Introduction to Periodontal Surgery1
Presented by Amelia Hemmati

Key References
Primary Textbooks and Resources2
- Lindhe’s Clinical Periodontology and Implant Dentistry, Seventh Edition, Volume 1
- Recommended for in-depth theoretical foundations.
- Newman and Carranza’s Clinical Periodontology and Implantology, 14th Edition
- A primary resource for detailed step-by-step surgical procedures.
- **Periodontology at a Glance
- EFP (European Federation of Periodontology) Clinical Practice Guidelines: Essential for evidence-based protocols and exam preparation.
- AAP (American Academy of Periodontology) Consensus Reports: Used for clinical standards and long-term stability data.**
 |  |
 |
Image Credits
All images contained within this presentation are sourced from the references listed above or are clinical photographs of my own patients, unless otherwise specified.
Additional Visual Resources
Visual aids and PDF documents are available on the EFP website, providing clinical visuals for each step of therapy.
Core Topics in Periodontal Surgery3
- Definition
- Objectives
- Indications
- Contraindications
- Steps of Periodontal Therapy
- Classification of Periodontal Surgical Procedures
- Including Resective, Regenerative, and Plastic procedures.
- Basic Surgical Principles
- Focusing on flap design, suturing, and healing.
- Biological Basis of Periodontal Surgery
- Complications
- Patient Communication and Consent
- Evidence-Based Perspective

Definition and Objectives
Definition of Periodontal Surgery4
Periodontal surgery refers to surgical procedures performed to:
- Arrest progression of periodontal disease
- Access root surfaces for debridement
- It involves creating an "open flap" to allow direct access to root surfaces for debridement.
- Reduce or eliminate periodontal pockets
- Regenerate lost periodontal tissues
- Improve aesthetics and function
It is typically indicated after completion of non-surgical periodontal therapy when residual pathology persists.
Primary and Secondary Objectives
Primary Objectives5
- Eliminate or reduce periodontal pockets
- Pocket Reduction/Elimination: Reducing deep pockets to a maintainable depth.
- Establish a maintainable periodontal environment
- Environmental Stability: Establishing a periodontal environment that the patient and clinician can effectively maintain.
- Arrest disease progression
- Disease Arrest: Stopping the progression of attachment loss.

Secondary Objectives
- Regenerate lost attachment apparatus
- Restoring lost attachment apparatus (bone, cementum, and PDL).
- Improve aesthetics
- Facilitate restorative/prosthodontic treatment
- Functional Support: Facilitating restorative or prosthodontic treatments (e.g., crown lengthening).
- Correct mucogingival defects
Clinical Indications and Contraindications
Indications for Surgery
- Residual pockets ≥5–6 mm with bleeding on probing after NSPT
- Infrabony (vertical) defects
- Class II furcation defects
- Grade III furcation defects that require specialized access
- Mucogingival defects (recession, lack of attached gingiva)
- Altered passive eruption
- Management of "gummy smiles" for aesthetic concerns
- Crown lengthening for restorative purposes
- Periodontal abscess not responding to non-surgical care
- Root surface irregularities (e.g., palatoradicular groove)
- Palato-radicular grooves are commonly found on maxillary lateral incisors
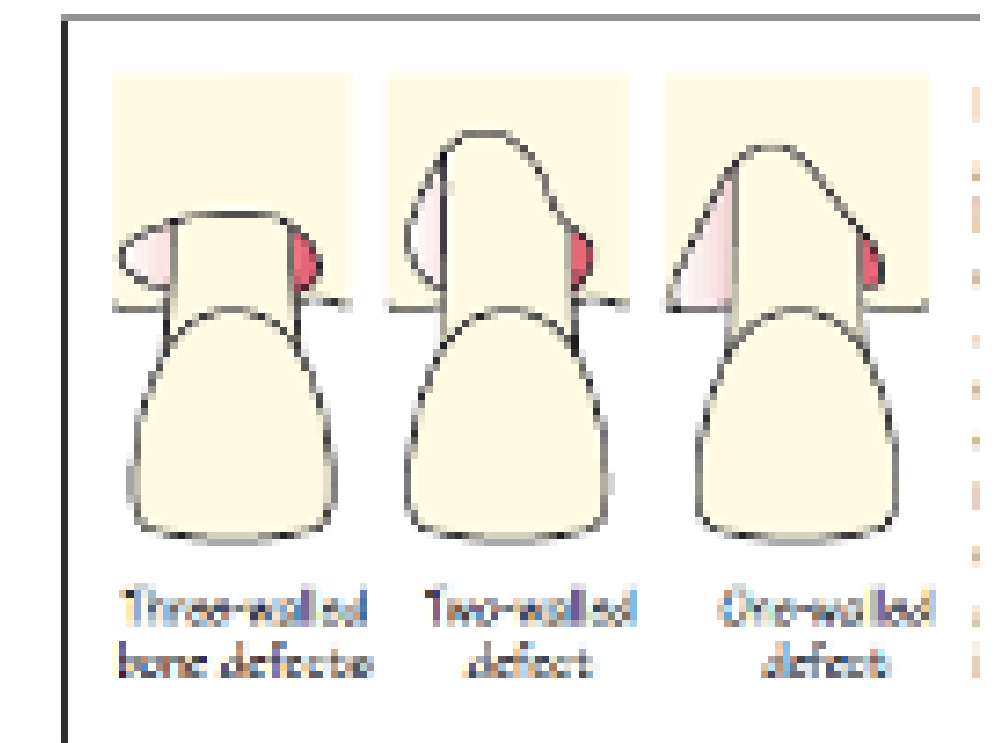
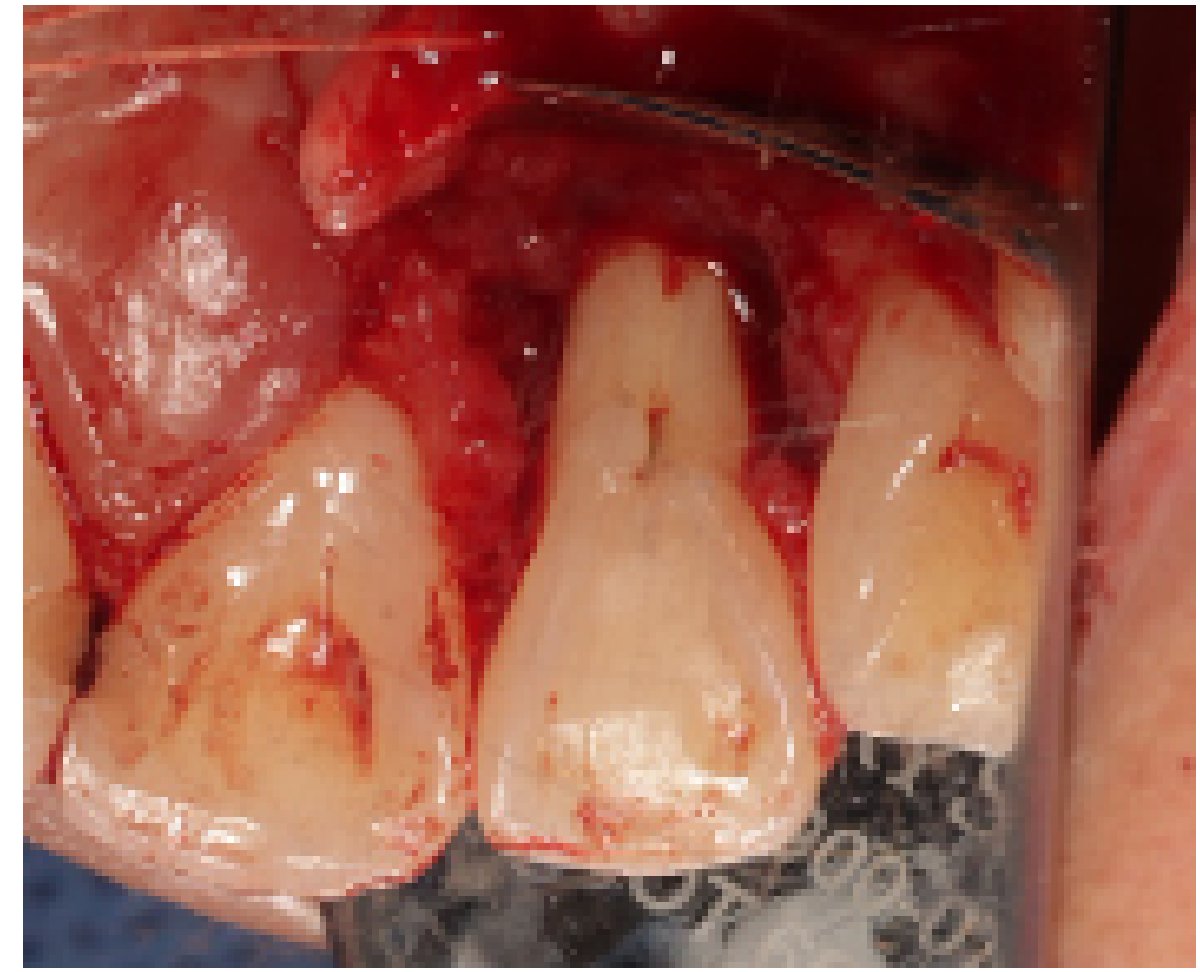
Anatomy of Bone Defects6
- Vertical and horizontal bone loss patterns
- Infrabony architecture
Healing Potential
Three-wall defects are considered the most favorable for healing and regenerative procedures due to better blood supply and clot stability.
 |  |
 |
Absolute and Relative Contraindications
Absolute Contraindications7
- Uncontrolled systemic disease (e.g., uncontrolled diabetes)
- Uncontrolled diabetes specifically leads to delayed wound healing
- Poor plaque control
- Non-compliant patient
 |  |
 |  |
Relative Contraindications
- Heavy smoking
- Heavy smokers experience significantly delayed healing and poorer outcomes
- Pregnancy (elective surgery deferred)
- Poor restorative prognosis
- Psychological limitations
Terminology Note
Steps 1 and 2 are collectively referred to as Non-surgical periodontal therapy (NSPT).
The Role of Surgery in Periodontal Therapy
Steps of Periodontal Therapy8
The EFP S3 Level Clinical Practice Guideline outlines a structured approach to therapy:
- Step 0: Prerequisite to Therapy
- Education, classification, diagnosis, risk assessment, and care planning.
- Step 1: Risk Factor Control
- Oral hygiene instruction (OHI), adjuncts for gingivitis, professional mechanical plaque removal (PMPR), and supra-gingival scaling.
- Step 2: Intervention
- Sub-gingival biofilm and calculus removal with or without adjuncts.
- Step 3: Evaluation of Non-Responders
- Re-evaluation of sites; consideration for repeated instrumentation or surgery.
- Step 4: Long-term Care
- Supportive periodontal care and rehabilitation planning.
 |  |
EFP Clinical Practice Guidelines for Step 3
Aim of Step 39
Treating sites not responding adequately to the second step of therapy to gain access to deep pocket sites, or aiming at regenerating or resecting lesions that add complexity (infrabony and furcation lesions).
 |  |
Clinical Indications
If periodontal pockets > 4 mm with bleeding on probing and/or deep pockets (≥ 6 mm) are still present at re-evaluation, options include:
- Repeated subgingival instrumentation with or without adjunctive therapies
- Access flap periodontal surgery
- Resective periodontal surgery
- Regenerative periodontal surgery
Endpoints of Success
- No periodontal pockets ≥ 5 mm with bleeding on probing
- No deep pockets (≥ 6 mm)
- Closed pockets (depths ≤ 4 mm without BOP)
- Absence of deep residual infection
Recommended Interventions
- Surgery should be performed by dentists with additional specific training or by specialists.
- In the presence of moderately deep residual pockets (4-5 mm), non-surgical subgingival instrumentation should be repeated.
Classification of Periodontal Surgical Procedures
Resective Surgery
Pocket Reduction Techniques10
- Pocket reduction surgery
- Osseous resective surgery
- Involves osseous resection and recontouring to create "positive architecture."
- Apically positioned flap
Clinical Consideration
This is less common today due to aesthetic concerns as it causes visible recession.
 |  |  |
 |  |
Furcation Management11
- Root resection
- Removing a single root (e.g., distobuccal root of a maxillary molar); requires prior endodontic treatment.
- Hemisection
- Splitting a mandibular molar into two separate "premolars."
- Furcation tunnelling
Risk Factor
Tunnelling increases susceptibility to root caries and sensitivity.
 |  |  |
 |  |
Tunnelling Approaches
- Adequate Keratinized Gingiva (KG): Scalloped incisions can be performed to expose the furcation area for self-performed cleaning.
- Reduced Keratinized Gingiva (KG): An apically repositioned flap is performed to preserve KG while exposing the furcation area.
Regenerative Surgery
Regenerative Modalities12
- Guided tissue regeneration (GTR)
- Bone grafting
- Enamel matrix derivative (Emdogain®)
- Biologics (e.g., growth factors)
- Aims for "True Regeneration": New bone, new cementum, and a functional periodontal ligament (PDL).
 |  |
 |
Enamel Matrix Derivative Procedure
- Surgical access to the site.
- Root surface conditioning with EDTA gel to remove the smear layer.
- Syringing Emdogain® gel directly onto washed roots.
- Because the gel is viscous, it is often mixed with a bone graft scaffold to keep it within the defect.
- Flap replacement.
- Flap replacement.
Guided Tissue Regeneration (GTR) Components
- Epithelium of replaced flap.
- Membrane placement to prevent epithelium and connective tissue from contacting the root surface.
- Promotion of cell migration from the periodontal ligament.
- Barrier membranes prevent fast-growing epithelial cells from migrating into the defect, allowing slower-growing bone and PDL cells to repopulate.
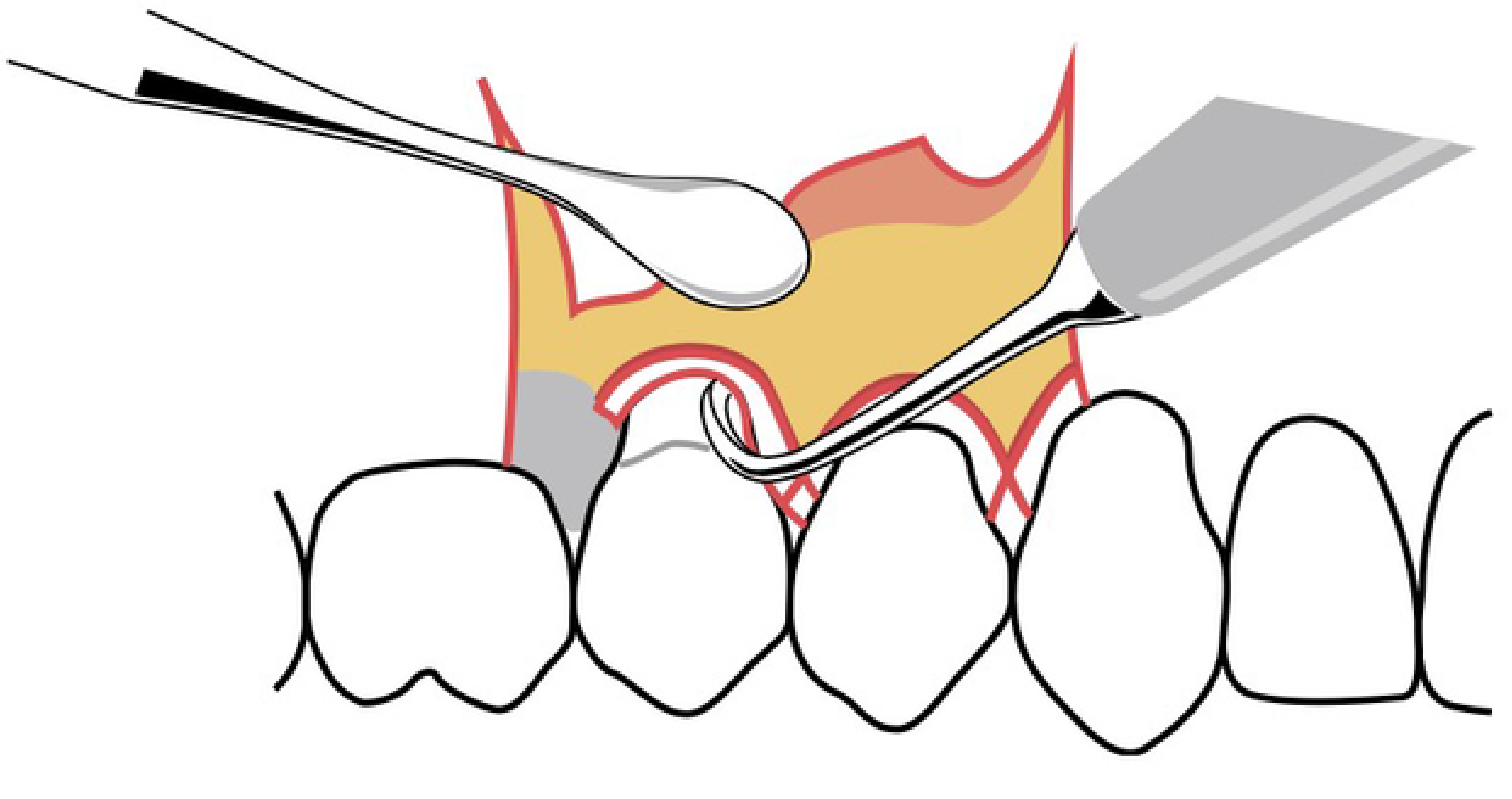
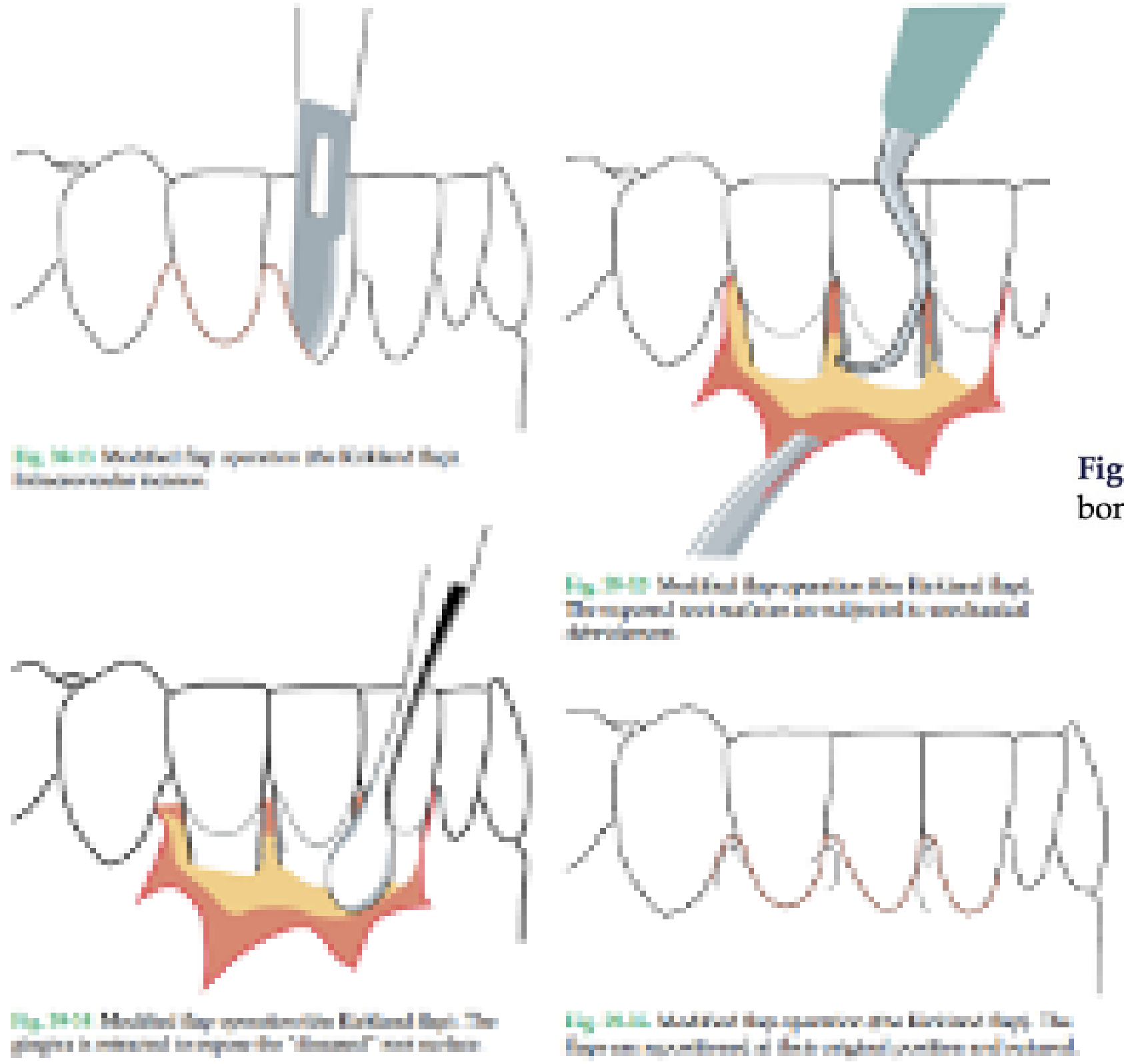
Access Flap Surgery
Techniques13
- Open Flap Debridement: Direct visualization and access for root surface cleaning.
- Modified Widman Flap: Facilitates instrumentation while minimizing tissue loss to maintain aesthetics.
 |  |
 |
Mucogingival and Plastic Surgery
Surgical Techniques14
- Coronally advanced flap
- Connective tissue graft
- Free gingival graft
- Tunnel technique
- A conservative, blunt-dissection approach that keeps the interdental papillae intact; no scalpel is used.
 |  |
 |
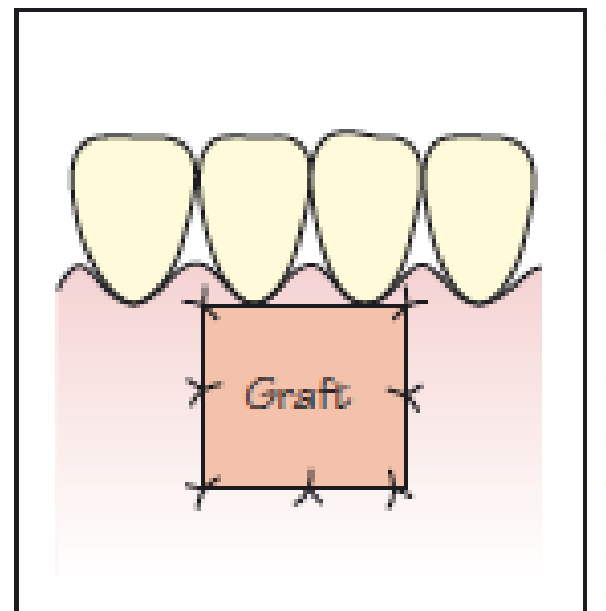
Grafting Procedures
-
Free Epithelialised Gingival Graft: Epithelium and outer connective tissue are removed from the recipient site via split dissection. The graft is harvested from a donor site and sutured.
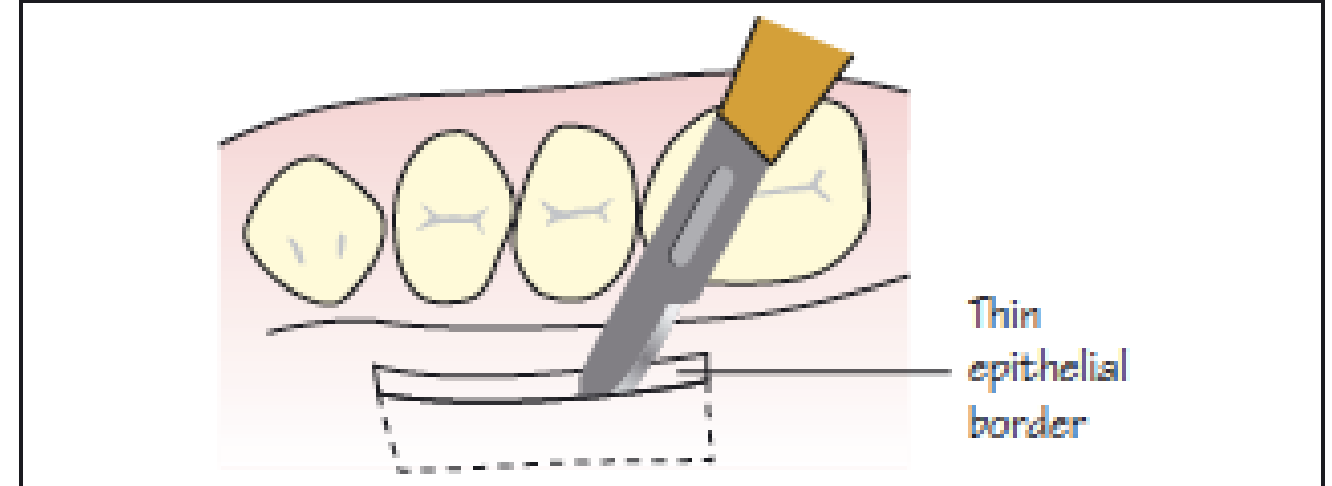
-
Subepithelial Connective Tissue Graft: Connective tissue is harvested from the palate with a thin epithelial border. It is sutured at the recipient site and covered by a flap (typically coronally advanced) for nutrition.
-
Alloderm: A commercial alternative derived from cadaver tissue, used when donor sites are limited or to avoid a second surgical site.
Crown Lengthening Surgery
Aesthetic Crown Lengthening15
Indicated for Altered Passive Eruption (APE). The procedure involves:
- Gingival margin measurement and demarcation.
- External bevel incision following CEJ anatomy.
- Gingival margin removal and contour finalization.
- Full-thickness flap elevation.
- Ostectomy and osteoplasty using burs to establish proper supracrestal tissue attachment.
- Suturing and ancillary procedures (e.g., labial frenectomy).

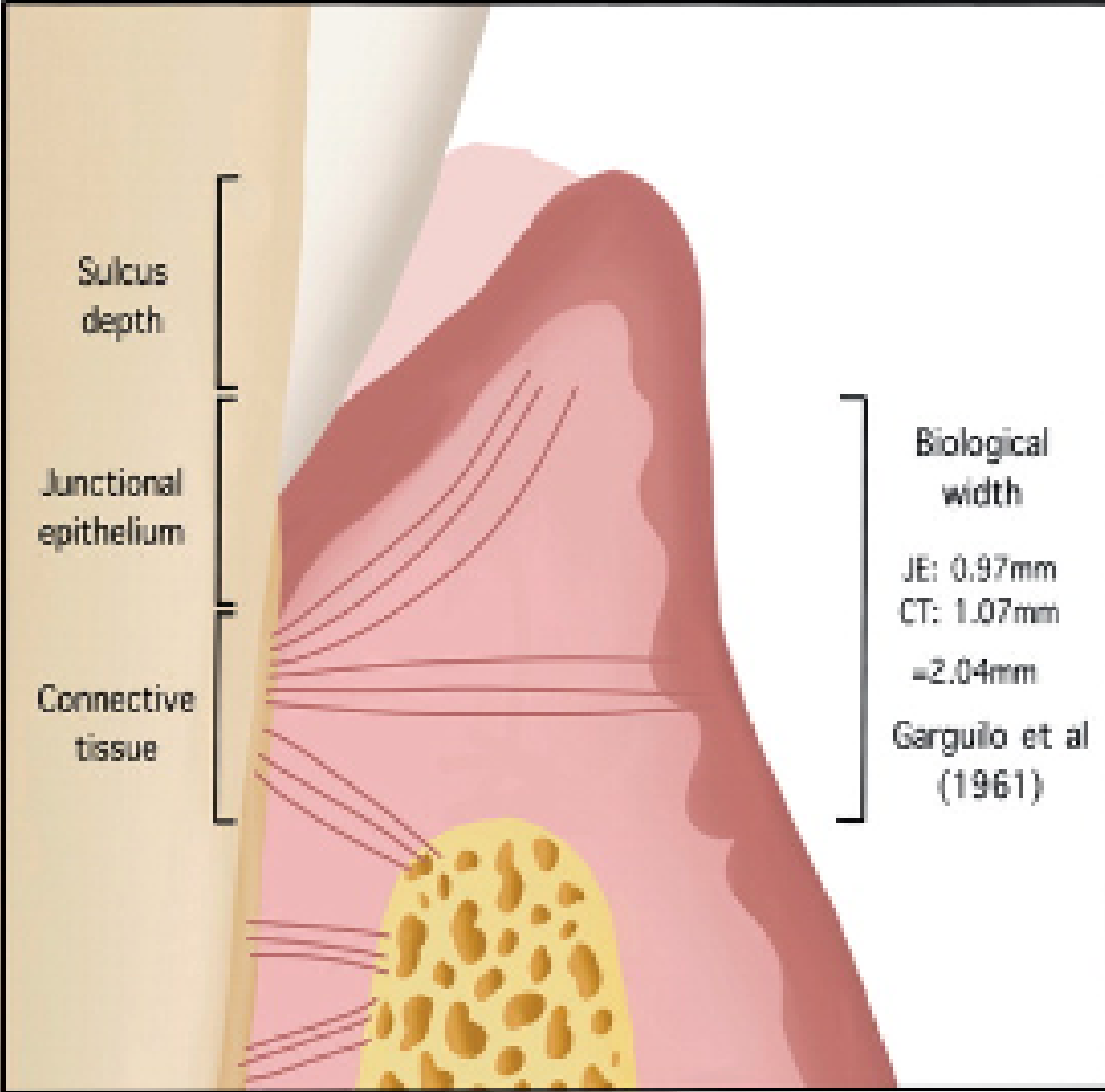
Functional Crown Lengthening16
- Surgical exposure for restorative margin placement.
- Management of supracrestal tissue attachment (formerly biological width) to ensure restorative margins do not compromise periodontal health.
 |  |
 |
Basic Surgical Principles
Patient Selection and Asepsis
Patient Selection Criteria17
- Stable systemic health.
- High level of plaque control (ideally <20% plaque score).
 |  |
Aseptic Protocols18
- Use of sterile instruments.
- Proper patient and surgical field draping.
- Pre-operative chlorhexidine rinse to reduce microbial load.

Flap Design and Incision Techniques
Flap Design Principles19
- Blood Supply: Flaps should be wider at the base to ensure adequate vascularity.
- Access: Ensure sufficient visibility of the underlying bone and root surfaces.
- Tearing the mucosa due to a small flap is a common error; ensure the flap is wide enough for access.
- Closure: Design allows for tension-free suturing.
- Papillary Integrity: Respect the interdental papilla to prevent recession and aesthetic defects.
- Preserve the interdental papilla as it is difficult to reconstruct once lost.

Incision Types
- Sulcular/Crevicular incisions.
- Vertical releasing incisions for apical access.
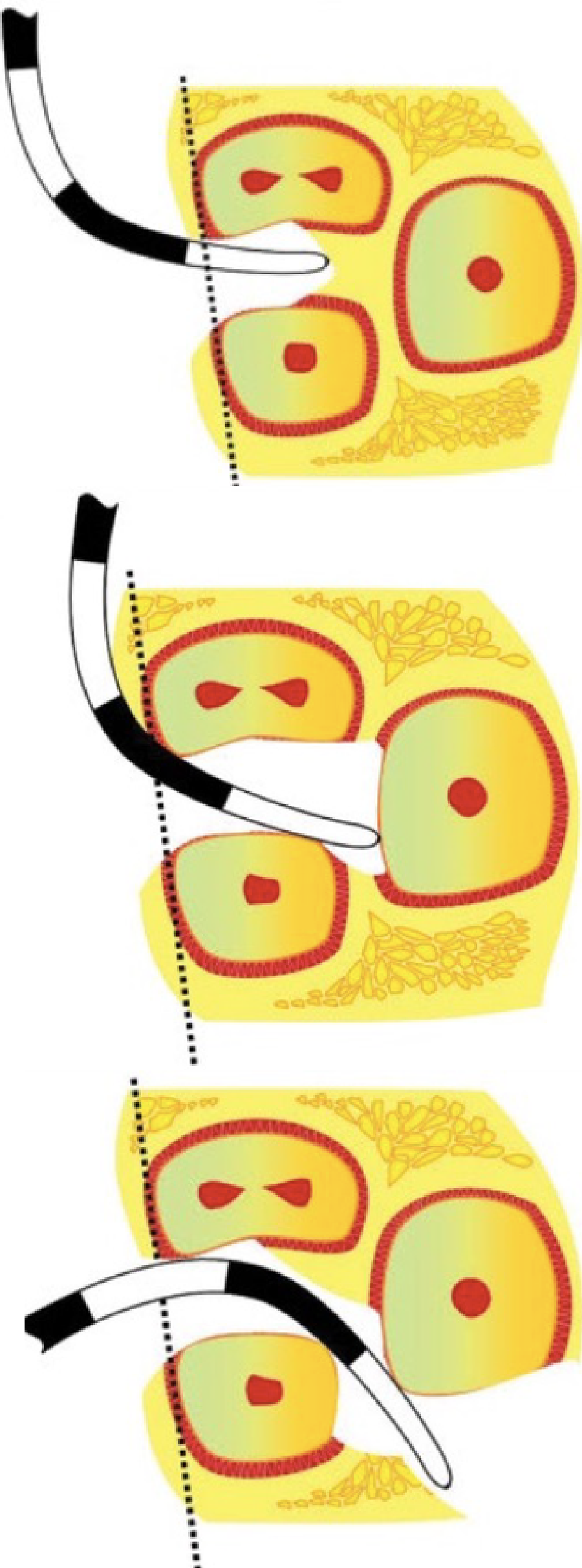
Surgical Incision Sequence20
- Internal Bevel Incision: The initial incision to remove the pocket lining and conserve gingiva.
- Crevicular Incision: Performed from the base of the pocket to the bone crest to release the tissue.
- Interdental Incision: Used to separate the collar of tissue from the interproximal areas
- Reflection of the flap: Gentle reflection to minimize trauma.
- Debridement/Treatment.
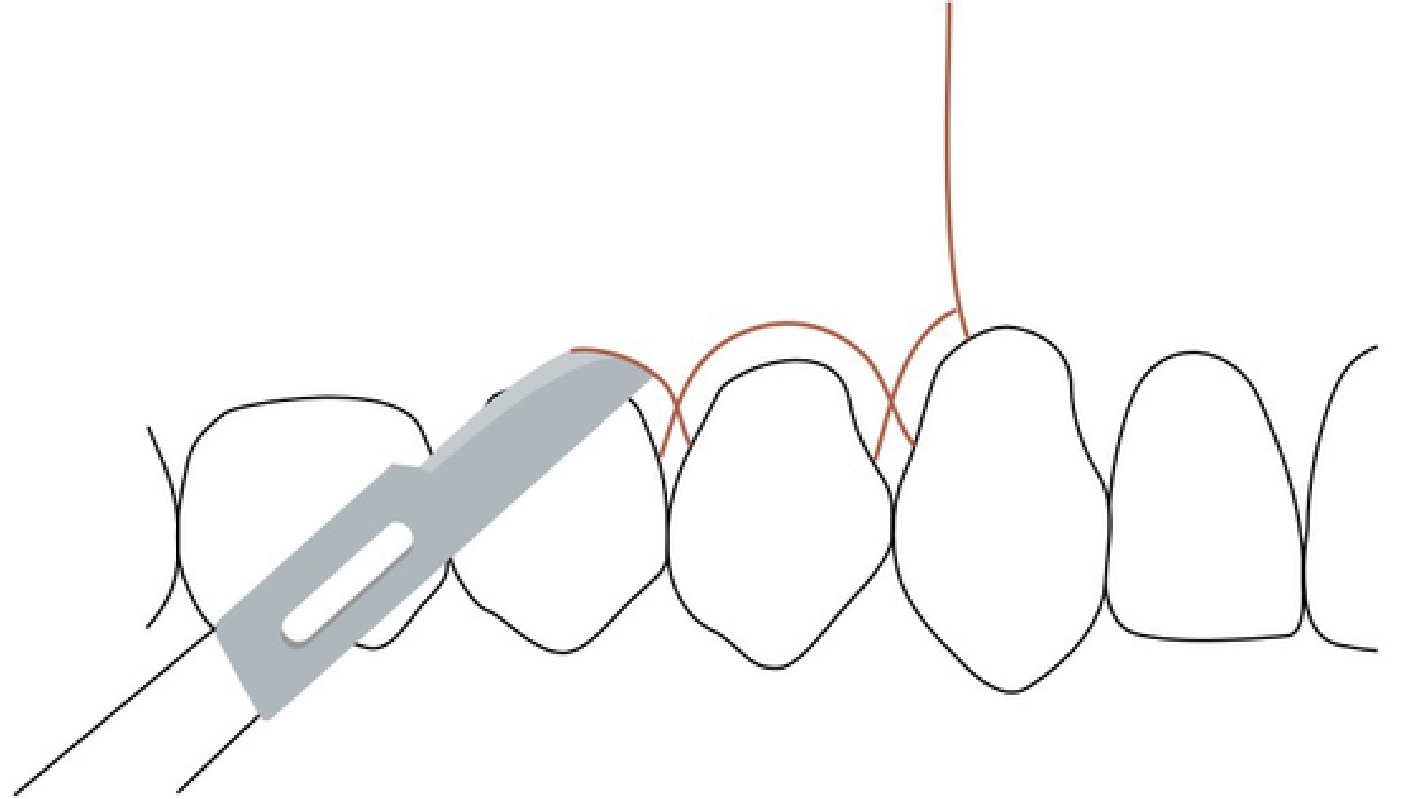
- Suturing: Simple interrupted, Horizontal mattress, or Vertical mattress. .

Footnotes
-
Original PDF page 1: L1 Introduction to Periodontal Surgery, p.1 ↩
-
Original PDF page 2: L1 Introduction to Periodontal Surgery, p.2 ↩
-
Original PDF page 3: L1 Introduction to Periodontal Surgery, p.3 ↩
-
Original PDF page 4: L1 Introduction to Periodontal Surgery, p.4 ↩
-
Original PDF page 5: L1 Introduction to Periodontal Surgery, p.5 ↩
-
Original PDF page 6: L1 Introduction to Periodontal Surgery, p.6 ↩
-
Original PDF page 7: L1 Introduction to Periodontal Surgery, p.7 ↩
-
Original PDF page 8: L1 Introduction to Periodontal Surgery, p.8 ↩
-
Original PDF page 9: L1 Introduction to Periodontal Surgery, p.9 ↩
-
Original PDF page 10: L1 Introduction to Periodontal Surgery, p.10 ↩
-
Original PDF page 11: L1 Introduction to Periodontal Surgery, p.11 ↩
-
Original PDF page 12: L1 Introduction to Periodontal Surgery, p.12 ↩
-
Original PDF page 13: L1 Introduction to Periodontal Surgery, p.13 ↩
-
Original PDF page 14: L1 Introduction to Periodontal Surgery, p.14 ↩
-
Original PDF page 15: L1 Introduction to Periodontal Surgery, p.15 ↩
-
Original PDF page 16: L1 Introduction to Periodontal Surgery, p.16 ↩
-
Original PDF page 17: L1 Introduction to Periodontal Surgery, p.17 ↩
-
Original PDF page 18: L1 Introduction to Periodontal Surgery, p.18 ↩
-
Original PDF page 19: L1 Introduction to Periodontal Surgery, p.19 ↩
-
Original PDF page 20: L1 Introduction to Periodontal Surgery, p.20 ↩