Periodontal Considerations for Direct and Indirect Restorations
Course Presenters1
- **Associate Professor Leticia A Miranda
- Speaker A: Primary Lecturer (Periodontist)**
- **Dr Anna Hughes
- Speaker B/C/D: Student Interlocutors**
The Interdisciplinary Relationship Between Periodontics and Restorative Dentistry23
Comprehensive dental therapy is founded on teamwork. An interdisciplinary approach is mandatory in modern dentistry.
Holistic Approach
Comprehensive dental therapy requires a holistic view of the patient where both disciplines are integrated into treatment planning, execution, and maintenance.
Periodontics and Restorative/Prosthodontics share an intimate and inseparable relationship in:
- Treatment planning
- Execution of procedures
- Achievement of outcomes
- Long-term maintenance
 |  |
Rationale for Interdisciplinary Integration4
- Periodontal Treatment Goals: Aims to control biofilm and inflammation to prepare sites for ideal prosthetic work. This provides a solid foundation for successful outcomes and aids in the longevity of restorations.
- Prosthodontic Goals: Aims to achieve proper restorative margins, shapes, and contacts to obtain harmony between the periodontium and reconstructions.
(Hsu et al. 2015)
The relationship between Periodontics and Restorative/Prosthodontics is not an “either/or” choice; successful clinical outcomes require the integration of both disciplines.
**Core Lecture Objectives5
- Impact of Periodontal Health on Restorative Therapy
- Impact of Restorative Factors on Periodontal Health
- Margins (location and fit)
- Biological width or supracrestal attachment maintenance
- Note: This is now formally referred to as "Supracrestal Attached Tissue"
- Contours
- Surface finish
Additional Considerations
- Proximal relationships (contact point/papillary relationship)
- Retraction techniques and the periodontium
- Trauma from occlusion
- Management of the reduced periodontium
Impact of Periodontal Health on Restorative Therapy
Periodontal health is the sine qua non—a prerequisite—of successful comprehensive dentistry.
To achieve long-term therapeutic targets of comfort, good function, treatment predictability, longevity, and ease of restorative and maintenance care, active periodontal infection must be treated and controlled before the initiation of restorative, aesthetic, and implant dentistry.
Prerequisites for Successful Comprehensive Dentistry6
(Melnick & Takei, 2019)
Consequences of Uncontrolled Periodontal Disease
Clinical Requirements for Control7
Active disease and contributing factors should be controlled before Prosthodontic treatment, ensuring:
- Biofilm control compatible with health
- Absence of inflammatory signs
- Absence of progressing attachment loss
- Reduction in probing depths
- Stability of attachment levels and pocket depths
- Resolution of inflammation to prevent tissue shifting after restorations are placed
Risks of Uncontrolled Disease
If periodontal disease is not controlled, long-term consequences may include:
- Progressive attachment loss and tooth loss
- Soft tissue changes resulting in impaired aesthetic outcomes
- Soft tissue changes (recession) that impair aesthetic outcomes, especially in the "aesthetic zone"
- Compromised prognosis for both individual teeth and the overall dentition
Site Preparation and Maintenance
- Soft and hard tissue management (e.g., soft tissue grafts, bone augmentation) to prepare sites for Prosthodontic treatment.
- Implementation of a structured maintenance program.
Clinical Benefits of Pre-Restorative Periodontal Stability
Predictability and Stability8
- Hemorrhage Control: Tissues that do not bleed during restorative manipulation allow for a more predictable restorative and aesthetic result.
- Healthy tissues do not bleed during manipulation, allowing for more accurate impressions and predictable aesthetic results.
- Margin Stability: Periodontal treatment is undertaken to ensure the establishment of stable gingival margins before tooth preparation.
- Tissue Integrity: Non-inflamed, healthy tissues are less likely to change (e.g., shrink) as a result of subgingival restorative treatment or post-restoration periodontal care.
Impact on Prosthetic Design9
Periodontal therapy should antecede restorative care because the resolution of inflammation may result in the repositioning of teeth or in soft tissue and mucosal changes. Failure to anticipate these changes may interfere with prosthetic designs planned or constructed before periodontal treatment. - Resolution of inflammation can lead to changes in mucosal texture.
Access and Retention
Certain periodontal procedures are designed to provide:
- Adequate tooth length for retention
- Access for tooth preparation and impression making
- Proper finishing of restorative margins
- Periodontal procedures (like crown lengthening) provide the necessary tooth length for retention and better access for preparation and finishing.
Failure to complete these procedures before restorative care can add to the complexity of treatment and introduce unnecessary risk for failure.
Impact of Restorative Factors on Periodontal Health
Plaque Retention and Inflammation10
- Overhanging restorations hinder plaque removal and predispose the site to periodontal inflammation (Lang et al. 1983, Pack et al. 1990, Jansson et al. 1994, Matthews & Tabesh 2004).
- Dental restorations, if poorly designed or compromised, may be predisposing factors by retaining or hindering the removal of plaque.
Defective Restorations and Overhangs11
Microbiological Shifts
- An association between overhang restorations and a shift to more virulent microflora and increased gingivitis has been demonstrated (Lang et al. 1983).
Clinical Management of Overhangs
Adjusting overhangs is difficult; specialized equipment like reciprocating handpieces may be needed, or the restoration may require replacement.
Defective restorations (overhangs, poor contacts, deficiencies) contribute to the establishment and progression of periodontal disease by:
- Increasing plaque accumulation
- Invading the biological width
Location of Restorative Margins12
One of the most important aspects of understanding the periodontal–restorative relationship is the location of the restorative margin relative to the adjacent gingival tissue. Margins are classified as:
- Subgingival
- Equigingival
- Supragingival

Supracrestal Attached Tissues and Biologic Width
The biologic width is defined as the dimension of the soft tissue attached to the portion of the tooth coronal to the crest of the alveolar bone.
Definition and Dimensions of Biologic Width13
It is comprised of:
- Epithelial attachment
- Connective tissue attachment
Gargiulo (1961) Average Measurements
- Sulcus Depth: 0.69 mm
- Length of Epithelial Attachment: 0.97 mm
- Connective Tissue Attachment: 1.07 mm
- Total Biologic Width: 2.04 mm
(Journal of Periodontology. 1961;32(3):261-7)
Variability in Dimensions
According to Schmidt et al. (2013):
- Mean values of the biologic width ranged from 2.15 to 2.30 mm.
- Large intra- and inter-individual variances were observed, with a range of 0.2 to 6.73 mm.
Conclusion: No universal dimension of the biologic width appears to exist.
(J Clin Periodontol 2013; 40: 493–504)

Function and Anatomy of the Natural Seal1415
The biologic width creates a natural seal (cuff) around teeth, protecting them from microbial invasion and traumatic insult. This biological width should not be violated.
The biologic width, also referred to as supra-crestal tissue attachment, is composed of:
- Junctional epithelium: Attached via hemidesmosomes.
- Connective tissue: Comprised of gingival fibers.
Anatomical Components
- Gingiva
- Junctional epithelium
- Connective tissue attachment
- Periodontal ligament
- Cementum
- Alveolar bone
2017 World Workshop Classification
According to the Classification of Periodontal and Peri-Implant Diseases and Conditions (Workgroup 1), the term “Biologic Width” is now formally referred to as Supra-crestal attached tissues.

Clinical Consequences of Biologic Width Violation1617
Violation of the biologic width triggers an inflammatory process as the body attempts to move apically and restructure lost dimensions. Consequences include:
- Chronic inflammation that does not resolve with oral hygiene alone
- Uncontrolled bone loss as the body attempts to recreate the necessary space
- Microbiota shift
- Tissue inflammation
- Attachment and bone loss
- Gingival recession
(Parma-Benfenati et al. 1985)
Clinical evidence demonstrates that violation of the Biologic Width (Supra-crestal Attached Tissues - SCAT) leads to localized periodontal destruction.
Determinants of Margin Location
- Extension of damage (caries/fracture)
- Retention and resistance form
- Aesthetics
Risks of Subgingival Margins
- Associated with increased plaque accumulation, gingival inflammation, and pocket formation (de Waal & Castellucci 1994, Schatzle et al. 2001).
- May cause damage to the attachment apparatus by violating the biological width (Tarnow et al. 1986, Tal et al. 1989).
Clinical Recommendations
- Supragingival margins should be chosen whenever possible.
- Subgingival margins already in place may require surgical crown lengthening to re-expose the margin (Padbury et al. 2003).
The significance of maintaining Supra-crestal Attached Tissues (SCAT) is paramount for long-term periodontal stability.
Violation of the attachment often results in:
- Alveolar bone loss
- Formation of pathological pockets
- Chronic inflammation
Aesthetic Failures
Encroachment on the attachment leads to alveolar bone loss and recession of the Free Gingival Margin (FGM), resulting in poor aesthetic outcomes.
Clinical Challenges
Subgingival restorations often present the following complications:
- Persistent plaque accumulation
- Chronic inflammation
- Recurrent caries
- Difficulty in obtaining accurate impressions
 |  |
Evidence of Adverse Effects from Subgingival Restorations
Parma-Benfenati (1986)18
- Study Model: Beagle dogs
- Method: Restorative margins placed at the level of the alveolar crest.
- Results: Observed gingival inflammation and loss of attachment.
- Finding: Approximately 5 mm of osseous resorption occurred.
Animal Studies on Osseous Resorption
(International Journal of Periodontics & Restorative Dentistry 6, 65–75)
Human Longitudinal and Microbiological Studies
Broadbent (2006)
- Study Type: Long-standing cohort study in New Zealand (884 members).
- Findings: Where a caries or restorative event occurred on an inter-proximal surface, attachment loss at that site was approximately twice as likely to be ≥3 mm compared to sound adjacent surfaces.
(J Clin Periodontol, 2006, 33(33), 803-10)
Schatzle M, Lang NP (2000)
- Study Type: 26-year longitudinal study.
- Comparison: Periodontal parameters of subgingival vs. supragingival margins.
- Findings: Confirmed detrimental effects of subgingival margins on gingival and periodontal health.
- Timeline: Increased loss of attachment is a slow process, typically detected clinically 1 to 3 years after restoration placement.
(J Clin Periodontol 2000; 28: 57–64)
Flores De-Jacoby (1989)
- Study Type: Microbiological analysis.
- Findings: Subgingival margins showed increased plaque scores, gingival scores, and probing depths.
- Microflora: Higher concentrations of spirochetes, fusiforms, rods, and filamentous bacteria were associated with subgingival margins.
(Int J Periodontics Restorative Dent. 1989;9:197-05)
Clinical Management of Restorative Margins
- Always aim for supragingival restorative margins.
- In the aesthetic zone, it is suggested that restorative margins should not be placed more than 0.5 mm below the gingival tissue (Nevins 1984).
Guidelines for Margin Placement19
(The International Journal of Periodontics & Restorative Dentistry. 1984;4(3):30-49)
Supragingival Location20
Ideal for periodontal health as it is easy to clean and does not interfere with Supra-crestal Attached Tissues (SCAT). Modern translucent materials and adhesive dentistry often allow for supragingival placement even in aesthetic areas.
Equigingival Location
Margins placed at the level of the gingival crest.
Subgingival Location Requirements
If subgingival margins are required, the following must be observed:
- Conservative subgingival extension.
- Sufficient width of Keratinized Tissue (KT) (at least 2 mm, including 1 mm of attached gingiva).
- Smooth restorative surfaces with properly finished margins.
- Avoidance of Biologic Width (BW) breach.
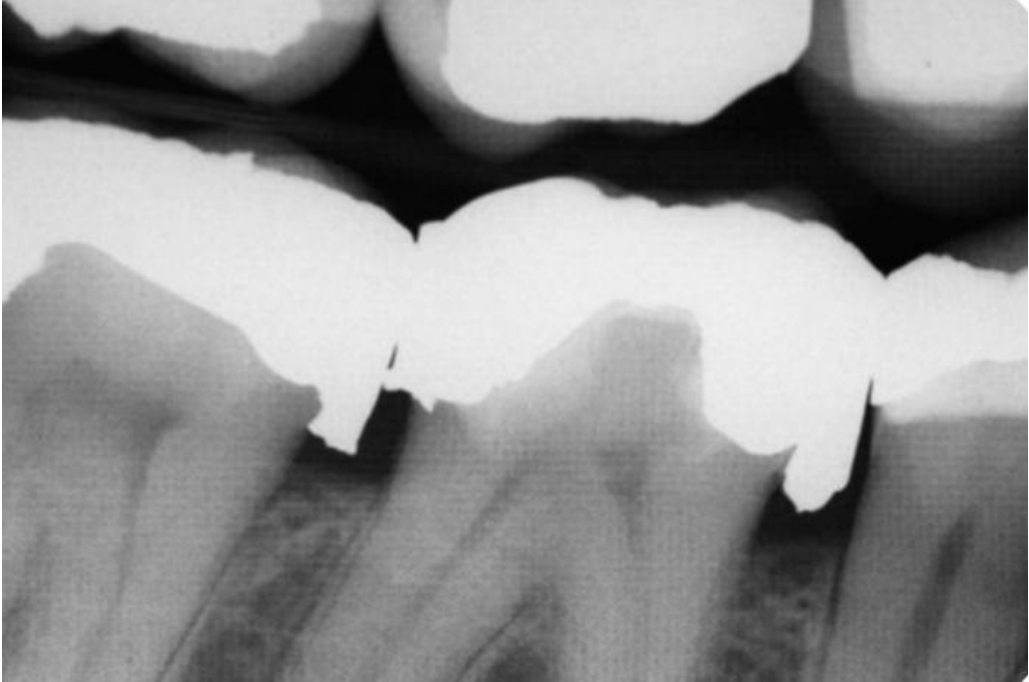
Indications for Subgingival Margins21
Subgingival margins may be necessary in the following clinical situations:
- Subgingival caries
- Tooth fractures
- Root resorption
- Perforations
- Existing subgingival preparations
- Short clinical crowns requiring increased retention
- Aesthetic requirements
Limitations of Simple Tissue Removal22
Using a bur, scalpel, laser, or electrosurgery to “snip off” gingiva for access is often insufficient because:
- The restoration becomes supragingival only temporarily.
- The Free Gingival Margin (FGM) will grow back, returning the restoration to a subgingival position.
- The SCAT space remains invaded, and margins remain in close proximity to the alveolar bone.

Surgical and Orthodontic Treatment Options232425
To manage subgingival margins effectively, the following treatment options are available:
- Surgery (with or without osseous recontouring)
- Orthodontic extrusion
- A combination of both
 |  |  |
 |  |  |
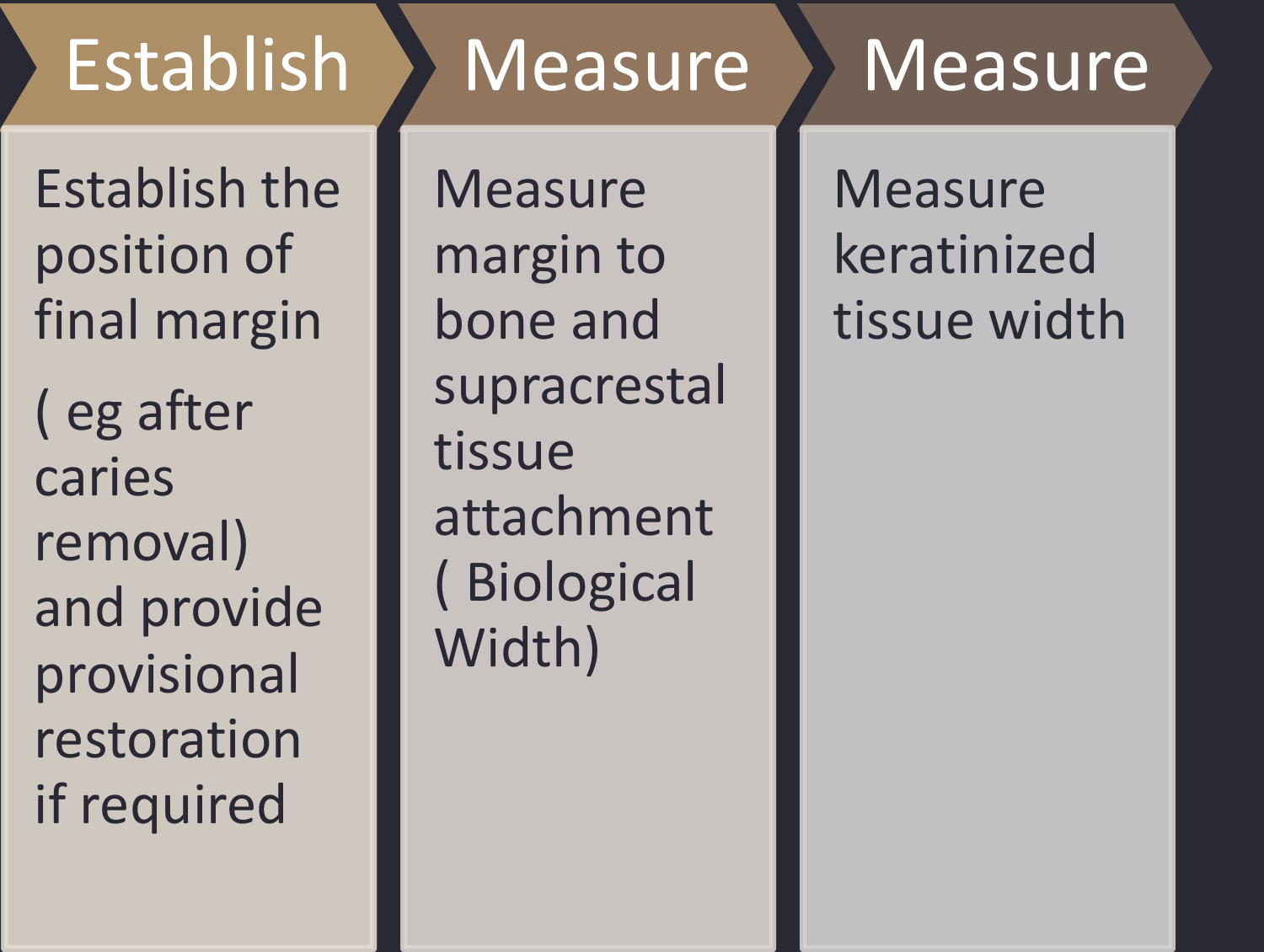
Clinical Assessment Steps26
- Establish Position: Determine the final margin position (e.g., after caries removal) and provide a provisional restoration if required.
- Measure BW: Measure the distance from the margin to the bone and assess the supracrestal tissue attachment.
- Assess KT: Measure the width of the keratinized tissue.
Management Guidelines (Carvalho et al. 2016)27
If No BW Invasion:
- Adequate KT: Gingivectomy or flap with marginal excision (no osteotomy).
- Inadequate KT: Apically positioned flap (no osteotomy).
If BW Invasion is Present:
- Adequate KT: Flap with marginal excision and osteotomy.
- Inadequate KT: Apically positioned flap and osteotomy.
Note: Orthodontic extrusion is also a viable alternative for managing BW invasion.
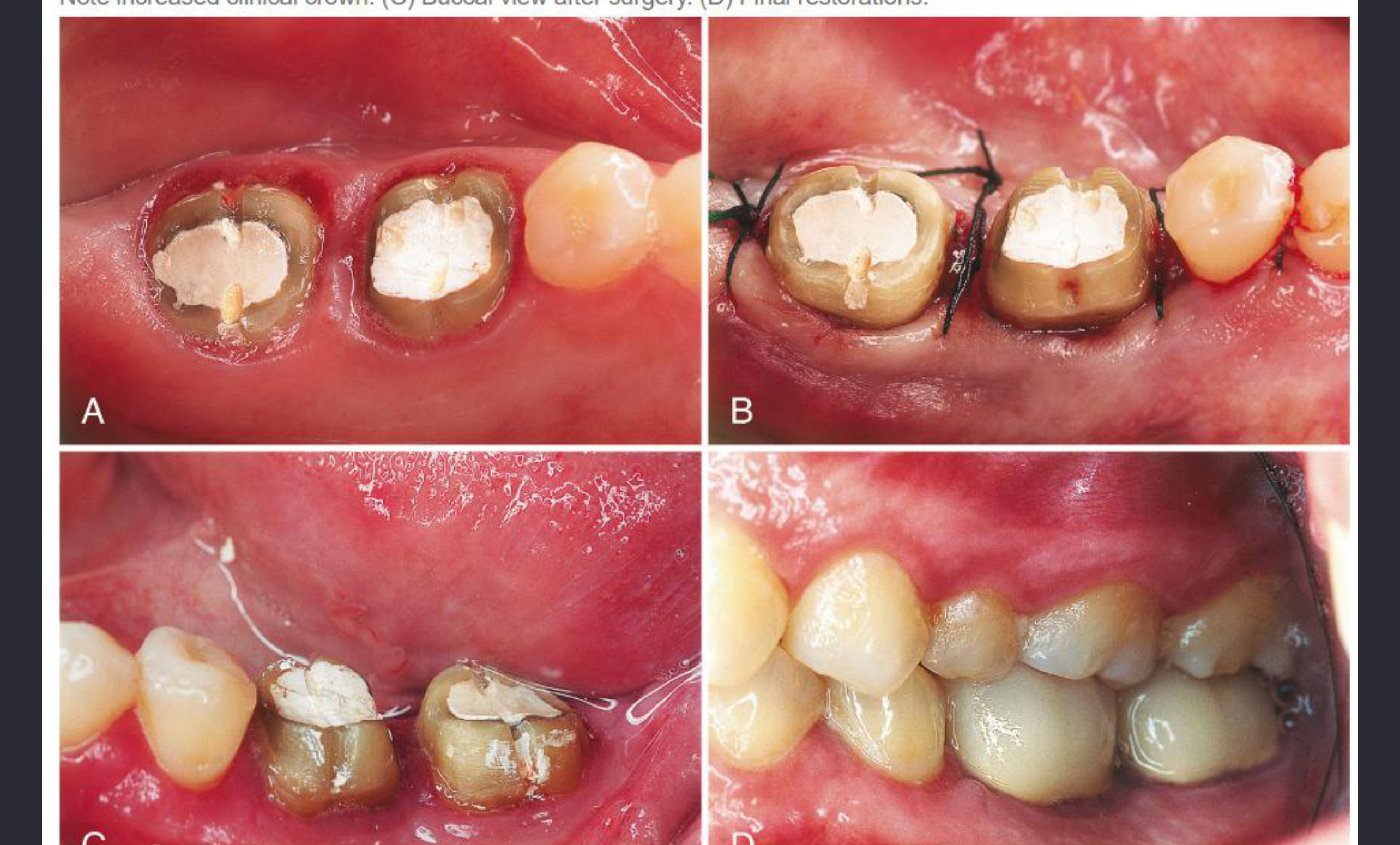
Orthodontic extrusion can effectively change the position of the restorative margin from subgingival to supragingival by moving the tooth structure coronally.
Clinical cases demonstrate the efficacy of combined periodontal and orthodontic approaches in managing compromised tooth structure.
 | |
Crown Lengthening Procedures
Crown lengthening is a procedure involving the controlled displacement of the alveolar bone, the supra-crestal attached tissues (Connective Tissue and Junctional Epithelium), and the Free Gingival Margin (FGM).
Definition and Diagnostic Measurements2829
Goal: To allow for supragingival placement of a restoration with minimum future changes in the surrounding periodontium.
In the early stages of restorative treatment planning, crown lengthening should be recommended if the clinician anticipates that the final restoration margin will be subgingival or in close proximity to the alveolar bone crest.
Diagnostic Methods for Measuring BW
- Transgingival/Periodontal Probing: Performed under anesthesia to identify the Cemento-Enamel Junction (CEJ) and Bone Crest (COA
- ==Bone Sounding: Probing under local anesthesia to the bone crest to measure the existing biological width.==).
- Radiographic Evaluation: Periapical (PA) radiographs or CBCT.
Clinical Benchmarks
- Sulcus/Junctional Epithelium: Typically measures ~2 mm.
- Total Supracrestal Attachment (including CT): Typically measures ~3 mm.
Indications for Flap and Osseous Surgery
A flap procedure and osseous recontouring are required for crown lengthening when there is:
- Less than 3 mm of soft tissue between the bone and the planned gingival margin.
- Less-than-adequate attached gingiva.
Surgical planning must account for the biological requirements of the soft tissue seal to prevent chronic inflammation post-restoration.
Aesthetic crown lengthening is utilized to correct “gummy smiles” or uneven gingival levels, ensuring the clinical crown height is harmonious with facial aesthetics.
Pre-surgical assessment must include an evaluation of the biological width to ensure the resulting gingival architecture remains stable over time.
Keratinized Tissue (KT) Considerations
A lack of KT can lead to difficulty in cleaning and increased susceptibility to recession, especially around restorative margins.
Surgical Techniques and Healing Timelines30
Surgical Techniques
- Soft Tissue Only (Gingivectomy): Indicated when there is no BW invasion and sufficient attached gingiva exists.
- Soft and Hard Tissue (Gingivectomy and Osteotomy): Indicated when BW invasion is present or expected.
Healing Timelines
Final restoration should be delayed to allow for tissue stabilization:
- Minimum: 3 months
- Ideal: Up to 6 months
(Lanning et al. 2003, Pontoriero et al. 2001, Bragger et al. 1992)
Crown lengthening procedures result in an increased clinical crown height, providing the necessary tooth structure for stable final restorations.
Apically Repositioned Flap
This technique is used if insufficient keratinized tissue is present. It involves: - ==Apically Repositioned Flap (ARF): Used when keratinized tissue is thin; preserves the existing gingiva.==
- Elevating a mucoperiosteal flap.
- Bone recontouring.
- Repositioning the flap to cover the alveolar bone while preserving or increasing the zone of attached gingiva.
Aesthetic Crown Lengthening
A female patient presented with a "gummy smile" and short clinical crowns. The lecturer performed extensive soft tissue and bone removal. Because the patient had a thin phenotype, an apically displaced flap was used rather than a simple gingivectomy to preserve the zone of keratinized tissue. Final veneers were delayed for six months to ensure the gingival margins had stabilized.
Restorative Design and Material Considerations
Impact of Poor Adaptation31
Poorly adapted restorations produce an inflammatory response in the periodontium. Open margins (even those measuring several tenths of a millimeter) can harbor large numbers of bacteria.

Biofilm Formation
Marginal Fit and Biofilm Formation
Confocal laser scanning microscopy (CLSM) and SEM imaging confirm the formation of biofilms at the interface between restorations and tooth structure, even in areas with low accessibility to nutrients and oxygen.
- Precise marginal fit is essential to prevent a shift toward pathogenic microflora.
(The Journal of Prosthetic Dentistry: Torresyap, Moshaverinia, & Chee)
Crown Contours and Plaque Accumulation
Ideal Crown Contours32
Crown contours should:
- Provide protection of gingival margins.
- Allow for the cleansing action of the musculature.
- Facilitate access for oral hygiene.

Risks of Overcontouring
Overcontouring has negative effects on the periodontium due to plaque accumulation. This should be mitigated by ensuring adequate tooth reduction for the specific restorative material being used.
Bulky Crowns
Bulky crowns, often resulting from insufficient tooth reduction, significantly hinder plaque removal and lead to accelerated periodontal breakdown.
Surface Finish and Material Roughness
Plaque Retention and Roughness33
Every restorative material has a different capacity for retaining plaque based on surface roughness and surface free energy (Bollen et al. 1997, Ababnaeh et al. 2011).
-
Rough Surfaces: Especially on interproximal and marginal areas, these act as predisposing factors for plaque accumulation and periodontal destruction (Pneumas et al. 1998, van Dijken et al. 1987).
-
Material Specifics: Highly glazed porcelain is less plaque-retentive than enamel. Conversely, metal pontics or composite restorations tend to encourage plaque formation (Wise & Dykema 1975
Conclusion and Summary3435
For restorations to survive long-term, the periodontium must remain healthy so that the teeth are maintained. Restorations must be critically managed in several areas—margins, contours, and surface finish—to ensure they exist in harmony with the surrounding periodontal tissues.
Key Requirements for Restoration Longevity
- ==Establishing health before restorative work==
- Respecting the supracrestal tissue attachment (biologic width)
- Ensuring smooth, well-contoured, and well-fitted margins
- Ongoing maintenance and monitoring
The successful integration of periodontal health and restorative excellence is the foundation of modern interdisciplinary dentistry.
 |  |
Reading Resources and References
2017 World Workshop36
- Dental prostheses and tooth-related factors
- Authors: Carlo Ercoli and Jack G. Caton
- Source for the new classification: "Supracrestal Tissue Attachment" replacing "Biologic Width."
- Updated Periodontal Classifications (Stages I-IV, Grades A-C).
- Authors: Carlo Ercoli and Jack G. Caton
 |  |
Clinical Research and Literature Reviews
-
Interdisciplinary interface between fixed prosthodontics and periodontics
- Authors: Jafaar Abduo and Karl M. Lyons
-
The periodontal restorative interface: esthetic considerations
- Authors: Vincent Bennani, Hadeel Ibrahim, Latfiya Al-Harthi, and Karl M. Lyons
Case Study: Non-Functional Third Molar (Patient Scenario)
An 87-year-old patient presented with a carious upper third molar (28) that has no opposing tooth and is non-functional.
- Lecturer's Advice: The tooth is likely "irrationally" treated if restored.
- Given the patient's age and the fact that the caries may be affecting the adjacent tooth, extraction is likely the best option.
- Surgical risks like sinus involvement or hypercementosis should be managed by oral surgery.
- Restoration would likely require crown lengthening, which is inappropriate for this clinical scenario. - Gargiulo (1961): Dimensions of the dentogingival junction. - Carvalho et al. (2016): Management guidelines for restorative margins. - Parma-Benfenati (1986): Impact of subgingival margins on bone.
Footnotes
-
Original PDF page 1: L4 Perio resto, p.1 ↩
-
Original PDF page 2: L4 Perio resto, p.2 ↩
-
Original PDF page 4: L4 Perio resto, p.4 ↩
-
Original PDF page 3: L4 Perio resto, p.3 ↩
-
Original PDF page 5: L4 Perio resto, p.5 ↩
-
Original PDF page 6: L4 Perio resto, p.6 ↩
-
Original PDF page 7: L4 Perio resto, p.7 ↩
-
Original PDF page 8: L4 Perio resto, p.8 ↩
-
Original PDF page 9: L4 Perio resto, p.9 ↩
-
Original PDF page 10: L4 Perio resto, p.10 ↩
-
Original PDF page 11: L4 Perio resto, p.11 ↩
-
Original PDF page 12: L4 Perio resto, p.12 ↩
-
Original PDF page 13: L4 Perio resto, p.13 ↩
-
Original PDF page 16: L4 Perio resto, p.16 ↩
-
Original PDF page 17: L4 Perio resto, p.17 ↩
-
Original PDF page 20: L4 Perio resto, p.20 ↩
-
Original PDF page 21: L4 Perio resto, p.21 ↩
-
Original PDF page 27: L4 Perio resto, p.27 ↩
-
Original PDF page 31: L4 Perio resto, p.31 ↩
-
Original PDF page 32: L4 Perio resto, p.32 ↩
-
Original PDF page 33: L4 Perio resto, p.33 ↩
-
Original PDF page 34: L4 Perio resto, p.34 ↩
-
Original PDF page 35: L4 Perio resto, p.35 ↩
-
Original PDF page 38: L4 Perio resto, p.38 ↩
-
Original PDF page 39: L4 Perio resto, p.39 ↩
-
Original PDF page 36: L4 Perio resto, p.36 ↩
-
Original PDF page 37: L4 Perio resto, p.37 ↩
-
Original PDF page 40: L4 Perio resto, p.40 ↩
-
Original PDF page 41: L4 Perio resto, p.41 ↩
-
Original PDF page 49: L4 Perio resto, p.49 ↩
-
Original PDF page 51: L4 Perio resto, p.51 ↩
-
Original PDF page 52: L4 Perio resto, p.52 ↩
-
Original PDF page 53: L4 Perio resto, p.53 ↩
-
Original PDF page 54: L4 Perio resto, p.54 ↩
-
Original PDF page 55: L4 Perio resto, p.55 ↩
-
Original PDF page 56: L4 Perio resto, p.56 ↩