Antibiotics, Local Anaesthetics and Analgesics in Paediatric Dentistry
Course Information1
- Module: Paediatric Dentistry Module (DENT 5312)
- Institution: UWA Dental School, The University of Western Australia
Presenter Details
- Dr Jilen Patel
- Specialist Paediatric Dentist
- Senior Lecturer, Clinical Dentistry
Prescription Writing Guidelines
Essential Therapeutic Guidelines2
To ensure safe and effective clinical practice, practitioners must refer to the Oral and Dental Therapeutic Guidelines (Version 3). Key chapters for review include:
Recommended Reading and Resources
- Dental prescriptions and prescription-writing: Fundamental protocols for issuing medication.
- Practical information on using drugs in dentistry: Clinical application and pharmacological considerations.
- Acute odontogenic infections: Management strategies and specific prescribing for dental infections
- Avoid broad-spectrum antibiotics when a narrow-spectrum agent is sufficient to prevent wiping out gut flora and causing gastrointestinal issues.
- PBS (Pharmaceutical Benefits Scheme): Use this online database to check drug availability, suspension concentrations, and prescribing restrictions.
- Melamed's textbooks are the primary reference for nerve block success rates in paediatric patients..
Legal and Clinical Requirements for Prescriptions
Essential Prescription Components3
All prescriptions must be legible and contain the following information to meet legal and clinical standards:
-
Prescriber Information
- Full name, practice address, and telephone number.
- Professional qualifications.
- Handwritten signature of the prescriber.
-
Patient Information
- Full name and address.
- Date of birth.
- Patient weight (this is critical for pediatric dosing calculations).
-
Medication Details
- Date the prescription is issued.
- Full drug name (avoid abbreviations).
- Drug strength (e.g., 250mg, 500mg).
- Drug form (e.g., tablet, capsule, suspension).
- Quantity of the drug to be dispensed.
-
Administration Instructions
- Specific dose, route of administration, frequency, and duration of treatment.
- Clear instructions for the patient (avoid vague phrases such as “take as directed”).
- The notation “for dental treatment only” must be included.
Instructor notes:
- Dentists cannot prescribe repeat scripts.
- Generic names (e.g., Metronidazole) must be used in full rather than brand names (e.g., Flagyl).
- Suspension concentrations must be specified in mg/mL.
- The route of administration (e.g., "Orally") must be explicitly stated.
- Practicality: For children, consider dosing "half an hour before each meal and the final dose at bedtime" rather than "one hour before meals" to improve compliance.
Case Study: Management of Odontogenic Infections
- Clinical Presentation: Patient with a dental alveolar abscess associated with tooth 84 (ICDAS 5 lesion). Radiographs showed gross radiolucency extending into the pulp space and significant furcal lucency.
- Findings: Qualitative (brown opacity) and quantitative (pitting) enamel defects on teeth 51 and 61. 2nd primary mandibular molar showed resorption of mesial and distal roots.
- Management Error: A GP had previously placed a stainless steel crown without a necessary pulpotomy, then performed incision and drainage twice and prescribed three courses of antibiotics without resolving the source.
- Outcome: Highlighted the necessity of knowing when to extract versus prescribe, and the importance of identifying sessile abscesses through soft tissue retraction.
Common Antibiotics in Paediatric Dentistry45
This section outlines the common antibiotics utilized within the field of paediatric dentistry.
Antibiotic Stewardship
Antibiotics should target the specific infection. Narrow-spectrum antibiotics are preferred over broad-spectrum agents to minimize impact on gut flora and reduce gastrointestinal problems.
The following antibiotics are commonly prescribed in paediatric dental practice:
- Phenoxymethylpenicillin (Penicillin V)
- Amoxycillin
- Cephalexin
- Clindamycin
- Metronidazole (to be used in addition to one of the above antibiotics for spreading odontogenic infections)
-
- Concentrations vary (e.g., 125mg/5mL vs. 250mg/5mL), and the specific concentration must be delineated on the prescription to avoid confusion.
-
Penicillins and Alternatives
Clinical Profile6
Phenoxymethylpenicillin Penicillin V
- Classification: Narrow spectrum penicillin.
- Activity: Effective against Actinomyces, most Strep spp., and Fusobacterium spp.
- Limitations: Inactivated by strains producing beta-lactamase enzymes.
- Indications: Drug of first choice in odontogenic infections due to its narrow and appropriate spectrum of activity.
- Tolerability: Has fewer gastrointestinal problems than amoxycillin and is less likely to cause a rash.
Dosage and Administration
- Dose: 12.5 mg/kg up to 500 mg orally.
- Frequency: Taken 6 hourly for 5 days.
- Timing: Administer 1 hour before meals or 2 hours after meals.
- Compliance: Consideration should be given to patient compliance with the 6-hourly regimen.
- Practically, often prescribed half an hour before meals and at bedtime to improve compliance.
- Available Preparations:
- 125 mg/5 mL
- 150 mg/5 mL
- 250 mg/5 mL
Pharmaceutical Benefits Scheme (PBS) Listings
Phenoxymethylpenicillin is available under the General Schedule for Dental Practitioners in various forms:
- Capsules: 250 mg (50), 500 mg (50)
- Tablets: 250 mg (25), 500 mg (25)
- Oral Liquid/Powder:
- 125 mg/5 mL powder for oral liquid (100 mL)
- 150 mg/5 mL oral liquid (100 mL)
- 250 mg/5 mL powder for oral liquid (100 mL)
Amoxycillin
Clinical Profile and Dosage
- Classification: Moderate spectrum penicillin.
- Administration: Not affected by food and requires fewer oral doses per day compared to Penicillin V.
- Dose: 12.5 mg/kg up to 500 mg orally.
- Frequency: Taken 8 hourly for 5 days.
- Available Preparations: 100 mg/mL; 125 mg/5 mL; 250 mg/5 mL; 500 mg/5 mL.
Note: Amoxicillin + clavulanate has a limited role in treating odontogenic infections
- If used, there is little need to supplement with Metronidazole as clavulanic acid targets many anaerobes..
Cephalexin
Clinical Profile and Dosage
- Classification: Moderate spectrum cephalosporin.
- Indications: May be an alternative for patients sensitive to penicillin (excluding those with immediate hypersensitivity).
- Contraindications: Not appropriate for patients on long-term penicillin or those who have taken a related penicillin more than once in the previous month.
- Caution in children with a history of acute rheumatic fever on routine antibiotics.
- Dose: 12.5 mg/kg up to 500 mg orally.
- Frequency: Taken 8 hourly for 5 days.
- Available Preparations: 125 mg/5 mL; 250 mg/5 mL.
Clindamycin
Clinical Profile and Dosage
- Indications: First choice in penicillin-allergic patients.
- Dose: 7.5 mg/kg up to 300 mg orally.
- Frequency: Taken 8 hourly for 5 days.
- Available Preparations: 150 mg capsules.

Management of Penicillin Allergy
 |  |
 |  |
Clinical Assessment7
- Clinical History: Evaluate the nature and severity of the reaction.
- Childhood Rash:
- Most often caused by viral infections or drug-virus interactions rather than a true allergy.
- Patients can be rechallenged under specialist guidance for definitive assessment.
- This prevents unnecessary use of alternative antibiotics (like Clindamycin) and supports antibiotic stewardship.
- Reaction Types: Can be immediate (IgE-mediated) or delayed (T-Cell mediated).
Cross-Reactivity Between Beta-Lactams8
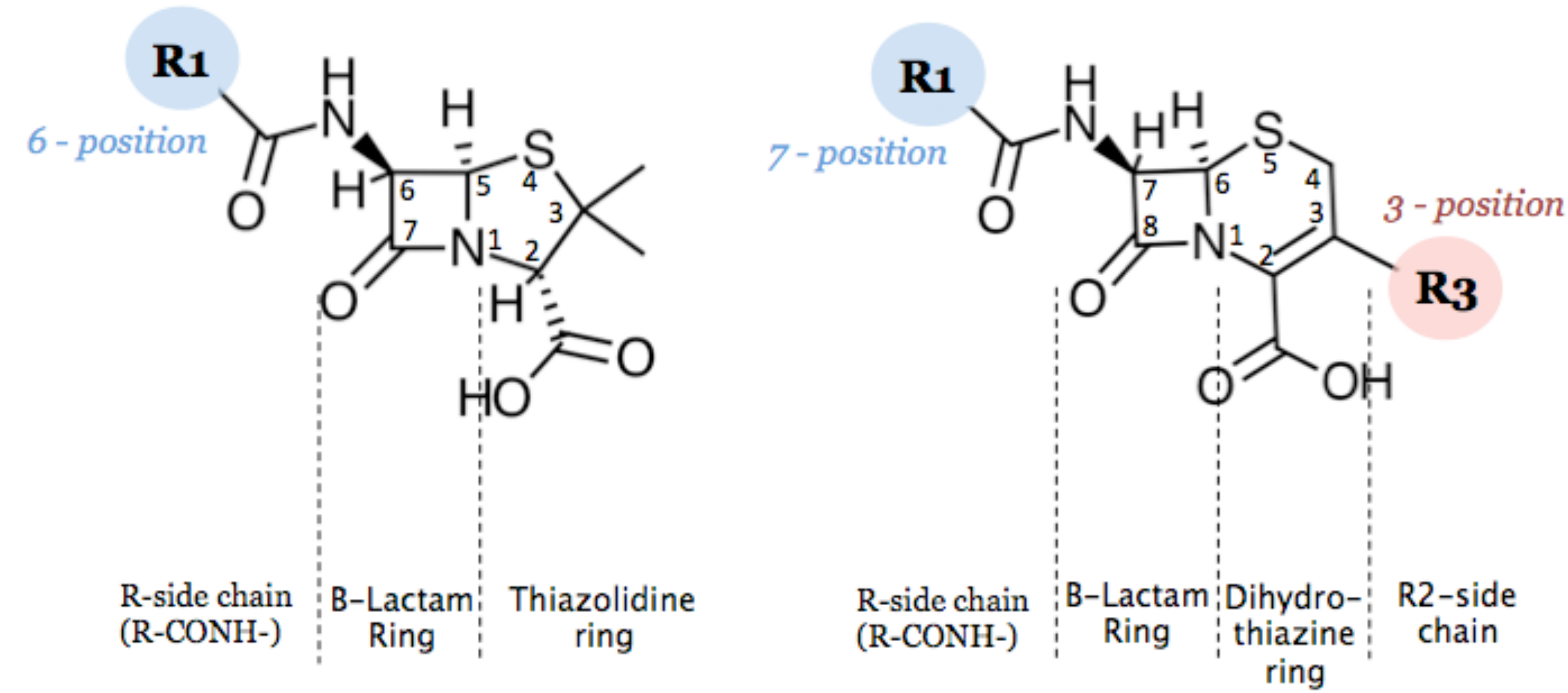
Cross-reactivity is determined by the structural components of the antibiotics:
- Penicillins: Consist of an R-side chain (R-CONH-), Beta-Lactam Ring, and Thiazolidine ring (R1 at 6-position).
- Cephalosporins: Consist of an R-side chain (R-CONH-), Beta-Lactam Ring, Dihydrothiazine ring, and R2-side chain (R1 at 7-position; R3 at 3-position
R1 Side Chain Significance
Current evidence suggests reactions often occur due to antigenic molecules on the R1 side chain. Drugs with similar or identical R1 side chains are more likely to cross-react. ).
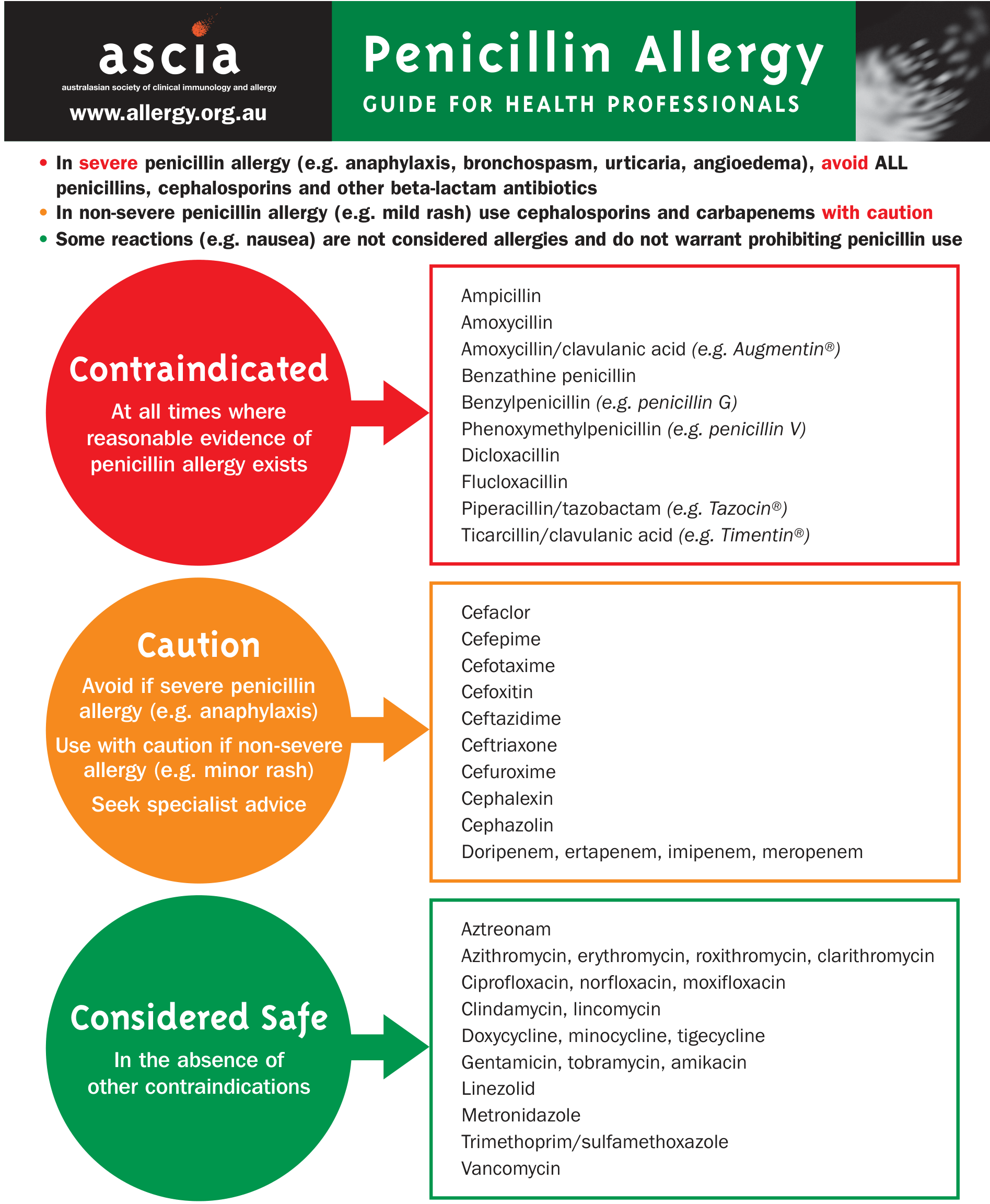
Management Guidelines9
- Severe Penicillin Allergy (e.g., anaphylaxis, bronchospasm, urticaria, angioedema): Avoid ALL penicillins, cephalosporins, and other beta-lactam antibiotics.
- Non-Severe Penicillin Allergy (e.g., mild rash): Use cephalosporins and carbapenems with caution.
- Non-Allergic Reactions: Symptoms like nausea are not considered allergies and do not prohibit penicillin use.
Documentation and Follow-up
- Record allergy alerts in the patient health record allergy section.
- Include drug name, reaction description, severity, date, and reporter’s name.
- Consult immunology for formal testing or desensitisation if indicated.
- Educate patients regarding true allergies vs. viral rashes to prevent long-term unnecessary avoidance of penicillins.
Metronidazole for Anaerobic Infections
 |  |
Clinical Profile and Dosage10
- Indications: Used as a supplement to penicillin or clindamycin for unresponsive or severe infections.
- Activity: Active against most anaerobic bacteria, including Peptoniphilus spp, P. gingivalis, and P. oralis.
- Dose: 10 mg/kg up to 400 mg orally.
- Frequency: Taken 12 hourly for 5 days.
- Available Preparations: 200 mg/5 mL.
Side Effects and Interactions11
- Side Effects: Nausea, vomiting, flushing, and headache.
- Alcohol Warning: Adults should avoid alcohol for at least 24 hours after completing the course.
- Drug Interactions: Interacts with several drugs, such as Warfarin.
Common Analgesics in Paediatric Dentistry12
This section covers the selection and administration of analgesics within the context of paediatric dental care.
Overview of Analgesic Options13
- Paracetamol (e.g., Panadol)
- Ibuprofen (e.g., Nurofen)
- Painstop (Historical/Review required)
- Aspirin (Historical/Review required)
First Line Analgesics
Paracetamol
Dosage and Administration14
- Dose: 15 mg/kg orally
- Frequency: 4 to 6 hourly
- Maximum Daily Dose: 4 g/day
- Concentration: 120 mg / 5 ml
Contraindications
- Impaired renal function
- Impaired hepatic function
Ibuprofen
Dosage and Administration
- Dose: 5-10 mg/kg orally
- Frequency: 6 to 8 hourly
- Maximum Daily Dose: 2400 mg/day
- Concentration: 100 mg / 5 ml
- Usage Note: Use the lowest effective dose for no more than 3 days without review.
Contraindications
- Hypersensitivity (e.g., asthma, rhinitis, urticaria)
- Renal or cardiac impairment
- Gastroenterological pathology
- Mechanism: NSAIDs inhibit cyclooxygenase enzymes, increasing bleeding risk and irritating gastric epithelium.
- Concurrent use of anticoagulants or corticosteroids
- Bleeding disorders: NSAIDs inhibit cyclooxygenase enzymes and platelet aggregation.
Clinical Considerations
Reference: Kent, A.P. et al. J Am Coll Cardiol. 2018;72(3):255-67.

Contraindicated Analgesics in Children
Historical Formulations (FOR HISTORICAL REFERENCE ONLY)15
Codeine and Combination Products
- Painstop (Paracetamol + Codeine):
- Composition: Paracetamol 120 mg/5 mL + Codeine Phosphate 5 mg/5 mL
- Historical dosage for acute pain: 0.8 ml/kg every 6 hours
- Painstop Night:
- Composition: Paracetamol 120 mg/5 mL + Codeine Phosphate 5 mg/5 mL + Promethazine Hydrochloride 6.5 mg/5 mL + Ethanol 0.5 mL/5 mL
- Historical dosage for acute pain and sedation: 0.5 ml/kg every 6 hours
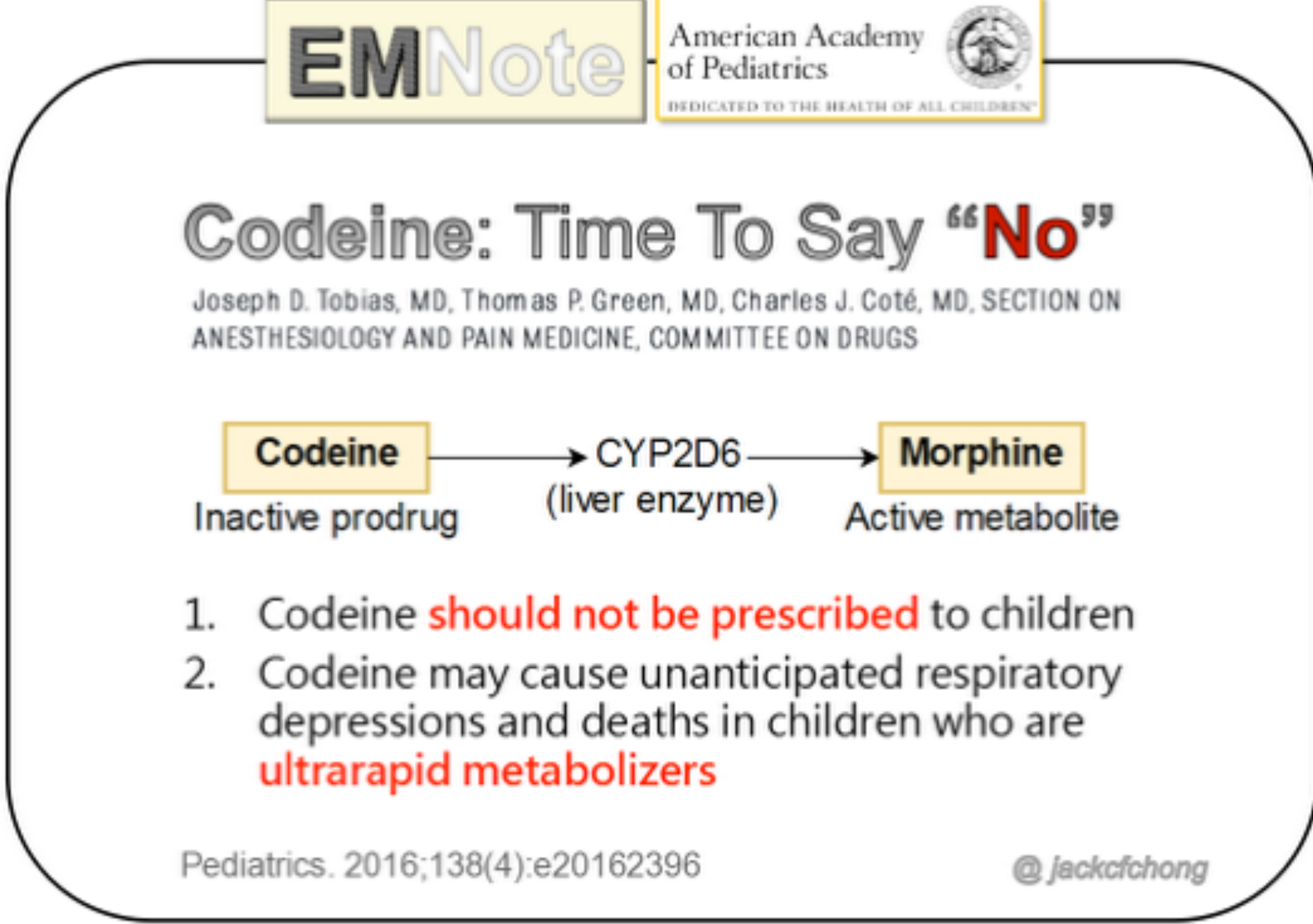
Safety Warnings and Metabolism
According to the American Academy of Pediatrics (Section on Anesthesiology and Pain Medicine):
- Metabolic Pathway: Codeine is an inactive prodrug converted by the liver enzyme CYP2D6 into its active metabolite, Morphine.
- Key Recommendations:
- Codeine should not be prescribed to children.
- Codeine may cause unanticipated respiratory depression and death in children who are ultra-rapid metabolizers.
- High Risk Groups: Children with Obstructive Sleep Apnea (OSA) are at particular risk due to opioid sensitivities.
- Guidance: Contraindicated by the WHO, FDA, and Australian authorities.
Reference: Pediatrics. 2016;138(4):e20162396.
TGA Safety Review and Regulatory Changes
The Therapeutic Goods Administration (TGA) implemented the following recommendations regarding codeine use:
- Age Restrictions: Codeine products should no longer be used in children under 12 years of age.
- Post-Surgical Restrictions: Contraindicated in children aged 12-18 years who have recently undergone tonsillectomy or adenoidectomy.
- Other Contraindications: Should not be used by breastfeeding mothers or patients known to be ultra-rapid metabolizers.
- Rescheduling: As of 1 February 2018, all codeine-containing products were rescheduled from Schedule 2/3 to Schedule 4 (Prescription Only Medicine).
 |  |
 |  |
Aspirin and Reye Syndrome
Clinical Evidence and Restrictions
There is a documented causal link between aspirin use in children and the development of Reye Syndrome.
- Age Restriction: Aspirin use is banned in individuals under 16 years of age.
- Key Literature:
- Reye’s syndrome: the case for a causal link with aspirin. Glasgow JF. Drug Saf. 2002.
- Aspirin and Reye syndrome: a review of the evidence. Schrör K. BMJ. 2002.
- Aspirin use to be banned in under 16 year olds. Macdonald S. BMJ. 2002.
Clinical Etiology and Incidence
- Etiology: Historically linked to children with viral illnesses taking aspirin. The mechanism is not fully defined but may involve genetic predisposition or errors in metabolism.
- Incidence: Decreased over the last 20 years, potentially due to reduced aspirin administration.
Local Anaesthesia in Paediatric Dentistry16
 |  |
Pharmacology and Agent Selection
 |  |  |
 |  |  |
 |  |  |
 |
Foundational Knowledge17
- Assumed knowledge: mechanisms of action of LA, types of LA, indications/contraindications, duration of onset, etc.
- Specific mechanisms include sodium channel blockade, pKa considerations, and membrane movement.
- Distinguish between soft tissue vs. hard tissue anesthesia duration.
- Be aware of variations in toxicity and reactions between different agent types.
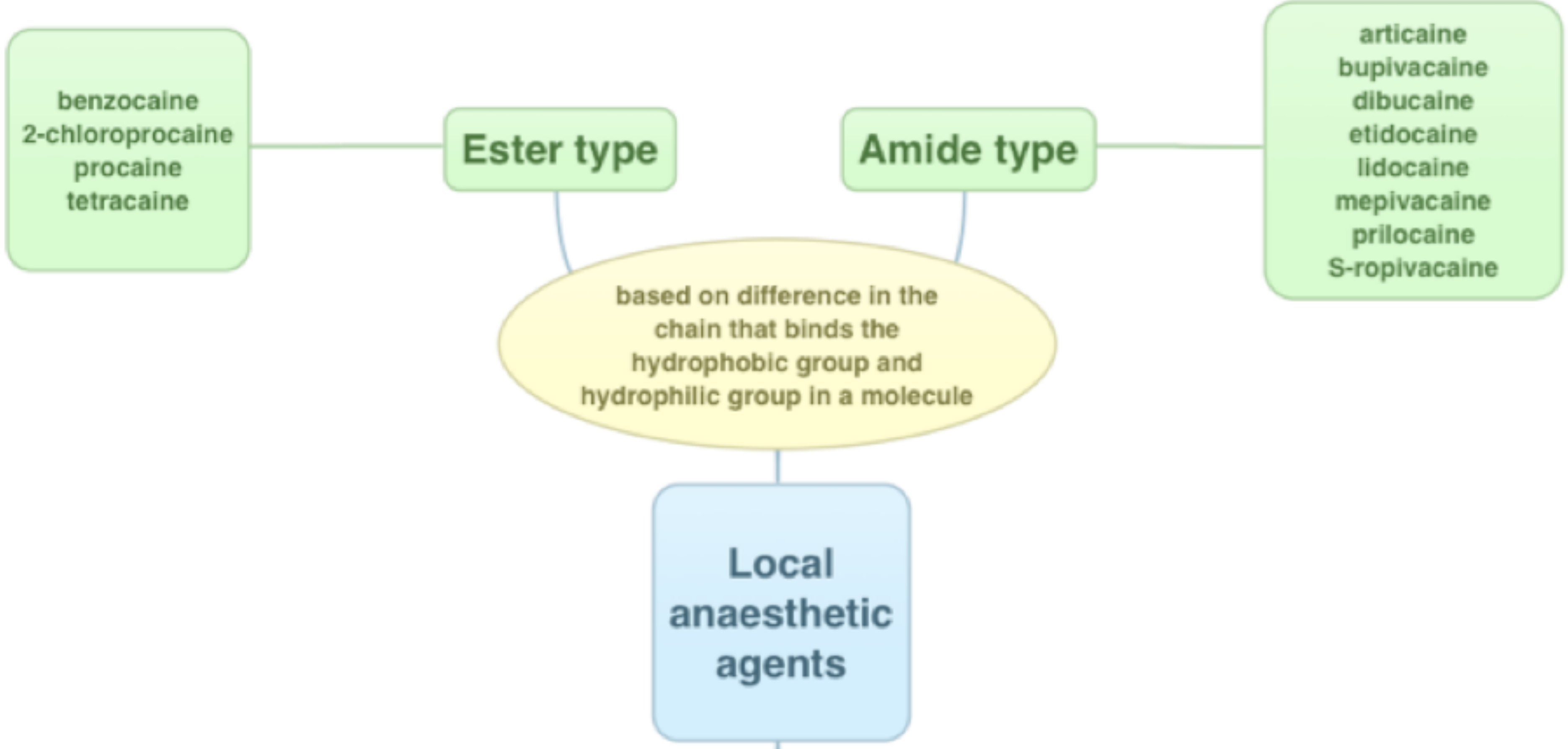
Classification of Local Anaesthetic Agents18
Local anaesthetic agents are categorized based on their mode of administration and pharmacological properties:
- Chemical Classification:
- Amides: Most common in dentistry (e.g., Lignocaine, Articaine, Prilocaine).
- Esters: Primarily found in topical formulations.
-
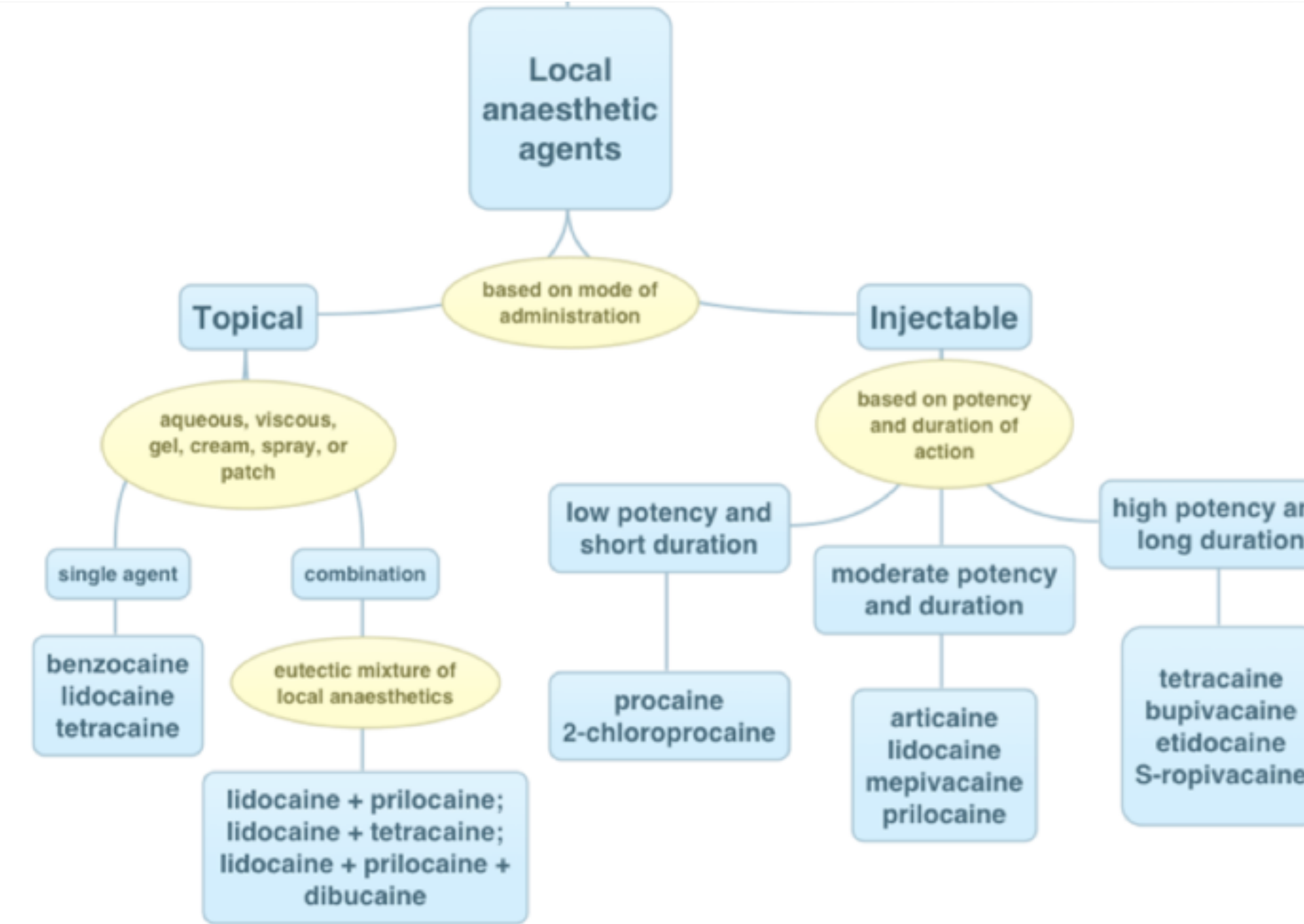
Topical Administration
- Based on formulation/composition: aqueous, viscous, gel, cream, spray, or patch.
- Clinicians must verify specific product concentrations (e.g., 5% Xylocaine adhesive vs. 10% ointment).
- Single Agents: Benzocaine, Lidocaine, Tetracaine.
- Combinations (Eutectic mixtures):
- Lidocaine + prilocaine
- Lidocaine + tetracaine
- Lidocaine + prilocaine + dibucaine
-
Injectable Administration
- Based on potency and duration of action:
- Low potency / Short duration: Procaine, 2-chloroprocaine.
- Moderate potency / Duration: Articaine, Lidocaine, Mepivacaine, Prilocaine.
- High potency / Long duration: Tetracaine, Bupivacaine, Etidocaine, S-ropivacaine.
- Based on potency and duration of action:
Common Formulations and Maximum Dosages19
- 2% Lignocaine with 1:80,000 Adrenaline
- Max dose: 7mg/kg
- 4% Articaine with Adrenaline 1:100,000
- Max dose: 7mg/kg
- Adrenaline at 1:80,000 is more effective for hemostasis during surgery/extractions than 1:100,000.
- Max dose: 7mg/kg
- 0.5% Bupivacaine with 1:200,000 Adrenaline
- Max dose: 2mg/kg
- Duration: Provides ~6 hours pulpal and 9 to 12 hours soft tissue anesthesia.
- Caution: Generally not recommended for routine paediatric restorative dentistry due to prolonged numbness risking soft tissue injury.
- Max dose: 2mg/kg
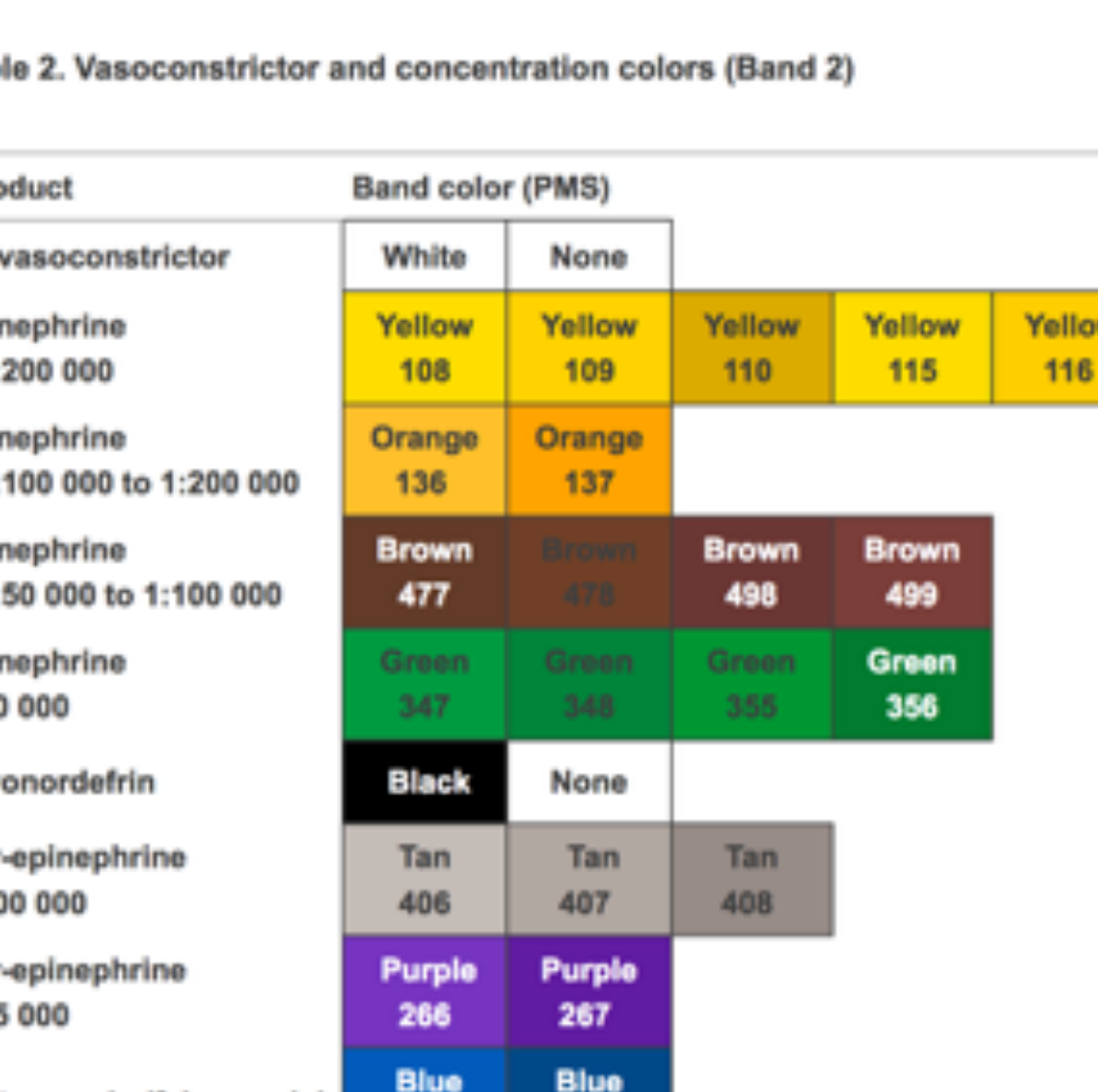
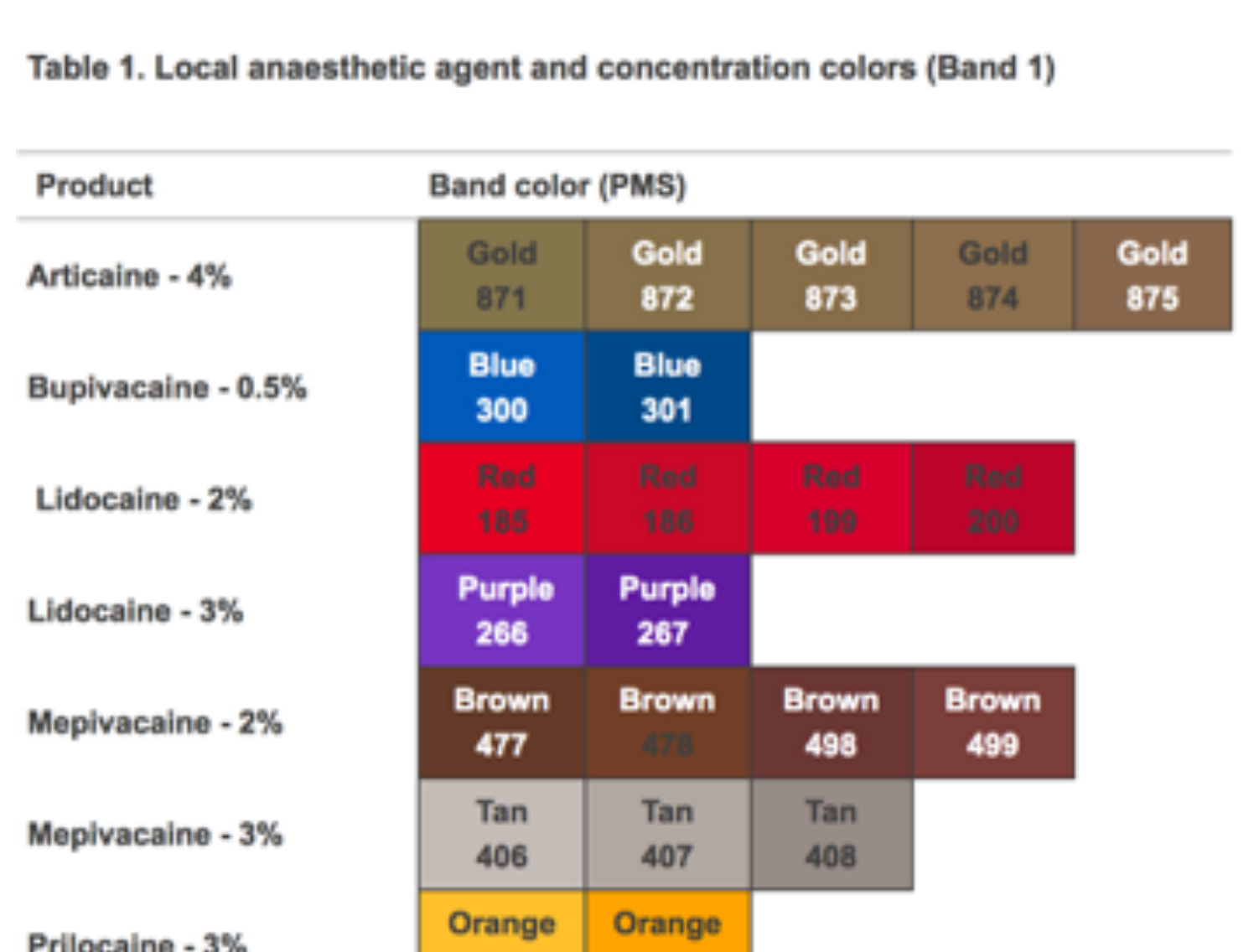
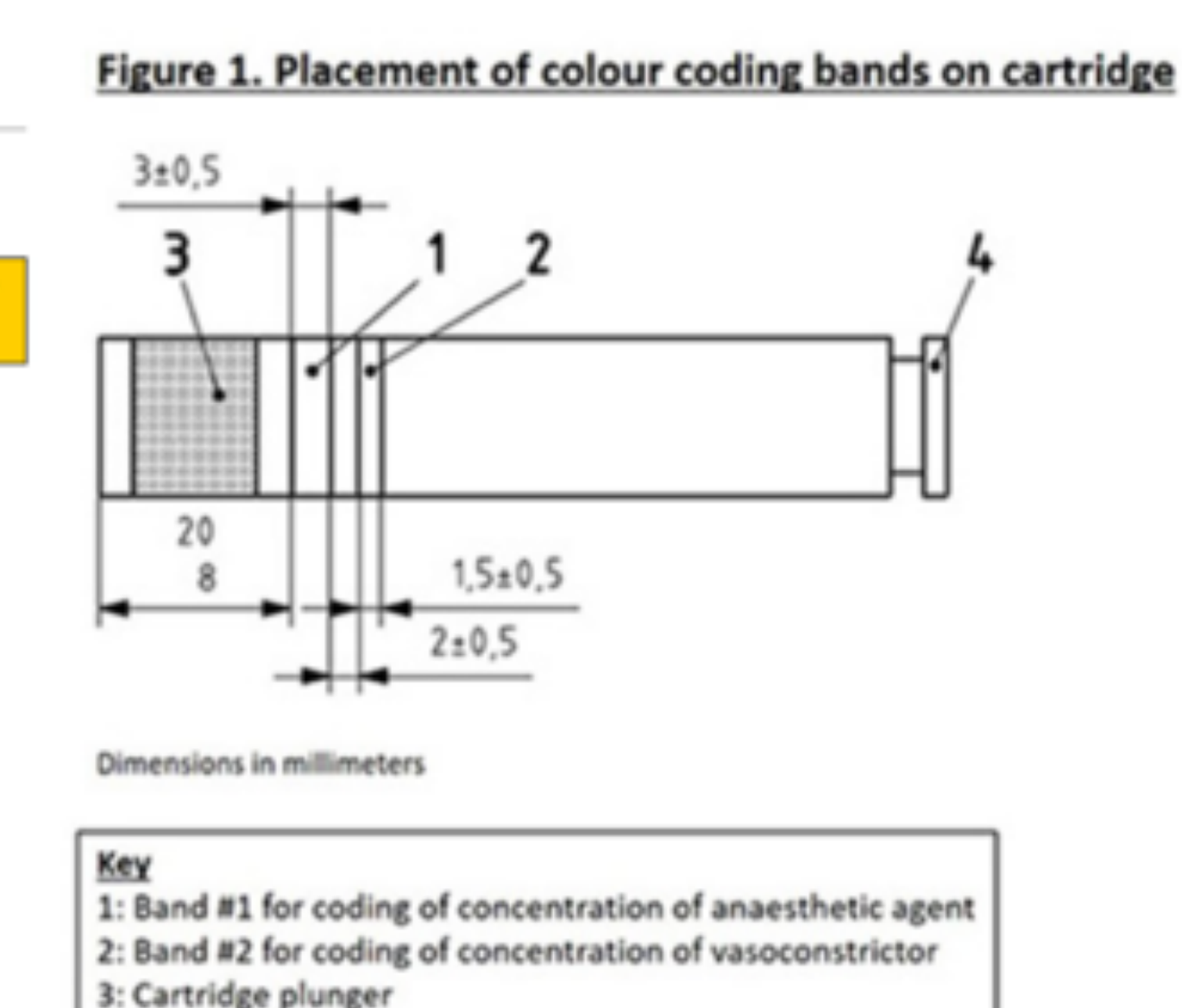
Regional Variations20
- Variations among countries/regions regarding available formulations and standards.
- Carpule Size: Australia uses 2.2 mL standard, while international regions often use 1.8 mL or 1.7 mL, which impacts dosage calculations.
R2 ISO standards for local anesthetic and regional variations
Dosage Calculation and Safety

Dosage Calculation: Option 121
Calculation based on solution percentage:
- A 1% solution contains 1g in 100mL, which equals 10mg/mL.
- 2% Lignocaine = 20mg/mL.
Content per Carpule (2% Lignocaine):
- 2.2mL carpule: 44mg
- 1.8mL carpule: 36mg
- 1.7mL carpule: 34mg
Clinical Example: 25kg Child22
Question: What is the maximum dose of 2% Lignocaine with adrenaline for a 25kg child?
- Calculate Maximum Dose in mg:
- 7mg/kg × 25kg = 175mg
- Convert to Volume (mL):
- 2% Lignocaine = 20mg/mL
- 175mg / 20mg/mL = 8.75mL
- Convert to Carpules:
- 8.75mL / 2.2mL per carpule ≈ 3.9 carpules
Dosage Calculation: Option 2 (Formula Method)23
To determine the maximum dose in milliliters (mL):
Example for 25kg child using 2% Lignocaine:
Clinical Documentation Standards
Essential Record Keeping24
Clinical documentation must be thorough and include:
- Type and Dosage: Specific local anaesthetic used and the total milligrams administered.
- Vasoconstrictors: Dosage and type (e.g., 44mg Lignocaine with 1:100,000 epinephrine).
- Injection Details: Type of technique used (e.g., infiltration, block, intra-osseous).
- Equipment and Response: Needle selection and the patient’s behavioral reaction (e.g., Behavior: +).
- Document if the reaction was positive throughout, or negative then positive with reinforcement/distraction to inform future treatment.
- Patient Weight: For patients where maximum dosage is a concern, weight must be documented preoperatively.
Injection Techniques
Overview of Techniques25
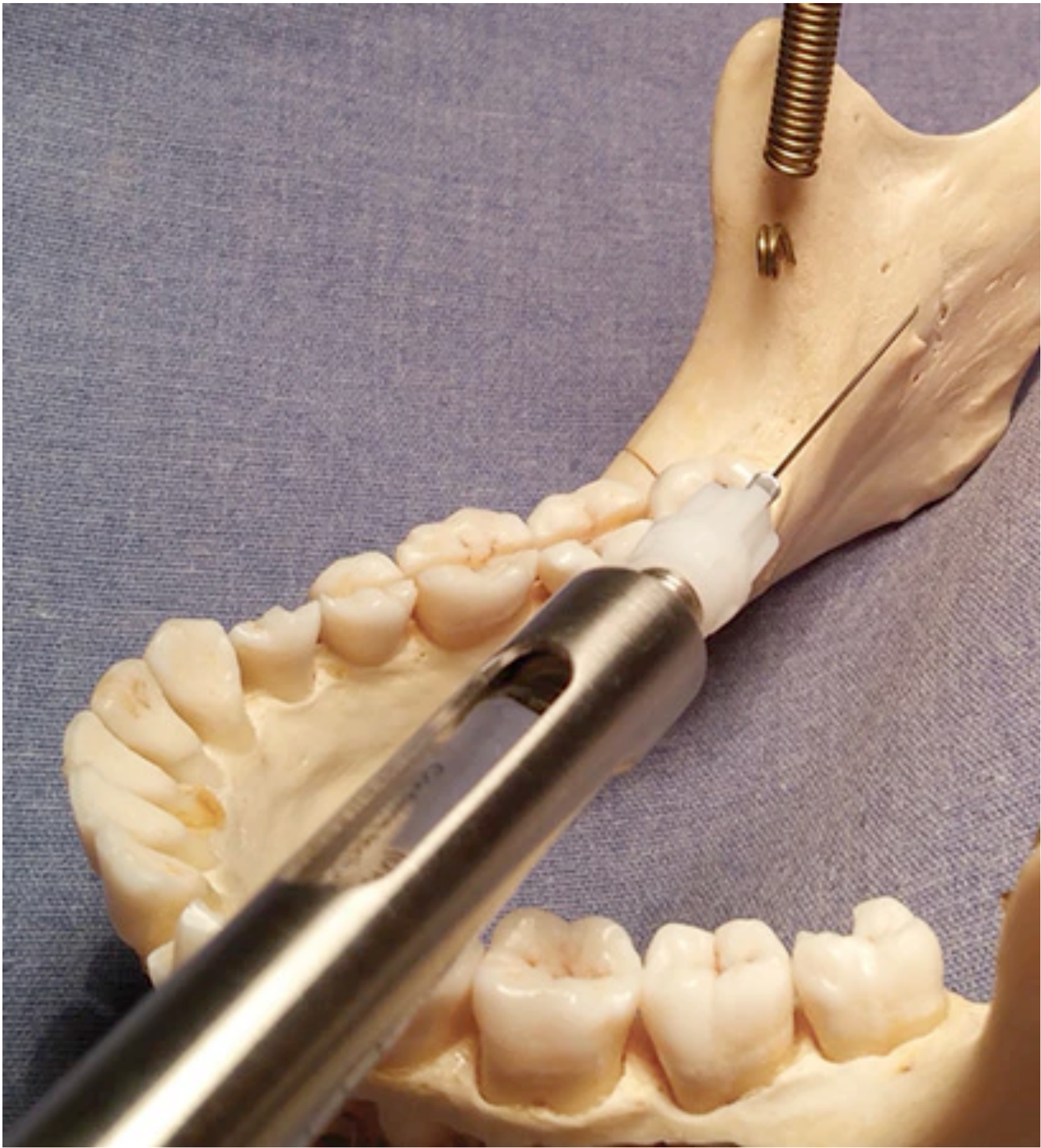
- Inferior Alveolar Nerve Block (IANB)
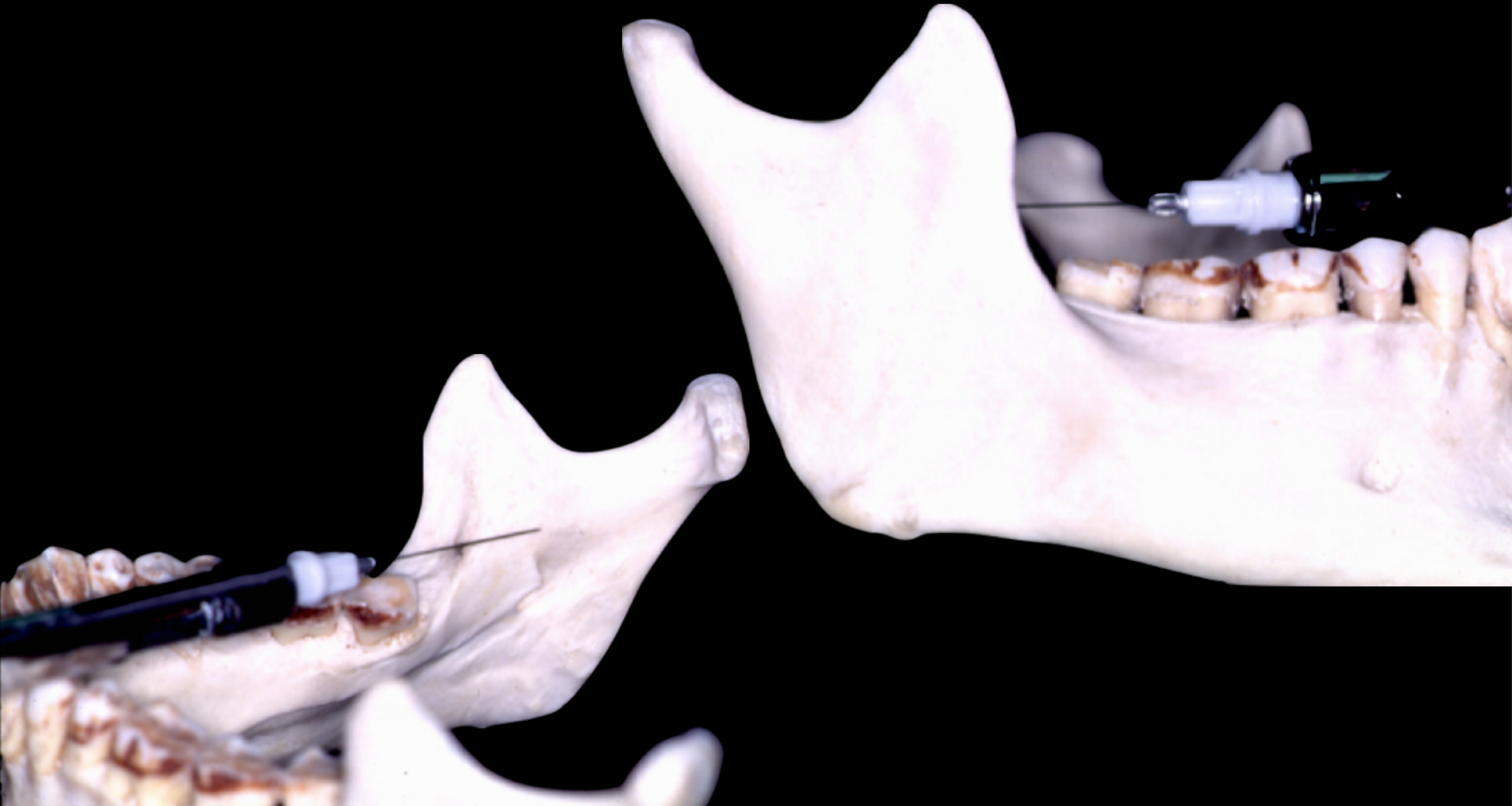
Inferior Alveolar Nerve Block
Success Rates
According to Malamed (2015), the IANB has the lowest success rate of all major nerve blocks in the human body.
Procedural Considerations
- Specific techniques for the Inferior Alveolar Nerve Block.
- Landmarks: Coronoid notch, pterygomandibular raphae, barrel overlying contralateral premolars, ~20mm to bony contact.
- Recommendation: Most routine paediatric restorative dentistry can be managed with Articaine infiltration rather than blocks.
Paediatric vs. Adult Anatomy
Key anatomical differences in children to consider for IANB:
- The ramus is shorter vertically.
- The ramus is narrower anterio-posteriorly.
- Needle selection: Consider using a short needle.
- Gauge: 27 to 30 gauge is typically used.
Clinical Best Practices
- Use precise technique.
- Practice aspiration technique.
- Use vasoconstrictors to improve efficacy and safety.
- Strictly adhere to maximum calculated doses.
- Staged Injection: Use half a carpule initially; re-inject only if the block is inadequate or missed.
- Provide comprehensive post-operative care instructions.
Case Study: Post-Operative Soft Tissue Injury
Patient: 8-year-old girl. Procedure: Extraction of lower left first permanent molar using 0.5% Bupivacaine (3 mLs). Complication: Massive 2-3 cm ulcer and swelling developed the next day. Initially misdiagnosed as an allergic reaction/angioedema. Cause: The child bit her numb lip for 4-5 hours. Bupivacaine’s 9-12 hour soft tissue anesthesia significantly increased this risk. Learning: Avoid long-acting agents in children and strictly reinforce post-op instructions. Nerve blocks are generally discouraged for routine cases due to this risk.
 |  |
 |  |
Toxicity and Physiological Considerations
Paediatric Physiological Factors26
Children have distinct physiological profiles that affect LA metabolism:
- High cardiac output and greater tissue perfusion.
- Higher basal metabolic rate.
- Immature liver enzymes: Detoxification of local anaesthetics is slower than in adults.
- Immature Central Nervous System (CNS) and Cardiovascular System (CVS): Increased susceptibility to toxicity at lower concentrations.
Manifestations of Systemic Toxicity27
High Doses of Local Anaesthetic:
- CNS: Depression, sleepiness.
- CVS: Decreased contractile force, decreased cardiac output.
- Pulmonary System: Respiratory arrest leading to death.
Accidental Intravenous (IV) Administration:
- Can cause analgesia, anxiety, restlessness, or symptoms mimicking General Anaesthesia (GA).
Delivery Systems and Camouflage2829
 |  |  |
 |  |  |
 |  |  |
 |
Computer-Regulated Delivery30
Modern delivery systems, such as the STA (Single Tooth Anaesthesia) system, include:
- Computer-regulated drive unit.
- Ergonomically designed handpiece.
- Foot control for regulated flow.
- Also known as "The WAND"; the needle tip can be hidden in the palm to reduce visual threat.
- Capable of PDL injections and senses tissue pressure to adjust flow rate.
Psychological Management31
- Delivery systems: Use of camouflage techniques to reduce patient anxiety.
- Needle-Free Injectors: Use high-pressure air but the "gunshot" sound can increase anxiety.
- Dental Vibe: Uses vibration (gate theory); however, evidence for pain reduction is conflicting.
- Camouflage Devices (e.g., alligator syringe): May have infection control issues and lack proper finger rests.
Thank You
Footnotes
-
Original PDF page 1: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.1 ↩
-
Original PDF page 2: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.2 ↩
-
Original PDF page 3: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.3 ↩
-
Original PDF page 4: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.4 ↩
-
Original PDF page 5: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.5 ↩
-
Original PDF page 6: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.6 ↩
-
Original PDF page 12: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.12 ↩
-
Original PDF page 13: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.13 ↩
-
Original PDF page 14: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.14 ↩
-
Original PDF page 9: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.9 ↩
-
Original PDF page 16: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.16 ↩
-
Original PDF page 17: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.17 ↩
-
Original PDF page 18: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.18 ↩
-
Original PDF page 7: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.7 ↩
-
Original PDF page 22: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.22 ↩
-
Original PDF page 26: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.26 ↩
-
Original PDF page 27: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.27 ↩
-
Original PDF page 28: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.28 ↩
-
Original PDF page 29: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.29 ↩
-
Original PDF page 30: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.30 ↩
-
Original PDF page 33: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.33 ↩
-
Original PDF page 34: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.34 ↩
-
Original PDF page 35: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.35 ↩
-
Original PDF page 36: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.36 ↩
-
Original PDF page 37: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.37 ↩
-
Original PDF page 41: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.41 ↩
-
Original PDF page 42: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.42 ↩
-
Original PDF page 44: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.44 ↩
-
Original PDF page 46: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.46 ↩
-
Original PDF page 43: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.43 ↩
-
Original PDF page 45: L6 -Antibiotics LA and Analgesics in Paediatric Dentistry, p.45 ↩