Classification and Prognosis Evaluation of Individual Teeth1
Classification and prognosis evaluation of individual teeth—A comprehensive approach
Nachum Samet, DMD¹ / Anna Jotkowitz, BDS²
Abstract2
Following a complete evaluation of the patient, treatment planning requires the analysis of individual teeth, accurate diagnosis, and prognosis evaluation. Currently, there is no accepted comprehensive, standardized, and meaningful classification system for the evaluation of individual teeth that offers a common language for dental professionals. A search was conducted reviewing existing literature relating to classification and prognostication of individual teeth. The dimensions determined to be of importance to gain an overall perspective of the individual relative tooth prognosis were the periodontal, restorative, endodontic, and occlusal plane perspectives. The authors present a comprehensive classification system by conjugating the literature and currently accepted concepts in dentistry. This easy-to-use system assesses the condition of individual teeth and enables a relative prognostic value to be attached to those teeth based on tooth condition and patient-level factors. (Quintessence Int 2009;40:377–387)
Key words: classification, dental assessment, endodontic, diagnosis, occlusal plane, periodontic, prognosis, restorability, tooth, treatment planning

Introduction
Currently there is no accepted standardized tool for assessing the overall status of teeth. Predicting whether a tooth is likely to be longstanding in the patient’s mouth, making it appropriate to be part of the overall rehabilitation of a patient, is one of the most challenging tasks in dentistry. An accurate diagnosis and prognosis evaluation are the basis of solid treatment planning and are essential when treatment options are considered. The aim of this article is to propose a comprehensive, standardized, and meaningful classification system for the evaluation of individual teeth. The classification system enables a relative prognostic value to be attached to each evaluated tooth for treatment planning purposes.
The proposed classification aims to become a systematic tool that would enhance communication among dental professionals, be used for evaluation of cases from a medicolegal perspective, generate a baseline for outcome assessment of treatment modalities, and enable young and experienced clinicians alike to evaluate dental conditions in a uniform way. It could also facilitate patient understanding of the condition of their teeth, enabling them to make informed decisions before they consent to various treatment options.
Prognosis Definition
Prognosis is defined as “a prediction of the probable course and outcome of a disease, and the likelihood of recovery from a disease.”¹ However, evidence-based published data aimed at evaluating the relevance of clinical and radiographic findings as predictors for long-term prognosis are lacking in the dental literature.²,³
Author Affiliations
¹Assistant Professor of Restorative Dentistry; Director, Predoctoral Prosthodontics, Department of Restorative Dentistry and Biomaterials Science, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
²Instructor in Restorative Dentistry, Department of Restorative Dentistry and Biomaterials Science, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
Correspondence: Dr Nachum Samet, Department of Restorative Dentistry and Biomaterials Science, Harvard School of Dental Medicine, 188 Longwood Avenue, Boston, MA 02115. Fax: (617) 432-0901. Email: nachum_samet@hsdm.harvard.edu
Literature Review of Prognostic Factors
disease process was controlled, whereas in the nonmaintained group, the above-mentioned factors were not all indicators of disease activity. Hence, these factors may not have been accurate at predicting disease progression. The study illustrates how periodontal maintenance and patient compliance influence long-term prognosis.
In the 1990s, McGuire and Nunn documented a series of papers based on a longitudinal investigation that followed 100 patients at 5, 8, and 15 years. The system categorized teeth as “good,” “fair,” “poor,” “questionable,” and “hopeless.” Their first 2 studies, similar to previously published articles, based the assessment of prognosis on commonly accepted clinical findings such as probing depth, bone loss, furcation involvement, mobility, crown-root ratio, and root form, and concluded that these clinical parameters were ineffective at predicting any outcome other than “good.” The third article evaluated the relationship of the above clinical parameters to tooth loss. They concluded that although there is a relationship between prognosis and tooth loss, initial prognosis did not adequately predict tooth survival. This led them to their fourth and final article, in which they began looking at host susceptibility as a further influencing factor. From this study, it seems that host factors such as the presence of interleukin-1 genotype improved the accuracy of predicting tooth loss, as did smoking.
In 2006, Muzzi et al directed a 10-year retrospective study to evaluate the ability of clinical, radiographic, and genetic variables to accurately predict tooth loss in a population undergoing a strict maintenance regimen. They concluded that the infrabony component of the defect and the amount of residual bone may be good prognostic factors for predicting tooth loss; however, more traditional methods were proven to be of little value.
More recently, an attempt to classify prognosis by the ability, or inability, to achieve periodontal stability was made. Periodontal stability can be monitored by routine clinical examinations and radiographs, and this system aims to help clinicians make decisions for treatment planning and patient management rather than just looking at the relationship of initial prognosis to tooth mortality as is done in previous systems. Furthermore, the need to differentiate between individual tooth prognosis and overall prognosis for the patient is recognized. Kwok and Caton’s system focuses on only periodontal factors, although it gives consideration to both local and systemic risk factors, which need to be reassessed over time.
Periodontal Maintenance and Compliance
Restorative Literature3
The restorative literature includes effective classification systems, but lacks a classification system that gives clinicians a tool to assess the condition and the prognostic value of individual teeth. It has been widely documented that the key to long-term success in the restoration of endodontically treated teeth is directly related to the amount of remaining sound coronal tooth structure. A recent systematic review concluded that the most critical aspect when dealing with a nonvital tooth is “tissue preservation.” Similarly, the importance of providing an adequate ferrule is generally accepted. Thus, the amount of remaining sound tooth structure should be considered key in assessing restorability.
Few attempts have been made to create an index that measures actual remaining coronal dentin or grades tooth restorability. The main problem with the development of such an index lies in the need to assess actual remaining sound tooth structure before actual caries removal. Bandlish et al took 20 teeth, produced casts, and derived a technique to assess the amount of remaining dentin present after crown preparation. A tooth restorability index was developed to assess the strategic value of the remaining dentin. This divided the teeth into sextants, and a score of 0 to 3 was attributed whether the amount of remaining dentin was “none,” “inadequate,” “questionable,” or “adequate,” such that a maximum of 18 could be scored for each tooth. The 20 teeth were analyzed by 3 experienced dentists, who used the combined cast of remaining coronal dentin to score the tooth restorability index for each tooth. This study concluded that the suggested system provided “moderate to good” agreement among the examiners and suggested that it was a good way of assessing restorability of a tooth.

Restorability and Structural Integrity
agreement among the examiners and suggested that it was a good way of assessing restorability of a tooth.
No other articles included for review attempted to produce a quantitative system to assess how much tooth structure remains. Other attempts at assessing restorability are less didactic and avoid quantification, leaving a nonprecise, subjective assessment as to how much remaining tooth structure is enough to make a tooth restorable.
Endodontic Literature4
The endodontic prognosis of a tooth in isolation of the other categories is largely linked to the difficulty of the case at hand. Potential problems include calcifications, inability to isolate the tooth, resorptive defects, extra roots and/or canals, retreatment cases, existing posts, ledges, and perforations. Many different guides have been compiled to help clinicians determine the degree of treatment difficulty for a given case. These include the UCSF (University of California, San Francisco) Endodontic Case Selection System, guidelines put out by the American Association of Endodontics, the Canadian Academy of Endodontics, and the Dutch Endodontic Treatment Index. The other factor influencing the endodontic prognosis is the presence of a periapical radiolucency. Clinical trials have shown a lower success rate in endodontic cases with periapical radiolucencies because the causative pathology has been present for a longer period. The ability to determine the cause of a radiolucency is key to understanding if a root canal can be predictably treated.
A strong association has been noted between the crowning of endodontically treated teeth and their long-term survival. This emphasizes the closely intertwined relationship between endodontic and restorative prognosis. It is commonly stated that endodontic therapy is not complete until a coronal restoration has been placed, and that the coronal seal is at least as important, if not more important, than the apical seal when looking at the long-term success of endodontically treated teeth.
Literature Related to the Occlusal Plane
No literature was found to measure the degree of super-eruption or amount of tooth tipping within an arch that determines at what point a tooth becomes nonsalvageable or inappropriate for inclusion in a restorative treatment plan. However, current accepted concepts suggest that it is beneficial to restore teeth to the correct occlusal plane and that over-erupted and tilted teeth can potentially prevent normal tooth contact during function and therefore require treatment. In partly edentulous patients, such teeth may create a problem when restoring the opposing arch. The scope of potential treatment ranges from enameloplasty or orthodontic treatment to extraction of severely tilted or over-erupted teeth. Moderate cases may require a partial or a full-coverage restoration. However, some cases may require a combination of endodontic treatment, crown-lengthening surgery, and a restoration to achieve a functional tooth that lies correctly within the occlusal plane. Special attention is required when analyzing these cases, since such procedures may result in a tooth that has an unfavorable crown-root ratio, and in certain cases may cause periodontal damage to itself and/or to neighboring teeth. Aggressive surgical procedures in which segments of the maxilla or the mandible are shifted from their original position have also been published; however, since these treatment modalities are not readily available, they are excluded from this classification.
Rationale of the Proposed Classification System
There are many types of classification systems. Simple but powerful classifications like Angle’s classification and the Kennedy classification have been used in dentistry for decades. This proposed classification system similarly aims to be simple while being comprehensive, standardized, and meaningful.
Endodontic Prognosis
Proposed Comprehensive Classification System
It does not aim to allow for perfect differentiation among all potential situations. Rather, it includes those criteria that generally make a significant impact on the condition of a specific tooth and therefore on its relative prognostic value.
An assumption is made that current accepted dental standards and best practices will be employed to treat the diagnoses.
Dental patient evaluation involves 2 sequential phases. The first phase takes patient-level considerations into account, and a second phase aims to classify individual teeth.
Patient-Level Considerations5
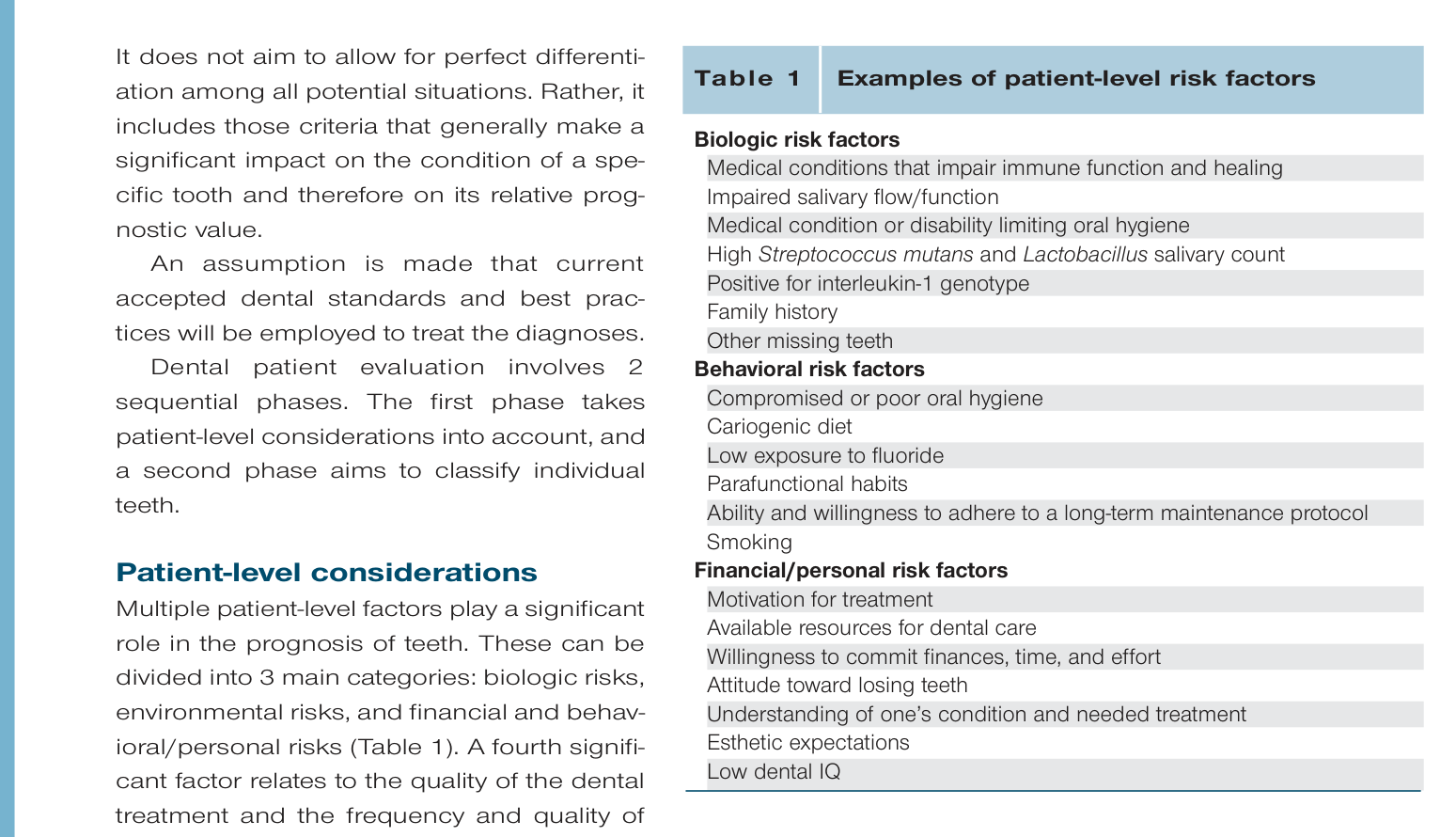
Multiple patient-level factors play a significant role in the prognosis of teeth. These can be divided into 3 main categories: biologic risks, environmental risks, and financial and behavioral/personal risks (Table 1). A fourth significant factor relates to the quality of the dental treatment and the frequency and quality of oral health maintenance. Each of these categories affects the progression of the disease, be it periodontal disease, caries, malocclusion, etc, and will influence the likelihood of recovery.
The number of risk factors present and their severity will determine the extent of their impact, as will the ability to modify and/or eliminate the risk factors. In general, risk factors that are associated with high caries rate and periodontal disease are those that will challenge prognosis evaluation. These can be best assessed by the various caries risk assessment (CAMBRA [caries management by risk assessment]) and periodontal risk assessment tools available. Such tools categorize patients into high, medium, or low risk groups, and management can be customized to control disease progression. Conditions that increase patient risk for caries—dry mouth, diet, habits, hygiene, unfavorable microflora, root exposure, and limited fluoride exposure—and factors that may result in future deterioration of the periodontal apparatus—oral hygiene, metabolic/systemic disease, unfavorable microflora, family history, smoking, age, and existing periodontal disease—potentially increase the patient’s likelihood of further disease progression.
Criteria and Assumptions
Parafunction may also increase the risk to individual teeth or to the entire dentition.
Because only some risk factors can be diminished or even eliminated, these should be divided into modifiable and nonmodifiable risk factors. If modifiable risk factors are managed during and following treatment, overall tooth prognosis should be reassessed. An alert can be captured in the patient chart to emphasize the need for appropriate management. Such treatments aim to diminish patient likelihood of further disease progression often through lifestyle changes. However, those patients who have multiple nonmodifiable or unsuccessfully controlled risk factors display an overall inferior case prognosis. There are publications presenting long-term success of oral rehabilitation of compromised dentitions. These are examples of how the prognosis evaluation of a tooth may be improved based on positive alterations of modifiable risk factors.
Financial constraints, as well as a patient’s behavior and personal factors (level of motivation for treatment, adherence to maintenance care protocols, phobia, unwillingness or inability to endure lengthy and involved procedures, refusing treatment, etc), may result in further deterioration. Therefore, they should also be factored into the overall relative prognosis of all teeth and will influence treatment decisions. Esthetic considerations play a significant role in a patient’s treatment choice, although they do not alter tooth prognosis per se. In certain cases, these factors may bring about a decision to extract a tooth that otherwise could be saved.
Table 1: Examples of patient-level risk factors
- Biologic risk factors
- Medical conditions that impair immune function and healing
- Impaired salivary flow/function
- Medical condition or disability limiting oral hygiene
- High Streptococcus mutans and Lactobacillus salivary count
- Positive for interleukin-1 genotype
- Family history
- Other missing teeth
- Behavioral risk factors
- Compromised or poor oral hygiene
- Cariogenic diet
- Low exposure to fluoride
- Parafunctional habits
- Ability and willingness to adhere to a long-term maintenance protocol
- Smoking
- Financial/personal risk factors
- Motivation for treatment
- Available resources for dental care
- Willingness to commit finances, time, and effort
- Attitude toward losing teeth
- Understanding of one’s condition and needed treatment
- Esthetic expectations
- Low dental IQ
Patient Factors and Esthetic Considerations
or inability to endure lengthy and involved procedures, refusing treatment, etc), may result in further deterioration. Therefore, they should also be factored into the overall relative prognosis of all teeth and will influence treatment decisions. Esthetic considerations play a significant role in a patient’s treatment choice, although they do not alter tooth prognosis per se. In certain cases, these factors may bring about a decision to extract a tooth that otherwise could be saved.
Evaluation of Individual Teeth6
Criteria for analysis. Four main criteria and 2 additional factors that may compromise these criteria are evaluated:
- Periodontal condition and alveolar bone support
- Restorability, ie, remaining sound tooth structure
- Endodontic condition
- Occlusal plane and tooth position
The 2 additional factors, which may compromise the above, are evaluated when applicable. These include:
- Anatomic irregularities
- Iatrogenic compromising factors
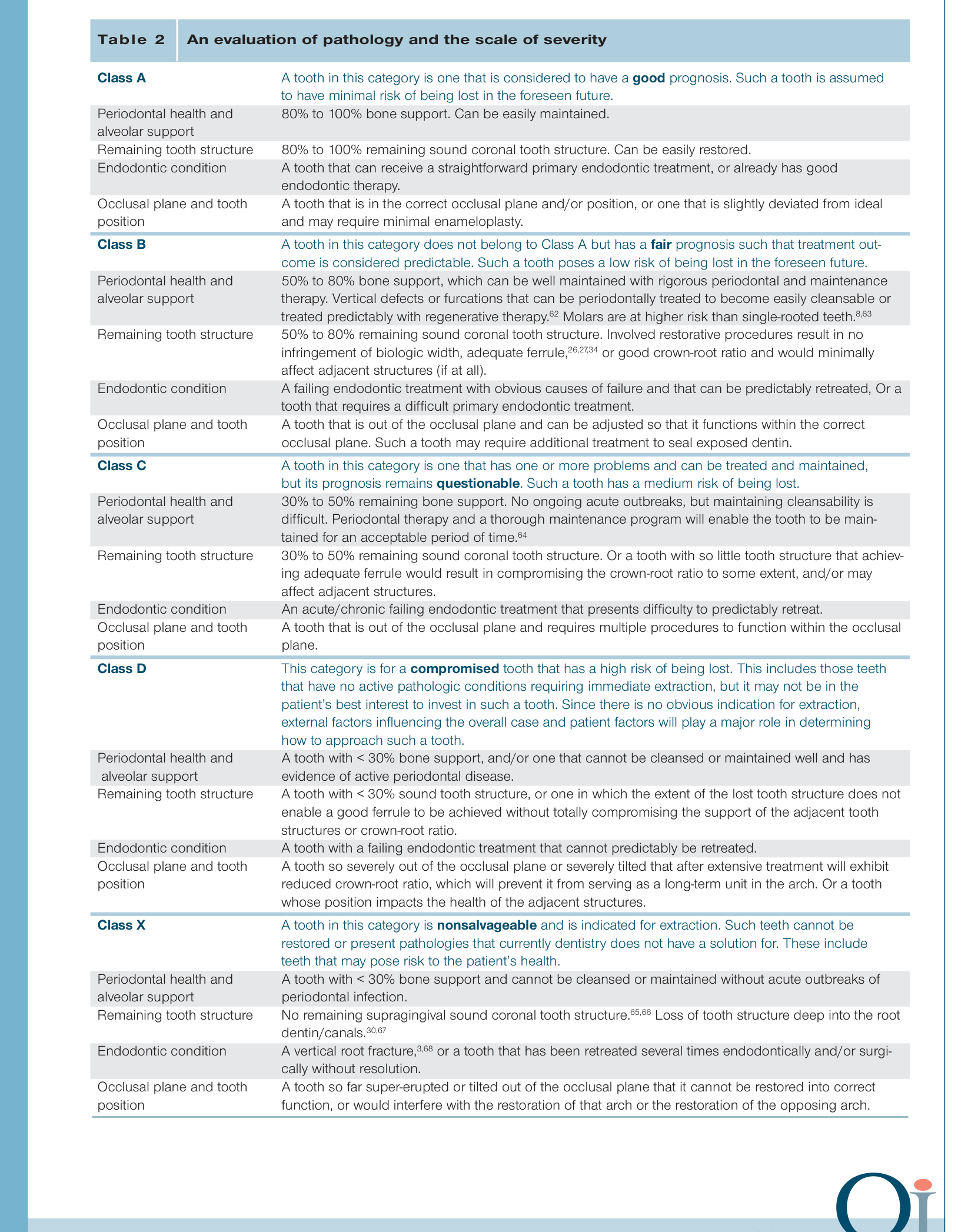
The classification rules. The proposed classification comprises 5 classes—A, B, C, D, and X—and requires 2 steps of analysis. An assumption is made that current accepted dental standards and best practices will be employed to treat the diagnoses.
Step 1. Each tooth is evaluated for each of the 4 criteria independently. The level of severity is evaluated both based on the presented condition and with consideration to the foreseen tooth status after caries removal. The single most severe of these criteria determines the tooth’s class (Table 2).
Step 2. Anatomic risk factors and/or iatrogenic compromising factors may result in a drop of a class for an individual tooth. More than 2 such findings in a tooth may require a further drop in class (Table 3).
Step 3. Patient-level risk factors may result in a decreased prognosis for the dentition. Therefore, a drop of 1 class for all teeth is suggested when considerable patient-level risk factors are diagnosed. Patient-level risk factors are reassessed over time. A decrease in class should be considered when no change in modifiable risk factors is observed, or when significant nonmodifiable factors are present. An increase in class should be considered when an obvious change in modifiable risk factors is observed.
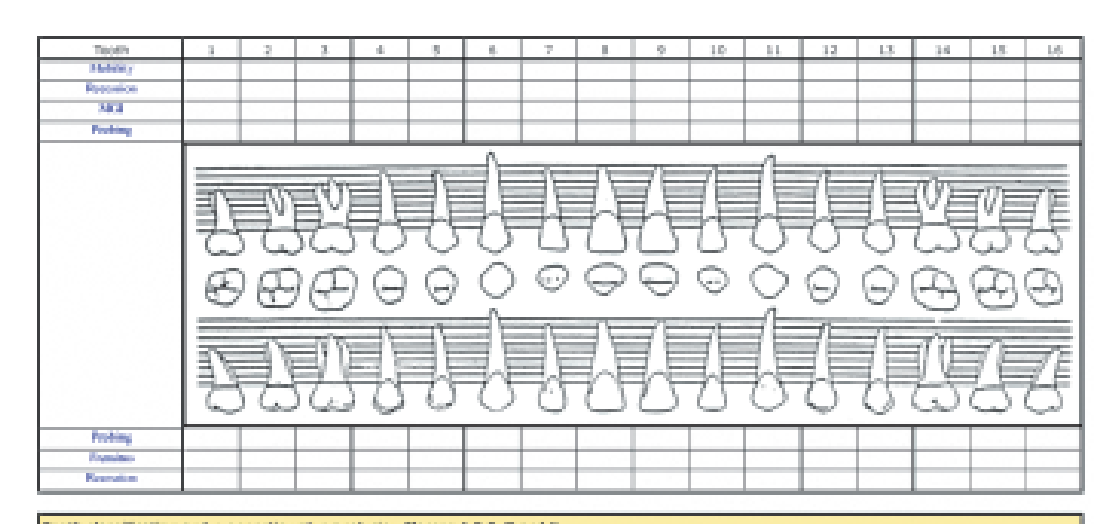
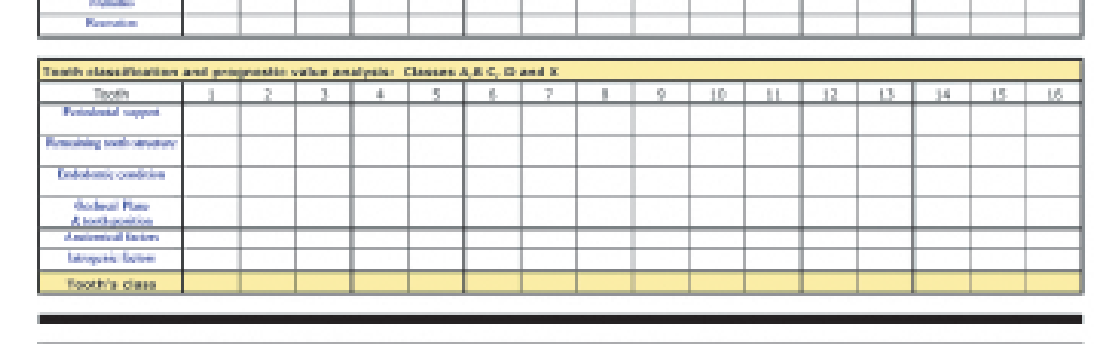
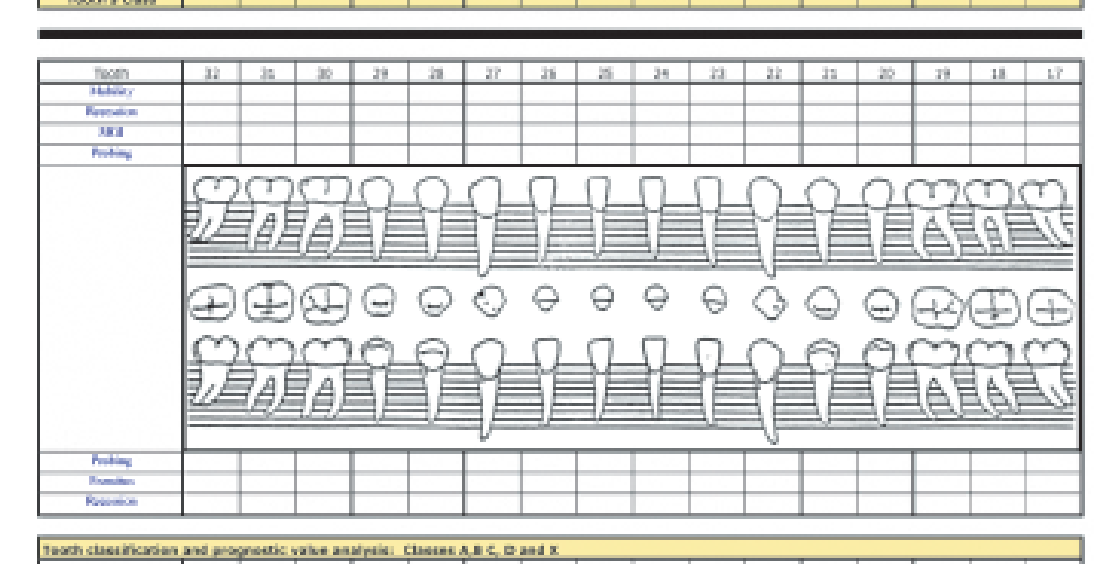
The system may be included into routine clinical examination and recorded on a periodontal and hard tissue chart. A suggestion is demonstrated based on the chart used at Harvard School of Dental Medicine (Fig 1).
Discussion
Treatment planning is a multistage process that involves the analysis of each tooth from various aspects. Many of the diseases affecting the dental structures are bacterial or infectious in nature. Other etiologies may also cause the destruction of tooth and supporting structures. Any chosen treatment modality requires management and monitoring of the cause and of the disease process in addition to mechanical/surgical treatment, as well as the adherence to a long-term maintenance protocol.
Based on the reviewed literature and accepted best practices, this proposal bases the classification of the condition of teeth and their relative prognosis on 4 main criteria and 2 additional factors. Patient-level factors may alter the overall prognosis of a case, especially when these factors cannot be modified by the patient or by treatment.
Periodontal status, endodontic status, tooth position, and iatrogenic and anatomic factors can be assessed based on clinical and radiographic indicators. Understanding of caries progression by using the CAMBRA protocol should help clinicians assess caries progression so a class can be determined. However, there may be cases in which the extent of tooth destruction by caries can only be accurately determined after mechanical removal.
Clinical Evaluation and Severity Scales
Table 2: An evaluation of pathology and the scale of severity
Class A — A tooth in this category is one that is considered to have a good prognosis. Such a tooth is assumed to have minimal risk of being lost in the foreseen future.
- Periodontal health and alveolar support: 80% to 100% bone support. Can be easily maintained.
- Remaining tooth structure: 80% to 100% remaining sound coronal tooth structure. Can be easily restored.
- Endodontic condition: A tooth that can receive a straightforward primary endodontic treatment, or already has good endodontic therapy.
- Occlusal plane and tooth position: A tooth that is in the correct occlusal plane and/or position, or one that is slightly deviated from ideal and may require minimal enameloplasty.
Class B — A tooth in this category does not belong to Class A but has a fair prognosis such that treatment outcome is considered predictable. Such a tooth poses a low risk of being lost in the foreseen future.
- Periodontal health and alveolar support: 50% to 80% bone support, which can be well maintained with rigorous periodontal and maintenance therapy. Vertical defects or furcations that can be periodontally treated to become easily cleansable or treated predictably with regenerative therapy. Molars are at higher risk than single-rooted teeth.
- Remaining tooth structure: 50% to 80% remaining sound coronal tooth structure. Involved restorative procedures result in no infringement of biologic width, adequate ferrule, or good crown-root ratio and would minimally affect adjacent structures (if at all).
- Endodontic condition: A failing endodontic treatment with obvious causes of failure and that can be predictably retreated, or a tooth that requires a difficult primary endodontic treatment.
- Occlusal plane and tooth position: A tooth that is out of the occlusal plane and can be adjusted so that it functions within the correct occlusal plane. Such a tooth may require additional treatment to seal exposed dentin.
Classification of Pathology and Prognosis7
Class C — A tooth in this category is one that has one or more problems and can be treated and maintained, but its prognosis remains questionable. Such a tooth has a medium risk of being lost.
- Periodontal health and alveolar support: 30% to 50% remaining bone support. No ongoing acute outbreaks, but maintaining cleansability is difficult. Periodontal therapy and a thorough maintenance program will enable the tooth to be maintained for an acceptable period of time.
- Remaining tooth structure: 30% to 50% remaining sound coronal tooth structure. Or a tooth with so little tooth structure that achieving adequate ferrule would result in compromising the crown-root ratio to some extent, and/or may affect adjacent structures.
- Endodontic condition: An acute/chronic failing endodontic treatment that presents difficulty to predictably retreat.
- Occlusal plane and tooth position: A tooth that is out of the occlusal plane and requires multiple procedures to function within the occlusal plane.
Class D — This category is for a compromised tooth that has a high risk of being lost. This includes those teeth that have no active pathologic conditions requiring immediate extraction, but it may not be in the patient’s best interest to invest in such a tooth. Since there is no obvious indication for extraction, external factors influencing the overall case and patient factors will play a major role in determining how to approach such a tooth.
- Periodontal health and alveolar support: A tooth with < 30% bone support, and/or one that cannot be cleansed or maintained well and has evidence of active periodontal disease.
- Remaining tooth structure: A tooth with < 30% sound tooth structure, or one in which the extent of the lost tooth structure does not enable a good ferrule to be achieved without totally compromising the support of the adjacent tooth structures or crown-root ratio.
- Endodontic condition: A tooth with a failing endodontic treatment that cannot predictably be retreated.
- Occlusal plane and tooth position: A tooth so severely out of the occlusal plane or severely tilted that after extensive treatment will exhibit reduced crown-root ratio, which will prevent it from serving as a long-term unit in the arch. Or a tooth whose position impacts the health of the adjacent structures.
Class X — A tooth in this category is nonsalvageable and is indicated for extraction. Such teeth cannot be restored or present pathologies that currently dentistry does not have a solution for. These include teeth that may pose risk to the patient’s health.
- Periodontal health and alveolar support: A tooth with < 30% bone support and cannot be cleansed or maintained without acute outbreaks of periodontal infection.
- Remaining tooth structure: No remaining supragingival sound coronal tooth structure. Loss of tooth structure deep into the root dentin/canals.
- Endodontic condition: A vertical root fracture, or a tooth that has been retreated several times endodontically and/or surgically without resolution.
- Occlusal plane and tooth position: A tooth so far super-erupted or tilted out of the occlusal plane that it cannot be restored into correct function, or would interfere with the restoration of that arch or the restoration of the opposing arch.
Anatomic and Iatrogenic Compromising Factors8
Table 3: Factors that result in a drop of the determined class
- Anatomic irregularities: Irregularly shaped roots, multiple canals and/or roots, thin and/or short roots, and excessively conical roots cause a drop in the prognosis and increase the risk to that tooth. This can often render a tooth with an otherwise fair or poor prognosis as critical or hopeless.
- Iatrogenic compromising factors: Perforations, extensive post preparations, minimal tooth structure thickness left after preparation, dental materials that cannot be removed, etc. Without evidence of active pathology, the prognosis of a tooth with iatrogenic dentistry may even be fair or good; however, if further treatment is planned or the tooth is found with other pathology or clinical or radiographic signs and symptoms, the prognosis level drops. In some cases, the tooth may even be indicated for extraction.
 |  |
 |  |
Clinical Application and Treatment Planning
The proposed classification system aims to help clinicians in the treatment planning process, by focusing on individual and overall prognostic value of teeth. Thus, if a tooth that was originally planned to serve as an abutment for a prosthetic unit is found to be a questionable tooth (Class C) or a compromised tooth (Class D), an alternative treatment plan should be considered. On the other hand, if these teeth were supposed to be restored as individual units, the patient goals, financial considerations, and plans may lead to preserving them as an interim solution. Patient-level factors influence the overall prognosis and the likelihood of recovery from the disease, be it periodontal disease, caries, trauma, malocclusion, etc, resulting in alternative clinical decisions being reached that are more appropriate for the overall rehabilitation on the patient. The success of a particular treatment modality may also affect long-term prognosis of individual teeth, but since this is determined by the knowledge, skills, and comfort zone of the treating clinician, incorporating it into the classification would impair its main purpose—which is to focus on the patient’s condition.
Summary9
Although the dental literature presents limited evidence-based data to support the use of specific criteria as prognostic tools, the profession has developed accepted guidelines for the evaluation of teeth. The authors developed the classification system, based on evidence-based data whenever available and on a Delphi method process so as to accumulate the profession’s accepted best practices. Preliminary evaluation of this classification system has been well received upon expert peer-review analysis. In the last few years, dental students at Harvard School of Dental Medicine have been using this classification system as an educational tool. Although they had no previous experience in evaluating teeth, they were able to attach realistic prognostic values to teeth more accurately and more promptly than their predecessors, who did not use this classification system. Furthermore, students were able to devise better and more appropriate treatment plan options for their patients. This article presents a classification system that aims to create a meaningful and standardized tool for use among dental professionals. The authors are aware of the complexities and the limitations of any tool that aims to attach prognostic values to teeth. However, modern dentistry would benefit from having a classification system that is comprehensive and standardized.
Acknowledgments
The authors wish to acknowledge the following specialists and faculty for their input (by alphabetic order): Dr John Da Silva, Harvard University; Dr Renee Duff, University of Michigan; Dr Jacqueline Duncan, University of Connecticut; Dr Bernard Friedland, Harvard University; Dr German Gallucci, Harvard University; Dr Hamasat Gedaf-Dam, Geneva, Switzerland; Dr Foroud Hakim, University of the Pacific; Dr Nadeem Karimbux, Harvard University; Dr David Kim, Harvard University; Dr Natalie Leow, Sydney, Australia; Dr Jarshen Lin, Harvard University; Dr Zeev Ormianer, Ramat Gan, Israel; Dr Sharon Siegel, Nova University; Dr Noah Stern, Hebrew University, Israel; Dr Hans-Peter Weber, Harvard University; Dr Robert White, Harvard University; and Dr Robert Wright, Harvard University.
References1011
- The American Heritage Medical Dictionary. Boston: Houghton Mifflin, 2007.
- Mordohai N, Reshad M, Jivraj S, Chee W. Factors that affect individual tooth prognosis and choices in contemporary treatment planning. Br Dent J 2007;202:63–72.
- Simon JF. Retain or extract: The decision process. Quintessence Int 1999;30:851–854.
- Dalkey N, Helmer O. An experimental application of the Delphi method to the use of experts. Management Science 1963;9:458–467.
- Scapolo F, Miles I. Eliciting experts’ knowledge: A comparison of two methods. Technological Forecasting Social Change 2006;73:679–704.
- McGuire MK. Prognosis vs outcome: Predicting tooth survival. Compend Contin Educ Dent 2000; 21:217–220, 222, 224 passim.
References
-
Mordohai N, Reshad M, Jivraj SA. To extract or not to extract? Factors that affect individual tooth prognosis. J Calif Dent Assoc 2005;33:319–328.
-
Muzzi L, Nieri M, Cattabriga M, Rotundo R, Cairo F, Pini Prato GP. The potential prognostic value of some periodontal factors for tooth loss: A retrospective multilevel analysis on periodontal patients treated and maintained over 10 years. J Periodontol 2006;77:2084–2089.
-
McGuire MK. Prognosis versus actual outcome: A long-term survey of 100 treated periodontal patients under maintenance care. J Periodontol 1991;62:51–58.
-
McGuire MK, Nunn ME. Prognosis versus actual outcome. II. The effectiveness of clinical parameters in developing an accurate prognosis. J Periodontol 1996;67:658–665.
-
McGuire MK, Nunn ME. Prognosis versus actual outcome. III. The effectiveness of clinical parameters in accurately predicting tooth survival. J Periodontol 1996;67:666–674.
-
Donovan TE. Longevity of the tooth/restoration complex: A review. J Calif Dent Assoc 2006;34:122–128.
-
Pjetursson BE, Sailer I, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part I: Single crowns. Clin Oral Implants Res 2007;18 (suppl 3):73–85.
-
Pjetursson BE, Bragger U, Lang NP, Zwahlen M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin Oral Implants Res 2007;18(suppl 3):97–113.
-
Sailer I, Pjetursson BE, Zwahlen M, Hammerle CH. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin Oral Implants Res 2007;18(suppl 3):86–96.
-
Davarpanah M, Martinez H, Tecucianu JF, Fromentin O, Celletti R. To conserve or implant: Which choice of therapy? Int J Periodontics Restorative Dent 2000; 20:412–422.
-
Iqbal MK, Kim S. A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with non-surgical endodontic therapy. J Endod 2008;34: 519–529.
-
Torabinejad M, Goodacre CJ. Endodontic or dental implant therapy: The factors affecting treatment planning. J Am Dent Assoc 2006;137:973–977.
-
Kwok V, Caton JG. Commentary: Prognosis revisited: A system for assigning periodontal prognosis. J Periodontol 2007;78:2063–2071.
-
Hirschfeld L, Wasserman B. A long-term survey of tooth loss in 600 treated periodontal patients. J Periodontol 1978;49:225–237.
-
Newman MG, Takei HH, Carranza FA. Carranza’s Clinical Periodontology, ed 10. St Louis: Saunders Elsevier, 2006.
-
Becker W, Berg L, Becker BE. The long-term evaluation of periodontal treatment and maintenance in 95 patients. Int J Periodontics Restorative Dent 1984;4:54–71.
-
Becker W, Becker BE, Berg LE. Periodontal treatment without maintenance. A retrospective study in 44 patients. J Periodontol 1984;55:505–509.
-
McGuire MK, Nunn ME. Prognosis versus actual outcome. IV. The effectiveness of clinical parameters and IL-1 genotype in accurately predicting prognoses and tooth survival. J Periodontol 1999;70:49–56.
-
Dietschi D, Duc O, Krejci I, Sadan A. Biomechanical considerations for the restoration of endodontically treated teeth: A systematic review of the literature—Part 1. Composition and micro- and macrostructure alterations. Quintessence Int 2007;38:733–743.
-
Pereira JR, de Ornelas F, Conti PC, do Valle AL. Effect of a crown ferrule on the fracture resistance of endodontically treated teeth restored with prefabricated posts. J Prosthet Dent 2006;95:50–54.
-
Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodontically treated teeth. J Prosthet Dent 1990;63:529–536.
-
Stankiewicz N, Wilson P. The ferrule effect. Dent Update 2008;35:222–224, 227–228.
-
Stankiewicz NR, Wilson PR. The ferrule effect: A literature review. Int Endod J 2002;35:575–581.
-
Rosenstiel SF, Land MF, Fujimoto J. Contemporary Fixed Prosthodontics, ed 4. St Louis: Mosby Elsevier, 2006.
-
Hobo S, Whitsett LD, Jacobi R, Brackett SE, Shillingburg HT. Fundamentals of Fixed Prosthodontics. Chicago: Quintessence, 1997.
-
Bandlish RB, McDonald AV, Setchell DJ. Assessment of the amount of remaining coronal dentine in root-treated teeth. J Dent 2006;34:699–708.
-
Smith CT, Schuman N. Restoration of endodontically treated teeth: A guide for the restorative dentist. Quintessence Int 1997;28:457–462.
-
Yeng T, Messer HH, Parashos P. Treatment planning the endodontic case. Aust Dent J 2007;52:S32–37.
-
Pothukuchi K. Case assessment and treatment planning: What governs your decision to treat, refer or replace a tooth that potentially requires endodontic treatment? Aust Endod J 2006;32:79–84.
-
Messer HH. Clinical judgement and decision making in endodontics. Aust Endod J 1999;25:124–132.
-
Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent 2002;87:256–263.
-
Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: An epidemiological study. J Endod 2004;30:846–850.
-
Tilashalski KR, Gilbert GH, Boykin MJ, Shelton BJ. Root canal treatment in a population-based adult sample: Status of teeth after endodontic treatment. J Endod 2004;30:577–581.
-
Nagasiri R, Chitmongkolsuk S. Long-term survival of endodontically treated molars without crown coverage: A retrospective cohort study. J Prosthet Dent 2005;93:164–170.
-
Stavropoulou AF, Koidis PT. A systematic review of single crowns on endodontically treated teeth. Dent 2007;35:761–767.
-
Begotka BA, Hartwell GR. The importance of the coronal seal following root canal treatment. Va Dent J 1996;73:8–10.
-
Chugal NM, Clive JM, Spangberg LS. Endodontic treatment outcome: Effect of the permanent restoration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:576–582.
-
Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: A review. Endod Dent Traumatol 1994;10:105–108.
-
Hommez GM, Verhelst R, Claeys G, Vaneechoutte M, De Moor RJ. Investigation of the effect of the coronal restoration quality on the composition of the root canal microflora in teeth with apical periodontitis by means of T-RFLP analysis. Int Endod J 2004;37:819–827.
-
Dawson PE. Functional occlusion: From TMJ to smile design. St Louis: Mosby, 2006.
-
Craddock HL, Youngson CC, Manogue M, Blance A. Occlusal changes following posterior tooth loss in adults. Part 2. Clinical parameters associated with movement of teeth adjacent to the site of posterior tooth loss. J Prosthodont 2007;16:495–501.
-
Craddock HL, Youngson CC, Manogue M, Blance A. Occlusal changes following posterior tooth loss in adults. Part 1: A study of clinical parameters associated with the extent and type of supraeruption in unopposed posterior teeth. J Prosthodont 2007;16:485–494.
-
Craddock HL, Youngson CC. Eruptive tooth movement—The current state of knowledge. Br Dent J 2004;197:385–391.
-
McGivney GP, Castleberry DJ, McCracken WL. McCracken’s Removable Partial Prosthodontics. St Louis: Mosby, 1994.
-
Graber TM, Vanarsdall RL, Vig KWL. Orthodontics: Current Principles and Techniques, ed 4. St Louis: Mosby, 2005.
-
Jenson L, Budenz AW, Featherstone JD, Ramos-Gomez FJ, Spolsky VW, Young DA. Clinical protocols for caries management by risk assessment. J Calif Dent Assoc 2007;35:714–723.
-
Featherstone JD. The caries balance: The basis for caries management by risk assessment. Oral Health Prev Dent 2004;2(suppl 1):259–264.
-
Featherstone JD, Adair SM, Anderson MH, et al. Caries management by risk assessment: Consensus statement, April 2002. J Calif Dent Assoc 2003;31:257–269.
-
Young DA, Buchanan PM, Lubman RG, Badway NN. New directions in interorganizational collaboration in dentistry: The CAMBRA Coalition model. J Dent Educ 2007;71:595–600.
-
Young DA, Featherstone JD, Roth JR, et al. Caries management by risk assessment: Implementation guidelines. J Calif Dent Assoc 2007;35:799–805.
-
Page RC, Krall EA, Martin J, Mancl L, Garcia RI. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc 2002;133:569–576.
-
Page RC, Martin J, Krall EA, Mancl L, Garcia R. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol 2003;30:819–827.
-
Amsterdam M, Weisgold AS. Periodontal prosthesis: A 50-year perspective. Alpha Omegan 2000;93:23–30.
-
Libby G, Arcuri MR, LaVelle WE, Hebl L. Longevity of fixed partial dentures. J Prosthet Dent 1997;78:127–131.
-
Lulic M, Bragger U, Lang NP, Zwahlen M, Salvi GE. Ante’s (1926) law revisited: A systematic review on survival rates and complications of fixed dental prostheses (FDPs) on severely reduced periodontal tissue support. Clin Oral Implants Res 2007;18(suppl 3):63–72.
-
Cortellini P, Stalpers G, Pini Prato G, Tonetti MS. Long-term clinical outcomes of abutments treated with guided tissue regeneration. J Prosthet Dent 1999;81:305–311.
-
Checchi L, Montevecchi M, Gatto MR, Trombelli L. Retrospective study of tooth loss in 92 treated periodontal patients. J Clin Periodontol 2002;29:651–656.
-
Fardal O, Johannessen AC, Linden GJ. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J Clin Periodontol 2004;31:550–555.
-
Sorensen JA. Preservation of tooth structure. J Calif Dent Assoc 1988;16:15–22.
-
Sorensen JA, Martinoff JT. Clinically significant factors in dowel design. J Prosthet Dent 1984;52:28–35.
-
Spear F. When to restore, when to remove: The single debilitated tooth. Compend Contin Educ Dent 1999;20:316–318, 322–323, 327–328.
-
Weine FS. Endodontic Therapy. St Louis: Mosby, 2004.
-
Holm-Pedersen P, Lang NP, Muller F. What are the longevities of teeth and oral implants? Clin Oral Implants Res 2007;18(suppl 3):15–19.
-
Tomasi C, Wennstrom JL, Berglundh T. Longevity of teeth and implants—A systematic review. J Oral Rehabil 2008;35(suppl 1):23–32.
Footnotes
-
Original PDF page 2: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.2 ↩
-
Original PDF page 1: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.1 ↩
-
Original PDF page 3: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.3 ↩
-
Original PDF page 4: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.4 ↩
-
Original PDF page 5: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.5 ↩
-
Original PDF page 6: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.6 ↩
-
Original PDF page 7: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.7 ↩
-
Original PDF page 8: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.8 ↩
-
Original PDF page 9: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.9 ↩
-
Original PDF page 10: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.10 ↩
-
Original PDF page 11: Samet and Jotkowitz - Classification and prognosis evaluation of individual teeth—A comprehensive approach, p.11 ↩