Restoration of Endodontically Treated Teeth1
Lecture 2: Post and Core Classification2
The University of Western Australia
Learning Outcomes3
By the end of this lecture, you should be able to:
- Discuss the evaluation of endodontically treated teeth before being restored
- Discuss the clinical indication of posts
- Understand the classification of post and cores
- Discuss different types of posts
Role of the Post – Updated View4
Evidence-Based Conclusions
- Posts do not reinforce endodontically treated teeth (ETT).
- Posts redistribute stress; depending on design, they may increase stress in some regions.
- With adequate tooth structure and ferrule, survival differences with and without posts are small.
Indications and Contraindications for Post Placement5
Indications for a Post
- Inadequate coronal tooth structure to retain a core or crown by adhesion and macro-retention alone.
- Need for a core that will support a full coverage restoration or FPD retainer.
Contraindications
- Sufficient tooth structure for bonded/core retention.
- Short or curved roots where a post would jeopardize integrity.
Assessment Factors for Intermediate Situations
Many cases fall between these clear categories. In these situations, clinicians must assess:
- Occlusal load
- Tooth position
- Type of opposing tooth
- Function: abutment of FPD or RPD
The guiding principle remains: preserve dentine and prioritize the ferrule.
Comparison Criteria
When evaluating options, consider modulus of elasticity (stiffness), stress behavior, bonding predictability, aesthetics, corrosion risk, and retrievability for potential endodontic retreatment.
Contemporary Protocol
Passive posts are more commonly used in modern restorative dentistry due to their favorable stress profiles.
Anatomic Posts
- Posts designed to match the specific cross-sectional anatomy of the root canal
Selection Principle
- Choose a design that fits the canal conservatively, provides adequate retention, and minimizes stress while avoiding unnecessary dentine removal
- Evidence suggests less root fracture when dentin is preserved
- Require more dentine removal apically compared to tapered designs
Modern Practice
Cast post and cores are reserved for selected cases where predictable adaptation and core form cannot be achieved with prefabricated posts and bonded cores.
- ==Limitations:== Poor adaptation in wide or irregular canals may require excessive cement thickness or additional dentine removal, reducing predictability and weakening the root
Clinical Applications of Posts6
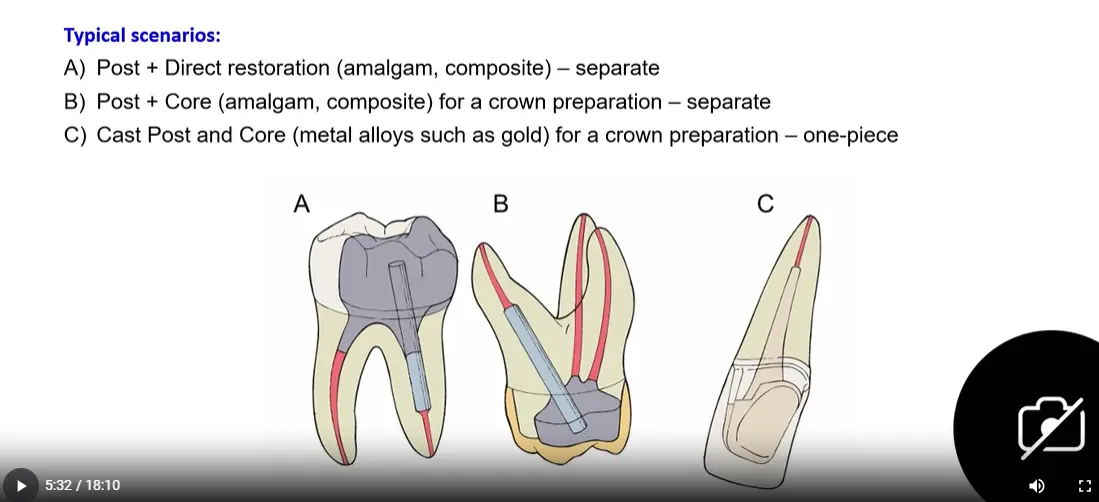
Typical Scenarios
- Post + Direct Restoration: Separate components using amalgam or composite.
- Post + Core: Separate components (amalgam or composite) prepared for a crown.
- Cast Post and Core: One-piece unit made from metal alloys (such as gold) for a crown preparation.
 Selection Considerations
Selection Considerations
- Canal anatomy and morphology
- Remaining dentinal walls
- Amount of remaining tooth structure
- Ferrule options available
- Ability to achieve predictable isolation and bonding for adhesive techniques
Post Classification78
Posts are classified based on the following criteria:
- Fabrication method: Prefabricated vs. custom cast
- Material: Metal, fiber-reinforced composite, ceramic
- Shape: Parallel, tapered, anatomic
- Surface: Smooth, serrated, threaded
Fabrication Method910
Prefabricated Posts
- Off-the-shelf, standardized dimensions.
- Best suited to relatively circular canals.
- Cemented in the root canal; the core is directly produced in composite or amalgam.
Custom Cast Posts and Cores
- Indicated in flared or irregular canals.
- Allow ideal fit and core shape but require more appointments.
- The post and the core are cast as a single unit.
Shape11
Parallel Posts
- Increased retention due to parallel walls.
- Produce uniform stress distribution along the post length.
- Lower incidence of root fracture.
- Stress concentration occurs at the apical portion.
Tapered Posts
- Follow natural canal form and configuration.
- Preservation of tooth structure at the post apex.
- Wedging effect leads to more stress.
- Stress concentration occurs at the coronal portion of the root.
- Lower retentive strength.
Surface Features12
Active Posts
- Engage the walls of the canal (threaded).
- More retentive.
- Introduce more stress into the root.
- Require a substantial amount of root dentin.
- Indication: Short roots in which maximum retention is needed (limited use).
Passive Posts
- Smooth or serrated surface.
- Retained strictly by the luting agent.
- Require close adaptation to the canal wall.
- Less stress introduced into the root.
- Fewer catastrophic failures.
- More commonly used.
Material13
Ideal Physical Properties
- Dentin-like stiffness: Modulus of elasticity close to dentin to promote favorable stress distribution.
- Reliable bondability: Strong adhesion to tooth structure (dentin) and core materials.
- Biocompatible: Corrosion-resistant in the oral environment.
- Energy-dissipating behavior: Helps absorb or attenuate functional forces rather than concentrate stress.
Clinical Reality
No single material satisfies all requirements perfectly. Selection requires balancing material properties against the major determinants of success: remaining tooth structure, ferrule, and durable coronal seal.
Pre-fabricated Posts
- Metal: Stainless steel, titanium, or titanium alloys.
- Fibre-reinforced composite (FRC): Glass fibre, quartz fibre, carbon fibre.
- Ceramic: Zirconia.
Custom / Cast Posts (Post–Core)
- Cast metal alloys:
- Noble / high-noble (e.g., gold-based).
- Base-metal (non-precious) alloys.
- Custom ceramic: Zirconia (CAD/CAM or laboratory-fabricated).
Metal Posts – Advantages and Risks14
Advantages
- Long clinical track record with predictable performance.
- High strength and stiffness resulting in low risk of post fracture.
- Good retention when properly designed and fitted.
- Higher retention reported for stainless-steel posts compared with certain fibre posts (e.g., carbon fibre).
Risks and Limitations
- High modulus of elasticity may concentrate stress in root dentin, increasing risk of root fracture.
- This biomechanical mismatch is particularly problematic when the ferrule is limited or dentinal walls are thin, resulting in potentially catastrophic root fracture.
- Corrosion possible with some alloys (rarely clinically significant, but may contribute to degradation).
- Aesthetic limitations under translucent ceramic crowns.
- Cast post–core requires increased chairside/lab time and cost, with more complex retreatment or removal.
- Retreatability challenges: While removable, metal posts can be challenging to extract without damaging the root.
Fiber Posts – Evidence and Limitations15
Advantages
- Modulus closer to dentin, leading to more favorable and repairable failure patterns.
- Repairable failure patterns: When failure occurs, it typically involves post debonding or core fracture rather than catastrophic root fracture, often allowing for repair.
- Esthetically compatible under all-ceramic crowns.
- Corrosion resistance.
- Biocompatible.
Limitations
- Technique-sensitive bonding to radicular dentin.
- Failure of cementation (adhesion to dentin is not always reliable).
Critical Consideration
Fiber posts do not replace the need for remaining tooth structure and ferrule; they merely complement these features when a post is needed for core retention.
- Debonding failures: Many clinical failures relate to loss of retention rather than post fracture.
- Strict protocol requirements: Success depends on:
- Excellent isolation (rubber dam)
- Proper canal cleaning and surface preparation
- Appropriate adhesive/cement selection
- Correct handling and placement technique
Ceramic and Zirconia Posts16
- Excellent aesthetics: Ideal for use under translucent all-ceramic crowns.
- High stiffness and brittleness: May concentrate stress and increase the risk of root fracture.
- Challenging retreatment: Difficult to remove if endodontic re-intervention is required.
- Clinical Evidence: Less robust clinical evidence compared with fibre and metal posts.
Footnotes
-
Original PDF page 1: L2 RETT 2026 Post and core classification, p.1 ↩
-
Original PDF page 2: L2 RETT 2026 Post and core classification, p.2 ↩
-
Original PDF page 3: L2 RETT 2026 Post and core classification, p.3 ↩
-
Original PDF page 4: L2 RETT 2026 Post and core classification, p.4 ↩
-
Original PDF page 5: L2 RETT 2026 Post and core classification, p.5 ↩
-
Original PDF page 6: L2 RETT 2026 Post and core classification, p.6 ↩
-
Original PDF page 7: L2 RETT 2026 Post and core classification, p.7 ↩
-
Original PDF page 13: L2 RETT 2026 Post and core classification, p.13 ↩
-
Original PDF page 8: L2 RETT 2026 Post and core classification, p.8 ↩
-
Original PDF page 9: L2 RETT 2026 Post and core classification, p.9 ↩
-
Original PDF page 10: L2 RETT 2026 Post and core classification, p.10 ↩
-
Original PDF page 11: L2 RETT 2026 Post and core classification, p.11 ↩
-
Original PDF page 12: L2 RETT 2026 Post and core classification, p.12 ↩
-
Original PDF page 14: L2 RETT 2026 Post and core classification, p.14 ↩
-
Original PDF page 15: L2 RETT 2026 Post and core classification, p.15 ↩
-
Original PDF page 16: L2 RETT 2026 Post and core classification, p.16 ↩