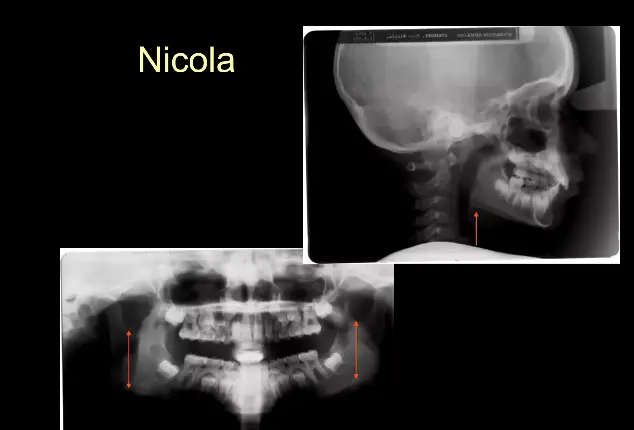
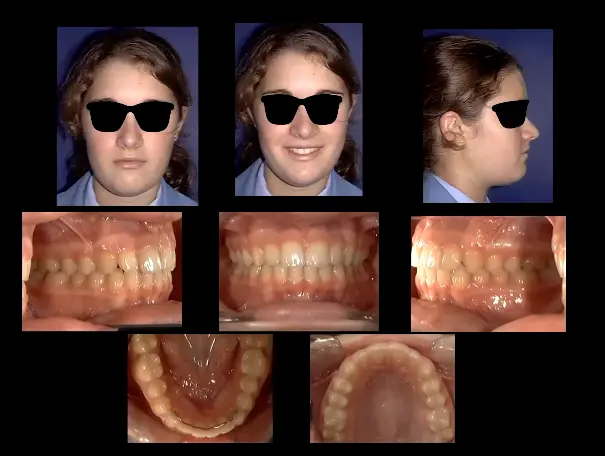
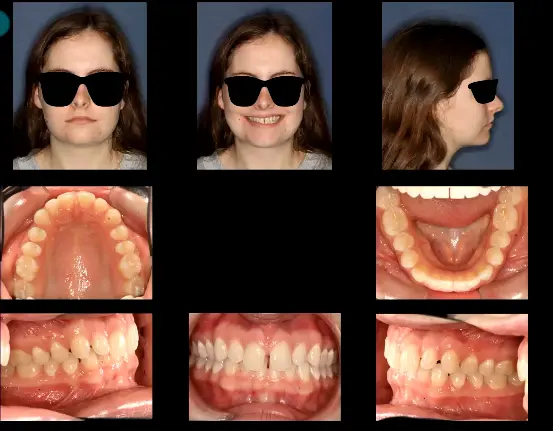
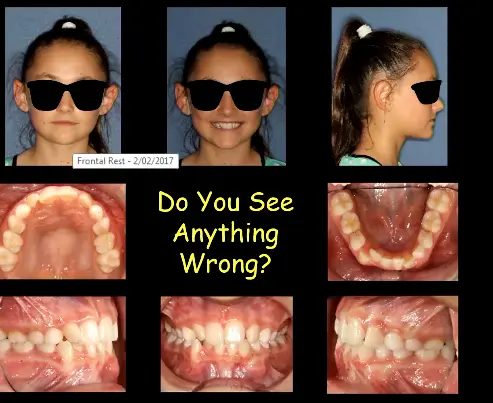
Case Study: Nicola – Class II Mandibular Deficiency with Asymmetry
Presentation: Mixed dentition with significant overjet, 70% deep overbite, and 2-3mm lower midline deviation.
Diagnosis: Class II mesial step molar relationship and skeletal mandibular deficiency with asymmetry (larger left condyle).
Treatment: Fixed appliances with a spring-loaded Class II corrector using differential activation to guide asymmetric growth.
- This was a mandibular deficiency, it needed to be moved forward
- They activate the right side more in order to try and correct the assymetry, otherwise it would need to be orthognathic surgery
-Spring is connected to the upper molars, it will stabilize them, that way you don’t move one side more than the other side
Outcome: Corrected anterior relationship and aligned midlines; monitored for late growth.

Case Study: Anterior Spacing with Occlusal Cant
- Presentation: Class I molar relationship with generalized spacing and deep overbite..
- Quite a few anterior spaces
- Treatment: Fixed appliance therapy focusing on vertical control to prevent excessive overbite closure while maintaining Class I engagement.
Case Study: Severe Crowding with Extractions
- Presentation: Adult patient with 10mm arch length discrepancy (no growth remaining).
- Treatment: Extraction of upper first premolars and one lower incisor to achieve stable alignment and minimize profile changes.
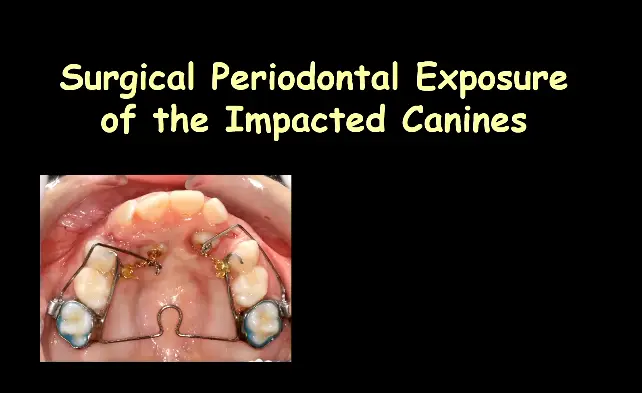
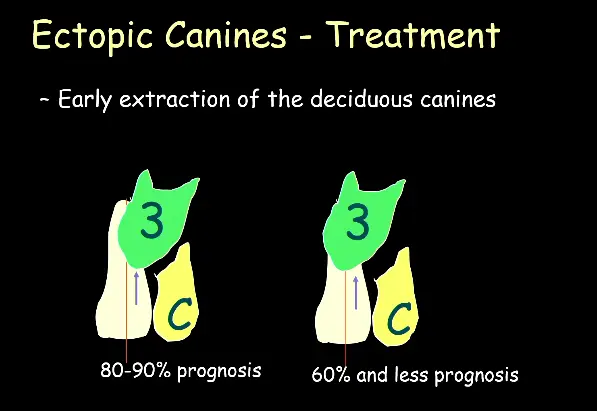
Case Study: Impacted Maxillary Canines – Early Intervention
==Presentation: 8-9-year-old patient with unerupted canines identified on radiograph. Management: Extraction of primary canines (C’s) to open space may allow spontaneous eruption if the permanent canine angulation is <30° to the lateral incisor root. Angulation Threshold: If the canine is >90° to the lateral incisor root, spontaneous eruption is unlikely (<10% probability); surgical exposure and orthodontic traction required. Goal: Early intervention prioritizes preventing resorption of lateral incisor roots over achieving perfect alignment.== .
Case Study: Canines Replacing Missing Lateral Incisors
==Presentation: Patient missing maxillary lateral incisors with impacted or palatally positioned canines.==
==Treatment: Extraction of contralateral lateral incisor (if present) for symmetry; surgical exposure of canines with gold chain traction.==
==Mechanics: Canines guided into lateral incisor positions using cantilevers; final reshaping (flattening cusps) mimics lateral incisor morphology. Outcome: A Class II molar relationship is accepted to achieve anterior aesthetics.== .
Case Study: Thumb Sucking and Open Bite Malocclusion
==Etiology: Persistent thumb sucking blocks anterior eruption (open bite) and allows posterior over-eruption (clockwise mandibular rotation).== You also have imbalance of the tngue and MOMs causing a cross-bite
==Treatment Protocol: Crib appliance (palatal barrier) for habit cessation; Quad helix or Rapid Maxillary Expander (RME) for transverse correction.==
==Vertical Control: High-pull headgear blocks maxillary posterior extrusion to allow counter-clockwise mandibular rotation; surgical posterior maxillary impaction (Lefort I) is the adult alternative.==

Adult Open bite:

Case Study: Anterior Crossbite with Functional Shift ()
==Presentation: Retroclined maxillary central incisors and edge-to-edge posterior occlusion causing a mandibular shift.==
> ==Treatment: Fixed appliances with Class III elastics to procline upper incisors. Once passed edge-to-edge, the lower incisors “step” forward naturally, stabilizing the TMJ.==
As long as we can procline the central incisors they will be edige to edge, as long as they pass a little bit the problem is solve
.
Case Study: Bilateral Mandibular Retraction using Bone Plates (TADs)
==Indication: Class III malocclusion requiring en masse distalization without extractions.==
==Technique: L-shaped bone plates screwed to the bilateral ramus provide absolute anchorage for retracting the entire lower dental arch.

Case Study: Severe Mandibular Deficiency – Distraction Osteogenesis
==Indication: Skeletal deformity exceeding orthognathic surgery limits (>12mm movement). Procedure: Bilateral mandibular osteotomy with a distraction device activated at 1mm per day to stretch bone and form a callus. Risks: Nerve/muscle stretching and high relapse rates if the consolidation period is insufficient; maximum safe activation is 20-25mm.==.
Anterior Cross-bite causing trauma:
Case: Ectopic canine

- At this stage you should remove the C’s
- You also have to do lots of follow up to prevent root resoprtion
- but the angulation is too high you need surgical exposure