Case 2: Dental Infection and Extraction
Patient Presentation1
- 5.5-year-old boy
- Presented to surgery this afternoon
- Lower right-hand-side submandibular swelling started this morning
- Lecturer noted: Parents report the child has never seen a dentist before.
Medical and Dental History2
- Medically fit and well, immunised
- History of chronic nocturnal pain
- Worsened over past few days
- Managing with analgesia
- No previous swellings or history of trauma
- No prior dental treatment
Clinical Considerations
- Questions for parents?
- Initial investigations before looking in mouth?
- ==Facial Swelling Dynamics: Swellings can occur very quickly if an infection is not draining and tracks into the soft tissue. A child may be fine or have minor pain the night before, and the face may “blow up” by the following morning.==
- ==Systemic Involvement: It is critical to determine if the infection is localized or showing systemic signs.==
- ==Fever: The most common systemic sign.==
- ==General Malaise: The patient may appear miserable, tired, withdrawn, or “off.”==
Initial Investigation and Findings
- ==Vaccination Status: Necessary to rule out conditions like Mumps, which usually presents as bilateral swelling but can be unilateral.==
- ==Pain History Details:==
- Type of pain (lingering vs. non-lingering).
- Location (swelling on one side does not rule out a painful tooth on the contralateral side).
- Aggravating/Relieving factors.
- ==Analgesia Use: Determine if the parents have already been administering pain relief.==
Clinical Findings
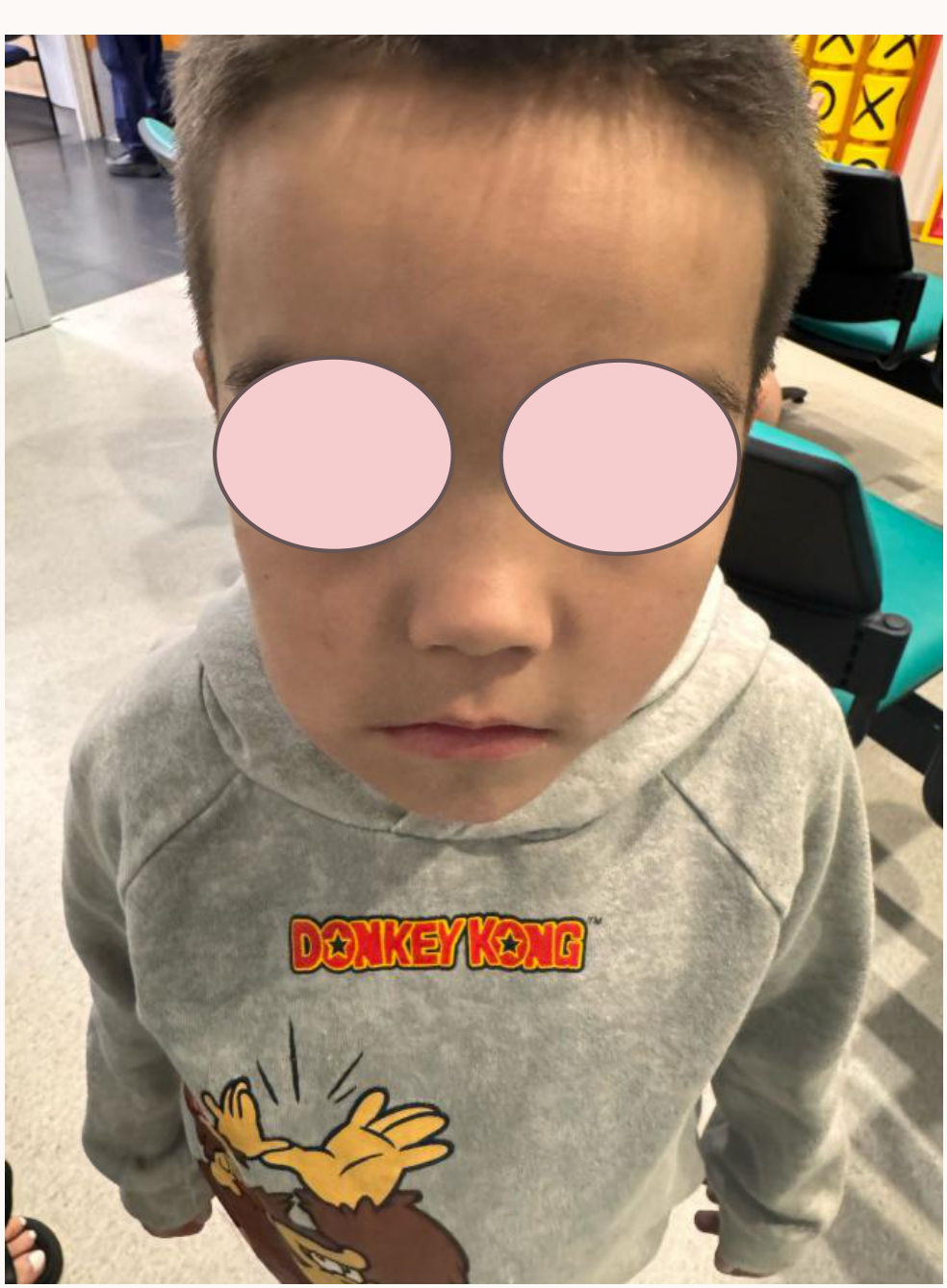
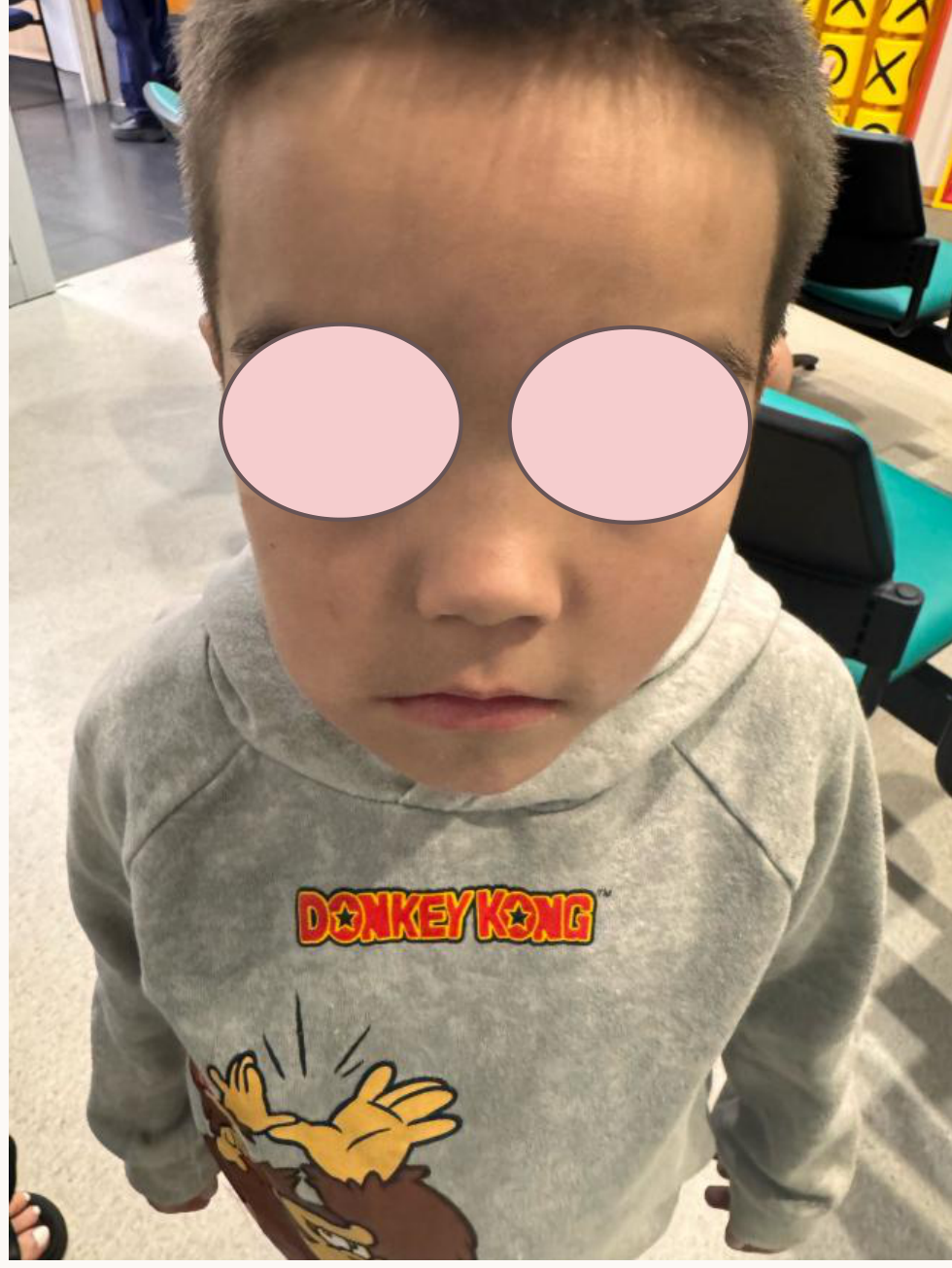
- Temperature: 38.5 degrees C
- Firm tender swelling localised to lower RHS
- Weight: 18kg
- ==Extraoral Examination:==
- ==Palpation: Firm, tender swelling localized to the lower right-hand side (submandibular).==
- ==Location: Submandibular swelling around the angle of the mandible or underneath is typically associated with lower teeth (as opposed to buccal swelling, which is often maxillary).==
- ==Visual: Overlying redness from inflammation may be present.==
- ==Temperature: Vital to check for fever to assess systemic spread.==
Intraoral Examination3
- Early mixed dentition
- 46, 85, 84 visible
- Large cavity with debris present at 85DO
- Loss of Q4 buccal sulcular depth
- ==Soft Tissue: The sulcus may look swollen or feel full upon palpation due to underlying inflammation or localized infection.==
Diagnostic and Management Planning
- Possible causes of 85 cavity?
- What will you see on an x-ray?
- Plan for today’s management
- Calculate dosages of any medications used (18kg)
Differential Diagnosis for 85 Cavity4
- HSPM (Hypomineralised Second Primary Molar)
- Note: If a child has HSPM, they have a 2.4 to 10 times higher chance of having similar defects in the permanent dentition.
- Dental caries
- Likely an occlusal lesion that has spread.
- Note: Contact point caries is less likely as the 46s have not been erupted long enough for significant progression.
- Failed existing restoration
- A previous filling that has fallen out.
- Trauma (fracture)
- Consideration of MIH (Molar Incisor Hypomineralisation) if HSPM is present
- ==Secondary Caries: Caries secondary to an enamel defect or breakdown.==

Radiographic Examination
Radiographic Modalities5
- Size 0 bitewing: Preferred if the child can tolerate it.
- OPG: An option if the child is uncooperative due to pain, though it provides less detail.
- Vertical bitewing
- PA with parent holding film: A PA can be taken with the parent holding the film (using a "carrot" technique) so the child does not have to bite down on a sore area.
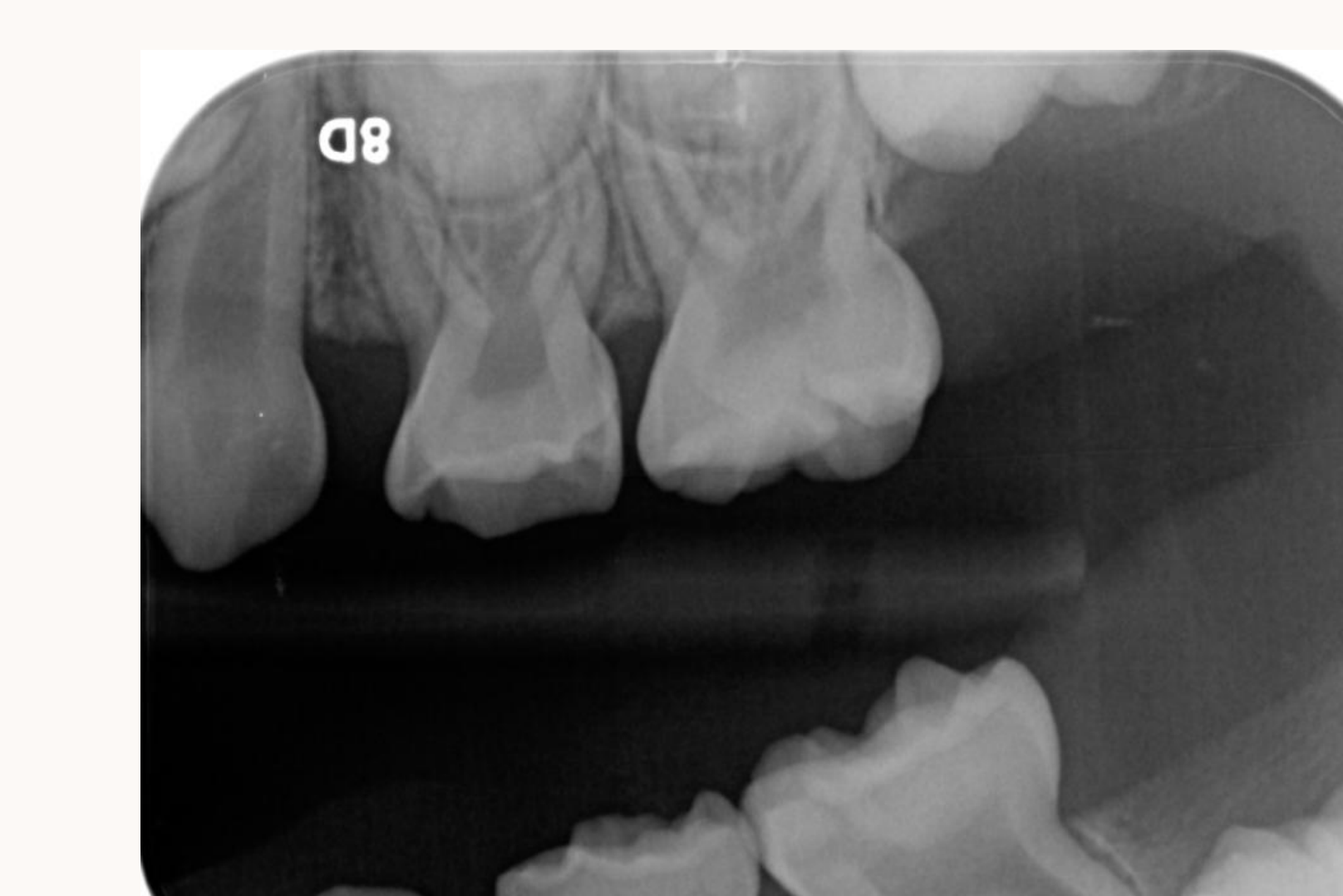
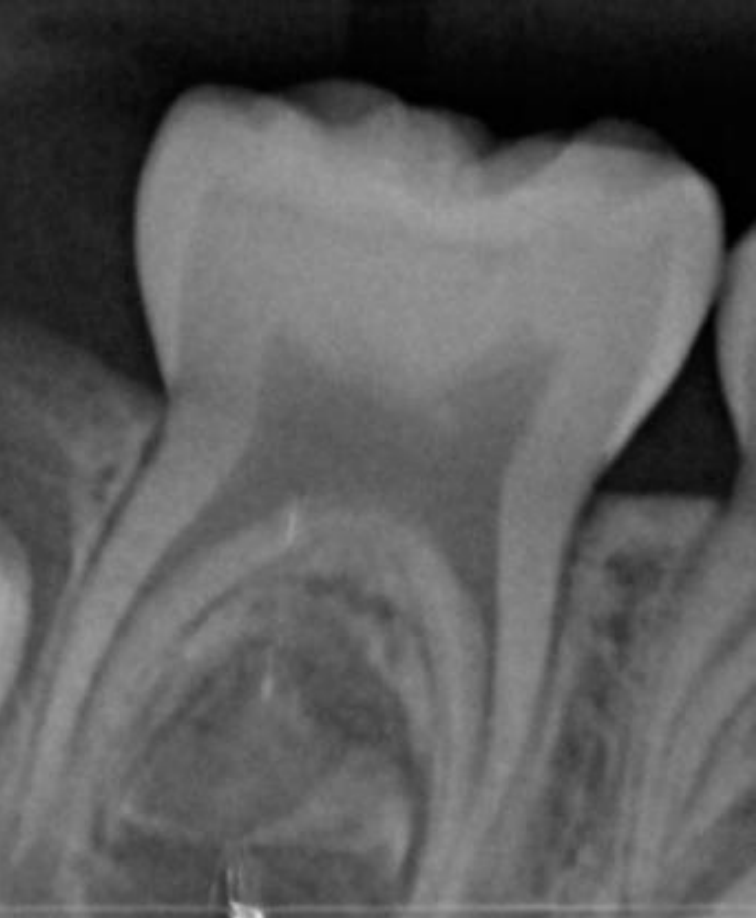
Radiographic Findings
- Cavity extending to pulp
- Furcation radiolucency
- In primary molars, signs of infection are most likely seen in the furcation region rather than the apex due to numerous accessory canals.
- Accessory canals in furcation area
- ==Comparison: To confirm a lucency, compare the area to the contralateral side or the opposing arch to observe differences in bony trabecular patterns and the PDL space.==
Pharmacological Management
Penicillin V Dosage
Dosage Calculation (18kg Patient)
- Recommended Dose: 12.5mg/kg (up to 500mg) orally every 6 hours for 5 days
- Standard range: 12.5 mg/kg to 17.5 mg/kg.
- Calculation: 12.5mg x 18kg = 225mg
- Preparation: Oral suspension 150mg/5ml
- Administration: 7.5ml every 6 hours for 5 days
Metronidazole Dosage6
Dosage Calculation (18kg Patient)
-
Recommended Dose: 10mg/kg (up to 400mg) orally every 12 hours for 5 days
-
Calculation: 10mg x 18kg = 180mg
-
Preparation: Oral suspension 40mg/ml (equivalent to 200mg/5ml)
-
Administration: 4.5ml every 12 hours for 5 days
-
Recommended Dose: 10mg/kg (up to 400mg) orally every 12 hours for 5 days
-
Calculation: 10mg x 18kg = 180mg
-
Preparation: Oral suspension 40mg/ml (equivalent to 200mg/5ml)
-
Administration: 4.5ml every 12 hours for 5 days
Prescription Documentation
Prescription Details
- Patient: Riley Child (DOB: 2/1/2020, Weight: 18kg)
- Address: 12 Macarena Place, Claremont WA 6010
- Date: 1/1/2025
- Prescriber: Dr Senior Student DMD (Prescriber no. 11094567)
- Instructions must include the specific milligram dose, volume (ml), frequency, and duration.
Medications Prescribed
- Penicillin V oral suspension
- Concentration: 150mg/5ml (200ml bottle)
- Instructions: Take 7.5ml orally every 6 hours for 5 days.
- Metronidazole oral suspension
- Concentration: 40mg/ml (200ml bottle)
- Instructions: Take 4.5ml every 12 hours for 5 days.
- Note: For dental treatment only.
- ==Antibiotics: Combination of Penicillin V and Metronidazole per current guidelines.==
- ==Analgesia: Paracetamol and Ibuprofen can be used together for better pain relief; Ibuprofen provides anti-inflammatory effects.==
Extraction Appointment Preparation
Immediate Symptom Management7
- Analgesia:
- Paracetamol: 15mg/kg, 4-6 hourly (max 4000mg/day)
- Ibuprofen: 10mg/kg, 6-8 hourly (max 2500mg/day)
- Dietary Advice: Soft diet
- ==Antibiotic Delay: If the environment is too acidic due to infection, local anesthetic (LA) will be less effective. In non-systemic cases, antibiotics can be started first, with the extraction booked for 5 days later at “peak effectiveness.”==
Emergency and Follow-up Protocols
- If symptoms worsen:
- Contact clinic immediately.
- Provide referral letter to PCH Dental. Call PCH Dental before the patient leaves the surgery.
- After hours: Attend PCH Emergency Department (ED).
- Scheduled Treatment: Book for extraction of 85 in approximately 1 week.
- ==Hospital Referral (PCH/Local Hospital): Justified if there is significant swelling, fever, or systemic signs.==
- ==Regional Management: In rural areas, patients may be sent to a local hospital for IV antibiotics or flown to PCH via the Royal Flying Doctor Service.==
- ==Referral Protocol: Always call the hospital dental team first. Advise the patient on fasting status if surgery is imminent. Calling ahead allows the patient to be listed as “expected,” reducing wait times in the Emergency Department.==
Local Anesthetic Techniques
Topical Anesthesia Protocol
- Agent: Topical lignocaine gel 2-5%
- Procedure:
- Dry surface
- Apply with cotton bud
- Leave in situ for 2 minutes
- Wipe away with damp gauze
Injection Technique
- Buccal and lingual infiltration (access lingual via interpapillary route)
- ==Effectiveness: LA is less effective in the presence of infection due to the acidic environment.==
Anatomical Considerations for Nerve Blocks
Pediatric vs. Adult Mandibular Anatomy
- Ramus is shorter vertically in children.
- Ramus is narrower anterio-posteriorly in children.
Local Anesthetic Agent Selection
- Primary Choice: 4% Articaine with adrenaline 1:100,000
- Rationale: More effective mandibular infiltration and short acting time.
- Alternative Choice: 2% Lignocaine with adrenaline 1:80,000
- Considerations: Acidic environment from infection may result in shorter acting time and require longer onset time.
Maximum Local Anesthetic Dose Calculation
Dosage Calculation for 4% Articaine (1:100,000)
- Patient Weight: 18kg
- Maximum safe dose calculation: 7mg/kg x 18kg = 126mg (Note: text indicates 146mg, but calculation 7x18 equals 126mg)
- Concentration: 4% Articaine = 40mg/ml
- Volume Limit: 126mg / 40mg/ml = 3.15ml
- Cartridge Limit: 3.15ml / 2.2ml = 1.4 carpules
Surgical Procedure and Instrumentation89
 |  |  |
 |  |  |
Surgical Instruments10
-
Forceps: Lower baby hawks
-
Luxators: 3S or 3C luxator
-
Forceps: Lower baby hawks
-
Luxators: 3S or 3C luxator
 |  |
Extraction Technique11
- Luxator Use: Wedge around the tooth to separate PDL fibres; drive gently in an apical direction.
- Forceps Technique:
- Engage molar beaks at the furcation area.
- Apply apical pressure (primary drive).
- Move lingually.
- Apply continuous buccal movement.
- Remove tooth towards the buccal aspect.
- The tooth (85) requires extraction once the infection is managed or if emergency intervention is required.
Post-Extraction Care
Immediate Post-Operative Steps12
- Irrigate with saline to rinse out pus.
- Apply digital pressure to compress socket walls.
- Have patient bite on sterile gauze to achieve haemostasis.
- Suture soft tissues if required.
Follow-up and Records131415161718123451920621722232425108911122627282930313233343536373839
- Provide verbal and written post-operative instructions.
- Complete clinical documentation.
: Original PDF page 1: W2 Case Based Discussion 2, p.1 : Original PDF page 2: W2 Case Based Discussion 2, p.2 : Original PDF page 3: W2 Case Based Discussion 2, p.3 : Original PDF page 4: W2 Case Based Discussion 2, p.4 : Original PDF page 5: W2 Case Based Discussion 2, p.5 : Original PDF page 6: W2 Case Based Discussion 2, p.6 : Original PDF page 7: W2 Case Based Discussion 2, p.7 : Original PDF page 8: W2 Case Based Discussion 2, p.8 : Original PDF page 9: W2 Case Based Discussion 2, p.9 : Original PDF page 10: W2 Case Based Discussion 2, p.10 : Original PDF page 11: W2 Case Based Discussion 2, p.11 : Original PDF page 12: W2 Case Based Discussion 2, p.12 : Original PDF page 13: W2 Case Based Discussion 2, p.13 : Original PDF page 14: W2 Case Based Discussion 2, p.14 : Original PDF page 15: W2 Case Based Discussion 2, p.15 : Original PDF page 16: W2 Case Based Discussion 2, p.16 : Original PDF page 17: W2 Case Based Discussion 2, p.17 : Original PDF page 18: W2 Case Based Discussion 2, p.18 : Original PDF page 19: W2 Case Based Discussion 2, p.19 : Original PDF page 20: W2 Case Based Discussion 2, p.20 : Original PDF page 21: W2 Case Based Discussion 2, p.21 : Original PDF page 22: W2 Case Based Discussion 2, p.22 : Original PDF page 23: W2 Case Based Discussion 2, p.23 : Original PDF page 24: W2 Case Based Discussion 2, p.24 : Original PDF page 25: W2 Case Based Discussion 2, p.25 : Original PDF page 26: W2 Case Based Discussion 2, p.26 : Original PDF page 27: W2 Case Based Discussion 2, p.27 : Original PDF page 28: W2 Case Based Discussion 2, p.28 : Original PDF page 29: W2 Case Based Discussion 2, p.29 : Original PDF page 30: W2 Case Based Discussion 2, p.30 : Original PDF page 31: W2 Case Based Discussion 2, p.31 : Original PDF page 32: W2 Case Based Discussion 2, p.32 : Original PDF page 33: W2 Case Based Discussion 2, p.33 : Original PDF page 34: W2 Case Based Discussion 2, p.34 : Original PDF page 35: W2 Case Based Discussion 2, p.35 : Original PDF page 36: W2 Case Based Discussion 2, p.36 : Original PDF page 37: W2 Case Based Discussion 2, p.37 : Original PDF page 38: W2 Case Based Discussion 2, p.38 : Original PDF page 39: W2 Case Based Discussion 2, p.39
Footnotes
-
Original PDF page 1 ↩
-
Original PDF page 2 ↩
-
Original PDF page 3 ↩
-
Original PDF page 4 ↩
-
Original PDF page 5 ↩
-
Original PDF page 6 ↩
-
Original PDF page 12 ↩
-
Original PDF page 13 ↩
-
Original PDF page 15 ↩
-
Original PDF page 17 ↩
-
Original PDF page 18 ↩
-
Original PDF page 19 ↩
-
Original PDF page 20 ↩
-
Original PDF page 26 ↩
-
Original PDF page 27 ↩
-
Original PDF page 28 ↩
-
Original PDF page 29 ↩
-
Original PDF page 30 ↩
-
Original PDF page 31 ↩
-
Original PDF page 32 ↩
-
Original PDF page 33 ↩
-
Original PDF page 34 ↩
-
Original PDF page 35 ↩
-
Original PDF page 36 ↩
-
Original PDF page 37 ↩
-
Original PDF page 38 ↩
-
Original PDF page 39 ↩