Sensitivity can be so severe that children avoid brushing, which significantly increases caries risk.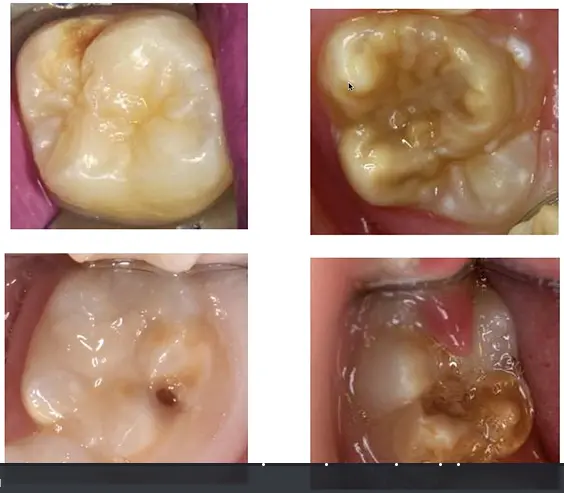 1/7# Molar Incisor Hypomineralisation and Hypomineralised Second Primary Molars1
1/7# Molar Incisor Hypomineralisation and Hypomineralised Second Primary Molars1
Lecture Outcomes2
Upon completion of this lecture, participants should be able to:
- Define Molar Incisor Hypomineralisation (MIH) and Hypomineralised Second Primary Molars (HSPM).
- Describe the prevalence of both conditions within the population.
- Comprehending the prevalence of both conditions globally and regionally
- Understand the clinical manifestations and diagnostic features of both MIH and HSPM.
- Explain the current aetiological concepts and suspected causes of MIH.
- Identify appropriate treatment options and management strategies for teeth affected by MIH and HSPM.
Definitions of Enamel Defects3
Enamel Hypoplasia4
Enamel hypoplasia is a quantitative deficiency of developmental defects of enamel, which usually arise from disruptions of matrix formation
- MIH is a specific type of enamel defect, as are fluorosis, amelogenesis imperfecta, and chronological hypoplasia—each with distinct definitions..

Clinical Presentation
It may be expressed as:
- Pits
- Grooves
- Thin enamel
- Missing enamel
(Source: Clarkson & O’Mullane, 1989)
Enamel Hypomineralisation5
Enamel hypomineralisation is a qualitative enamel defect usually associated with altered enamel mineralisation.
Visual Characteristics
- May be expressed as changes in the translucency or opacity of the enamel.
- Defects may be diffuse or demarcated.
- Coloration can vary between white, yellow, or brown.
- MIH specifically presents as demarcated opacities where the border can be traced.
- This is distinct from fluorosis, which presents as diffuse, patchy opacities where borders are difficult to trace.

Comparative Classification
Developmental defects of enamel are categorized into two primary types:
- Hypoplasia: A quantitative defect related to enamel thickness.
- Hypomineralisation: A qualitative defect related to enamel translucency and mineral content
Mixed Defects Presentation case
A patient presented with both conditions occurring simultaneously:
- Tooth 1.1: Creamy yellow-white opacity on the labial surface (hypomineralisation)
- Tooth 2.1: Localized enamel pitting on the surface (hypoplasia)
- Tooth 2.2 and 3.1: Presented with opacities to varying degrees
- Diagnostic principle: A formal diagnosis requires examination of the patient as a whole, including medical history. Avoid immediate diagnosis based on isolated clinical findings, as amelogenesis imperfecta may present similarly..

Molar Incisor Hypomineralisation67
Molar Incisor Hypomineralisation (MIH) is defined as hypomineralisation of systemic origin affecting one, two, three, or all first permanent molars with/without the permanent incisors.
Affected Dentition
- Primary involvement: First permanent molars and permanent incisors.
- Occasional involvement: Second primary molars and the tips of the permanent canines may also be affected.
- Incisor Hypomineralisation alone exists as a subset condition
- Extended scope now recognizes involvement of second primary molars (HSPM) and both permanent and primary canines
(Source: Weerheijm et al. 2001 and 2003)
Molar Incisor Hypomineralisation (MIH) is a clinical condition of systemic origin affecting one or more of the first permanent molars (FPMs), with or without the involvement of the permanent incisors.
Clinical Presentation and Characteristics
- Enamel Appearance: The condition is characterized by demarcated qualitative defects of enamel. These appear as opacities that vary in color from white-cream to yellow-brown.
- Defect Distribution: The defects are typically asymmetrical. While one molar may be severely affected, the contralateral tooth may appear healthy or have only minor defects.
- Structural Integrity: The enamel thickness is initially normal at eruption, but the hypomineralised areas are porous and mechanically weak. This often leads to post-eruptive breakdown (PEB) under the forces of mastication.
Diagnostic Challenges
- Sensitivity: Affected teeth are often hypersensitive to thermal and mechanical stimuli, making clinical examination and treatment difficult.
- Caries Progression: Due to the porous nature of the enamel and the rapid breakdown of the tooth surface, these teeth are highly susceptible to dental caries, which can progress rapidly to the pulp.
- Aesthetic Concerns: When the permanent incisors are involved, the white or yellow-brown opacities can cause significant aesthetic distress for the child and parents.
Prevalence and Impact
MIH is a global phenomenon with prevalence rates reported between 3% and 25% depending on the population studied. It represents a significant burden for pediatric dentistry due to the high treatment need, the difficulty in achieving effective local anesthesia, and the frequent failure of restorative materials in affected enamel.
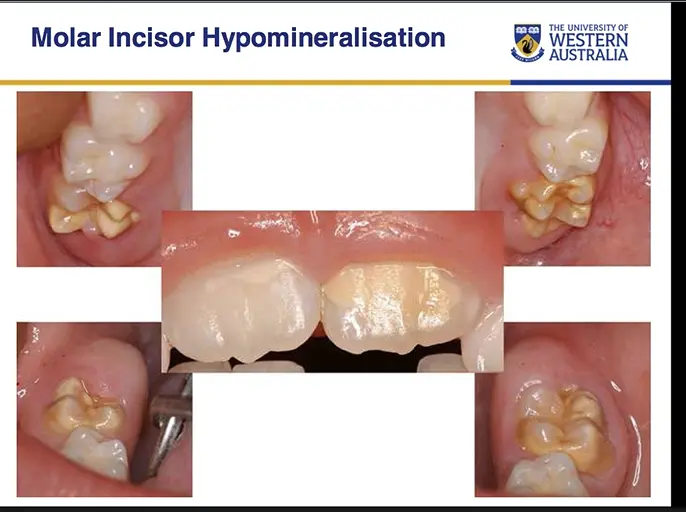
Case Study: Full Mouth Involvement
A child presented with all four first permanent molars affected, demonstrating that involvement does not need to be symmetrical or uniform. The patient also displayed demarcated opacities on the incisors, though incisor involvement remains variable in MIH.
Prevalence8910
Global and Regional Statistics
- The worldwide prevalence varies from 2.4% to 40.2% (Jälevik, 2010).
- Australia: 22% – 44% (Arrow et al. 2008; Balmer et al. 2005).
- New Zealand: 14.9% – 18.8% (Mahoney & Morrison, 2009, 2011).
Diagnostic Timing
Accurate assessment requires examination at 6–7 years of age when all first permanent molars and incisors have erupted. Examination before eruption leads to underestimation.
Systematic Review Findings (Zhao et al. 2018)
A systematic review and meta-analysis of 70 eligible studies identified the following trends in Molar Incisor Hypomineralization (MIH) prevalence:
-
Global Prevalence: The pooled prevalence of MIH is approximately 14.2% globally (roughly 1 in 7 children
- Global average is approximately 1 in 6 children worldwide according to some studies.). -1/7, 1/6 is the accepted
-
Demographics:
- No significant difference was found between males (14.3%) and females (14.4%).
- Prevalence is higher in children aged 10 years or younger (15.1%) compared to older children (12.1%).
Clinical Implications
Due to the high global incidence, particularly in younger children, there is a critical need for appropriate dental healthcare strategies and further research into the etiology of MIH to support prevention.
Aetiology
The exact aetiology of MIH remains unknown, though several systemic factors during tooth development are implicated.
Examination Tip
Do not state the etiology is “unknown” in examination settings; rather, acknowledge that while the exact mechanism is not fully understood, specific associations exist.
Prenatal and Perinatal Factors11
Prenatal Events
Research by Lygidakis et al. (2008) suggests several prenatal influences:
- Pregnancy complications
- Febrile illness during the prenatal period
- Maternal hypertension.
- Medication/drugs administered during delivery (e.g., N2O).
- Assisted delivery or emergency caesarean section.
Perinatal Events
Research by Alaluusua (2010) identifies factors occurring around the time of birth:
- Foetal distress.
- Oxygen deprivation.
- Birth weight complications (low birth weight or high birth weight).
- Premature birth.
Postnatal Factors12
Environmental and Medical Influences
Various postnatal factors have been associated with the development of MIH:
- Environmental Toxins: Exposure to environmental pollutants (Jalevik et al. 2001).
- Metabolic Disturbances: Disruptions in calcium and phosphate metabolism (Jontell and Lindhe 1986).
- Medical Conditions and Treatments:
- Prolonged use of antibiotics (Jalevik et al. 2001).
- Otitis media (Jalevik et al. 2001).
- Frequent febrile childhood diseases (Jalevik et al. 2001).
- Respiratory diseases, including asthma (Jalevik et al. 2001).
Genetic Factors
- Genetic Predisposition: Recent studies have shown an association between the SCUBE1 gene and MIH (Kuhnish et al. 2014).
HSPM Etiology Considerations
- The etiology of HSPM is more perplexing than MIH
- Conventionally, primary teeth develop around the fourth fetal month; however, if this were the sole factor, all primary teeth should be affected, not predominantly the second primary molars
- This suggests complex genetic and environmental interactions distinct from MIH
- Association with the SCOOB1 gene has been identified
- Twin studies indicate confounding factors including maternal smoking, socioeconomic status, and vitamin D levels
Clinical Features1314
Enamel Characteristics
MIH presents as demarcated enamel defects, characterized by an abnormality in the translucency of the enamel, known as opacity (Weerheijm et al. 2001, 2003).
Clinical Presentation and Variability
The severity and presentation of MIH vary greatly among patients:
Clinical Recording Essentials
When documenting MIH, avoid vague terms like “hypomin” or “caries.” Ensure you record the color of the opacity (critical for prognosis), the presence or absence of post-eruptive breakdown (PEB), and the tooth's sensitivity response to stimuli like air or cold.
- Opacities: Clearly demarcated opacities.
- Enamel Integrity: May or may not be associated with post-eruptive enamel breakdown (PEB).
- Symmetry: Defects may appear symmetrically or asymmetrically across the dentition.
- Coloration: Opacities can range in color, including white, creamy yellow, yellow, yellow-brown, or brown.
- Distribution:
- Number of permanent molars affected ranges from 1 to 4.
- Incisors may be unaffected in mild cases or only minimally affected.
- Sensitivity: Affected teeth are often sensitive to cold, heat, and tooth brushing (Fagrell 2008).
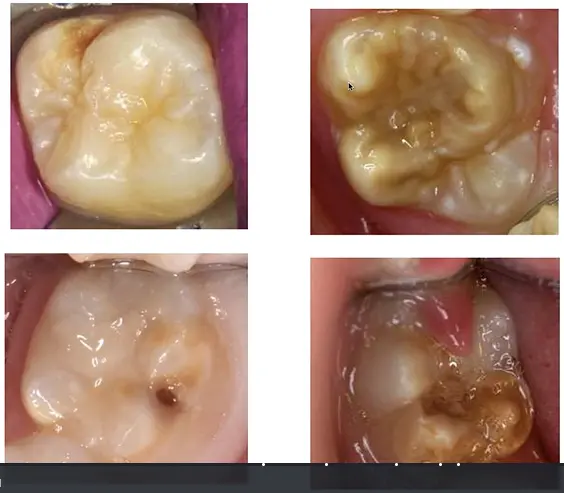
The clinical presentation of Molar Incisor Hypomineralisation (MIH) and Hypomineralised Second Primary Molars (HSPM) is characterized by qualitative enamel defects. These defects vary significantly in severity and distribution between individual patients and even between different teeth in the same mouth.
Visual Characteristics of Enamel Opacities
- Color Variation: Hypomineralised areas appear as demarcated opacities. The color can range from white and cream to yellow or dark brown.
- Mineral Correlation: Darker colors (brown) indicate less mineral density and higher carbon/organic content.
- Protein Content: Brown enamel contains 15–20 times greater protein content (primarily albumin-related) than sound enamel, which severely compromises structural qualities.
- Translucency: The affected enamel lacks the normal translucency of healthy tooth structure, appearing more opaque or matte.
- Demarcation: Unlike fluorosis, which often presents with diffuse patterns, MIH/HSPM lesions show a distinct boundary between the affected and sound enamel.
Severity and Post-Eruptive Breakdown (PEB)
- Mild Presentation: Opacities are present but the enamel surface remains intact. There is no loss of tooth structure, and sensitivity is usually minimal.
- Moderate to Severe Presentation: The enamel is porous and mechanically weak. Shortly after eruption, the forces of mastication can cause the fragile enamel to fracture, leading to post-eruptive breakdown.
- Mechanism of PEB: Due to reduced enamel density, the enamel fractures away under occlusal forces as the tooth erupts into function.
- Consequences: This creates irregular surfaces that lead to plaque accumulation and secondary caries; it is a developmental breakdown that leads to caries susceptibility rather than being primary caries.
- Atypical Restorations: In many cases, the presence of restorations extending onto the buccal or palatal/lingual surfaces in patterns not typical of dental caries is an indicator of underlying hypomineralisation.
Case Study: Atypical Breakdown Patterns
A partially erupted first molar with an operculum showed extensive breakdown of the occlusal surface. This occurred in an atypical location (cuspal surface) and was identified as developmental PEB rather than caries. Breakdown commonly occurs on cuspal surfaces, buccal smooth surfaces, and proximal areas—locations not typical for primary caries.
Distribution Patterns
- Asymmetry: One first permanent molar (FPM) may be severely affected while the contralateral molar remains sound or shows only minor opacities.
- Incisor Involvement: While the molars are the primary diagnostic teeth, the permanent maxillary incisors are frequently involved. Mandibular incisors are less commonly affected and usually exhibit milder defects.
- HSPM Correlation: There is a documented clinical correlation where the presence of hypomineralisation in the second primary molars often serves as a predictor for MIH in the permanent dentition.
Composition15
Mineral and Chemical Characteristics
-
Darker lesions: Characterized by lower mineral content (decreased Calcium/Phosphorus ratio) and increased carbon content.
-
Brown enamel: Contains a 15–21-fold higher protein content compared to sound enamel.
-
White/opaque and yellow enamel: Contains an eight times higher protein content compared to sound enamel
-
Hypomineralization extends deep into enamel and can reach dentine, with a transition zone to unaffected enamel
-
The enamel structure is highly porous, allowing bacterial ingress into dentine even when the tooth appears macroscopically intact
-
Brown and yellow opacities demonstrate significantly lower tooth mineral density compared to normal enamel.
Protein Composition
Protein found in Molar Incisor Hypomineralisation (MIH) enamel consists mainly of serum proteins, including:
- Albumin
- Alpha-1-antitrypsin
- Antithrombin III
Diagnosis16
Clinical Assessment Criteria
- Patient history
- Clinical examination of the teeth
- Radiographic examination
- Evaluation of associated medical conditions
Differential Diagnosis
- Amelogenesis imperfecta (AI)
- Enamel hypoplasia
- Diffuse opacities (fluorosis)
- Tetracycline staining
- Non-carious tooth surface loss
- Normal physiological cuspal and ridge opacities
Judgement Criteria
-
Demarcated opacities (white, yellow, or brown)
-
Presence or absence of post-eruptive breakdown (PEB)
-
Atypical restorations (unusual size, shape, or location)
-
History of first permanent molar extractions
-
Eruption status (noting that unerupted teeth limit classification)
-
Natal and perinatal history is crucial for a complete diagnostic history
-
Radiographic diagnosis is difficult unless obvious post-eruptive breakdown or structural integrity changes are present
-
Examine the patient holistically before assigning a diagnosis
Management Overview1718
Clinical Challenges in Treatment
-
Biological Factors:
- Presence of large immature pulps
- Reduced clinical crown height
- Difficulty in achieving profound local anaesthesia
- Nerve distribution differs in immature teeth, making anesthesia a clinical challenge rather than anecdotal difficulty
-
Structural and Restorative Concerns:
- Poor enamel quality may preclude effective bonding
- High protein content in hypomineralised enamel further compromises bonding strength
- Difficulty in achieving restoration retention
- Increased risk of rapid dental caries progression
- Poor enamel quality may preclude effective bonding
The management of Molar Incisor Hypomineralisation (MIH) and Hypomineralised Second Primary Molars (HSPM) is complex and should be tailored to the individual needs of the child. Key considerations include the severity of the condition, the child’s age, dental anxiety levels, and the long-term prognosis of the affected teeth.
Core Management Objectives
- Symptom Relief: Addressing hypersensitivity, which is a common and distressing feature of hypomineralised enamel.
- Prevention of Breakdown: Implementing strategies to strengthen enamel and prevent post-eruptive breakdown (PEB).
- Restoration of Function and Aesthetics: Utilizing appropriate materials and techniques to restore tooth structure and improve the appearance of anterior teeth.
- Long-term Planning: Determining whether to maintain severely affected teeth or plan for timely extractions and orthodontic intervention.
Clinical Challenges
Management is often complicated by several factors inherent to hypomineralised enamel:
- Hypersensitivity: Difficulty in achieving profound local anesthesia due to underlying subclinical pulp inflammation.
- Material Adhesion: Reduced bond strength of adhesive restorative materials to porous, poorly mineralised enamel.
- Rapid Progression: The potential for rapid transition from intact enamel to extensive cavitation following tooth eruption.
- Behavioral Management: High levels of dental anxiety in children due to previous painful experiences or sensitivity during treatment.
Integrated Treatment Approach
A multi-step approach is recommended, beginning with stabilization and moving toward definitive care:
- Risk Assessment: Identifying the child’s caries risk and the severity of the hypomineralisation.
- Remineralisation and Desensitisation: Use of topical fluorides, casein phosphopeptide-amorphous calcium phosphate (CPP-ACP), or desensitising agents.
- Early Protection: Application of pit and fissure sealants or glass ionomer cements as soon as the tooth is sufficiently erupted.
- Definitive Restoration: Use of composite resins, preformed metal crowns (PMCs), or laboratory-fabricated restorations depending on the extent of the defect.
Lifelong Restorative Burden
Placing a filling on a young permanent tooth commits the child to a lifelong cycle of replacements and increasingly invasive treatments (RCT, crowns, implants). In some cases, timely extraction may be preferable to avoid 50–60 years of operative intervention.
Prevention19
Preventative strategies focus on reducing sensitivity, post-eruptive breakdown (PEB), and secondary caries through the following methods:
Note
While the developmental defect itself cannot be prevented, these strategies aim to prevent secondary complications like PEB and sensitivity.
- Appropriate dietary advice
- Use of fluoride
- Fluoride toothpaste (1000 ppm)
- Fluoride varnish
- Fluoride mouthwashes
- Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP)
- Sugar-free gums
- Fissure sealants
- Regular recall appointments
Management of Sensitivity20
The management of sensitivity involves both home-care techniques and clinical interventions:
Physiological Basis
Pulpal expression of TRPV1 (heat) receptors is significantly higher in MIH-affected teeth. This, combined with a higher innervation density, explains the chronic inflammation and hypersensitivity. Sensitivity can be so severe that children avoid brushing, which significantly increases caries risk.
- Plaque removal using a soft toothbrush and warm water
- Use of fluoride products:
- Fluoride toothpaste (1000 ppm)
- Fluoride varnish
- Fluoride mouthwashes
- CPP-ACP (e.g., Tooth Mousse Plus)
- Desensitizing toothpaste (e.g., Pro-Argin; Colgate)
- Sealing with resin
- Sealing with Glass Ionomer Cement (GIC)
- Resin infiltration
- Compomers
- Clinical caution: Avoid using the triplex (cold air) on brown or yellow opacities without warning; perform a visual inspection first.
- Definitive resin infiltration or sealing should be performed once the tooth has sufficiently erupted.
Restorative Management212223
Various materials and techniques are available for the restorative management of affected teeth:
- Resin composite
- Polyacid modified composite resins (compomers)
- Glass ionomers
- Resin-modified glass ionomers
- Stainless steel crowns (SSCs)
- Cast metal restorations (Gold or semi-precious metal onlays)
- Porcelain fused to metal crowns
Management with Extractions2425
The decision to manage cases via extraction is based on several clinical factors:
Extraction Indications26
- Degree and extent of hypomineralisation or hypoplasia
- Presence of post-eruptive breakdown
- Severity of sensitivity
- Age and level of cooperation of the child
- Any developing malocclusion
- Number of teeth present or missing (specifically third molars)
Extraction Timing Options27
There are three primary strategic options for timing extractions:
- Immediate extraction: Indicated when the tooth is infective or severely broken down.
- Delayed extraction: Timed to optimize the eruption of surrounding teeth (specifically to allow second molars to migrate into the first molar space).
- the tradiational time is when the bifurcation of the 7 is develpoing
- Orthodontic extraction: Performed as a planned component of comprehensive orthodontic treatment.
Contraindications for Extraction28
Extractions may be contraindicated in the presence of certain dental or skeletal conditions:
- Class II malocclusion
- Deep bite
- Lip trap
- Brachyfacial facial type
- Existing spacing
Radiographic Case Study: Pre-Extraction
A panoramic radiograph of a 9-year-old female presents a case with an orthodontic plan to extract all first molars due to severe hypomineralisation. Clinical attention is directed toward the positions of the lower second premolars.
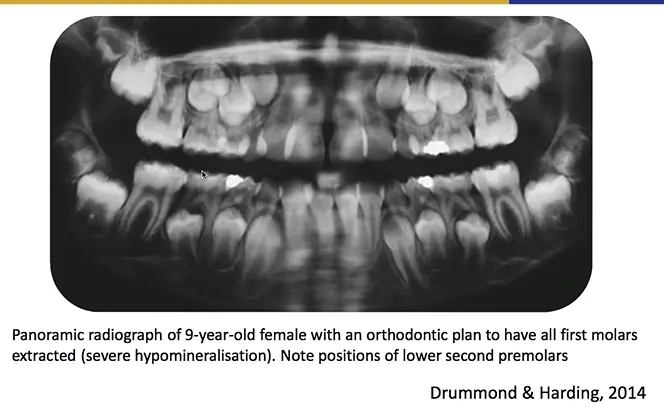
- the concept with extraction is to let the 7’s and 8’s move in
Radiographic Case Study: Post-Extraction
A follow-up panoramic radiograph taken 3 years after the extractions shows the development and eruption paths of the lower second premolars.
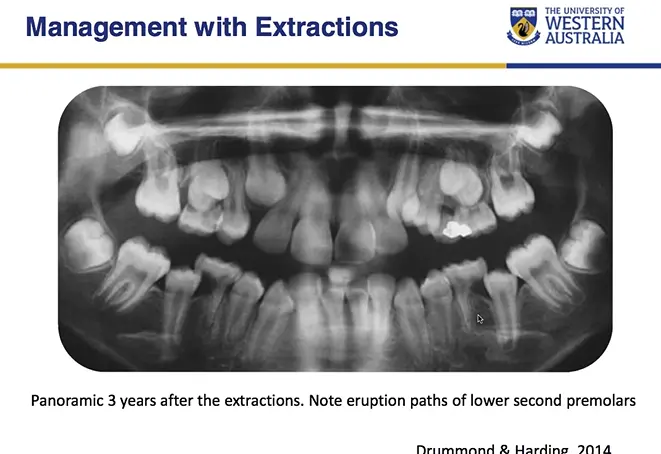
- the lower second molars in this case actually erupted distally and resorbed part of the E
- this case gone awry is why orthodontic consideration is important in a regular management plan
Management of Anterior Teeth293031
Permanent Anterior Teeth
Management options for permanent anterior teeth affected by hypomineralisation include:
-
Begin with conservative spectrum: microabrasion, resin infiltration, or etch-bleach-seal techniques
-
Avoid porcelain veneers or crowns on immature teeth to prevent a 50–60 year restorative burden
-
Micro-abrasion (with or without bleaching)
-
PMMA resin
-
Composite veneers
-
Zirconia veneers or crowns
Microabrasion Techniques
Clinical documentation of microabrasion procedures used in the management of anterior tooth defects.
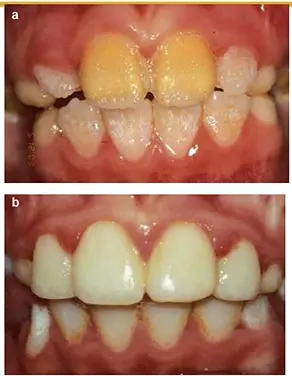
Case Study: Microabrasion Success
A patient with demarcated opacities on incisors underwent 2–3 cycles of microabrasion using rubber dam isolation and pumice-acid slurry (hydrochloric or phosphoric acid).
- Protocol: 30–60 seconds per tooth per cycle with remineralization phases between
- Outcome: Excellent aesthetic improvement without irreversible tooth structure removal
- Safety: Mandatory isolation prevents gingival burns; avoid over-treatment to prevent sensitivity
The management of anterior teeth affected by Molar Incisor Hypomineralisation (MIH) primarily focuses on addressing aesthetic concerns and managing any associated sensitivity. The clinical presentation can range from creamy-white or yellow-brown opacities to more severe enamel breakdown.
Aesthetic Management Strategies
- Microabrasion: This technique is effective for superficial opacities. It involves the controlled removal of a thin layer of enamel using an abrasive paste (typically hydrochloric acid and pumice) to improve the appearance of the tooth surface.
- Bleaching (Tooth Whitening): External bleaching can be used to lighten the color of the affected enamel, making the opacities less noticeable. This is often used in conjunction with other treatments.
- Resin Infiltration: A minimally invasive approach where a low-viscosity resin is used to penetrate the porous enamel of the white spot lesions. This changes the optical properties of the enamel, often making the lesion blend in with the surrounding healthy tooth structure.
- Composite Veneers: For more significant aesthetic defects or where conservative measures are insufficient, direct or indirect composite veneers can be used to mask the discoloration and restore the tooth’s contour.
Case Study: Composite Veneer Limitations
A case of enamel pitting managed with composite veneers showed marginal staining, gingival inflammation, and discoloration at follow-up.
Advantage: Because tooth structure was preserved (minimal/no prep), these issues are easy to rectify compared to irreversible preparations.
this is a case of hypoplasia due to amelogenesis imperfecta
- Porcelain Veneers: Generally reserved for older patients once gingival maturation is complete, porcelain veneers provide a durable and highly aesthetic long-term solution.
Sensitivity and Surface Protection
- Topical Fluorides: Application of high-concentration fluoride varnishes can help reduce sensitivity and promote remineralization of the hypomineralised areas.
- Casein Phosphopeptide-Amorphous Calcium Phosphate (CPP-ACP): Products containing CPP-ACP can be used to deliver bioavailable calcium and phosphate to the tooth surface, aiding in the stabilization of the enamel and reduction of sensitivity.
- Fissure Sealants and Flowable Resins: In cases where there is minor surface pitting or loss of integrity, flowable resins can be used to seal the surface and prevent further breakdown or staining.
Clinical Considerations for Extraction
When planning extractions, clinicians must evaluate the extent of hypomineralization, the child's level of cooperation, and any existing malocclusion or missing teeth. An orthodontic consultation is often necessary to ensure optimal long-term outcomes.
Management Decisions
Extraction Strategies
- Immediate
- Indicated for severe pain or infection.
- Intermediate
- Extract when second permanent molars (7’s) are in the correct position.
- Manage sensitivity, pulp health, and enamel fractures in the interim.
- Long term
- Extract as part of a comprehensive orthodontic treatment plan.
- Manage sensitivity, pulp health, and enamel fractures until extraction.
Extraction Timing and Planning32
Long-Term Restoration Planning
- Immediate Phase
- Use of Compomer, Stainless Steel Crowns (SSC), or Glass Ionomer Cement (GIC).
- Intermediate Phase
- Use of Stainless Steel Crowns (SSC) or Composite resin.
- Long term Phase
- Final restorations such as gold/metal overlays or full crowns.
Management Options by Severity3334
Management Strategies for Hypomineralised Teeth (Revised Dec 2018)
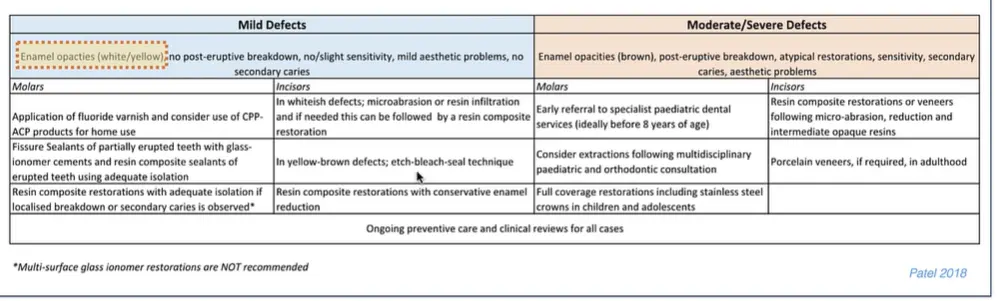 Mild Defects
Characteristics: Enamel opacities (white/yellow), no post-eruptive breakdown, no/slight sensitivity, mild aesthetic problems, no secondary caries.
Mild Defects
Characteristics: Enamel opacities (white/yellow), no post-eruptive breakdown, no/slight sensitivity, mild aesthetic problems, no secondary caries.
- Molars
- Application of fluoride varnish.
- Consider use of CPP-ACP products for home use.
- Fissure sealants: Use glass-ionomer cements for partially erupted teeth; use resin composite sealants for fully erupted teeth with adequate isolation.
- Resin composite restorations with adequate isolation if localised breakdown or secondary caries is observed.
- Preventive resin restorations
- Note: Multi-surface glass ionomer restorations are NOT recommended.
- Incisors
- Whitish defects: Microabrasion or resin infiltration; can be followed by resin composite restoration if needed.
- Yellow-brown defects: Etch-bleach-seal technique.
- Resin composite restorations with conservative enamel reduction.
Moderate/Severe Defects Characteristics: Enamel opacities (brown), post-eruptive breakdown, atypical restorations, sensitivity, secondary caries, aesthetic problems.
- Molars
- Early referral to specialist paediatric dental services (ideally before 8 years of age).
- Consider extractions following multidisciplinary paediatric and orthodontic consultation.
- Full coverage restorations, including stainless steel crowns, for children and adolescents.
- Indirect restorations
- Orthodontic extraction plans
- Incisors
- Resin composite restorations or veneers following micro-abrasion, reduction, and intermediate opaque resins.
- Porcelain veneers, if required, in adulthood.
Referral Rationale
Treatment on young patients is complex; decisions made may significantly compromise long-term tooth survival.
General Care
- Ongoing preventive care and clinical reviews are required for all cases.
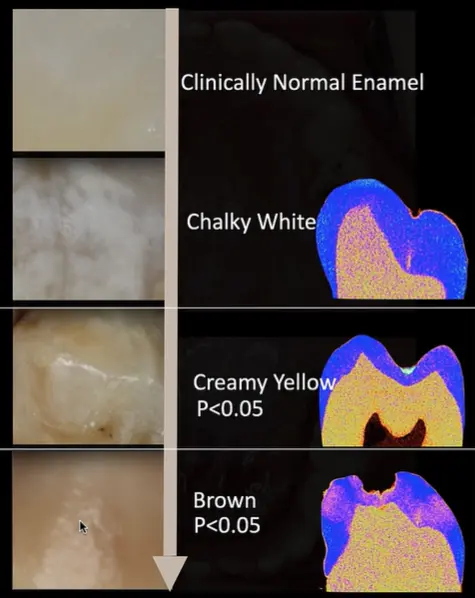
Tooth Mineral Density (TMD) in Hypomineralised Molars
Research Summary: Micro-CT Analysis (Eur Arch Paediatr Dent. 2017)
This study evaluated the tooth mineral density (TMD) for different lesion types in hypomineralised first permanent molars (FPMs) compared to unaffected enamel.
-
TMD Findings by Lesion Type:
- Brown Lesions: 1.79 g/cm³ (Lowest density; P < 0.05)
- Yellow/Creamy Lesions: 2.21 g/cm³ (P < 0.05)
- White Lesions: 2.43 g/cm³ (Similar to unaffected enamel)
- Unaffected Enamel: 2.46 g/cm³
-
Density Gradients:
- Brown and Yellow/Creamy: TMD increased from the outer-third to the inner-third of the enamel (P < 0.05).
- White and Unaffected: TMD decreased from the outer-third to the inner-third of the enamel (P < 0.05).
-
Conclusion: TMD is significantly lower in brown and yellow/creamy lesions. White lesions do not show a statistical difference in TMD compared to clinically normal enamel.
- Children with HSPM have 4.66 times greater odds (up to 6x in some studies) of developing MIH.
- Children with HSPM have 4.66 times greater odds (up to 6x in some studies) of developing MIH.
Hypomineralised Second Primary Molars35363738
Clinical Prevalence and Associations
-
Prevalence
- Approximately 10% globally; a recent Australian study (Owen et al. 2017) reported 14%.
-
Predictive Value for MIH
- Hypomineralised lesions on second primary molars (HSPM) are a predictive sign of Molar Incisor Hypomineralisation (MIH).
- Odds Ratio (OR): 4.66.
- Co-occurrence prevalence: ~20% (Garot et al. 2018).
-
Associated Findings
- There is a noted association between HSPM and hypomineralised primary canines.
Hypomineralised Second Primary Molars (HSPM) is a condition characterized by qualitative structural defects of the enamel in one to four second primary molars. This condition is often considered a precursor or clinical predictor for Molar Incisor Hypomineralisation (MIH) in the permanent dentition.
Clinical Presentation and Diagnosis
The clinical appearance of HSPM is similar to that of MIH, featuring demarcated opacities that vary in color from white and cream to yellow and brown. These defects are typically limited to the enamel and are frequently found on the occlusal and buccal surfaces of the second primary molars.
- Demarcated Opacities: Clear boundaries between the affected and sound enamel.
- Post-Eruptive Breakdown (PEB): In severe cases, the weakened enamel may fracture under occlusal forces shortly after eruption, leading to rapid dental caries progression.
- Sensitivity: Affected teeth may exhibit hypersensitivity to thermal and mechanical stimuli, complicating oral hygiene and clinical treatment
- Disproportionate breakdown of second primary molars (last to erupt, shortest time in mouth) compared to other teeth.
- Higher DMFT values due to plaque accumulation in irregular surfaces and sensitivity-related cleaning avoidance.
- Atypical lesion locations (palatal surfaces, buccal surfaces) despite good plaque control elsewhere..
Prevalence and Association with MIH
Research indicates a significant correlation between the presence of HSPM and the subsequent development of MIH in the permanent first molars. Children diagnosed with HSPM are at a higher risk of having MIH.
- Epidemiological Trends: Prevalence rates vary globally but generally range between 5% and 15%.
- Predictive Value: The presence of even a single hypomineralised second primary molar should alert the clinician to monitor the eruption of permanent first molars closely.
Etiological Factors
The etiology of HSPM is believed to be multifactorial, involving systemic disturbances during the prenatal, perinatal, or early postnatal periods. Potential contributing factors include:
- Maternal illness or medication use during pregnancy.
- Complications during childbirth (e.g., low birth weight, hypoxia).
- Early childhood illnesses such as high fevers, respiratory infections, or gastrointestinal disturbances.
- Environmental factors and nutritional deficiencies.
Etiological Complexity
Unlike MIH, which aligns with birth timing, HSPM is perplexing because primary teeth calcify at the fourth fetal month, yet usually only second primary molars are affected. Twin studies suggest associations with maternal smoking, socioeconomic factors, and vitamin D levels.
Management Strategies for HSPM
Effective management of HSPM requires early identification and a proactive approach to prevent tooth loss and manage discomfort.
-
Preventive Care:
- High-frequency fluoride varnish applications to promote remineralization.
- Use of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) pastes.
- Application of pit and fissure sealants on intact but opacified surfaces.
-
Restorative Interventions:
- Glass Ionomer Cements (GIC): Often used as interim restorations due to their fluoride-releasing properties and chemical bond to enamel.
- Composite Resins: Suitable for smaller defects where moisture control can be achieved.
- Preformed Metal Crowns (PMCs): Recommended for teeth with extensive post-eruptive breakdown or severe sensitivity to provide full coverage and prevent further deterioration.
Long-term Monitoring
Regular follow-up appointments are essential to monitor the integrity of restorations and the eruption pattern of the permanent dentition. Early intervention in the primary dentition serves as a critical step in reducing the future burden of care for MIH.
Turner Tooth Risk
Chronic infection or inflammation associated with HSPM can disrupt amelogenesis of the underlying permanent successor (e.g., tooth 4.5 developing below infected 8.5), resulting in hypomineralization of the permanent tooth (Turner tooth).
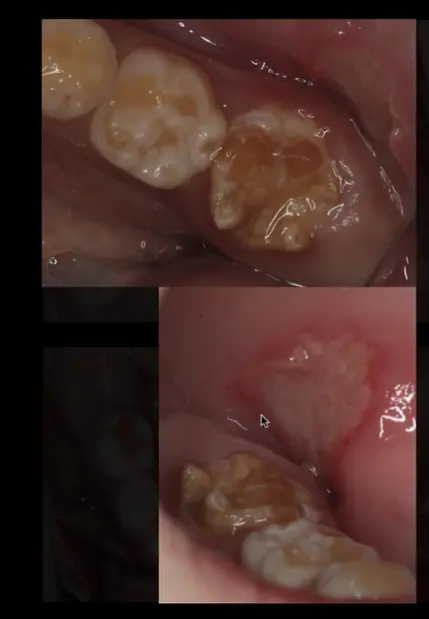
Case Study: Primary Dentition Presentation
A child aged 3–5 years presented with lower second primary molars (Es) completely broken down, despite good plaque control on other teeth and no other cavitated lesions. Brown opacities were noted on primary canines (6.3, 7.3), leading to a diagnosis of HSPM rather than caries as the primary etiology.

case study
Not caries but HSPM< child 3-5, peb in E’s

Case Study: Mixed Dentition with HSPM and MIH
A comprehensive case demonstrating the 4x odds ratio:
- Tooth 5.5: Large GIC restoration breaking down (should have been a stainless steel crown).
- Tooth 6.5: Previously restored with GIC, now completely broken down.
- Tooth 4.6: Large ICDAS 6 disto-occlusal-palatal lesion in an atypical location.
- Tooth 2.6 and 3.6: Demarcated brown opacities on cuspal areas (MIH).
- Tooth 7.5: Restoration in atypical location (disto-occlusal-buccal) indicating developmental defect.
Global Prevalence Study (Zhao et al. 2018)
A systematic review and meta-analysis of 70 studies was conducted to estimate the pooled prevalence of Molar Incisor Hypomineralization (MIH) globally.
- Pooled Prevalence: 14.2% worldwide.
- Regional Variations:
- South America: 18.0%
- Spain: 21.1% (highest reported prevalence)
- Demographics:
- No significant difference between males (14.3%) and females (14.4%).
- Children ≤ 10 years old showed a significantly higher prevalence (15.1%) compared to older children (12.1%).
Clinical Implications
Due to the high global incidence, particularly in younger children, there is an imperative need for appropriate dental healthcare strategies and further research into the etiology of MIH for prevention.
Judgement Criteria for MIH39
Diagnostic Definitions (Weerheijm et al. 2003)
-
Demarcated Opacity
- An alteration in enamel translucency of variable degree.
- Enamel is of normal thickness with a smooth surface.
- Colors range from white to yellow or brown.
-
Posteruptive Enamel Breakdown (PEB)
- A defect indicating surface deficiency occurring after tooth eruption.
- Often associated with a pre-existing demarcated opacity.
-
Atypical Restoration
- Restorations where the size and shape do not conform to typical caries patterns.
- In molars, these often extend to buccal or palatal smooth surfaces, frequently with an opacity at the border.
- In incisors, buccal restorations not related to trauma are suspected.
-
Extracted Molar due to MIH
- Absence of a first permanent molar (FPM) evaluated in the context of the remaining dentition.
- Suspected if other FPMs have opacities/atypical restorations or if FPMs are missing in a dentition where incisors show demarcated opacities.
-
Unerupted
- The subject molar or incisor has not yet entered the oral cavity.
Clinical Notes and Exclusions
- Caries Interaction: Large caries lesions with demarcated opacities at the borders or on non-carious surfaces should be judged as MIH.
- Differential Diagnosis: The following conditions should be excluded:
- Amelogenesis imperfecta
- Hypoplasia
- Diffuse opacities / Fluorosis
- White spot lesions (caries)
- Tetracycline staining
- Erosion
- White cuspal and marginal ridges
Ultra Structural Considerations4041
Pulpal Expression of TRPV1 (Rodd et al. 2007)
This study investigated the expression of the transient receptor potential ion channel (TRPV1), a noxious heat receptor, to understand the biological mechanisms underlying thermal hypersensitivity in MIH teeth.
- Methodology: Quantitative immunocytochemical analysis of 17 sound and 18 hypomineralised molars (10 intact, 8 with enamel loss).
- Key Findings:
- Mean neuronal and vascular TRPV1 expression was significantly greater in hypomineralised teeth compared to sound samples.
- This increase was observed in both intact hypomineralised enamel and teeth with enamel loss.
- Conclusion: Increased TRPV1 expression suggests underlying pulpal inflammation, which may explain the heat sensitivity reported by patients.
Histological Analysis Regions
Quantitative analysis focused on three specific pulpal areas:
- Pulp horn
- Subodontoblastic plexus
- Mid-coronal region
Comparative Data Metrics
- Innervation Density: Measured via % area PGP 9.5.
- Leucocyte Accumulation: Measured via % area LCA.
- Vascularity: Measured via % area UEA I.
Bacterial Invasion of Dentinal Tubules (Fagrell et al. 2008)
This histological study examined whether bacteria could penetrate apparently intact but hypomineralised enamel in MIH-affected permanent molars.
- Findings in Hypomineralised Areas:
- Bacteria were identified in dentinal tubules beneath hypomineralised enamel, even when the surface appeared intact.
- In areas with bacterial penetration, a zone of reparative dentin was often found.
- One specimen showed an active inflammatory reaction in the coronal pulp.
- SEM Observations:
- Bacteria were found located on the surface of odontoblast processes.
- Odontoblast processes appeared larger in areas where bacteria were present.
- No bacteria were found in close proximity to the pulp itself.
- Findings in Normal Areas:
- Sections from sound areas showed normal pulp free from bacteria or inflammatory infiltrates.
- SEM revealed empty dentinal tubules without signs of bacteria or odontoblast processes in these regions.
Conclusion
Oral bacteria may penetrate through porous hypomineralised enamel into the dentin, contributing to the hypersensitivity and pulpal reactions characteristic of MIH.
Clinical Implications of Enamel Composition
- Albumin-related proteins are significantly elevated in affected enamel, contributing to its structural weakness.
- Compromised adhesion occurs due to altered enamel structure; however, deproteinizing with sodium hypochlorite may improve bond strength.
- Maintaining sound enamel margins is crucial for the long-term success of restorations in MIH-affected teeth.
Behavioural Considerations42
Long-term Outcomes and Dental Anxiety (Jälevik and Klingberg 2012)
A longitudinal study followed children with severe MIH from age 9 to age 18 to assess treatment burden and psychological impact.
-
Treatment Burden:
- By age 18, the MIH group had a significantly higher DMFT (Decayed, Missing, Filled Teeth) score.
- MIH patients underwent treatment of their first permanent molars 4.2 times more frequently than the control group.
-
Behavioral Management:
- Behavior Management Problems (BMP) remained significantly more common in the MIH group at age 18.
-
Dental Fear and Anxiety (DFA):
- While DFA was high in childhood, it reduced by age 18 to levels comparable with the control group.
- Satisfaction with dental visits (DVSS scores) did not differ significantly between groups at age 18.
-
Sensitivity impact: Children often avoid brushing sensitive areas, which significantly increases their caries risk.
-
Anesthesia challenges: Altered nerve distribution in MIH teeth makes local anesthesia less effective, which can be traumatizing for the child.
-
Treatment anxiety: Repeated failed restorations create cycles of repair and replacement, leading to increased fear and behavioral management issues.
-
Clinical Goal: Identify MIH early to manage it appropriately and avoid condemning the child to lifelong restorative cycles.
Conclusion
Patients with severe MIH require significantly more dental treatment throughout adolescence, though their dental fear tends to normalize by adulthood.
Treatment Criteria For MIH43
Management Strategies by Dental Age (Lygidakis et al. 2010)
| Level of Severity | Early Mixed Dentition | Late Mixed Dentition | Full Permanent Dentition |
|---|---|---|---|
| Mild | - Prevention - Adhesive + sealant | - Composite restoration - Anterior: Microabrasion, bleach + sealant | - Composite restoration |
| Severe | - Prevention & symptom control - Posterior: Adhesive + sealant | - Anterior: Microabrasion, bleach + sealant - Glass ionomer restoration | - Composite restoration - Preformed metal crown - Orthodontic extraction - Cast restoration |
Clinical Considerations
- For young dental age with severe breakdown, clinicians should weigh the benefits of extraction versus the placement of stainless steel crowns.
- In the permanent dentition phase, the focus shifts toward permanent restorations such as crowns and onlays.
- Regarding anterior aesthetics, it is recommended to delay invasive procedures until growth is complete whenever possible.
Bonding Strategies for MIH Affected Enamel44
Adhesion to MIH-Affected Tissues (Krämer et al. 2018)
This study evaluated resin composite bonding to enamel and dentin affected by MIH using various adhesive systems (Clearfil SE Bond, Scotchbond Universal, and OptiBond FL).
-
Bonding to Enamel:
- Sound enamel has significantly higher bond strength (μ-TBS) than MIH-affected enamel.
- Conventional phosphoric acid etching produces a weak, less pronounced etching pattern in MIH enamel.
- Two-step self-etch and two-step etch-and-rinse adhesives showed the lowest values and highest pre-test failure rates in affected enamel.
- OptiBond FL performed better than Clearfil SE Bond on affected enamel.
- Pre-treatment with NaOCl or Icon did not increase bond strength but did reduce pre-test failures.
- Bond strength is significantly compromised due to high protein content and porosity.
- Deproteinization using sodium hypochlorite may improve bonding.
- Moisture control on partially erupted teeth is extremely difficult; rubber dam, gingival retraction, or even gingivectomy may be necessary.
- Avoid complex multi-surface composites in favor of full coverage when bonding is compromised.
-
Bonding to Dentin:
- Bond strengths to MIH-affected dentin were independent of the adhesive used.
- MIH-affected dentin can be bonded using conventional strategies.
Clinical Significance
The primary limiting factor in MIH restorations is the porous, hypomineralised enamel. While dentin bonding remains reliable, the resin-enamel interface is the weak link due to the altered structural morphology of the affected enamel.
Note Taking Guide45
Clinical Assessment Criteria
When evaluating molar hypomineralisation, distinguish between qualitative and quantitative defects and document the following clinical features:
- Colour: Note the specific shade of the opacities (e.g., white, yellow, or brown).
- Severity and Structural Integrity: Assess the extent of the defect and check for the presence of post-eruptive breakdown (PEB).
- Symptoms: Record patient reports of sensitivity, particularly to thermal changes or airflow.
Inappropriate Documentation
Avoid non-descriptive entries such as "1.6 hypo" or "2.6 caries" as they provide no information on severity, prognosis, or treatment planning needs.
Clinical Case Example
- Tooth 16 (Upper Right First Permanent Molar):
- Appearance: Creamy yellow opacities involving the majority of the coronal surface.
- Structural Status: Mild mesiopalatal (MPal) breakdown.
- Sensitivity: Significant (++) sensitivity to air.

Systematic Examination Protocol
- Count all teeth systematically.
- Examine all surfaces (not just where eyes are drawn).
- Check soft tissues.
- Look for anomalies (supernumeraries, missing teeth, discoloration).
- Avoid jumping immediately to obvious findings without systematic review, which may lead to missed diagnoses (e.g., missing intrinsic discoloration on 5.1 while focusing on 2.1).
Case Study: Differential Diagnosis Importance
A child presented with severe posterior breakdown and opacities initially suspected as MIH. However, the child had a history of oncology treatment and graft-versus-host disease. The breakdown was related to medical treatment affecting calcification, not MIH. This highlights the importance of comprehensive medical history before assigning diagnosis.
Footnotes
-
Original PDF page 1: L5 - MIH and HSPM, p.1 ↩
-
Original PDF page 2: L5 - MIH and HSPM, p.2 ↩
-
Original PDF page 5: L5 - MIH and HSPM, p.5 ↩
-
Original PDF page 3: L5 - MIH and HSPM, p.3 ↩
-
Original PDF page 4: L5 - MIH and HSPM, p.4 ↩
-
Original PDF page 6: L5 - MIH and HSPM, p.6 ↩
-
Original PDF page 7: L5 - MIH and HSPM, p.7 ↩
-
Original PDF page 8: L5 - MIH and HSPM, p.8 ↩
-
Original PDF page 9: L5 - MIH and HSPM, p.9 ↩
-
Original PDF page 38: L5 - MIH and HSPM, p.38 ↩
-
Original PDF page 10: L5 - MIH and HSPM, p.10 ↩
-
Original PDF page 11: L5 - MIH and HSPM, p.11 ↩
-
Original PDF page 12: L5 - MIH and HSPM, p.12 ↩
-
Original PDF page 13: L5 - MIH and HSPM, p.13 ↩
-
Original PDF page 14: L5 - MIH and HSPM, p.14 ↩
-
Original PDF page 15: L5 - MIH and HSPM, p.15 ↩
-
Original PDF page 16: L5 - MIH and HSPM, p.16 ↩
-
Original PDF page 17: L5 - MIH and HSPM, p.17 ↩
-
Original PDF page 18: L5 - MIH and HSPM, p.18 ↩
-
Original PDF page 19: L5 - MIH and HSPM, p.19 ↩
-
Original PDF page 20: L5 - MIH and HSPM, p.20 ↩
-
Original PDF page 21: L5 - MIH and HSPM, p.21 ↩
-
Original PDF page 22: L5 - MIH and HSPM, p.22 ↩
-
Original PDF page 26: L5 - MIH and HSPM, p.26 ↩
-
Original PDF page 27: L5 - MIH and HSPM, p.27 ↩
-
Original PDF page 23: L5 - MIH and HSPM, p.23 ↩
-
Original PDF page 24: L5 - MIH and HSPM, p.24 ↩
-
Original PDF page 25: L5 - MIH and HSPM, p.25 ↩
-
Original PDF page 28: L5 - MIH and HSPM, p.28 ↩
-
Original PDF page 29: L5 - MIH and HSPM, p.29 ↩
-
Original PDF page 30: L5 - MIH and HSPM, p.30 ↩
-
Original PDF page 31: L5 - MIH and HSPM, p.31 ↩
-
Original PDF page 32: L5 - MIH and HSPM, p.32 ↩
-
Original PDF page 33: L5 - MIH and HSPM, p.33 ↩
-
Original PDF page 34: L5 - MIH and HSPM, p.34 ↩
-
Original PDF page 35: L5 - MIH and HSPM, p.35 ↩
-
Original PDF page 36: L5 - MIH and HSPM, p.36 ↩
-
Original PDF page 37: L5 - MIH and HSPM, p.37 ↩
-
Original PDF page 39: L5 - MIH and HSPM, p.39 ↩
-
Original PDF page 40: L5 - MIH and HSPM, p.40 ↩
-
Original PDF page 41: L5 - MIH and HSPM, p.41 ↩
-
Original PDF page 42: L5 - MIH and HSPM, p.42 ↩
-
Original PDF page 43: L5 - MIH and HSPM, p.43 ↩
-
Original PDF page 44: L5 - MIH and HSPM, p.44 ↩
-
Original PDF page 45: L5 - MIH and HSPM, p.45 ↩