Case 1: Primary Herpetic Gingivostomatitis
Patient History1
- 20-month-old boy
- Fit and well
- Fever for 3 days
- Poor oral intake (accepting only ice cream)
 |  |
Clinical Considerations
- Questions for parents?
- When did the symptoms start?
- Were there ulcers in the mouth before the current presentation?
- What medications have been given for management?
- Are there any other medical problems?
- Diagnosis?
- Primary Herpetic Gingivostomatitis.
- Causative agent?
- Herpes Simplex Virus (HSV), most likely Type 1.
- Infectiousness?
- Highly infectious; transmitted through secretions.
- Peak incidence?
- 12 to 18 months.
- Management
- Reassurance: Parents are often distressed because the child is upset, not eating, and has had a fever; reassurance is a key part of the clinical interaction.
- Differential Diagnosis: While some may mistake palatal sloughing for calculus, the age range and clinical presentation strongly suggest an infectious viral presentation.
Clinical Presentation and Diagnosis
Etiology and Epidemiology2
- Causative Agent: Herpes simplex Virus Type I
- Peak Incidence: 12-18 months
- ==Epidemiology: Very common viral presentation for this age group.==
 |  |
Systemic Symptoms
- Fever (Often present for a few days before the clinician is consulted)
- Headaches
- Malaise
- Irritability (The child may be generally "off" or irritable for several days)
- Cervical lymphadenopathy (Swollen cervical lymph nodes may be palpable)
- Dysphagia: Difficulty or pain when eating and swallowing.
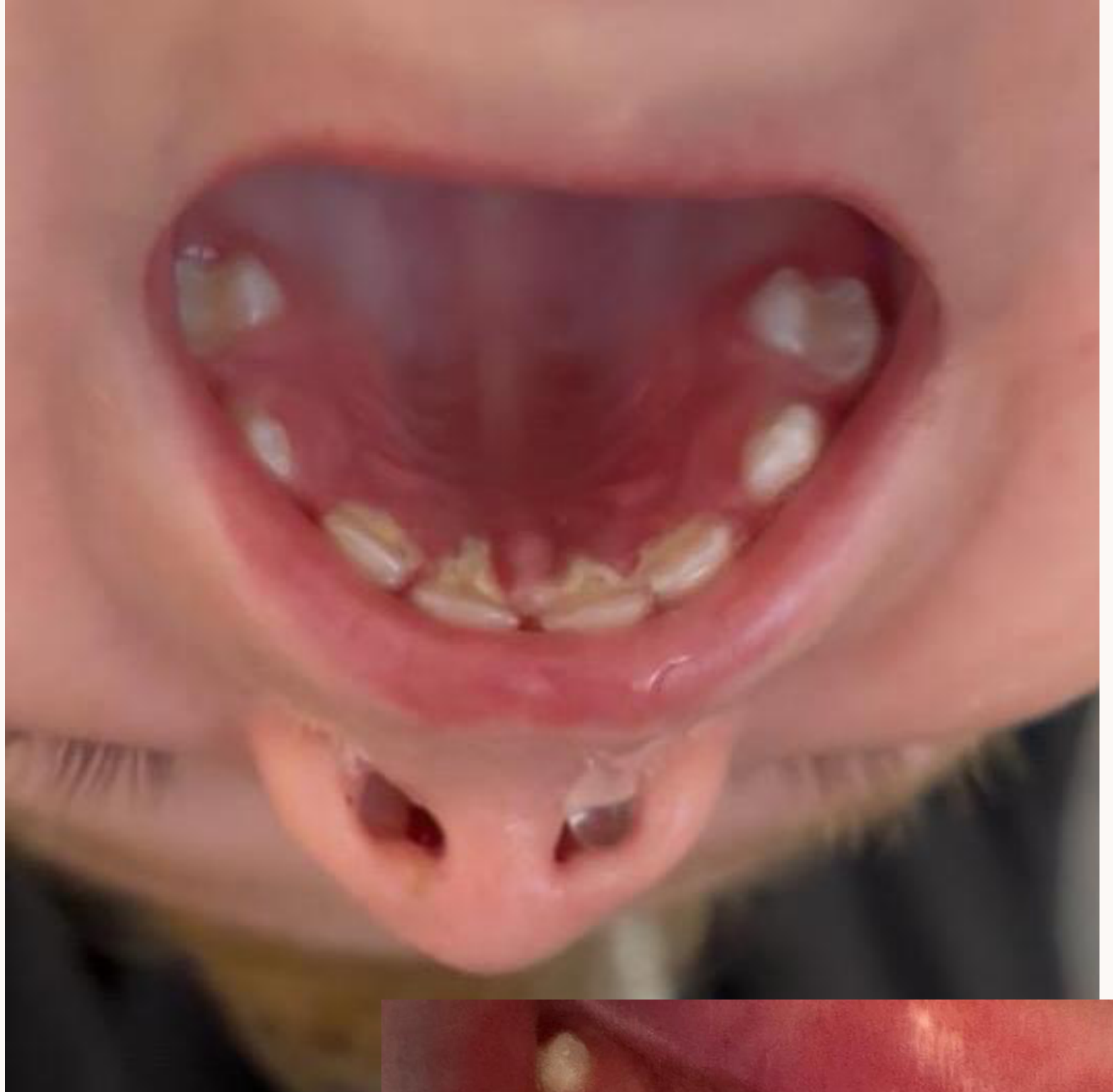
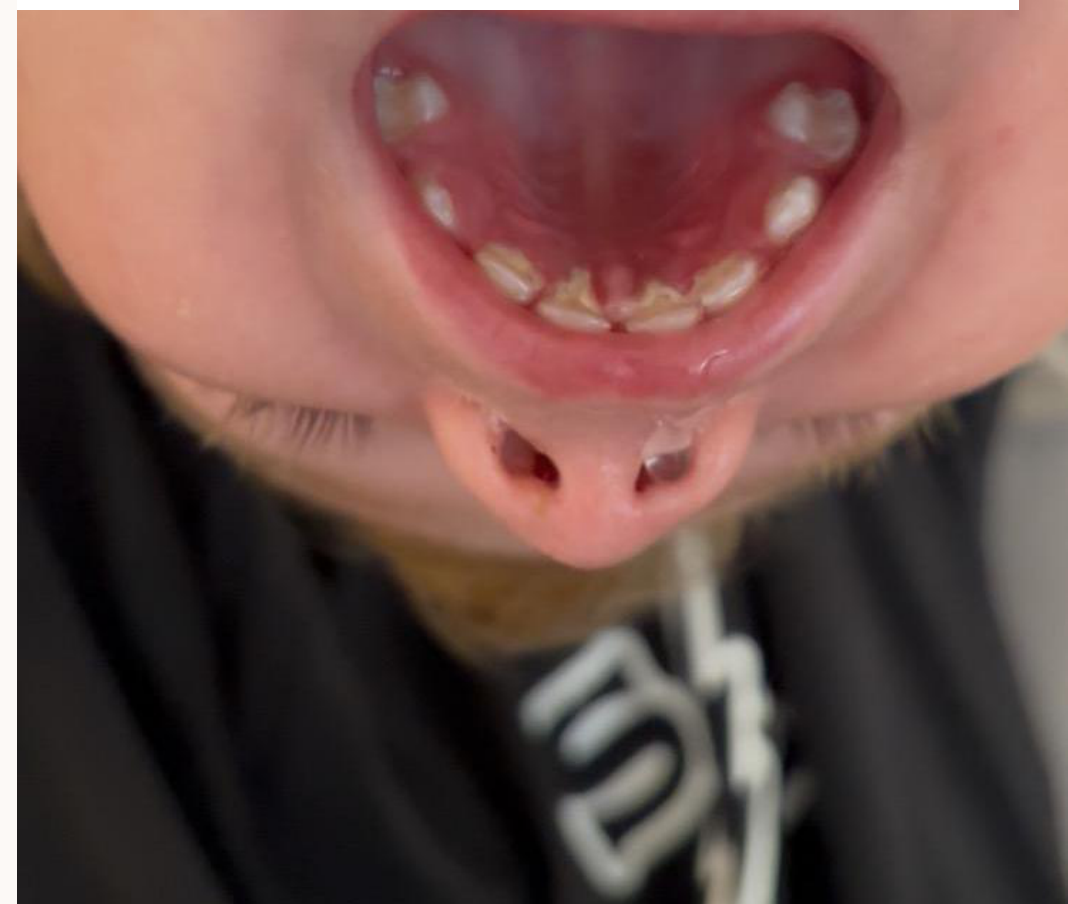
Oral Manifestations
- Oral pain and mild dysphagia
- Stomatitis (General inflammatory pattern)
- Appearance of intraepithelial fluid-filled vesicles (Typically starts as multiple small vesicles and ulcers that may eventually coalesce)
- Painful, enlarged gingiva (Generally red gingival tissues)
- Erosions of the free gingival margin
- Sloughing: White areas of necrotic gingiva, particularly around palatal surfaces.
Transmission and Disease Course
Disease Progression3
- Incubation Time: 3-5 days (Usually a couple of days)
- Initial Presentation: 48-hour history of irritability, pyrexia, and malaise
- ==Prodromal Phase: 24 to 48 hours of fever before ulcers appear.==
- Course of Disease: Self-limiting; typically heals within 10-14 days
- ==Follow-up: If symptoms do not improve or resolve within 14 days, the patient should re-present.==
- ==Recurrence: Patients may experience secondary presentations (recurrence) later.==

Transmission
- Direct contact with active lesions
- Contact with infected oral secretions
- ==Risk Factors: Children of this age frequently put hands in their mouths and touch objects.==
- ==Isolation: Infected children should not attend daycare, kindergarten, or playgroups due to the infectious nature of the virus.==
Management and Analgesia
Symptomatic Care4
- Maintain intake of oral fluids (Hydration with water is critical)
- Bed rest
- Soft diet (e.g., ice cream) (Soft, cold foods are soothing and easier to swallow)
- ==Topical Care:==
- ==Chlorhexidine Gel: Applying with a swab twice a day can keep the area clean and prevent secondary bacterial infection, though it does not speed up viral healing.==
- ==Avoid Topical Anesthetics: Teething gels (lidocaine/benzocaine) are not recommended for children under six due to the risk of methemoglobinemia and the difficulty in controlling ingestion/dosage.==

Pharmacological Management
- Analgesia calculation based on patient weight (12kg)
- ==Antivirals (Acyclovir):==
- Limited evidence for use in healthy children under 2 years old.
- Primarily reserved for immunocompromised patients.
- Must be administered within the first 72–96 hours to be effective; once the virus has replicated, they are of little use.
- ==Antipyretics/Analgesics: Paracetamol is used to manage fever and pain.==
Dosage Calculation for 12kg Patient
Paracetamol Dosage:
- Standard Dose: 15mg/kg every 4-6 hours
- Maximum Limits: 1g per dose, 4g per day (Caution must be taken not to exceed the daily maximum dose)
- Calculation: 15mg x 12kg = 180mg every 4-6 hours
Administration (Panadol 1-5yrs Suspension):
- Concentration: 24mg/ml
- Volume Calculation: 180mg / 24mg/ml = 7.5ml every 4-6 hours
- ==Note: Volume (mL) varies depending on the specific product concentration (e.g., different age-specific formulations).==
 |  |
 |  |
: Original PDF page 1: W2 Case Based Discussion 2, p.1 : Original PDF page 2: W2 Case Based Discussion 2, p.2 : Original PDF page 3: W2 Case Based Discussion 2, p.3 : Original PDF page 4: W2 Case Based Discussion 2, p.4 : Original PDF page 5: W2 Case Based Discussion 2, p.5 : Original PDF page 6: W2 Case Based Discussion 2, p.6 : Original PDF page 7: W2 Case Based Discussion 2, p.7 : Original PDF page 8: W2 Case Based Discussion 2, p.8 : Original PDF page 9: W2 Case Based Discussion 2, p.9 : Original PDF page 10: W2 Case Based Discussion 2, p.10 : Original PDF page 11: W2 Case Based Discussion 2, p.11 : Original PDF page 12: W2 Case Based Discussion 2, p.12 : Original PDF page 13: W2 Case Based Discussion 2, p.13 : Original PDF page 14: W2 Case Based Discussion 2, p.14 : Original PDF page 15: W2 Case Based Discussion 2, p.15 : Original PDF page 16: W2 Case Based Discussion 2, p.16 : Original PDF page 17: W2 Case Based Discussion 2, p.17 : Original PDF page 18: W2 Case Based Discussion 2, p.18 : Original PDF page 19: W2 Case Based Discussion 2, p.19 : Original PDF page 20: W2 Case Based Discussion 2, p.20 : Original PDF page 21: W2 Case Based Discussion 2, p.21 : Original PDF page 22: W2 Case Based Discussion 2, p.22 : Original PDF page 23: W2 Case Based Discussion 2, p.23 : Original PDF page 24: W2 Case Based Discussion 2, p.24 : Original PDF page 25: W2 Case Based Discussion 2, p.25 : Original PDF page 26: W2 Case Based Discussion 2, p.26 : Original PDF page 27: W2 Case Based Discussion 2, p.27 : Original PDF page 28: W2 Case Based Discussion 2, p.28 : Original PDF page 29: W2 Case Based Discussion 2, p.29 : Original PDF page 30: W2 Case Based Discussion 2, p.30 : Original PDF page 31: W2 Case Based Discussion 2, p.31 : Original PDF page 32: W2 Case Based Discussion 2, p.32 : Original PDF page 33: W2 Case Based Discussion 2, p.33 : Original PDF page 34: W2 Case Based Discussion 2, p.34 : Original PDF page 35: W2 Case Based Discussion 2, p.35 : Original PDF page 36: W2 Case Based Discussion 2, p.36 : Original PDF page 37: W2 Case Based Discussion 2, p.37 : Original PDF page 38: W2 Case Based Discussion 2, p.38 : Original PDF page 39: W2 Case Based Discussion 2, p.39