Case 2: Gingival Recession and Abnormal Lucencies
Patient Presentation[^9]
- Chief Complaint: The patient is primarily concerned with the aesthetic appearance of their gingival recession.
- ==Symptoms:==
- No pain or discomfort reported.
- No history of trauma.
- ==Clinical Findings:==
- ==Vitality: All lower anterior teeth tested vital.==
- ==Caries/Fractures: No evidence of caries or tooth fractures.==
- ==Periodontal Status: Minor periodontal bone loss and presence of calculus on enamel surfaces.==
==Radiographic Assessment==
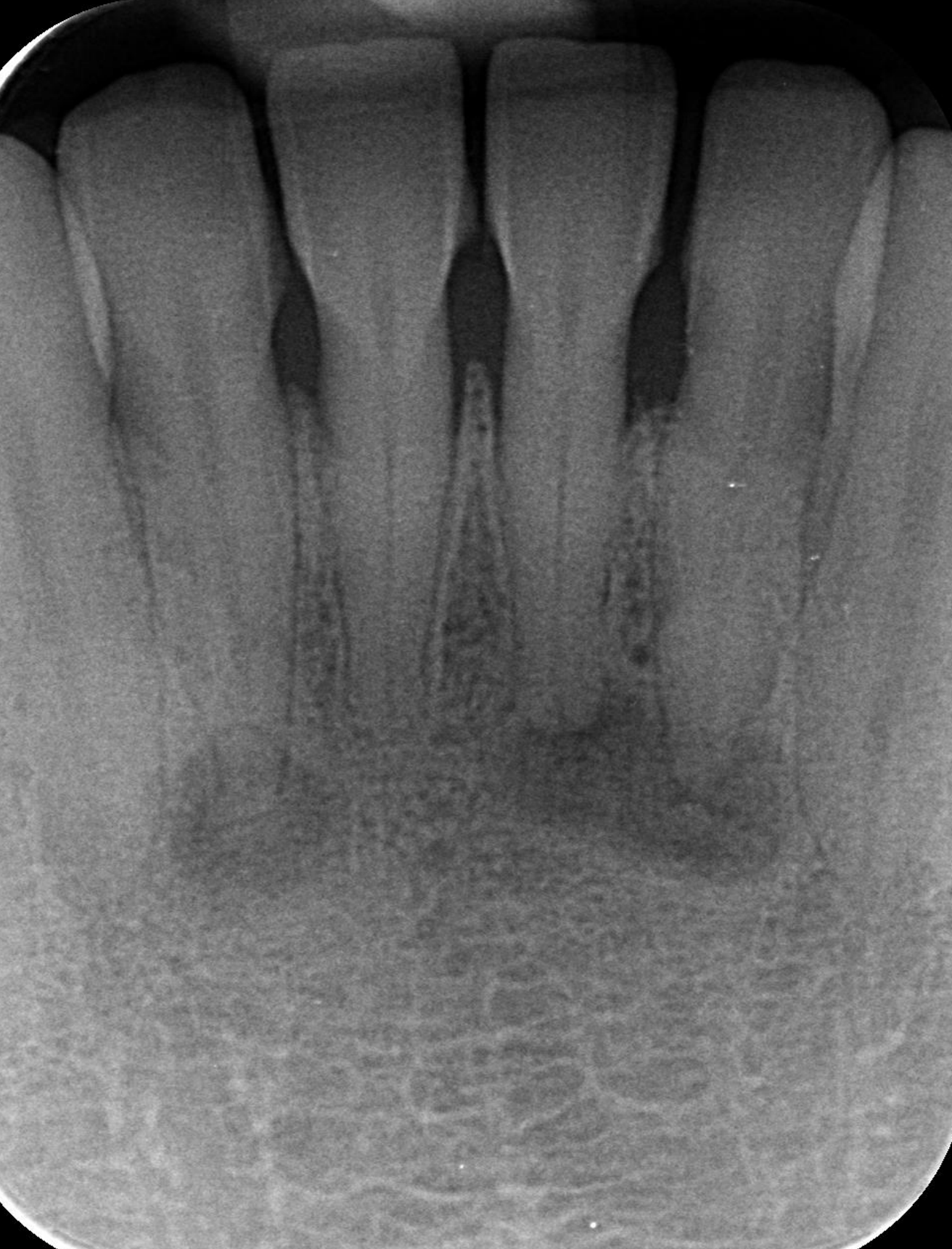
- ==View: PA of the anterior mandible (showing teeth 43 to 33).==
- ==Findings:==
- ==Lucencies: Presence of radiolucencies at the periapical regions of teeth 32, 31, and 42.==
- ==Lesion Characteristics: The lesions involving 32 and 31 appear as one continuous lobular lesion, while there is a solitary lesion at the apex of 42.==
- ==Differential Diagnosis: Inflammatory lesions in this area are typically associated with caries, fractures, or other coronal issues.==
Radiographic Findings
Identify and describe the abnormal lucencies present in the image:
- List at least three distinct radiographic features.
- Not completely radio opaque; ==presents as decreased density (pinpoint areas) in the periapical region of the lower anterior teeth (specifically around teeth 32 and 31).==
- Most likely Cemento osseous dysplasia (COD). The bone is not eroded, but the density is altered.
- Radiographic bone loss (minor periodontal bone loss).
- Calculus on enamel surfaces.
- ==Progression/Maturation:==
- ==These lesions can mature over time, transitioning from radiolucent to radiopaque as they form abnormal, brittle bone.==
- Once the lesion is mature (opaque), it typically stops growing.
Diagnostic Considerations
-
Provide a differential diagnosis (ddx).
- Periapical granuloma. Vitality testing is the most important step to rule out pulp necrosis/inflammatory lesions caused by blunt trauma or caries. Inflammatory lesions usually involve bone erosion, whereas COD may just show decreased density initially.
- Cemento osseous dysplasia (still differential because it has to be confirmed).
- ==Epidemiology: Extremely common, particularly in Australia/Perth.==
- ==Demographics: More prevalent in females and individuals with African, Asian, or Mediterranean backgrounds.==
- ==Age: Typically an “older person’s disease”; if seen in a young child, COD can likely be ruled out.==
-
Determine if further imaging is necessary.
- Another PA should be taken after 2 years to see if the COD lesion has matured or is still active.
- If the lesion remains stable or has matured (become opaque) after two years, no further radiographs are needed unless the tooth becomes symptomatic.
- When it matures it looks more radiopaque (not radiolucent).
==Management and Follow-up==
== Clinical Management==
==Treatment: No active treatment or extirpation is required.==
- ==Warning: Avoid unnecessary intervention, as “infected COD” can involve the entire bone.==
- ==Diagnosis: A confirmed diagnosis requires histology, which is unnecessary as the condition is asymptomatic and requires no management.==