==Comprehensive Examination: The OPG should be viewed as a comprehensive examination to identify abnormal lucencies and opacities.==
==Patient Positioning: Note that the patient in this case is tilted; the orbital floor and mandible are higher on the right side than the left.==
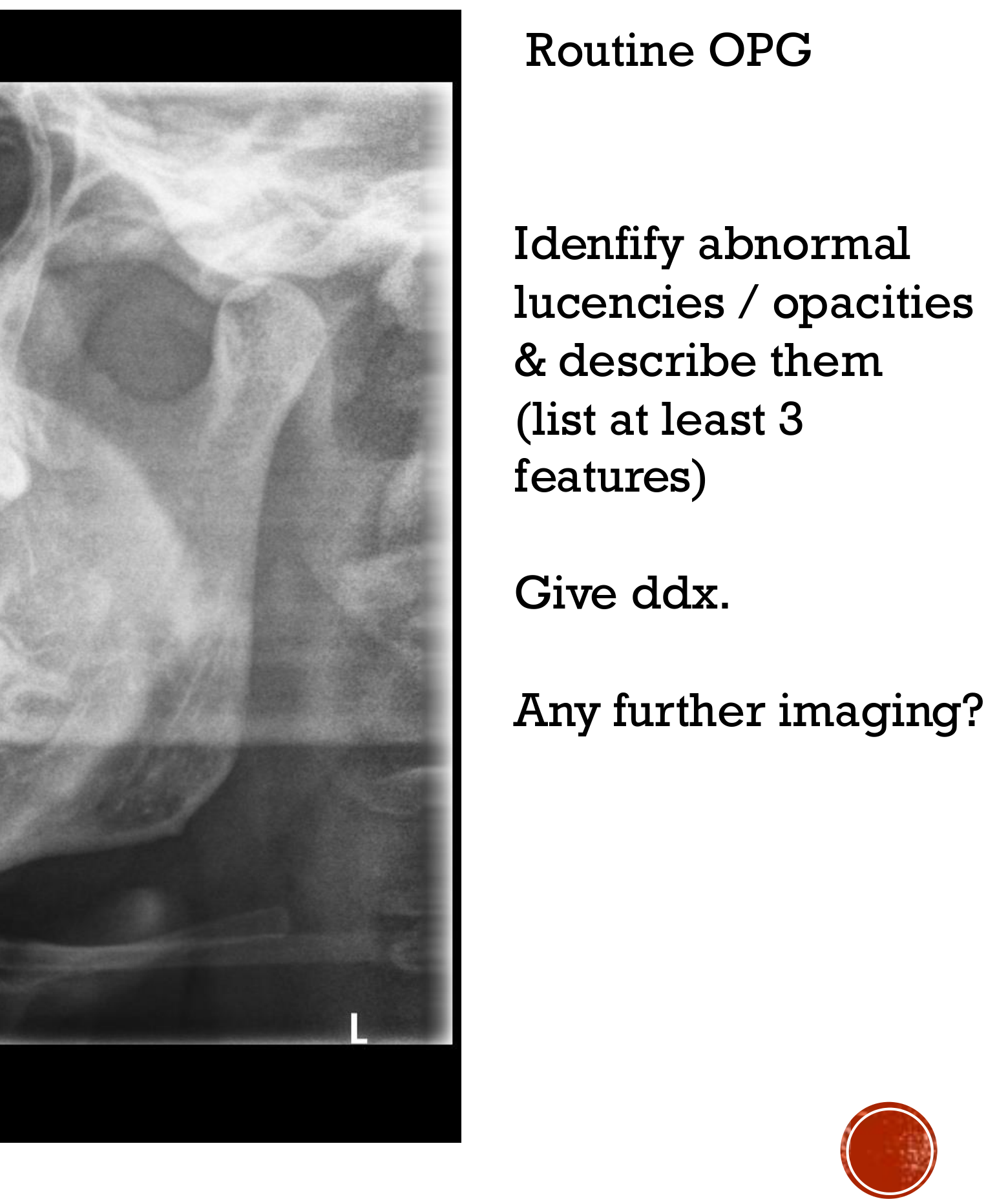
Quadrant 3 (Left Mandible):
radiolucency in the 33 in the left side of the mandible
==Location: Radiolucency at the periapical region of tooth 33, extending mesially to the apex of 32.==
Well defined
some lucency at the distal aspect of the 33 root
but the lamina dura and pdl is preserved, thus it is only a loss of density
there is no apperent resorption. This indicates a lack of structural loss or frank resorption of the tooth.
==Quadrant 4 (Right Mandible):==
==Third Molar (48): Partially erupted with adjacent sclerotic changes (increased bone density) near the residual follicular space.==
==Bone Density: The bone at the 48 site is more opaque compared to the normal trabecular density seen at the 38 site.==
==Visual Artifacts: A lucency appears below the opacity at 48, but this is often an optical illusion caused by the surrounding sclerotic bone; it is likely a large marrow space.==
Differential Diagnosis
[!example] Differential Diagnosis for Mandibular Lesions
==Inflammatory Lesions:==
==Periapical Lesion: Rule out by testing vitality. If the tooth is vital and the patient is not in pain, it is likely non-odontogenic.==
==Chronic Pericoronitis: Likely cause for the sclerotic changes seen around the partially erupted 48.==
==Cervical Burnout: Apparent lucency at the distal area of 33 and 45 is likely cervical burnout/overlapping rather than caries.==
==Cemental Osseous Dysplasia (COD):==
A strong differential if there is "bone tightness" or internal opacities within the lesion.
More common in older female patients.
Can degenerate into simple bone cysts over time.
==Simple Bone Cyst (Solitary/Traumatic Bone Cyst):==
Common in the mandible of younger patients.
Appears as a solitary lucent lesion.
==Tumors (e.g., Ameloblastoma):==
Ruled out in this case because tumors typically cause root resorption, which is absent here.
==Normal Anatomy:==
==Large Marrow Spaces: Commonly found in the posterior third molar regions; can look cystic but do not displace the mandibular canal.==
Further Imaging
==Clinical Correlation: Perform vitality testing on teeth associated with lucencies (e.g., 33).==
==Specialist Referral: Any bony lesions should be referred to an oral surgeon for management, as they can occasionally increase in size.==
==Radiological Consultation:==
==Second Opinions: Seek opinions from radiologists if unsure. This can be done via the reporting clinic or online Australian radiology services.==
==Professional Relationships: Establishing a relationship with a radiology clinic allows for informal consultations or formal reports on OPGs taken in-house.==