Oral Maxillofacial Pathology Surgical Management1
Magdalen Foo
Discipline Lead Oral Maxillofacial Surgery
Introduction and Learning Outcomes
Prerequisite Knowledge Areas2
-
Oral mucosal lesions
-
Common benign salivary gland tumours
-
Bone lesions
-
Dental anatomy and tooth development
-
Head and neck anatomy
-
==Anatomy and Physiology: Understanding the normal architecture of the jaw, including the relationship between the maxilla, mandible, and the teeth they carry.==
-
==Systemic Health: Knowledge of how systemic conditions (e.g., Paget’s disease, hyperparathyroidism, renal failure) manifest in the oral cavity.==
-
==Pharmacology: Awareness of medications like bisphosphonates and Prolia (denosumab) and their impact on bone healing (MRONJ risk).==
Clinical Competencies3
-
Discuss appropriate investigations, including imaging and biopsy techniques.
-
Understand the surgical management of oral and maxillofacial pathology.
-
==Patient Autonomy: Recognizing that while a clinician can advise on the “ideal” treatment plan (e.g., orthodontic traction for an impacted tooth), the patient has the right to refuse.==
-
==Differential Diagnosis: Developing a list of potential conditions based on radiographic and clinical findings before referring for biopsy.==
-
==Vitality Testing: Using pulp testing (e.g., on teeth adjacent to a lesion) to determine if a pathology is odontogenic or bone-related.==
-
This growth pattern differs from aggressive tumors, which tend to resorb adjacent teeth rather than displace them
Mechanism of Recurrence
This high rate is attributed to 'satellite' or 'daughter' cells and a very thin, friable lining that is easily left behind during surgery.
Jaw Cysts
Definition and Characteristics4
- Cysts are pathological fluid-filled cavities lined by epithelium
- Most cysts in the jaws are formed from epithelium (odontogenic cysts)
- The most common odontogenic cyst of the jaws is the periapical (radicular) cyst
Diagnostic Probability
If you guess ‘radicular’ for a jaw cyst, you will be correct roughly two out of three times.
- Non-odontogenic cysts include the nasopalatine duct cyst and the nasolabial cyst
Relative Frequency5
- Periapical: 65–70%
- Dentigerous: 15–18%
- Odontogenic keratocyst: 3–5%
- Nasopalatine: 5–10%
- Lateral periodontal: <1%
- Paradental: <1%
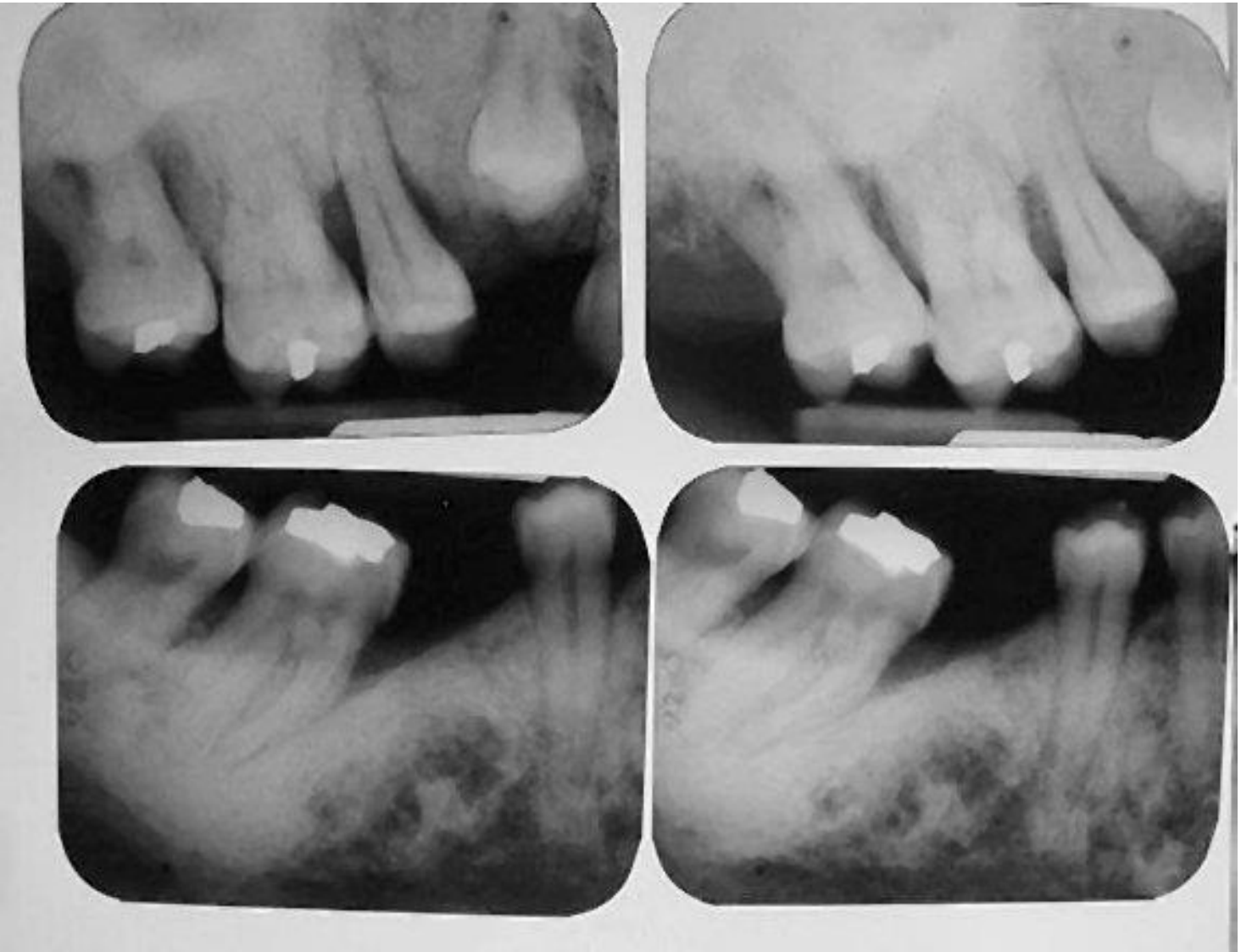
Clinical Features and Diagnosis6
Clinical Presentation7
- Sharply defined radiolucencies with smooth borders
- Fluid may be aspirated
- Slow growing, displacing rather than resorbing teeth
- Symptomless unless infected and usually change radiographic findings
May have identical radiographic appearances and diagnosis ultimately depends on histopathology.

Diagnostic Identification8
Radiographic assessment is used to identify the specific location and extent of the lesion within the jawbone.
- Radicular cysts generally do not recur once treated
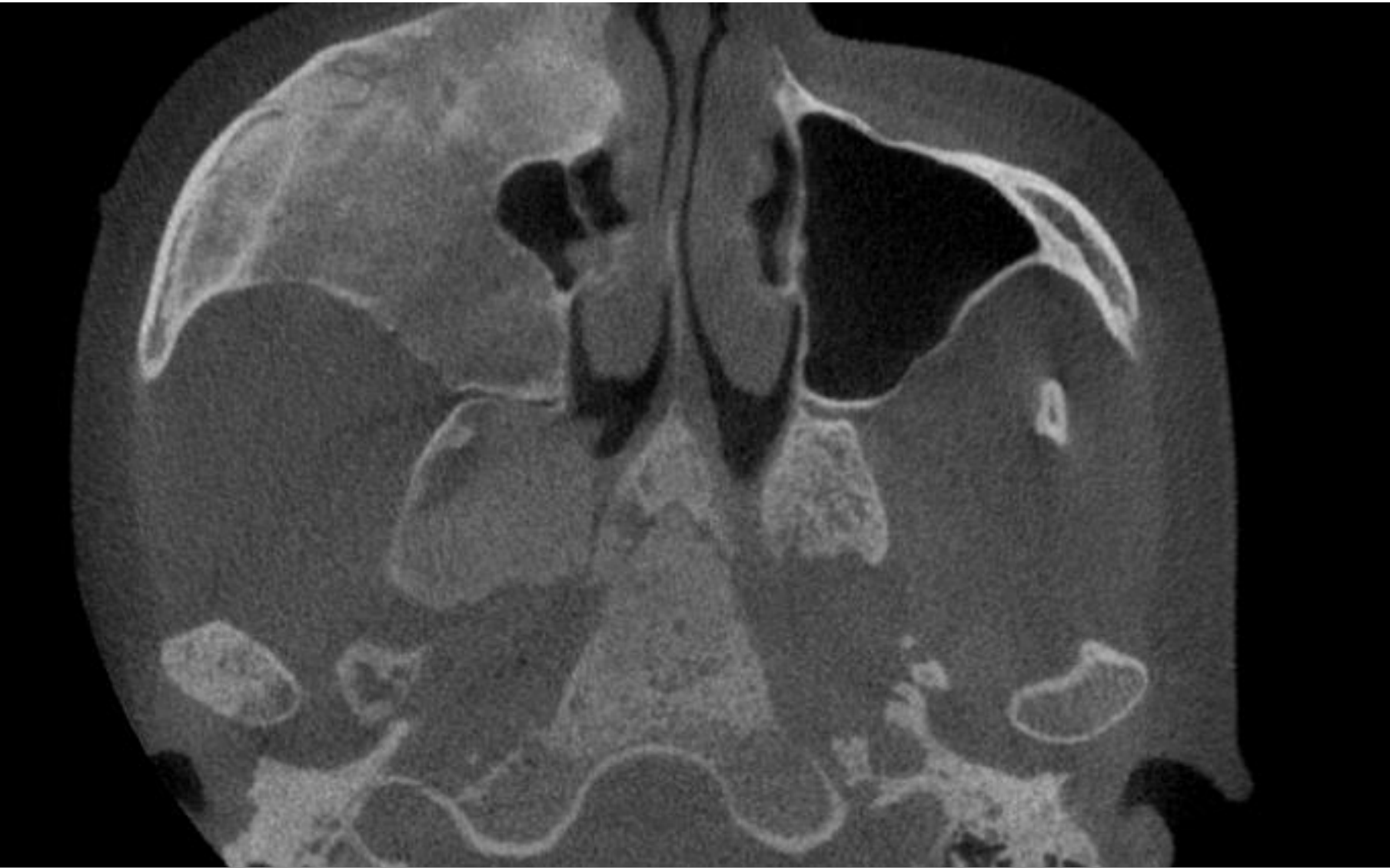
- CT or Cone Beam CT (CBCT) is particularly useful to assess the degree of bony expansion and the relationship to vital structures (nerves, sinuses)
- Clinicians should use the unaffected side of the jaw as a comparative baseline when reading scans
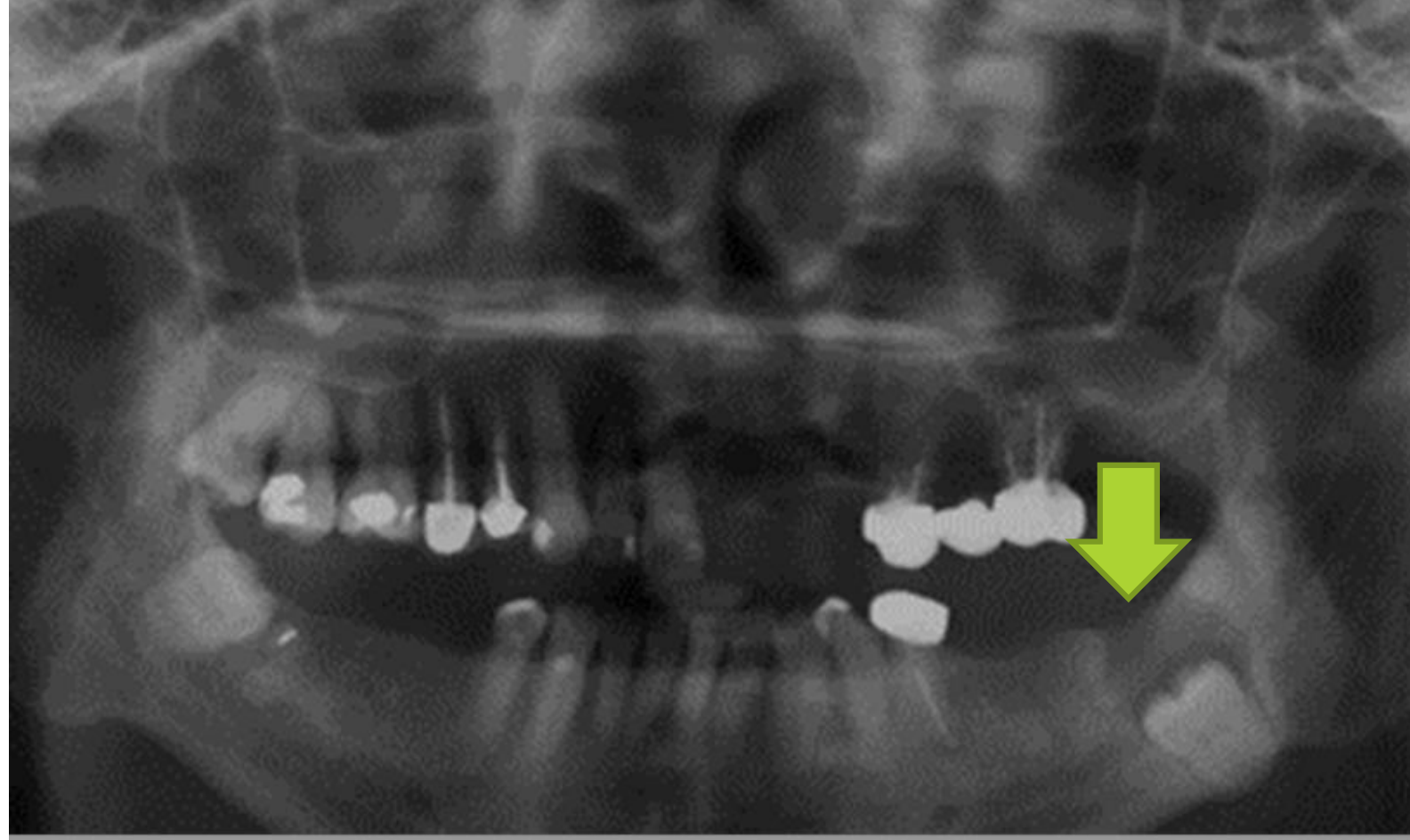 |  |
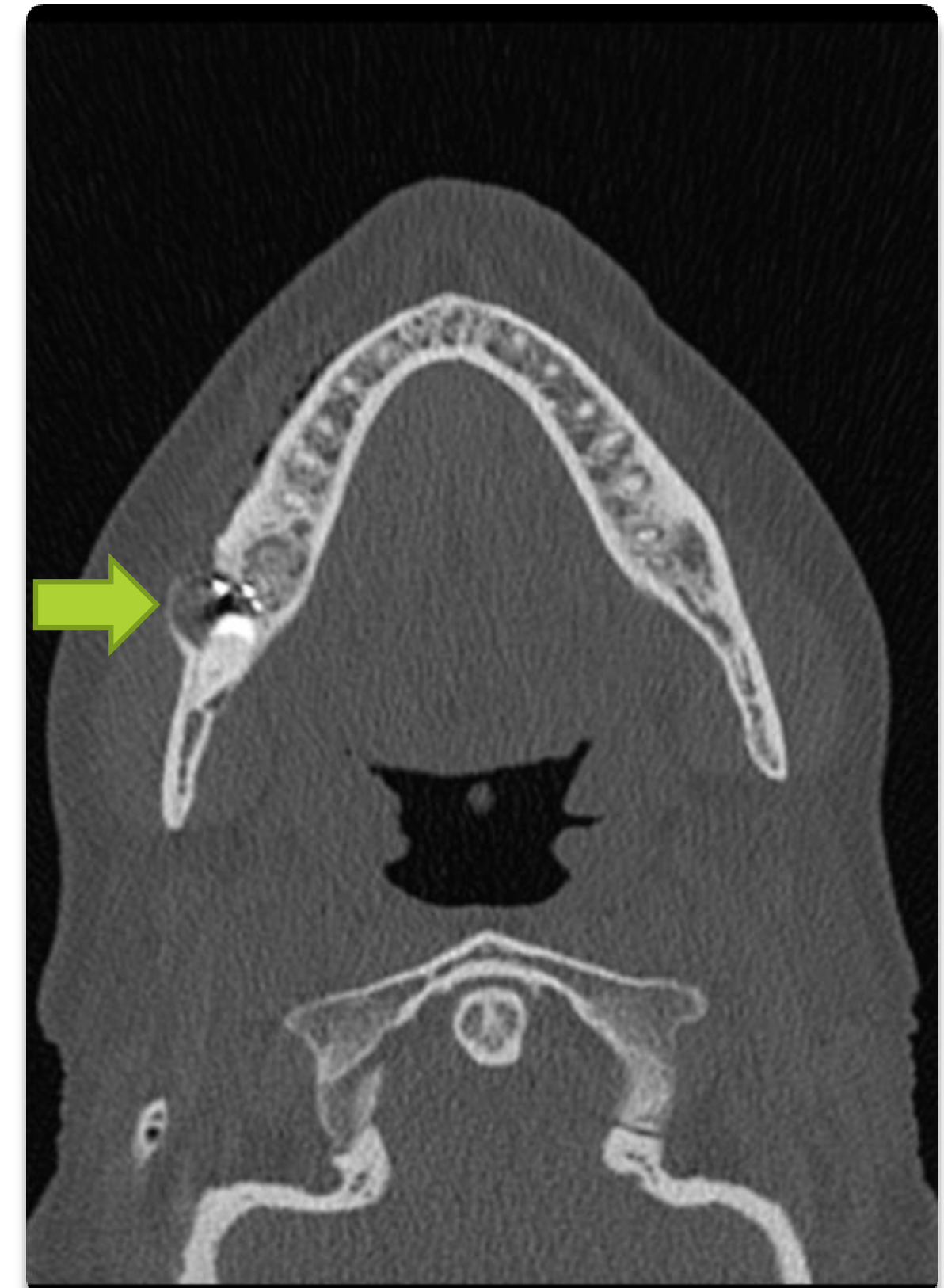
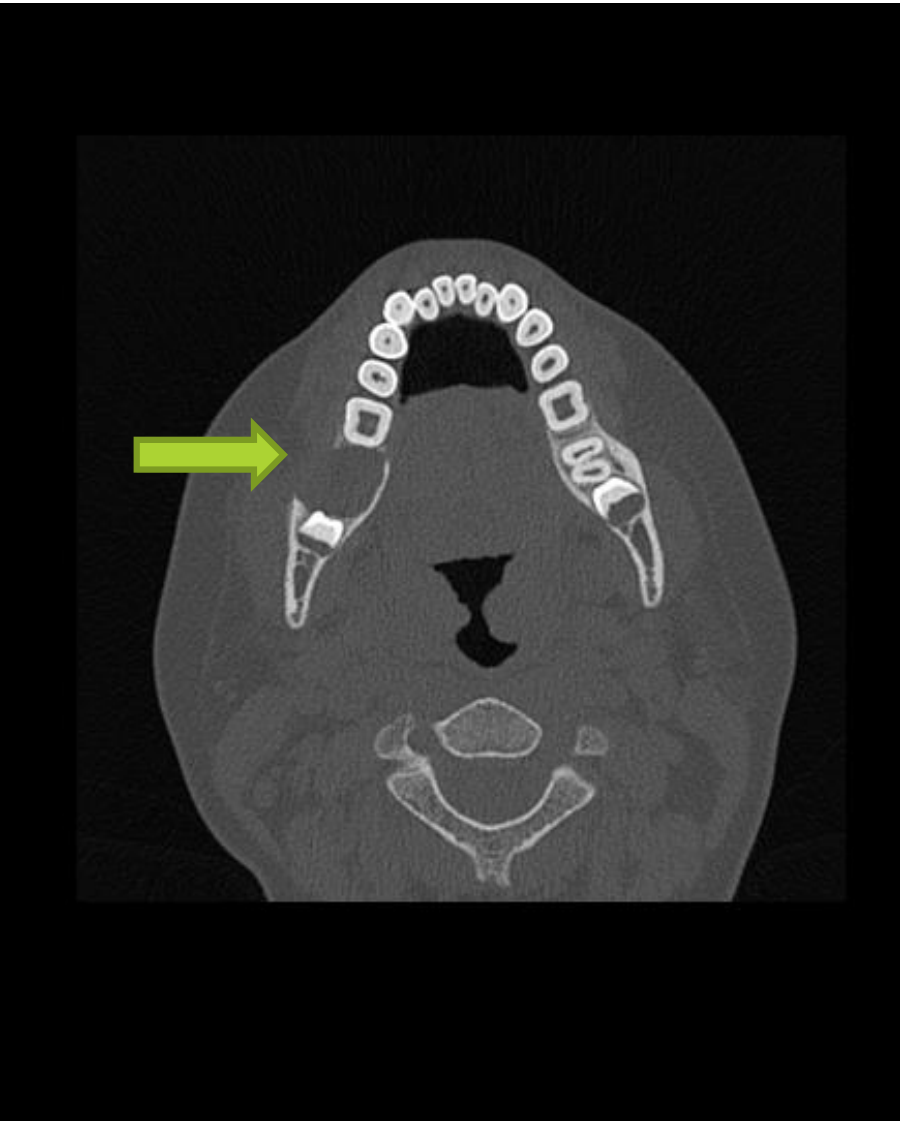
Imaging – CT Scan9
Lucent lesion in the right mandibular angle/body likely reflects an odontogenic keratocyst. Appearances are not classical for a dentigerous cyst.
Odontogenic Cysts10
Cyst lining derived from epithelium involved in tooth development.
- Periapical cyst (inflammatory)
- Dentigerous cyst (developmental)
- Odontogenic keratocyst (developmental)
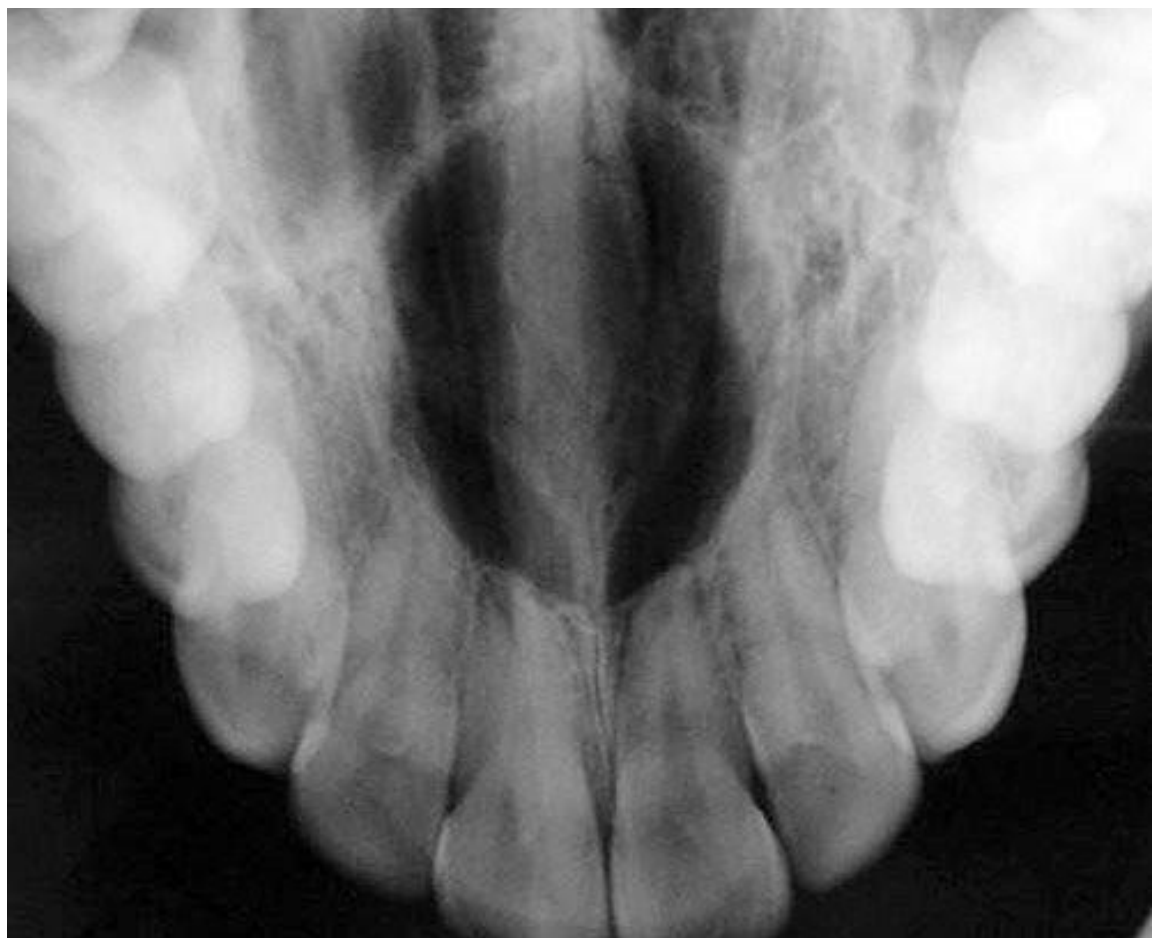
Periapical Cyst
Clinical and Radiographic Features
- Rounded, well circumscribed, corticated radiolucency at apex of nonvital tooth
Management
- Enucleation after extraction or endodontic treatment
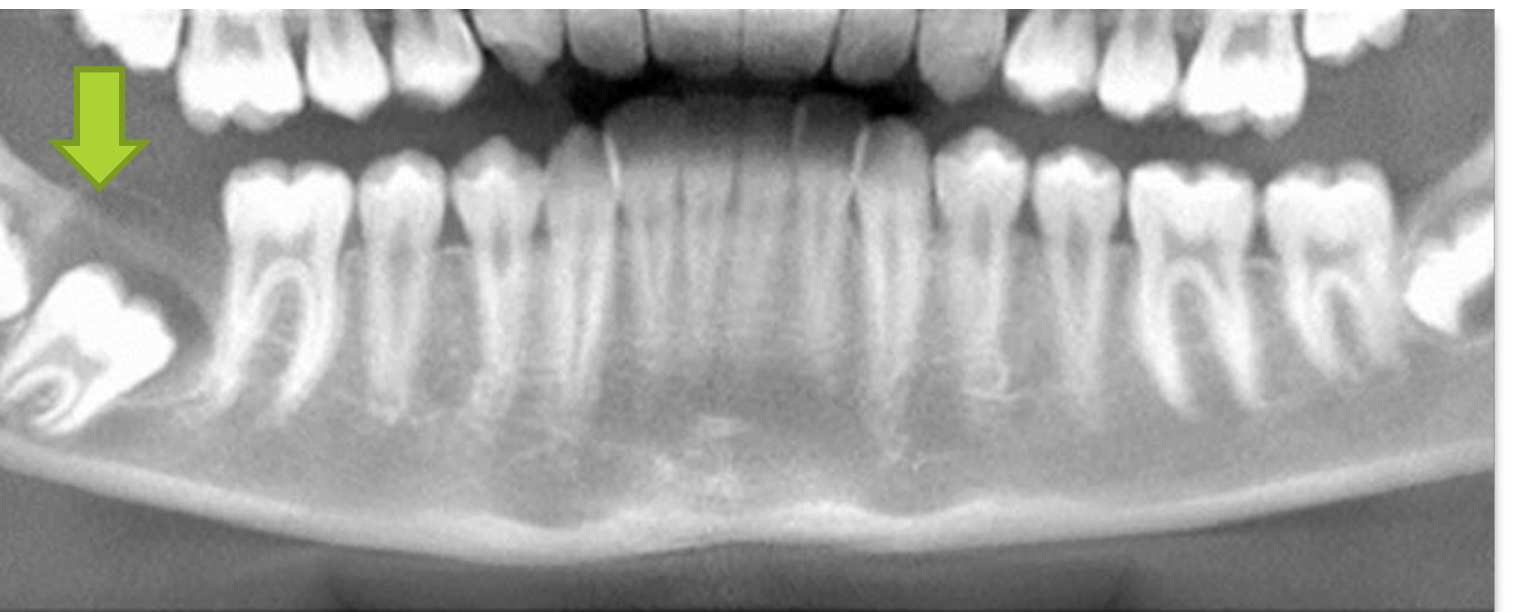
Dentigerous Cyst
Pathogenesis and Presentation
- Odontogenic cyst that surrounds the crown of an impacted tooth
- Accumulation of fluid between the reduced enamel epithelium and the enamel surface
- This results in a cyst with the crown inside the lumen and the roots outside
- Commonly associated with impacted teeth (e.g., tooth 47)
Surgical Management
- Treatment is surgical enucleation
- The associated tooth is extracted at the time of cyst enucleation
- Alternatively, the cyst is marsupialized +/- the tooth brought into alignment in the arch with orthodontic appliance
- Alternatively, surgical exposure of the Cemento-Enamel Junction (CEJ) may be attempted to encourage eruption, though patients must be warned that the tooth may remain stationary
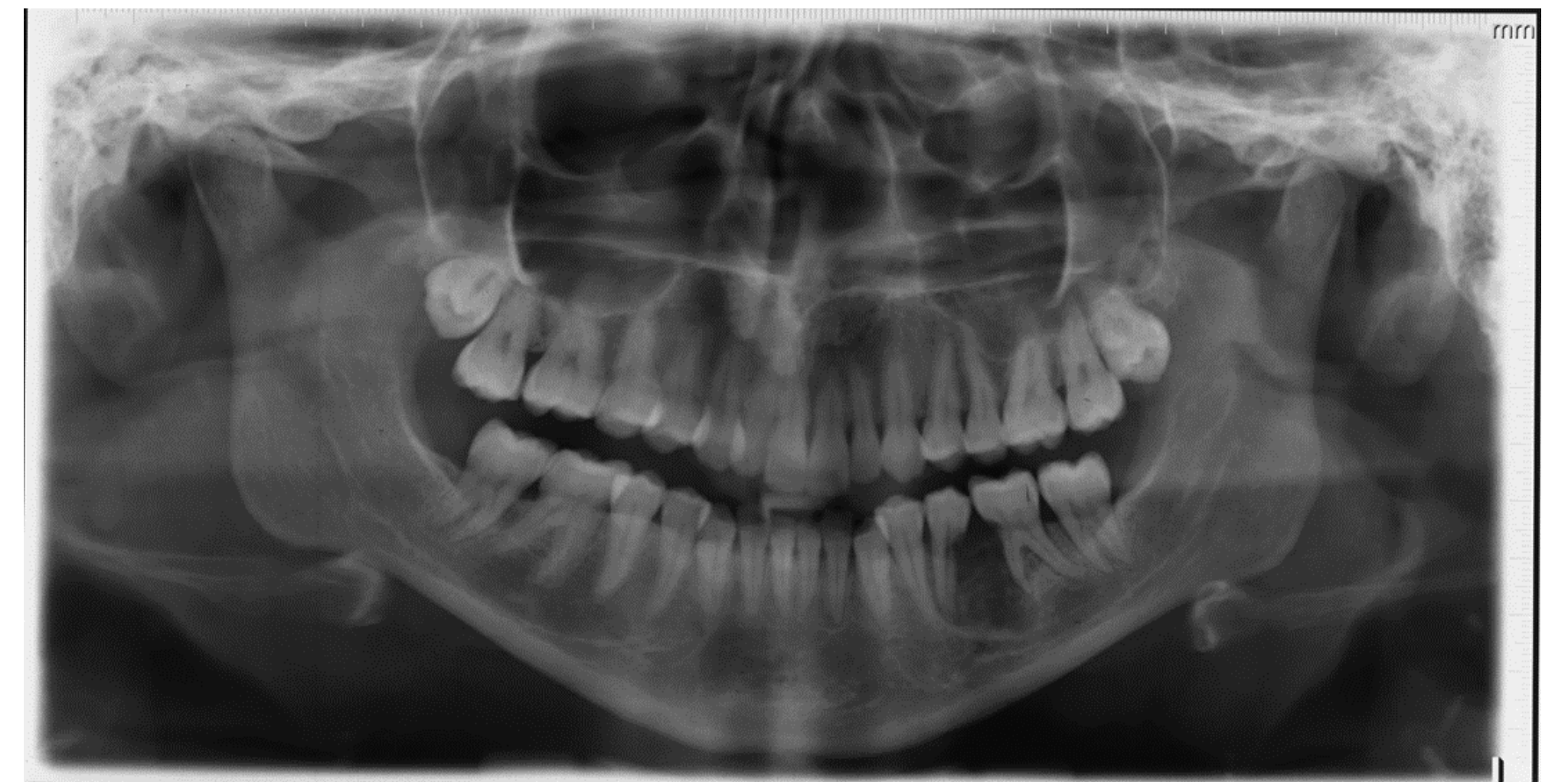
Marsupialization of Jaw Cyst
Radiographic imaging (panoramic X-ray) demonstrates the application of marsupialization for large radiolucent areas in the lower jaw.
Marsupialization Technique
This procedure 'turns the cyst inside out' or exteriorizes it to decompress the lesion, allowing bone to lay down and shrinking the cyst to a manageable size for later removal.
Odontogenic Keratocyst11
Clinical Features
- Wide age range (1-80), peak incidence 10-30 years
- Multiple OKCs are a feature of Gorlin-Goltz syndrome
- OKC appears as a well-defined solitary lesion or as a multilocular, polycystic radiolucency
Histopathology
Histologically, OKC has 4 characteristics:
- Uniform lining of parakeratinized squamous epithelium (6-10 cells thick)
- Palisaded columnar or cuboidal basal cells
- Corrugated layer of parakeratin on its luminal surface
- Lack of rete pegs
Treatment and Prognosis
- Treatment is surgical enucleation
- Recurrence rate of OKC is up to 30%
- Clinicopathological factors predicting high risk for recurrence:
- Large size
- Cortical perforation
- Tooth involvement in the lumen of the cyst
- Presence of daughter cysts
- Recurrence can be reduced with peripheral ostectomy, cryotherapy, or application of Carnoy’s solution
Odontogenic keratocyst (OKC)
 |  |
Bone Lesions
Classification of Bone Lesions12
-
Benign Fibro-Osseous Lesions
- Cemento-osseous lesions
- Fibrous dysplasia
- Cherubism
-
Metabolic Conditions
- Paget disease
- Hyperparathyroidism
-
Benign Tumours and Cysts
- Torus
- Osteoma
- Giant cell lesions (Aneurysmal bone cyst, central giant cell lesion, peripheral giant cell granuloma)
- Traumatic bone cyst
-
Malignant Tumours
- Chondrosarcoma
- Ewing sarcoma
-
Many bone lesions are manifestations of systemic conditions and may not require local surgical treatment.
-
Exostoses (such as Tori) are benign and only require removal if they interfere with prosthetic rehabilitation (e.g., dentures).
Fibro Osseous Lesions13
 |  |
Cemento-Osseous Lesions14
These are benign fibro-osseous lesions of the jaws specifically associated with the apices of teeth. Types include:
-
Periapical cemental dysplasia
-
Florid cemento-osseous dysplasia
-
Often identified radiographically; if the associated tooth is vital, no treatment is typically required.

Juvenile Fibrous Dysplasia15
-
Prevalence: This is the most common monostotic deformity in the head and neck.
-
Progression: Characterized by a slow-growing distortion of the affected bone. Overgrowth typically continues until body growth ceases in the late teens or early twenties.
-
Indications for Treatment: Intervention is performed for cosmesis or when the lesion interferes with vital functions such as sight, breathing, mastication, or speech.
-
Pathologically, normal bone architecture is replaced by fibrous tissue.
-
Clinically, this presents as facial asymmetry and may interfere with vision or breathing depending on the specific bones involved.
Polyostotic Fibrous Dysplasia16
Craniofacial fibrous dysplasia is a form of polyostotic fibrous dysplasia. In this condition, lesions occur in the bones of the jaws and cranium or may be diffused throughout the entire skeleton.
Management is primarily focused on cosmetics or functional interference rather than eradication of the lesion.
Metabolic Conditions17
Hyperparathyroidism

Management of Hyperparathyroidism18
Treatment strategies depend on the underlying cause of the condition:
-
Surgical Intervention
- Parathyroidectomy and subtotal parathyroidectomy are used to correct excessive parathyroid hormone secretions.
-
Medical Management
- Utilized for milder forms in patients over 50 with no progressive bone loss.
- Therapeutic options for patients with end-stage renal disease include calcitriol and hormone replacement to maintain bone mineral density.
-
Pharmacological Support
- Bisphosphonates are indicated for patients at risk of bone fracture.
-
The parathyroid gland regulates calcium; patients with renal failure often develop secondary hyperparathyroidism.
-
Clinical presentation may include "brown tumors" or patchy bone loss.
-
Dental Management for Renal Patients:
- Avoid treatment on hemodialysis days due to heparin use (bleeding risk).
- Be aware of low bone density and potential bisphosphonate use.
Giant Cell Lesions
Central Giant Cell Granuloma Presentation19
Clinical presentation typically includes:
-
Swelling (e.g., on the left side of the mandible).
-
Expansion of the buccal cortex.
-
Mobility of the associated teeth.
-
Diagnostic workup should include vitality testing of adjacent teeth to rule out periapical pathology.
Characteristics and Treatment of Central Giant Cell Granuloma20
-
Pathology: An intraosseous destructive lesion composed of multinucleated giant cells.
-
Clinical Effects: Causes expansion of cortical plates, movement of teeth, and root resorption.
-
Treatment: The standard treatment is curettage.
-
While usually benign, definitive diagnosis requires biopsy.

Aneurysmal Bone Cyst21
-
Classification: A giant cell lesion.
-
Composition: Contains large blood-filled spaces separated by bands of fibrous tissue containing giant cells.
-
Demographics: Occurs in individuals aged 1–30 years, with a peak incidence between 10–19 years.
-
Location: Most lesions are found in the posterior mandible.
-
This is not a "true" cyst as it lacks an epithelial lining; it is an empty, blood-filled space.
-
Radiographically, it appears as a well-defined lesion that scallops between the roots of teeth without causing resorption.
-
Management:
- Primary treatment is curettage.
- Recurrence occurs in approximately 20% of cases, requiring retreatment.
-
Curettage induces bleeding, and the resulting hematoma eventually organizes into new bone.
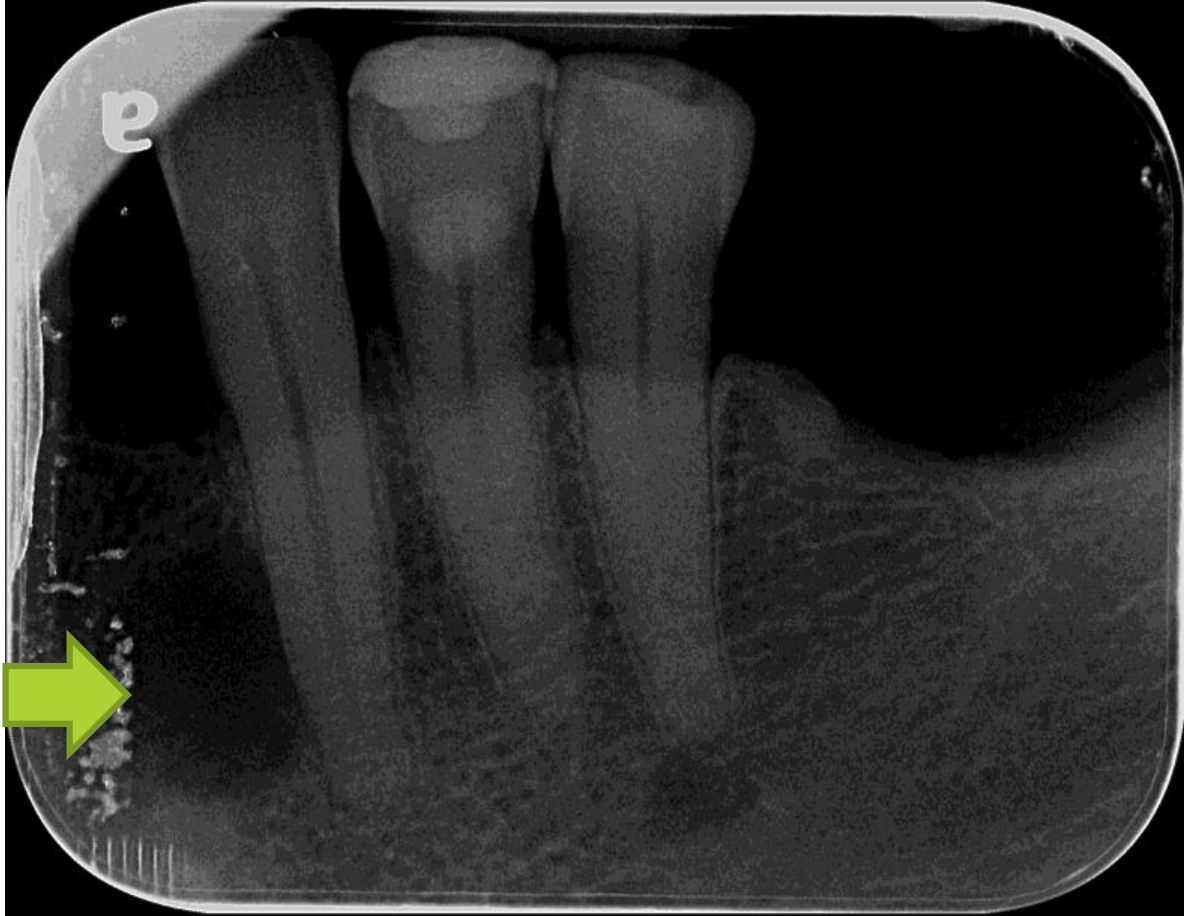
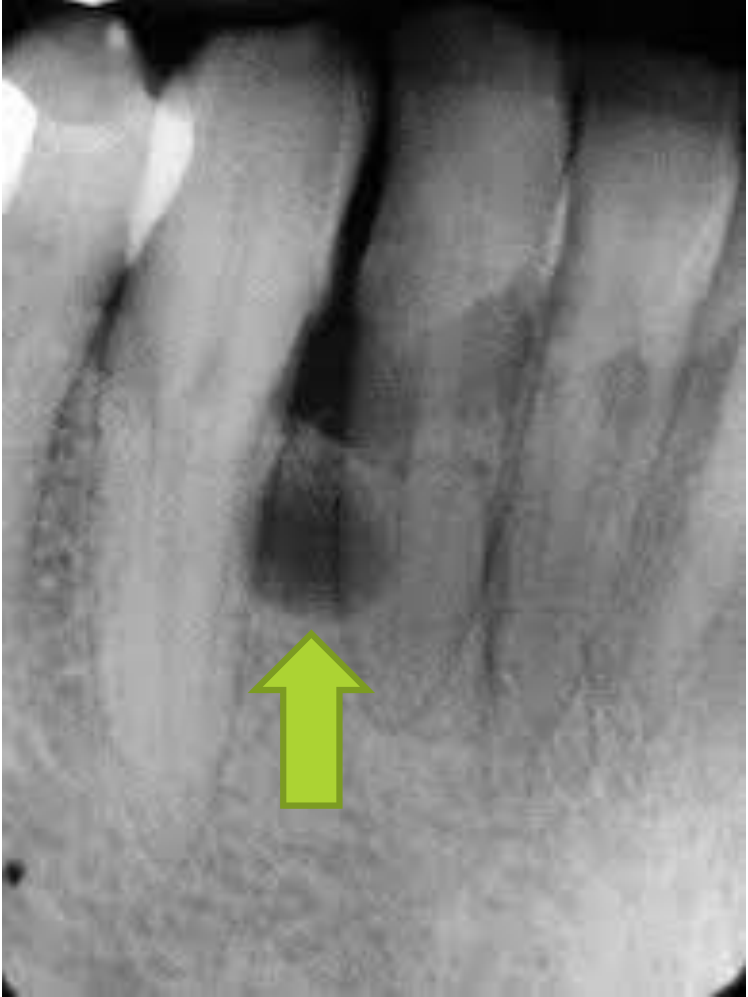
Traumatic Bone Cyst
Clinical Features and Management22
-
Demographics: Typically affects patients under age 20 with a slight female predilection.
-
Presentation: An asymptomatic intraosseous empty cavity, primarily located in the mandible.
-
Histology: Lined by a thin, loose connective tissue membrane.
-
Radiographic Appearance: Appears as a well-circumscribed radiolucency extending between the roots of associated teeth, producing a characteristic scalloped appearance.
-
Treatment: Hemorrhage during biopsy and subsequent curettage usually achieves complete resolution of the lesion.
-
Similar to aneurysmal bone cysts, these are often empty cavities found incidentally on radiographs. Management involves surgical exploration to confirm the diagnosis and stimulate healing.
Avoid Marsupialization
Requires aggressive surgical resection rather than simple marsupialization to ensure all margins are clear.

Odontogenic Tumours
Odontogenic tumours are unique to the jaws and originate from tissue associated with tooth development.
Malignant Odontogenic Neoplasms Characteristics
Malignant odontogenic neoplasms are rare and typically present with aggressive bone resorption and unexplained tooth mobility in a localized area. They are classified based on their tissue of origin:
Classification of Odontogenic Tumours23
- Benign Epithelial Neoplasms
- Ameloblastoma
- Calcifying epithelial odontogenic tumour
- Benign Mixed Epithelial and Connective Tissue Neoplasms
- Ameloblastic fibroma
- Benign Connective Tissue Neoplasms
- Cementoblastoma
- Odontogenic myxoma
- Malignant Odontogenic Neoplasms
- Odontogenic carcinoma
- Primary intraosseous carcinoma
Ameloblastoma
Clinical Characteristics24
- Most common neoplasm of the jaws.
- Neoplasm of odontogenic epithelium.
- Locally invasive but does not metastasize.
- Typically asymptomatic.
- Commonly forms in the posterior mandible.
- Benign but locally aggressive with a high chance of recurrence
 |  |
Radiographic and Pathological Presentation
- Appears as multilocular radiologically.
- Can be unilocular or solid/multicystic type.
- Often described radiographically as having a "soap bubble" appearance
Management
- Treated by curettage or radical excision.
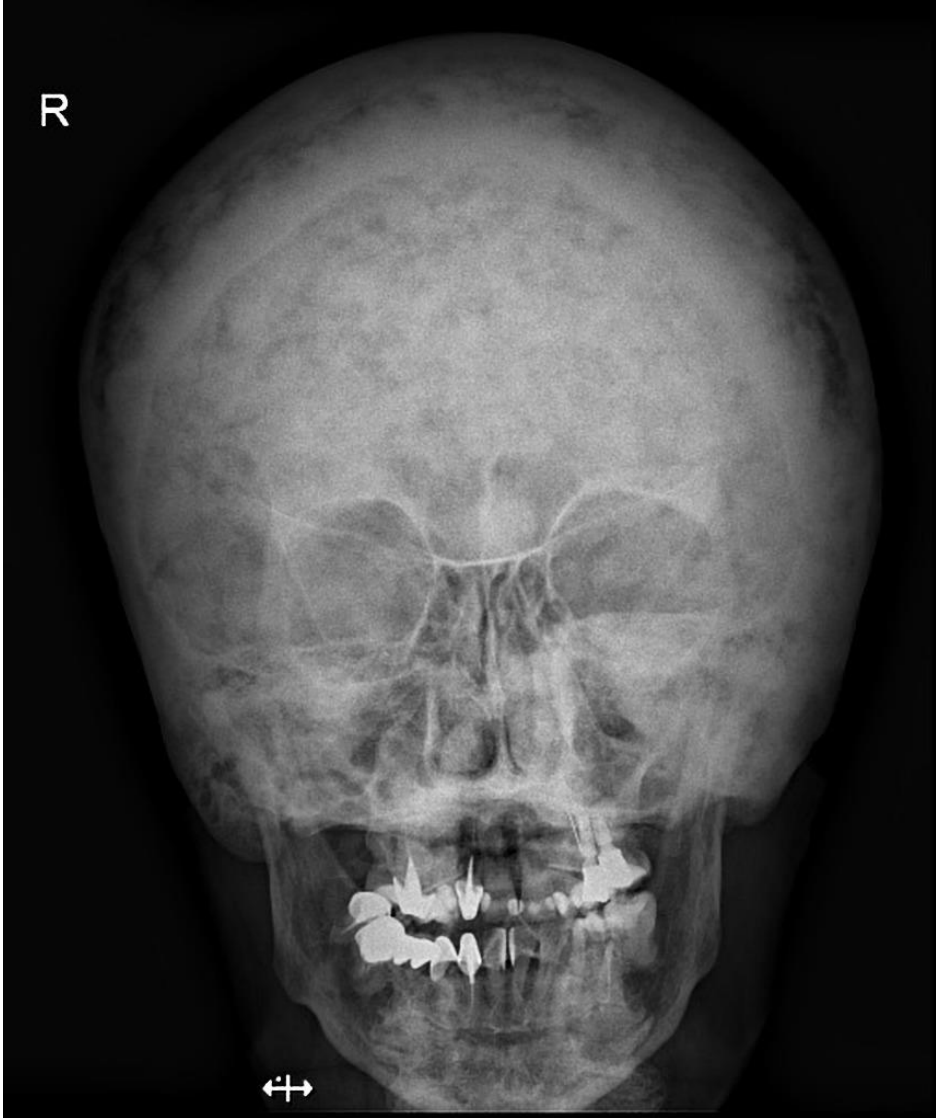
Diagnostic Imaging25
Comprehensive imaging for assessment typically includes:
- OPG (Orthopantomogram): Provides a panoramic radiographic view of the mandible and dental anatomy.
- CT Scan: Offers detailed cross-sectional imaging for surgical planning and assessment of bone involvement.
 |  |
Clinical Significance26
- The solid/multicystic type is the most clinically significant odontogenic tumour.
- The tumour is often locally aggressive and may have a significant impact on patient morbidity and mortality.
Histopathology Case Study
Clinical Details
- Cyst associated with unerupted tooth.
Macroscopic Description
- Right mandible cyst: Multiple tan irregular mucosal fragments measuring from 6mm up to 21mm in greatest dimension.
- Processing: Largest mucosal fragment trisected (Block A); remaining fragments (Block B).
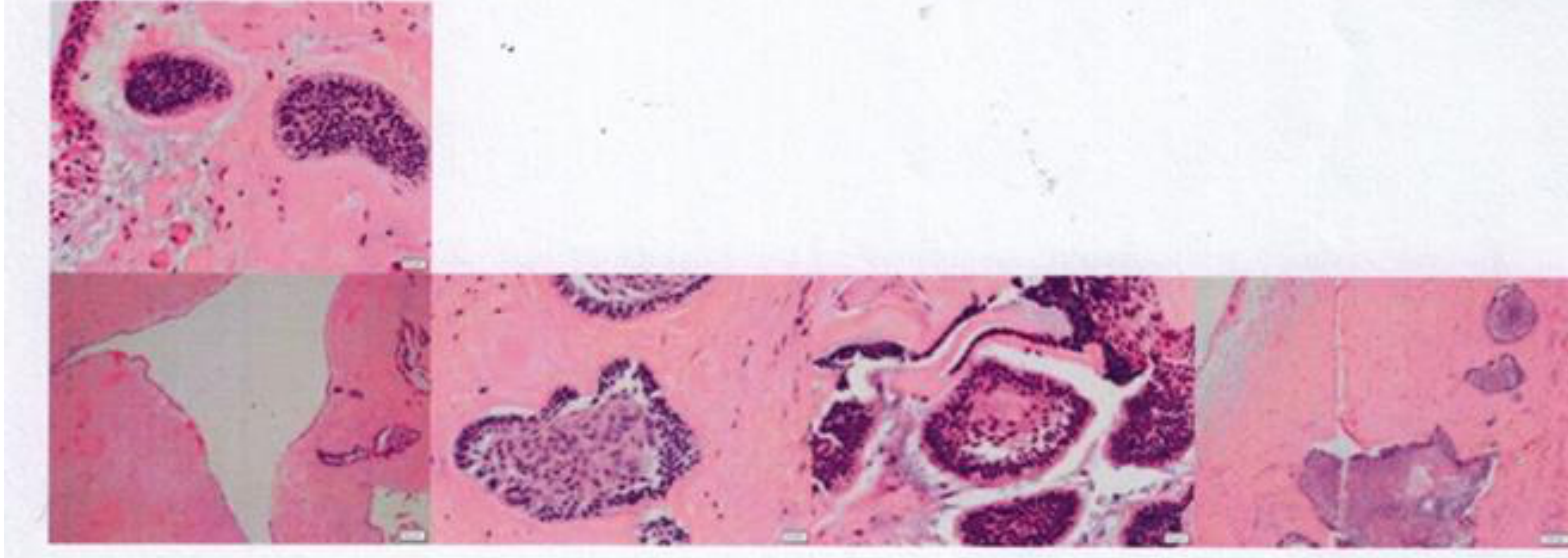
Microscopic Description
- Lesion Architecture: Partially cystic lesion lined by thin epithelium with a thick fibrous wall.
- Epithelial Features: Islands and strands of epithelium showing typical morphological features of follicular ameloblastoma within the connective tissue wall.
- Cellular Detail: Columnar peripheral cells surrounding stellate reticulum-like epithelium with evidence of cystic degeneration.
- Additional Findings: Fragments of calcified tissue and a sparse chronic inflammatory cell infiltrate.
Conclusion
- Mandible: Consistent with solid/multicystic ameloblastoma.
- Recommendation: Correlate with clinical and radiology findings.
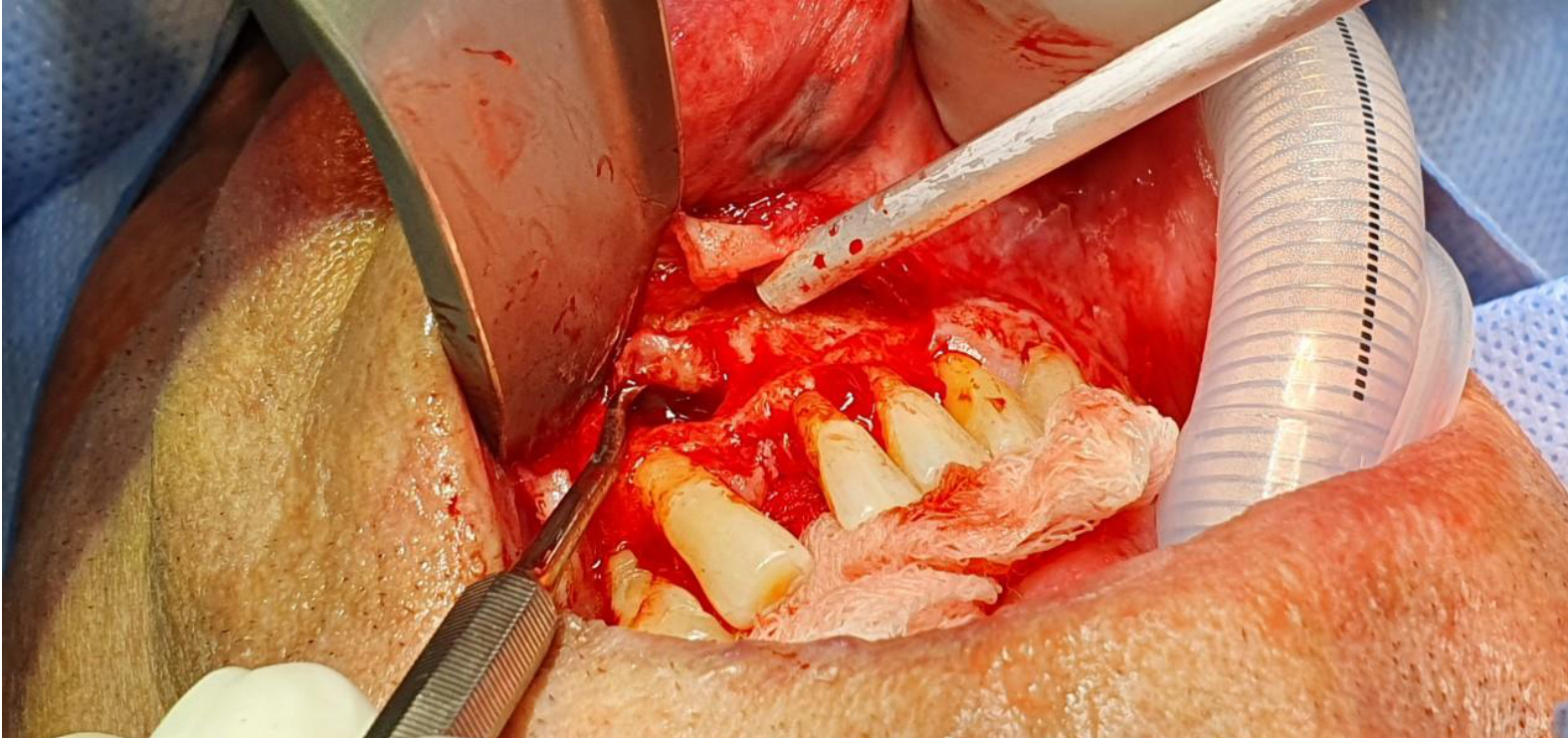
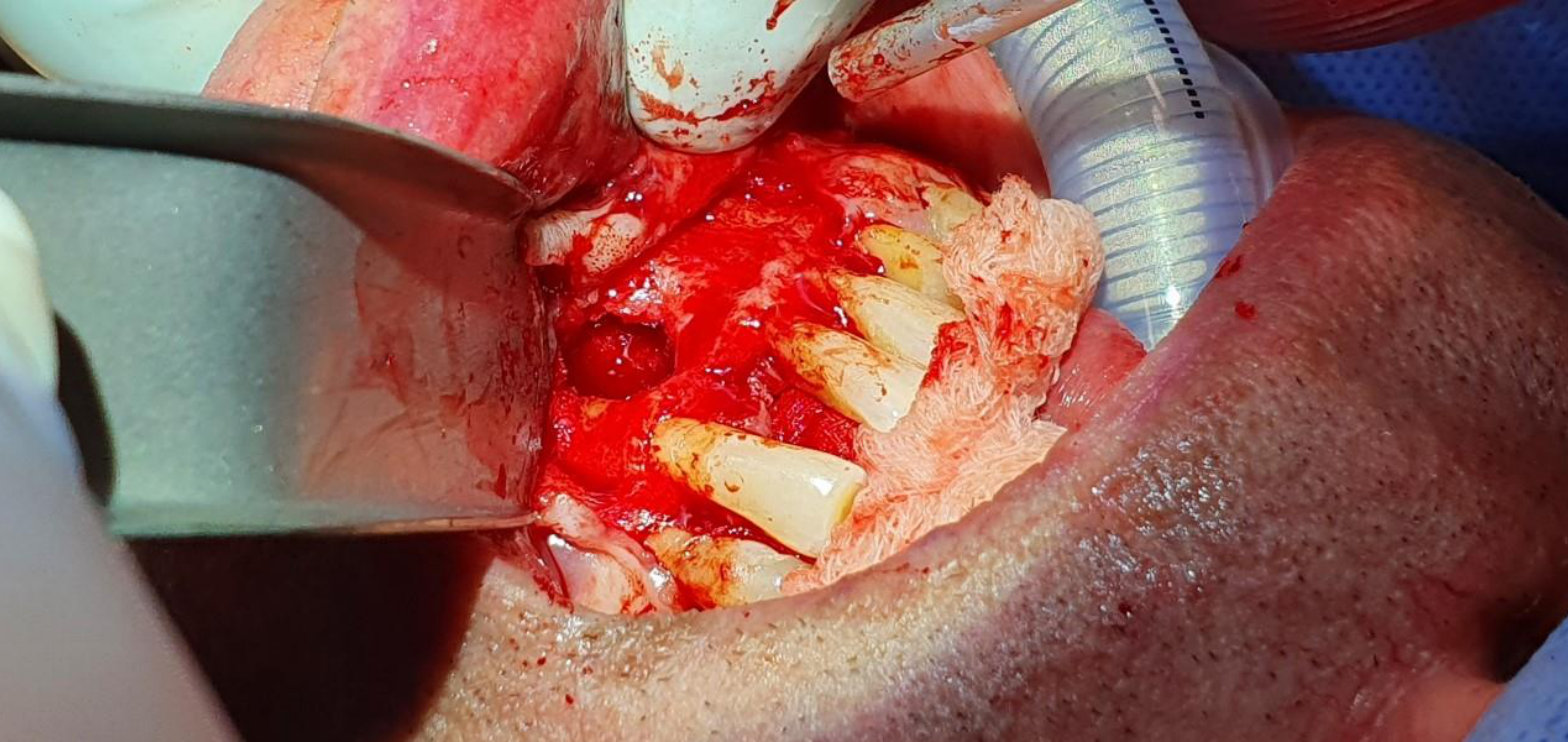
Surgical Management and Reconstruction
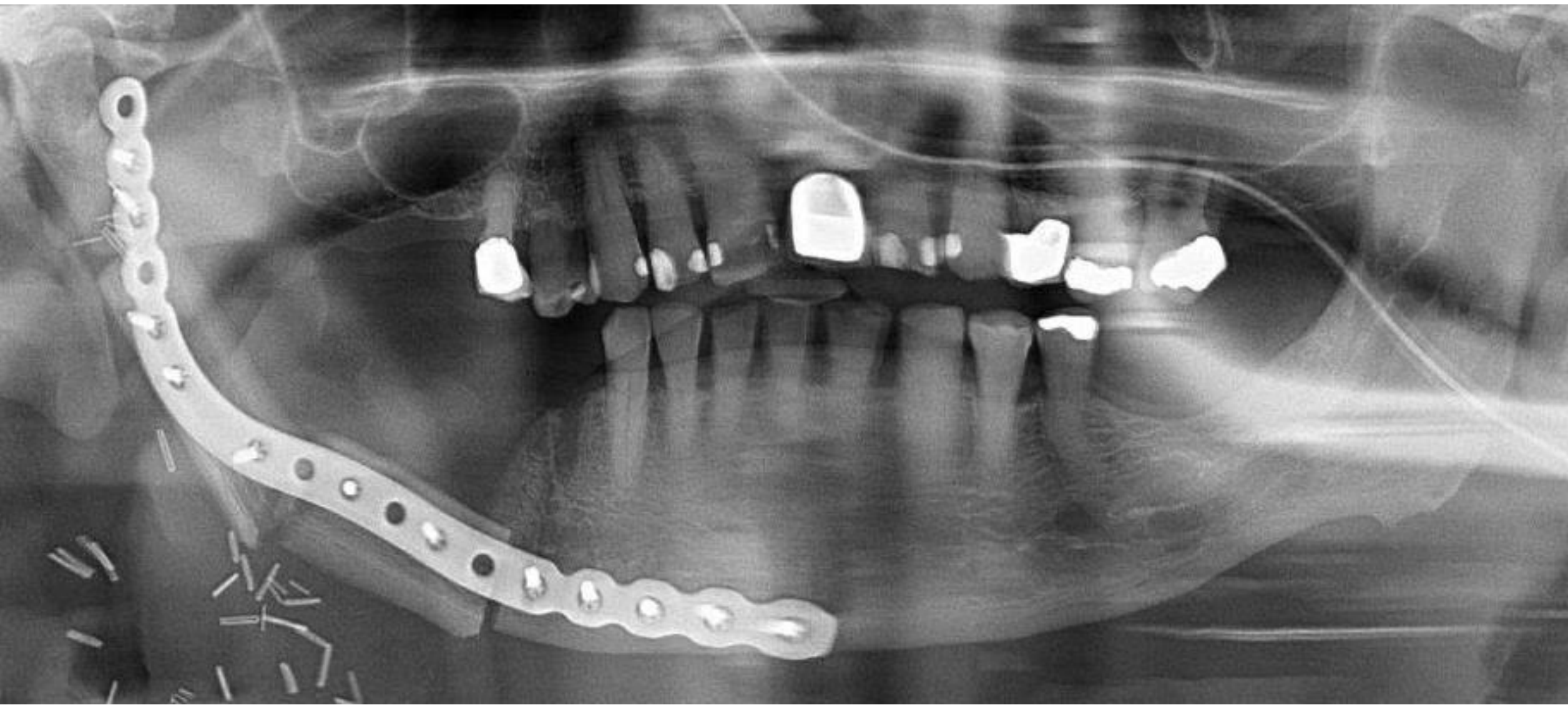
Surgical Intervention27
Management of aggressive odontogenic tumours often requires radical resection and complex reconstruction. This typically involves:
- Radical Resection: Removal of the affected portion of the jaw with appropriate margins to prevent recurrence.
- Reconstruction: Restoration of the mandible using osteotomy techniques, stabilized with surgical plates and screws to maintain function and facial profile.
Case Study: Medication-Related Osteonecrosis of the Jaw (MRONJ)
Scenario: Patients on bisphosphonates or Prolia (denosumab) for osteoporosis or bone malignancies.
Management Protocol:
- For Prolia (administered every 6 months), extractions should ideally be timed when drug levels are at their lowest (just before the next dose)
- Healing Time: A “drug holiday” or waiting period is not enough; the clinician must allow 3 to 6 weeks for the extraction socket to epithelialise and for the hematoma to begin organizing into bone before the next dose is administered
- Risk: Even with careful timing, the risk of necrosis is reduced but not eliminated
Case Study: Paget's Disease of Bone
Pathophysiology: A dysregulation of bone turnover (excessive laying down and resorption) leading to disorganized, “weak” bone and increased alkaline phosphatase.
Systemic Signs:
- Saber Tooth Tibia: Bowing of the legs
- Deafness: Sclerosis of the tiny bones in the middle ear (malleus, incus, stapes) prevents sound conduction
Dental Significance:
- Radiographic Appearance: “Cotton wool” or “woolly” appearance of the skull/jaws
- Hypercementosis: Excessive cementum on roots makes extractions extremely difficult and often necessitates surgical intervention to avoid jaw fracture
- Reconstruction often utilizes bone grafts (e.g., from the fibula/leg) in addition to reconstruction plates
- Prosthetic consideration: Preservation of the lingual sulcus is critical; if soft tissue is stitched too tightly to the tongue, the sulcus is lost, preventing denture wear
Footnotes
-
Original PDF page 1: W3 Surgery and Aggressive cysts, p.1 ↩
-
Original PDF page 2: W3 Surgery and Aggressive cysts, p.2 ↩
-
Original PDF page 3: W3 Surgery and Aggressive cysts, p.3 ↩
-
Original PDF page 4: W3 Surgery and Aggressive cysts, p.4 ↩
-
Original PDF page 5: W3 Surgery and Aggressive cysts, p.5 ↩
-
Original PDF page 7: W3 Surgery and Aggressive cysts, p.7 ↩
-
Original PDF page 6: W3 Surgery and Aggressive cysts, p.6 ↩
-
Original PDF page 8: W3 Surgery and Aggressive cysts, p.8 ↩
-
Original PDF page 9: W3 Surgery and Aggressive cysts, p.9 ↩
-
Original PDF page 10: W3 Surgery and Aggressive cysts, p.10 ↩
-
Original PDF page 17: W3 Surgery and Aggressive cysts, p.17 ↩
-
Original PDF page 18: W3 Surgery and Aggressive cysts, p.18 ↩
-
Original PDF page 22: W3 Surgery and Aggressive cysts, p.22 ↩
-
Original PDF page 19: W3 Surgery and Aggressive cysts, p.19 ↩
-
Original PDF page 20: W3 Surgery and Aggressive cysts, p.20 ↩
-
Original PDF page 21: W3 Surgery and Aggressive cysts, p.21 ↩
-
Original PDF page 23: W3 Surgery and Aggressive cysts, p.23 ↩
-
Original PDF page 24: W3 Surgery and Aggressive cysts, p.24 ↩
-
Original PDF page 25: W3 Surgery and Aggressive cysts, p.25 ↩
-
Original PDF page 26: W3 Surgery and Aggressive cysts, p.26 ↩
-
Original PDF page 27: W3 Surgery and Aggressive cysts, p.27 ↩
-
Original PDF page 28: W3 Surgery and Aggressive cysts, p.28 ↩
-
Original PDF page 29: W3 Surgery and Aggressive cysts, p.29 ↩
-
Original PDF page 30: W3 Surgery and Aggressive cysts, p.30 ↩
-
Original PDF page 31: W3 Surgery and Aggressive cysts, p.31 ↩
-
Original PDF page 32: W3 Surgery and Aggressive cysts, p.32 ↩
-
Original PDF page 33: W3 Surgery and Aggressive cysts, p.33 ↩