Seminar Summary: Caries Detection, ICDAS, and Developmental Enamel Defects
This document summarizes key points from the seminar on caries detection, the International Caries Detection and Assessment System (ICDAS), and developmental defects of enamel (with emphasis on MIH and HSPM). It includes practical guidance for clinical and epidemiological scoring, diagnostic tips, and examples of common pitfalls.
Objectives
- Review dental caries as a disease process and the importance of early detection.
- Describe limitations of traditional visual assessment and benefits of validated systems.
- Explain ICDAS coding (focus on lesion scoring) and its clinical implications.
- Present classification and scoring for developmental defects of enamel, particularly MIH and HSPM.
- Provide practical steps and examples for calibration and scoring in clinical and field settings.
1. Dental Caries: Concepts and Diagnostic Goals
Key points:
- Dental caries is a dynamic, multifactorial disease involving cycles of demineralization and remineralization. Focusing only on cavitated lesions neglects the broader disease process.
- Ideal diagnostic tools should:
- Detect lesions at the earliest stage possible.
- Be valid for risk assessment across age groups.
- Determine lesion activity and allow monitoring over time.
- No current diagnostic method fully meets all ideal criteria. Visual and radiographic assessments remain the mainstays, each with strengths and limitations.
Limitations of traditional, qualitative diagnosis:
- Descriptive terms (e.g., “soft and sticky,” “brown spot,” “watch”) are subjective and poorly reproducible.
- Subjectivity leads to inconsistent diagnosis and may drive over- or under-treatment.
- There is a professional need for greater standardization.
Radiographic adjuncts:
- Bitewing radiographs are highly accurate for proximal lesions, especially when the lesion extends past the DEJ.
- Radiographs are less sensitive for occlusal lesions (study cited: only ~33% of occlusal lesions detected by bitewings). Use radiographs as an adjunct, especially for proximal disease.
Practical diagnostic principles:
- Use validated systems when possible to improve reliability.
- Clean teeth (prophy, brushing, water + gauze) before assessment; plaque can mask lesions.
- Dry teeth to reveal early white spot lesions (important for differentiating ICDAS 1 vs 2 on smooth surfaces).
2. ICDAS: Purpose, Structure, and Use
Overview:
- ICDAS (International Caries Detection and AssessmentAZ System) is a validated, evidence-based system for standardized visual scoring of coronal caries.
- ICDAS uses a two-digit code (first digit for restorations/tooth status; second digit for lesion severity). For routine scoring we often focus on the second digit (lesion code 0–6).
Principles:
- Aligns with minimal intervention dentistry: if unsure, score lower (prefer under-calling to over-calling).
- Enables monitoring lesion progression or regression over time.
- Linked with treatment recommendations (preventive/microinvasive vs operative).
ICDAS second-digit codes (0–6)
- 0 — Sound tooth surface (no evidence of caries after cleaning and drying).
- 1 — First visual change in enamel (seen only after drying or confined to pit/fissure).
- Pit/fissure: lesion confined to pits/fissures.
- Smooth surface: visible only after drying.
- 2 — Distinct visual change in enamel (visible when wet or seen without drying); on pits/fissures or smooth surfaces beyond pits/fissures.
- 3 — Localized enamel breakdown (microcavitation) without visible dentine involvement.
- 4 — Underlying dark shadow from dentine (an undermining grey shadow), with or without enamel breakdown; no frank cavitation into dentine visible.
- 5 — Distinct cavity with visible dentine; less than half the surface involved.
- 6 — Extensive distinct cavity with visible dentine; more than half the surface involved.
Treatment linkage (general guidance):
- ICDAS 0–4: preventive or microinvasive approaches favored (monitoring, remineralization, sealants, minimally invasive restorations).
- ICDAS 5–6: operative treatment typically indicated.
Decision rules and tips:
- For pit and fissure surfaces: code 1 if lesion confined to pits/fissures; code 2 if lesion extends beyond pits/fissures.
- For smooth surfaces: code 1 if visible only after drying; code 2 if visible when wet.
- If more than one feature on a tooth, record the most severe relevant code (with exceptions—see developmental defects section).
- If in doubt, choose the lower code.
Practical note for field epidemiology:
- ICDAS 1 and 2 require thorough cleaning and drying. In many field settings these are difficult to reliably identify, so epidemiological surveys often focus on ICDAS 3+ (microcavitation and beyond).
3. Visual Assessment Practical Steps
Workflow for a reliable visual exam:
- Clean the teeth (remove plaque and debris).
- Dry surfaces to identify initial enamel changes (when feasible).
- Inspect each surface systematically, using ICDAS criteria.
- Use radiographs as adjuncts for proximal detection (especially bitewings).
- Record both tooth-level and surface-level findings.
- When multiple presentations appear on a single tooth, document:
- The most severe lesion for opacities (color/severity).
- Both developmental defect features and caries codes when applicable (e.g., post-eruptive breakdown + ICDAS 5).
Common pitfalls to avoid:
- Interpreting white or brown opacities without considering alternative causes (fluorosis, developmental defects, trauma).
- Charting ambiguous notations like “watch” without specifying lesion type/score.
- Confusing non-carious tooth surface loss (attrition, abrasion) with caries.
Histological basis of white spot lesions:
- Loss of mineralization creates porosities that alter light refraction, producing “white spot” appearance (ICDAS 1–2).
4. Distinguishing White Spots and Causes
White/brown opacities can reflect different etiologies. Common diagnoses to consider:
- Carious white spot (ICDAS 1–2): localized, associated with plaque, often in caries-prone areas.
- Fluorosis (diffuse opacities): symmetrical, generalized pattern, affects many teeth.
- Developmental defects of enamel (e.g., MIH): well-demarcated opacities often in incisors and first permanent molars; can be white, yellow, or brown.
- Hypomineralization due to trauma/infection (Turner’s tooth): localized defect on a single tooth, often associated with prior infection/trauma to the primary predecessor.
Clinical clues:
- Distribution/pattern across the dentition (generalized vs localized).
- Location on the tooth (pit/fissure, cervical, incisal third, palatal cusp, cusp tip).
- Associated signs: gingivitis, plaque accumulation, atypical restorations, post-eruptive breakdown.
5. Developmental Defects of Enamel — MIH and HSPM
Definitions:
- MIH (Molar Incisor Hypomineralization): systemic-origin hypomineralization affecting one to all first permanent molars, with possible incisor involvement.
- HSPM (Hypomineralized Second Primary Molars): similar condition affecting second primary molars and sometimes primary canines.
Epidemiology:
- MIH: estimated prevalence ~1 in 7 children.
- HSPM: estimated prevalence ~1 in 10 children.
Diagnostic criteria (for MIH/HSPM):
- Opacities (white, yellow, brown) with well-demarcated borders.
- Post-eruptive enamel breakdown (PEB) in atypical locations (e.g., cusp tips, palatal surfaces).
- Atypical restorations (unusual shape, location, or extensive restorations in young children).
- Atypical caries/extractions that do not match expected cariogenic patterns.
Opacity characteristics:
- Color range: white → yellow → brown.
- Well-demarcated borders differentiate these opacities from diffuse fluorosis.
- Severity correlates with tooth mineral density: yellow/brown opacities often indicate poorer mineralization and higher risk of PEB.
Post-eruptive enamel breakdown (PEB):
- Typical locations are low caries-risk areas (cusps, palatal surfaces); margins are rough and irregular.
- PEB often precedes or coexists with secondary caries.
- When PEB and cavitation into dentine are both present, record both PEB and the appropriate ICDAS (usually 5 or 6).
Atypical restorations and extractions:
- Restorations with unconventional margins or on atypical surfaces in children suggest underlying developmental defects rather than classic caries patterns.
- Extractions of first permanent molars or second primary molars at atypical ages or for unusual reasons may indicate developmental enamel defects.
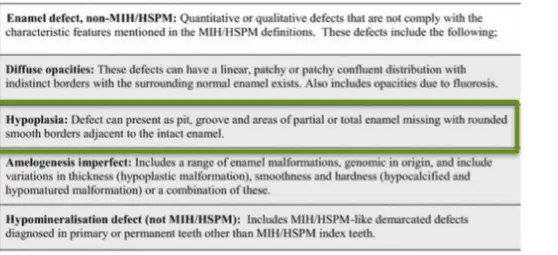
Coding developmental and non-MIH/HSPM defects (epidemiological approach)
- Non-MIH/HSPM categories:
- Diffuse opacities (e.g., fluorosis) — generalized pattern.
- Hypoplasia/chronological defects — quantitative enamel loss affecting single or multiple teeth.
- Amelogenesis imperfecta — hereditary, typically affects the whole dentition.
- Localized hypomineralization due to infection/trauma (Turner’s tooth).
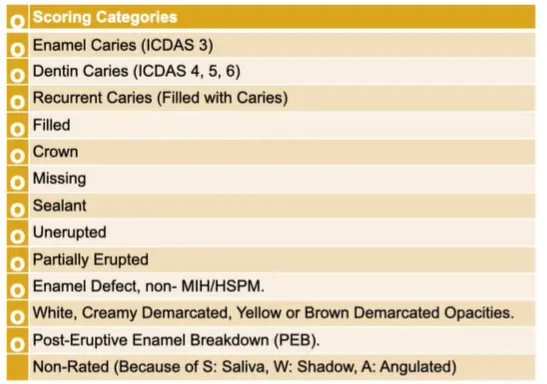
- MIH/HSPM categories:
- Opacity (white, yellow, brown) — score severity; choose most severe if multiple on same tooth.
- PEB — record when present, in addition to caries coding if cavitation is present.
- Atypical restorations or atypical extraction history — indicate developmental origin.
6. Rules for Recording and Scoring (Practical Guidance)
 General recording rules:
General recording rules:
- Score both tooth and surface where relevant (different surfaces may have different lesion status).
- When multiple distinct features are present on one tooth:
- For opacities: record the most severe color (brown > yellow > white).
- For PEB + cavitation: record PEB and the ICDAS code for cavitation (often ICDAS 5 or 6).
- If image quality or visibility is inadequate, do not score (record as non-rated).
- Do not score teeth that are exfoliated (unless known to be extracted due to caries or developmental defect).
- Do not score non-carious tooth surface loss (attrition, abrasion) as caries or developmental defect.
Specific scoring decisions:
- If cavitation involves dentine and affects less than half of the tooth surface → ICDAS 5.
- If cavitation involves dentine and affects more than half → ICDAS 6.
- If gray shadow from dentine exists without visible cavitation → ICDAS 4.
- If microcavitation limited to enamel → ICDAS 3.
- Use ICDAS 1–2 only when cleaning and drying are achievable; otherwise focus on ICDAS 3+ in epidemiological/field work.
Example combinations to record:
- Tooth with brown opacity and microcavitation into enamel → record brown opacity + ICDAS 3.
- Tooth with PEB and obvious cavitation into dentine (more than half) → record PEB + ICDAS 6.
- Tooth with atypical large restoration on palatal/occlusal aspect in a child → note atypical restoration (MIH/HSPM indicator) and code caries/restoration status.
7. Clinical Examples and Common Scenarios (Synthesis)
Patterns suggesting developmental defects rather than primary caries:
- Severe enamel breakdown on palatal surfaces, cusp tips, or other atypical sites in a child with otherwise low plaque accumulation.
- Multiple first permanent molars and/or incisors with demarcated opacities.
- Early extensive restorations or atypically shaped restorations in young children.
- Localized defects on a single erupting premolar associated with history of infection/trauma to the primary predecessor (Turner’s tooth).
Field scoring practicalities:
- Many clinical images have limitations (saliva, mirror reflections, incomplete views). If a surface cannot be reliably visualized, leave it non-rated.
- In population surveys, prioritize detection of ICDAS 3+ and of MIH/HSPM features (opacities, PEB, atypical restorations/extractions).
8. Key Takeaways
- Caries should be approached as a disease process; early detection and preventive strategies are essential.
- Traditional qualitative descriptions are subjective; ICDAS provides a validated, standardized approach that improves diagnostic consistency and links directly to evidence-based treatment decisions.
- Always clean teeth before assessment and dry surfaces when distinguishing ICDAS 1 vs 2; in field settings focus on ICDAS 3+.
- MIH and HSPM are common and frequently misdiagnosed as caries; consider lesion pattern, location, color, and patient history when differentiating.
- Record both developmental defect features (opacities, PEB, atypical restorations) and caries severity (ICDAS codes) when applicable.
- When uncertain, err on the side of scoring lower to avoid over-treatment.
9. Next Steps for Participants
- Calibration exercises: the seminar will include case-based scoring to assist calibration.
- Formal assessment: an online quiz will be provided to validate and standardize participants’ use of ICDAS and enamel defect scoring in clinical and epidemiological contexts.
For further reading, consult the primary ICDAS publications and recent systematic reviews on MIH/HSPM diagnosis and management.