Oral Cancer: Resection and Reconstruction
Presenter Information1
Magdalen Foo
Oral Maxillofacial Surgeon
Learning Objectives
Clinical Knowledge and Management2
- Describe the clinical aspect, diagnosis, and management of oral cancer.
- Patient-Centered Care: The focus is not just on managing the cancer itself, but on managing the cancer patient dentally.
- Early Diagnosis: Understanding that early detection significantly improves prognosis.
- Systematic Examination: Developing a consistent clinical routine to ensure no pathology is missed.
Collaborative Care
- Understand the role of the Multidisciplinary Team in head and neck cancer management.
- Understanding the role of the dentist within the broader medical framework, particularly in the Multidisciplinary Team (MDT).
Dental Professional Contributions
- Appreciate the contribution of the dentist pre, during, and post head and neck cancer treatment.
- Functional Restoration: Never underestimate the importance of chewing, speaking, and social eating. The dentist's role is to maintain or restore these functions to improve the patient's quality of life.
- Motivation: Providing psychological support and motivation throughout the treatment journey.
Epidemiology and Diagnosis
National Impact and Prevalence3
 |  |
Head and Neck Cancer Statistics in Australia45
- 7th most commonly diagnosed cancer in Australia
- >5000 new cases of head and neck cancer diagnosed in 2020
- >1000 deaths from head and neck cancer in 2020
- ==Pathological Types: Most oral cancers are primary tumors of the mucosa, with 90% being Squamous Cell Carcinomas (SCC)==
- ==Rare Cases: Occasionally, clinicians may encounter salivary gland cancers or metastases from other parts of the body to the mandible==
 |  |  |
 |  |  |
 |
Clinical Presentation and Signs
Common Indicators6
- Lump in the neck
- Mobile teeth
- Swelling or sore on the lip that won’t heal
- Difficulty or painful swallowing
- Changes in speech
- Bleeding or numbness in the mouth
- White or red patches on the mouth, tongue or gums
- ==Ulcers: Any ulcer that does not heal within two to three weeks must be taken seriously==
- ==Induration: A key sign of malignancy where the ulcer is “sunk in” with firm, heaped-up, irregular edges==
- ==Coloration: Mixed red and white patches (erythroleukoplakia)==
- ==Mobility: Unexplained tooth mobility should be noted if localized to one area while the rest of the mouth is healthy, unlike generalized Periodontitis==
- Unexplained weight loss
Diagnostic Investigations
Diagnostic Procedures7
- Biopsy: Removal of a small amount of tissue sent to a pathologist to determine if cancer cells are present.
- Radiographs: OPG and chest x-ray.
- Imaging: PET, CT, and MRI scans to determine the location, stage, and spread of cancer.
- Endoscopy: A flexible nasal endoscope is used to examine the nose, sinuses, larynx, and pharynx.
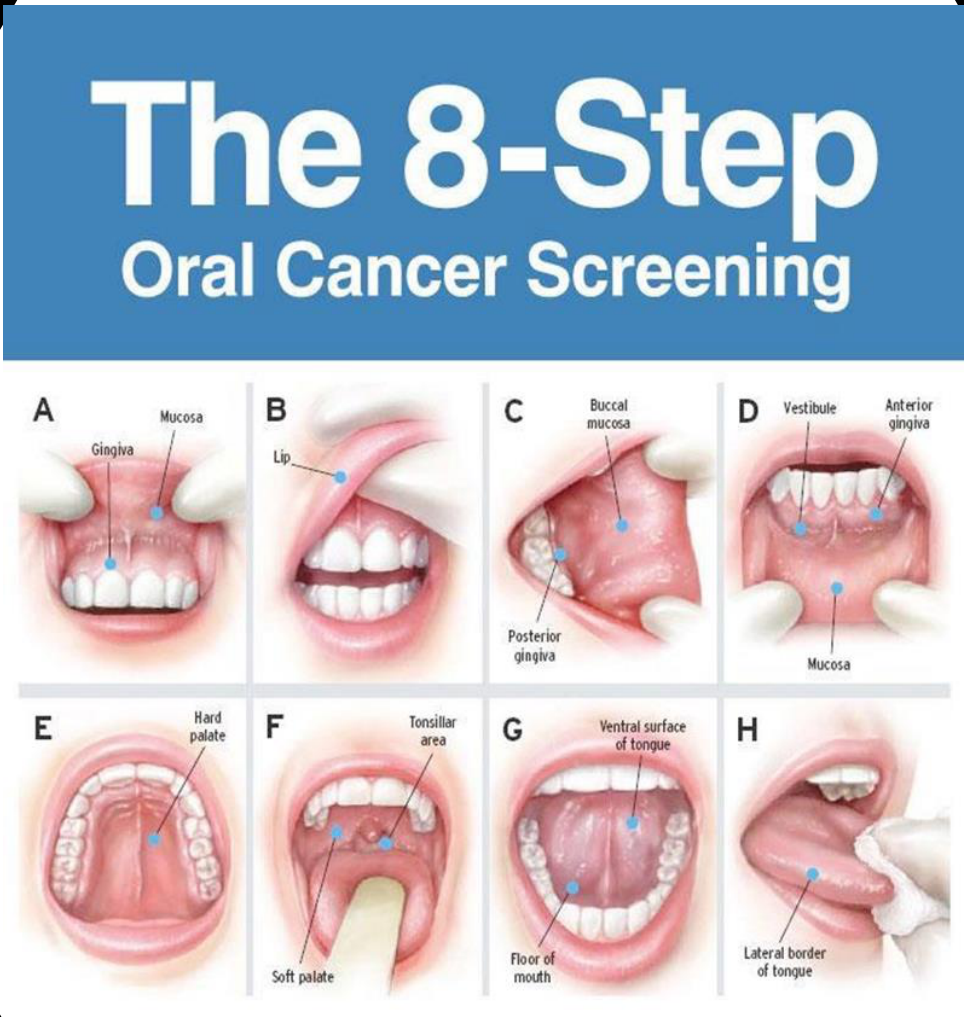
- ==Systematic Oral Exam: Bimanual palpation of cervical lymph nodes; thyroid check (ask patient to swallow water to differentiate from Adam’s apple); visual inspection of high-risk areas including the lateral tongue, ventral tongue (floor of mouth), and lingual sulcus==
- ==Imaging Details: OPG to detect unusual patterns of bone loss or “floating teeth”; CT, MRI, or PET scans for local spread and distant metastasis==
- ==Biopsy - Punch Technique: A highly recommended tool for dentists using a circular cutting rim where adequate depth is more important for diagnosis than width==
- ==Biopsy - Procedure: Steady tissue with gauze, perform one clean punch, detach base with scissors/forceps, and place immediately in formalin==
- ==Biopsy - Clinician Responsibility: The clinician performing the biopsy must label the specimen, provide clinical history to the pathologist, and interpret results (e.g., Mild vs. High-grade Dysplasia)==
Clinical Staging (TNM System)
Purpose and Utility of TNM Staging8
-
Used to designate the extent of disease and to determine the most appropriate treatment for the patient.
-
Provides a uniform staging system to allow for comparisons of results across different types of treatment.
-
==TNM Components: Staging determines the extent of the Tumor (T), involvement of lymph Nodes (N), and presence of Metastasis (M)==
-
==Treatment Planning: The stage directly dictates whether the patient receives surgery alone or surgery combined with adjuvant therapies==
-
Helps predict treatment response and clinical outcomes.
-
Decisions are made in MDT meetings where "two heads are better than one" and all specialists must agree on the treatment trajectory.
Treatment and Management
Every patient diagnosed with oral cancer should be presented at a Multidisciplinary Team (MDT) meeting to ensure comprehensive care.
Multidisciplinary Team Approach
Collaborative Care Planning9
- An integrated team approach involves medical and allied health professionals.
- All relevant treatment options are considered collaboratively.
- An individualized care plan is developed for each patient.
 |  |
Core MDT Members10
- Dentist: Evaluates and treats the mouth and teeth before, during, and after treatment.
- General Practitioner (GP)
- Head and Neck Surgeon
- Radiation Oncologist
- Medical Oncologist
- Radiologist
- Pathologist
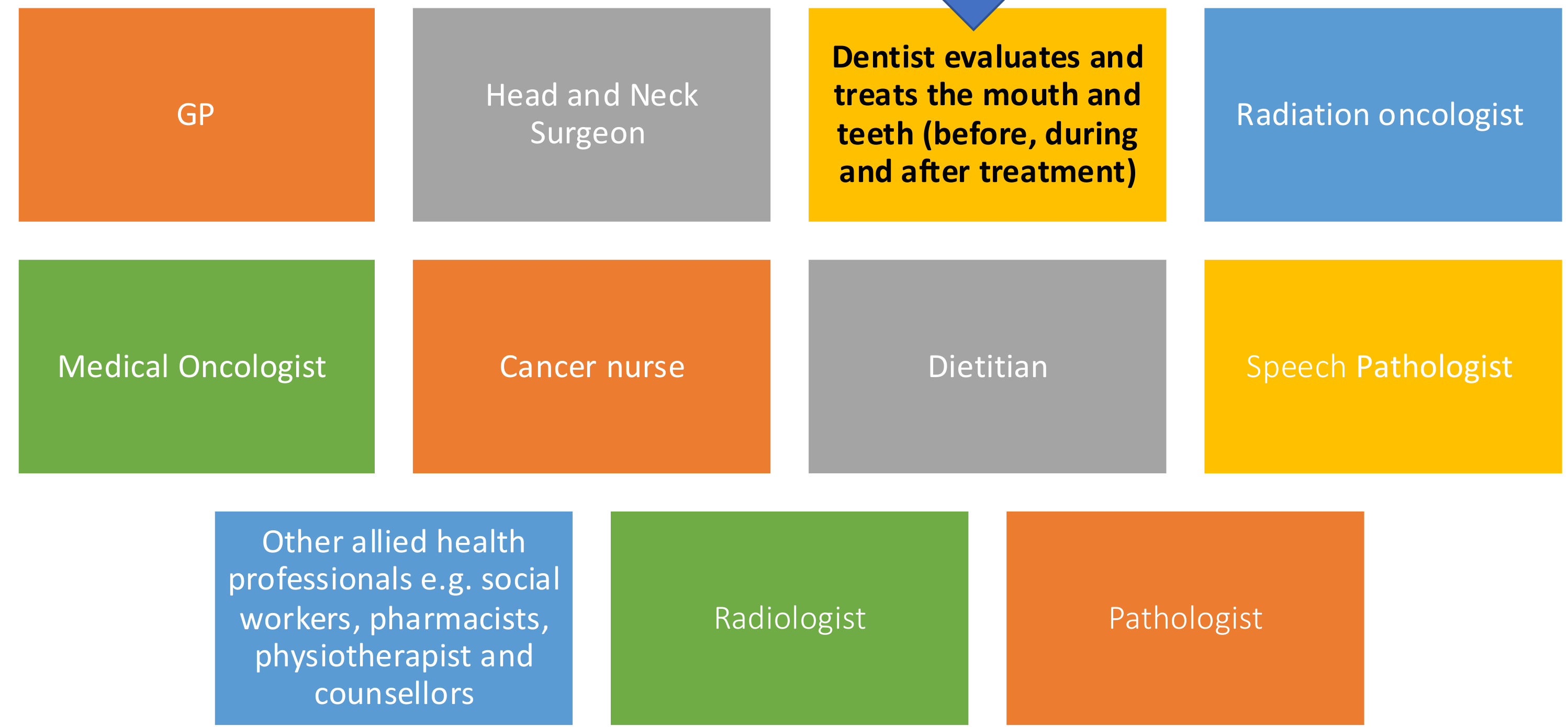
Nursing and Allied Health Support
- Cancer Nurse
- Dietitian
- Speech Pathologist
- Other Allied Health Professionals: Social workers, pharmacists, physiotherapists, and counsellors.
- Speech pathologists and physiotherapists are essential, especially if a significant portion of the tongue is resected.
Treatment Modalities
Primary Treatment Goals11
- Curative: Aimed at eliminating the disease.
- Palliative: Aimed at symptom relief and quality of life.
Surgical Intervention
- Surgery is the primary modality of treatment for oral cancer.
- It involves the removal of the tumor and associated lymph nodes.
- Specifically, surgery involves tumor ablation and usually a neck dissection to remove lymph nodes where the cancer may have spread.
Radiation and Chemotherapy
- Adjuvant Radiotherapy: Utilized based on pathological staging, surgical margins, and nodal status.
- Adjuvant therapy is specifically indicated when pathology shows poorly differentiated cells or confirmed nodal involvement.
- Primary Radiotherapy: Used as a standalone treatment for organ preservation (e.g., oropharyngeal cancers), often concurrently with chemotherapy.
- Chemotherapy: Considered the standard of care in locally advanced head and neck squamous cell carcinoma (SCC).
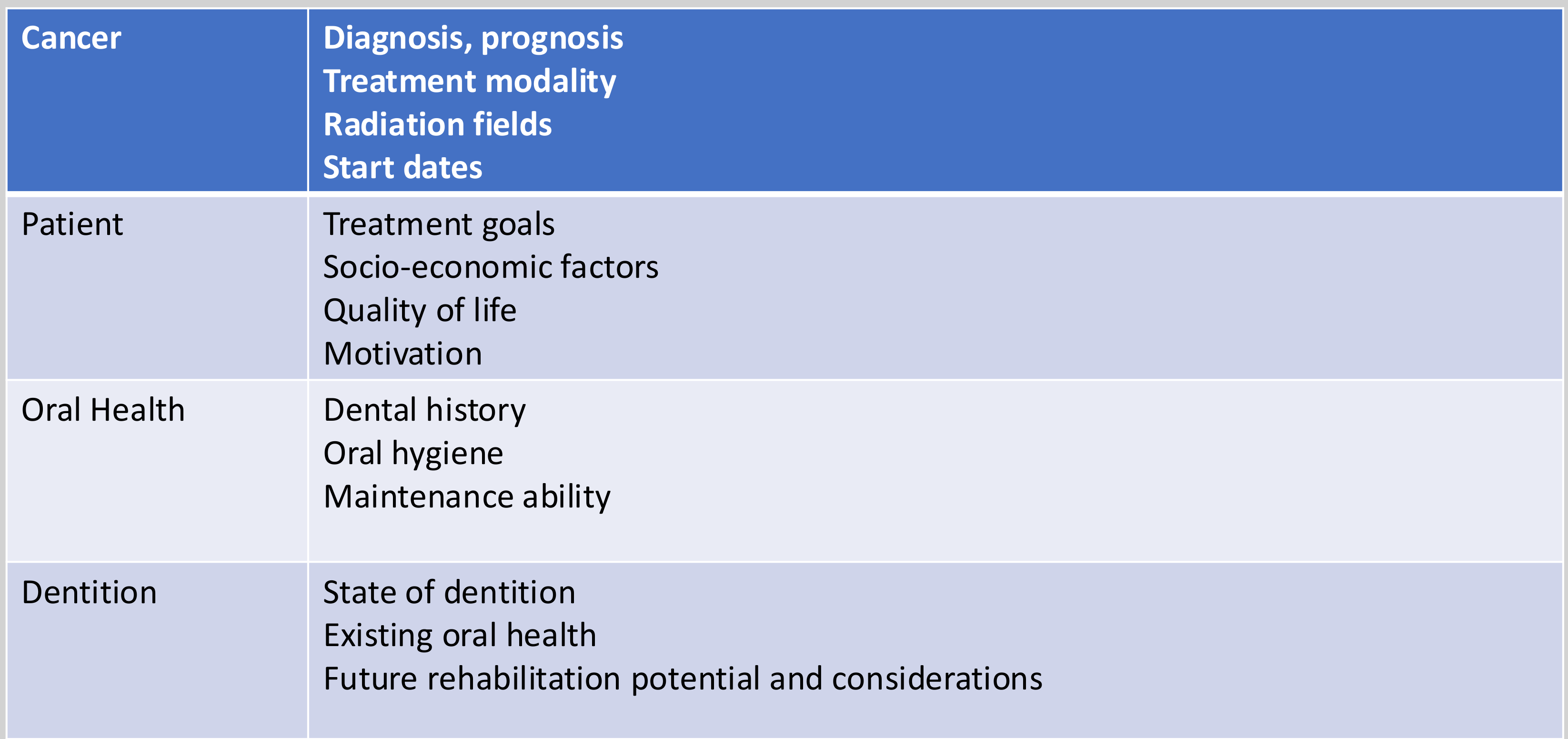
Clinical Assessment Factors12
-
Cancer Factors
- Diagnosis and prognosis
- Treatment modality
- Radiation fields
- Treatment start dates
-
Patient Factors
- Treatment goals
- Socio-economic factors
- Quality of life
- Motivation
-
Oral Health Factors
- Dental history
- Oral hygiene
- Maintenance ability
-
Dentition Factors
- State of dentition
- Existing oral health
- Future rehabilitation potential and considerations
-
Additionally, clinicians must assess fitness for surgery and specific social risk factors including smoking, alcohol, and betel nut use.
Dental Management and Follow-Up
Clinical Considerations During Active Treatment13
- Changes in taste: Common side effect during therapy.
- Oral hygiene maintenance: Managing complications such as mucositis.
- Systemic considerations: Monitoring for pancytopenia and opportunistic infections.
The 50-55 Gray Rule
Teeth in the direct path of high-dose radiation (>55 Gy) with questionable prognosis should be extracted. Teeth receiving <50 Gy may be managed conservatively depending on patient motivation.
- Dental clearance should ideally be completed before radiotherapy starts.
- Be aware that pancytopenia involves low hemoglobin (anemia), low white cells (infection risk), and low platelets (bleeding risk).
Regular Review and Maintenance14
Regular review and maintenance are crucial to ensure the longevity and functionality of dental restorations and procedures. This involves periodic check-ups and necessary adjustments or repairs as needed.
- Manage xerostomia with saliva substitutes (e.g., Oral 7) to prevent rampant decay, and monitor for candidiasis from dry mucosa.
 |  |
Patient Motivation
Motivation is key in encouraging patients to adhere to their post-treatment care guidelines. It involves fostering a positive mindset towards oral health and providing support and education to help patients stay on track with their dental management plan.
Success depends on the patient’s willingness to maintain oral hygiene and quit smoking and alcohol.
Clinical Follow-Up Schedule15
- Initial Phase: 3-monthly reviews focusing on caries and periodontal management.
- Stabilization Phase: Once the oral condition stabilizes, move to 6-monthly recalls.
- These frequent recalls are necessary to monitor for recurrence and manage treatment side effects.
Monitoring and Prevention
- Screening: During recalls, monitor for:
- Mucosal changes
- Xerostomia
- Candidiasis
- Changes in occlusion
Osteoradionecrosis (ORN)
ORN is a lifelong risk. Avoid extractions in irradiated bone if possible; if a tooth must be removed, it is a high-risk procedure.
- Fluoride Therapy: Administer at each recall, including Neutrafluor 5000 toothpaste and fluoride varnish.
Surgical Principles16
Surgery serves as the primary modality of treatment for oral cancer. The surgical process is generally divided into three main components:
- Ablation: The surgical removal of the primary tumor.
- Neck Dissection: The management and removal of regional lymph nodes.
- Reconstruction: The restoration of form and function following tissue loss.
Assessment of Mandibular Involvement
Diagnostic Utility of Imaging17
Research into the utility of CT and MRI for assessing mandibular involvement in oral cavity cancer (Nae et al., 2019) indicates the following:
- Combined CT and MRI have diagnostic utility in detecting mandibular invasion by oral cancer.
- These imaging modalities are associated with a significant false positive rate.
- Identification of bone invasion changes the resection from "soft tissue only" to "bone resection"
Prognostic Factors for Treatment Failure18
Several factors serve as significant predictors for recurrence and treatment failure in oral cancer:
-
Inadequate margins or failure to address the neck nodes are primary drivers of treatment failure
-
Histological Grading: Acts as a significant predictor for treatment failure and recurrence.
-
Tumor Size: A critical prognostic factor in patient outcomes.
-
Lymph Node Status: A key indicator for determining prognosis.
 |  |
Surgical Margins and Outcomes
Margin Definitions and Impact19
Surgical margins are categorized based on the distance between the tumor and the edge of the resected tissue:
- Clear Margins: 5 mm or greater.
- Close Margins: 1 mm to 5 mm.
- Involved (Positive) Margins: Less than 1 mm.
 |  |
 |
Clinical Implications
- Positive surgical margins have a significant negative impact on recurrence rates and overall survival.
- Adjuvant radiotherapy or chemotherapy cannot fully compensate for the presence of close or positive margins.
Determining Adequate Resection Margins20
Systematic evaluation of surgical margins (Nason et al., 2009) suggests the following regarding survival and pathology:
- Patient survival improves with each additional millimeter of clear surgical margin.
- An adequate resection in oral cancer should provide a margin of greater than 3 mm on the permanent pathology section.
- The pathology report confirms if the margins are clear under a microscope
Ablation and Neck Dissection21

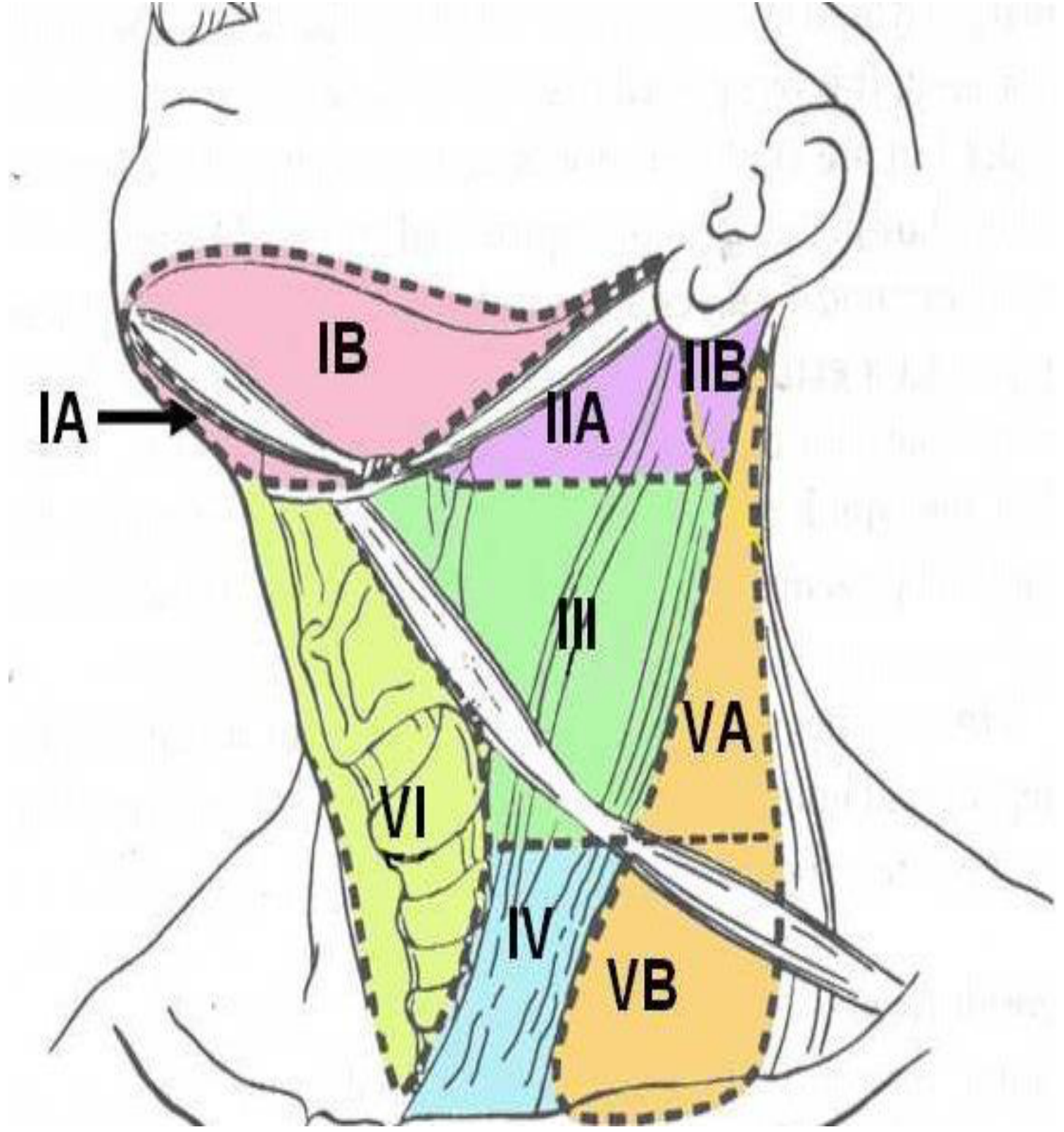
Evolution of Neck Dissection22
- Radical Neck Dissection: First described by Crile in 1906, this procedure involved the removal of all lymphatic structures between the mandible and the clavicles.
- Nodal Stratification: Shah stratified cervical lymph nodes into six group levels to better organize surgical approaches.
- Modern Approach: Current practice favors selective neck dissection, which focuses on the preservation of non-lymphatic structures.
- This approach targets specific levels of the neck to reduce morbidity while ensuring cancer control
The surgical management of oral cancer involves a coordinated approach of tumor ablation and neck dissection to ensure regional control of the disease.
Reconstruction Requirements and Techniques23
- After resection, more than 50% of cases require reconstruction of the resulting defect.
- Reconstruction may involve soft tissue alone or include bony reconstruction.
- Maxillomandibular resection is classified by the extent of bone removal:
- Marginal (Rim) Resection: Removal of a portion of the bone.
- Segmental Resection: Removal of a complete segment of the bone.
- Reconstruction methods vary by the type of resection:
- A marginal mandibulectomy can be reconstructed using local flaps or skin grafts.
- A segmental mandibulectomy requires an osteocutaneous flap.
Reconstruction Techniques
Reconstructive Ladder Hierarchy24
The selection of reconstruction techniques follows a progressive ladder from simple to complex treatments:
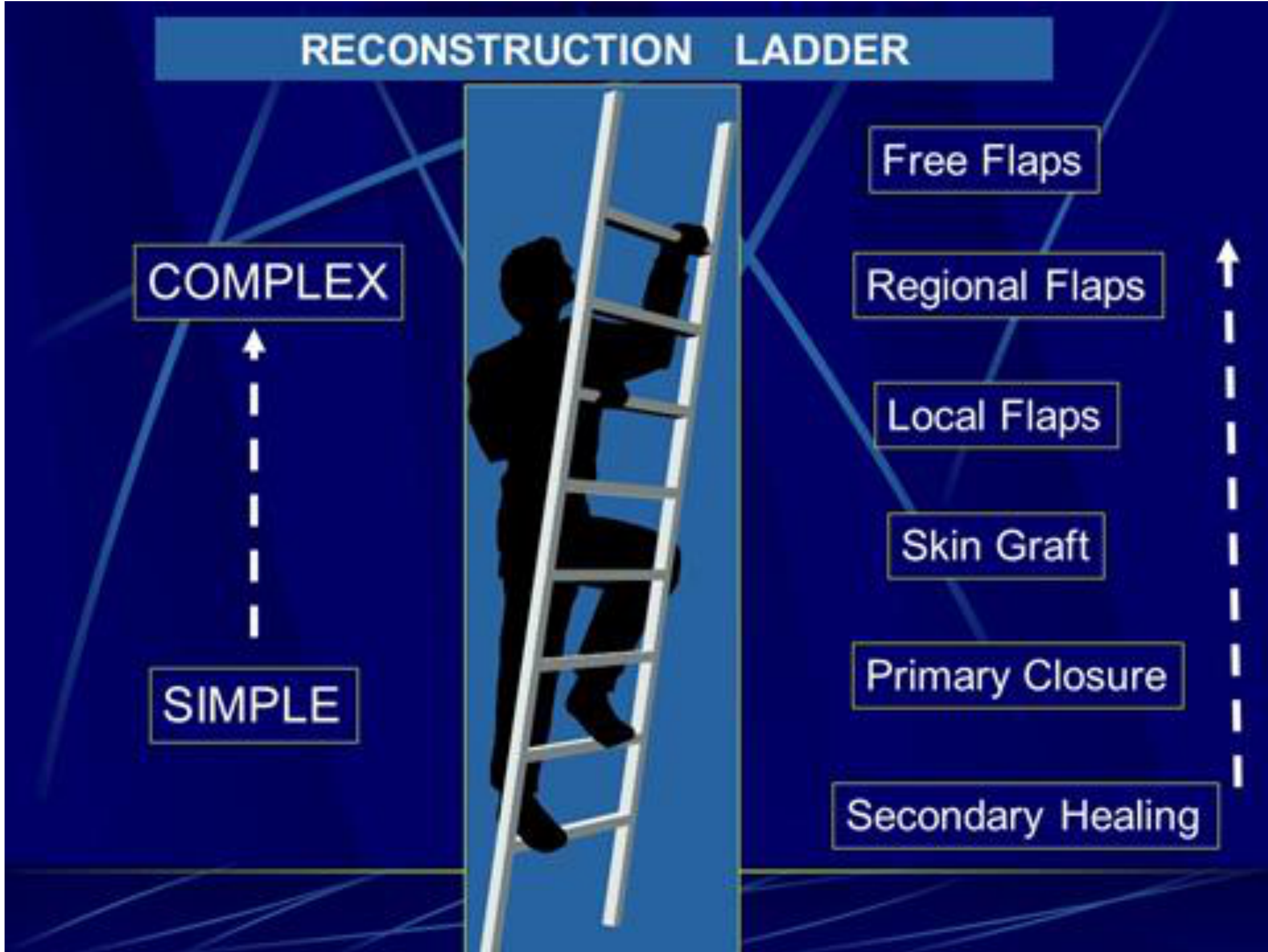
Reconstructive Ladder and Flap Types25
-
Secondary Healing
- Inject and closure
-
Primary Closure
-
Skin Graft
-
Local Flaps
-
Regional Flaps
-
Free Flaps (Restorative Flaps)
-
Primary closure involves stitching the wound together for small defects.
-
Healing by secondary intention allows the wound to close on its own.
-
Regional flaps rotate nearby tissue into the defect.
-
Free flaps detach tissue (skin, muscle, or bone) from a distant site (such as the leg or arm) and reattach blood vessels to the neck.
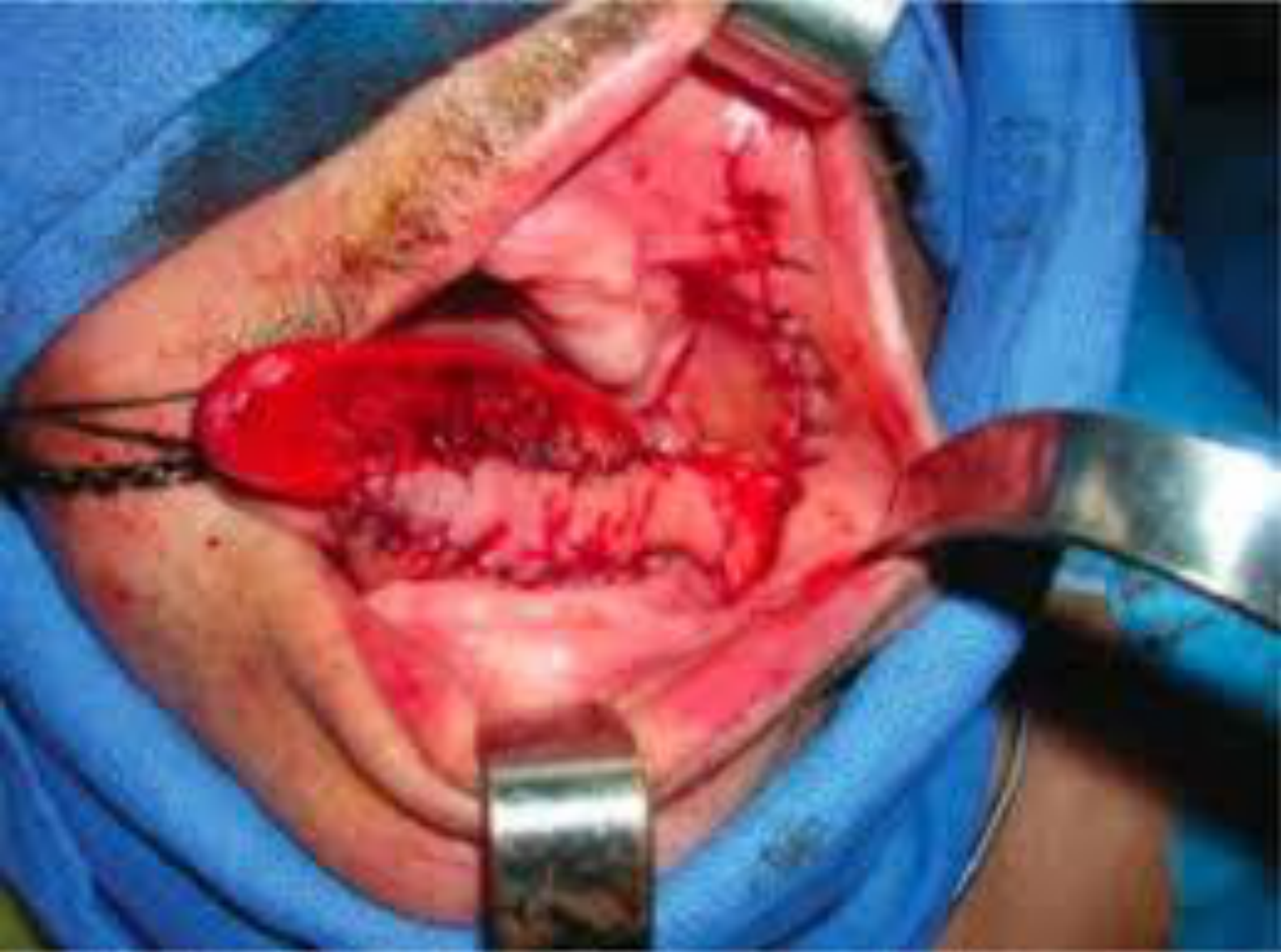
T1 SCC Lateral Tongue26
- Primary closure is utilized for small defects such as T1 Squamous Cell Carcinoma (SCC) of the lateral tongue.
 |  |
Regional Flap Options27
- Temporalis muscle flap: A regional flap used in head and neck reconstruction.
 |  |
History and Progress of Reconstruction
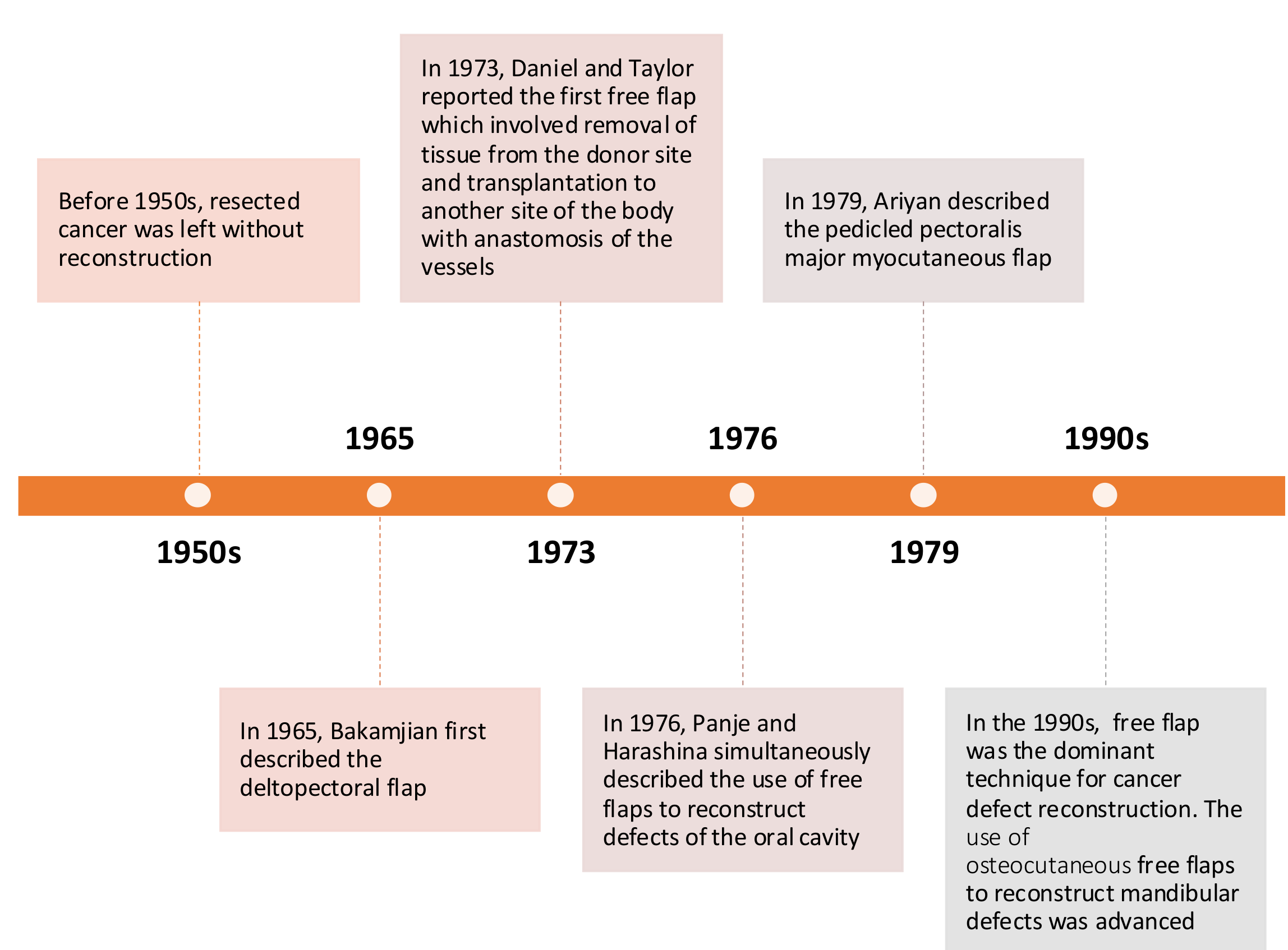
Timeline of Reconstruction Progress28
- Before 1950s: Resected cancer was typically left without reconstruction.
- 1965: Bakamjian first described the deltopectoral flap.
- 1973: Daniel and Taylor reported the first free flap, involving tissue removal from a donor site and transplantation to another site with vascular anastomosis.
- 1976: Panje and Harashina simultaneously described the use of free flaps for oral cavity reconstruction.
- 1979: Ariyan described the pedicled pectoralis major myocutaneous flap.
- 1990s: Free flaps became the dominant technique for cancer defect reconstruction, specifically advancing the use of osteocutaneous free flaps for mandibular defects.
Challenges in Jaw Reconstruction
Impact of Bone Graft Malposition29
Incorrect positioning of bone grafts can lead to significant negative outcomes, including:
- Impaired facial symmetry and appearance
- Loss of structural support
- Compromised occlusal function and masticatory movement
- Difficulties in dental rehabilitation
- Specific complications include a skewed chin position leading to aesthetic dissatisfaction and functional issues such as drooling.

Inferior Jaw Reconstruction Risks30
- Incorrect positioning of the fibular free flap.
- Inadequate fixation of the bone graft.
Digital Surgical Planning and 3D Printing
Evolution of 3D Planning31
- 1981: 3D printing was first described by Hideo Kodama, beginning with the manufacture of 3D plastic models
Virtual Surgical Planning
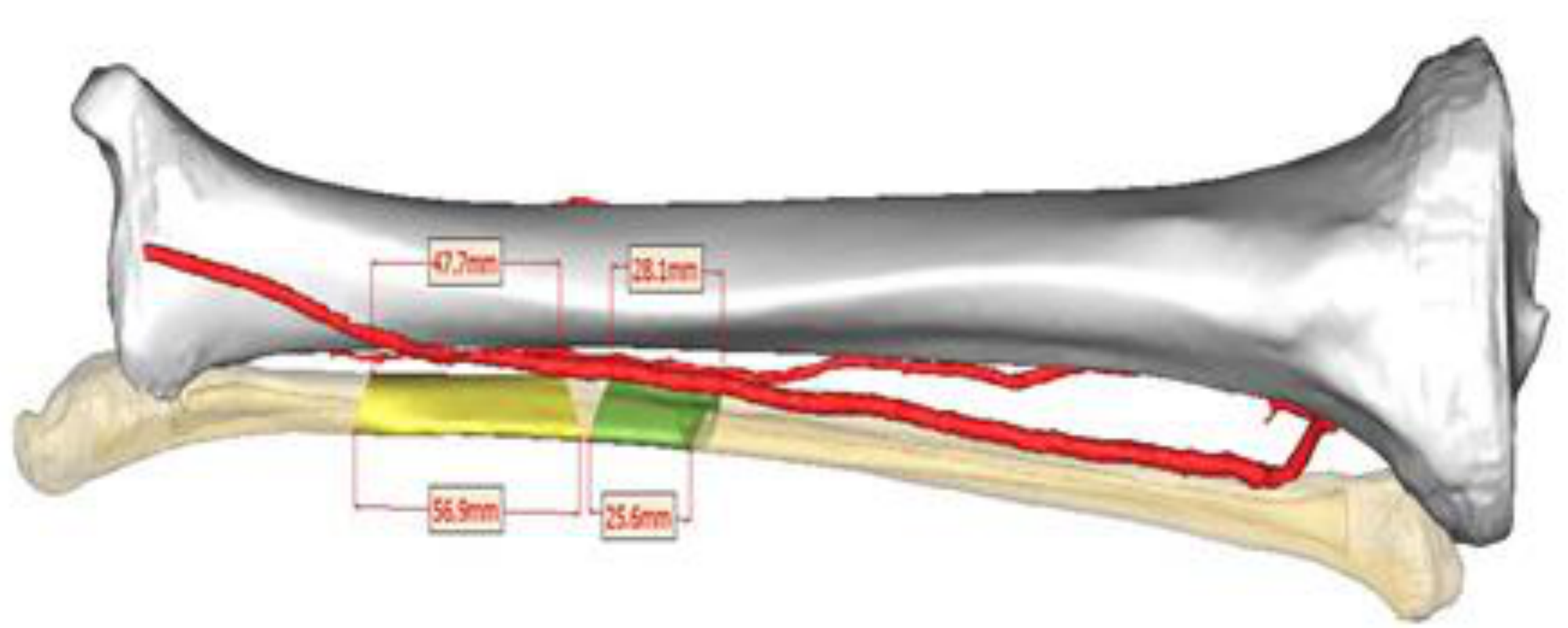
Modern techniques utilize Virtual Surgical Planning (VSP) to improve aesthetic outcomes. 3D-printed surgical guides allow surgeons to cut bone (e.g., from the fibula) at the exact angles needed to recreate the jaw. .
- Advancements: Improved surgical planning has facilitated more precise resection, flap harvesting, and graft positioning.
 |  |
Benefits of Surgical Planning323334
- Increased accuracy
- Improved bone-to-bone contact
- Decreased operating room time
- Lower surgeon stress
- Reduced ischemia time in microvascular free flap reconstruction
- Enhanced treatment outcomes
 |  |
 |
Preoperative Imaging35
- Preoperative high-resolution computed tomography (CT) is essential for planning the resection.

Simulation and Design Tools36
- PROPLAN CMP®: Software used for graft design and stereolithographic guide creation.
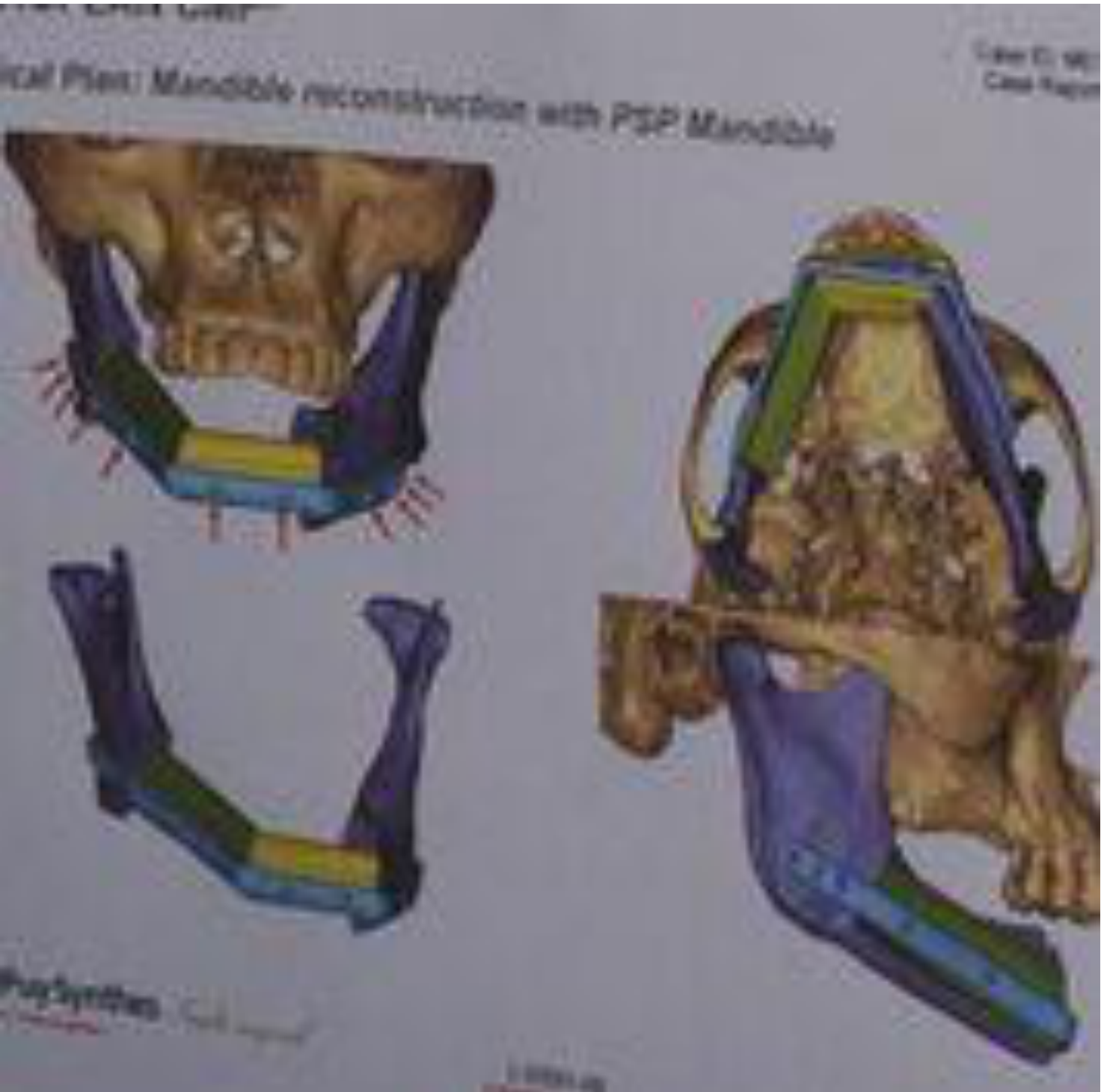
- PSP Mandible: Patient-specific planning for mandible reconstruction designed based on individual patient asymmetry compared to virtual anatomical standards.
 |  |
 |
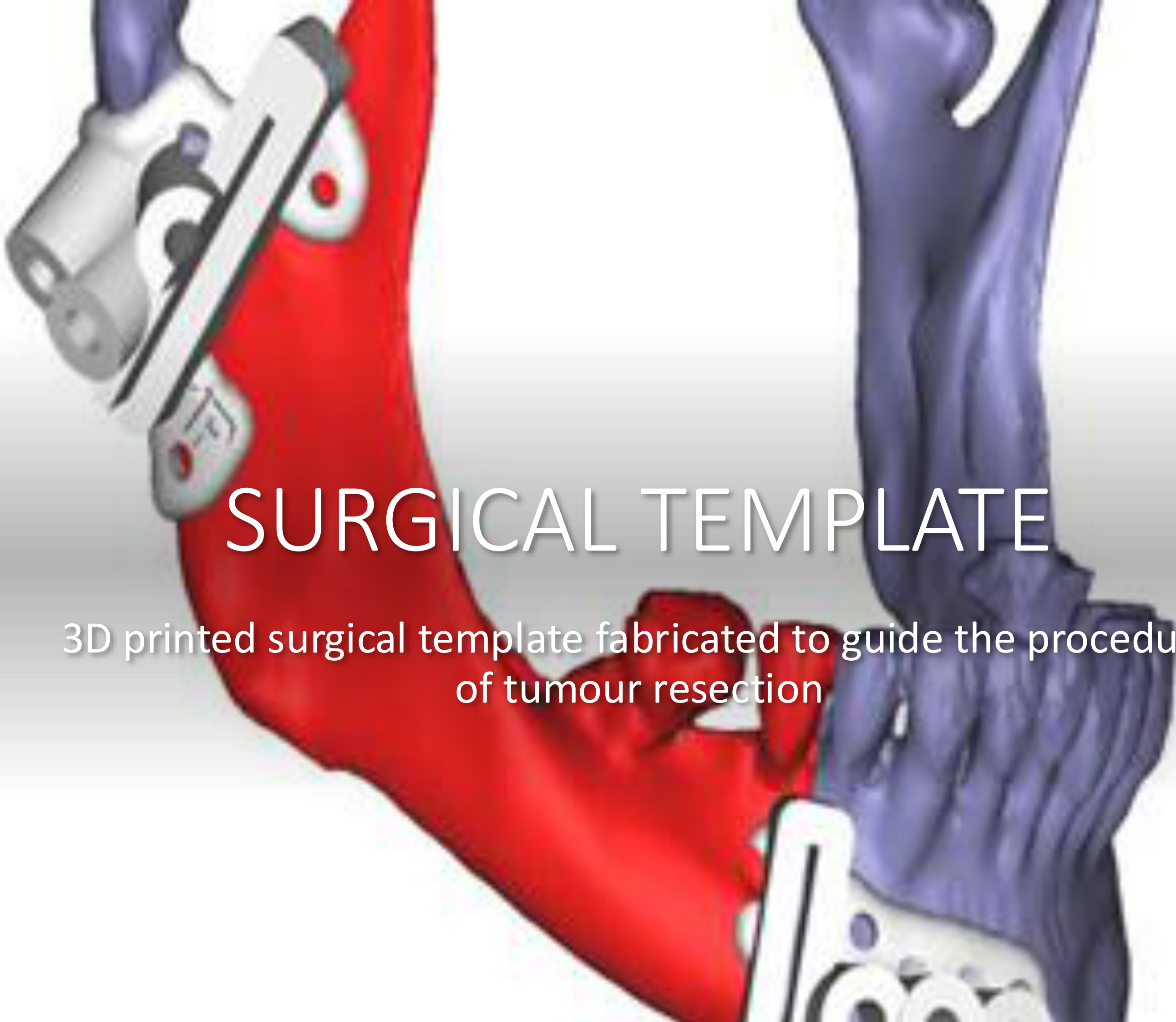
Surgical Templates37383940
- 3D printed surgical templates are fabricated to guide the precise procedure of tumor resection.
 |  |
 |
Post-Operative Documentation41
- Clinical photography is used to document post-operative results and facial symmetry.

Specific Flap Applications42
 |  |
Flap Selection for Facial Defects43
- Scapular Flap: Utilized for reconstruction of the lower lip and chin area.
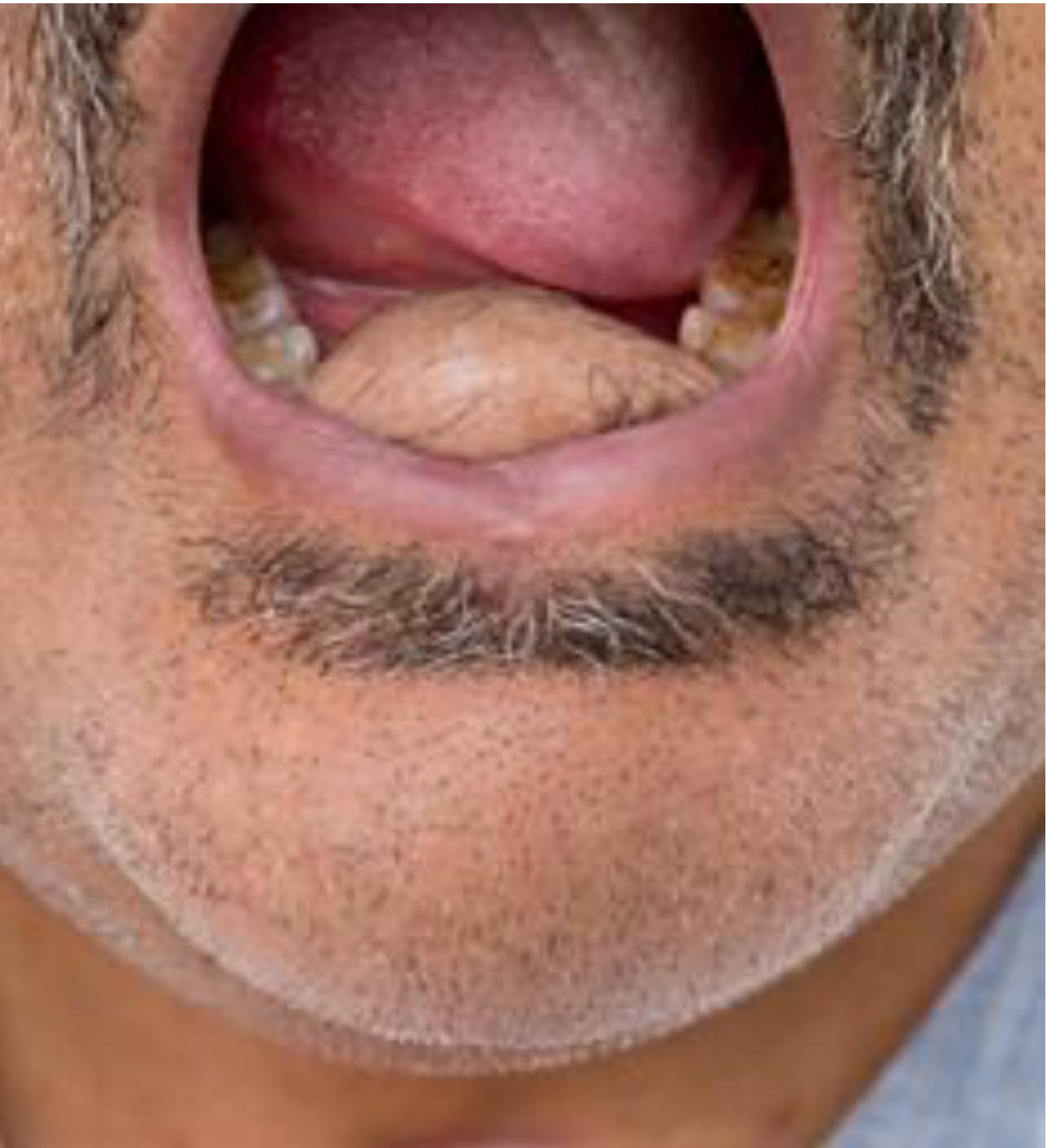
- Osteocutaneous Flap: Applied to complex defects involving the mouth and chin area requiring both bone and skin.
| ![[#]] | ![[#]] |  |
 |  |  |
 |
Pre-operative Assessment44
- Allen’s Test: Performed as part of the pre-operative assessment to ensure adequate collateral circulation before harvesting certain flaps (e.g., radial forearm).

Marginal Mandibulectomy Reconstruction45
- Radial forearm free flap: A common choice for reconstruction following a marginal mandibulectomy
- When only a portion of the mandible is removed, the goal is to maintain the continuity of the jaw..
 |  |
Oral Rehabilitation
Integrated Rehabilitation46
- The final goal of treatment is the successful integration of surgical reconstruction and functional oral rehabilitation.
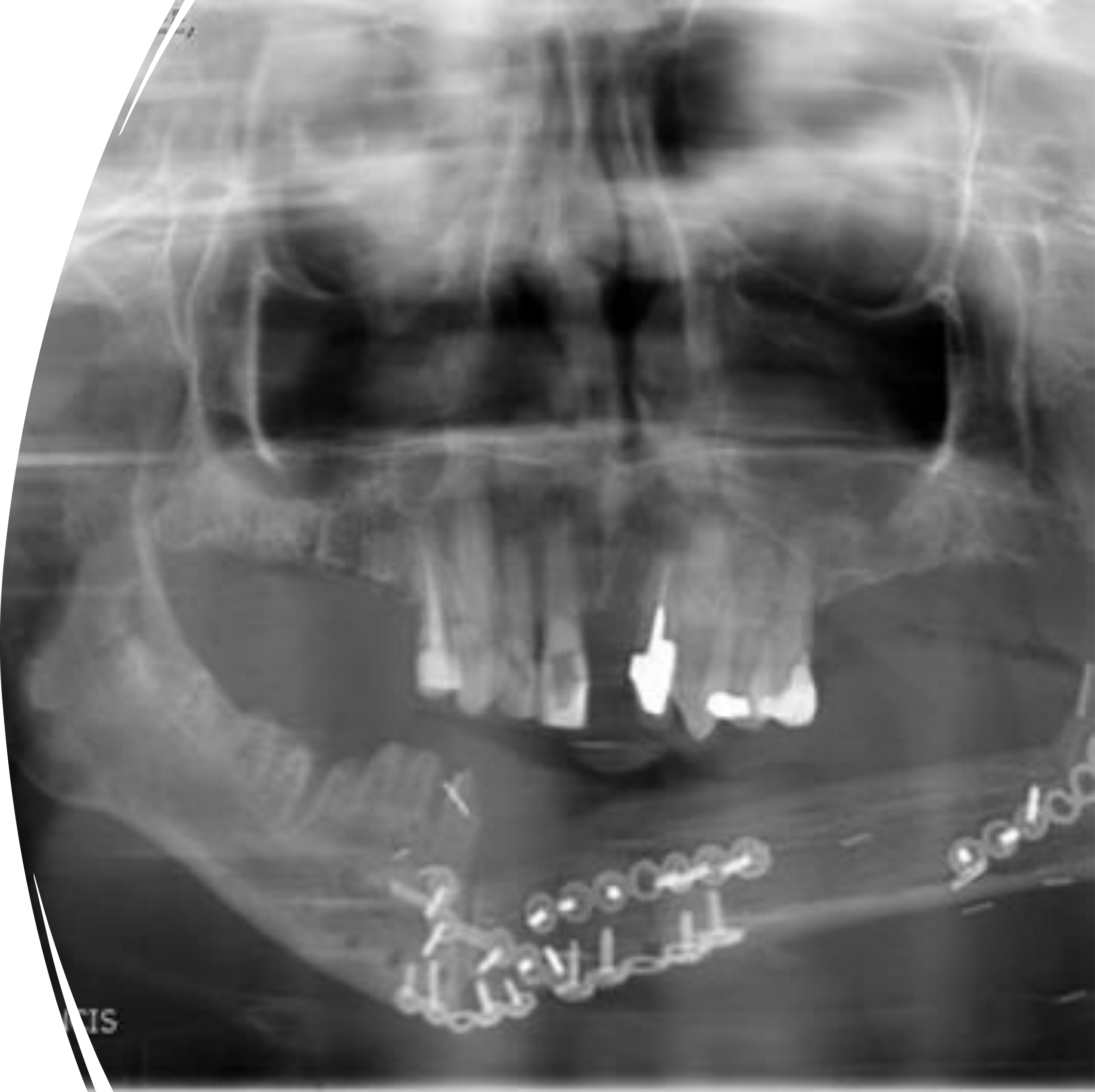
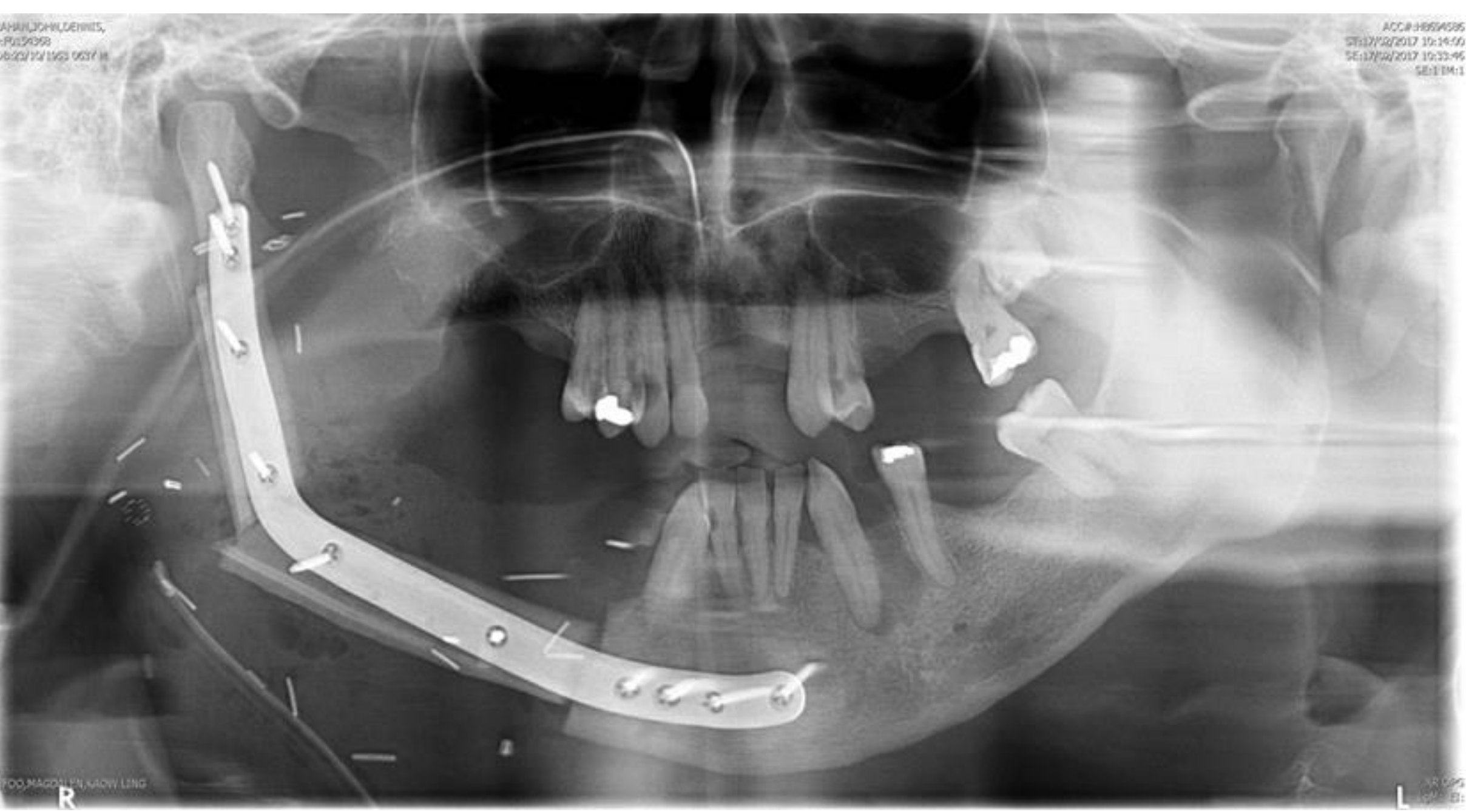
Case Study: Mandibular SCC and Reconstruction
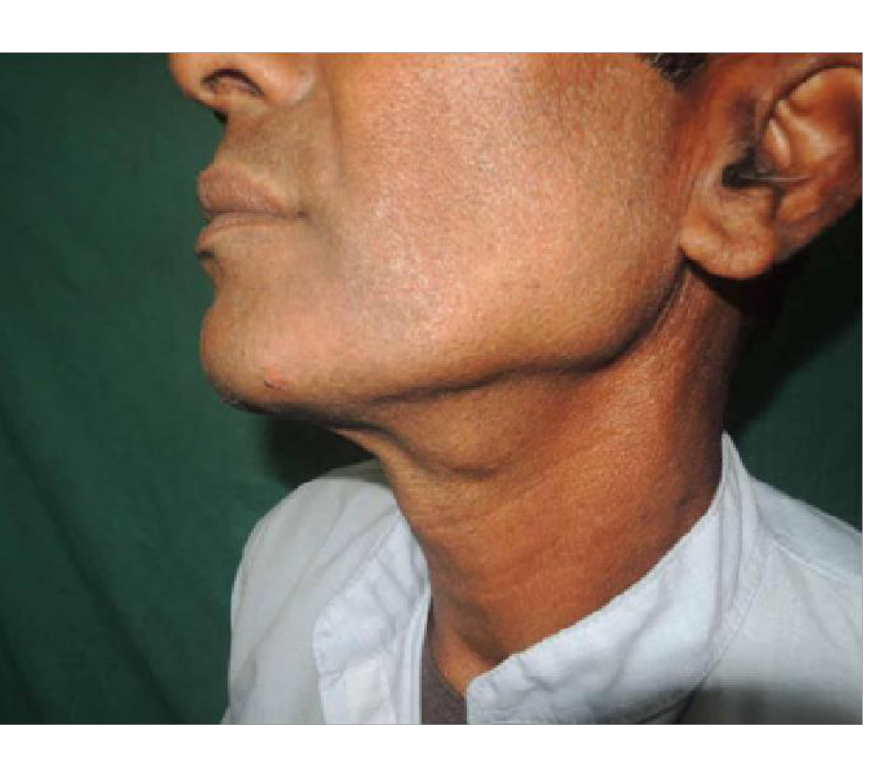
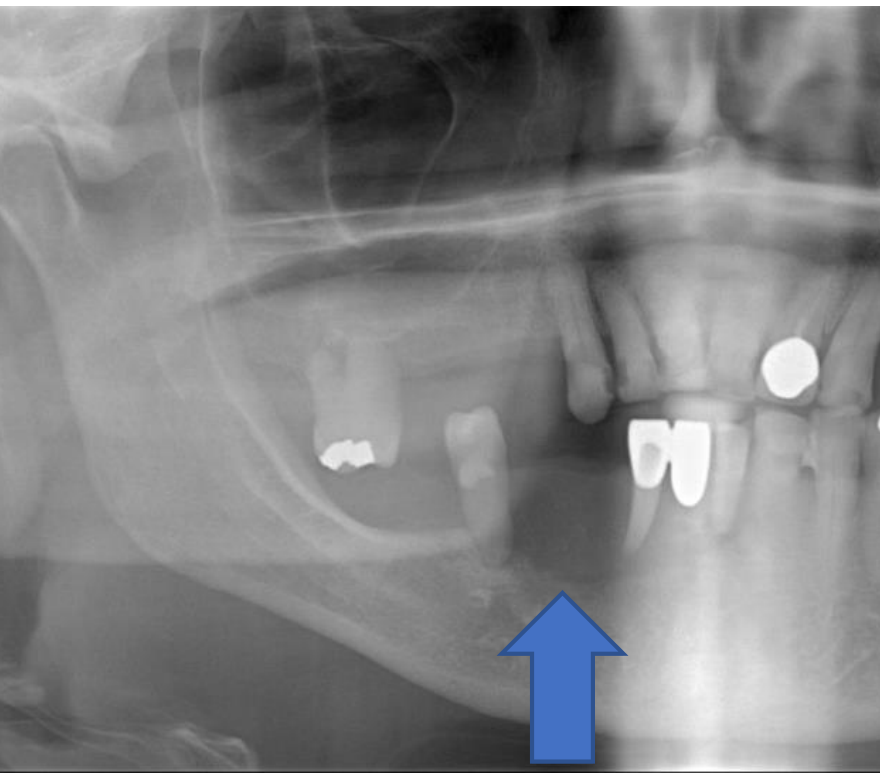
- Presentation: A patient presented with a loose tooth (48) and an unusual red/white patch in the retromolar area.
- Diagnosis: OPG showed localized bone loss (floating tooth appearance). Biopsy confirmed SCC.
- Treatment: The mandible was resected. A leg bone (fibula) was harvested using 3D-printed templates.
- Outcome: The bone was secured with a pre-bent reconstruction plate, resulting in a functional and aesthetic success.
 |  |
Quality of Life Assessment
Quality of Life (QoL) is defined as an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards, and concerns.
Quality of life (QoL) is a subjective measure of the patient's well-being post-surgery.
Definition and Outcome Scores47
 |  |
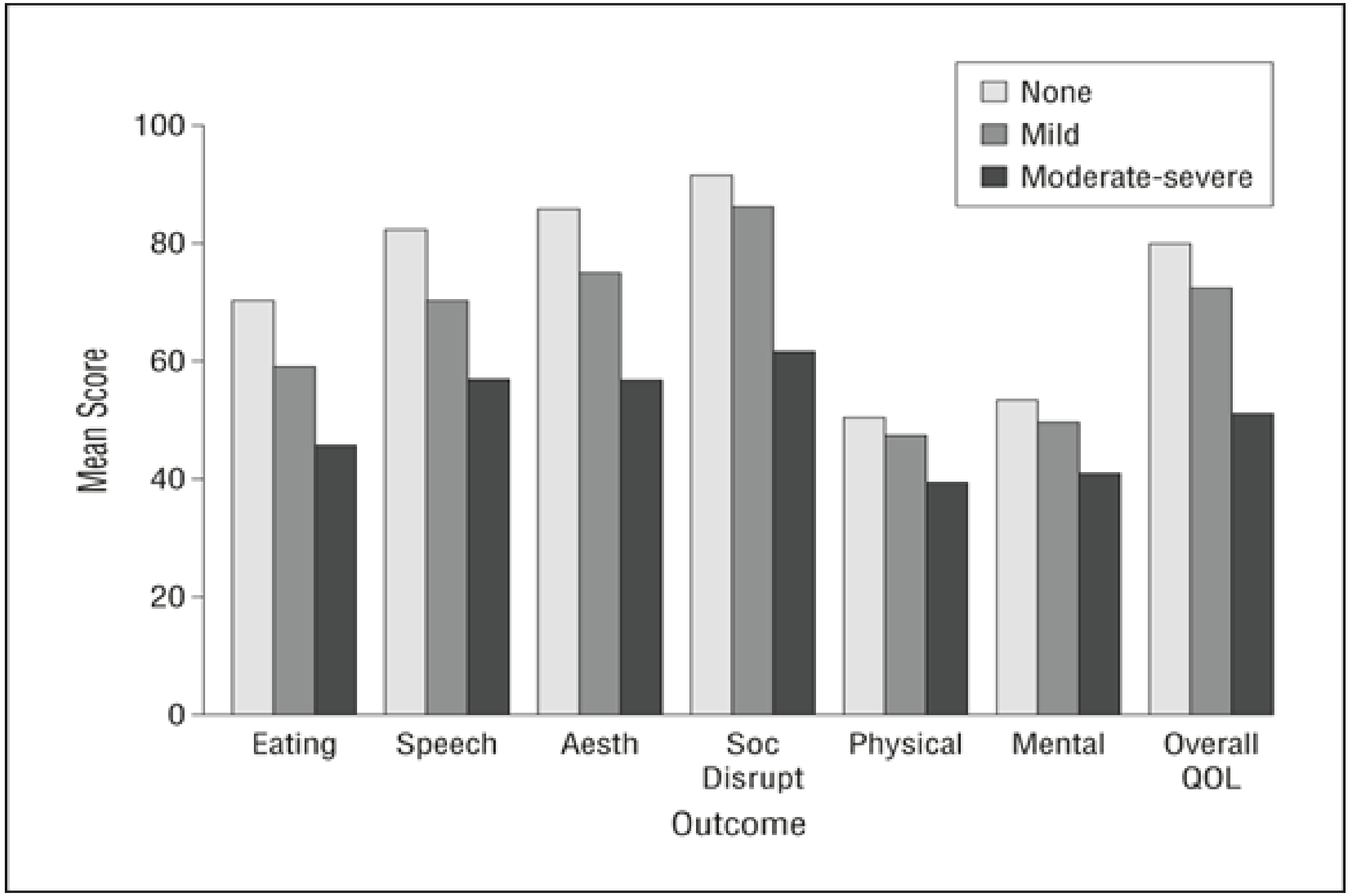
Mean Outcome Scores by Severity48
| Outcome | None | Mild | Moderate-Severe |
|---|---|---|---|
| Eating | ~70 | ~58 | ~45 |
| Speech | ~82 | ~70 | ~56 |
| Aesthetics | ~85 | ~75 | ~56 |
| Social Disruption | ~91 | ~86 | ~61 |
| Physical | ~50 | ~47 | ~39 |
| Mental | ~52 | ~49 | ~40 |
| Overall QOL | ~80 | ~72 | ~50 |
Quality of Life Questionnaires
University of Washington Quality of Life Questionnaire49
The questionnaire assesses the following domains:
- Pain
- Appearance
- Activity
- Recreation
- Swallowing
- Chewing
General Assessment Questions
- Health-Related QoL: Assessment of the month before developing cancer.
- Recent Health-Related QoL: Assessment during the past 7 days.
- Overall QoL: General perception of current quality of life.
Impact of Treatment on Quality of Life
Patient Priorities and Treatment Impact50
- Primary Patient Concerns: The two issues identified as most important to patients are activity and mood.
- Adjuvant Radiotherapy: A greater proportion of patients who received adjuvant radiotherapy rated their Quality of Life as worse than at the time of diagnosis compared to those who received primary surgery only.
- Symptom Burden: The radiotherapy group experienced higher levels of pain and poorer swallowing function.
- ==The “Trampoline” Effect: If a surgeon reconstructs a mouth but fails to create a sulcus (the groove between the cheek and gums), the dentist cannot fit a stable denture. The denture will simply “bounce” on the tissue.==
- ==Clinical Application: Dentists must communicate with surgeons to ensure the reconstruction allows for future prosthetic rehabilitation (e.g., vestibuloplasty or dental implants).==
 |  |
Clinical Application of QoL Data51
- Treatment Planning: Health-related Quality of Life data should be integrated into treatment planning and used to provide more personalized follow-up support.
- Patient Counseling: These results are invaluable when counseling patients with a new diagnosis regarding their expectations and potential outcomes.
 |  |
Footnotes
-
Original PDF page 1: W3 Oral Cancer, p.1 ↩
-
Original PDF page 2: W3 Oral Cancer, p.2 ↩
-
Original PDF page 3: W3 Oral Cancer, p.3 ↩
-
Original PDF page 4: W3 Oral Cancer, p.4 ↩
-
Original PDF page 5: W3 Oral Cancer, p.5 ↩
-
Original PDF page 6: W3 Oral Cancer, p.6 ↩
-
Original PDF page 7: W3 Oral Cancer, p.7 ↩
-
Original PDF page 8: W3 Oral Cancer, p.8 ↩
-
Original PDF page 9: W3 Oral Cancer, p.9 ↩
-
Original PDF page 10: W3 Oral Cancer, p.10 ↩
-
Original PDF page 11: W3 Oral Cancer, p.11 ↩
-
Original PDF page 12: W3 Oral Cancer, p.12 ↩
-
Original PDF page 13: W3 Oral Cancer, p.13 ↩
-
Original PDF page 14: W3 Oral Cancer, p.14 ↩
-
Original PDF page 15: W3 Oral Cancer, p.15 ↩
-
Original PDF page 16: W3 Oral Cancer, p.16 ↩
-
Original PDF page 17: W3 Oral Cancer, p.17 ↩
-
Original PDF page 18: W3 Oral Cancer, p.18 ↩
-
Original PDF page 19: W3 Oral Cancer, p.19 ↩
-
Original PDF page 20: W3 Oral Cancer, p.20 ↩
-
Original PDF page 22: W3 Oral Cancer, p.22 ↩
-
Original PDF page 21: W3 Oral Cancer, p.21 ↩
-
Original PDF page 23: W3 Oral Cancer, p.23 ↩
-
Original PDF page 24: W3 Oral Cancer, p.24 ↩
-
Original PDF page 26: W3 Oral Cancer, p.26 ↩
-
Original PDF page 25: W3 Oral Cancer, p.25 ↩
-
Original PDF page 27: W3 Oral Cancer, p.27 ↩
-
Original PDF page 28: W3 Oral Cancer, p.28 ↩
-
Original PDF page 29: W3 Oral Cancer, p.29 ↩
-
Original PDF page 30: W3 Oral Cancer, p.30 ↩
-
Original PDF page 31: W3 Oral Cancer, p.31 ↩
-
Original PDF page 32: W3 Oral Cancer, p.32 ↩
-
Original PDF page 33: W3 Oral Cancer, p.33 ↩
-
Original PDF page 34: W3 Oral Cancer, p.34 ↩
-
Original PDF page 35: W3 Oral Cancer, p.35 ↩
-
Original PDF page 36: W3 Oral Cancer, p.36 ↩
-
Original PDF page 37: W3 Oral Cancer, p.37 ↩
-
Original PDF page 38: W3 Oral Cancer, p.38 ↩
-
Original PDF page 39: W3 Oral Cancer, p.39 ↩
-
Original PDF page 40: W3 Oral Cancer, p.40 ↩
-
Original PDF page 41: W3 Oral Cancer, p.41 ↩
-
Original PDF page 45: W3 Oral Cancer, p.45 ↩
-
Original PDF page 42: W3 Oral Cancer, p.42 ↩
-
Original PDF page 43: W3 Oral Cancer, p.43 ↩
-
Original PDF page 44: W3 Oral Cancer, p.44 ↩
-
Original PDF page 46: W3 Oral Cancer, p.46 ↩
-
Original PDF page 47: W3 Oral Cancer, p.47 ↩
-
Original PDF page 48: W3 Oral Cancer, p.48 ↩
-
Original PDF page 49: W3 Oral Cancer, p.49 ↩
-
Original PDF page 50: W3 Oral Cancer, p.50 ↩
-
Original PDF page 51: W3 Oral Cancer, p.51 ↩