Orofacial Infections In Paediatric Dentistry
Course Information1
- Course Code: DENT 5312
- Module: Paediatric Dentistry Module
- Focus: Diagnosis and management of common orofacial infections, with a primary emphasis on viral conditions.
Presenter Details
- Dr Jilen Patel
- Specialist Paediatric Dentist
- Senior Lecturer, Clinical Dentistry
- UWA Dental School
Introduction and Recommended Resources
Required Reading2 readings
- Handbook of Pediatric Dentistry
- Authors: Cameron and Widmer (4th Edition)
- Access: Ebook available through UWA Onesearch
- Chapter 10 is considered a "must-read" resource as it provides concise snippets of conditions with extensive clinical imagery.
Specific Study Areas
- Chapter 10: Paediatric oral medicine, oral pathology and radiology
Learning Objectives
- Understanding the scope of practice regarding pharmacological management.
- Knowledge of drug dosages based on pediatric age and weight.
- Triaging: Determining if a case requires immediate Emergency Department (ED) referral or specialist consultation.
Diagnostic Framework
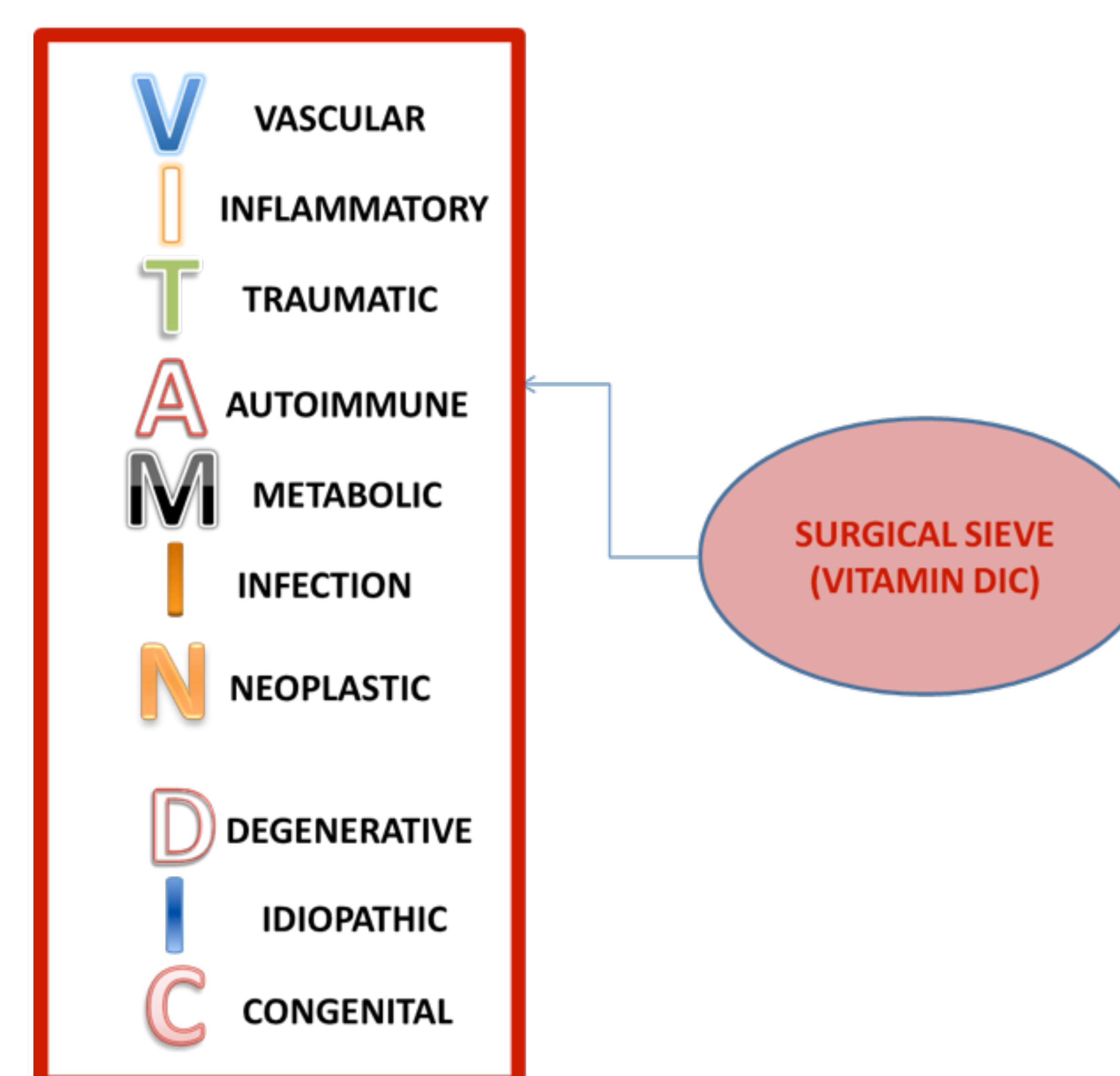
The Diagnostic Sieve (VITAMIND IC)3
The diagnostic sieve is a structured framework used to categorize potential causes of a clinical presentation.
| Letter | Category |
|---|---|
| V | VASCULAR |
| I | INFLAMMATORY |
| T | TRAUMATIC |
| A | AUTOIMMUNE |
| M | METABOLIC |
| I | INFECTION |
| N | NEOPLASTIC |
| D | DEGENERATIVE |
| I | IDIOPATHIC |
| C | CONGENITAL |
- ==Vascular: Red/purple hue, blanches under pressure (e.g., venous malformations).==
- ==Inflammatory: Cardinal signs of inflammation (e.g., gingivitis).==
- ==Traumatic: Requires history of injury (e.g., cheek biting post-local anesthetic).==
- ==Autoimmune: Oral manifestations of systemic disease (e.g., Sjogren’s syndrome, Lupus).==
- ==Metabolic: (e.g., Diabetes-related oral changes).==
- ==Neoplastic: Assessing changes in size, shape, and displacement of structures (e.g., Squamous cell carcinoma).==
- ==Degenerative: Rare in children (e.g., TMJ osteoarthritis).==
- ==Idiopathic: Unknown etiology (e.g., idiopathic root resorption).== - ==Congenital: Present from birth (e.g., Port-wine stain/Sturge-Weber syndrome).==
Differential Diagnosis of Orofacial Infections4
Orofacial infections in paediatric dentistry are generally categorized into three primary types:
- Bacterial
- Viral
- Fungal
Bacterial Infections
- Odontogenic Infections
- Dental caries
- Periodontal disease
- Systemic and Localized Bacterial Infections
- Scarlet fever
- Tuberculosis
- Atypical mycobacterial infection
- Actinomycosis
- Syphilis
- Impetigo
- Osteomyelitis
Fungal Infections5
- Candidosis
Bacterial and Viral Differential List6
- Bacterial
- Odontogenic (dental caries, periodontal disease)
- Scarlet fever
- Tuberculosis
- Atypical mycobacterial infection
- Actinomycosis
- Syphilis
- Impetigo
- Osteomyelitis
Management of Bacterial Infections
First-line treatment for localized infection is source removal (extraction/pulpotomy). Antibiotics are reserved for systemic involvement.
- Viral
- Primary herpetic gingiva-stomatitis
- Herpes labialis
- Herpangina
- Hand, foot and mouth disease
- Infectious mononucleosis
- Varicella
Fungal
- Candidosis
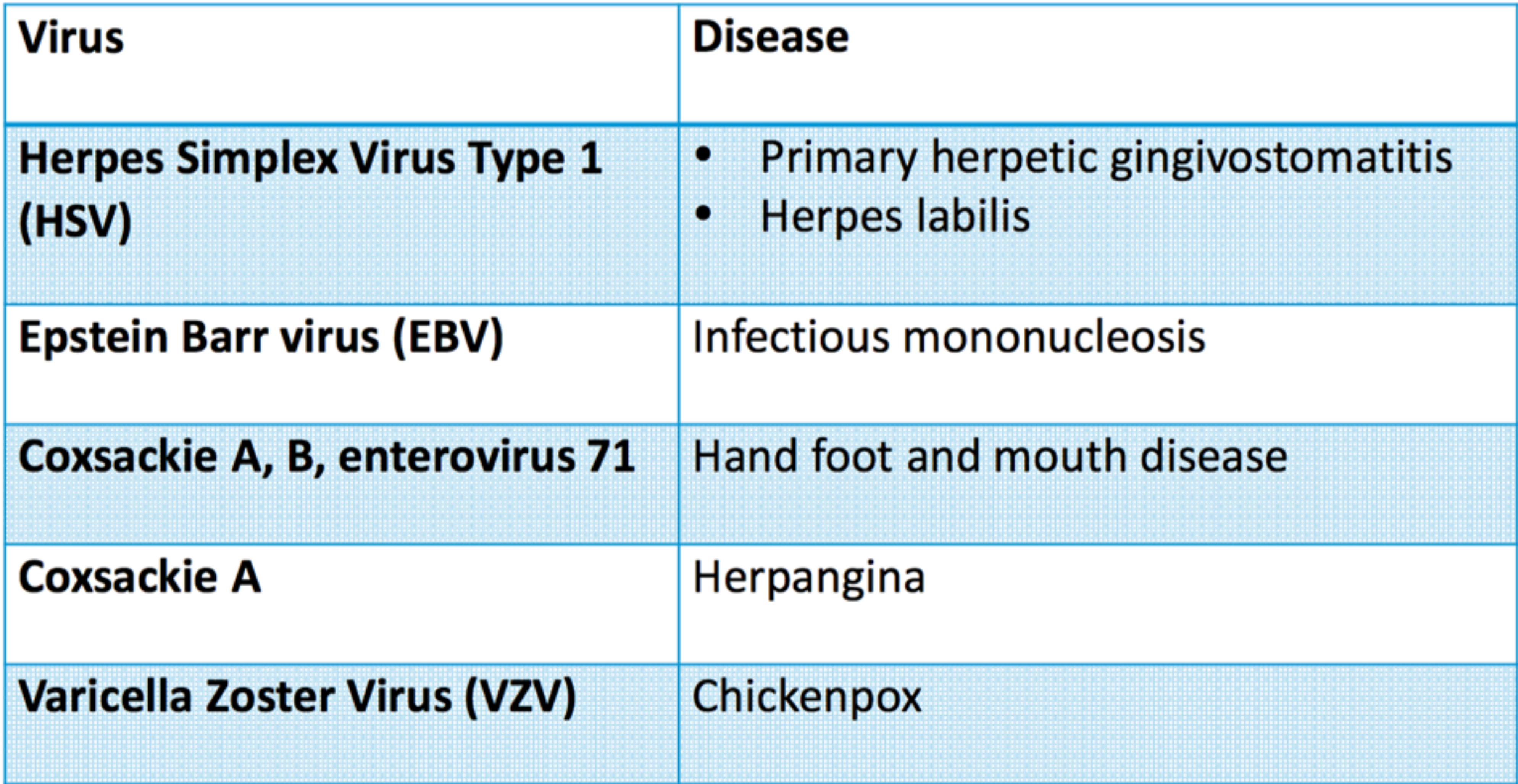
Viral Infections Overview78
| Virus | Disease |
|---|---|
| Herpes Simplex Virus Type 1 (HSV) | • Primary herpetic gingivostomatitis • Herpes labialis |
| Epstein Barr virus (EBV) | Infectious mononucleosis |
| Coxsackie A, B, enterovirus 71 | Hand foot and mouth disease |
| Coxsackie A | Herpangina |
| Varicella Zoster Virus (VZV) | Chickenpox |
Visual clinical markers of viral orofacial infections often include redness, blisters, and ulcerations on the lips and tongue, characteristic of the Herpes Simplex Virus family.
Viral Diagnosis
Ulceration is the most common manifestation of herpes simplex . Diagnosis relies on background history, systemic signs, and the specific location/pattern of oral ulcers.
 |  |  |
 |  |
Primary Herpetic Gingivostomatitis
Etiology and Epidemiology
Viral Agents9
- Herpes simplex type 1 virus
- Herpes simplex type 2 virus (occasional cases related to genital herpes or sexual abuse)
Demographics
- Age: Primary infection usually occurs after 6 months of age, with peak incidence between 12 and 18 months.
- Approximately 60% of the population is infected with the virus, though only about 1% of those infected will manifest acute primary symptoms.
- The peak incidence around 6 months of age often coincides with the eruption of the lower incisors.
- Gender: No gender predilection.
Clinical Presentation10
 |  |
 |  |
General Systemic Features11
- Febrile illness (37.8-38.9 °C / 100-102 °F)
- Headaches, malaise, and irritability
- Cervical lymphadenopathy
- Difficulty eating and drinking due to pain, which presents a significant risk of dehydration.
Oral Manifestations
- Oral pain and mild dysphagia
- Stomatitis
- Vesicles: Characteristic intraepithelial fluid-filled vesicles appearing on the tongue, lips, buccal, and palatal mucosa.
- Ulcerations:
- Solitary ulcers: Small (3 mm), painful, with erythematous margins.
- Larger ulcers: Irregular margins resulting from the coalescence of individual lesions. - Ulcers are typically well-demarcated, featuring a characteristic red halo and a yellow or grey central slough.
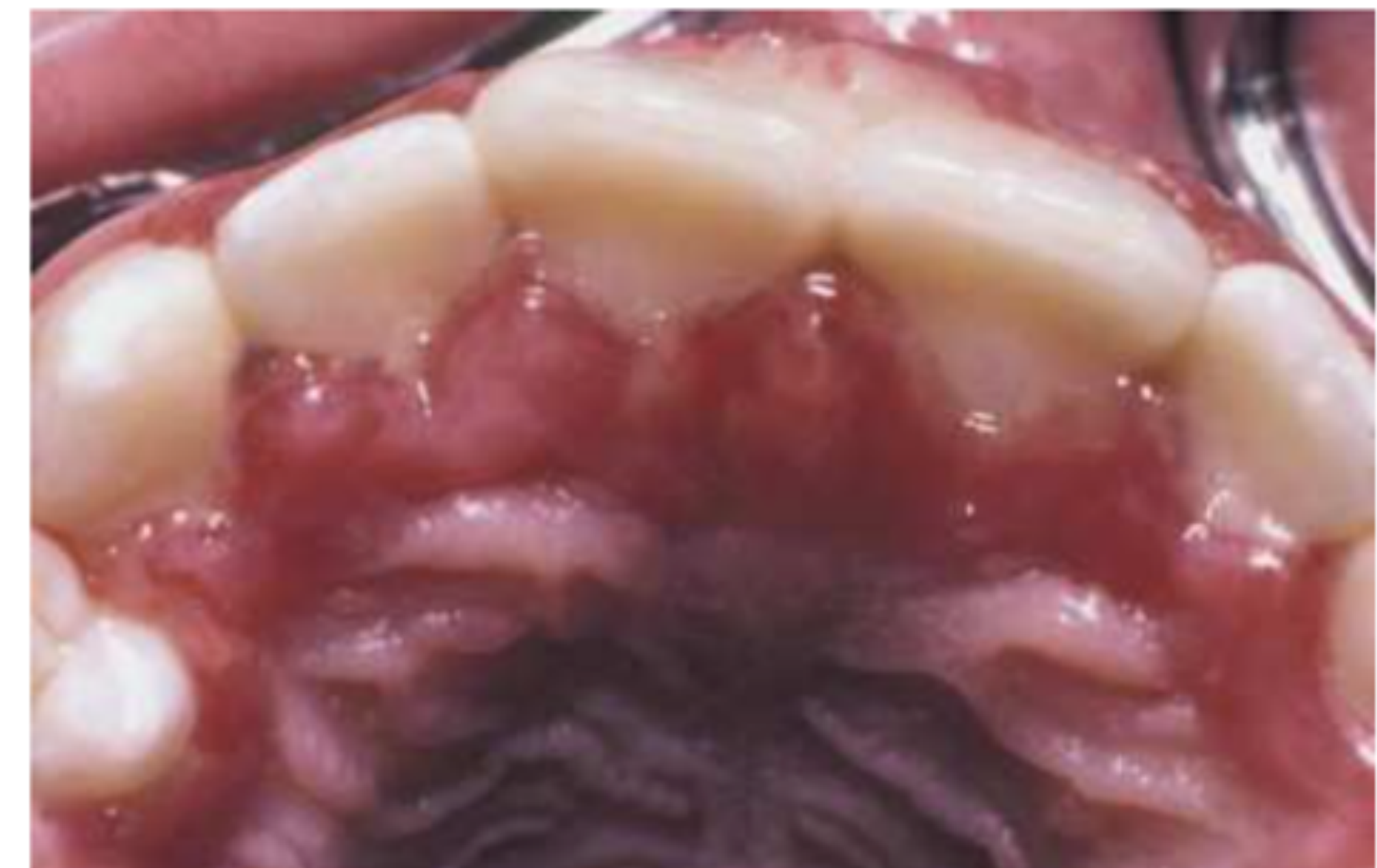
Clinical presentation of Primary Herpetic Gingivostomatitis typically involves widespread oral lesions and significant gingival inflammation.
Gingival Involvement12
- Painful, enlarged, and erythematous palatal gingiva.
- Painful, enlarged, and erythematous facial gingiva.
- Notable erosions of the free gingival margin.
- Gingiva appears diffuse, erythematous, and shiny.
- Significant edema and friable tissues often lead to spontaneous bleeding.
 |  |
Transmission and Disease Course
Incubation and Transmission13
- Incubation Time: 3–5 days, often preceded by a 48-hour prodromal history of irritability, pyrexia, and malaise.
- Transmission:
- Direct contact with active lesions.
- Contact with infected oral secretions (droplet infection).
Prevention of Autoinoculation
Children should be closely monitored and discouraged from touching their mouths and subsequently touching their eyes to prevent the spread of the infection (herpetic keratoconjunctivitis).
Disease Course
- The disease is self-limiting.
- Ulcers typically heal spontaneously without scarring within 10–14 days.
- Following the primary infection, the virus travels to the neuronal ganglia (typically the trigeminal ganglion) where it remains in a latent state.
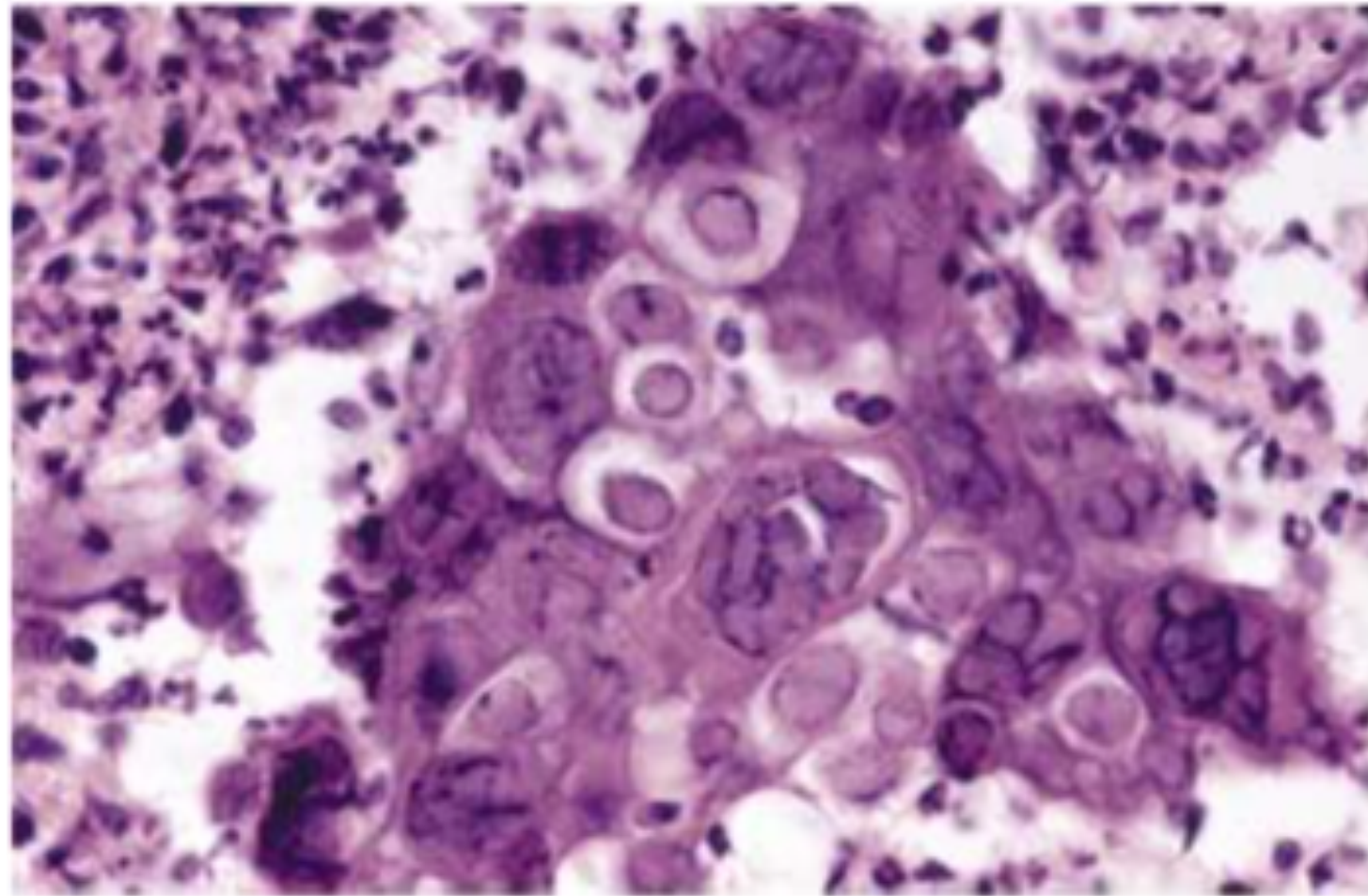
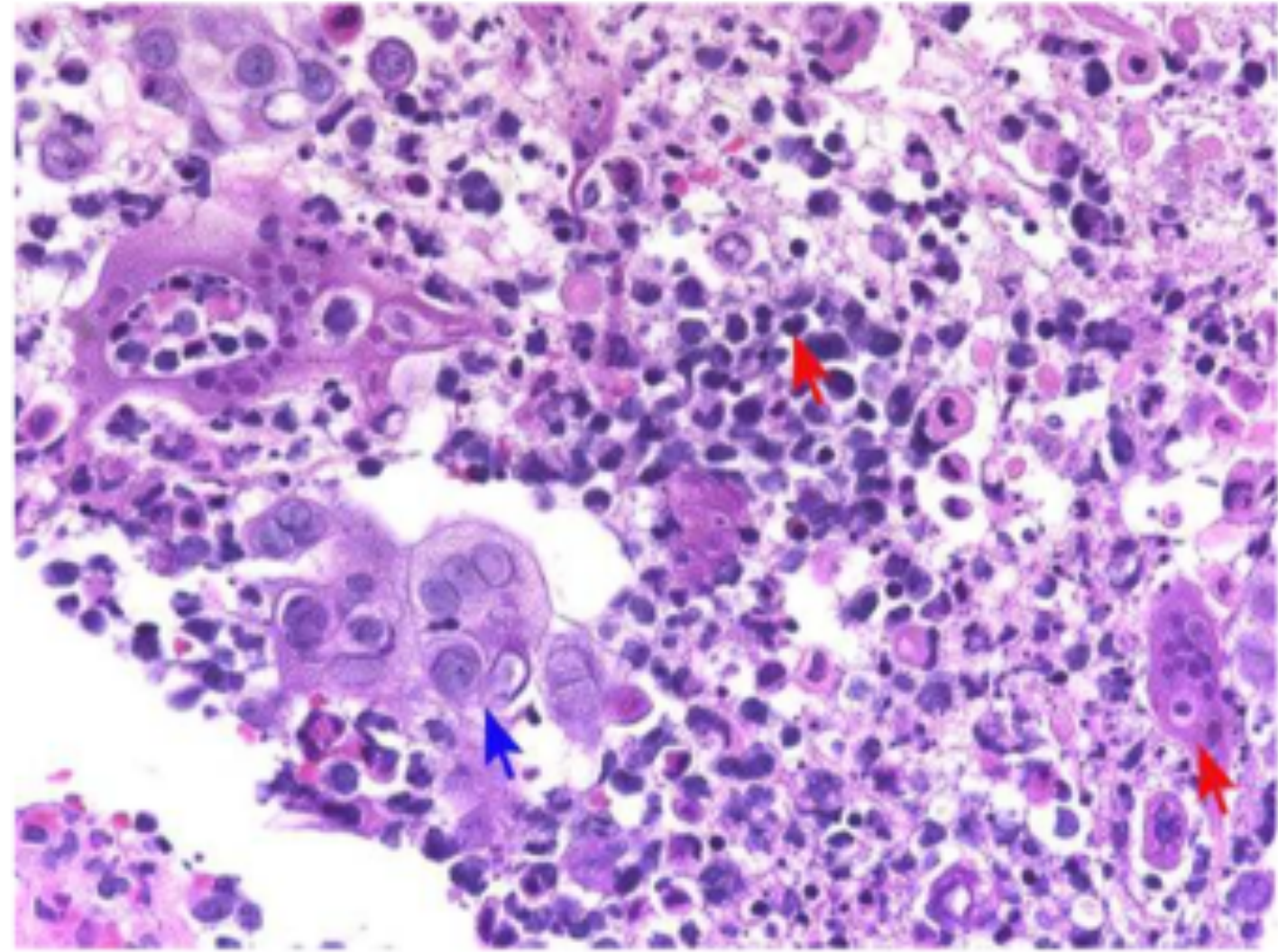
Histology and Diagnosis
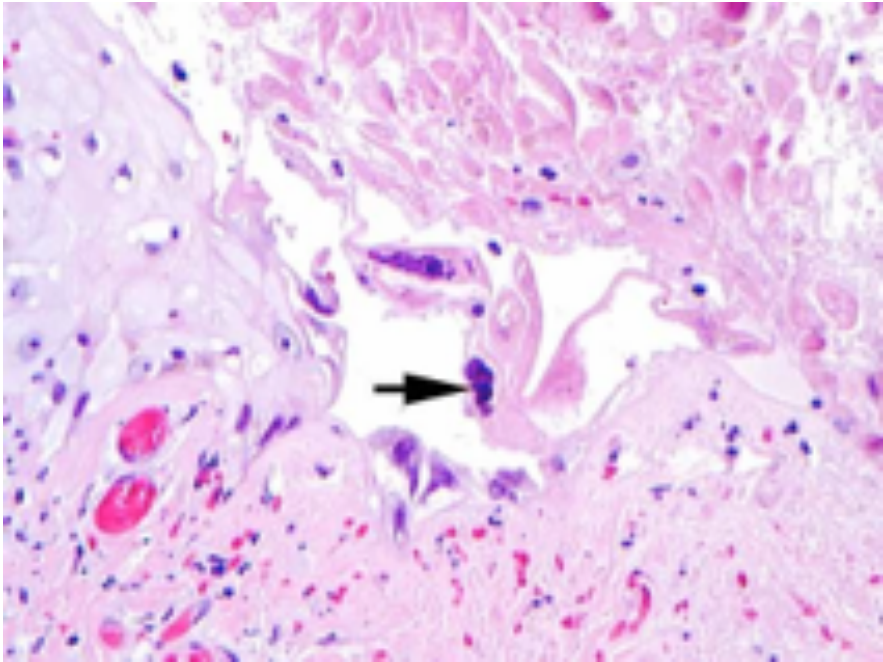
Histopathological Features14
- Tzanck Cells: Multinucleated giant cells with a “jig-saw” nucleus.
- Viral Inclusion Bodies: Present within affected tissues.
 |  |
Diagnostic Methods
- Clinical Assessment: Based on history, clinical features, and the age group of the child.
- Exfoliative Cytology: Rapid diagnosis via identification of multinucleated giant cells.
- Laboratory Testing:
- Viral antigen testing
- Viral culture
- Viral antibody detection in blood samples - Diagnosis can be confirmed via a viral swab of the lesions if the clinical presentation is unclear.
Differential Diagnosis and Complications
Differential Diagnosis15
- Necrotizing ulcerative gingivitis
- Erythema multiforme
- Herpangina

Complications16
While rare, severe complications can include:
- Aseptic meningitis
- Encephalitis
 |  |
 |
Management and Pharmacotherapy
Symptomatic Care17
- Encourage high fluid intake.
- Recommend bed rest and a soft diet.
Analgesics and Pain Control
- Paracetamol: 15 mg/kg, every 4-6 hours.
- Topical Therapy Precautions:
- 2% viscous lidocaine is not recommended due to systemic overdose risks and the child’s inability to spit.
- Topical benzocaine gel should be avoided in children under 6 years old to prevent methaemoglobinaemia.
Mouthwashes18
-
Young Children (Severe Ulceration): 0.2% chlorhexidine may be swabbed over affected areas using cotton wool.
-
Older Children: Chlorhexidine gluconate 0.2%, 10 mL every 4 hours.
-
Children Over 12 Years: Tetracycline or minocycline mouthwashes may be beneficial.
-
Combination Therapy: Benzadamine hydrochloride 0.15% & chlorhexidine 0.12% (Difflam C™) may offer advantages over chlorhexidine alone.
Antiviral Chemotherapy19
- Aciclovir: Approved for use in children for managing primary herpetic gingivostomatitis.
- Timing: Administration within the first 72–96 hours of infection provides the most benefit.
- Aciclovir is most effective when administered during the prodromal phase; its efficacy during the eruptive phase is currently a subject of clinical debate.
- Dosage:
- Oral (PO): 20 mg/kg body weight, 5 times daily (or TDS depending on clinical guidance).
- Intravenous (IV): 10 mg/kg body weight.
- Note: Evidence for oral use in children under two years of age is limited.
Herpes Labialis
Etiology and Triggers
Etiology and Site20
- Agent: Herpes simplex type 1 virus
- Recurrent/secondary activation of latent HSV
- Occurs at the mucocutaneous junction of the lip.
- Common Names: Cold sore, fever blister.
- Site: Vermilion border and adjacent skin of the lips.
 |  |
Triggering Factors
- Ultraviolet (UV) light
- Physical trauma
- Stress
- Fever
- Seasonal changes
Clinical Signs and Symptoms
Prodromal Phase21
- Symptoms are most severe in the first 8 hours.
- Sensations: Pain, burning, itching, tingling, and localized warmth.
- Erythema appears 6–24 hours before lesions develop.
Lesion Development
- Multiple small, erythematous papules develop.
- These form clusters of fluid-filled vesicles.
- Vesicles typically rupture and crust within 2 days.
Course of Disease
- Self-limiting; healing usually occurs within 7 to 10 days.
Clinical Progression Summary22
- Initial 8 Hours: Peak prodromal symptoms (tingling, itching).
- 6–24 Hours: Erythema of the involved epithelium.
- Vesicular Stage: Formation of fluid-filled clusters.
- Crusting Stage: Rupture and crusting within 48 hours.
- Resolution: Spontaneous healing in 7–10 days.
Infectious Mononucleosis
Etiology and Transmission
Etiology23
- Agent: Epstein-Barr virus (EBV or HHV-4).
- Terminology: Mono, Glandular Fever, Kissing Disease.
Transmission
- Occurs via intimate contact, primarily through blood or saliva.
- Children: Often infected via contaminated saliva on fingers, toys, or objects.
- Adults: Direct salivary transfer (e.g., shared straws, kissing).
- Persistence: Once exposed, EBV remains in the host for life.
Demographics
- Common in children aged 1 to 5 (often asymptomatic).
- No specific gender predilection noted.
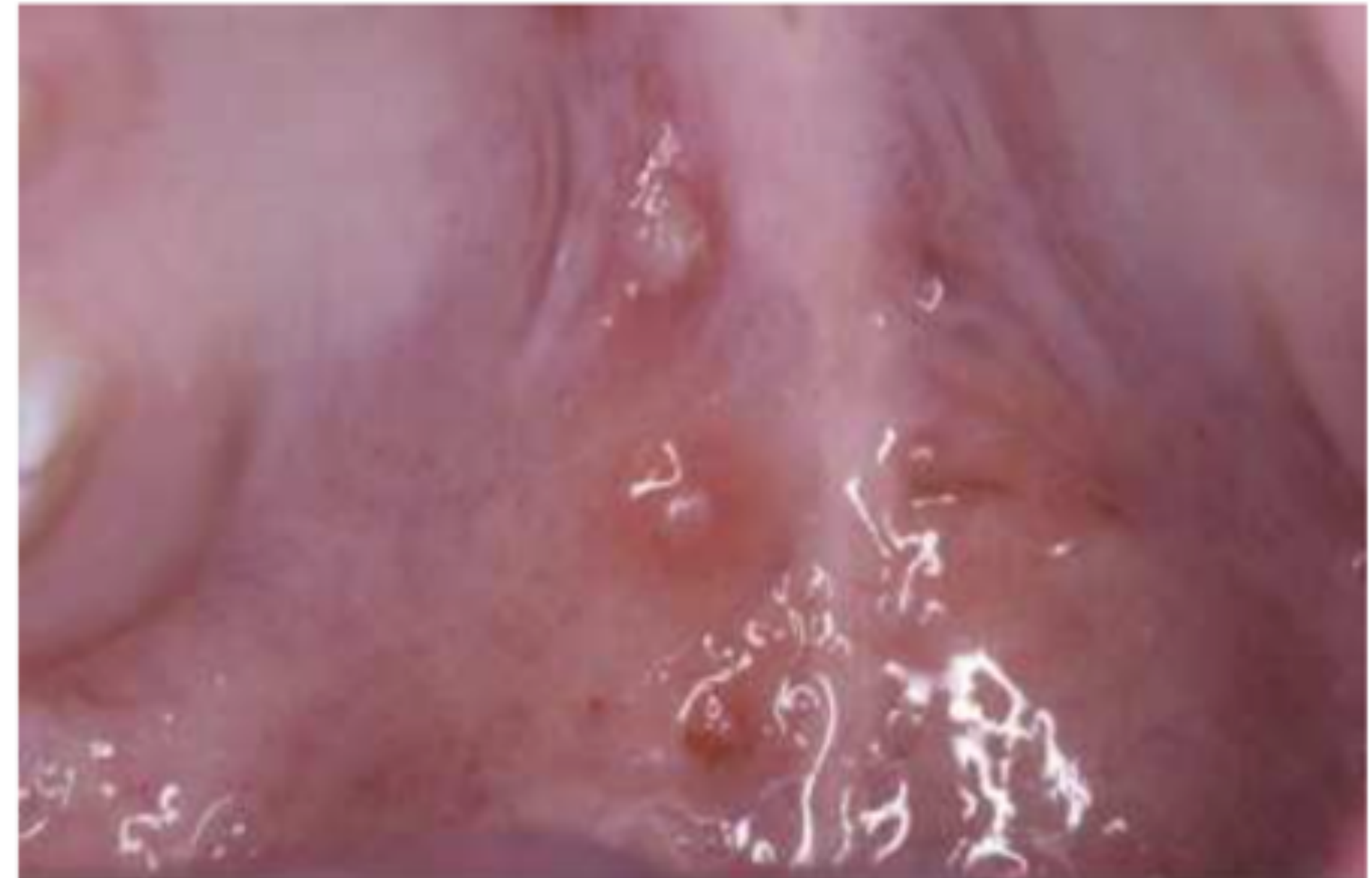
Clinical Presentation and Oral Lesions24
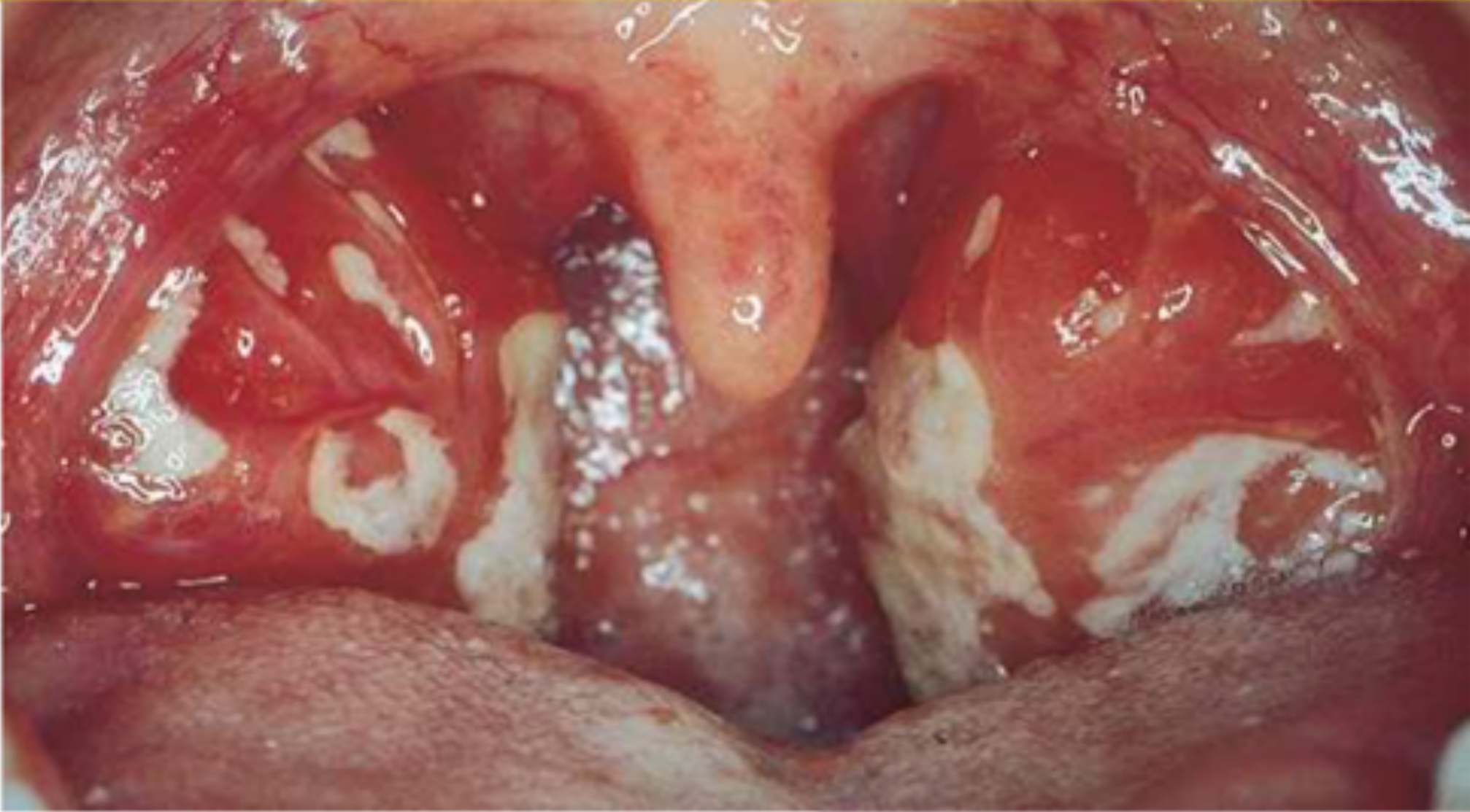 |  Hyperplastic Pharyngeal tonsils with yellowish crypt exudates Hyperplastic Pharyngeal tonsils with yellowish crypt exudates |
 Numerous Petechiae of the soft palate Numerous Petechiae of the soft palate |
Systemic Symptoms25
- Low-grade fever
- Hepatosplenomegaly
- Rhinitis or cough
- Malaise and headache
- Cervical lymphadenopathy and tenderness
- Posterior cervical chain involvement is particularly characteristic
Oral Lesions
- Oral ulcers
- Palatal petechiae
- Pinpoint hemorrhages typically located on the soft palate
- Gingival ulcerations (Necrotizing Ulcerative Gingivitis)
- Tonsillitis with or without pharyngitis
Disease Course
- Self-limiting; typically resolves within one to two weeks. Young adults are at the highest risk for symptomatic disease.
Histopathology and Differential Diagnosis
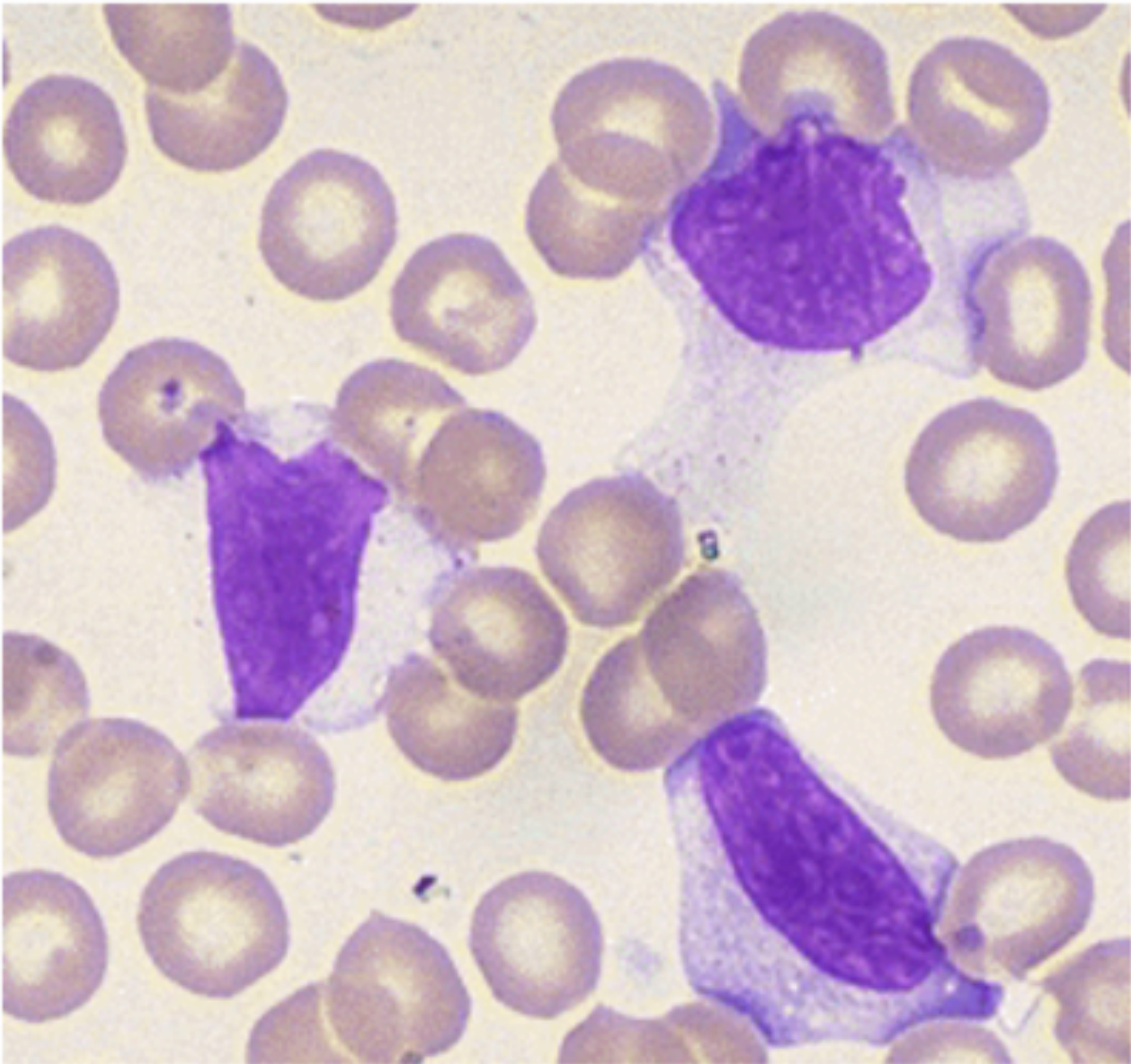
Histopathology26
- Downey Cells: Atypical lymphocytes; considered a diagnostic feature.
Differential Diagnosis
- Trauma
- Reactive gingival lesions
- Hematologic Disorders:
- Thrombocytopenia
- Platelet disorders
- Hereditary hemorrhagic telangiectasia
Diagnosis and Treatment
Diagnostic Criteria27
- Clinical history and presentation.
- Identification of atypical lymphocytes on a blood film.
- Heterophile Antibody Tests:
- Monospot test
- Paul–Bunnell agglutination test
- Advanced Testing:
- Indirect immunofluorescent assays
- Real-time PCR
Treatment Protocol28
- Most cases resolve spontaneously within 4 to 6 weeks.
- Supportive Care:
- Bed rest
- Maintenance of fluid intake and adequate nutrition
- Analgesia and antipyretics
Complications of EBV
Significant Complications29
- Splenic rupture
- Thrombocytopenia
- Autoimmune hemolytic anemia
- Aplastic anemia
- Neurologic problems
- Myocarditis
- Hemophagocytic lymphohistiocytosis
- Chronic fatigue (lasting weeks to months in <10% of cases)
- Increased risk for developing multiple sclerosis later in life
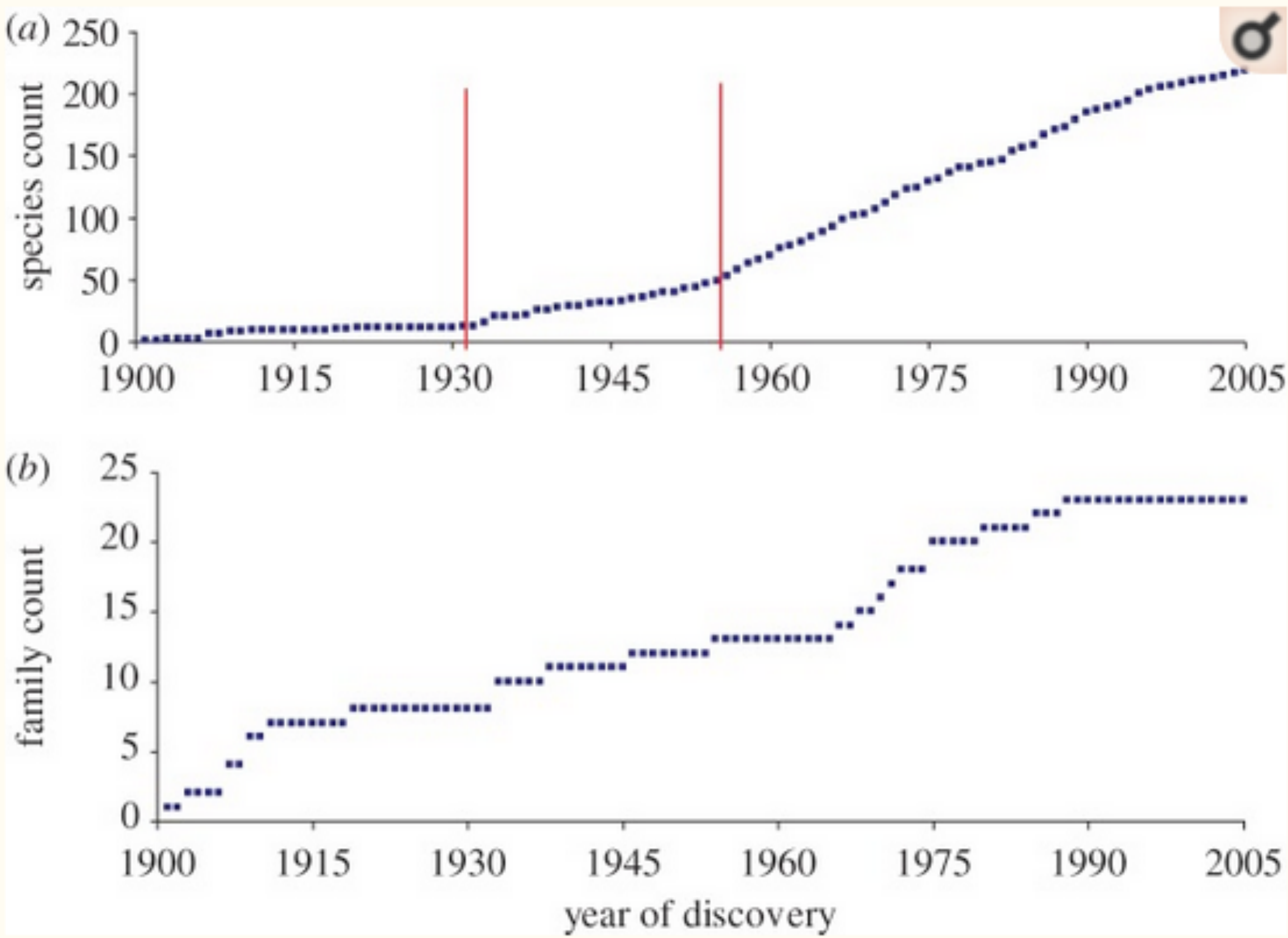
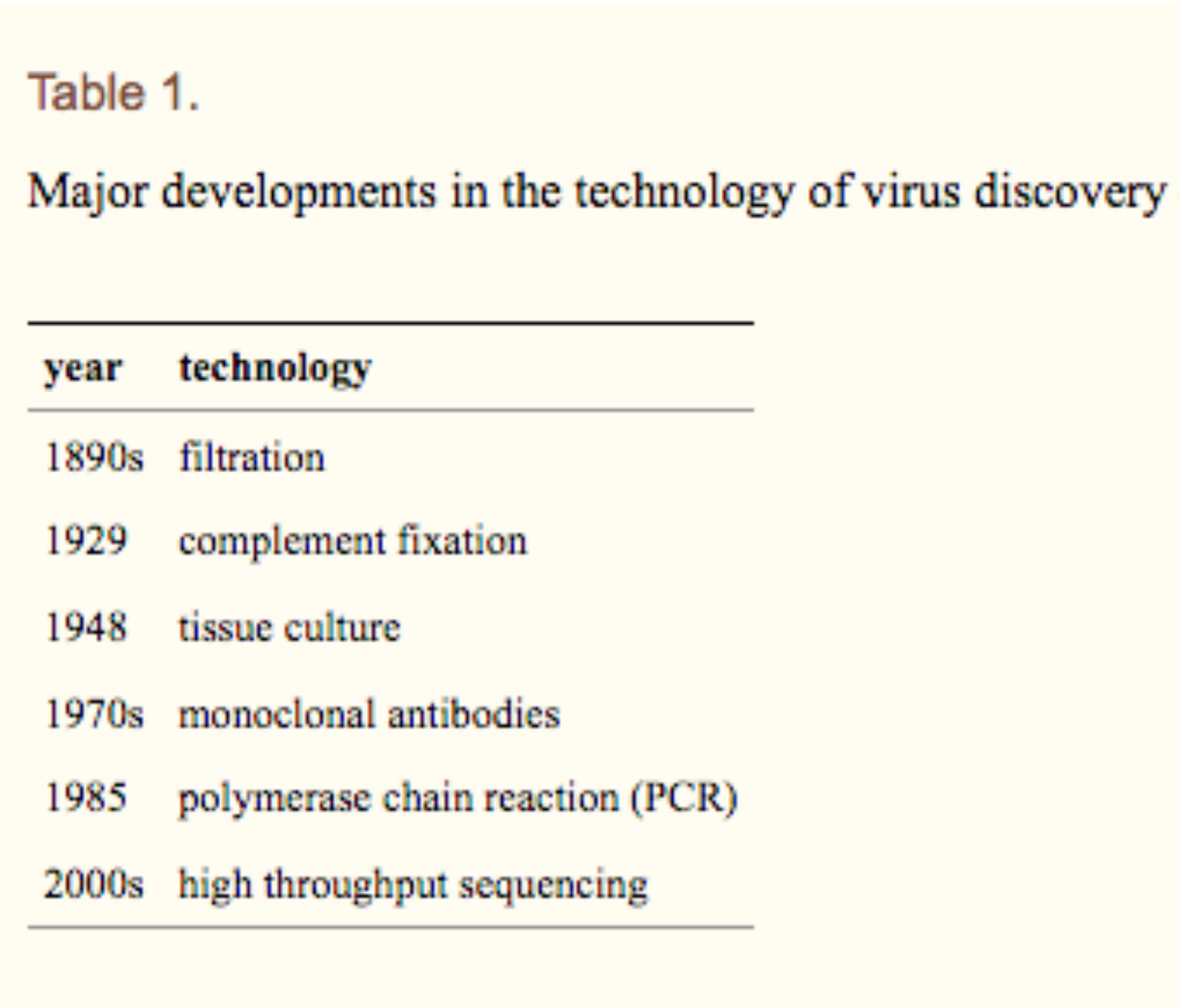
Discovery of Epstein Barr Virus
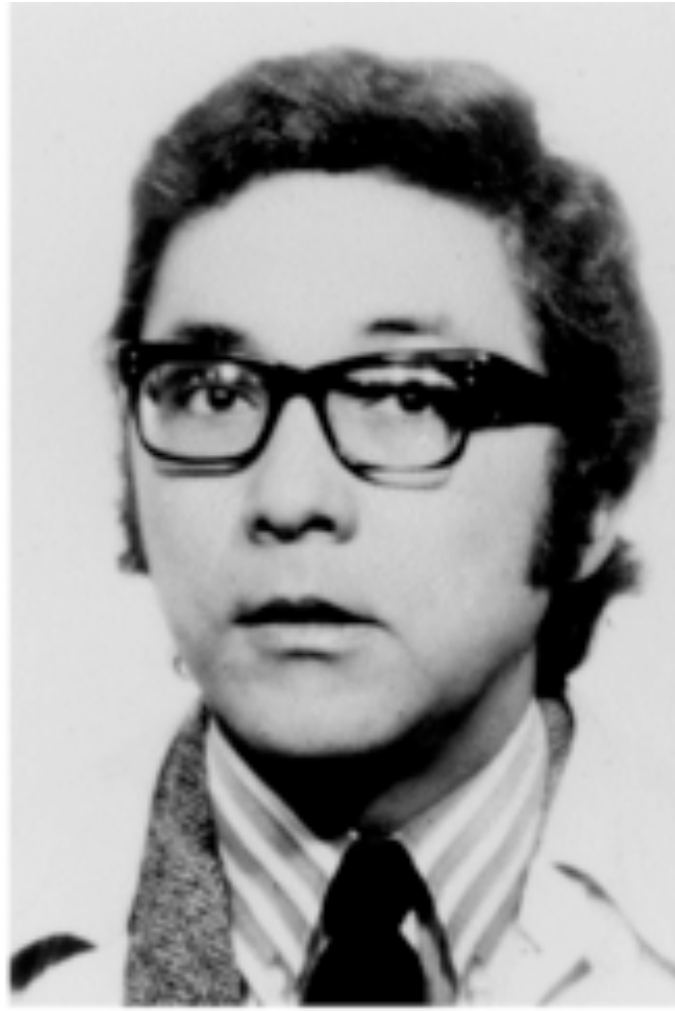
Historical Context30
- Discovered by M.A. Epstein, B.G. Achong, and Y.S. Barr in 1964.
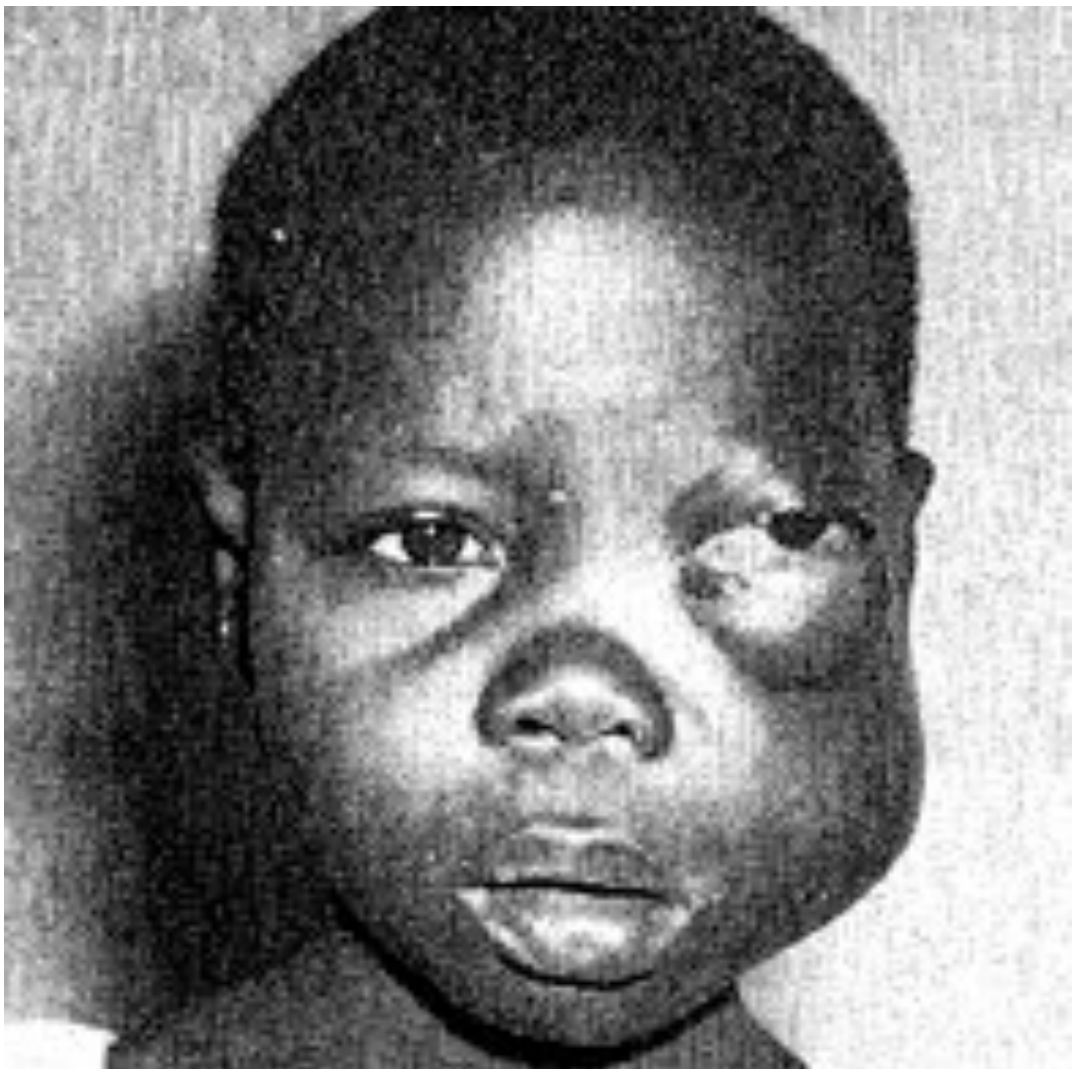
Connection to Burkitt Lymphoma
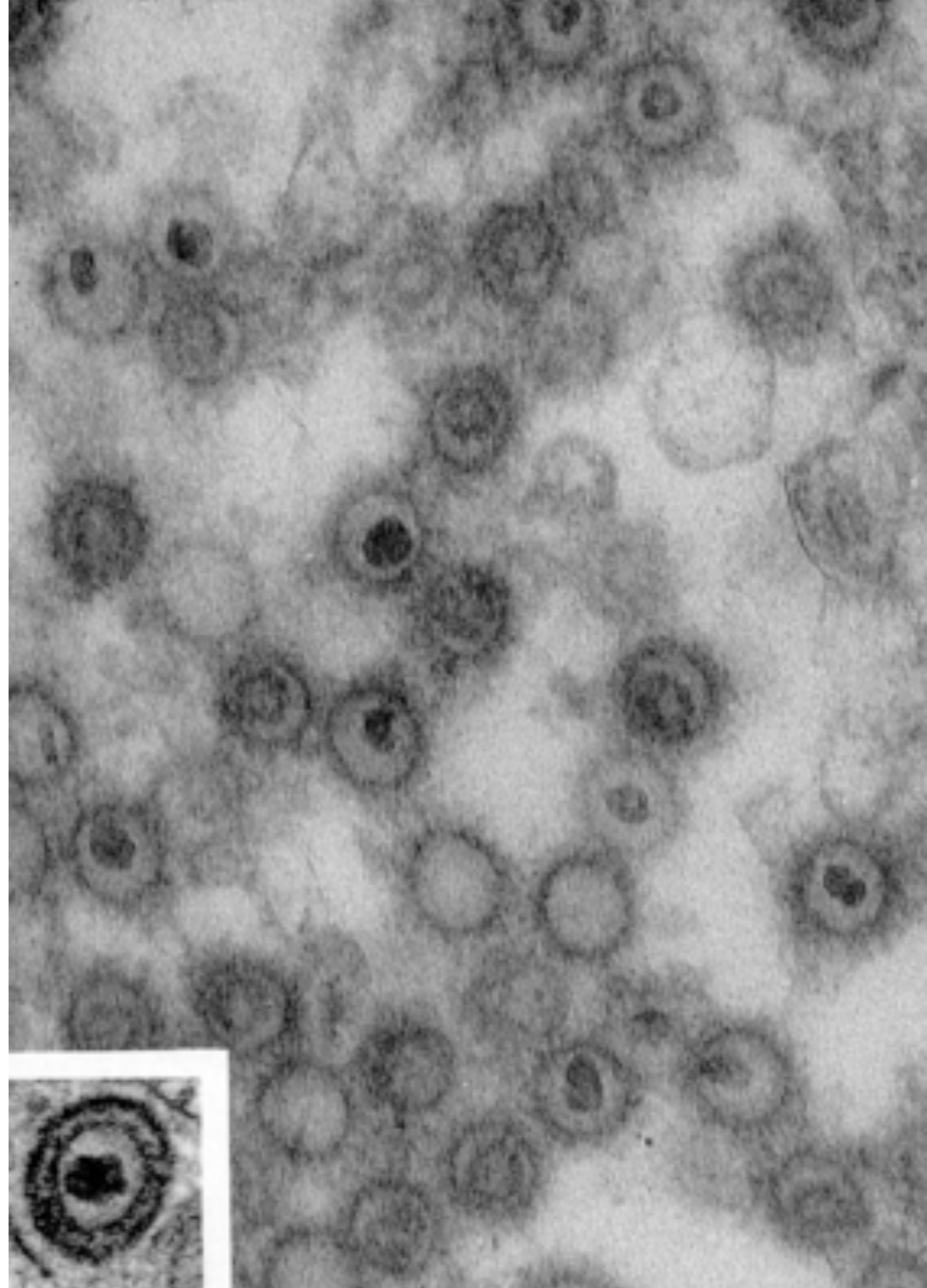
In 1958, Dr. Burkitt identified aggressive jaw tumors in African children (Burkitt Lymphoma). By 1964, Anthony Epstein and Yvonne Barr identified viral particles in these B-cell lymphocytes using electron microscopy.
 |  |  |
 |  |
Virology
-
Electron microscopy reveals immature virions and mature enveloped particles.
-
Identified as a member of the herpesvirus family based on structural characteristics.
-
EBV specifically infects B-cells, causing rapid division
-
Genetic "mistakes" during this rapid division, combined with the virus, can lead to the development of Burkitt Lymphoma
Herpangina
Historical Background31
- First described as “Herpetic Sore Throat” (1920) and later named “Herpangina” (1924) by Dr. John Zahorsky.
- Also historically referred to as “Aphthous Pharyngitis.”
 |  |
Etiology and Epidemiology
Etiology32
- Agent: Coxsackie group A viruses.
Epidemiology and Transmission
- Age: Primarily affects children up to 10 years of age.
- Gender: No gender predilection.
- Transmission: Fecal-oral route.
- Incubation Time: 4 to 7 days.
Clinical Presentation
General Symptoms33
- Low-grade fever, malaise, and headache.
- Sore throat, dysphagia, anorexia, and rhinorrhea.
- Gastrointestinal distress (vomiting, diarrhea) and myalgia.
Oral Manifestations
- Lesions: Red macules (typically 2–6) that form fragile vesicles and rapidly ulcera
- Posterior oropharynx and soft palate are the primary diagnostic locations for these lesions.te (2–4 mm).
- Site: Palate, pillars of the fauces, and pharynx.
- Distinction: Unlike other infections, herpangina lesions do not coalesce into large ulcerated areas.
Course of Disease
- Self-limiting; healing occurs within 1–2 weeks.
Clinical Appearance34
- Numerous aphthous-like ulcerations localized to the soft palate.

Diagnosis and Histopathology
Histopathology35
- Intraepithelial vesicles containing eosinophilic exudate.
- Nuclear ballooning degeneration of epithelial cells.
Diagnosis
- Based on clinical appearance and history.
- Recognition of known epidemics.
- Viral culture from a swab.
Differential Diagnosis
- Other viral mucosal ulcers including Herpes Simplex Virus (HSV), Cytomegalovirus (CMV), and Epstein-Barr Virus (EBV).
- Hand-Foot-and-Mouth Disease (often caused by similar enteroviruses).
Epidemiological Reports36
- Significant outbreaks have been documented globally, including large-scale events in Hangzhou, China (2015) and France (2010).
- Outbreaks are frequently associated with Coxsackievirus A6, A10, and other enteroviruses.

Management and Complications
Management37
- Symptomatic care focusing on adequate hydration.
- Use of analgesics for pain and antipyretics for fever.
Potential Complications
- Pneumonia and pulmonary edema.
- Hemorrhage.
- Acute flaccid paralysis.
- Encephalitis and meningitis.
- Carditis.
Hand Foot and Mouth Disease
Etiology and Epidemiology
Etiology38
- Coxsackie A virus
- Coxsackie B virus
- Enterovirus 71
Epidemiology
- Age: Primarily affects children up to 10 years of age.
- Gender: No gender predilection.
Clinical Presentation
General Symptoms39
- Low-grade fever and malaise.
- Sore throat and dysphagia.
- Occasional cough, rhinorrhea, anorexia, vomiting, diarrhea, myalgia, and headache.
Oral Manifestations
- Appearance: Resemble herpangina but are typically more numerous (1 to 30 lesions).
- Lesions: Red macules that form fragile vesicles and rapidly ulcerate (2–4 mm).
- Sites: Frequently involves anterior regions including buccal mucosa, labial mucosa, and tongue, as well as the palate, fauces, and pharynx.
Cutaneous Manifestations40
- Sites: Primarily the borders of palms and soles, and the ventral surfaces/sides of fingers and toes. Occasionally involves buttocks, genitals, and legs.
- Progression: Erythematous macules develop central vesicles; these heal without crusting.
- Nail Changes: Nail loss or Beau lines (ridges) may occur several weeks post-infection.
Course of Disease
- Self-limiting; healing typically occurs within 1 week.
Visual Clinical Markers41
- Multiple aphthous-like ulcerations in the mucobuccal fold.
- Numerous cutaneous vesicles on the sides of the fingers and the skin of the toes.
 |  |
 |
Post-Infection Nail Changes42
Clinical evidence shows that Hand, Foot and Mouth Disease can lead to significant changes in the nail plate, including shedding or the development of deep ridges.
- ==Onychomadesis: Complete shedding of the nail==
- ==Beau’s Lines: Transverse ridging due to temporary arrest of the nail matrix==

Histopathology and Diagnosis
Histopathology43
- Early Stages: Intraepithelial vesicles with intra-cytoplasmic eosinophilic inclusion bodies.
- Later Stages: Shallow ulcerations and erosions with marginal epithelium regeneration.
- Submucosa: Superficial inflammatory cell infiltrate.
Differential Diagnosis
- Herpetic gingivostomatitis
- Herpangina
- Varicella
- Aphthous stomatitis
Diagnosis
- Clinical appearance and history.
- Recognition of epidemic patterns.
- Viral culture from a swab.
Management and Complications
Management44
- Symptomatic care and hydration.
- Antipyretics and analgesics for pain control.
- Typical disease course lasts 7–10 days
Complications
- Neurological complications.
- Viral meningitis.
- Encephalitis.
- Cerebellar ataxia.
Varicella Chickenpox
Etiology and Transmission
Etiology45
- Agent: Varicella-zoster virus (VZV or HHV-3).
Transmission
- Spread via air droplets.
- Direct contact with active lesions.
- Incubation Period: 10 to 21 days (average of 15 days).
Epidemiology
- Chickenpox: Primary form affecting children.
- Shingles: Recurrent form affecting older adults.
- Gender: No gender predilection.
Clinical Presentation
Presentation in Immunized Children46
- General: Low or no fever.
- Skin: Maculopapular cutaneous rash with a small number of lesions.
- Oral: Few or no vesicles.
- Course: Shortened duration of approximately 4 to 6 days.
Presentation in Unimmunized Individuals47
- General: Malaise, pharyngitis, rhinitis, headache, myalgia, and nausea.
- High fever
- Intensely pruritic (itchy) rash
- Skin Rash:
- Intensely pruritic exanthema starting on the face/trunk and spreading to extremities.
- Vesicular Stage: “Dewdrop on a rose petal” appearance (vesicle on an erythematous base).
- Lesions erupt over 4+ days; various stages (crusted and new) appear simultaneously.
 |  |
Oral Manifestations (Unimmunized)48
- Lesions: Begin as 3–4 mm white, opaque vesicles that rupture into 1–3 mm ulcerations.
- Sites: Frequently the vermilion border and palate; also buccal mucosa and gingiva.
- Severity:
- Mild: 1–2 ulcers healing in 1–3 days.
- Severe: Up to 30 ulcers persisting for 5–10 days.
National Immunisation Program
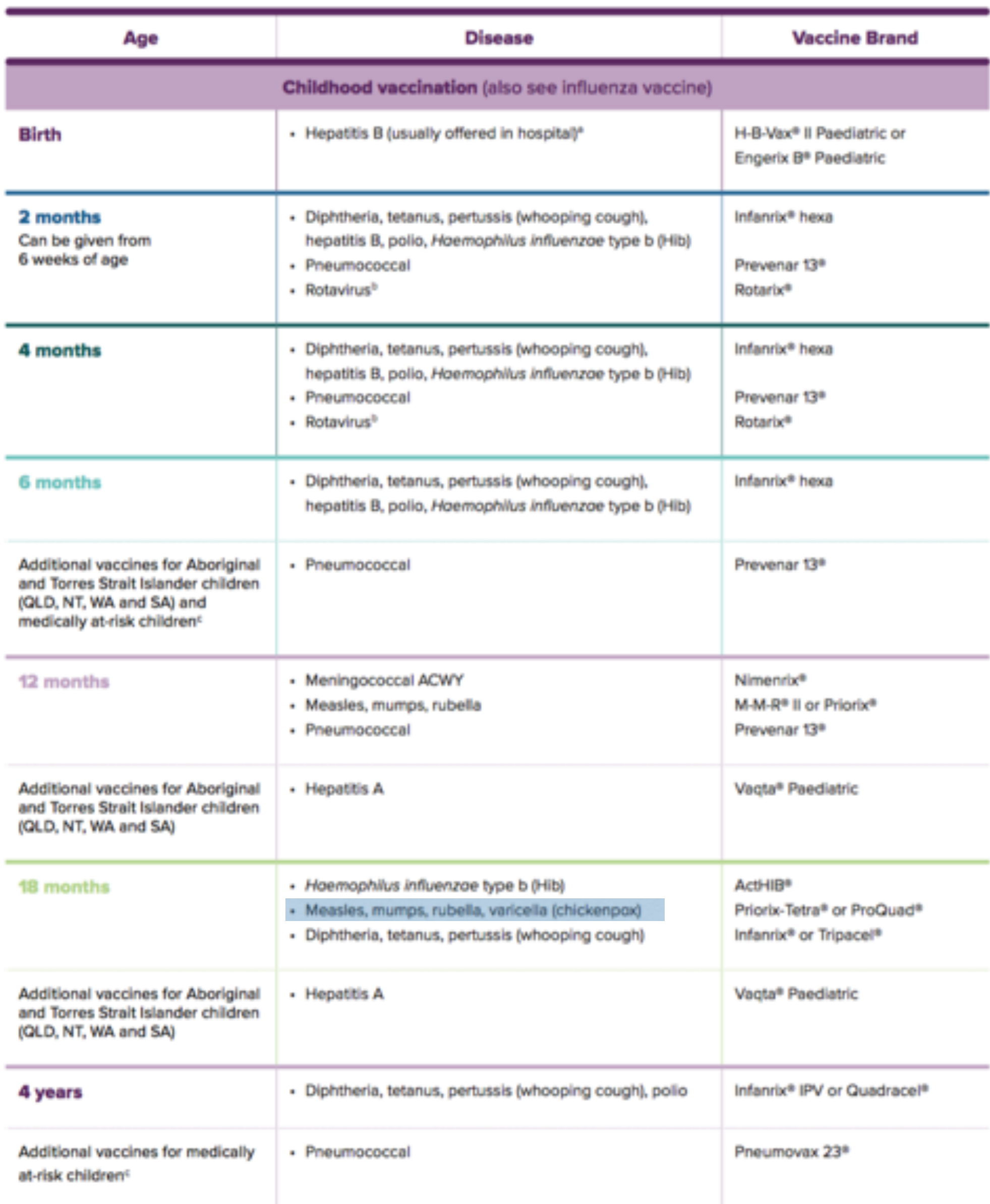
Childhood Schedule (Selected Entries)49
- 12 Months: Meningococcal ACWY; Measles, mumps, rubella (MMR); Pneumococcal.
- 18 Months: Hib; Measles, mumps, rubella, varicella (MMRV - e.g., Priorix-Tetra® or ProQuad®); DTPa.
 | 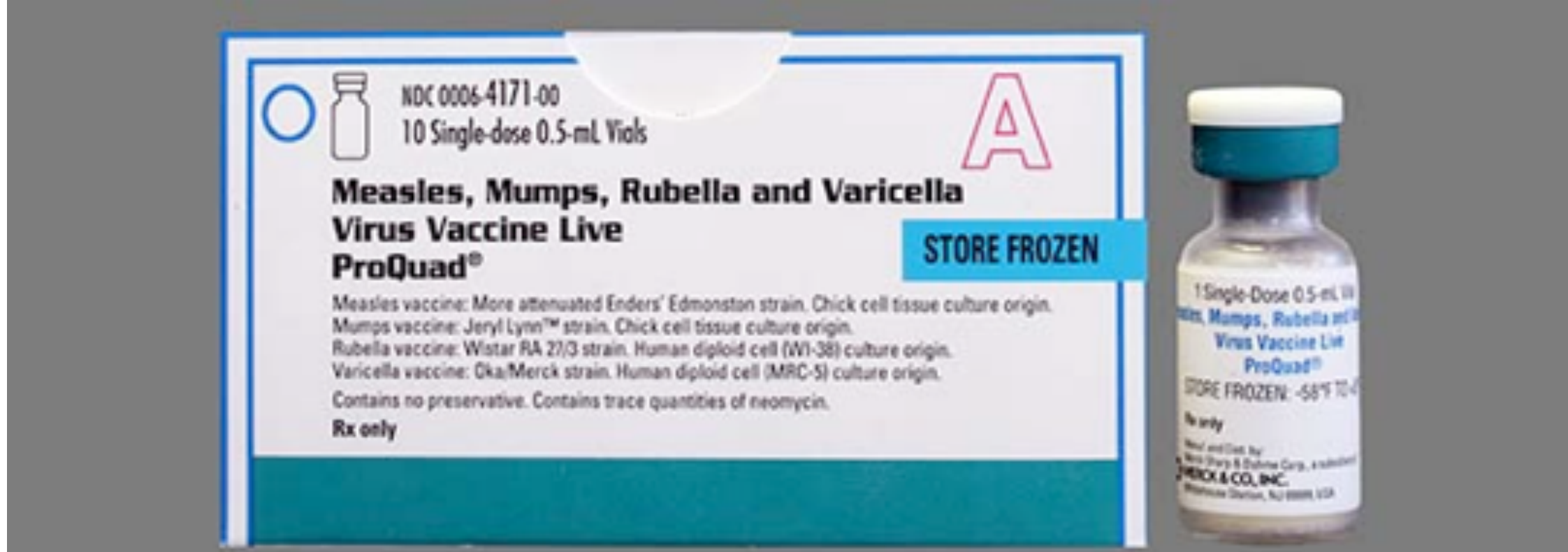 |
Vaccine Details (ProQuad®)
- Combined live virus vaccine for Measles, Mumps, Rubella, and Varicella.
- Varicella component: Oka/Merck strain.
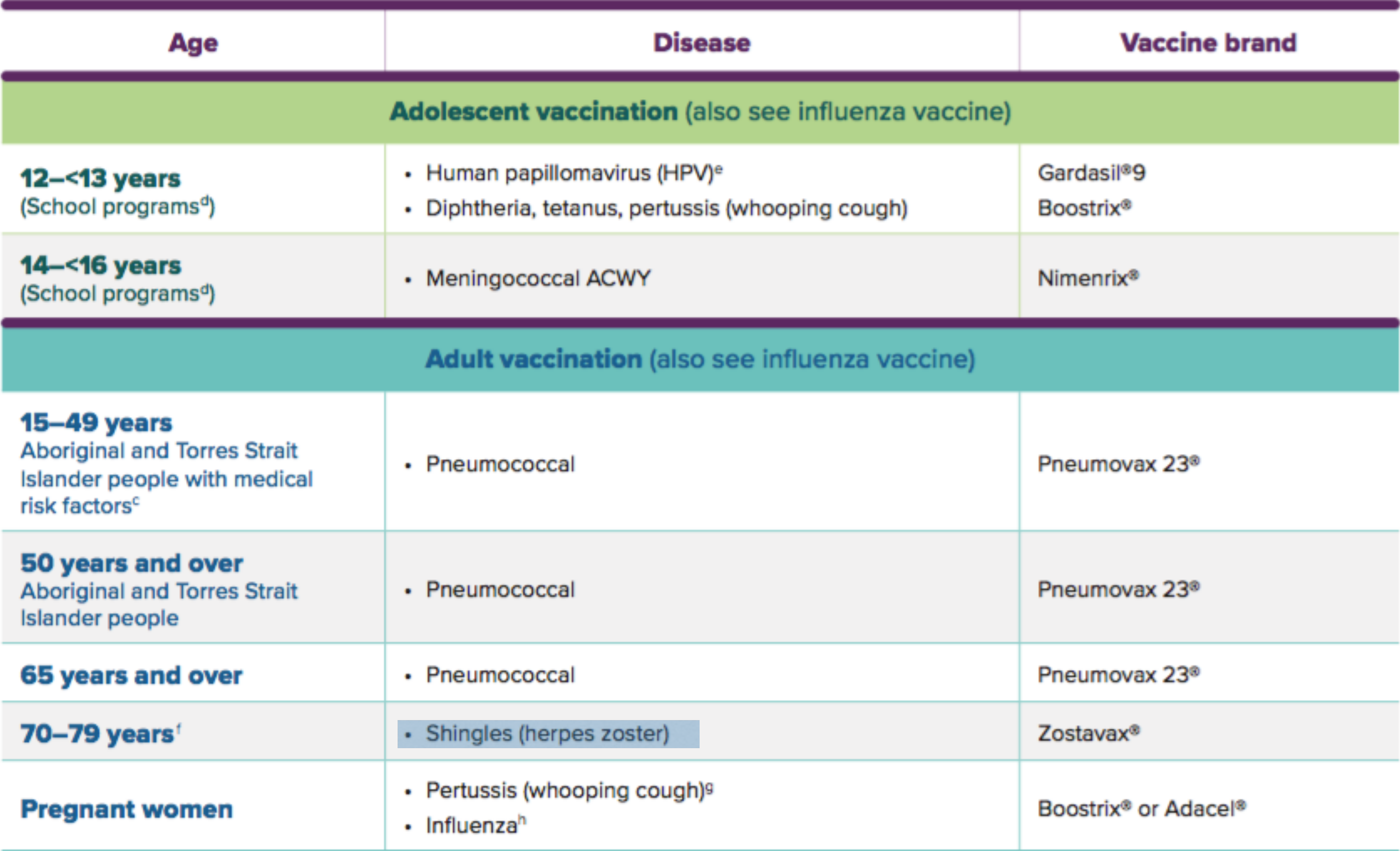
Adolescent and Adult Schedule50
- 12–13 Years: HPV (Gardasil®9) and DTPa (Boostrix®).
- 14–16 Years: Meningococcal ACWY.
- 70–79 Years: Shingles (Zostavax®).
- Pregnant Women: Pertussis and Influenza.
Diagnosis and Histopathology
Histopathology51
- Cytologic alterations are virtually identical to HSV.
- Features include acantholysis and the formation of free-floating Tzanck cells with nuclear margination of chromatin and multinucleation.
- Acantholysis involves the disruption of desmosomes and intercellular junctions.
Diagnosis
- Viral cytology.
- PCR: Performed on vesicular fluid, lesion base cells, or scabs.
- Direct fluorescent antibody assay.
Treatment and Complications52
Symptomatic Treatment53
- Relief of pruritus: Warm baths (with baking soda or oatmeal), calamine lotion, and antihistamines.
- Antipyretic: Acetaminophen.
Antiviral Medications
- Agents: Acyclovir, valacyclovir, and famciclovir.
- Effectiveness: Reduces duration and severity if administered within 24 hours of rash onset.
Complications54
- Secondary skin infections (often Group A β-hemolytic streptococci).
- Severe Systemic Conditions:
- Encephalitis
- Pneumonia
- Necrotizing fasciitis
- Septicemia
- Toxic shock syndrome
Conclusion of clinical review on Varicella complications and management.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Footnotes
-
Original PDF page 1: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.1 ↩
-
Original PDF page 2: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.2 ↩
-
Original PDF page 3: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.3 ↩
-
Original PDF page 4: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.4 ↩
-
Original PDF page 5: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.5 ↩
-
Original PDF page 6: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.6 ↩
-
Original PDF page 7: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.7 ↩
-
Original PDF page 8: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.8 ↩
-
Original PDF page 9: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.9 ↩
-
Original PDF page 11: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.11 ↩
-
Original PDF page 10: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.10 ↩
-
Original PDF page 12: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.12 ↩
-
Original PDF page 13: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.13 ↩
-
Original PDF page 14: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.14 ↩
-
Original PDF page 15: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.15 ↩
-
Original PDF page 29: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.29 ↩
-
Original PDF page 16: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.16 ↩
-
Original PDF page 17: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.17 ↩
-
Original PDF page 18: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.18 ↩
-
Original PDF page 19: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.19 ↩
-
Original PDF page 20: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.20 ↩
-
Original PDF page 21: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.21 ↩
-
Original PDF page 22: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.22 ↩
-
Original PDF page 24: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.24 ↩
-
Original PDF page 23: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.23 ↩
-
Original PDF page 25: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.25 ↩
-
Original PDF page 26: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.26 ↩
-
Original PDF page 27: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.27 ↩
-
Original PDF page 28: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.28 ↩
-
Original PDF page 30: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.30 ↩
-
Original PDF page 31: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.31 ↩
-
Original PDF page 33: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.33 ↩
-
Original PDF page 34: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.34 ↩
-
Original PDF page 35: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.35 ↩
-
Original PDF page 36: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.36 ↩
-
Original PDF page 37: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.37 ↩
-
Original PDF page 38: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.38 ↩
-
Original PDF page 39: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.39 ↩
-
Original PDF page 40: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.40 ↩
-
Original PDF page 41: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.41 ↩
-
Original PDF page 42: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.42 ↩
-
Original PDF page 43: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.43 ↩
-
Original PDF page 44: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.44 ↩
-
Original PDF page 45: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.45 ↩
-
Original PDF page 46: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.46 ↩
-
Original PDF page 47: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.47 ↩
-
Original PDF page 48: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.48 ↩
-
Original PDF page 49: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.49 ↩
-
Original PDF page 50: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.50 ↩
-
Original PDF page 51: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.51 ↩
-
Original PDF page 52: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.52 ↩
-
Original PDF page 55: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.55 ↩
-
Original PDF page 53: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.53 ↩
-
Original PDF page 54: Lecture 7 - Orofacial Infections in Paediatric Dentistry, p.54 ↩