Restoration of Endodontically Treated Teeth1
This document provides comprehensive guidelines and clinical considerations for the restoration of teeth following endodontic therapy.
Lecture 1: Introduction2
Oral Health Centre of Western Australia
Foundational Principles
The restoration of endodontically treated teeth requires understanding that most failures result not from inherent brittleness of the root-filled tooth, but from loss of tooth structure and compromised stress distribution. The primary therapeutic goals are to protect remaining tooth structure, achieve an excellent coronal seal, and design the restoration around sound biomechanical principles.
- Restorability and prognosis: Assessing whether the tooth can be successfully restored
- Preservation of dentin: Especially in the cervical (peri-cervical) area
- Ferrule creation: Establishing a circumferential collar of sound dentin where possible
Lecture Scope
This lecture establishes the foundation for decision-making before discussing specific post systems and techniques. Key areas covered include assessing restorability, identifying factors that most strongly predict survival, and understanding the biomechanical concepts that guide coronal restoration after root canal treatment.
Learning Outcomes3
By the end of this lecture, you should be able to:
- Understand the changes in the tooth structure after root canal treatment
- Discuss the factors that make endodontically treated tooth more susceptible to fracture
- Discuss restorative options for endo treated tooth (with and without a post)
- Discuss the function, indication, importance and clinical application of posts
- Understand and describe the concept of Ferrule and discuss the importance of the ferrule effect
- Understand the factors that affect the ferrule and the longevity of endodontically treated teeth
- Define key terms: post, core, ferrule, and peri-cervical dentin
- Conduct a structured assessment of:
- Endodontic readiness (healing status)
- Periodontal support
- Remaining tooth structure
- Occlusal risk factors
- Connect biomechanical principles to practical treatment planning, including:
- Justifying the need for cuspal coverage
- Explaining why ferrule matters significantly more than post selection
- Understanding why posts primarily provide retention for the core rather than strengthening roots
- Managing cases with limited ferrule
- Understanding how different restorative choices influence failure patterns
What Is Post and Core Restoration
- A post is typically made of metal or fibre-reinforced composite and is placed into a prepared root canal of a natural tooth.
- Together with a core, it provides retention (and some resistance form) for a definitive coronal restoration (e.g., crown).
- Posts may also support attachment systems and serve as a foundation for overdenture post–copings where indicated.
Post Definition and Purpose
A post is a component (typically metal or fiber-reinforced composite) placed within the prepared root canal space. Its primary function is to retain the core when there is insufficient coronal tooth structure remaining.
Critical misconceptions to avoid:
- ==Posts do not reinforce or strengthen the root==
- ==Posts are not routine for every root canal-treated tooth==
- ==Post placement can actually increase stress within root dentin if excessive dentin is removed during canal enlargement or over-preparation==
Clinical Principle: Consider the post as a retentive anchor for the core, used only when necessary and only after planning how to preserve dentin and create adequate ferrule.
Post Definition and Purpose4
Core Definition and Role5
A core is a foundation restoration that replaces missing coronal tooth structure.
- It rebuilds coronal anatomy to support the definitive restoration (e.g., crown/onlay) and helps establish proper form, contour, and occlusion.
- A core may be placed in vital or endodontically treated teeth.
- It should provide adequate retention and resistance form, while preserving remaining tooth structure.
- ==Materials: May include composite, amalgam, or other buildup materials.==
Key Principle
The core should be well-retained, well-sealed, and conserve remaining dentin. The tooth structure and ferrule provide most of the fracture resistance; the core mainly restores shape and retention for the final crown.
Treatment Planning Process6
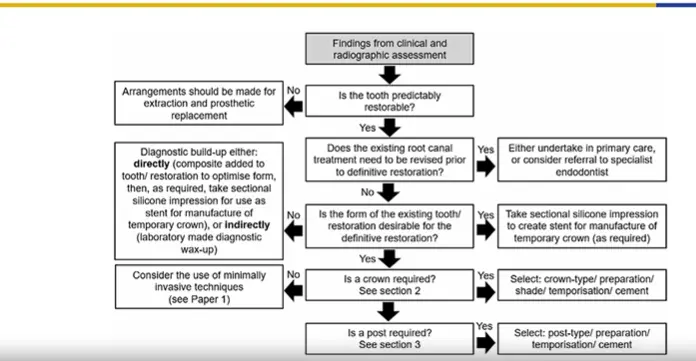
Clinical Decision Flowchart (R. J. R. Smith et al)
- Assessment: Findings from clinical and radiographic assessment.
- Restorability: Is the tooth predictably restorable?
- No: Arrange for extraction and prosthetic replacement.
- Yes: Proceed to Endodontic evaluation.
- Endodontic Status: Does the existing root canal treatment need to be revised?
- Yes: Undertake in primary care or refer to specialist.
- No: Proceed to Form evaluation.
- Form and Anatomy: Is the form of the existing tooth/restoration desirable for the definitive restoration?
- No: Perform diagnostic build-up (Directly via composite/stent or Indirectly via lab wax-up).
- Yes: Take sectional silicone impression for temporary crown stent.
- Coronal Restoration: Is a crown required?
- No: Consider minimally invasive techniques.
- Yes: Select crown type, preparation, shade, and cement.
- Post Requirement: Is a post required?
- Yes: Select post type, preparation, and cement.
Critical Decision Point
Determine early if the tooth is restorable and what procedures are required to make it restorable:
- Caries control
- Periodontal management
- Crown lengthening
- Orthodontic extrusion
Fundamental Concepts Prognosis7
- Properly treated, root-filled teeth can function long-term and serve as abutments.
- Restoration usually fails before the endodontic treatment fails.
- Survival is driven mainly by remaining tooth structure, presence of cuspal coverage, ferrule, occlusal loading, and quality of restoration.
Endodontic Readiness Biological Criteria8
Before definitive restoration, confirm:
- Adequate root canal filling and apical seal.
- No sinus tract, exudate, or persistent swelling.
- No tenderness to percussion or palpation.
- Radiographic healing or stability of periapical area.
- No unresolved procedural errors compromising prognosis.
Periodontal and Structural Readiness9
- Evaluate periodontal support and crown-to-root ratio.
- Check for mobility and furcation involvement.
- Assess presence and height of potential ferrule.
- Consider need for crown lengthening or orthodontic extrusion.
- Decide early if the tooth is restorable or if extraction/implant is preferable.
Detailed Assessment Protocol:
Periodontal evaluation:
- Mobility (shaking test)
- Furcation involvement
- Crown-to-root ratio
- Position of margin relative to bone and gingiva
Structural evaluation:
- Presence of cracks
- Undermined cusps
- Deep caries
- Insufficient axial wall height
Critical Requirement
Create a ferrule on sound dentin above the gingival margin without violating biological width. If ferrule is inadequate, plan early for crown lengthening or orthodontic extrusion.
Role of Tooth Type and Position10
- Anterior teeth: Often less axial load, but high esthetic and guidance demands.
- Often exposed to oblique forces, especially with deep bites, parafunction, or traumatic occlusion
- Require attention to ferrule location and palatal support
- Premolars: Small cross-section, susceptible to fracture (especially maxillary premolars).
- Molars: Larger roots and pulp chambers; often restored without posts using chamber retention.
- Frequently require cuspal coverage when significant structure is lost
- Prone to cuspal fracture when marginal ridges and cusps are weakened
- Experience higher vertical loads
- ==Posterior teeth:==
- Abutments: Teeth serving as abutments for FDP (Fixed Dental Prosthesis) or RPD (Removable Partial Denture) face higher functional demands.
- Require more robust restoration design
Remaining Tooth Structure Key Predictor11
- Height, thickness, and number of residual walls strongly influence survival.
- Studies show that teeth with substantial dentin height perform significantly better, independent of post type or crown material.
- Once remaining wall height is <2 mm, failure risk increases steeply.
Peri Cervical Dentin Why It Matters12
Critical Stress-Bearing Zone
- The peri-cervical dentin (~4 mm above and 4 mm below the crestal bone) is key for resisting bending and shear forces.
- Over-flaring and aggressive preparation in this region markedly reduce fracture resistance.
- When preparing post space, remove only what is necessary—avoid unnecessary enlargement that sacrifices peri-cervical dentin.
Mechanical Properties of Tooth Structure After Root Canal Treatment13
- Common belief: Endodontically treated teeth (ETT) are weaker because dentin becomes “brittle.”
- Evidence: Experimental studies show minimal change in dentin hardness/elastic modulus after RCT and dehydration.
- Any small changes are usually related to dehydration or aging, not the endodontic procedure itself
- Clinical Reality: Fracture risk rises mainly due to tooth structure loss (caries, restorations, access) and altered load paths.
- Specific structural losses include marginal ridges or cusps compromised during access preparation
- Conclusion: Treat ETT as structurally compromised and restore to protect remaining dentin.
Distinction Between Structural and Biological Weakness
Endodontically treated teeth are structurally compromised, not biologically weak. Restoration planning should also focus on controlling occlusal loading.
Why Dentin Properties Vary Even Without RCT14
- Non-uniformity: Dentin tubule density and orientation (crown, cervical, or root) affect stiffness and toughness.
- Stiffness and toughness are not uniform within the same tooth.
- Age and Sclerosis: Aging changes dentin behavior; it often becomes more mineralized and less compliant.
- Moisture: Dehydration can reduce toughness, but the impact is usually secondary to structural loss.
- Procedural Impact: Instrumentation, irrigants, and post preparation can affect surfaces; preserve dentin and minimize over-preparation.
Practical message
Conservative dentin management preserves dentin when it matters most. Avoid unnecessary enlargement. - These procedures may create defects or remove critical dentin.
The Main Biomechanical Problem After Root Canal Treatment15
Tooth Structural Loss
- Major contributors: Caries, existing restorations, access cavity, and loss of marginal ridges/cusps.
- Thin cusps and walls become stress concentrators where cracks initiate and propagate.
Clinical Assessment
When planning restoration, ask: ”What tooth structure is left? Where are the stress concentrators? How will my restoration reduce these stresses?”
- Goal of coronal restoration: Redistribute forces and protect weakened tooth structure.
- This is commonly achieved through rebuilding missing walls and providing cuspal coverage
Progression of Failure
- Tooth tissue loss: Access + caries + restorations
- Stress concentration: Thin walls/cusps + loss of marginal ridges
- Cracks / fracture: Catastrophic failure or repairable
Biomechanical Principles
- Preserve peri-cervical dentin (≈4 mm above and below the bone crest) to resist bending and shear.
- Remaining wall height, thickness, and number strongly predict survival, often independent of post type.
- When remaining wall height is <2 mm, failure risk rises steeply.
- A circumferential ferrule (often ~1.5–2 mm) improves fracture resistance and reduces catastrophic failures.
Priority
These biomechanical factors matter more than the choice of post material or cement. Before choosing a post system, ensure sufficient remaining dentin to create adequate ferrule.
Adequate ferrule design also shifts failure toward favorable (repairable) patterns.
Predictors of Survival16
Stress Distribution17
- Cervical Dentin: Finite element studies show cervical dentin often carries the highest stress under vertical loading.
- Post Influence:
- Under vertical load: Posts may shift some stress apically.
- Under oblique load: Posts may not reduce overall stress and can increase apical stress.
- Key Principle: Posts retain the core; they do not automatically “strengthen” roots
- Excessive dentin removal during post preparation can increase stress in apical or cervical regions.
- Priorities: Ferrule, conservative post preparation, and occlusal risk management.
- Durable canal seal
- Occlusal design that minimizes destructive lateral forces
Ferrule
A ferrule is a ring or cap, typically a metal one, which strengthens the end of a handle, stick, or tube and prevents it from splitting or wearing.
A ferrule is analogous to a reinforcing band that prevents a structure from splitting under load. In dentistry, it refers to the collar of sound dentin encircled by the crown margin.
Function: Provides a bracing effect that resists functional lever forces and reduces the tendency for root fracture.
Three critical dimensions to consider:
- Ferrule height
- Ferrule width (dentin thickness)
- Ferrule location
These dimensions are often more important than the post material selected.
Definition and General Concept18
Ferrule Effect and Diagram Explanation19
- Definition: A 360-degree metal collar of the crown surrounding the parallel walls of the dentine extending coronal to the shoulder of the preparation.
Clinical contrast: A tooth with an adequate dentin collar versus one without a ferrule demonstrates that when the crown margin sits on the core without surrounding dentin, the restoration is more vulnerable to debonding and catastrophic fracture.
- Mechanical Benefits:
- Increased resistance form.
- Decreased stress within the tooth (Tooth Protection).
- Components of the System:
- Crown
- Core
- Ferrule
- Post
- Gutta-percha
Ferrule Height20
- Minimum Ferrule Height: 1.5 – 2 mm.
- Determination: Based on the amount of sound tooth structure above the gingival margin.
- Biological Considerations: Requires at least 4 – 5 mm of tooth structure coronal to the bone crest (accounting for 2 – 3 mm of biological width).
This consists of:
- ==2–3 mm for subcrestal tissue attachment (biological width)==
- ==1.5–2 mm for ferrule height==
Clinical implication: You cannot discuss ferrule height without considering periodontal anatomy. If the tooth is too short, surgical crown lengthening or orthodontic extrusion may be necessary to gain sound structure safely.
- Clinical Rule: The greater the height of remaining tooth structure above the preparation margin, the better the fracture resistance (Akkayan B 2014).
Ferrule Width21
- Minimal Thickness: Remaining dentine should be 1 - 2 mm thick.
- Influencing Factors: The axial reduction of the crown preparation and the width of the post preparation determine the final ferrule width (dentin thickness).
Risk: Over-reduction on the outside and over-enlargement on the inside can leave a thin, fragile dentin ring.
Principle: Balance retention needs with conservation. The best ferrule consists of sound dentin, not a thin shell created by aggressive preparation.
Ferrule Location22
- Ideal: Circumferential ferrule (360 degrees).
- Barriers to Ideal Location:
- Caries
- Erosion and abrasion (more common on the buccal wall)
- Over-reduction during tooth preparation
- Clinical Guideline: An incomplete ferrule is a better option than a complete lack of ferrule.
Planning approach: Identify where dentin remains and position margins and preparation to maximize ferrule in high-stress areas.
Partial Ferrule in Anterior Teeth23
Influence of Location on Fracture Resistance
- The location of the ferrule is critical for fracture resistance.
- Maxillary Incisors: The palatal ferrule is the most important for providing longevity for the restoration.
Functional forces are typically oblique, and the palatal aspect serves as the key compression zone during loading.
Clinical strategy: When ferrule is limited, prioritize preserving or gaining dentin in areas that best resist functional loading for that specific tooth.
Clinical Significance of Adequate Ferrule24
Providing an adequate ferrule lowers the impact of the post and core system, luting agents, and the final restoration on overall tooth performance.
- ==Dominant factor: Ferrule dominates the biomechanics. A good ferrule can forgive variations in post type and cementation choice because the dentin collar performs most of the work in resisting lever forces.==
- ==Clinical takeaway: Before debating post brands, cements, or types, invest effort in creating sound dentin structure for a ferrule through conservative preparation, margin planning, or surgical/orthodontic procedures.==
Managing Absence of Ferrule25
If a tooth is deemed restorable but lacks structure for a ferrule, you must expose tooth structure above the gingival margin via:
Restorability Assessment
==First, reassess restorability. If prognosis is poor due to cracks, inadequate periodontal support, or unfavorable crown-to-root ratio, extraction may be the better option.==
- Crown lengthening: A surgical procedure.
- Orthodontic extrusion.
Crown Lengthening Versus Orthodontic Extrusion26
- Both procedures reduce root length.
- Surgical Crown Lengthening: Reduces root length (R’) and increases crown length (C’).
- Orthodontic Extrusion: May be limited by time and cost factors.
Case selection considerations:
- Periodontal biotype
- Smile line
- Root length and morphology
- Long-term restorative plan
Other Factors That Affect the Ferrule
- Anterior Teeth: Face oblique forces; influenced by deep bite, parafunction, and dietary habits.
- Posterior Teeth: Face vertical forces along the axis; influenced by group function and high cusps.
- Clinical Note: Non-desirable forces (interferences, poor occlusal design) are likely more critical for survival than the specific post and core system used
Key insight
Managing occlusal risk and designing restorations that minimize destructive forces is essential. .
Tooth Type and Load Direction27
Type of Post28
- Options: Pre-fabricated vs. Cast post and core.
- Current Trends: Literature favors bonded fiber-reinforced posts (pre-fabricated) over metal posts (cast).
- Failure Patterns: Fiber posts show more favorable failure patterns, fewer root fractures, and fractures that occur more occlusally
Important caveat
Case selection, ferrule presence, and remaining tooth structure strongly influence outcomes. .
- Priority: A 1.5–2 mm ferrule in sound tooth structure is more important for fracture resistance than post design or type.
Core Materials for Prefabricated Posts
Amalgam29
- Advantage: High compressive strength; good for posterior teeth.
- Disadvantage: Does not bond to tooth structure; requires retentive features (undercuts) that may weaken remaining walls.
Composite
- Advantage: Bonds to tooth structure (though dentin bonding is less reliable); modulus of elasticity is similar to dentin.
- Disadvantage: Technique sensitive; weak composite/tooth interface may compromise the restoration.
- Note: Some consider that composite may reinforce residual structure due to its bonded nature.
GIC30
- Primary Use: Used to block out undercuts in vertical walls (away from margins).
- Comparison: Amalgam and Composite remain the primary core materials for prefabricated posts
Selection criteria
Choose based on remaining structure, moisture control, time available, and planned definitive restoration.
Additional practical points:
- Avoid creating or deepening undercuts near the margin when building a core (can lead to thin walls and future fracture)
- If undercuts exist in vertical walls away from the margin, use glass ionomer base to block them before buildup
- Avoid additional retentive features (pins) as these may weaken tooth structure or create periodontal/aesthetic problems
- Modern approach prefers adhesive retention and conservative preparation over mechanical retentive devices .
Amalgam Coronal Radicular Dowel and Core Technique31
- Retention: Natural divergence of canals and undercuts in the pulp chamber provide extra retention.
- Requirement: Natural coronal structure is still necessary for resistance form and ferrule effect
Critical limitation
This technique still relies on remaining coronal tooth structure for resistance form and ferrule. It is not a substitute for adequate dentin or sound restorative planning. .
Clinical Technique
- Remove Gutta-percha (GP) from the pulp chamber and 2 to 4 mm into the canal.
- Maintain undercuts and divergence of canals.
- Remove unsupported tooth structures.
- Place matrix band.
- Condense amalgam into the cavity, starting from the root canal.
- Restore tooth anatomy.
- Perform crown preparation in the subsequent session.
References32
Endodontic and Prosthodontic Literature
- Akkayan B. An in vitro study evaluating the effect of ferrule length on fracture resistance of endodontically treated teeth restored with fiber-reinforced and zirconia dowel systems. J Prosthet Dent 2004; 92: 155-162.
- Barnes, J., Patel, S. Contemporary endodontics – part 1. Br Dent J 211, 463–468
- Bryant et al. Modulus of elasticity in bending of composites and amalgams. Journal Of Prosthetic Dentistry 1986
- Fusayama and Maeda. Effect of pulpectomy on dentin hardness J Dent Res. 1969
- Glossary of Prosthodontic Terms 4th ed
- Goodacre et al. The Prosthodontic Management of Endodontically Treated Teeth: A Literature Review. Part I. Success and Failure Data, Treatment Concepts. J Prosthod 1994;3:243-250.
- Gutmann The dentin-root complex: Anatomic and biologic considerations in restoring endodontically treated teeth. J PROSTHET DENT 1992;67:468-67
- Heifer et al. Determination of the moisture content of vital and pulpless teeth Oral Surg Oral Med Oral Pathol. 1972 Oct;34(4):661-70
- Huang et al. Effects of Moisture Content and Endodontic Treatment on Some Mechanical Properties of Human Dentin. Journal of Endodontics. 18(5), 1992.
- Juloski et al. Ferrule Effect: A Literature Review. Journal of Endodontics 38 (1)2012 (11-19)
- Juloski et al. Rethinking ferrule – a new approach to an old dilemma. British Dental Journal 2010; 209: 25–33
- Ko et al. Effects of post on dentin stress distribution in pulpless teeth J Prosthet Dent 1992
- Lewinstein and Grajower Root dentin hardness of endodontically treated teeth JOURNAL OF ENDODONTICS VOL 7, NO 9, SEPTEMBER 1981
- Nayyar et al. An amalgam coronal-radicular dowel and core technique for endodontically treated posterior teeth JOURNAL OF PROSTHETIC DENTISTRY 1980
- Ng et al Influence of remaining coronal tooth structure location on the fracture resistance of restored endodontically treated anterior teeth J Prosthet Dent 2006;95:290-6.
- Papa et al Moisture content of vital vs endodontically treated teeth. Endod Dent Traumatol. 1994 Apr;10(2):91-3.
- Randow K, Glantz PO. On cantilever loading of vital and non-vital teeth. An experimental clinical study. Acta Odontol Scand 1986;44:271–7
- Rosenstiel et al. Contemporary Fixed Prosthodontics 4th ed
- Sedgley et al. Are Endodontically Treated Teeth more Brittle? Journal of Endodontics 18(7),1992
- Sjbgren et al. Factors Affecting the Long-term Results of Endodontic Treatment. Journal Of Endodontics. 16 (10) 1990
- Tang et al. Identifying and Reducing Risks for Potential Fractures in Endodontically Treated Teeth. JOE — Volume 36, Number 4, April 2010
- Torabinejab and Walton. Endodontic Principles and Practice 4th ed.
The lecture references key papers and textbook chapters discussing:
- Ferrule effect
- Failure patterns
- Biomechanics of endodontically treated teeth
Recommended focus when reviewing:
- Preserving tooth structure as priority
- Ferrule importance
- Designing restorations to manage occlusal risk
Footnotes
-
Original PDF page 1: L1 RETT Introduction, p.1 ↩
-
Original PDF page 2: L1 RETT Introduction, p.2 ↩
-
Original PDF page 3: L1 RETT Introduction, p.3 ↩
-
Original PDF page 4: L1 RETT Introduction, p.4 ↩
-
Original PDF page 5: L1 RETT Introduction, p.5 ↩
-
Original PDF page 6: L1 RETT Introduction, p.6 ↩
-
Original PDF page 7: L1 RETT Introduction, p.7 ↩
-
Original PDF page 8: L1 RETT Introduction, p.8 ↩
-
Original PDF page 9: L1 RETT Introduction, p.9 ↩
-
Original PDF page 10: L1 RETT Introduction, p.10 ↩
-
Original PDF page 11: L1 RETT Introduction, p.11 ↩
-
Original PDF page 12: L1 RETT Introduction, p.12 ↩
-
Original PDF page 13: L1 RETT Introduction, p.13 ↩
-
Original PDF page 14: L1 RETT Introduction, p.14 ↩
-
Original PDF page 15: L1 RETT Introduction, p.15 ↩
-
Original PDF page 16: L1 RETT Introduction, p.16 ↩
-
Original PDF page 17: L1 RETT Introduction, p.17 ↩
-
Original PDF page 18: L1 RETT Introduction, p.18 ↩
-
Original PDF page 19: L1 RETT Introduction, p.19 ↩
-
Original PDF page 20: L1 RETT Introduction, p.20 ↩
-
Original PDF page 21: L1 RETT Introduction, p.21 ↩
-
Original PDF page 22: L1 RETT Introduction, p.22 ↩
-
Original PDF page 23: L1 RETT Introduction, p.23 ↩
-
Original PDF page 24: L1 RETT Introduction, p.24 ↩
-
Original PDF page 25: L1 RETT Introduction, p.25 ↩
-
Original PDF page 26: L1 RETT Introduction, p.26 ↩
-
Original PDF page 27: L1 RETT Introduction, p.27 ↩
-
Original PDF page 28: L1 RETT Introduction, p.28 ↩
-
Original PDF page 29: L1 RETT Introduction, p.29 ↩
-
Original PDF page 30: L1 RETT Introduction, p.30 ↩
-
Original PDF page 31: L1 RETT Introduction, p.31 ↩
-
Original PDF page 32: L1 RETT Introduction, p.32 ↩