Endodontic and Periodontal Diseases
Course Instructors1
- Dr. Anna Hughes
- Dr. Tina Choo
- Special thanks to Prof. Paul Abbott
- Dr. Saleh (Referenced for clinical case studies)
Learning Objectives and Clinical Aims
Clinical Objectives2
- Understand the presentation of endodontic, periodontal, and combined or concurrent endodontic-periodontal diseases.
- Learn how to differentiate between endodontic and periodontal diseases.
- Recognize that other distinct conditions may have endodontic and periodontal implications, requiring specific management:
- Root perforations and fractures
- Cracks
- Caries
- Root resorption
- Orthodontic complications
- Developmental anomalies - Developmental anomalies (e.g., palatal grooves)

Diagnostic and Management Goals
- Emphasize the importance of achieving the correct diagnosis.
- Understand the prognosis and management of the presenting condition.
- Review both old and new classification systems.
- Achieve a better understanding of how to sequence treatment.
- Familiarize students with the new periodontal classification system.
Characteristics of Periodontal Disease
Diagnosing Periodontitis: Signs and Symptoms3
- Attachment loss and deep pockets
- Bleeding
- Tooth mobility
- Plaque and calculus deposits
- Positive response to cold/pulp tests
- Radiographic bone loss
- Generally painless
- Pain Profile: Generally painless unless associated with necrotizing diseases or acute abscesses.

Characteristics of Pulpal Disease
Clinical Presentation of Pulpal Disease4
- Reversible Pulpitis: Sensitivity to cold or hot which does not linger long.
- Irreversible Pulpitis: Severe pain, lasting throbbing, and an altered response to pulp tests.
- Periodontal Involvement: Inflammation may extend to the periodontal ligament, making the tooth tender to pressure, biting, or tapping.
- Tenderness to percussion (TTP) is a key clinical indicator of periodontal ligament involvement.
- Necrosis: If left untreated, pulp necrosis occurs, leading to eventual infection, bone resorption, and radiolucency around the apex, in the furcation, or lateral to the root.

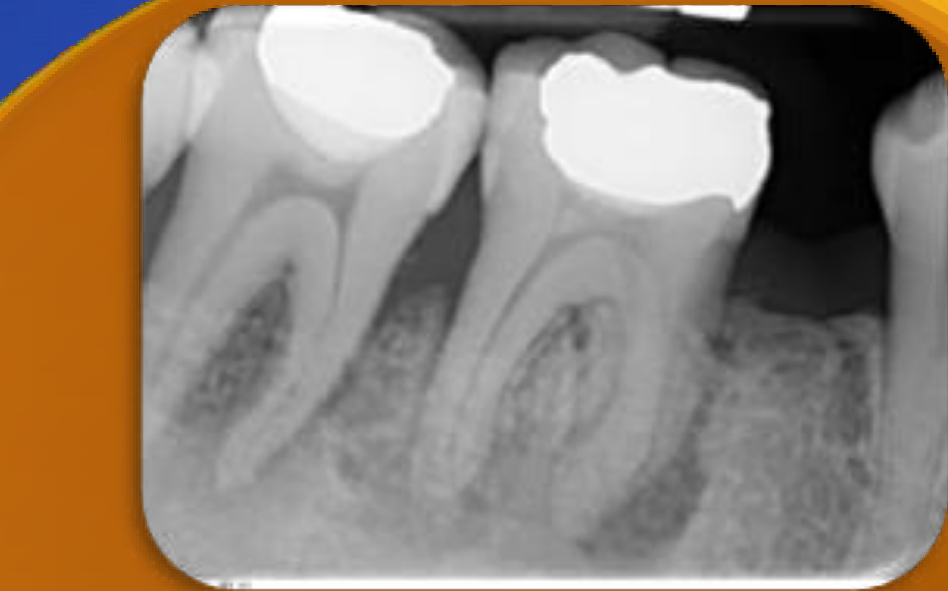
Pathways of Communication Between Pulp and Periodontium5

Impact of Pulpal Infection on the Periodontium6
- Pulpal disease can cause periodontal changes.
- Infections in the pulp can spread through lateral and accessory canals into the periodontal ligament.
- This spread can lead to the destruction of bone.
- Bacteria (specifically gram-negative anaerobes) can penetrate through various channels due to their relative size compared to the anatomy of the tooth.
- Communication can also occur via cracks and dentinal tubules.
Potential pathways of communication between the pulp and periodontium are illustrated through various anatomical channels.
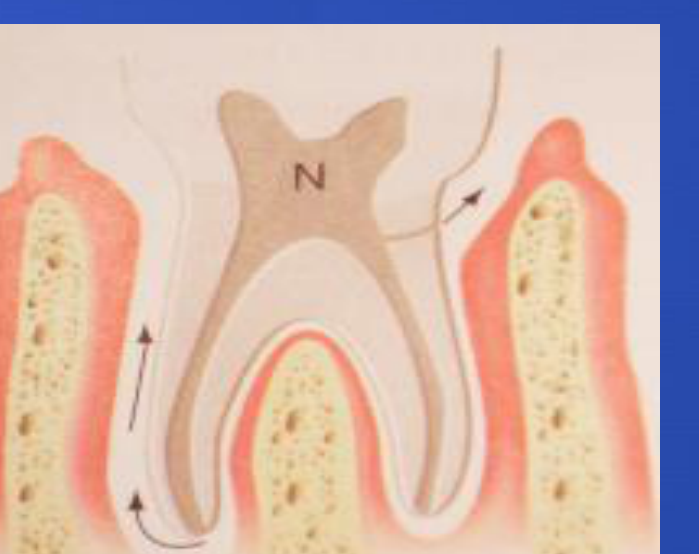 | 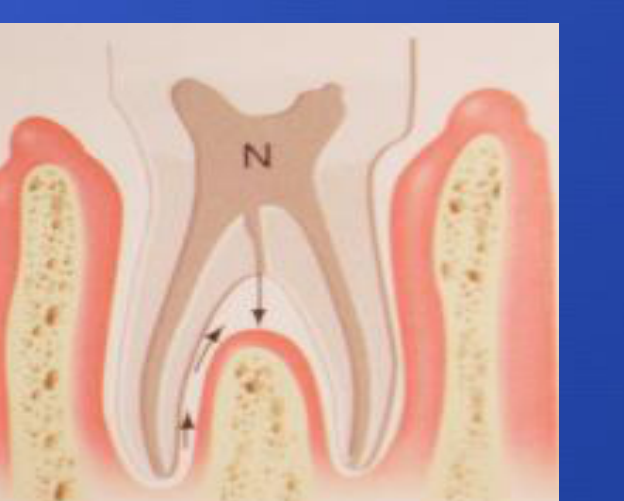 |
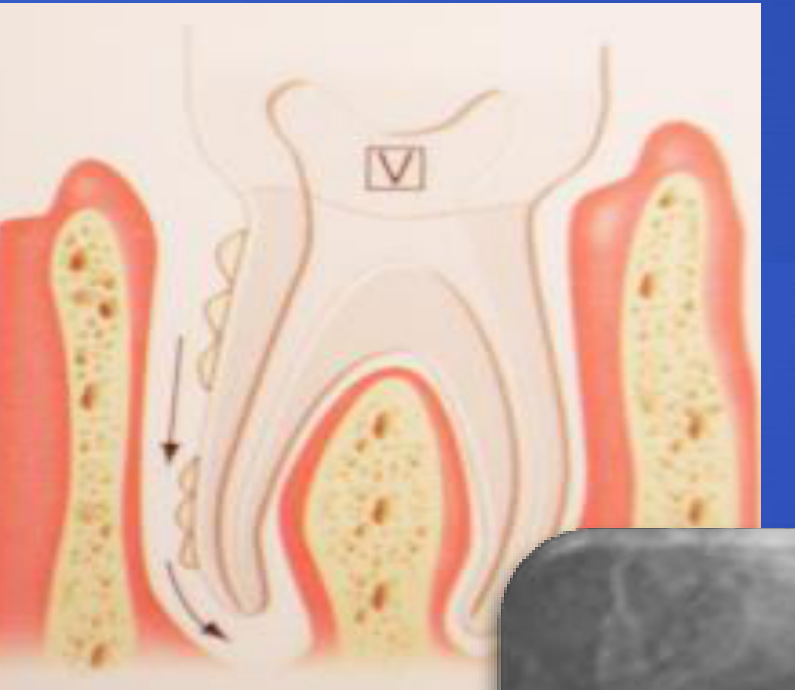
Communication Pathways7
Specific anatomical pathways (labeled A through F) facilitate communication between the internal pulp chamber and the external periodontal environment (Source: Abbott & Castro Salgado 2009).
- Lateral and Accessory Canals: Found mostly in the apical region and in the furcations of molars (up to 30% of molars).
- Dentinal Tubules: Exposed via cracks or loss of cementum.
- Anatomical Anomalies: Root invaginations and palatal grooves.

Impact of Periodontal Infection on the Pulp8
- The effect of periodontal disease on the pulp is less definitive than the reverse.
- Normal pulps are observed in the majority of teeth with advanced periodontal disease.
- A small percentage of teeth with advanced periodontal disease may develop pulp infections if the apical foramina is invaded.
Defense Mechanisms
The PDL has a robust vasculature and immune system that helps prevent microbial spread, whereas a necrotic pulp lacks blood supply and cannot defend itself.
 |  |
Diagnosis of Combined Endo-Perio Disease9
Advanced periodontitis can allow bacteria to gain access to the pulp via accessory canals or the apex of the root, leading to pulpal infection.
 |  |
 |
Clinical Examination and Sensibility Testing
Diagnostic Tools and Requirements10
Diagnosis of combined lesions can be complex. The most important clinical examination tools include:
-
The "Essential Three": Pulp sensibility tests, periodontal probing (full mouth), and radiographs (Periapical minimum; CBCT for detail).
-
Pulp sensibility tests
-
Periodontal probing (full chart, checking for suppuration and mobility)
-
Radiographs (Periapicals, CBCT)
-
Comprehensive history (trauma, previous procedures, symptoms)
-
Visual appearance of soft tissues
-
Assessment of caries, restorations, and anatomical factors
-
Transillumination
Determining the Origin of the Lesion11
- Vital Pulp Test: A positive result helps rule out endodontic origin, except in multi-rooted teeth with partial necrosis (necrobiosis).
- Non-responsive Pulp: When the pulp is non-responsive and the infection is traced to a lateral canal or apical foramen, the lesion is suspected to be of endodontic origin.
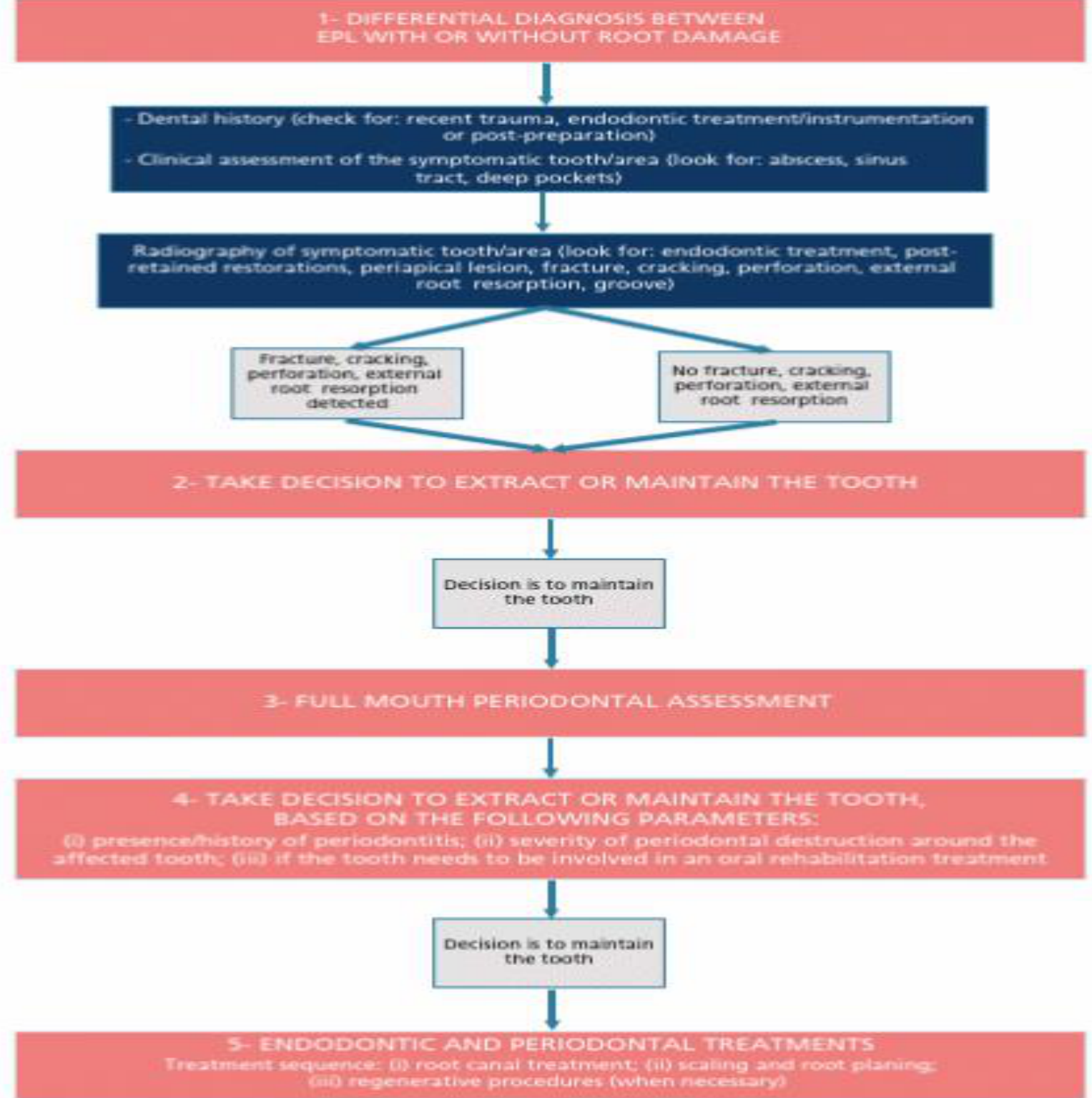
Management Steps for Endo-Periodontal Lesions (EPL)12
- Differential Diagnosis: Distinguish between EPL with or without root damage.
- Utilize decision trees (e.g., Linde) to categorize the lesion based on clinical findings.
- Check dental history for trauma, endodontic treatment, or post-preparation.
- Clinical assessment for abscesses, sinus tracts, or deep pockets.
- Radiographic review for periapical lesions, fractures, cracks, perforations, or resorption.
- Initial Decision: Determine whether to extract or maintain the tooth.
- Full Mouth Periodontal Assessment: Conducted if the decision is to maintain the tooth.
- Secondary Decision: Re-evaluate maintenance based on:
- Presence/history of periodontitis.
- Severity of periodontal destruction.
- Role of the tooth in overall oral rehabilitation.
- Treatment Sequence:
- Root canal treatment.
- Scaling and root planing.
- Regenerative procedures (when necessary).
Sensibility Test Considerations13
- Pulp tests are not always reliable; using two tests (e.g., Cold/CO2 and EPT) is preferred.
- In multi-rooted teeth, partial necrosis may still allow for a positive response to testing.
 |  |
 |
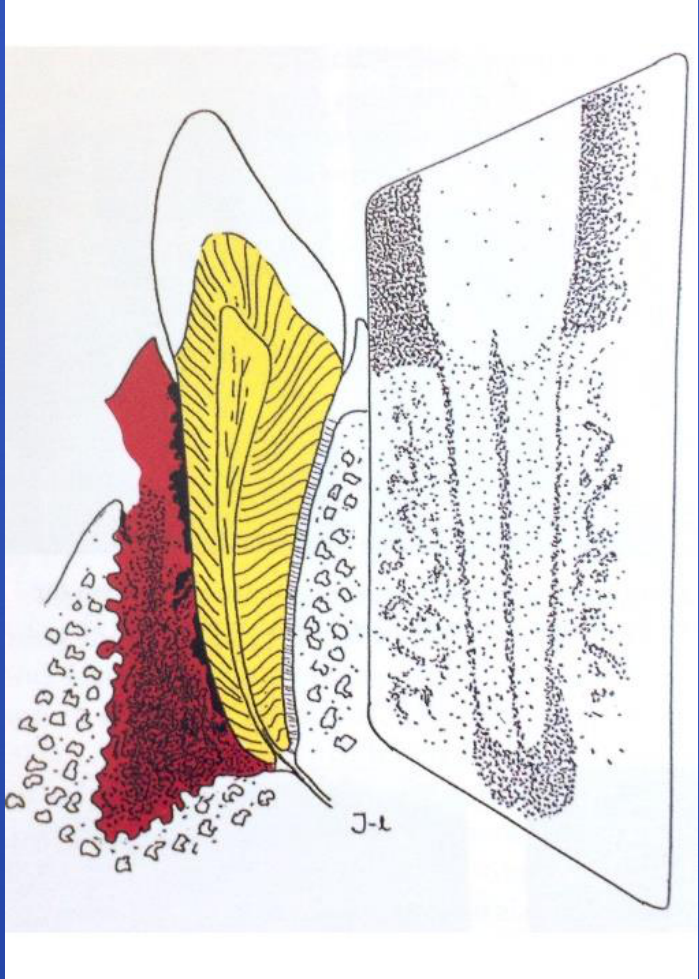
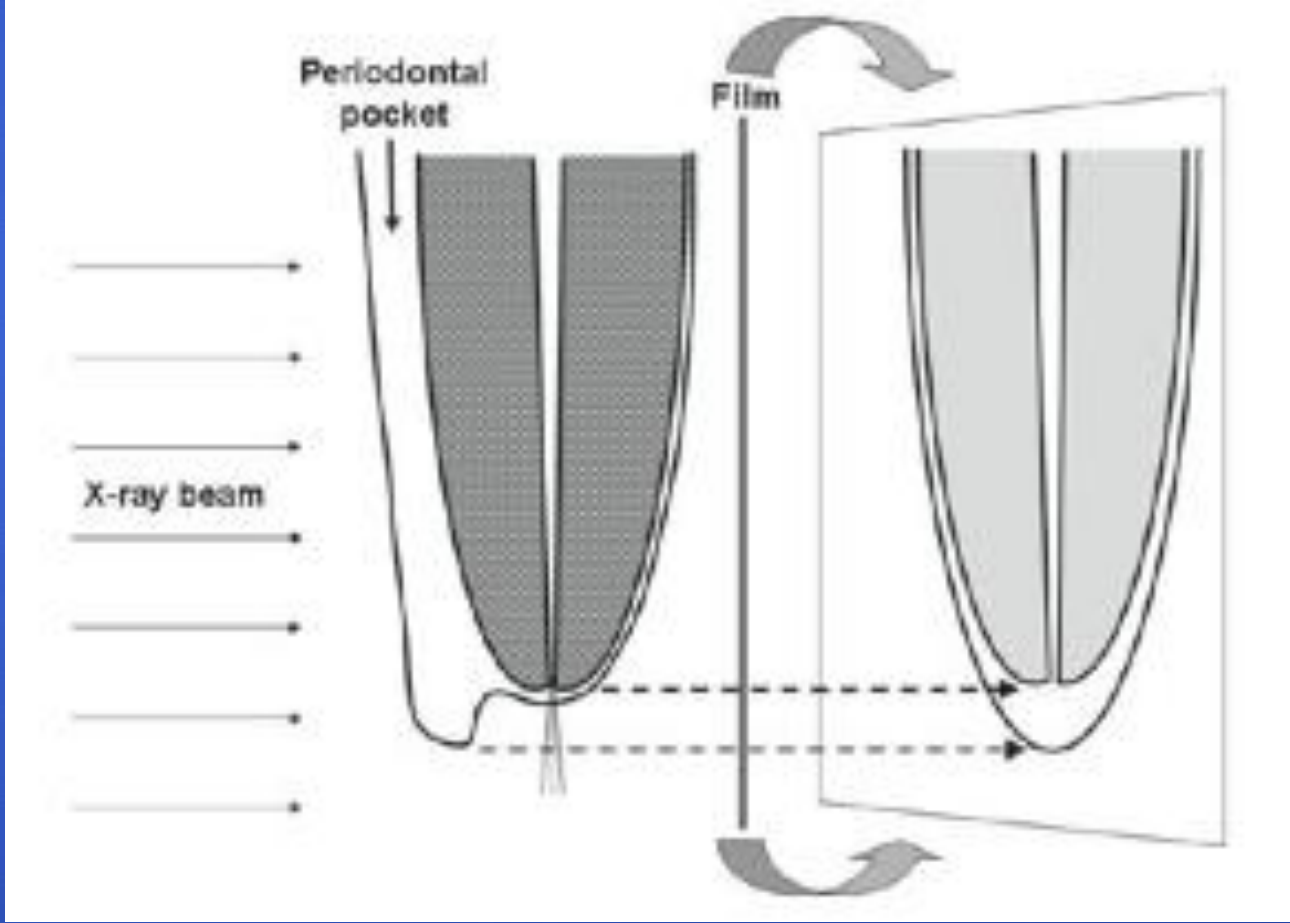
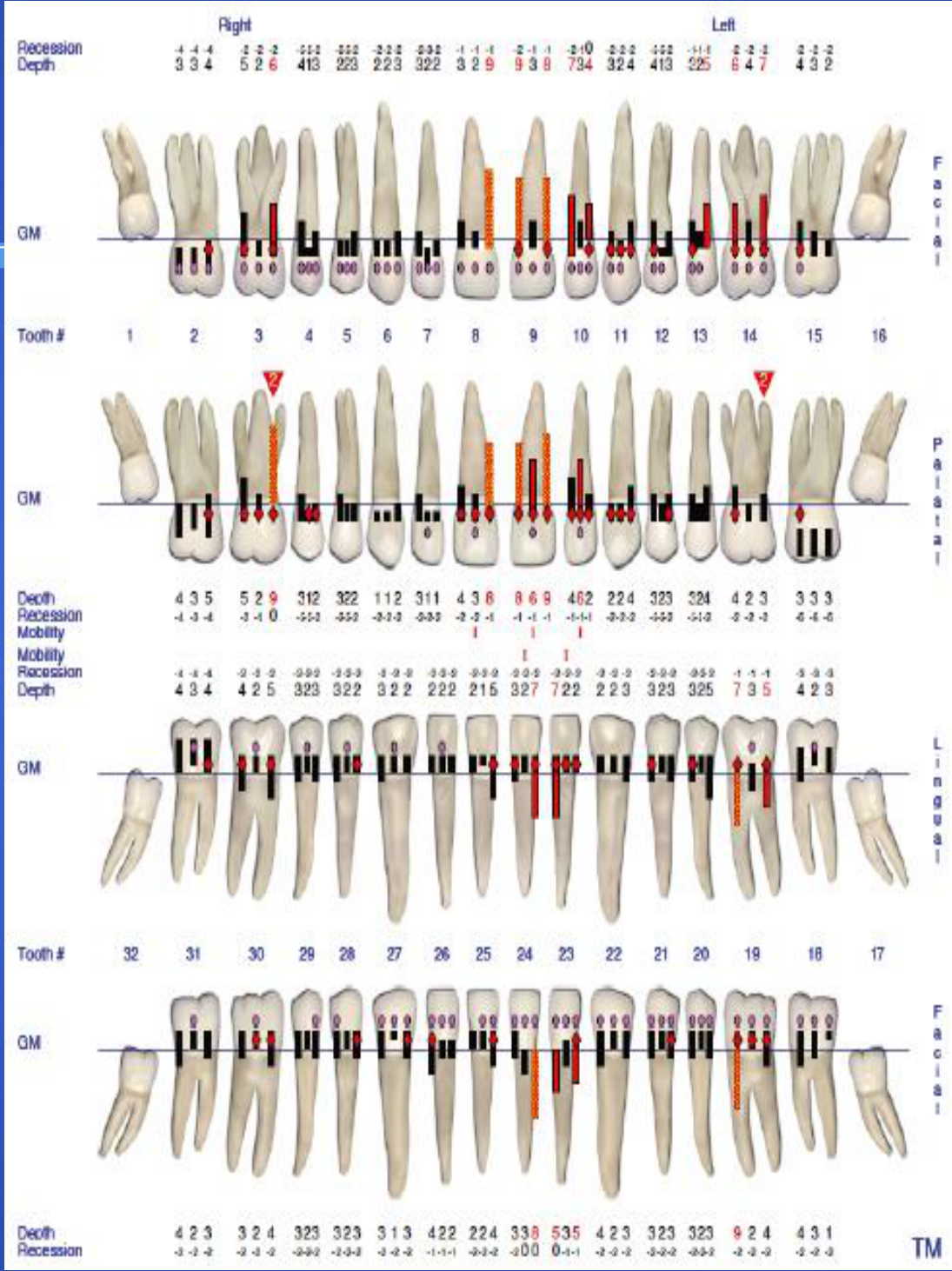
Radiographic Examination and Probing Defects1415
Radiographic examination is a critical component in diagnosing the extent and origin of endo-perio lesions.
Detailed radiographic assessment is required to identify bone loss patterns and pulpal pathology.
 |  |
 |
Characteristics of Endodontic Probing Defects16
- Probing defects of endodontic origin are typically narrow and long.
- These are often referred to as narrow sinus tract-type probing.
- The lesion likely drains through the bone rather than the periodontal ligament, mimicking a periodontal defect.
- Key Difference: Endodontic "pockets" are often narrow and point directly to the apex, whereas periodontal pockets are typically wider and associated with generalized bone loss.

Differential Diagnosis and Case Studies DiagnosticClassifications Diagnosis
Differential Diagnosis Table17
| Signs | Endodontic | Periodontal | Combined |
|---|---|---|---|
| Localized to Tooth | + | - | +/- |
| Extensive Caries/Restoration | + | - | +/- |
| Pulp Sensibility Tests | - | + | - |
| Probing Defect | Narrow | Wide | Wide |
| Crestal Bone Loss | - | + | + |
| Percussion | +/- | +/- | +/- |
| Palpation | +/- | +/- | +/- |

Transient Pulpal Response18
Transient pulpal responses, such as tooth discoloration, can occur following periodontal treatment/instrumentation, particularly in cases of aggressive periodontitis.
Transient Pulpal Response
Deep non-surgical debridement in very deep pockets can cause temporary pulp non-responsiveness and discoloration that may later resolve.
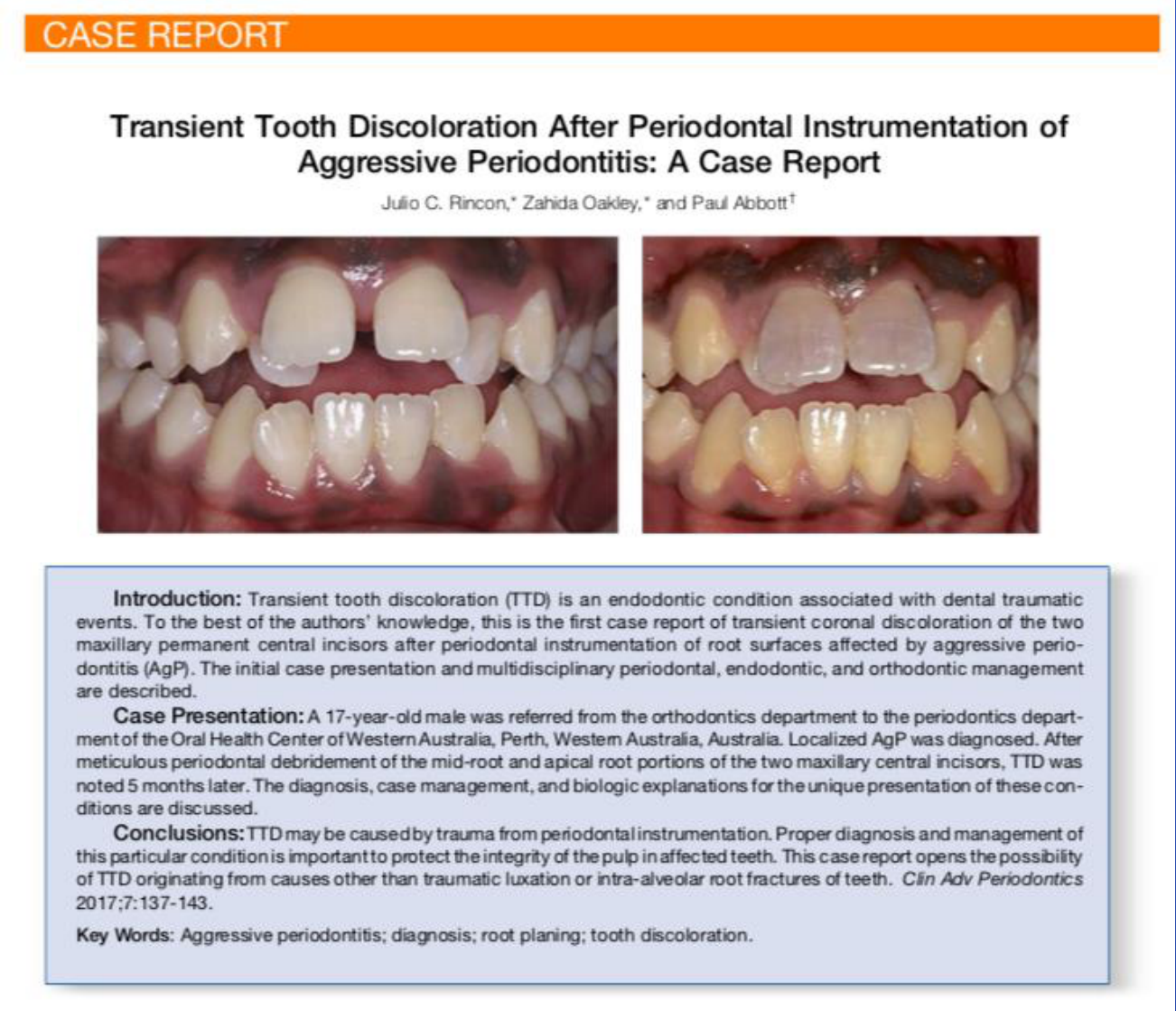
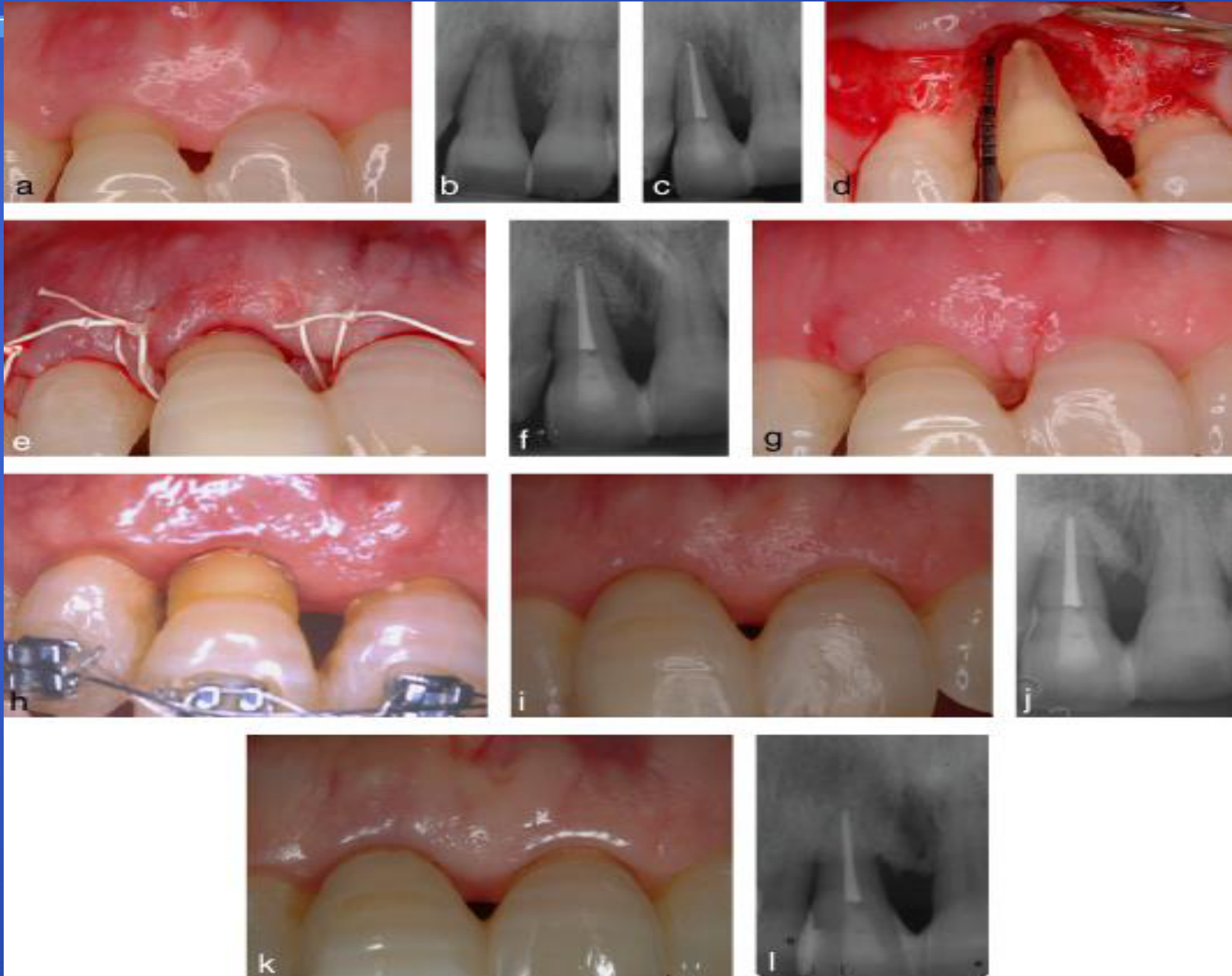
Case Report: Tooth Discoloration and Aggressive Periodontitis19
- Patient: 17-year-old male, Black African from Eritrea.
- Referral: Orthodontic department to Periodontal department (July 2010).
- Medical History: Clear
- Clinical Presentation: Severe bone loss on incisors and molars (formerly localized juvenile periodontitis).

Clinical Presentation20
Initial clinical views of the upper and lower anterior teeth show extensive gingival recession and mobility.
 |  |
 |  |
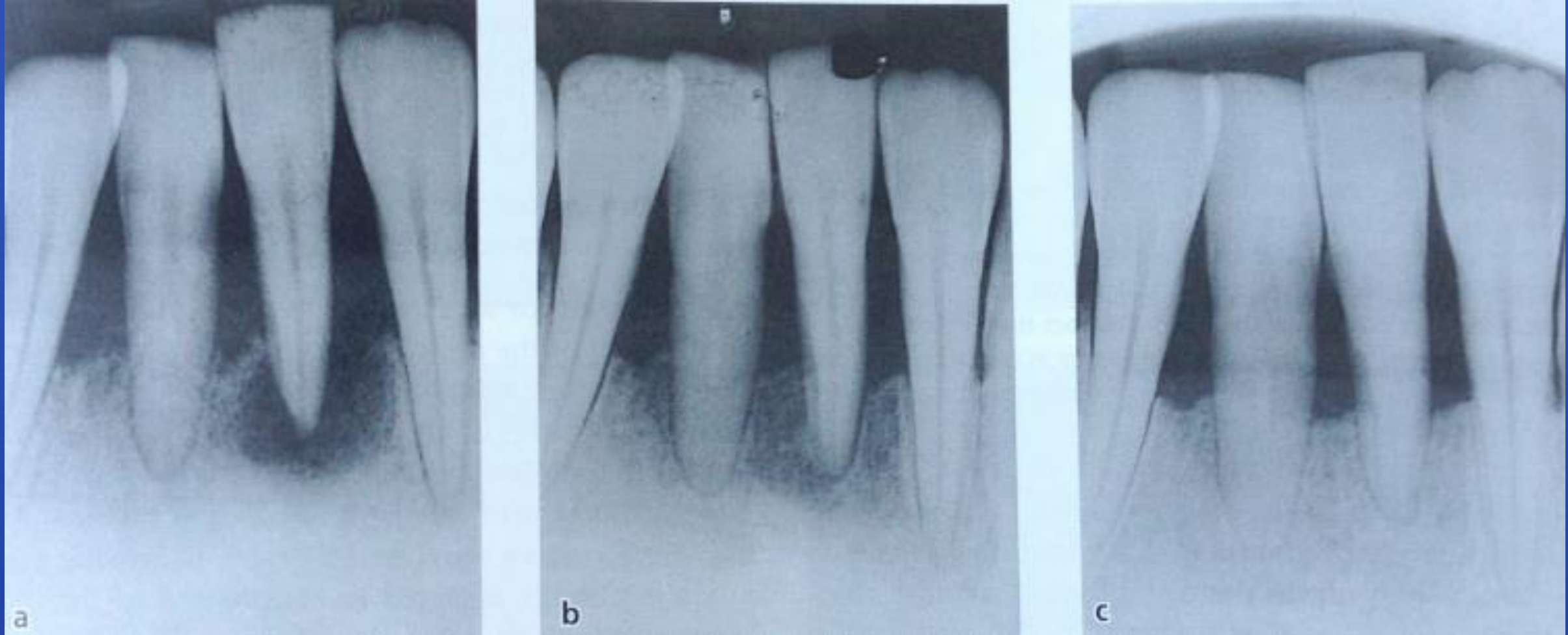
Periodontal Review (November 2010)21
Follow-up assessment of the patient’s periodontal status.
- Following non-surgical treatment, teeth showed grey/rosy discoloration and were non-responsive to pulp testing.

Second Periodontal Review (January 2011)22
Observations included grey/rosy pulp discoloration and results from pulp testing.
- Clinical healing observed; tooth color improved.
 |  |
 |
Periodontal Maintenance (August 2011)23
Long-term follow-up and maintenance phase for the aggressive periodontitis case.
- Pulps responded normally to stimulation.
 |  |
 |  |
Diagnostic Pitfalls24
Clinicians must be aware of conditions that mimic endo-perio lesions:
- Incomplete coronal fractures (cracked tooth) extending into the root.
- Crown-root or vertical root fractures.
- Root resorption.
- Palatal grooves.
Clinical Caution
Clinicians must be careful not to perform unnecessary root canals on teeth experiencing "transient pulpal response" following deep scaling.

Classification of Endo-Perio Lesions
Historical and Modern Classification Systems
Simon, Glick & Frank Classification (1972)25
- Primary Endodontic lesion.
- Primary Endodontic lesion with secondary Periodontal involvement.
- Primary Periodontal lesion.
- Primary Periodontal lesion with secondary Endodontic involvement.
- “True” Combined lesion.

Limitations of Historical Classifications26
- Difficulty in identifying the primary source of infection.
- Ambiguity regarding whether lesions are communicating or separate.
- Lack of specific guidance for prognosis or treatment planning.
Modern Classification of Endo-Periodontal Lesions27
DiagnosticClassifications 1. Endo-periodontal lesion with root damage
- Root fracture or cracking
- Root canal or pulp chamber perforation
- External root resorption
2. Endo-periodontal lesion without root damage
- In Periodontitis Patients:
- Grade 1: Narrow deep periodontal pocket in 1 tooth surface.
- Grade 2: Wide deep periodontal pocket in 1 tooth surface.
- Grade 3: Deep periodontal pockets in > 1 tooth surface.
- In Non-Periodontitis Patients:
- Grade 1: Narrow deep periodontal pocket in 1 tooth surface.
- Grade 2: Wide deep periodontal pocket in 1 tooth surface.
- Grade 3: Deep periodontal pockets in > 1 tooth surface.

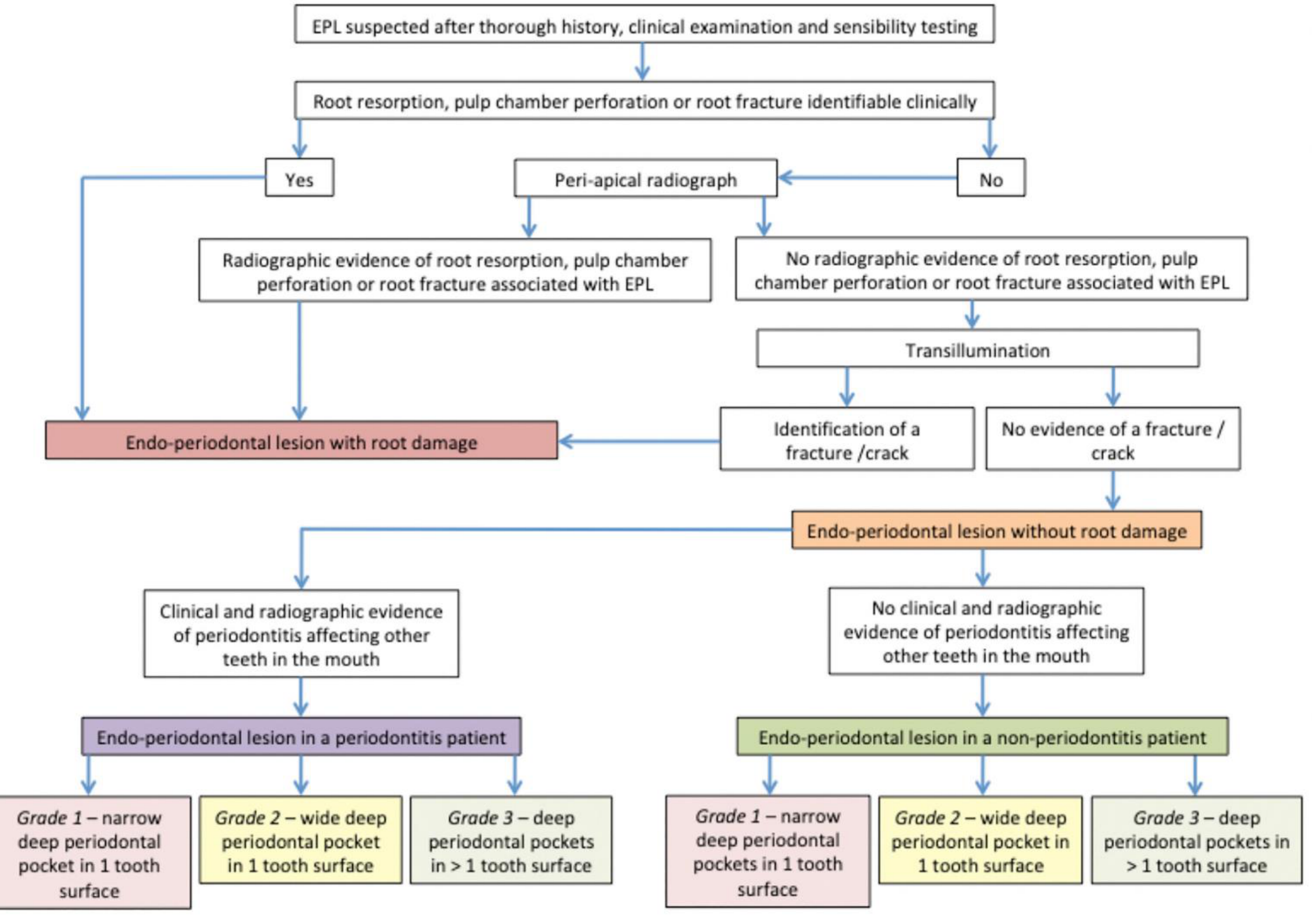
Diagnostic Decision Tree28
- Step 1: Suspect EPL after history, clinical exam, and sensibility testing.
- Step 2: Identify root damage (resorption, perforation, fracture) clinically or radiographically.
- If Yes: Classify as Endo-periodontal lesion with root damage.
- If No: Use transillumination to check for cracks.
- Step 3: Assess for systemic periodontitis.
- If periodontitis is present in other teeth: Classify as EPL in a periodontitis patient.
- If no periodontitis elsewhere: Classify as EPL in a non-periodontitis patient.
- Step 4: Assign Grade (1, 2, or 3) based on pocket width and number of surfaces involved.
Prognosis Assessment
Establishing Prognosis29
Prognosis is categorized as:
-
Hopeless
-
Poor
-
Favourable
-
Factors influencing prognosis include restorability, the total amount of attachment loss, complex root anatomy such as furcations, and patient compliance.
Considerations:
- Is the tooth worth treating?
- Alternative options must be discussed.
- Significant cost and time requirements.

Strategies for Management (Abbott & Castro Salgado)30
Management Principle
The overall management strategy is heavily dictated by whether the endodontic and periodontal lesions communicate via the periodontal pocket.
- Diagnosis: Determine if both diseases are present as independent infections or manifestations of one another.
- Communication: Determine if the diseases communicate via the periodontal pocket.
- Treatment Sequence: If the root canal is infected, endodontic treatment should precede periodontal therapy to remove intracanal infection before cementum removal.
- Medication: Use non-toxic intracanal medicaments to destroy bacteria and encourage tissue repair.
 |  |
Management Strategies for Combined Lesions
Classification by Communication (Abbott & Castro 2009)31
- Concurrent Endodontic and Periodontal diseases without communication.
- Concurrent Endodontic and Periodontal diseases with communication.
 |  |
 |  |
Prognostic Differences32
- Prognosis is better for lesions without communication.
- Combined lesions with communication have a worse prognosis.
 |  |
 |
Concurrent Disease Without Communication
Management of Lesions Without Communication33
- Requires combined periodontal and endodontic therapy.
- Treat the acute condition first.
- Start endodontic treatment and medicate canals first; infected root canals can hinder periodontal healing.
- Prognosis depends on the extent of periodontal involvement and the cause of pulpal disease.
 |  |
 |
Concurrent Disease With Communication34
 |  |
Management Protocol for Lesions With Communication35
- Treat the acute condition.
- Remove restorations/caries to assess restorability.
- Initiate endodontic treatment: clean and medicate canals (e.g., Ledermix or 50:50 Ledermix/Calcium Hydroxide).
- Wait a minimum of 4 weeks before starting periodontal therapy.
- Rationale: This sequence prevents endodontic infection from interfering with periodontal healing and reduces the risk of ankylosis (replacement resorption) which can occur if cementum is removed in the presence of active infection.
- Wait 3 months; redress canals and repeat periodontal treatment until the prognosis is clear.
- Ensure interim restorations are cleansable.
- Complete endodontic treatment only once a favorable prognosis is established.
Management of concurrent periodontal and endodontic lesions with communication requires long-term monitoring, often up to 6 months, to assess healing.

Clinical and Radiographic Monitoring36
Monitoring involves periapical radiographs and potentially 3D CT scans to track bone lesions and gingival inflammation during the healing phase.
Clinical Decision Making
If healing is observed during the monitoring phase, complete the root canal treatment. If no improvement is seen, consider redressing the canals or proceeding with extraction.
 |  |
 |  |
Factors Influencing Prognosis37
Periodontal prognosis can be difficult to determine initially and depends on:
- Cause of disease and remaining tooth structure.
- Amount of attachment loss and mobility.
- Root anatomy, furcation involvement, and healing response.
- The periodontal healing response is often the most difficult factor to predict and typically determines the ultimate success of the tooth.
- Oral hygiene and compliance with Supportive Periodontal Therapy (SPT).
- Restoration longevity and clinician skill.
Regenerative Therapy and Alternative Surgical Options
Periodontal Regeneration Research38
Study: Periodontal regeneration versus extraction and prosthetic replacement of teeth severely compromised by attachment loss to the apex (Cortellini et al. 2011).
Cortellini 2011 Study Details39
- Sample: 50 “hopeless” teeth with perio-endo lesions and/or attachment loss to the apex.
- Control Group (n=25): Extraction and replacement with fixed prosthesis or implants.
- Test Group (n=25): Regenerative strategy.
- Follow-up: 5 years.
Study Outcomes (Cortellini 2011)40
- Survival Rate: Similar between groups (92%–100%).
- Complication Rate: Similar between groups (16%–17%).
- Conclusion: Regenerative therapy can change the prognosis of a tooth from “hopeless” to fair or favourable, serving as a suitable alternative to extraction.
 |  |
Alternative Surgical and Prosthetic Options41
- Root resections (e.g., Langer et al. 1981).
- Hemisections or premolarization (with or without root removal).
- Hemisection or premolarization involves dividing a molar into two separate units to manage localized disease.
- Extraction without replacement or using the natural crown as a pontic.
- Fixed or resin-retained bridges, dentures, or implants.
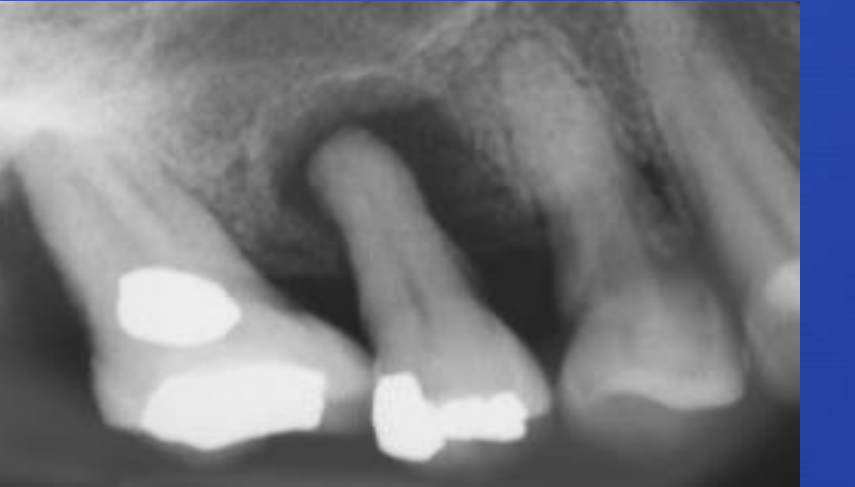
Case Study: Endo-Perio with Disto-Buccal (DB) Root Resection42
- Pre-operative: Lateral periodontal abscess buccal to UL6 and radiographic evidence of infection.
- Non-surgical Phase: Root canal treatment of UL6 with a composite plug in the disto-buccal canal.
- Surgical Phase: Resection of the disto-buccal root.
- Outcome: Post-operative radiographs and clinical presentation following successful root resection
Long-term Maintenance
With meticulous oral hygiene and regular Supportive Periodontal Therapy (SPT), teeth treated with root resection can maintain long-term stability.
 |  |  |
 |  |  |
Summary and Conclusions4344
 |  |
Final Summary45
- Accurate diagnosis is essential to determine the sequence of treatment and a reliable prognosis.
- Always get a periodontal opinion early to ensure the tooth is "savable" before investing in complex endodontics.
- For communicating lesions, endodontic treatment should begin at least 4 weeks before periodontal therapy.
- Success often depends on periodontal healing; early periodontal consultation is recommended to optimize outcomes and manage patient expectations.
References and Exam Study Materials
Core Textbooks and Classifications46
- Lindhe (7th Ed):
- Volume 1, p 475-481
- EFP New classification: Systemic and other periodontal conditions, Endo-periodontal conditions
- Linde (Decision trees)
Journal Articles
- Dental Update: Assessment and management of Endo-Periodontal Lesions — Hoyle et al, 2019; 46:930-941
- Cortellini et al. (2011): Regenerative therapy vs. extraction
- Dental Update: Recommended for easy-to-read summaries of endo-perio topics
The Periodontal–Endodontic Controversy47
Gerald W. Harrington, David R. Steiner & William F. Ammons, Jr
Over the past century, the dental literature has consistently reflected a controversy related to the effect of periodontal disease on the dental pulp and, more recently, the effect of pulpal necrosis on the initiation and progression of marginal bone loss. Two basic questions have been raised:
- Is periodontal disease a cause of pulp necrosis?
- Can a pulpless tooth be the cause of periodontal disease?
The answers to these questions are of clinical importance for treatment planning, such as determining if root canal treatment should be carried out prophylactically for teeth with advanced periodontal disease, or if a pulpless tooth should be replaced with an implant.
 |  |
THANK YOU
Footnotes
-
Original PDF page 1: L3 endo-perio, p.1 ↩
-
Original PDF page 2: L3 endo-perio, p.2 ↩
-
Original PDF page 3: L3 endo-perio, p.3 ↩
-
Original PDF page 4: L3 endo-perio, p.4 ↩
-
Original PDF page 6: L3 endo-perio, p.6 ↩
-
Original PDF page 5: L3 endo-perio, p.5 ↩
-
Original PDF page 7: L3 endo-perio, p.7 ↩
-
Original PDF page 8: L3 endo-perio, p.8 ↩
-
Original PDF page 9: L3 endo-perio, p.9 ↩
-
Original PDF page 10: L3 endo-perio, p.10 ↩
-
Original PDF page 11: L3 endo-perio, p.11 ↩
-
Original PDF page 12: L3 endo-perio, p.12 ↩
-
Original PDF page 13: L3 endo-perio, p.13 ↩
-
Original PDF page 14: L3 endo-perio, p.14 ↩
-
Original PDF page 15: L3 endo-perio, p.15 ↩
-
Original PDF page 16: L3 endo-perio, p.16 ↩
-
Original PDF page 17: L3 endo-perio, p.17 ↩
-
Original PDF page 18: L3 endo-perio, p.18 ↩
-
Original PDF page 19: L3 endo-perio, p.19 ↩
-
Original PDF page 20: L3 endo-perio, p.20 ↩
-
Original PDF page 21: L3 endo-perio, p.21 ↩
-
Original PDF page 22: L3 endo-perio, p.22 ↩
-
Original PDF page 23: L3 endo-perio, p.23 ↩
-
Original PDF page 24: L3 endo-perio, p.24 ↩
-
Original PDF page 25: L3 endo-perio, p.25 ↩
-
Original PDF page 26: L3 endo-perio, p.26 ↩
-
Original PDF page 27: L3 endo-perio, p.27 ↩
-
Original PDF page 28: L3 endo-perio, p.28 ↩
-
Original PDF page 29: L3 endo-perio, p.29 ↩
-
Original PDF page 30: L3 endo-perio, p.30 ↩
-
Original PDF page 31: L3 endo-perio, p.31 ↩
-
Original PDF page 32: L3 endo-perio, p.32 ↩
-
Original PDF page 33: L3 endo-perio, p.33 ↩
-
Original PDF page 35: L3 endo-perio, p.35 ↩
-
Original PDF page 34: L3 endo-perio, p.34 ↩
-
Original PDF page 36: L3 endo-perio, p.36 ↩
-
Original PDF page 37: L3 endo-perio, p.37 ↩
-
Original PDF page 38: L3 endo-perio, p.38 ↩
-
Original PDF page 39: L3 endo-perio, p.39 ↩
-
Original PDF page 40: L3 endo-perio, p.40 ↩
-
Original PDF page 41: L3 endo-perio, p.41 ↩
-
Original PDF page 42: L3 endo-perio, p.42 ↩
-
Original PDF page 46: L3 endo-perio, p.46 ↩
-
Original PDF page 47: L3 endo-perio, p.47 ↩
-
Original PDF page 43: L3 endo-perio, p.43 ↩
-
Original PDF page 44: L3 endo-perio, p.44 ↩
-
Original PDF page 45: L3 endo-perio, p.45 ↩