13 ↩
-
Original PDF page 12: W3.1 Salivary gland surgery, p.12 ↩