Introduction
Introduction
Before viewing this program, you should have looked at “The Study of Physical Growth”, the first module in the series. In the following program we will go into craniofacial growth in more detail. As with this and all the computer teaching programs, it’s important to read the assigned material in Contemporary Orthodontics (5th edition, pages 33-40; 4th ed., 40-47;) as well as view the program, and then take the self-test at the end.
Learning Objectives
The general learning objectives for this module are to:
- Distinguish the various types of growth in the skeletal system, and understand important related concepts
- Describe the pattern of growth of the craniofacial skeleton in detail
To meet these educational objectives, be sure that you are able to:
- describe the cellular processes involved in physical growth and the differences in soft tissue and hard tissue growth
- describe the growth of the calvarium and cranial base in 3 planes of space, identifying the sites and mode of growth
- similarly describe the growth of the maxilla, identifying the chief sites of growth, the role of surface remodeling and the effect of secondary displacement
- describe the basic processes involved in growth of the mandible and the changes that occur in each area
- describe the growth of the dental arches and identify the chief sites of growth.
Types of Skeletal Growth
Bone Growth: Cellular Level
At the cellular level, there are only three possibilities when growth occurs:
- Hyperplasia - an increase in the number of cells
- Hypertrophy - an increase in size of the cells
- Secretion of extracellular material, which contributes to an increase in size independent of the number or size of the cells themselves.
All three of these phenomena are important in craniofacial growth, including the production of extracellular material that later calcifies into bone.
Skeletal Growth: Soft Tissues vs. Hard Tissues
Calcification of extracellular material leads to a critical distinction between the soft or non-calcified tissues of the body and the hard calcified tissues.
Hard tissues are bones, teeth, and sometimes cartilages. Soft tissues are everything else. Most of the cartilage we will be talking about for craniofacial growth behaves like soft tissue and should be thought of in that way.
Growth of soft tissues occurs mostly by a combination of hyperplasia and hypertrophy. These processes go on within the tissues at all points, and the result is interstitial growth, which simply means growth inside the tissues. Secretion of extracellular material also can accompany interstitial growth, but hyperplasia primarily and hypertrophy secondarily are its characteristics.
Endochondral Ossification: Interstitial Growth
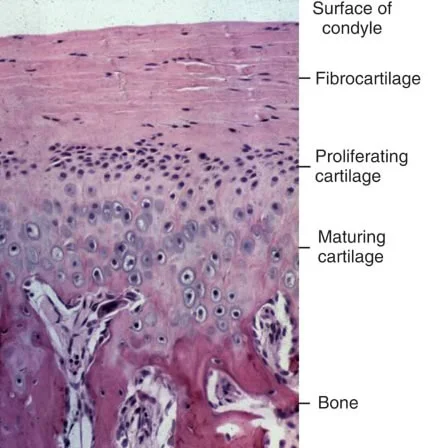
Interstitial growth is shown well in this view of a growing area at the top of the mandibular condyle. This is endochondral ossification, in which cartilage is doing the growing and then is replaced by bone (a process we will review in detail later in this program).
The cartilage is growing by all three of the methods we have described. Hyperplasia, formation of new cells, is occurring in the area below the fibrocartilage that covers the surface of the bone. Below that, note the enormous increase in the size of the maturing cartilage cells. This, of course, is hypertrophy. In addition, the cartilage cells are producing an extracellular material that lies between the cells and separates them. The hypertrophic changes are in preparation for the formation of new bone as it replaces the mature cartilage. Interstitial growth is a characteristic of uncalcified cartilage and other soft tissues.
Bone Growth: Growth of Hard Tissues
In contrast, when calcification takes place so that hard tissue is formed, interstitial growth in the calcified area becomes impossible. Significant growth occurs only at surfaces, not within the calcified mass. The interior of the calcified material can and does remodel, but it can’t grow larger because it’s too hard and rigid to expand internally.
Growth of hard tissue, therefore, occurs in two ways. The first is direct addition to the calcified tissue on its free surfaces. This occurs through the activity of cells in the periosteum, the soft tissue membrane covering the bone. Formation of new cells occurs in the periosteum, and extracellular material is secreted that then calcifies into bone. The second way is by replacement of soft tissue that grew before calcification occurred.
Many bones are modeled in cartilage originally, and the cartilage model is replaced by bone, thus the term “endochondral ossification.” In this situation, the cartilage does the growing while the bone merely replaces it. Cartilage can and does grow interstitally; bone can’t. It’s an attractive intuitive notion that bones expand more or less like a balloon being inflated. In fact, they can’t and don’t grow like that.
Growth of Long Bones: Endochondral Ossification
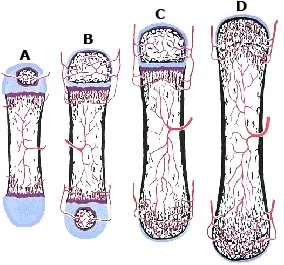
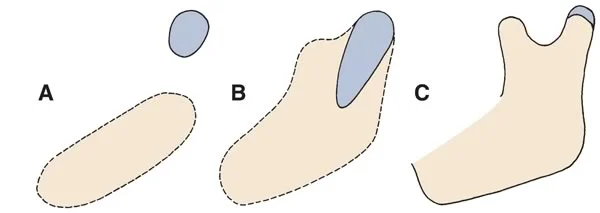
Endochondral ossification of a typical long bone with a cartilaginous precursor begins with bone formation on the surface of the cartilage. This is followed by invasion of blood vessels that produce a hollowed-out center with bone formation in that area (A in the figure).
Ingrowth of blood vessels leads to an ossification center in the cartilaginous caps on either end (B), but a band of cartilage remains between what we can now call the diaphysis (the central part) and epiphyses. These cartilage bands are the epiphyseal plates.
The bone grows longer as the cartilage of the epiphyseal plates grows, matures, and is replaced by bone (C). Eventually, the rate of replacement of the cartilage with bone exceeds the rate of cartilage growth, all the cartilage is replaced—and the bone then is as long as it can get (D).
Bone Growth: Endochondral Ossification (cont.)
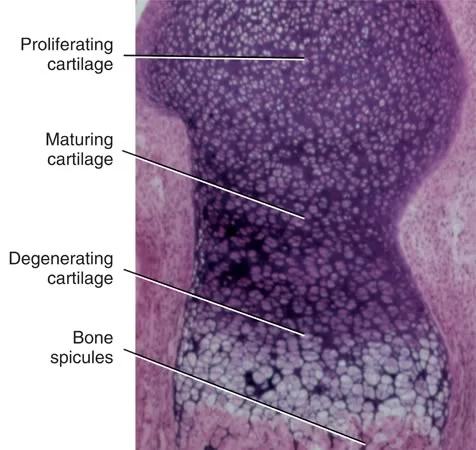
A histologic view of endochondral ossification at an epiphyseal plate shows the areas of proliferating and maturing cartilage, then replacement of degenerating mature cartilage by spicules of bone.
It is important to keep in mind that in addition to the endochondral replacement, periosteum is actively forming bone on the outer surfaces. The bone grows longer by endochondral ossification. It grows wider by direct formation of new bone on the surface.
Bone Growth: Endochondral vs. Surface Ossification
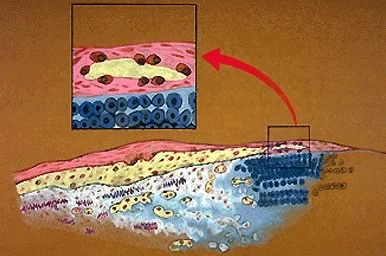
The combination of surface apposition of bone and endochondral replacement can be seen in this drawing of a growing bone. Periosteal bone formation on the surface is different from the endochondral bone formation occurring beneath it.
For endochondral bone formation, a complex maturational pattern of the cartilage is required. In direct bone formation by the periosteum, osteoblasts secrete their matrix directly in connective tissue, and it calcifies there without any intermediate formation of cartilage.
The details of this process are a review of what you learned in histology and will not be emphasized further here, but you must understand it.
Bone Growth: Endochondral vs. Surface Ossification (cont.)
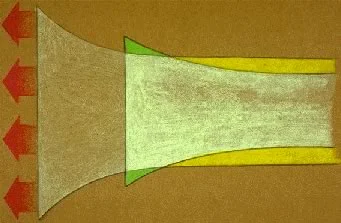
Growth at the epiphyseal plate requires corresponding changes in the surface of the bone. Not all the surface changes can be met by adding new bone. Because the contour of the long bones calls for a knob on the end, a continuous remodeling of the surface is required as endochondral growth occurs, meaning that bone must be added to the surface in some areas and removed in others.
The periosteum, therefore, must and does contain cells whose purpose is to remove bone as well as cells to make it, and there is a balance between apposition of bone in some areas and resorption in others. Addition of bone in some areas while old bone is removed in others is an essential component of the growth process.
Bone Growth: Internal Remodeling
We have said that growth within a calcified mass is impossible, but that doesn’t mean that metabolic change is impossible. In fact, osteocytes embedded in the bone are alive, and quite capable of producing internal remodeling of the bone. Calcified tissue in bones is turned over through a constant process of remodeling.
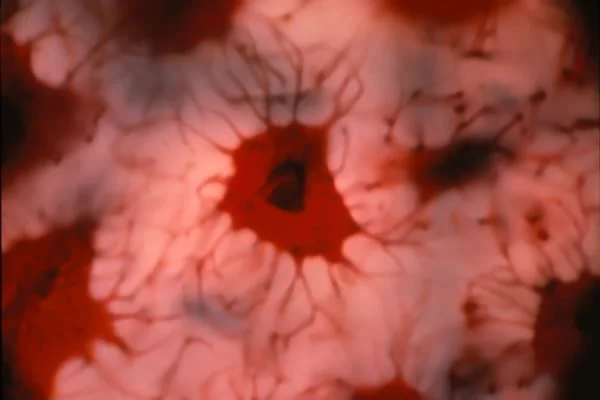
In this vital-stained section, you can see the live osteocyte with its processes extending out into the calcified bone around it. This makes it obvious how activity by a cell like this can affect calcified tissue at a distance from the cell body of the osteocyte.
Remodeling of the internal structure of bone has two major functions: it serves as a means of adapting the bone to mechanical stresses, and it also makes calcium and phosphate ions available for exchange with blood. Exchange of calcium and phosphate occurs near periosteal surfaces and around Haversian systems.
Bone Growth: Internal Remodeling (cont.)
In this decalcifed section from a bone, the larger holes are where a blood vessel was, the smaller lacunae are where the cells were. Osteocytes cluster around vascular channels, as you can see. Ingrowth of blood vessels into an area of cartilage or connective tissue is essential for ossification. It also is essential for maintenance of the calcified tissue.
A complex like the one shown here, with osteocytes surrounding a blood vessel, is called a Haversian system, and it’s constantly remodeled during life. This internal remodeling, however, does not significantly contribute to growth or change the shape of the bone. The bone can’t get bigger through internal remodeling.
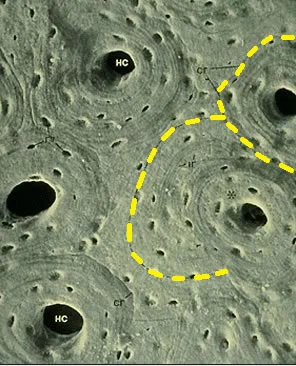
In this section of bone, you can see remnants of an old Haversian system (dotted yellow lines) being replaced by a smaller new one as the bone remodels. Bone is a dynamic tissue, constantly being rebuilt. It’s a mistake to think of it as just an inert scaffold on which the other tissues are suspended.
Cranial and Maxillary Growth
Regions of the Cranium and Face
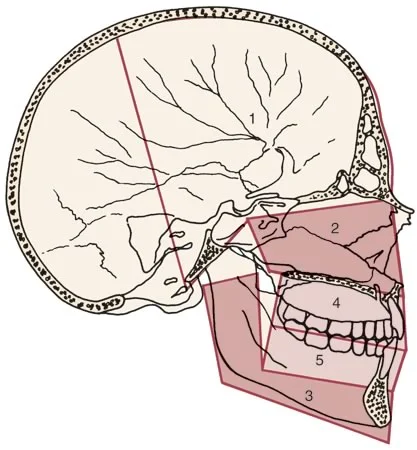
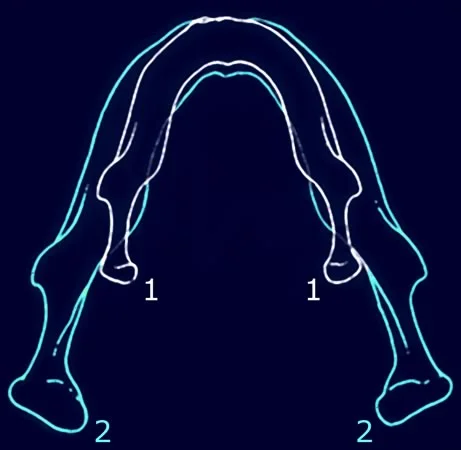
With the general principles of bone growth established, let’s look in more detail at growth of the cranium and face. For this discussion, it will be convenient to divide the cranium and face into two areas each:
For the cranium (labeled 1 in this image): The cranial vault and cranial base.
For the face: The naso-maxillary complex (2) and the mandible(3).
The special features of growth of the dentoalveolar processes (4, 5) and eruption of the teeth will be considered later.
Skeletal Growth: Cranial Vault
Let’s begin by examining the cranial vault. It is made up of a number of flat bones that are formed directly by periosteum. Endochondral bone formation has no role here, and there’s never any cartilage in the vicinity. Instead, growth occurs entirely by periosteal activity at the surfaces of the bones, both at the flat inner and outer surfaces and the periosteum-lined spaces between them.
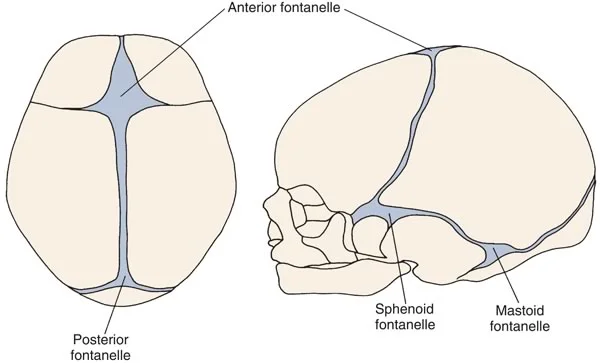
At birth, the bones are rather widely separated by connective tissues, and these open spaces are called fontanelles. The presence of the fontanelles allows considerable deformation at birth, which is important in getting the relatively large head through the birth canal.
Apposition of bone along the edges of the fontanelles eliminates these open spaces fairly quickly after birth, but the bones remain separated by thin periosteum-lined sutures for years.
Despite their small size, apposition of bone at the sutures is the major mechanism for growth of the cranial vault. In addition, there is a tendency for bone to be removed from the inner surface of each bone and added to the outer surface, especially in some areas where contours change. The magnitude of the remodeling changes, however, is much less than the growth at sutures.
Skeletal Growth: Cranial Base
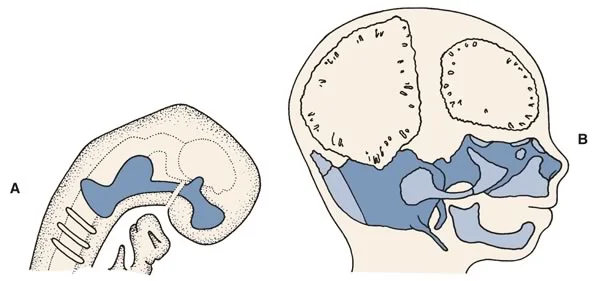
In contrast to the cranial vault, the bones of the cranial base (particularly in the midline) are formed initially in cartilage, then transformed into bone. At about 8 weeks in utero (image A), before any bone formation has begun, an essentially solid bar of cartilage extends beneath the brain from the nasal capsule anteriorly to the occipital area posteriorly. This cartilage is called the chondocranium.
At 12 weeks (image B), ossification centers have appeared in the midline cartilage structures. In addition, intramembranous bone formation has begun in the cranial vault (B in the Figure). From this point on, bone (dark blue color) replaces the original chondrocranium rapidly, but remnants of it persist as small cartilaginous synchondroses and remain between the developing occipital, sphenoid and ethmoid bones.
Skeletal Growth: Cranial Base (cont.)
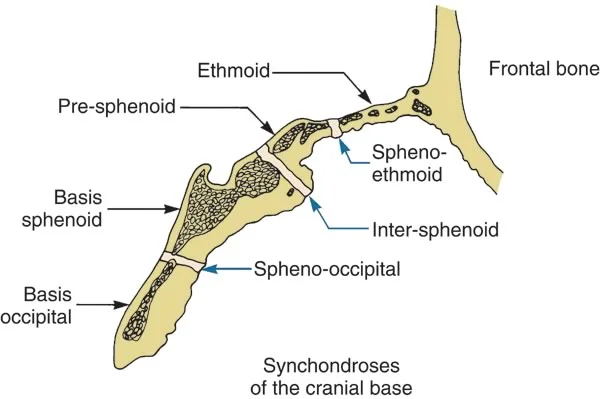
It should come as no surprise that the lengthening of the cranial base is largely due to endochondral replacement. As one moves laterally beneath the brain, growth at sutures and surface remodeling become more important, but the cranial base is essentially a midline structure, and the synchondroses are important growth sites. The most important ones are the spheno-occiptal, inter-sphenoid and spheno-ethmoidal synchondroses.
Synchondrosis vs. Suture
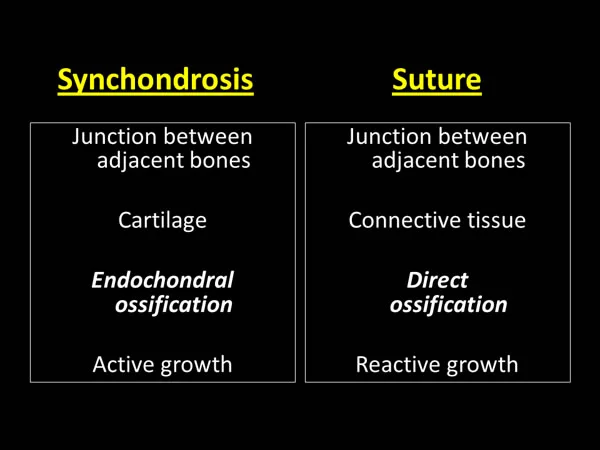
Be sure you understand the difference between a suture and a synchondrosis. Both are thin soft tissue areas between adjacent bones, but the synchondrosis is filled with cartilage. A band of proliferating cartilage cells is located in the center of the synchondrosis, and a band of maturing cartilage extends in both directions away from the center. Endochondral ossification occurs at both margins.
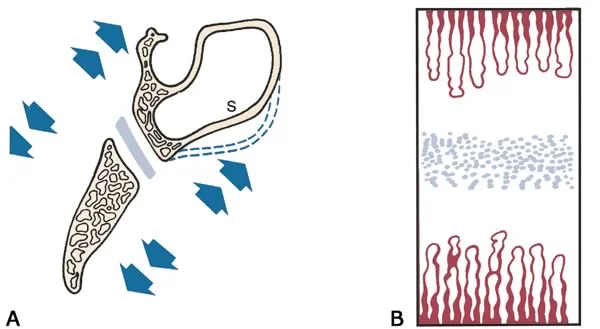
Synchondrosis vs. Suture (cont.)
In contrast, a suture has only periosteum and connective tissue. At the synchondrosis, bone formation proceeds by cartilage replacement, while for sutures, there is no intermediate cartilage stage.
As you will see when we review growth control, the difference is significant: the cartilage at synchondroses is capable of active, independent growth while the connective tissue at sutures only reacts to what happens in its surroundings.
Skeletal Growth: Maxilla
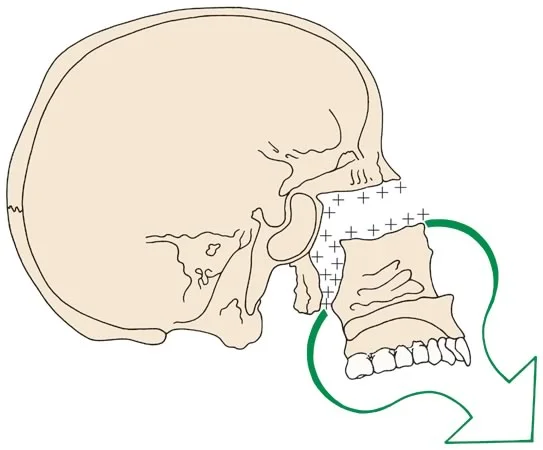
Now let’s consider the maxilla and the associated smaller nasal and palatine bones. Postnatally, the face grows downward and forward from the cranium, and the maxilla must move a considerable distance. How this occurs, and what changes accompany the growth, are what we must focus on now. In the case of the maxilla, there is no pre-existing cartilage, so maxillary growth is a matter of sutures and surface remodeling.
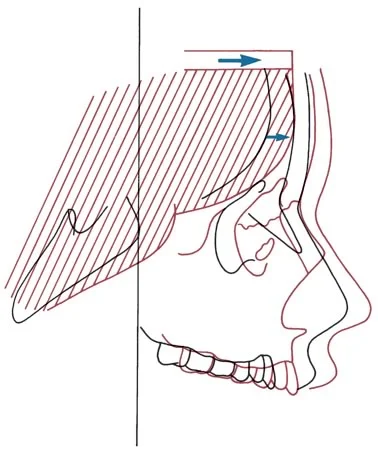
In contrast to the cranial vault, however, surface remodeling changes are quite dramatic and important. In addition, as this figure shows, the naso-maxillary complex is affected indirectly by the endochondral growth of the cranial base, which pushes the maxilla forward and thereby contributes to its forward translation. How long would this mechanism of growth be effective? Only as long as the cranial base is growing—and that ends at about the time brain growth ends, at about age 6.
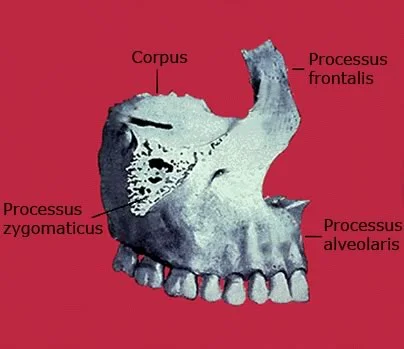
Skeletal Growth: Maxilla (cont.)
Let’s look in more detail at the right half of the maxilla in this figure. Note that it forms the floor of the orbit, the lateral wall of the nose, the roof of the mouth and the lateral aspects of the facial skeleton. There are sutures posteriorly along the maxillary tuberosity, superiorly at the end of the frontal process, and superiorly-laterally along the zygomatic process.
There’s also a suture in the midline down the middle of the palate, providing a mechanism for the midface and upper dental arch to become wider. Growth occurs by apposition at the sutures and by remodeling of the surfaces.
Growth at Sutures and Surfaces of the Maxilla
It is apparent that the posterior and superior sutures of the maxilla are ideally situated to allow downward and forward repositioning. As the maxilla moves in that direction, new bone is added at the sutures to maintain its connection to the cranium.
The space that would otherwise open up at the sutures is filled in by proliferation of bone, so the sutures remain the same width but the various processes of the maxilla become longer. As the drawing illustrates, this requires moving the maxilla away from the structures above and behind it.
Part of the posterior border of the maxilla, in the tuberosity area, is a free surface. Bone is added to this area, creating additional space into which the molar teeth can erupt.
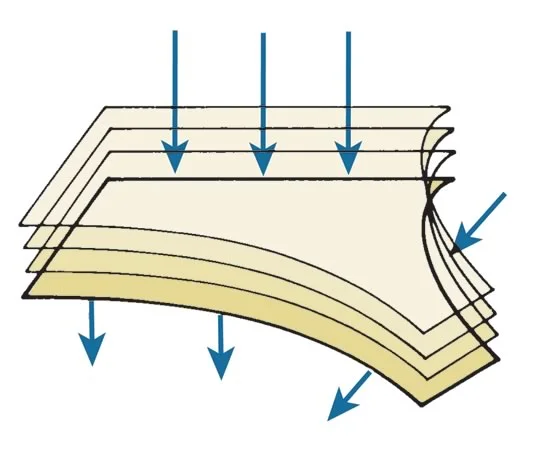
Surface Resorption in Growth of Maxilla
As the maxilla grows down and forward, its front surfaces are remodeled, and bone is actually removed from most of the anterior surface.
In this three-quarter view (Image 1), areas of resorption are more darkly shaded. Note that almost the whole anterior surface is a resorptive area–which seems backward to what you might think it should be. If you look at it in profile (Image 2), there’s a little apposition at the anterior nasal spine and just below it, but all the other surfaces are resorptive.
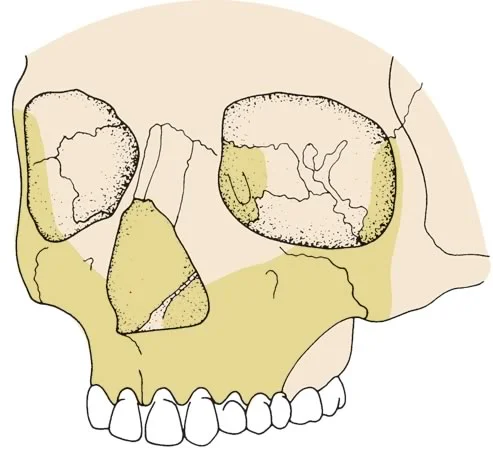 Image 1 Image 1 | 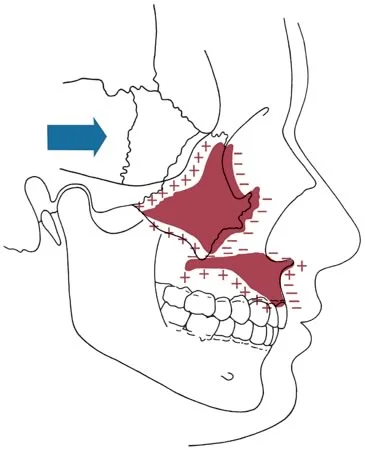 Image 2 Image 2 |
Translation and Remodeling
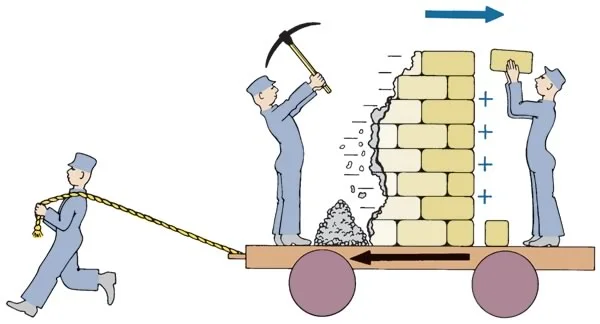
What takes place as the maxilla grows is represented by this cartoon. The whole bone is moving downward and forward relative to the cranium, being translated in space. This is exemplified in the cartoon by the platform on wheels.
At the same time, the front surface, represented in the cartoon by the wall, is being reduced on its anterior side and built up posteriorly, so that it moves in space opposite to the direction of overall growth.
How do we know this remodeling occurs? Vital staining shows this quite nicely, as you saw with the zygomatic arch in Module 1. How do we know that translation occurs? Superimposed tracings of cephalometric x-rays are a good way to show that.
Translation and Remodeling (cont.)
It’s not always true that surface remodeling opposes the direction of translation. Depending on location, translation and remodeling may have an additive effect or may oppose each other. Look in more detail at what happens to surfaces in the palatal area during growth.
The maxilla is being translated downward and forward. At the same time the floor of the nose is resorbing and bone is being added to the roof of the mouth, so remodeling adds to the movement of those structures. But the front surface below the anterior nasal spine is resorbing, so the surface changes opposes the direction of translation there.
Translation and Remodeling: An Overall View
In this overall view of the movement of the dental portions of the maxilla during growth (using cephalometric tracings superimposed on the cranial base), you can see that the maxilla seems to be moving more downward than forward.
It looks like that because the direction of surface remodeling opposes forward translation of the maxilla but adds to the downward component.
Summary: Overall Pattern of Maxillary Growth
The overall pattern of maxillary growth can be summarized as follows:
- As the bone moves downward and forward, new bone is added at the sutures and the tuberosity.
- Anterior surfaces resorb, while the roof of the mouth moves further down by remodeling.
- The remodeling of the roof of the mouth means, among other things, that you can’t judge how much a tooth has erupted by measuring how far it is from the height of the palatal vault.
If you understand that, you have grasped the concept of remodeling in relation to maxillary growth. If you don’t, go back and review this section and make some drawings.
Mandibular and Dento-Alveolar Bone Growth
Skeletal Growth: Mandible
Growth of the mandible is different in many ways from growth of the maxilla. The difference begins with its relationship to the chondro-cranium. The mandible has a cartilage model, of sorts (Meckel’s cartilage, a cartilaginous bar in the mandibular arch whose proximal ends eventually ossify to form the malleus of the middle ear). But the mandible develops more in association with that cartilage than by replacing it.
Bone formation begins just lateral to Meckel’s cartilage and spreads posteriorly along it without any direct replacement of the cartilage by the newly forming bone.The two halves fuse very early, so for all practical purposes, a growing mandible, even in fetal life, is a single bone extending across the midline.
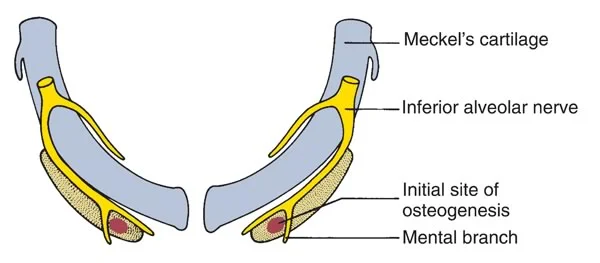
Origin and Growth of the Condylar Cartilage
There is some cartilage that covers the surface of the condyle at the temporomandibular (TM) joint, but it appears relatively late in embryonic life and is not derived from Meckel’s cartilage. It begins formation separately from the body of the mandible and fuses with the bone at about 4 months in utero, as shown in the figure.
This cartilage is not like the cartilage at an epiphyseal plate or synchondrosis, but hyperplasia, hypertrophy, and endochondral replacement do occur there. All other areas of the mandible are formed and grow by direct surface apposition and remodeling.
Pattern of Mandibular Growth
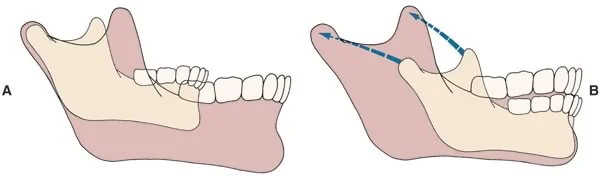
The overall pattern of growth of the mandible can be represented in two ways. Depending on your frame of reference, both are correct.
If you hold the cranium constant and look at mandibular growth relative to it (A), the chin moves downward and forward a long way relative to the cranium, so you might think that new bone was added anteriorly. But, if you look specifically at the sites of growth on the bone as revealed by vital staining and similar techniques, very little change occurs at the chin and most of the growth is posteriorly (B). Superimposing on the chin correctly shows that the body of the mandible grows longer by apposition of bone on the posterior surface, and the ramus grows higher by endochondral replacement at the condyle and by surface remodeling.
Pattern of Mandibular Growth (cont.)
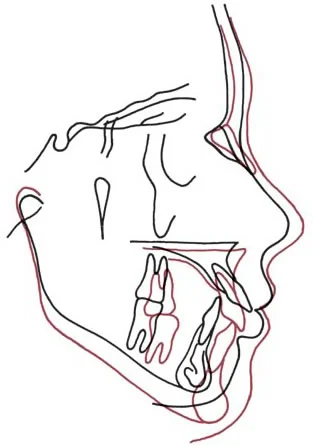
From cephalometric tracings superimposed on the cranial base, the overall growth pattern of the mandible looks like this: the bone moves downward and forward, taking the teeth with it (Image 1).
The position of the TM joint can change because of changes in the posterior cranial base, but usually it remains about in the same place.
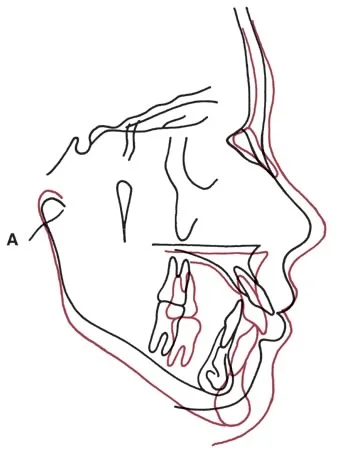
If the x-ray tracings are superimposed at the chin so that the anterior mandible is held constant, then it appears that the mandible grows upward and backward (Image 2). In fact, this is where new bone is added, by a combination of endochondral replacement at the head of the condyle and surface apposition.
Can you visualize the correctness of the statement that the mandible grows upward and backward, but the effect of this growth is a downward and forward translation of the chin? If that’s clear, you understand an important concept.
| Image 1, superimposition of a growing patient, registered on the cranial base: Superimposed on the cranial base, the maxilla, mandible, and teeth all appear to have moved downward and forward with growth. The red tracing represents the second time point. | Image 2, superimposition registered on the chin: Superimposition on the chin shows the correct pattern of mandibular growth: growth is upward and backward at the condyle and ramus. |
Remodeling Resorption
Nowhere is there a better example of remodeling resorption than in the backward movement of the ramus of the mandible. During growth, new bone is added on the posterior surface of the ramus. At the same time, bone is removed—large quantities of bone—from the anterior surface of the ramus. Bone from the tip of the condylar process early in life can be found at the anterior surface of the ramus some years later. The body of the mandible grows longer as the ramus moves away from the chin.
Growth by Remodeling of the Mandible
How is this possible? Remember the previous cartoon: this movement occurs the same way as a wall could be moved by removing stones from the front side and adding them to the back.
Looking at mandibles at different ages, you might think there had to be a growth center somewhere under the teeth, so the chin could grow forward away from the ramus. But that is not possible, since interstitial bone growth is impossible. Instead, the ramus remodels. What was the posterior surface at one time becomes the center at a later date, and eventually may become the anterior surface and then disappear.
Removing bone from the posterior surface of the ramus also makes space available for the molar teeth to erupt.
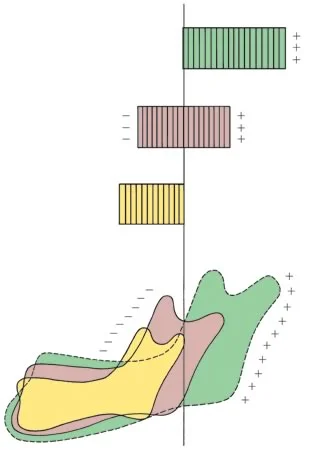
Growth by Remodeling of the Mandible (cont.)
Looking down on top of the mandible, the effect of this remodeling can be seen clearly. This is the type of superimposition that metallic implants make possible. Note that surface remodeling also has made the bone wider.
There’s no midline suture like the one for the maxilla, so the ramus also is widened by surface remodeling. The old condyles are totally resorbed after a while, as the ramus widens by removing bone from the inside and adding it outside.
Summary: Growth of the Mandible
Mandibular growth can be summarized like this:
- a large amount of bone is added on the posterior and superior surfaces of the ramus
- nearly as much bone is removed from the anterior surface of the ramus
- there are smaller remodeling changes elsewhere
- bone is added to some outer surfaces and removed from some inner surfaces, especially in the extensive remodeling of the ramus.
Skeletal Growth: Alveolar Processes of Maxilla and Mandible
In talking about craniofacial bone growth, we have made little mention of the alveolar processes of the maxilla and mandible. In both jaws, growth of the bone that supports the teeth is an important aspect of the overall growth process.
One way to think about it is that the mandible grows downward away from the maxilla, creating more space between the jaws. As the jaws grow, the teeth are actively erupting (they have to in order to maintain contact), and as they erupt they bring alveolar bone with them, so that the alveolar processes become taller. Note in this cephalometric superimposition how the teeth erupted to compensate for greater downward movement of the mandible than the maxilla. If new alveolar bone didn’t form, the teeth would just grow right out of the bone. We’ll be looking more at what happens to the teeth during growth in the later part of this course.
Summary
To summarize the important points:
First, you certainly should understand that bone cannot grow interstitially, and the growth of the facial skeleton cannot be explained in that way. Where interstitial growth is important for the skeleton, a layer of cartilage in that area does the growing, and then bone replaces it.
Second, with regard to the sites and types of growth in the cranium and cranial base:
- Growth of the cranium occurs largely at the sutures, with a little surface remodeling;
- The cranial base grows largely by endochondral replacement at the mid-line synchondroses, but also by apposition at sutures laterally;
Additionally, with regard to the sites and types of growth in the jaws and face:
- Growth of the maxilla and associated structures is a combination of growth at sutures and surface remodeling. As the maxilla is translated downward and forward during growth, bone fills in at the superior and posterior sutures and is added at the tuberosity;
- The mandible grows largely by apposition and remodeling resorption of the ramus, and by endochondral replacement at the condyles;
- The alveolar processes of both jaws grow as the teeth erupt, bring bone with them.
Self-Test Referral
Now take the self-test in the following section of this module to ensure that you understand what you have learned. Before you do, be sure you have read the assigned material in Contemporary Orthodontics (5th edition: pages 33-40; 4th edition: pages 40-47).
Self-Test
Question 1
In growth of the craniofacial skeleton, which of the following cellular activities is most active?
- Hyperplasia
- Hypertrophy
- Secretion of extracellular material ✓
- All are equally important
Correct
That is correct. Although all the cellular processes are important, secretion of extracullar material is particularly important in growth of the skeletal system, in which the extracellular material later calcifies into bone. Cartilage cells mature and secrete extracellular matrix that becomes calcified; osteoblasts also later form new bone by secreting extracellular matrix that calcifies.
Incorrect
No, that’s incorrect. Although all the cellular processes are vital for growth, secretion of extracellular material is particularly important in growth of the skeletal system, in which the extracellular material later calcifies into bone. Cartilage cells mature and secrete extracellular matrix that becomes calcified; osteoblasts also later form new bone by secreting extracellular matrix that calcifies.
Question 2
In growth of the cranial and facial soft tissues, which of the following cellular activities is the least important?
- Hyperplasia
- Hypertrophy
- Secretion of extracellular material ✓
- All are equally important
Correct
That’s right. Secretion of extracellular material can occur as soft tissues are formed, but this is not an important characteristic of growth of the craniofacial soft tissues.
Incorrect
No, that’s wrong. Secretion of extracellular material can occur as soft tissues are formed, but is not an important characteristic of growth of the craniofacial soft tissues. Hyperplasia primarily and hypertrophy secondarily are the major characteristics of soft tissue growth.
Question 3
(A) Interstitial growth does not occur in the growth of calcified tissues because (B) the rigid calcified tissue mass cannot expand internally.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A True, B false
- A false, B true
- A and B false
Correct
That’s right. Calcified tissues don’t grow by interstitial growth that leads to external expansion, because it’s physically impossible. So these statements are both true and they’re related.
Incorrect
No, you’re wrong. Both statements are true and related. Calcified tissues don’t grow by interstitial growth that leads to external expansion, because it’s physically impossible.
Question 4
Which of the following statements best describes the growth of a long bone of the limbs?
- The bone is formed in cartilage and replaced by endochondral ossification
- Cartilage does all the growing, then is replaced by bone
- A little cartilage is present originally, but most of the growth is bone apposition
- Both replacement of cartilage and direct apposition of bone are major contributors to the growth ✓
- None of the above, there’s no role for cartilage except in facial growth
Correct
That’s right. Replacement of cartilage that grows at the epiphyseal plates is very important, but so is direct apposition of bone at the periosteum.
Incorrect
No, that’s wrong. The correct answer is (4). Both replacement of cartilage and direct apposition of bone are major contributors to the growth. Replacement of cartilage that grows at the epiphyseal plates is very important, but so is direct apposition of bone at the periosteum. As important as the cartilage growth is, you mustn’t overlook the equal importance of the apposition (and remodeling) at the periosteal surface.
Question 5
(A) Significant interstitial remodeling of long bones occurs around Haversian systems because (B) the final increments of bone growth are obtained in this manner.
- A true, B true, A And B related
- A true, B true, A and B not related
- A true, B false ✓
- A false, B true
- A and B false
Correct
That’s correct. It’s true that long bones remodel internally around their Haversian systems, but this has almost nothing to do with growth, so the first statement is true but the second is false.
Incorrect
No, that’s incorrect. It’s true that long bones remodel internally around their Haversian systems, but this has almost nothing to do with growth, so the first statement is true and the second statement is false.
Question 6
(A) Formation of bone always requires the intermediate step of cartilage formation because (B) osteoblasts must secrete their matrix on a framework of calcified cartilage.
- A true, B true, A And B related
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false ✓
Correct
That’s correct, both statements are false. Bone can be (and often is) formed without an intermediate cartilage step, because osteoclasts can secrete their matrix directly in connective tissue.
Incorrect
That’s incorrect, both statements are false. Bone can be (and often is) formed without an intermediate cartilage stop, because osteoclasts can secrete their matrix directly in connective tissue.
Question 7
Growth of the cranial vault involves which of the following processes?
(1) endochondral ossification at multiple growth centers
(2) apposition of new bone at sutures
(3) apposition of new bone on external surfaces
(4) apposition of new bone on internal surfaces
- 1 and 2
- 2 and 3 ✓
- 2, 4 and 4
- All of the above
Correct
That’s right, the cranial vault grows primarily by apposition of new bone at the sutures, and to a smaller extent by adding new bone on the outer surfaces, so the second and third statements are correct. There aren’t any growth centers in the cranium and no endochondral ossification, and bone is removed rather than added on the internal surfaces, so the first and last statements are incorrect.
Incorrect
No, that’s wrong. The cranial vault grows primarily by apposition of new bone at the sutures, and to a smaller extent by adding new bone on the outer surfaces, so the second and third statements are correct. There aren’t any growth centers in the cranium and no endochondral ossification, and bone is removed rather than added on the internal surfaces, so the first and last statements are incorrect.
Question 8
Which of the following types of growth is most important in the cranial base?
- endochondral ossification at multiple growth centers ✓
- apposition of new bone along suture lines
- apposition of new bone on external surfaces
- removal of bone from internal surfaces
Correct
That’s right, all of these processes are involved to some extent in growth of the cranial base—but cartilage growth and endochondral replacement of bone at the midline synchondroses are particularly important in lengthening the cranial base and projecting the midface forward.
Incorrect
No, that’s incorrect. All of these processes are involved to some extent in growth of the cranial base–but cartilage growth and endochondral replacement of bone at the midline synchondroses are particularly important in lengthening the cranial base.
Question 9
Growth of the maxilla involves which of the following processes?
(1) endochondral ossification at multiple growth centers
(2) apposition of new bone along suture lines
(3) apposition of new bone on external surfaces
(4) removal of bone from external or internal surfaces
- 1 and 2
- 2 and 3
- 3 and 4
- 2, 3 and 4 ✓
- all of the above
Correct
That’s right, there’s no direct endochondral ossification and no cartilaginous growth centers in maxillary growth, and both growth at sutures and surface remodeling are important. Compared to the cranium, the maxilla has less sutural growth and more remodeling partly because it’s pushed forward by growth of the cranial base behind it and remodeling occurs in response to that.
Incorrect
No, that’s wrong. There’s no direct endochondral ossification and no cartilaginous growth centers in maxillary growth, so the first statement is incorrect. Both growth at sutures and surface remodeling (in the form of internal and external apposition and resorption) are important, so the other three statements are correct. Compared to the cranium, the maxilla has less sutural growth and more remodeling, partly because it’s pushed forward by growth of the cranial base behind it and remodeling occurs in response to that.
Question 10
What is the major area for addition of new bone to the surface of the maxilla during growth?
- tuberosity ✓
- upper anterior surface
- lower anterior surface
- paranasal areas
- all of the above, bone is added to all surfaces about equally
Correct
That’s right, the main area of the maxilla where bone is added during growth is the tuberosity. Formation of new bone here allows the dental arch to become longer during growth and provides space of the molar teeth as they erupt. Most of the anterior surfaces, in contrast, are resorbed rather than added to during growth.
Incorrect
No, that’s wrong. The main area of the maxilla where bone is added during growth is the tuberosity. Formation of new bone here allows the dental arch to become longer during growth and provides space of the molar teeth as they erupt. Most of the anterior surfaces, in contrast, are resorbed rather than added to during growth.
Question 11
Which of the following mechanisms move the roof of the mouth downward during growth?
(1) endochondral ossification at the back of the maxilla
(2) displacement of the maxillary core from the cranium and cranial base
(3) apposition of bone on the inferior surface of the palatal bone
(4) resorption of bone on the nasal surface of the palatal bone
- 1 only
- 2 only
- 2 and 3
- 2, 3 and 4 ✓
- all of the above
Correct
That’s right. No endochondral ossification is involved in downward movement of the roof of the mouth, but displacement of the core of the maxilla and remodeling of the bony surfaces are important. In some instances, with the roof of the mouth being an excellent example, the direction of remodeling is the same as the direction of displacement.
Incorrect
That’s wrong. No endochondral ossification is involved in downward movement of the roof of the mouth, but displacement of the core of the maxilla and remodeling of the bony surfaces are important. The first statement is incorrect, the other three are correct. In some instances, with the roof of the mouth being an excellent example, the direction of remodeling is the same as the direction of displacement.
Question 12
(A) Most aspects of mandibular growth can be explained by endochondral ossification because (B) a cartilaginous model of the mandible forms early in embryonic life and then resorbs.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true ✓
- A and B false
Correct
That’s correct. The first statement (A) is false, but the second statement (B) is true. Mandibular growth is mostly a surface phenomenon, and endochondral ossification at the condyle plays a smaller role, so the first statement is false. It’s true that a cartilaginous model of the mandible forms early in life and then resorbs, although the new, primarily membranous mandible forms alongside it without really replacing it in the classic form of endochondral bone growth.
Incorrect
No, that’s wrong. Mandibular growth is mostly a surface phenomenon, and endochondral ossification at the condyle plays a smaller role, so the first statement is false. It’s true that a cartilaginous model of the mandible forms early in life and then resorbs, so the second statement is true, although the cartilage resorbs and the new, primarily membranous mandible forms alongside it without really replacing it in the classic form of endochondral bone growth.
Question 13
Which of the following is the best illustration of remodeling resorption?
- backward movement of the mandibular ramus ✓
- forward movement of the chin
- lateral movement of the mandibular alveolar process
- backward movement of the maxillary tuberosity
Correct
That’s correct. The ramus moves backward as bone is removed from its front surface and added to the back. There’s so much remodeling that in a young child, what at one time was the back surface eventually becomes the front surface and then is resorbed away.
Incorrect
No, that’s incorrect. The best illustration of remodeling resorption in the face by far is the backward movement of the mandibular ramus. It moves backward as bone is removed from its front surface and added to the back. There’s so much remodeling that in a young child, what at one time was the back surface eventually becomes the front surface and then is resorbed away. There’s a little remodeling at the chin and the alveolar process, next to none at the tubererosity.
Question 14
Which of the following is not an area of significant bone apposition during mandibular growth?
- posterior border of ramus
- superior border of ramus
- alveolar process
- chin ✓
Correct
That’s right. Little or no bone is added at the chin during mandibular growth, and the area immediately above the chin prominence usually is resorptive. In contrast, there is major apposition of bone in the other areas.
Incorrect
No, that’s incorrect. Little or no bone is added at the chin during mandibular growth, and the area immediately above the chin prominence usually is resorptive. Bone is added all along the posterior and superior (but not the anterior) surfaces of the ramus and at the alveolar process. The correct answer is (4) chin.
Question 15
After it first comes into occlusal contact with its antagonists at about age 6, how much further does a typical permanent first molar erupt?
- stops after coming into occlusion
- 1-2 mm
- 3-5 mm
- 10 mm or more ✓
Correct
That’s correct, after it comes into occlusion a typical first molar has to erupt a centimeter or more. The mandible grows away from the maxilla, creating a space into which the teeth have to erupt to stay in occlusion, and there’s a lot of vertical growth after age 6.
Incorrect
No, that’s wrong. After it comes into occlusion a typical first molar has to erupt a centimeter or more. The mandible grows away from the maxilla, creating a space into which the teeth have to erupt to stay in occlusion, and there’s a lot of vertical growth after age 6. If the teeth don’t erupt, an open bite develops.
Question 16
Which of the following is a site of interstitial growth?
- synchondrosis of cranial base ✓
- roof of the mouth
- ramus of the mandible
- maxillary tuberosity
- none of the above
Correct
That’s right, the synchondrosis contains cartilage that can and does grow interstitially, but the other bony areas can’t grow interstitially.
Incorrect
No, that’s incorrect. The synchrondoses of the cranial base contain cartilage that can and does grow interstitially, but the other bony areas can’t do that.