Dental Anomalies Part 1
DENT5312 Dr Jilen Patel
Lecture Outcomes1
Students should be able to:
- Understand the stages of tooth development and the associated anomalies that can occur at different stages
- Explain the difference between anomalies and traits
- Define anomalies of tooth size and shape
- Define and differentiate between various anomalies of tooth number (hyperdontia, hypodontia) and size (microdontia, macrodontia)
- Explain the aetiology, prevalence, clinical characteristics, implications and potential management strategies for anomalies of tooth size and shape
- Identify anomalies of tooth size and shape through visual and radiographic examinations
Stages of tooth development2
Note
Tooth development is primarily an ectodermal process involving the migration of neural crest cells and the condensation of ectomesenchyme.
graph LR Initiation --> Bud_stage[Bud stage] Bud_stage --> Cap_stage[Cap stage] Cap_stage --> Bell_stage[Bell stage] Bell_stage --> Dentinogenesis Dentinogenesis --> Amelogenesis Amelogenesis --> Continued_dentinogenesis["Continued dentinogenesis/amelogenesis"] Continued_dentinogenesis --> Eruption Eruption --> Mature
Developmental Stages and Associated Anomalies3
Additional Anomalies & Activities from Lecture
The lecture provides a slightly different classification for some anomalies and adds details:
- Cap Stage Anomalies: Gemination, Fusion, Dens in dente
- Bell Stage (Histodifferentiation) Anomaly: The lecture associates Amelogenesis/Dentinogenesis Imperfecta with this stage.
- Crown Stage (Calcification) Activity: Hardening of matrix
- Crown Stage (Calcification) Anomaly: Hypocalcification
| Stage | Process | Activity | Associated anomalies |
|---|---|---|---|
| Bud | Initiation | Migration of neural crest cells into arches | Tooth number (supernumerary teeth, hypodontia...) |
| Cap | Proliferation | Condensation of ectoderm and formation of dental organ and dental papilla | Odontogenic cysts |
| Bell | Morphodifferentiation | Proliferation of inner enamel epithelium to form the shape of the crown | Tooth size and shape (macrodontia, microdontia...) |
| Histodifferentiation | Differentiation of precursor cells ameloblasts and odontoblasts | Regional odontodysplasia | |
| Crown | Apposition | Reciprocal induction and laying down of mantle dentine and first enamel | Enamel hypoplasia |
| Calcification | Amelogenesis Imperfecta Dentinogenesis Imperfecta | ||
| Maturation | Enamel crystal formation | Enamel hypomineralisation | |
| Eruption | Emergence of tooth and continued development of roots | Impacted teeth |
Anomaly or trait?4
- Anomaly: when a variant occurs rarely in a given population
- eg anomalies in tooth number, size, shape, structure
- Trait: when a variant is exhibited by a significant number of people in a population such that it is considered a trait for the dentition of that population
- eg incisor shovelling, cusp of Carabelli, protostyloid(additional buccal cusp on molars)
ANOMALIES OF TOOTH NUMBER56
Hyperdontia
Definition
Any tooth or structure formed from a tooth germ that is in excess of the usual number for any given region of the dental arch
The term 'structure' is used because these may not always be well-organized teeth.
Terminology
- Supernumerary
- Polyphodontism (Gibbs, 1913)
- Third dentition, superdentition (Gissen, 1935)
- Duplicate teeth (Werther & Rothenberg, 1939)
- Supplemental (Glassington, 1893)
- Aberrant (Nodine, 1943)
- Conoidal (Fashlicht, 1943)
Preferred Terminology
==Hyperdontia and Supernumerary teeth are the preferred clinical terms.==
Etiology7
- Remains unclear
- Various theories have been postulated:
- Result of hyperactivity of the dental lamina (Black, 1909)
- Tooth germ dichotomy (split of tooth germ): an imbalance between molecules can cause the tooth germ to divide into two parts, of equal or different size (Gardiner, 1961)
- Genetic predisposition
- Environmental factors
- Multifactorial, a combination of environmental and genetic factors (Brook, 1984)
Prevalence8
- Permanent dentition > primary dentition (Clayton, 1956)
- Primary dentition: 0.2-0.8%
- Permanent dentition: 0.5-3.5%
- (Garvey et al. 1999; Sasaki et al. 2007; Ferrés-Padró et al. 2009; Kaya et al. 2011)
- Male > Females
- Male : Female = 1.18 : 1.0
- (Brook, 1984; Fernandez Montenegro et al. 2006; Liu et al. 2007; Ferres-Padro et al. 2009)
- Maxillary incisor region > mandibular premolar > maxillary molar region
- (Grahnen and Lindalh, 1961; King et al. 1993)
Additional Prevalence Data
- The true prevalence may be as high as 10% because many supernumerary teeth remain unerupted and undiagnosed.
- Some studies report that males are affected twice as often as females (a 2:1 ratio), a higher rate than other reports.
Supernumerary Teeth9
Definition
- Any tooth or odontogenic structure that is formed from a tooth germ in excess of the usual number for any given region of the dental arch (Shafer, 1983)
- The term “hyperdontia” is preferred by some authors to describe the dentition which contains one or more supernumerary teeth
Classification of Supernumerary10
graph LR S[**Supernumerary**] --- L[**Location**] L --- L1["• **Mesiodens** • Paramolar • Distomolar • Parapremolar"] subgraph Ref1 [ ] direction TB R1[Bolk, 1914; 1917] end L -.-> Ref1 S --- M[**Morphology**] M --- M1["• **Conical** • Tuberculate • Supplemental (or eumorphic) • Odontome - Complex - Compound"] subgraph Ref2 [ ] direction TB R2["Di Biase, 1969; Foster and Taylor, 1969"] end M -.-> Ref2 S --- O[**Orientation**] O --- O1["• Vertical or normal • **Inverted** • Horizontal"] S --- P[**Position**] P --- P1["• Buccal • Palatal • Transverse"] style S fill:#C0E8FF,stroke:#00AEEF style L fill:#C0E8FF,stroke:#00AEEF style M fill:#C0E8FF,stroke:#00AEEF style O fill:#C0E8FF,stroke:#00AEEF style P fill:#C0E8FF,stroke:#00AEEF style L1 fill:#C0E8FF,stroke:#00AEEF,text-align:left style M1 fill:#C0E8FF,stroke:#00AEEF,text-align:left style O1 fill:#C0E8FF,stroke:#00AEEF,text-align:left style P1 fill:#C0E8FF,stroke:#00AEEF,text-align:left style Ref1 fill:none,stroke:none style Ref2 fill:none,stroke:none
(Primasch, 1981; Garvey, 1999; Rajab and Hamdan, 2002)
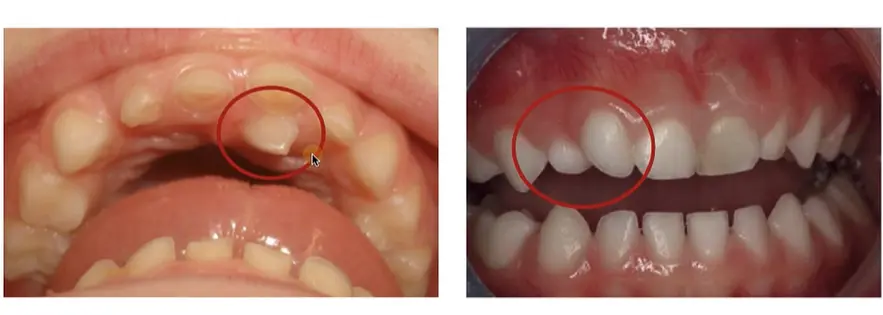
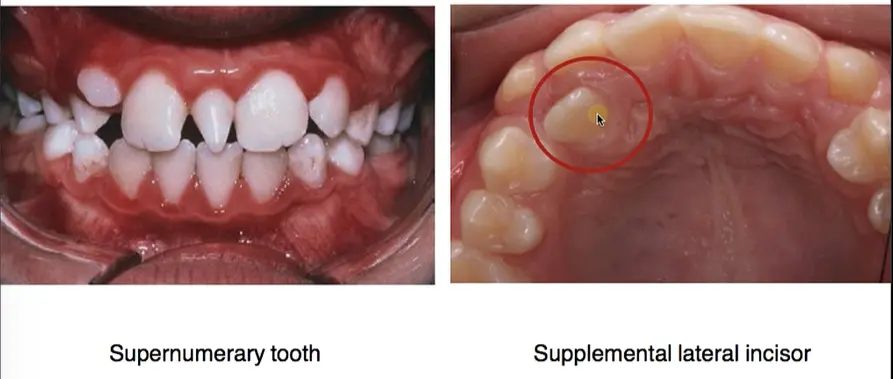
- ==Conical: Small, peg-shaped.==
- ==Tuberculate: Barrel-shaped with multiple cusps; often inhibits eruption of permanent teeth.==
- ==Supplemental: Looks exactly like a normal tooth and can be difficult to distinguish.==
- ==Odontome: A haphazard mass of dental tissue.==
Mesiodens11
-
Mesiodens: the most “mesially invested tooth”…”the lost incisor” (Bolk,1917)
-
Most common type of supernumerary
-
Supernumerary tooth in the primary dentition
-
Located in the anterior maxillary midline, though rarely exactly on the midline. It is usually conical and may be inverted.

Conditions and Syndromes Associated with Hyperdontia1213
- Cleft lip and palate
- Associated with both extra and missing teeth.
- Cleidocranial Dysplasia
- Characterized by missing clavicles and multiple supernumerary teeth throughout the mouth.
- Gardner Syndrome (Familial Adenomatous Polyposis)
- Associated with gastrointestinal polyps and multiple supernumerary teeth/osteomas.
- Nance-Horan Syndrome
- Tricho-Rhino-Phalangeal Syndromes
- Fabry Anderson’s syndrome
- Chondroectodermal dysplasia (Ellis–Van Creveld syndrome)
- Ehlers– Danlos syndrome
- Incontinentia pigmenti
Odontomes1415
- Odontomes occur because of disordered differentiation and often present because of failure of eruption of a permanent tooth
NOTE
They are considered "hamartomas" (disordered growth) rather than true neoplasms.
Types:
- Complex: haphazard arrangement of enamel, dentine and cementum
- Compound: consists of discrete tooth-like structures
Management:
- Surgical enucleation
- May require surgical exposure and orthodontic alignment
Clinical Signs of hyperdontia16
-
Spacing e.g midline diastema
-
Failure of adjacent teeth to erupt
- This should be suspected especially if the contralateral tooth has already erupted.
- Especially with failure of upper incisors to erupt
- Also may cause retention of primary incisors
-
Displacement
- May cause displacement of permanent tooth from mild rotation to complete displacement
-
Eruption into mouth
-
Local crowding or irregularity
Complications17
-
Failure of eruption of permanent teeth
-
Displacement or rotation or crowding
-
Ectopic eruption of permanent teeth
-
Abnormal diastema or premature space closure
-
Dilaceration, delayed or abnormal root development of permanent teeth
-
Pathology (dentigerous cyst formation)
- There is a ~10% risk of developing a dentigerous cyst, usually in the 3rd or 4th decade of life.
-
Rare complication
- root resorption/loss of viability
- nasal eruption
Case Report Note: Endoscopic removal of supernumerary tooth from the nasal cavity of a child: a case report (Clementini et al 201)
Diagnosis and Treatment1819
Diagnosis:
- Clinical - failed or eruption disturbance of permanent tooth
- Routine radiographic finding
- As part of a syndrome e.g. cleidocranial dysplasia
Treatment:
- Depends on type and position of supernumerary
-
Long term monitoring
-
Extraction
-
Surgical removal
-
Research (Omer, 2010) suggests removal before age 7 is beneficial to reduce complications for permanent successors.
-
Hypodontia2021
Definition
- Developmental absence of one or more teeth excluding third molars (Gooman, 1994)
Terminology
- Hypodontia: less than six missing teeth
- Oligodontia: six or more missing teeth
- Anodontia: no teeth present
- Agenesis of teeth associated with syndromes or systemic abnormalities
- (Gorlin et al. 1978)
Classification22
- Mild: 1-2 missing teeth
- Moderate: 3-5 missing teeth
- Severe: 6 or more missing teeth (oligodontia)
- (Goodman, 1994, Dhanrajjani, 2002; Jones, 2009)
Clinical Note
==In Western Australia, eligibility for referral to Perth Children’s Hospital requires 10 or more missing permanent teeth (excluding 3rd molars).==
Prevalence8
- Most common congenital malformation
Primary dentition:
- Uncommon
- 0.1-4.1% (Saito, 1959, Brook, 1974, Tongkoom, 1994)
- F = M
- Often associated with hypodontia in permanent dentition
Permanent dentition:
- 4-6% Caucasian (Niswander and Sujaku, 1983; Brook, 1974; Tsai, 1996)
- F > M; F: M = 3:2 (Nunn, 2003; Larmour, 2005)
- Variation between continents, racial groups and gender (Polder, 2004)
- (Brook, 1974; Tongkoom 1994; Tsai, 1996; McKeown et al. 2002: Khalaf et al. 2014)
Distribution by Jaw and Tooth Type23
- Higher percentage of missing teeth in the maxilla (53.2%) than in the mandible (46.8%)
- The teeth most commonly missing are the last teeth in each series (namely the upper lateral incisors, the second premolars and third molars)
==Butler’s Field Theory (1939): The most distal tooth in each “field” is most likely to be missing:==
- ==Molar field: 3rd molars.==
- ==Premolar field: 2nd premolars (most common missing tooth overall).==
- ==Incisor field: Lateral incisors.==
Prevalence by Tooth Type (Khalaf et al. 2014):
| Tooth Type | Prevalence |
|---|---|
| Mandibular second premolars | 29.9% |
| Maxillary lateral incisors | 24.3% |
| Maxillary second premolars | 13.7% |
| Mandibular central incisors | 6.1% |
| Mandibular lateral incisors | 4.3% |
| Maxillary first premolars | 3.6% |
| Mandibular first premolars | 2.7% |
| Maxillary canine | 2.5% |
| Mandibular second molars | 1.8% |
| Maxillary second molars | 1.5% |
| Mandibular canines | 1.3% |
| Maxillary first molars | 1.1% |
| Mandibular first molars | 1% |
| Maxillary central incisors | 1% |
Sequence of Affected Teeth (Polder et al 2004):
| Category | Prevalence (%) | Sequence |
|---|---|---|
| Common | 1.5–3.1 | P2ᵢ > I2ₛ > P2ₛ |
| Less common | 0.1–0.3 | I1ᵢ > I2ᵢ & P1ₛ > Cₛ & M2ᵢ |
| Rare | 0.01–0.04 | M2ₛ & M1ₛ > Cᵢ > M1ᵢ & I1ₛ |
| (s, maxilla; i, mandible) |
Aetiology242526272829
- Several theories – both genetic and environmental factors
- Hypodontia commonly associated with small teeth (Graber, 1978)
- It can be an isolated non-symdromic feature or a part of a complex syndrome
Genetic Basis:
- Homeobox genes involved:
- MSX1
- PAX9
- AXIN2 (Cobourne, 2007)
Environmental Factors:
- Intra-uterine effects of drugs e.g. Thalidomide
- Early radiotherapy & chemotherapy
- Trauma e.g. alveolar fracture or jaw fracture, jaw surgery, iatrogenic damage to the permanent tooth germ from traumatic extraction of overlying primary tooth
- Infection e.g Rubella
- (Winter, 1996; Brook et al. 2009)
Syndromes Associated with Hypodontia30
Hypodontia is a major clinical feature of over 50 syndromes including:
- Hypohidrotic Ectodermal Dysplasia (HED)
- Affects hair, sweat glands, and teeth (teeth are often missing or conical).
- Hypohidrotic Ectodermal Dysplasia with Immune Deficiency (HED-ID)
- Dento-alveolar clefting
- Trisomy 21 (Down syndrome)
- Oral–Facial–Digital Syndrome Type I (OFDI)
- Williams (Beuren) Syndrome (WBS)
- Solitary Median Maxillary Central Incisor (SMMCI)
- A single central incisor exactly in the midline; a red flag for systemic midline defects (e.g., cardiac issues).
- Axenfeld–Rieger Syndrome (Rieger Syndrome)
- Oligodontia and Colorectal Cancer Syndrome
- Odonto-Onycho-Dermal Dysplasia (OODD)
- Incontinentia Pigmenti
- Wolf–Hirschhorn Syndrome
- Witkop Syndrome
- Ectrodactyly, Ectodermal Dysplasia and Clefting (EEC)
- Ellis-van Creveld Syndrome (EVC)
- Weyers Acrofacial Dysostosis Syndrome (Curry–Hall Syndrome)
- Van der Woude Syndrome (VWS)
- Angel-Shaped Phalango Epiphyseal Dysplasia (ASPED)
- Lacrimoauriculodentodigital Syndrome (LADD)
- Kallmann Syndrome (KS; KAL2)
- Bloom Syndrome (BS, BLS)
- Rothmund–Thomson Syndrome
- Diastrophic Dysplasia Syndrome
- Johanson–Blizzard Syndrome
- Kabuki Syndrome
Specific Syndrome Note: Solitary Median Maxillary Central Incisor syndrome ⏰⏰🚩!
Clinical Features31323334
-
Delayed/asymmetric eruption of permanent teeth
-
Retained or infraoccluded deciduous teeth
- Primary teeth (often the 2nd primary molar) "sink" below the occlusal plane because they are ankylosed to the bone while the rest of the arch grows.
-
Absent deciduous teeth
-
Microdontia of existing teeth
-
Can be associated with short root anomaly
-
Patients with hypodontia often present a tendency to:
- Lip protrusion (Chung, 2000)
- Increased overbite
- Increased rotations of teeth (Bacetti, 1998)
- Increased prevalence of ectopic maxillary canines
- Reduced mandibular plane angle
Treatment of hypodontia35
- Acid-etch retained, composite resin build-ups of conical teeth
- Orthodontic management of spaces
- Specifically, space closure or space opening for future implants/bridges.
- Removable prosthesis:
- Partial dentures
- conventional dentures
- overdentures
- Fixed prosthesis:
- composite resin veneers
- crowns
- bridges
- Autotransplantation
- Osseointegrated implants (usually after the cessation of growth).
Terminology
The term microdont lateral incisor is preferred over peg lateral.
Microdontia3637
Definition
- It is described as teeth which are smaller than normal and outside the usual limits of variation (Rushton, 1948)
- In general microdontia, the teeth are small, the crowns short, and normal contact areas between the teeth are frequently missing (Boyle, 1955)
- Alternative terminology: Microdentism, Microdontism (Shafer et al. 1974)
Prevalence8
- Permanent dentition > primary dentition (Shafer, 1974)
- Female > male (Brook, 1974, Tongkoom, 1994; Tsia, 1996)
- More frequently in the maxillary teeth than the mandibular teeth
- Most prevalence data are available only for maxillary lateral incisors
Primary dentition:
- 0.5- 6.3% (Brook, 1974; Tongkoom, 1994; Ooshima et al. 1996)
Permanent dentition:
- 1.9- 6.9% (Brook, 1974; Ooshima et al. 1996; Tsai, 1996; Aldred et al. 2012)
Classification22
- True generalised microdontia
- Generalised relative Microdontia
- Localised microdontia
- (Shafer et al. 1958)
True Generalised Type38
- All the teeth are smaller than normal
- All of the teeth are of a normal morphological form
- Exceedingly rare
- Reported in:
- radiation or chemotherapeutic treatment during the developmental stage of the teeth (Van der waal, 1988)
- pituitary dwarfism (Shafer, 1958)
- fanconi’s anemia (Opinya et al. 1988)
Generalised Relative Microdontia3940
- Normal or slightly smaller than normal teeth but the jaws are somewhat larger than normal — impression of microdontia
Localised Microdontia41
Involving a single tooth & further subdivided into:
- Microdontia of the whole tooth
- Microdontia of the crown of the tooth
- Microdontia of the root alone
- (Ufomata, 1988)
- Rather common
- Affects mostly the maxillary lateral incisor (Peg-shaped laterals)
- Supernumerary teeth are frequently small in size
Peg Laterals4243
- Common form in lateral incisors
- The mesial and distal surfaces converge or taper incisally forming a peg-shaped or cone-shaped crown
- The roots are frequently shorter than normal
Conditions and Syndromes Associated with Microdontia44
- Patients with ectodermal dysplasia often present with microdontia
- Pituitary dwarfism
- Down syndrome
- Facial Hemiatrophy
- Gorlin-Chaudhry-Moss syndrome
- Williams’s syndrome
- Chromosome d/u, 45X [Ullrich-Turner syndrome]
- Chromosome 13 [trisomy 13]
- Rothmund-Thomson syndrome
- Hallermann-Streiff
- Orofaciodigital syndrome (type 3)
- Oculo-mandibulo-facial syndrome
- Tricho-Rhino-Phalangeal type 1
- Branchiooculo-facial syndrome
Treatment35
- Composite resin build-up
- Porcelain veneers
- Ceramic crown
- Cast restoration
- Orthodontic alignment and extraction of the tooth
- Autotransplantation
- Extraction and implants
Treatment Planning
Conservative options (composite bonding, veneers) are preferred initially, often in coordination with orthodontics.
Case Study: KBG Syndrome
A patient with KBG syndrome typically presents with macrodont central incisors (unusually wide crowns) and may also have missing premolars.
Macrodontia45
Definition
- Tooth size that is outside the usual limits of variation for that type (Shafer et al. 1974)
- Terminology: Megalodontia, Megadontia, Gigantism (Shafer et al. 1974; Dugmore, 2001)
- For practical purpose this is a tooth that is 1 mm larger than their antimere or the mean dimension of the tooth, and exhibits normal crown, root and pulp morphology (Chaudhary et al. 1997)
- The affected teeth may be of normal or abnormal morphology
Prevalence8
- Male > Female (Brook, 1974; Tonghkoom, 1994; Oashima et al. 1996; Tsai, 1996)
- Primary dentition: 0-2.3% (Brook, 1974; Tonghkoom, 1994; Oashima et al. 1996)
- Permanent dentition: 1.1-3.6% (Brook, 1974; Oashima et al. 1996; Tsai, 1996)
Classification22
- True generalised macrodontia
- Generalised relative macrodontia
- Localised macrodontia
- (Shafer et al. 1958; Nemes and Alberth, 2006; Dugmore, 2001)
True Generalized Type46
- Extremely rare
- All or at least multiple teeth are larger than normal
- Associated with:
- Pituitary gigantism
- Hemifacial hyperplasia
- Otodental syndrome
- Klinefelter syndrome
- KBG syndrome (Herrmann-Pallister-Opitz Syndrome)
- Pineal hyperplasia with hyperinsullinism
Generalized Relative Type4748495051
- Somewhat more common
- Normal or slightly larger sized teeth in smaller jaws
- An illusion of generalized macrodontia
- Hereditary factors
Isolated Macrodontia52
- Involving a single tooth
- Relatively uncommon
- Unknown etiology
- Tooth may appear normal in every aspect except for its size
- Frequently reported in:
- incisors
- canines
- Can be seen in:
- second mandibular premolars
- mandibular molars or premolars
- third molars
- (Dugmore, 2001; Kumar, 2009; Almandey et al. 2010)
Complications17
- Problems with aesthetics
- Arch length discrepancies
- Crowding
- Disruption of the developing occlusion
- Teeth predispose to caries
- Can be very difficult to manage
Treatment35
- Stripping of the macrodont
- Stripping combined with composite resin build-up of the antimere if only one tooth affected
- Extraction and replacement by:
- fixed prosthesis
- removable prosthesis
- implant
- Autotransplantation
Thank You5354
Footnotes
-
Original PDF page 1: L2 Dental Anomalies Part 1, p.1 ↩
-
Original PDF page 2: L2 Dental Anomalies Part 1, p.2 ↩
-
Original PDF page 3: L2 Dental Anomalies Part 1, p.3 ↩
-
Original PDF page 4: L2 Dental Anomalies Part 1, p.4 ↩
-
Original PDF page 5: L2 Dental Anomalies Part 1, p.5 ↩
-
Original PDF page 6: L2 Dental Anomalies Part 1, p.6 ↩
-
Original PDF page 7: L2 Dental Anomalies Part 1, p.7 ↩
-
Original PDF page 8: L2 Dental Anomalies Part 1, p.8 ↩ ↩2 ↩3 ↩4
-
Original PDF page 9: L2 Dental Anomalies Part 1, p.9 ↩
-
Original PDF page 10: L2 Dental Anomalies Part 1, p.10 ↩
-
Original PDF page 11: L2 Dental Anomalies Part 1, p.11 ↩
-
Original PDF page 12: L2 Dental Anomalies Part 1, p.12 ↩
-
Original PDF page 13: L2 Dental Anomalies Part 1, p.13 ↩
-
Original PDF page 16: L2 Dental Anomalies Part 1, p.16 ↩
-
Original PDF page 17: L2 Dental Anomalies Part 1, p.17 ↩
-
Original PDF page 18: L2 Dental Anomalies Part 1, p.18 ↩
-
Original PDF page 19: L2 Dental Anomalies Part 1, p.19 ↩ ↩2
-
Original PDF page 20: L2 Dental Anomalies Part 1, p.20 ↩
-
Original PDF page 21: L2 Dental Anomalies Part 1, p.21 ↩
-
Original PDF page 22: L2 Dental Anomalies Part 1, p.22 ↩
-
Original PDF page 23: L2 Dental Anomalies Part 1, p.23 ↩
-
Original PDF page 24: L2 Dental Anomalies Part 1, p.24 ↩ ↩2 ↩3
-
Original PDF page 26: L2 Dental Anomalies Part 1, p.26 ↩
-
Original PDF page 27: L2 Dental Anomalies Part 1, p.27 ↩
-
Original PDF page 28: L2 Dental Anomalies Part 1, p.28 ↩
-
Original PDF page 29: L2 Dental Anomalies Part 1, p.29 ↩
-
Original PDF page 30: L2 Dental Anomalies Part 1, p.30 ↩
-
Original PDF page 31: L2 Dental Anomalies Part 1, p.31 ↩
-
Original PDF page 32: L2 Dental Anomalies Part 1, p.32 ↩
-
Original PDF page 33: L2 Dental Anomalies Part 1, p.33 ↩
-
Original PDF page 34: L2 Dental Anomalies Part 1, p.34 ↩
-
Original PDF page 35: L2 Dental Anomalies Part 1, p.35 ↩
-
Original PDF page 36: L2 Dental Anomalies Part 1, p.36 ↩
-
Original PDF page 37: L2 Dental Anomalies Part 1, p.37 ↩
-
Original PDF page 38: L2 Dental Anomalies Part 1, p.38 ↩ ↩2 ↩3
-
Original PDF page 39: L2 Dental Anomalies Part 1, p.39 ↩
-
Original PDF page 40: L2 Dental Anomalies Part 1, p.40 ↩
-
Original PDF page 44: L2 Dental Anomalies Part 1, p.44 ↩
-
Original PDF page 45: L2 Dental Anomalies Part 1, p.45 ↩
-
Original PDF page 46: L2 Dental Anomalies Part 1, p.46 ↩
-
Original PDF page 47: L2 Dental Anomalies Part 1, p.47 ↩
-
Original PDF page 48: L2 Dental Anomalies Part 1, p.48 ↩
-
Original PDF page 49: L2 Dental Anomalies Part 1, p.49 ↩
-
Original PDF page 50: L2 Dental Anomalies Part 1, p.50 ↩
-
Original PDF page 52: L2 Dental Anomalies Part 1, p.52 ↩
-
Original PDF page 55: L2 Dental Anomalies Part 1, p.55 ↩
-
Original PDF page 56: L2 Dental Anomalies Part 1, p.56 ↩
-
Original PDF page 57: L2 Dental Anomalies Part 1, p.57 ↩
-
Original PDF page 58: L2 Dental Anomalies Part 1, p.58 ↩
-
Original PDF page 59: L2 Dental Anomalies Part 1, p.59 ↩
-
Original PDF page 60: L2 Dental Anomalies Part 1, p.60 ↩
-
Original PDF page 61: L2 Dental Anomalies Part 1, p.61 ↩
-
Original PDF page 66: L2 Dental Anomalies Part 1, p.66 ↩
-
Original PDF page 67: L2 Dental Anomalies Part 1, p.67 ↩