Gingival Recession and Gingival Overgrowth
Clinical Perspective
Gingival recession is primarily a soft tissue issue rather than a hard tissue problem. Its management and the predictability of surgical outcomes are heavily dependent on the level of interproximal attachment.
Amelia Hemmati
Presentation Overview1
- Gingival Recession
- Gingival Overgrowth
Key References2
- Gingival overgrowth is often plaque-modified and frequently associated with specific medications.
- Maintenance therapy is critical for managing both recession and overgrowth. All images are sourced from the primary references, as well as the following supplemental texts:
- Periodontics: The Complete Summary (2021)
- Periodontal Review Q&A (2020)
Gingival Recession3
- Definition
- Epidemiology
- Aetiology
- Classification
- Clinical Consequences
- Indications for Treatment
- Management
- Prognostic Factors
- Evidence-Based Perspective
Gingival Enlargement
- Classification
- Pathogenesis of Drug-Induced Overgrowth
- Clinical Features
- Complications
- Management
- Recurrence
Gingival Recession4
Part 1 - Gingival Recession
Definition and Epidemiology
Definition5
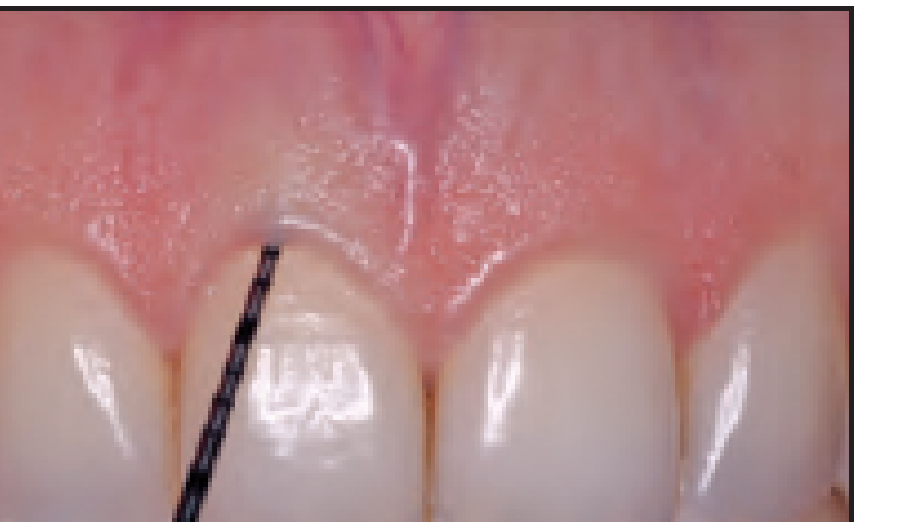
Gingival recession is the apical displacement of the gingival margin relative to the cemento-enamel junction (CEJ), resulting in root surface exposure.

Epidemiology6
- Increases with age
- Common in patients with history of periodontitis
- Frequently seen in patients with high traumatic toothbrushing habits
- Highly prevalent in thin periodontal phenotypes
 |  |
Aetiology of Recession
Anatomical and Inflammatory Factors
Anatomical Factors
- Thin periodontal phenotype
- Dehiscence and fenestration
- Prominent roots
- High frenum attachment
Inflammatory Factors
- Plaque-induced gingival inflammation
- History of periodontitis
Clinical Observations
- Plaque-induced gingivitis: Visible plaque, blunted interdental papillae, and red, slightly swollen, inflamed marginal gingiva.
- Chronic periodontitis: Swollen, inflamed gingivae with recession/clinical attachment loss, blunted gingival margins, and loss of contour.
Traumatic and Iatrogenic Factors
Traumatic Factors7
- Aggressive toothbrushing
- Abrasive dentifrices
- Oral piercings
- Traumatic Occlusion: Physical stress from biting forces
- Mechanical Trauma: Use of medium bristle toothbrushes

Iatrogenic Factors8
- Orthodontic tooth movement beyond alveolar envelope
- Subgingival restorative margins
- Poorly designed RPD clasps
 |  |
 |
Classification Systems
Miller Classification9
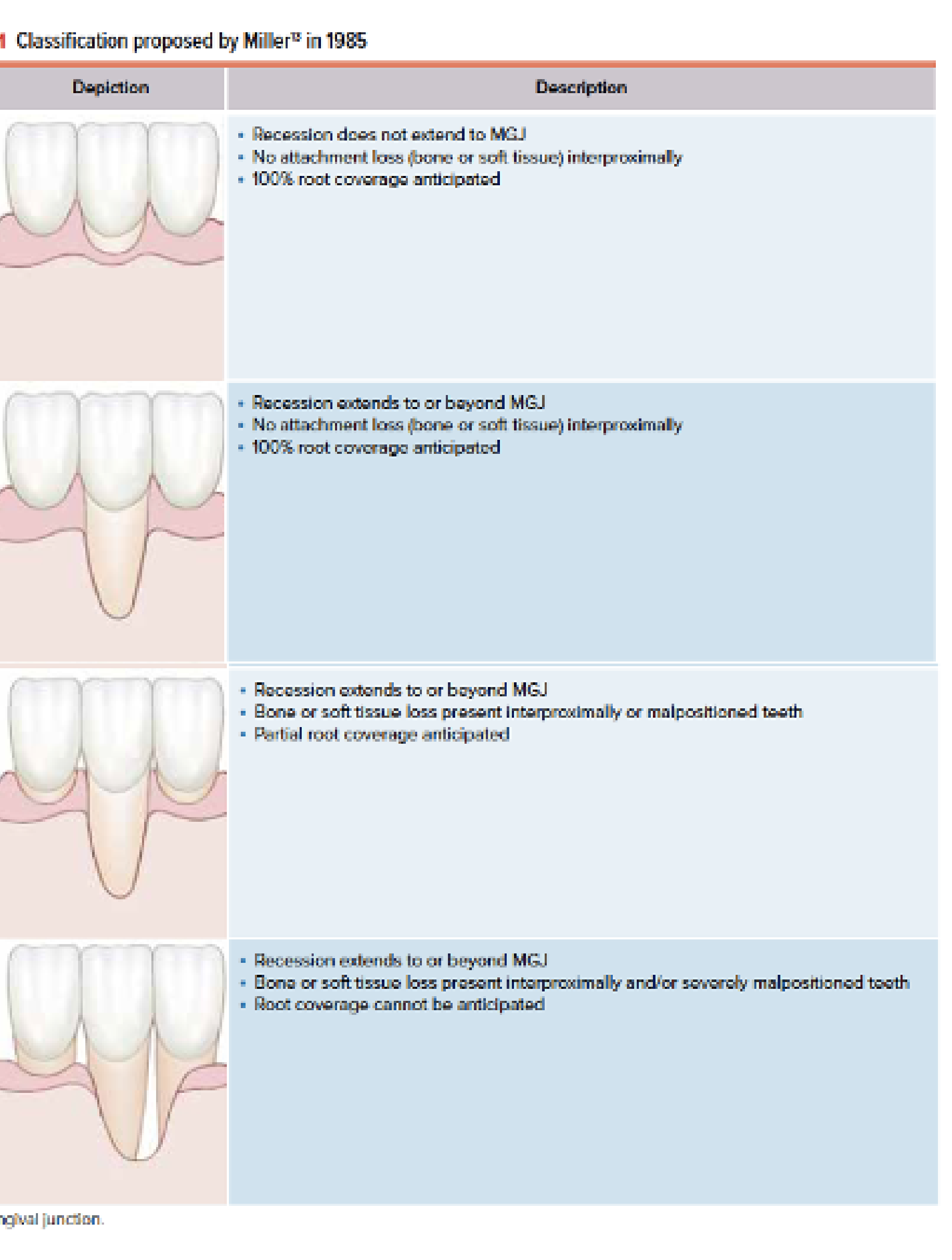
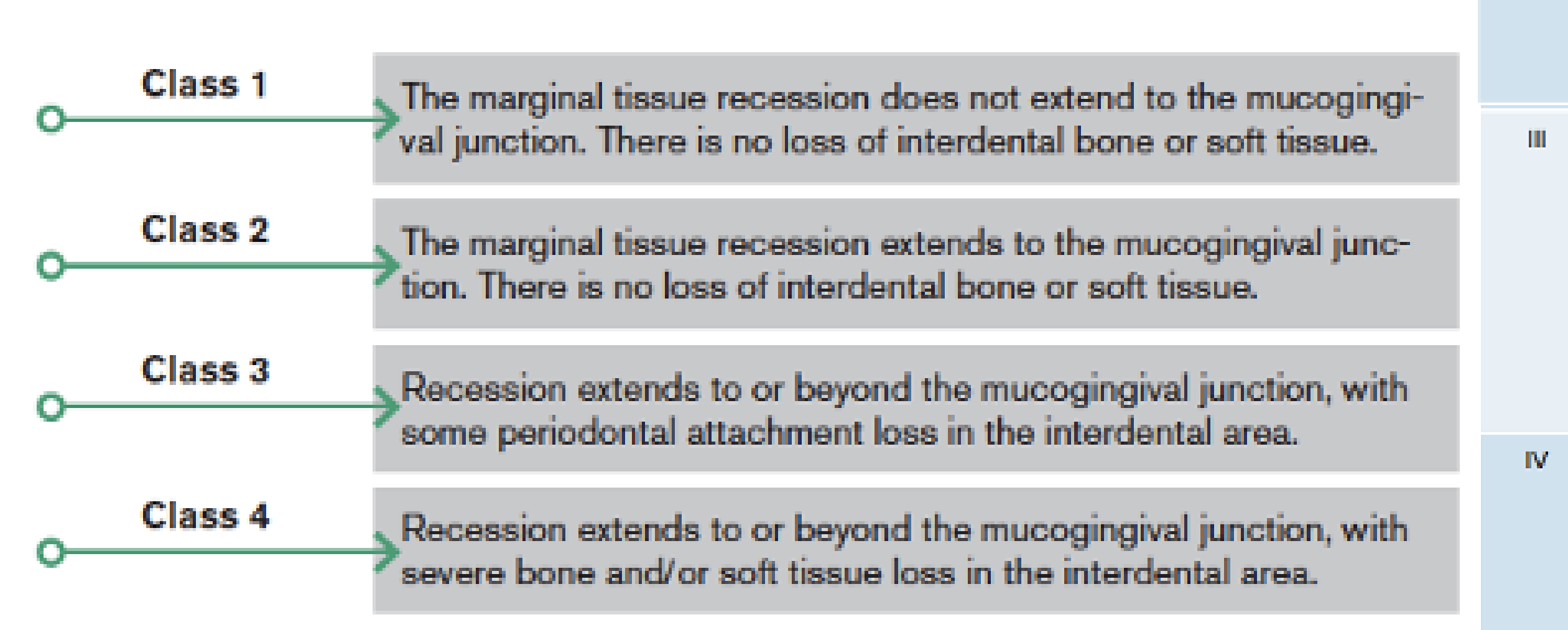
The Miller Classification (1985) categorizes recession into four classes based on interdental tissue loss:
- Class 1: Marginal tissue recession does not extend to the mucogingival junction. No loss of interdental bone or soft tissue.
- Class 2: Marginal tissue recession extends to the mucogingival junction. No loss of interdental bone or soft tissue.
- Class 3: Recession extends to or beyond the mucogingival junction, with some periodontal attachment loss in the interdental area.
- Class 4: Recession extends to or beyond the mucogingival junction, with severe bone and/or soft tissue loss in the interdental area.
 |  |
Sullivan and Atkins Classification10
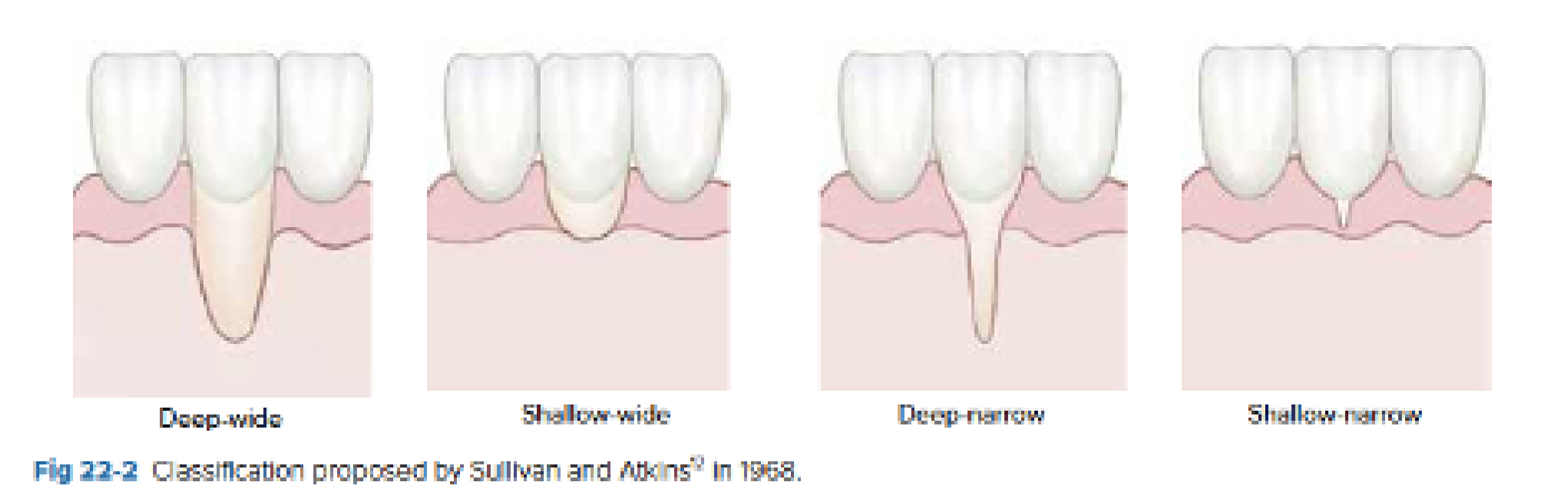
The Sullivan and Atkins (1968) classification categorizes defects by depth and width:
- Deep-wide: The most difficult area to treat. The graft should cover at least 5 mm of the connective tissue bed. Expect 1 to 2 mm of coverage.
- Shallow-wide: Expect 1 to 2 mm of new tissue over the apical portion.
- Deep-narrow: Rarely seen; expect complete coverage.
- Shallow-narrow: Maintain by conservative therapy.
 |  |
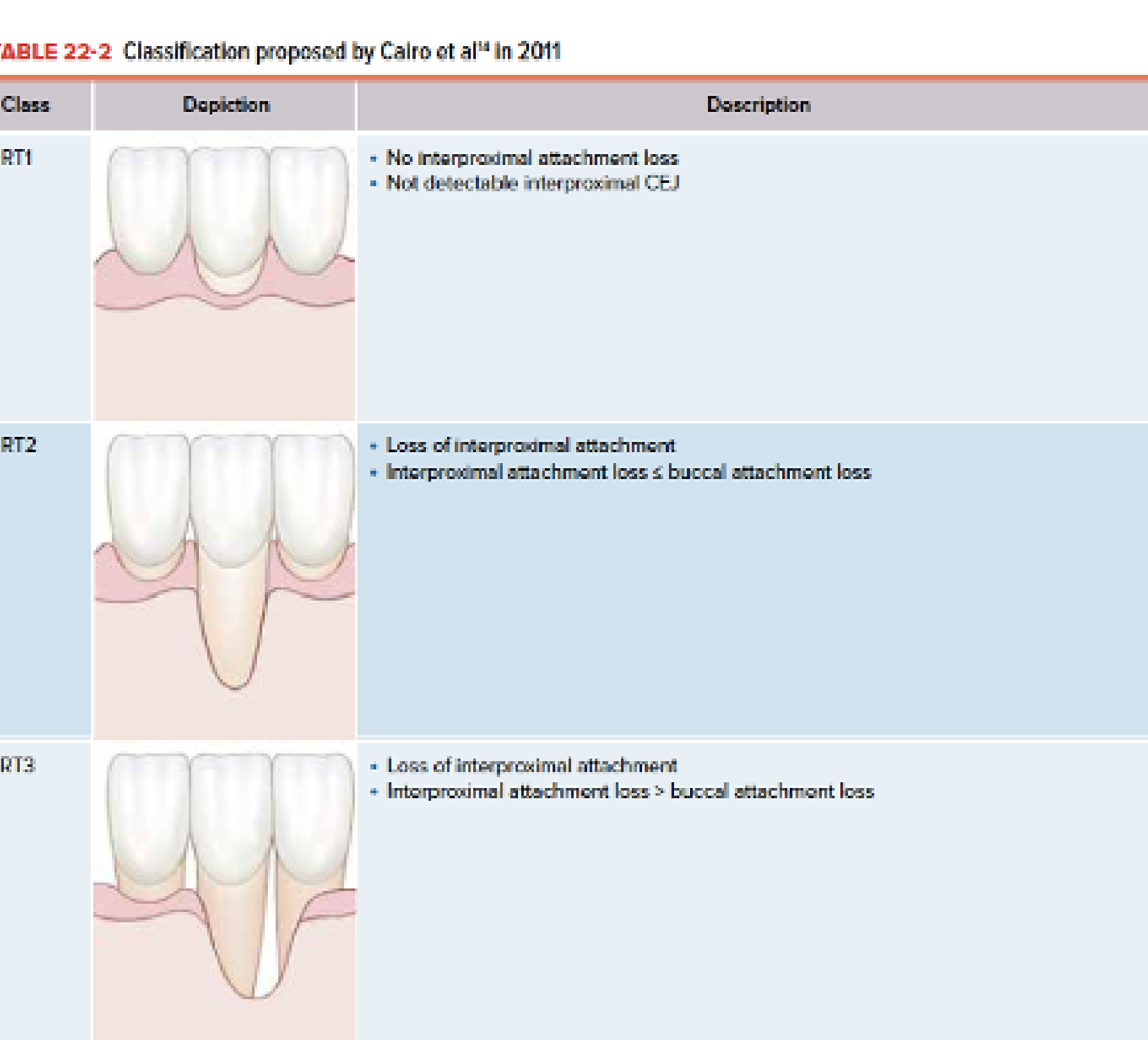
Cairo Classification11
Developed following the 2017 World Workshop, the Cairo classification is now the preferred system:
- RT1: No interproximal attachment loss; interproximal CEJ is not detectable.
- RT2: Loss of interproximal attachment where interproximal loss is less than or equal to buccal attachment loss.
- RT3: Loss of interproximal attachment where interproximal loss is greater than buccal attachment loss.
 |  |
Clinical Consequences and Indications
Clinical Consequences12
- Root sensitivity
- Root caries
- Non-carious cervical lesions
- Aesthetic concerns
- Plaque retention
- Cervical abrasion
- Hypertension (as mentioned in the transcript)
 |  |
 |  |
Indications for Treatment13
- Aesthetic concerns
- Dentine hypersensitivity
- Progressive recession
- Root caries
- Patient request
- Pre-prosthetic or orthodontic considerations

Management of Recession
Non-Surgical Management
- Oral hygiene modification
- Switching to electric toothbrushes with pressure sensors
- Desensitising agents
- Monitoring
- Risk factor control
- Adjusting traumatic occlusion or liaising with orthodontists
Surgical Root Coverage Procedures
Coronally Advanced Flap (CAF)14
- Considered the gold standard for RT1 defects.
CAF + Connective Tissue Graft (CTG)15
- Most predictable technique
- Improves tissue thickness
- Utilized in bilaminar techniques
- Uses the palate as a donor site
- The epithelium is removed from the graft
- Improves aesthetics
Free Gingival Graft (FGG)16
- Increases keratinised tissue
- Less aesthetic outcome compared to other methods
- Includes the top layer of epithelium

Tunnel Technique17
- Minimally invasive
- Suitable for multiple recession defects
- Blunt dissection (no scalpel)
- The interdental papilla remains intact; the graft is slid underneath and sutured
- May use "Alloderm" (acellular dermal matrix)
Laterally Positioned Flap (Lateral Sliding Flap)18
- Soft tissue mesial or distal to the exposed root is used for coverage.
- Indicated for the treatment of isolated recession defects.
Prognostic Factors and Evidence
Prognostic Factors19
- Defect depth and width
- Interproximal attachment is critical as a blood source for the graft
- Interproximal attachment level
- Tissue thickness
- Smoking status
- Operator skill
- Patient compliance
- Ceasing traumatic habits

Evidence and Predictability20
Clinical Evidence
The American Academy of Periodontology (2015) identified CAF + CTG as providing the highest predictability for complete root coverage.
- CAF + CTG provides the highest predictability for complete root coverage.
- A thick phenotype improves long-term stability.
- Long-term stability depends on plaque control and maintenance.

Gingival Overgrowth21
Part II - Gingival Overgrowth
Definition and Classification
Definition22
Gingival overgrowth (enlargement) is an increase in gingival volume due to inflammatory, drug-induced, systemic, or idiopathic causes.

Classification23
A. Inflammatory Enlargement
- Plaque-induced
- Chronic or acute
B. Drug-Induced Gingival Overgrowth (DIGO) Common drugs include:
- Phenytoin
- Cyclosporine
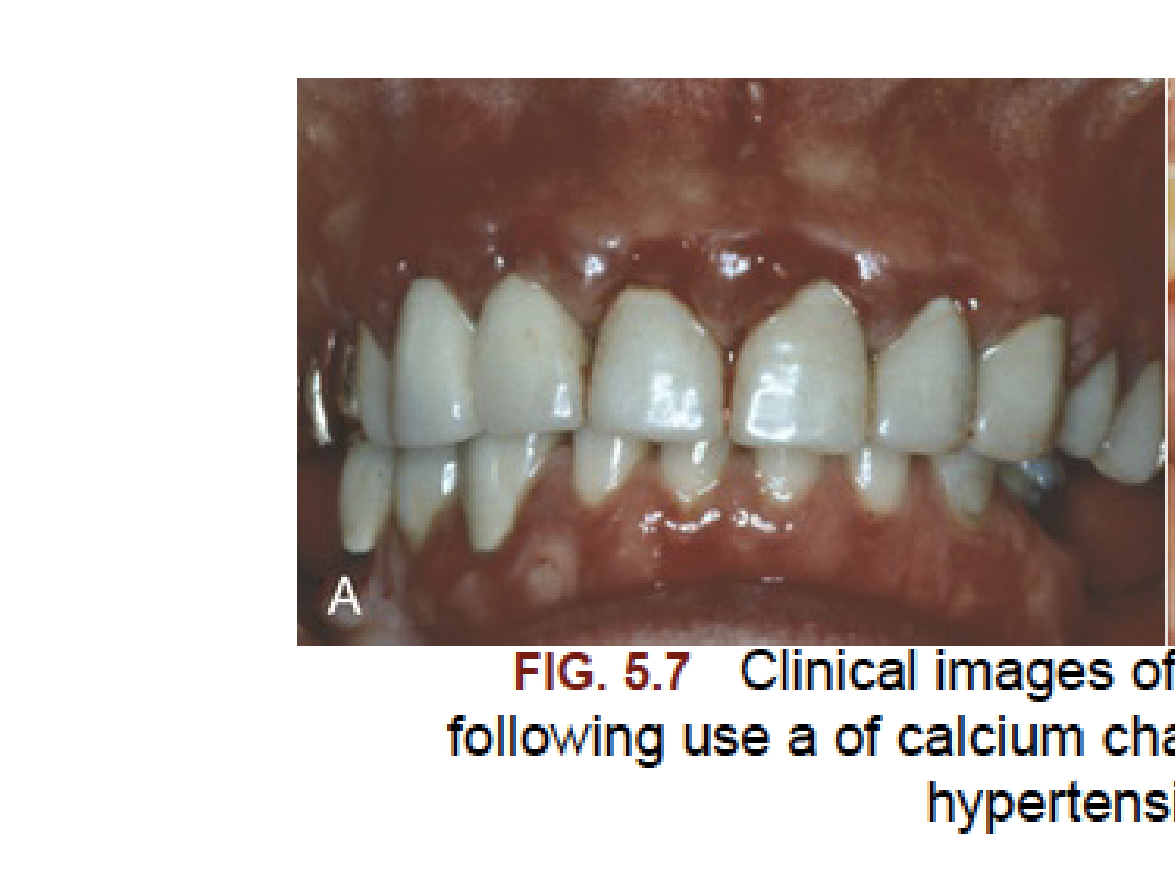
- Calcium channel blockers (e.g., nifedipine, amlodipine)
C. Systemic-Associated
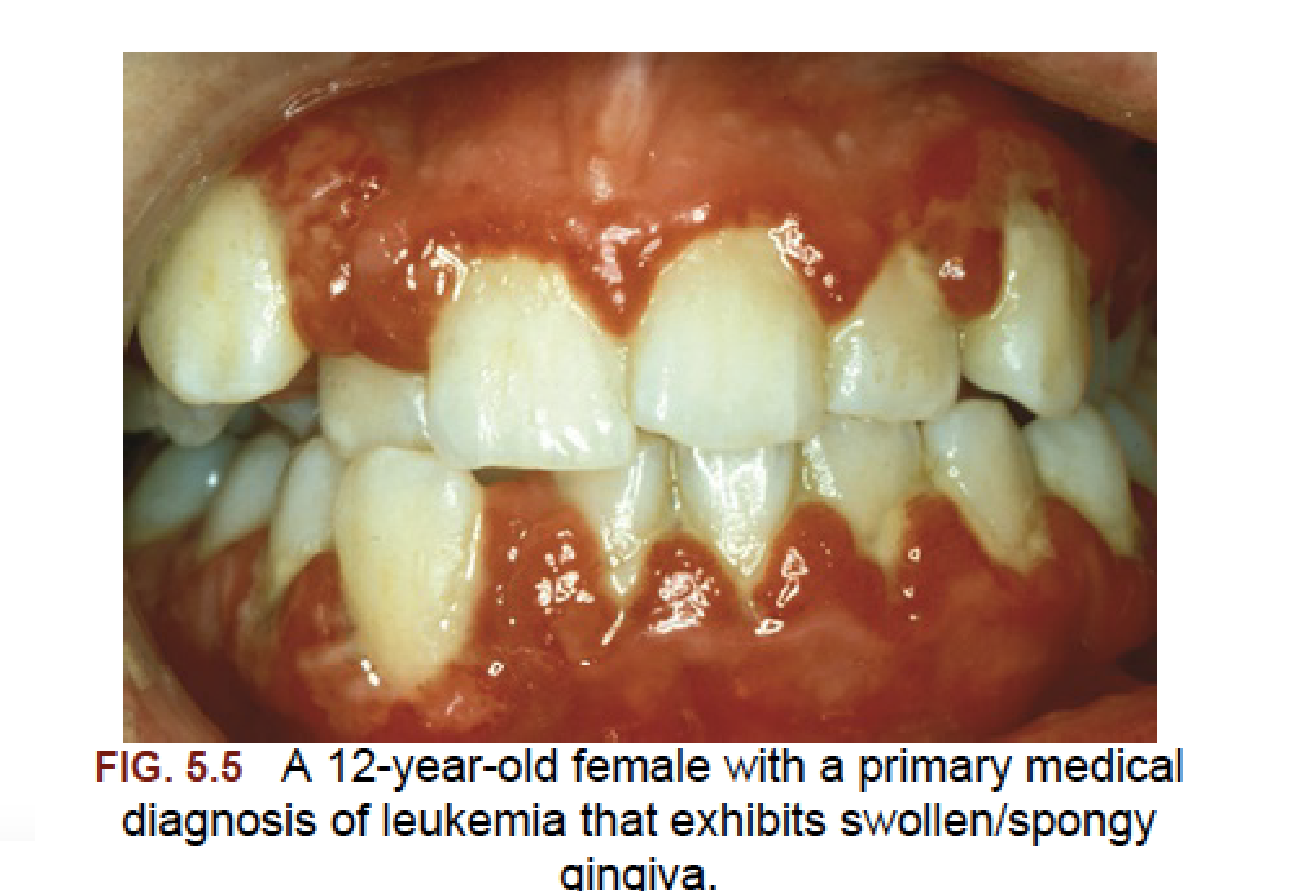
- Leukemia
- Hormonal changes (pregnancy, puberty)
D. Hereditary Gingival Fibromatosis
Clinical Examples
- Puberty gingivitis: Associated with poor hygiene, crowding, and mouth breathing; hyperplasia typically confined to anterior regions.
- Localized gingival enlargement: Can occur during pregnancy (e.g., appearing in the fourth month and progressing through the seventh month).
 |  |
Pathogenesis and Clinical Features
Pathogenesis of Drug-Induced Overgrowth24
- Altered fibroblast function
- Increased extracellular matrix production
- Reduced collagen degradation
- Exacerbated by plaque accumulation
- Genetic susceptibility
Histological Features
-
Chronic inflammatory enlargement shows an inflamed connective tissue core and strands of proliferating epithelium.
-
Inflammatory enlargement is typically erythematous, oedematous, and bleeds easily due to its association with plaque.
-
Drug-induced overgrowth is firm and fibrotic; it typically starts at the interdental papilla and can progress to cover the crowns.
-
Leukemic enlargement presents as boggy and hemorrhagic tissue with spontaneous bleeding.

Clinical Presentations25
- Chronic inflammatory enlargement: Often localized to the anterior region.
- Leukemia-associated enlargement: Presents as swollen or spongy gingiva.
- Calcium channel blocker-induced overgrowth: Resulting from medication used to control hypertension.
 |  |
 |  |
Complications and Management
Complications26
- Plaque retention
- Pseudopockets
- Difficulty in oral hygiene
- Aesthetic compromise
- Impaired mastication
- Speech interference (in severe cases)
- Hypertension (often as a co-morbidity in patients taking calcium channel blockers).

Management Strategies27
Non-Surgical Management
- Intensive plaque control
- Scaling and root planing
- Chlorhexidine adjunct
- Liaison with physician for medication substitution
Medical Liaison
Consulting a physician for medication substitution is a key step, such as replacing Calcium Channel Blockers with alternative antihypertensives to reduce overgrowth.
Surgical Management Indicated when a fibrotic component persists, there is functional/aesthetic compromise, or persistent pseudopockets are present. Procedures include:
- Gingivectomy (external or internal bevel)
- Flap surgery (if true pockets are present)
- Laser excision
- Periodontal flap treatment: Involves reverse bevel incision, thinning of enlarged tissue, and suturing the flap to the alveolar bone.

Recurrence and Key Takeaways
Recurrence28
Recurrence is common in Drug-Induced Gingival Overgrowth (DIGO) and is dependent on:
- Continuation of the associated drug
- Quality of plaque control
- Genetic factors
Key Take-Home Messages29
-
Gingival recession is primarily a soft tissue deficiency problem.
-
Predictability of treatment depends on interproximal attachment.
-
Gingival overgrowth is often plaque-modified and drug-associated.
-
Maintenance therapy is critical for the long-term management of both conditions.
-
Healing sites should generally not be probed for six months following periodontal surgery to avoid disturbing the healing process.
-
General dentists can perform these procedures if they have appropriate training but must manage any complications.
-
Shared care between a general dentist and a periodontist involves coordinated maintenance and monitoring.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Case Study: Habit Correction and Monitoring
A patient using a medium bristle toothbrush presented with recession. The clinician spent a year reviewing the patient to ensure the traumatic habit was ceased and the recession stabilized before proceeding with surgery. This highlights that if the original habit (e.g., improper brushing) remains, the recession will recur even after surgical intervention.
Footnotes
-
Original PDF page 1: L2 Gingival Recession Gingival Overgrowth, p.1 ↩
-
Original PDF page 2: L2 Gingival Recession Gingival Overgrowth, p.2 ↩
-
Original PDF page 4: L2 Gingival Recession Gingival Overgrowth, p.4 ↩
-
Original PDF page 3: L2 Gingival Recession Gingival Overgrowth, p.3 ↩
-
Original PDF page 5: L2 Gingival Recession Gingival Overgrowth, p.5 ↩
-
Original PDF page 6: L2 Gingival Recession Gingival Overgrowth, p.6 ↩
-
Original PDF page 9: L2 Gingival Recession Gingival Overgrowth, p.9 ↩
-
Original PDF page 10: L2 Gingival Recession Gingival Overgrowth, p.10 ↩
-
Original PDF page 11: L2 Gingival Recession Gingival Overgrowth, p.11 ↩
-
Original PDF page 12: L2 Gingival Recession Gingival Overgrowth, p.12 ↩
-
Original PDF page 13: L2 Gingival Recession Gingival Overgrowth, p.13 ↩
-
Original PDF page 14: L2 Gingival Recession Gingival Overgrowth, p.14 ↩
-
Original PDF page 15: L2 Gingival Recession Gingival Overgrowth, p.15 ↩
-
Original PDF page 17: L2 Gingival Recession Gingival Overgrowth, p.17 ↩
-
Original PDF page 18: L2 Gingival Recession Gingival Overgrowth, p.18 ↩
-
Original PDF page 19: L2 Gingival Recession Gingival Overgrowth, p.19 ↩
-
Original PDF page 20: L2 Gingival Recession Gingival Overgrowth, p.20 ↩
-
Original PDF page 21: L2 Gingival Recession Gingival Overgrowth, p.21 ↩
-
Original PDF page 22: L2 Gingival Recession Gingival Overgrowth, p.22 ↩
-
Original PDF page 23: L2 Gingival Recession Gingival Overgrowth, p.23 ↩
-
Original PDF page 24: L2 Gingival Recession Gingival Overgrowth, p.24 ↩
-
Original PDF page 25: L2 Gingival Recession Gingival Overgrowth, p.25 ↩
-
Original PDF page 26: L2 Gingival Recession Gingival Overgrowth, p.26 ↩
-
Original PDF page 27: L2 Gingival Recession Gingival Overgrowth, p.27 ↩
-
Original PDF page 28: L2 Gingival Recession Gingival Overgrowth, p.28 ↩
-
Original PDF page 29: L2 Gingival Recession Gingival Overgrowth, p.29 ↩
-
Original PDF page 30: L2 Gingival Recession Gingival Overgrowth, p.30 ↩
-
Original PDF page 31: L2 Gingival Recession Gingival Overgrowth, p.31 ↩
-
Original PDF page 32: L2 Gingival Recession Gingival Overgrowth, p.32 ↩