The Clinical Examination: Paediatric Dentistry1
Lecture Outcomes2
Students should be able to:
- compare and contrast the differences between a clinical examination of a child and an adult
- construct a comprehensive history for a paediatric patient from consultation with their parent/guardian
- identify the fundamental elements that form part of an extra and intra-oral clinical examination of child
- interpret various tooth numbering systems used in dentistry
- make use of a history and examination in order to inform treatment planning in the context of paediatric dentistry
- Examinable content: Chapter 1 (Handbook of Paediatric Dentistry, Cameron & Widmer)
What is different in Children3
- May not be confident with strangers
- Cannot sit still for long
- Clinical time should be limited to 30–40 minutes maximum.
- Have little experience of:
- noise
- taste
- smells
- paresthesia
- Teeth are smaller
- Pulp are proportionally larger
- This means pulp horns are closer to the surface.
- Access is more limited
Examining Children4
Personal details
- Name
- Date of birth
- Date of examination
- Parent’s name
Info
Always double-check identity using at least two or three identifiers (e.g., name, date of birth, address, or parent’s name) to ensure the correct patient is being treated.
History5
History should be:
- taken in a logical and systematic way
- updated regularly
Reason for visit
- Referred by
- Routine examination
- Recall - check what was done before
- Painful teeth
**Current problem
parent’s own words, using quotation marks. Key variables that dictate treatment urgency include whether the pain affects the child's ability to sleep, eat, or drink. m**
Document the presenting complaint in the
- Pain
- nature
- onset or type of pain
- relieving and exacerbating factors
- Not sleeping
- Not eating
- Irritable
- Loose tooth/ teeth
- Broken tooth/restoration
- No problem
History – Medical history6
It should be taken in a systematic fashion, covering all system areas of the body. The major areas include:
- Cardiovascular system (e.g. cardiac lesions, blood pressure, rheumatic fever)
- Central nervous system (e.g. seizures, cognitive delay)
- Endocrine system (e.g. diabetes)
- Gastrointestinal tract (e.g. hepatitis)
- Respiratory tract (e.g. asthma, bronchitis, upper respiratory tract infections)
- Bleeding tendencies (e.g. family history of bleeding problems)
- Urogenital system (renal disease, ureteric reflux)
- Allergies
- Past operations or hospital admissions
Pregnancy history6
- Length of confinement
- Birth weight
- Apgar scores
- Type of delivery (any complications)
- Antenatal and perinatal problems, especially during delivery
- Prematurity and treatment in a special or neonatal intensive care nursery
Info
Issues during pregnancy or delivery (e.g., preterm birth, C-section complications) can correlate with developmental defects in enamel, as these events often occur while teeth are calcifying.
Growth and development
- Developmental milestones
- Speech and language development
- Motor skills
- Socialization
Info
Assess milestones to understand the child’s motor skills and socialization levels (e.g., Piaget’s stages). This informs behavior management strategies.
Current medical treatment
- Medications, including complementary medications
- Current treatments
- Immunizations
Clinical Considerations
- Cardiovascular System: Crucial due to the interaction with dental drugs; children have higher cardiac output and basal metabolic rates.
- Medications/Immunizations: Ask about regular tablets, asthma preventers, and history of hospitalizations or general anesthesia.
- Language: Use age-appropriate terms (e.g., "Do you take tablets every morning?" instead of "Are you on drugs?").
Dental history
- Previous dental treatment
- What preventive treatment has been undertaken previously
- Methods of pain control used previously
- How the child coped with the treatment
- Use the Frankl behaviour scale!
Family and Social history
- Helps build a picture
- Family history of serious illness
- Family make up
- Place of birth
- No of siblings
- Schooling, performance in class
- Speech and language problems
- Likes, dislikes
- Other interests (pets, hobbies, sports, television, books, movies, video games)
Parent’s comment
- Record what the parent says
- Concerns may be different than reason for appointment
Reason for visit
- Record the referral source and the primary reason for the appointment (e.g., routine check-up, recall, or specific symptoms).
Current problem
- ==Document the presenting complaint in the parent’s own words (using quotation marks)==. Key variables that dictate treatment urgency include:
- Is the pain affecting the child’s ability to ==sleep==?
- Is the pain affecting their ability to ==eat or drink==?
- Other factors: Irritability, loose teeth, or broken restorations.
Examination7
Extra oral examination
- General appraisal of the child’s well-being
- General interaction with the parents or peers
- Child’s gait
- Height and weight assessment
Checklist
Frontal profile
- round / tapering / square / symmetrical /asymmetrical Lateral profile
- straight / convex / concave Skeletal pattern
- I / II / III Lips
- Lips: competent / incompetent / lip trap
 Eyes
Eyes- Appearance of the globe, sclera, pupils and conjunctiva
- Movements of the globe: indicate squints or palsy Skin/Soft tissue
- Colour
- Appearance – lacerations, scars, vesicles
Info
Check for lesions that might indicate systemic issues like chickenpox, measles, or hand-foot-and-mouth disease.
Extra oral examination8
Temporomandibular joints
- movements
- sounds
- symptoms
Info
Generally involves simple opening/closing observation; deep palpation is usually unnecessary unless symptomatic.
Lymph nodes
- cervical
- submandibular
- occipital
Intra-Oral Examination
Soft Tissues First
Do not look at the teeth immediately.
Soft tissues
- Lips
- Tongue
- Mucosa
- Gingiva
- Frenums
- Floor of mouth
- Palate
- Salivary glands
- Oropharynx
-
Tonsils
-
Uvula
enlarged tonsils (snoring/sleep issues) or a bifid uvula (indicator of submucous cleft).
Check for
-
Alveolar Mucosa:
Look for subtle signs of infection (abscesses in children are often small, not always large and fluctuant)
- Trauma/Biting: Be aware of post-local anesthetic lip biting, which presents as a large ulcer
- Abscesses can also be subtle
- Use fingers to affect the upper and lower lip
Important
Always look around the buccal and lingual of teeth that have large restorations or abnormal physiology such as intrinsic discolouration or signs of trauma
Various types of lesions
-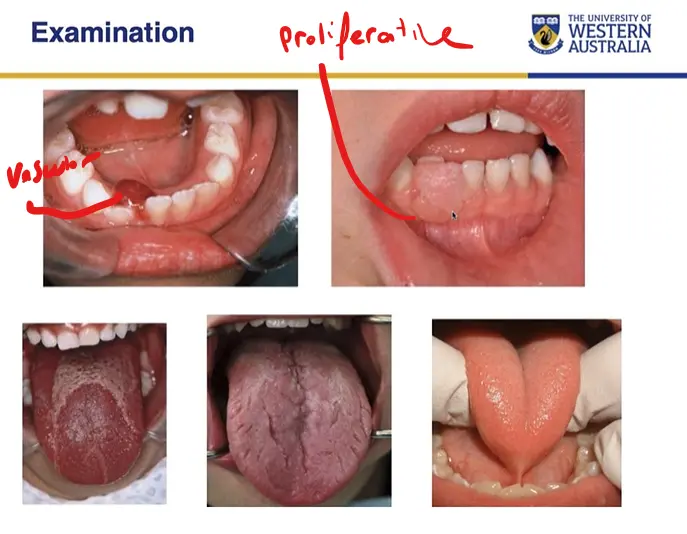
Describing Lesions
- Oral medicine terms should be used
- Furthermore lesions should be comprehensively and systematically described
- location
- colour
- size
- texture
- history
- onset
Oral hygiene
- Plaque disclosing
- Record
- Plaque location
- Quantity
Periodontal status
- Healthy
- Unhealthy
- Developmental
- Why?
Info
Use plaque disclosing solution as an educational tool. Assess if hygiene issues are due to lack of dexterity, lack of motivation, or a symptomatic tooth the child is avoiding.
Dental hard tissues
Teeth
- Tooth identification
- Dental charting
- Systems
- Dental caries / restorations
- Anomalies
- Abnormalities
Clinical Notes
- Anomalies: Count the teeth to identify supernumerary teeth or congenitally missing teeth.
- Developmental Defects: Differentiate between caries and defects like ==Molar Incisor Hypomineralization (MIH) or Turner’s Tooth== (enamel defect on a premolar caused by infection of the preceding primary tooth).
- Universal or ADA System
- Palmer notation system
- FDI or international system
Occlusion and orthodontic relations
- Eruption
- Normal
- Abnormal
- Terminal plane
Molar Relationship910
- Flush terminal plane
- Mesial step
- Distal step
- Angles classification for permanent teeth
Canine Relationship
Occlusion and orthodontic relations
- Canine
- Canine relationship
Occlusion and orthodontic relations
- Overjet
- Overbite
- Crossbite
- Rotations
Occlusion and orthodontic relations
- Midline
- Dentition
-
spacing
-
crowding
-
arch deformity
-
==Anomalies: Count the teeth to identify supernumerary teeth or congenitally missing teeth.==
-
==Developmental Defects: Differentiate between caries and defects like Molar Incisor Hypomineralization (MIH) or Turner’s Tooth (enamel defect on a premolar caused by infection of the preceding primary tooth).==
-
Occlusion and orthodontic relations
Habits
- Digit sucking
- Mouth breathing
- Tongue thrusting
Radiographs11
- Bitewing radiographs
- The "gold standard" for caries detection. Use Size 0 for young children. In primary dentition, bitewings are preferred over Periapicals (PAs) because they capture the furcation area where pediatric infections usually manifest.
- Periapical radiographs
- often not needed in primary dentition because most infection starts in the furcal area, thus a good bitewing will give enough information to classify it
- Occlusal films
- A maxillary occlusal is excellent for checking growth, development, or supernumerary teeth and is often easier for children to tolerate than a PA.
- Panoramic radiographs
- Extra-oral facial films
- Cone-beam CT
Intra oral Film Sizes
- 0, 1, 2 anterior occlusal
Show
- Dental caries - interproximal and occlusal
- Alveolar bone health
- Enamel defects
- Root health
- Developing teeth
- Pulp chamber
- Outline of restorations
- Sequential radiographs
- Disease progression
Panoramic
-
Developing teeth
-
TMJ
-
Bone health
-
Pathology
-
Useful in the mixed dentition (ages 9–12) for "canine checks" if the permanent canines cannot be palpated.
Special Tests12
- Photographs
- Diagnostic cast
- Blood investigations
- Microbiology
- Salivary tests
- Caries activity tests
- Diet analysis
- Caries risk assessment
Photographs
- Clinical record
- Medico-legal record
- Especially important in trauma cases.
- Before and after treatment
- Provides record of growing children
Diagnostic cast
- Essential in treatment planning
- Study Model Analysis
- Space measurement
- Space maintenance?
- Space regaining?
- Cross bite correction
Pulp sensibility (viability) test
Reliability in Children
Pulp sensibility tests are often unreliable and subjective in children. They should only be used if other diagnostic findings are inconclusive.
- Thermal
- Electrical stimulation
- Percussion
- Mobility
- Useful for trauma follow-ups (checking for ankylosis) or monitoring exfoliation.
- Transillumination
Blood investigations
- Full blood count with differential white cell count
- Clinical chemistry
Microbiological investigations
- Culture of microorganisms and antibiotic sensitivity
- Cytology
- Serology
- Direct and indirect immunofluorescence
- Plaque pH activity
- S mutans count
Quantity of saliva
- Salivary flow rate
- unstimulated (resting)
- Stimulated
- Salivary Buffering Capacity
Quality of saliva
- Measuring resting salivary pH
Caries Risk Assessment13
- Past disease experience
- Current dental status
- Family history and carer status
- Diet considerations
- Oral hygiene
- Concomitant medical conditions
- Future expectations of disease activity
- CAMBRA
Low risk of disease
- No caries present
- Favourable family history (appropriate diet, dentally healthy siblings, motivated parents and caregivers)
- Good oral hygiene
- Access to community water fluoridation
Moderate risk
- One or two new lesions per year
High risk or future high risk
- Three or more new lesions per year
- Orthodontic treatment
- Chronic illness or hospitalization
- Medically compromised children
- Social risk factors
Goal
Move the child out of the "restorative spiral" through oral health promotion and prevention.
Diagnosis/problem List14
- Acute
- Dental age
- Caries risk
- Periodontal status
- Oral hygiene
- Behaviour
- Occlusion
- Trauma
- Other
Example
Compile all findings into a list (e.g., "High caries risk," "Gingivitis," "Delayed dental age").
“…diagnostic skills cannot be learnt from textbooks alone, but require clinical training ” (Nyvad, 2004)
Treatment plan15
- Based on the assessed need of the child
- Addresses all oral conditions, dental diseases & injuries
- Establishes a preventive programme
- Allows for forward planning by all involved
- Know number of visits required
- Scheduling of these visits
- Time off school, time off work
- Baby sitters for siblings
- Appointments can be so treatment is completed in weeks rather than months
- Clinician prepared before child arrives
- Endpoint - Child to reach adulthood with a healthy mouth, positive attitude to dental care
Figuring out how children cope with visits
- A fissure seal visit will tell you how well the chlid will cope with longer more complex visits
What needs to be included?
- Medical management
- Behaviour management
- Relief of pain/ emergency care
- Prevention
- Restorative needs
- Surgical treatment
- Orthodontic treatment
- Extensive restorative or further surgical management
- Growth & Development
- Aesthetic considerations
- Payment agreement
- Recall Timing
- Referral
- Consent - who is able to give consent?
- Ensure the person accompanying the child is the legal guardian.
Personalised
- All children are different
- Social needs
- Medical
- Dental
- Age
- Expectations – child’s/ parents child’s / parent’s understanding management concerns
- Financial constraints
- Appointments
Holistic
- Treating a child not a tooth
- Not a list of procedures
- Behaviour shaping
- Prevention
- Growth and development
- Interceptive orthodontics?
- Consider if a treatment (like a traumatic extraction) will cause long-term dental phobia. If so, refer for specialist care or General Anesthesia (CORGA/DEGA).
Flexible
- Circumstances & dental status change
- flexible to both the child and the parents needs
Sequenced
- Gradual introduction of new experiences
- e.g. prophy, fissure sealants to build confidence
- Prophylaxis
- Small restorations before large
- Upper teeth before lower
Forward thinking
- Longer term picture
- Interventions – reduce complexity of future treatment
Realistic
- Remember you are treating a patient – a young patient
- Not able to keep still for hours
- Keep appointments short.
Summary Note16
- It has been said that the major difference between adult and pediatric dental patients is that the latter did not request the treatment and frequently they do not even understand why they are at the dentist’s office!
NOTE
The clinician’s role is to provide a positive experience that shapes the child’s lifelong view of dental health.
Footnotes
-
Original PDF page 1: L1 The Paediatric Clinical Examination LMS, p.1 ↩
-
Original PDF page 2: L1 The Paediatric Clinical Examination LMS, p.2 ↩
-
Original PDF page 3: L1 The Paediatric Clinical Examination LMS, p.3 ↩
-
Original PDF page 4: L1 The Paediatric Clinical Examination LMS, p.4 ↩
-
Original PDF page 5: L1 The Paediatric Clinical Examination LMS, p.5 ↩
-
Original PDF page 7: L1 The Paediatric Clinical Examination LMS, p.7 ↩ ↩2
-
Original PDF page 14: L1 The Paediatric Clinical Examination LMS, p.14 ↩
-
Original PDF page 28: L1 The Paediatric Clinical Examination LMS, p.28 ↩
-
Original PDF page 31: L1 The Paediatric Clinical Examination LMS, p.31 ↩
-
Original PDF page 32: L1 The Paediatric Clinical Examination LMS, p.32 ↩
-
Original PDF page 36: L1 The Paediatric Clinical Examination LMS, p.36 ↩
-
Original PDF page 39: L1 The Paediatric Clinical Examination LMS, p.39 ↩
-
Original PDF page 45: L1 The Paediatric Clinical Examination LMS, p.45 ↩
-
Original PDF page 46: L1 The Paediatric Clinical Examination LMS, p.46 ↩
-
Original PDF page 47: L1 The Paediatric Clinical Examination LMS, p.47 ↩
-
Original PDF page 53: L1 The Paediatric Clinical Examination LMS, p.53 ↩