Pre-Emergent Eruption
Introduction
Dentists, of course, deal with erupting human teeth all the time—because although tooth eruption declines to a very slow level in adults, it never really stops as long as the very slow jaw growth that is characteristic of human adults continues. We will be talking more about adult growth in a later module, but probably you already know that jaw growth usually continues in adults up to and often beyond age 50. In children and adolescents, you already have learned about the major changes in the developing dentition and when they occur.
But it has been very difficult to determine both the mechanism that produces eruption of the permanent teeth and how their eruption is controlled. This goal of this module is to bring you up to date on what we know about the process of tooth eruption.
In addition to viewing the module, be sure to read pages 74-80 in the 5th edition of Contemporary Orthodontics (87-93 in the 4th ed.)
Sequence of Steps in Tooth Eruption
Eruption of human teeth is most conveniently described in the context of two major phases and six total steps or stages.
The first major phase is pre-emergent eruption, defined as the events that occur while the tooth is moving within the bone of the jaws and penetrating the gingiva. It has two steps:
- crown formation
- movement toward emergence
The second major phase is post-emergent eruption, defined as the events that occur after the tooth has emerged into the oral cavity. It has four steps:
- the post-emergent spurt, as the tooth moves up to the occlusal plane
- juvenile occlusal equilibrium
- pubertal eruption spurt
- adult occlusal equilibrium
In the latter three steps, the rate of eruption coincides with the rate of vertical growth of the face.
Crown Formation
In a sense, crown formation is the first step in tooth eruption, but only in an honorary sense—because the tooth doesn’t move from the spot where crown formation began until formation of the root begins. It’s what doesn’t happen that’s important.
You have learned about cell types and their interaction during crown formation in histology, and we do not need to review the differentiation of cell types and formation of enamel and dentin at this point. What you need to know now is how these events relate to eruptive movement of the developing tooth. The point is, of course, that they don’t. In contrast, root formation and formation of cementum do relate to eruption. Eruptive movement of a tooth begins as soon as enamel formation ends and root formation begins.
You already have learned something about the use of implants in the jaws to create markers that don’t move as surface changes in the bone occur. How do we know that teeth don’t begin eruptive movements until crown formation starts? Because you can see this when implant superimpositions are done. The tooth stays in the same place relative to its surrounding bone until crown formation is completed. Knowing this now allows us to use teeth at this stage as points for superimposition of cephalometric radiographs, in the same way as metallic implants. Third molars are still in the crown formation stage at the ages when orthodontic treatment usually occurs, and are the teeth most likely to be used in this way.
Pre-Emergent Eruptive Movements
In order for pre-emergent eruption to occur, two things have to happen: resorption of bone over the crown of the tooth, and development of a force to move the tooth. It seems reasonable that as root formation begins, the tooth is forced against the overlying bone and primary tooth roots (if it’s a succedaneous tooth), and this activates osteoclasts and causes the resorption.
Some years ago, an anatomist did an interesting experiment. He ligated tooth buds in young beagle dogs to the lower border of the mandible so that teeth couldn’t erupt. What happened? The teeth didn’t erupt, but bone resorption occurred anyway, opening a path along which the tooth was meant to erupt. The experiment showed that the controlling element in pre-emergent eruption wasn’t the development of an eruption force. Instead, resorption removed bone, and then the tooth moved along the path that had been cleared.
Odontoclasts begin to remove bone over the crown of a tooth just at the point that root formation begins. How do they know that root formation has started? As we outlined previously in Module 6, the inhibition of the osteoclasts over the crown that related to amelogenesis ends, and they are up-regulated and become active as cementogenesis begins.

Human Evidence
Inadvertent experiments in humans have demonstrated that the same thing happens in humans when a forming tooth is ligated to the bone. This has happened several times when a jaw fracture was wired in place, and the wire passed through a tooth bud.
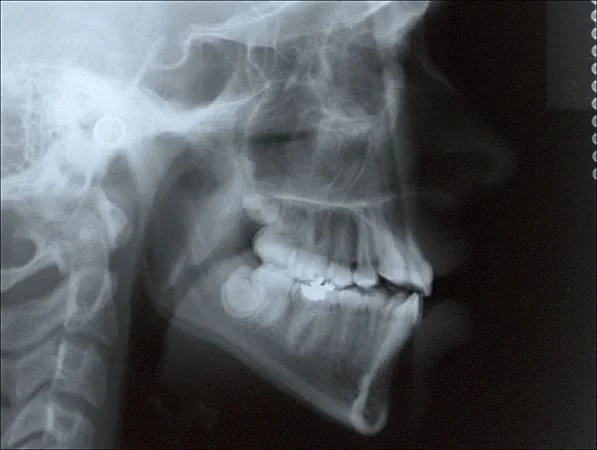
You have already seen the dramatic contrast in eruption of mandibular canines when one of them was ligated during treatment of a mandibular fracture (images 1 and 2). The eruption path was cleared on both sides, the unimpeded tooth followed the path and the ligated one didn’t. Image 3 shows the same thing, a cleared eruption path that the tooth couldn’t follow, with a second molar that was wired in place when a jaw fracture was treated in Raleigh, NC.
Normally, an erupting tooth follows closely along the path that has been cleared for it, as the right canine did in image 2. A cleared path with no eruption along it (described as an uncoupling of resorption from eruption) means that there’s a problem with the eruption mechanism—either mechanical interference, as in these patients, or because something is wrong with the mechanism itself.
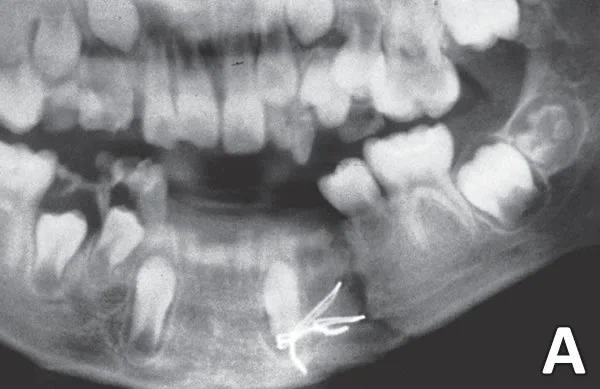 Image 1: Age 10, immediately after treatment for a mandibular fracture through the body of the mandible on the right side. Image 1: Age 10, immediately after treatment for a mandibular fracture through the body of the mandible on the right side. | 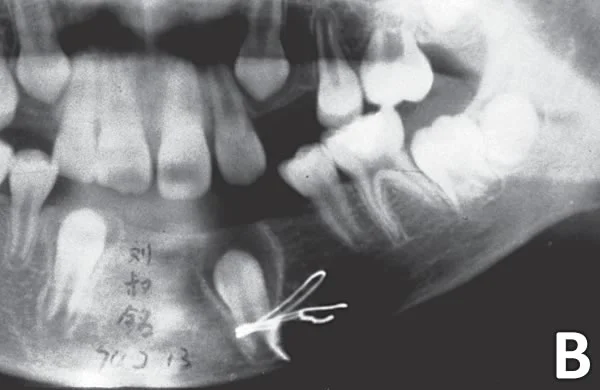 Image 2: One year later (courtesy Dr. John Lin). Image 2: One year later (courtesy Dr. John Lin). |
 Image 3: An inadvertently ligated second molar in another child treated for a mandibular fracture. Note that the eruption path has been cleared even though the tooth can’t move along it.. Image 3: An inadvertently ligated second molar in another child treated for a mandibular fracture. Note that the eruption path has been cleared even though the tooth can’t move along it.. |
Altered Eruption Paths
What would happen if the crown of an unerupted tooth was not oriented toward the occlusal plane? Would an eruption path aimed in the wrong direction be the result?
The answer is yes—an eruption path in the wrong direction is entirely possible. For some reason this is particularly likely to occur with mandibular second premolars. It happens almost as often with maxillary canines, and can affect any tooth.
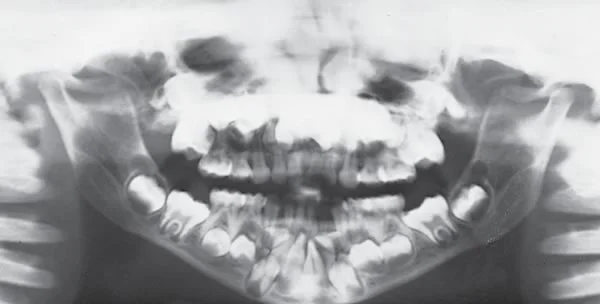
This series of images shows mandibular second premolars with various degrees of improper orientation and eruption in the wrong direction. In image 1, note the distally-oriented 2nd premolars bilaterally. On the right side, the 2nd premolar probably will be guided into position by the root of the 1st molar. On the left side the first molar has been lost, and the 2nd premolar has erupted toward the 2nd molar, which may guide it to erupt into the space where the first molar used to be. If the 2nd premolar is oriented almost horizontally, it can cause resorption of molar roots (images 2 and 3), and can go into the ramus and to the tip of the coronoid process if all the molars are lost (image 4). The osteoclasts just keep clearing a path, and the tooth moves along it!
When the osteoclasts run out of bone and into soft tissue that isn’t gingiva, they usually stop, but canines have been known to erupt into the nose.
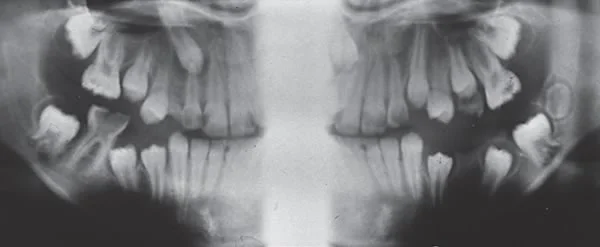 Image 1: Note the distally-oriented mandibular 2nd premolars on both sides. Image 1: Note the distally-oriented mandibular 2nd premolars on both sides. | 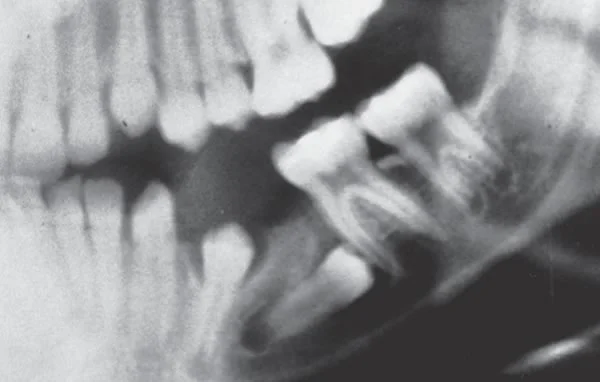 Image 2: Resorption over the crown of this horizontally-positioned 2nd premolar is likely to cause resorption of the roots of the 2nd molar. Image 2: Resorption over the crown of this horizontally-positioned 2nd premolar is likely to cause resorption of the roots of the 2nd molar. |
 Image 3: For this patient, both the 1st and 2nd premolars erupted beneath the 1st and 2nd molars, causing obvious root resorption. Image 3: For this patient, both the 1st and 2nd premolars erupted beneath the 1st and 2nd molars, causing obvious root resorption. | 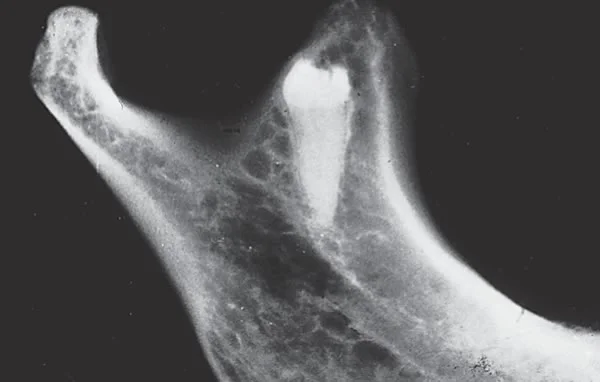 Image 4: If all the molars are missing, a distally-oriented 2nd premolar can move into the mandibular ramus and erupt upward along the mandibular canal. Image 4: If all the molars are missing, a distally-oriented 2nd premolar can move into the mandibular ramus and erupt upward along the mandibular canal. |
Eruptive Mechanism
We’ve seen that resorption to allow movement through the bone controls the amount of eruption. What is the mechanism that moves the erupting tooth after its path has been cleared? Although many experiments have been done to determine it, it’s easier to say what the mechanism isn’t than to be sure what it is.
An obvious thought would be that there’s cellular activity where the root is forming, and that this formation of new tissue generates a force to move the tooth. That isn’t the case. In experimental animals and in rare human cases where this occurred by accident, after the tooth root is sectioned above the apex, the crown and what’s left of the root keeps right on erupting. In this see that the maxillary second premolar has emerged and moved toward the occlusal plane with less than the normal amount of root formation. We will come back to exactly why that happened, but it makes the point that the amount of root isn’t a key factor in pre- or post-emergent eruption.

Eruption Mechanism Theories
If the root apex is not needed for eruption, it seems clear that somehow the force to cause eruptive movements must be generated within the periodontal ligament. Three theories have been offered:
- Contraction by myofibroblasts in the periodontal ligament. Fibroblasts do have some contractile ability, which they exhibit primarily during scar maturation. Whether there are enough of these to move a tooth toward the mouth, and especially whether there are enough oriented in the right direction, seems doubtful.
- Fluid pressure from blood flow within the PDL. It has been suggested for a long time that some pattern of arterio-venous shunts could produce fluid pressure that would lead to pre-emergent tooth eruption. The problem is that it has been very difficult to locate such shunts or discover exactly how they would work. There is evidence that soon after a human tooth emerges from the gingiva, changes in PDL blood flow produce changes in eruption rates—we’ll discuss it later in this module. It seems at present that the blood flow theory is likely to be correct, even if the exact mechanism has not yet been worked out.
- Shortening of collagen fibers as they mature. There is no doubt that this happens, and as we will see in the next section of this module, the collagen mechanism is important in post-emergent eruption. But prior to emergence of the tooth, the collagen fibers are so randomly arranged that they couldn’t be the source of pre-emergent movements (images 1,2). For shortening of collagen fibers to be effective in producing eruptive movements, they have to be arranged as they are after a tooth comes into the mouth, hooked to the bone above the point where they connect to the tooth (images 3,4). This mechanism, therefore, can’t be the source of force to move a tooth along a path that has been cleared in the bone.
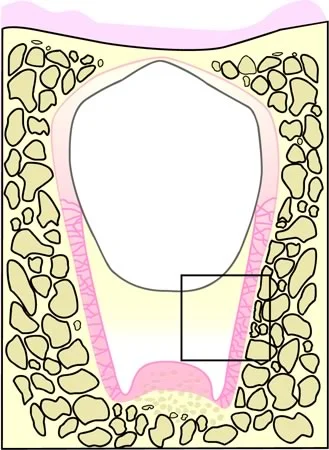 Image 1: Collagen fibers oriented in parallel as they are after a tooth erupts, attached to the bone above where they are attached to the tooth, so that their shortening would lead to tooth eruption. Image 1: Collagen fibers oriented in parallel as they are after a tooth erupts, attached to the bone above where they are attached to the tooth, so that their shortening would lead to tooth eruption. | 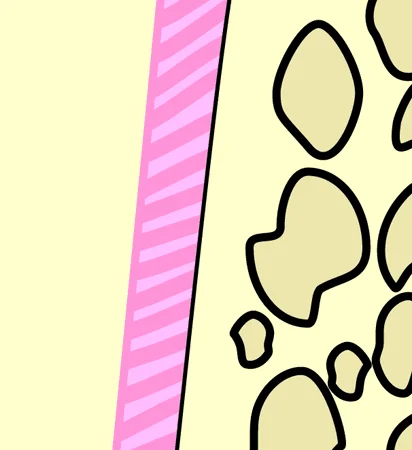 Image 2: Close-up, collagen fibers in parallel orientation. Image 2: Close-up, collagen fibers in parallel orientation. |
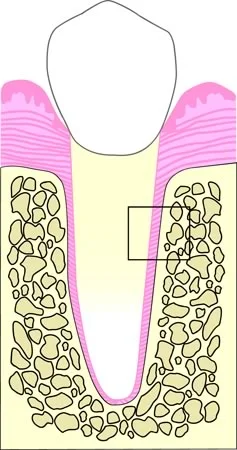 Image 3: Collagen fibers oriented randomly, as they are before a tooth comes into the mouth. Shortening of the fibers would not produce eruption. Image 3: Collagen fibers oriented randomly, as they are before a tooth comes into the mouth. Shortening of the fibers would not produce eruption. | 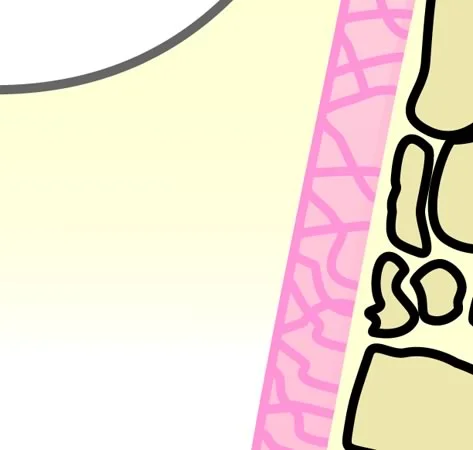 Image 4: Close-up, randomly oriented collagen fibers. Image 4: Close-up, randomly oriented collagen fibers. |
Pre-Emergent Eruptive Movements: Summary
The bottom line on normal pre-emergent eruption:
- resorption produced by osteoclasts over the crown of a tooth clears an eruptive path that the tooth follows
- an eruption mechanism that we still don’t fully understand, probably based on differential blood flow in the periodontal ligament, pushes the tooth along that path at a rate determined by the resorptive activity
- accelerated emergence of a succedaneous tooth occurs when inflammatory resorption exposes the crown, which is further evidence that clearance of the eruption path is the controlling element in pre-emergent eruption.
Post-Emergent Eruption
Effect of Early Loss of Primary Tooth: Premature Eruption
After a tooth breaks through the bony surface, it still has to penetrate the gingiva. Osteoclastic activity has to transform to fibroclastic activity to produce this, but once a tooth is free of the bone, it emerges relatively quickly.
What would be the effect of early loss of a primary tooth on the eruption of its permanent successor? Would this speed up eruption of the permanent tooth, or perhaps delay it? The answer is interesting and clinically important: “It depends …” What it depends on is the extent to which early loss of the primary tooth led to removal of bone over the permanent tooth.
If the primary tooth is lost at a point when the permanent tooth is nearly through the bone, and inflammatory resorption or some other pathologic process removes the rest of the bone over the crown, the permanent tooth erupts more quickly. The most likely cause would be a periapical abscess of the primary tooth. Sometimes an abscess destroys bone above a permanent tooth well before the tooth has enough root formation to be ready to erupt. When this happens, as you see in this patient who lost a mandibular primary 2nd molar to an abscess, the permanent tooth erupts quite rapidly, and may end up in the mouth with barely enough root to support it.

Effect of Early Loss of Primary Tooth: Delayed Eruption
On the other hand, if a primary tooth is lost quite early and a considerable amount of bone remains over its permanent successor (which would be the case, for instance, when a 3-year-old knocks out a primary tooth), eruption of the permanent tooth often is delayed. This occurs because after the primary tooth is gone, bone that remains over the permanent tooth becomes less vascular and thereby more resistant to resorption—and if the rate at which the eruption path is cleared decreases, of course the tooth will take longer to emerge.
It would be nice if the permanent centrals erupted faster after the maxillary primary centrals were lost quite early to trauma, but it usually doesn’t work that way. Rather than appearing to be a toothless wonder from age 3 (image 1) to age 6 or 7 when the permanent centrals were expected), the child is more likely to look like that until age 8 or 9. Knowing that the permanent teeth were likely to be delayed and he’d probably have no central incisors for 5 years, this boy’s parents opted to have the missing teeth replaced prosthetically. In fact, the permanent centrals were delayed for about a year, and finally erupted at age 8.
The same thing can happen when the dentist needs to remove primary canines or primary molars early to encourage the permanent canines or premolars to erupt more quickly. The timing of extraction becomes important. If it’s done too soon, it may delay the permanent tooth instead of speeding it up.

Mechanism of Post-Emergent Eruption
Once a tooth comes into occlusal function, it’s exposed to the heavy forces that go with chewing and other forces that oppose eruption. At that point, as you have already seen, the periodontal ligament does organize itself so that the collagen fibers attach to the bone above the point where they attach to the root of the tooth. Then shortening of collagen fibers as the collagen matures and shrinks would move the tooth occlusally.
It was noted by sheep herders many years ago that if the animals ate a certain weedy plant, their teeth would become loose and might fall out. The problem turned out to be a plant constituent that inhibited cross-linking and maturation of collagen. Chemicals of this type are called lathyrogens.
That led to animal experiments on the effect of lathyrogens on tooth eruption. Sure enough, teeth that are already in the mouth stop erupting when lathyrogens are given. From this experimental evidence, it seems clear that shortening of collagen fibers is the mechanism of post-emergent eruption.
It’s important to keep in mind that collagen fibers in the periodontal ligament resorb and are replaced rather quickly. New ones are always forming, attaching and then shortening as they mature. So an eruption mechanism based on this would be active constantly.
Animal Experiments
It seems obvious that after a tooth emerges, forces against the tooth that oppose eruption must be a major part (if not all) of the mechanism that controls eruption. But exactly how does this work?
Experiments to determine the control of post-emergent eruption are difficult because an erupting tooth moves so slowly that extremely precise measurements are necessary to observe its movements. Three new measurement techniques were developed in the late 1980s and 1990s that could be used in tooth eruption experiments. The first two had a precision of 1-2 microns, the third could resolve a fraction of a micron (a micron is .001 millimeter).
The first technique used a variable capacitance displacement transducer (VCDT). If two plates are separated by a small distance, as they are in a capacitor, even a very small change in their separation produces a measurable change in capacitance. This allowed studies at UNC of eruption in rabbits, which were chosen because like all rodents, they have continuously erupting incisors that move much more rapidly than human teeth, and can be used in terminal experiments. The goal was to evaluate how much force was needed to affect eruption, and how long that force had to be maintained.
The instrumentation for the rabbit studies is shown in image 1. The rabbit has to lie very still—which means paralysis with curare. Then a respirator is needed, and body temperature must be controlled. The measuring device has one plate attached to the jaw, and another mounted on the tooth (image 2).
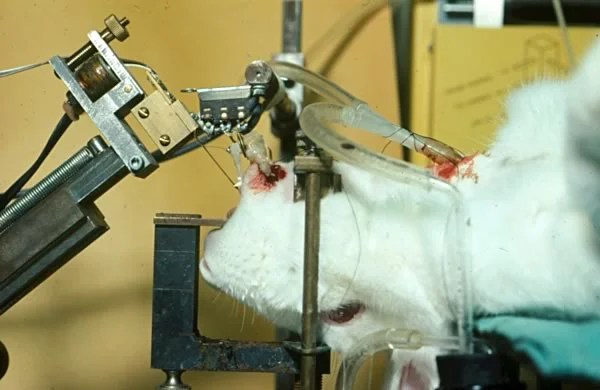 Image 1: Overview of instrumentation for rabbit eruption experiments. Image 1: Overview of instrumentation for rabbit eruption experiments. | 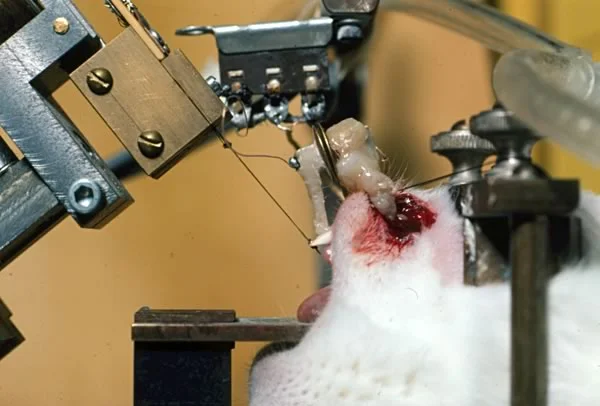 Image 2: One plate of the VCDT is mounted to the jaw, the other to the incisor. Image 2: One plate of the VCDT is mounted to the jaw, the other to the incisor. |
Animal Experiments: Force to Resist Eruption
In this close-up view, you can see that the two plates forming the VCDT that almost touch. A change in their position as small as 1-2 microns will cause a change in capacitance.
You also can see a thin flat steel beam that contacts the incisal edge of the erupting tooth. For these experiments, the beam was mounted so that it could be moved into or out of contact with the tooth. A strain gauge on the beam allowed measurement of the amount of force it placed against the tooth.
This allowed measurement of the force of eruption, by letting the tooth erupt into contact with the beam and observing how much force it took to stop the tooth. That turned out to be a very light force, only a gram or less. The same thing has been observed in other animal experiments—it takes only a very small amount of force to stop an erupting tooth if the force is continuous, as it would be if the beam were left in position.
In the mouth, a tooth would almost never receive continuous force. What would happen if the force opposing eruption were intermittent?
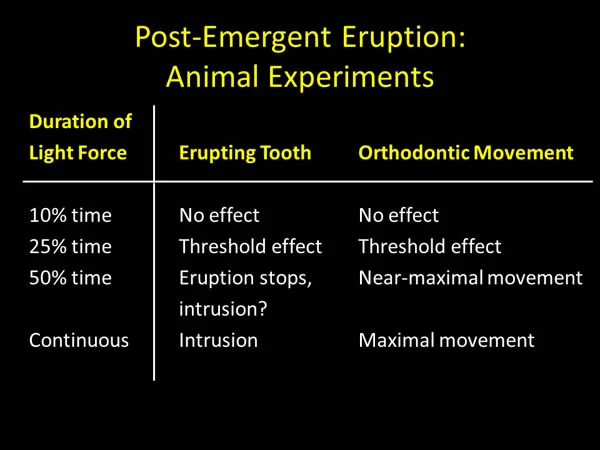
Animal Experiments: Duration of Force to Resist Eruption
These graphs show the effect of intermittent force, with a load of 1-2 grams against the erupting rabbit incisor. This force is more than enough to stop eruption with continuous application. The beam was brought into contact with the erupting tooth in an on-off fashion, with 3 cycles:
- on for 1 second, then off for 9 seconds (10% time)
- on for 1 second, then off for 3 seconds (25% time)
- on for 1 second, off for 1 second (50% time)
After an hour of intermittent force application, the tooth was allowed to erupt without applied force, then another hour of force application followed, and then a final recovery hour. There were at least three animals in each group.
Note that with 10% force application, there was little or no effect on the rate of eruption (image 1). The tooth continued to erupt at about the same rate when it was being loaded as when it was not. With 25% time, there was a marginal effect (image 2). Note that for all 3 animals, eruption stopped during one but not both of the hours that the tooth was loaded. With 50% time, eruption was stopped and intrusion began to occur (image 3). The tooth continued to erupt after the force was removed.
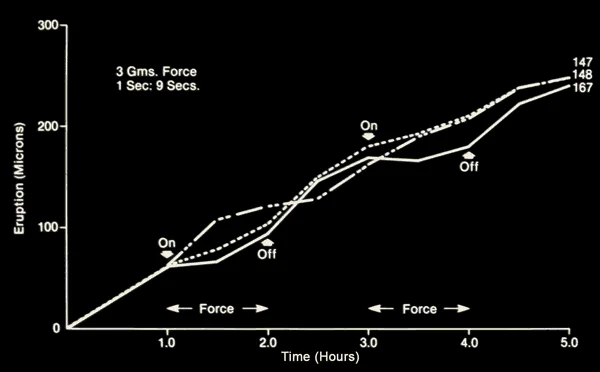 Image 1: Effect on eruption of 10% time force application (minimal effect) Image 1: Effect on eruption of 10% time force application (minimal effect) | 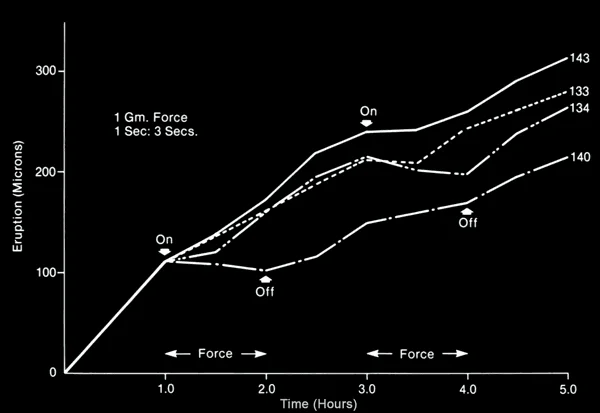 Image 2: Effect on eruption of 25% time force application (marginal effect) Image 2: Effect on eruption of 25% time force application (marginal effect) |
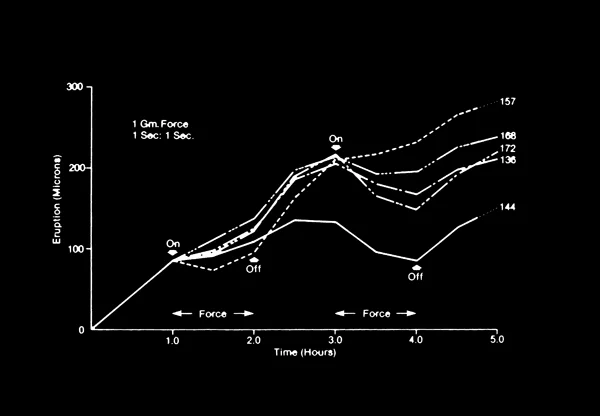 Image 3: Effect on eruption of 50% time force application (nearly total effect) Image 3: Effect on eruption of 50% time force application (nearly total effect) |
Animal Experiments: Eruptive Force and Orthodontic Tooth Movment
These results showed that in the rabbit model, if a force large enough to stop eruption is applied for 50% of the time, the effect is very similar to that of continuous force. The same force 10% of the time has little or no effect. Applying the force 25% of the time seems to be about the threshold for an effect on eruption.
This is remarkably similar to what has been learned about the amount and duration of force to move a tooth orthodontically. For orthodontic tooth movement, the amount of force can be quite small if it is maintained continuously. And if a removable appliance is used, unless it is worn for at least 4-8 hours/day (about 25% time), the teeth don’t respond. A removable appliance that is worn regularly for 12 hours/day (50% time) is reasonably effective in moving teeth, although full time is at least somewhat better.
The bottom line: it looks as if heavy intermittent force opposing eruption, as from chewing, would not have enough duration to effectively control eruption. But light pressures from soft tissue contacts with the teeth, as from tongue or lip-cheek position during sleep, would have the right characteristics.
Human Experiments
Rodent incisors are rather different from human teeth. Similar experiments in humans would be possible only if non-invasive instrumentation could be used, so VCDT measurements would not be possible.
Robert Paterson, a senior engineer at IBM / Lexmark and long-time collaborator with dental research, suggested in the 1990s that a video microscope system might make it possible to follow the eruptive movements of a human second premolar in its post-emergent spurt (image 1). At this stage, the premolar erupts at an average rate of about 4 microns/hour. If an optical ruling was bonded to the premolar and viewed through a reference ruling bonded to a bar between the first premolar and first molar (image 2), it should be possible to observe 1-2 micron changes in position.
The major problem would be to get the two rulings in focus when a child with an erupting premolar was positioned for video microscope imaging. In image 3, the child’s cheek is retracted and the video microscope is being focused on the rulings. The video output is seen on the screen in front of the patient. By recording the video output and then capturing the a video frame that did have the rulings in focus, the needed measurements were possible.
 Image 1: Second premolar in post-emergent spurt stage. Image 1: Second premolar in post-emergent spurt stage. | 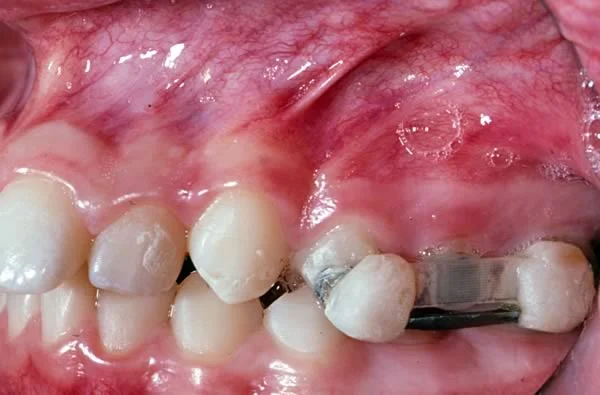 Image 2: Reference and moving rulings bonded in place for measurement of amount of eruption between observations. Image 2: Reference and moving rulings bonded in place for measurement of amount of eruption between observations. |
 Image 3: Position of rulings being observed with a video microscope. Image 3: Position of rulings being observed with a video microscope. |
Video Microscope Studies
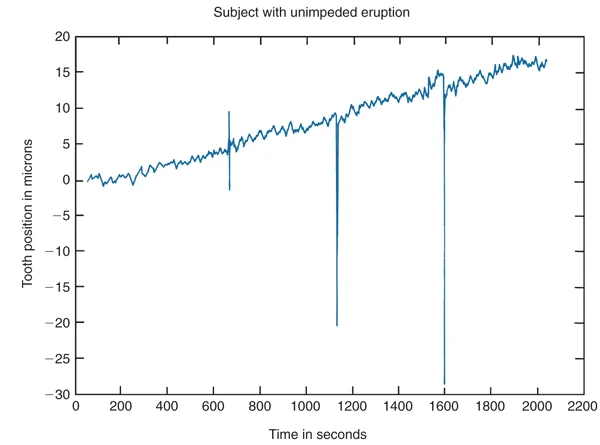
The video microscope studies, with observations repeated each hour, produced an unexpected finding: during the post-emergent spurt, teeth only erupt in the evening, not during the day! Instead of erupting steadily at about 4 microns/hour (the average rate), they don’t erupt—and may and even intrude—during the day, then erupt surprisingly rapidly during the evening, at rates of 20 microns/hour or more.
The instrumentation was changed to allow a continuous view of eruption, using a flexible fiber optic cable to transmit an image of the rulings to the video microscope (image 1). Then children could spend the night on a cot in the laboratory, and eruption could be observed while they slept.
This showed that eruption started in the early evening and stopped around midnight (image 2). The tooth was likely to intrude somewhat after that until the next phase of eruption began in the early evening the next day.
| Image 1: Child during continuous video microscope observation, using a fiber optic cable to carry a focused image to the video microscope. | 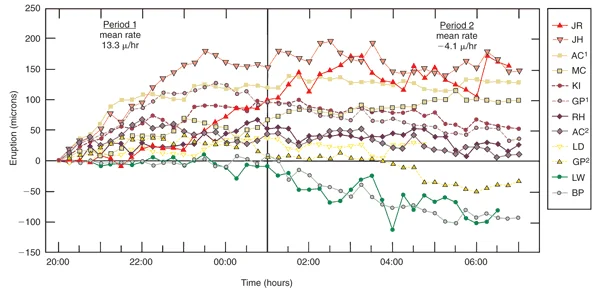 Image 2: Plots of premolar eruption for individual children. Note the consistent pattern of eruption in the evening, then no eruption or intrusion after midnight. Image 2: Plots of premolar eruption for individual children. Note the consistent pattern of eruption in the evening, then no eruption or intrusion after midnight. |
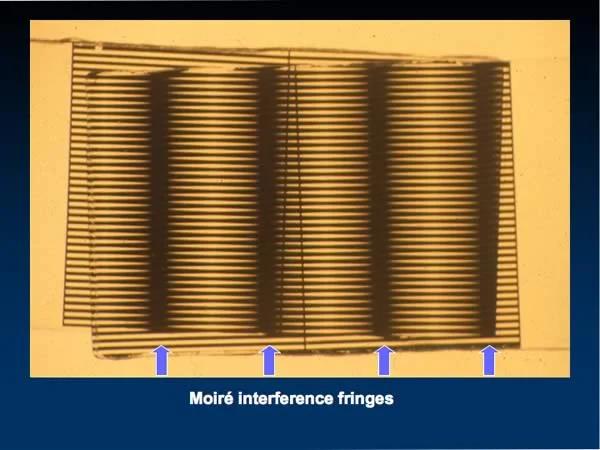
Very High Resolution: Moiré Magnification
If experiments to see the effect of manipulating eruption were to be done with humans, resolution of a fraction of a micron in changes in position of optical rulings attached to the teeth of would be required. An optical phenomenon called Moiré magnification (image 1) would be a step in this direction, but the rulings would have to be oriented very precisely, to something like a thousandth of a degree, and the orientation must be maintained as movement occurs.
Paterson and his colleagues at IBM realized that if a mirror was placed behind a ruling shaped like a sergeant’s chevrons, its inverted reflection back onto the ruling could be used to create the interference fringes. The orientation of the actual and virtual rulings then would be determined by how accurately the lines were drawn when the ruling was produced, not on how two rulings were oriented in the mouth.
The theoretical resolution of the Moiré device was 0.02 micron. Its actual resolution was about 0.04 micron, definitely better than 0.1 micron. A device of this type could be miniaturized and used intra-orally (image 2). With continuous observation at this degree of accuracy, experiments with erupting human teeth became possible.
Moiré Magnification: Effect of Applied Force
Using the Moiré magnification device, a series of experiments with children with an erupting second premolar were carried out to evaluate the amount of force necessary to stop eruption and to judge the effect of intermittent force.
The results were very similar to those in the animal experiments: a light force maintained continuously against the tooth stopped its eruption and was likely to lead to intrusion. Intermittent force against the erupting tooth deflected it, but as you can see in this plot, eruption usually continued at the same rate.
It appears, therefore, that for control of eruption, as for orthodontic tooth movement, the duration of the force is much more important than its magnitude. Teeth are very well adapted to withstand quite heavy force of short duration during mastication. Heavy intermittent force from chewing does not affect the periodontal ligament because it is cushioned by fluid that fills the space between the tooth root and the bony walls of the socket.
Moiré Magnification: Effect of Decreasing Blood Flow
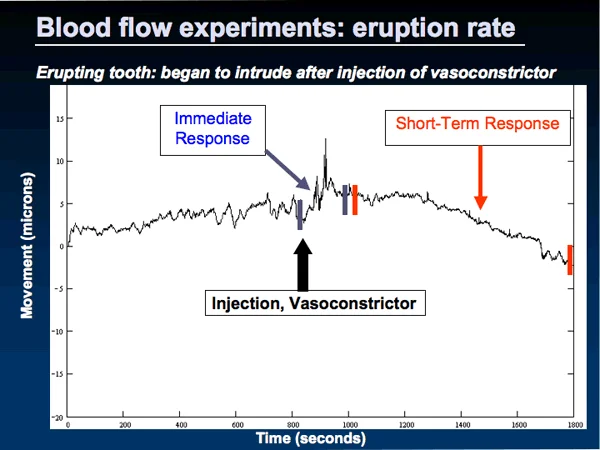
As we have discussed, blood flow in the periodontal ligament seems to be the major component of the mechanism of eruption prior to the time that a tooth erupts and the PDL becomes organized to support it. Would blood flow affect the eruption of a human premolar during the pre-occlusal spurt?
A series of experiments using Moiré magnification indicate that it would. Dental anesthetics often contain epinephrine to constrict blood vessels so the anesthetic agent is retained longer, which is particularly needed because most local anesthetics dilate vessels and increase blood flow.
As this image from a typical experiment with a child shows, injecting a local anesthetic with epinephrine over the apex of an erupting premolar stops eruption and may lead to intrusion of the tooth.
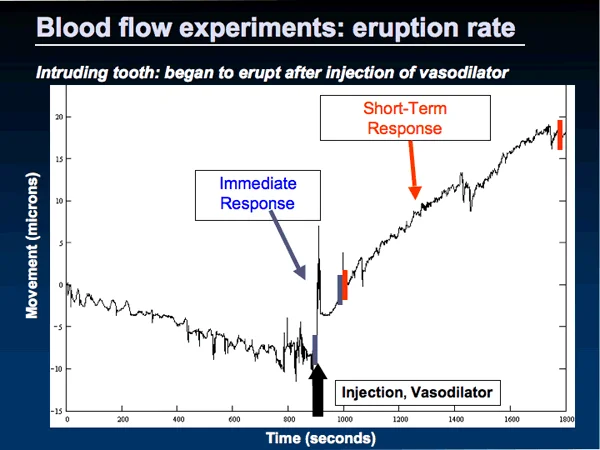
Moiré Magnification: Effect of Increasing Blood Flow
In contrast, as this chart from another experiment shows, increasing blood flow causes eruption. Note that prior to the injection of a local anesthetic without epinephrine (a vasodilator), this premolar was intruding; it began to erupt after the injection.
What Causes the Daily Rhythm in Eruption?
An increase in blood flow in the PDL appears to be the way that tooth eruption during the evening is created—but what leads to this cycle of increased blood flow?
It is interesting that skeletal growth and tooth eruption follow the same pattern. A child is taller at midnight than at 6 PM, doesn’t grow any more for the rest of the night, actually loses a little height (but not all of the previous evening’s height gain) during the next day, then grows again the next evening. Tooth eruption mimics this pattern of growth.
The growth in height, and probably also tooth eruption, is influenced by the cycle of release of growth hormone. A child has an increase in growth hormone levels beginning in the early evening that lasts until about midnight. That’s when he or she grows, and when a tooth erupts.
Preliminary experiments with growth hormone-deficient children (who have delayed eruption of their teeth) suggest that an increase in the rate of eruption is one of the effects of injecting growth hormone. So it seems reasonable that the cause of the tooth eruption cycle is the same as the cause of the growth cycle: PDL blood flow probably changes because of growth hormone effects.
The Bottom Line
It’s important to keep in mind that both the mechanism and control of pre- and post-emergent eruption are different.
For pre-emergent eruption:
- mechanism is pressure generated by differential blood flow in the PDL (exactly how remains unknown)
- control is by the rate of resorption over the crown of the erupting tooth
For post-emergent eruption:
- mechanism (after a tooth comes into function) is collagen fiber maturation and shortening. It appears still to be the blood flow mechanism during the pre-occlusal spurt.
- control is by force opposing eruption, but the force that counts is light force that’s prolonged for hours, not heavy intermittent force from chewing
Diagnosis and Treatment of Eruption Problems
Impacted Teeth: Third Molars
An impacted tooth, by definition, is one that has failed to emerge into the oral cavity. This can happen with any tooth from a variety of causes, but the usual cause is a displaced path of eruption because of lack of space in the dental arch. The most frequently impacted teeth are 3rd molars, especially mandibular 3rd molars, and maxillary canines.
In modern humans, it is unusual for the jaw to grow long enough to accommodate the 3rd molars. Remember that space for all the molars is created by resorption along the front of the mandibular ramus and addition of new bone at the maxillary tuberosity. If there isn’t enough room for it, the third molar may break through the bone but still be covered by soft tissue distal to the second molar, even if it’s upright (image 1). In this situation oral pathogens have access to the 3rd molars via a communication behind the 2nd molars.
Upper third molars are less likely to become impacted, in part because they are more likely to be small, and often erupt when lower third molars have problems (image 2). Even if lower third molars become horizontally impacted (image 3), there’s still likely to be a communication between the oral cavity and the area around the crown of the tooth. Because the oral flora have access to a 3rd molar that has penetrated through the bone, this type of impaction is more likely to be a clinical problem than a bony impaction.
Can third molars like these push the rest of the lower teeth forward and cause incisor crowding? That’s an important developmental question that we’ll come back to at the end of this module.
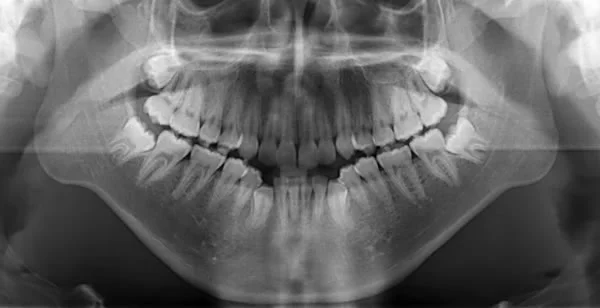 Image 1: Mandibular 3rd molars that broke through the bone over them but still were unable to erupt. Image 1: Mandibular 3rd molars that broke through the bone over them but still were unable to erupt. |  Image 2: Both lower 3rd molars impacted, one maxillary 3rd molar erupted (the other one was congenitally missing). Image 2: Both lower 3rd molars impacted, one maxillary 3rd molar erupted (the other one was congenitally missing). |
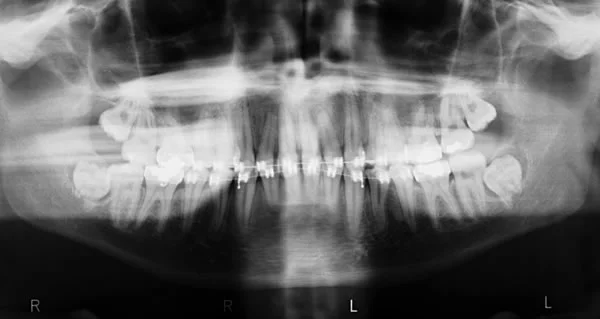 Image 3: Mandibular 3rd molars, horizontal impaction; maxillary 3rd molars tipped distally with no room for eruption. Image 3: Mandibular 3rd molars, horizontal impaction; maxillary 3rd molars tipped distally with no room for eruption. |
Impacted Maxillary Canines
In a previous module, we have already noted that maxillary canines sometimes miss connecting with the root of the primary canine, and can become impacted if this happens.
Like any other tooth, the maxillary canines follow the path that has been cleared for them. It is interesting, and clinically significant, that if the primary canine is extracted when the path of the permanent canine is being deflected away from the primary root, the permanent tooth often changes its direction toward erupting in the right place.
This is an excellent example of a clinical intervention based on what we know about the control of pre-emergent eruption. If you clear the path for a tooth to erupt, it tends to follow the path. For this patient, one permanent canine was in poor position, mesial to the root of the primary canine (image 1). After extraction of the primary canine (image 2), the permanent canine erupted downward through the extraction site into its proper position.
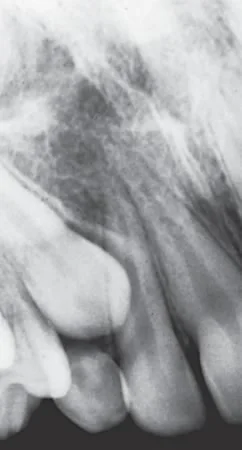 Image 1: Unerupted maxillary canine that is mesial to the root of the primary canine. From this position impaction and damage to the lateral incisor roots is quite likely. Image 1: Unerupted maxillary canine that is mesial to the root of the primary canine. From this position impaction and damage to the lateral incisor roots is quite likely. | 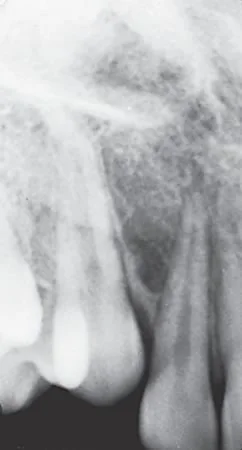 Image 2: Same patient 12 months after the primary canine was extracted. The permanent canine has changed its eruption path and is erupting into its correct position. Image 2: Same patient 12 months after the primary canine was extracted. The permanent canine has changed its eruption path and is erupting into its correct position. |
Cleidocranial Dysplasia
An unusual syndrome, cleidocranial dysplasia, is characterized by two things that would seem to have nothing in common: absence of clavicles (collar bones) and multiple unerupted permanent teeth. In a child with this condition, the primary teeth erupt normally, and so do the permanent molars. You remember, of course, that the permanent molars are derived from the primary dental lamina, and developmentally can be considered primary teeth that last indefinitely—so if the primary teeth can erupt, it makes sense that the permanent molars also would erupt.
As this image shows, the succedaneous teeth do not erupt, and the reason is obstruction of their eruption path. Three things work together to make it almost impossible for these teeth to make it into the oral cavity: multiple supernumerary teeth usually are present, the alveolar bone is resistant to resorption, and if a tooth does get past the first two obstacles, the heavy and fibrous gingiva still impedes eruption.
Cleidocranial Dysplasia: Treatment
If the problem is mechanical obstruction, clearing the eruption path should lead to eruption of the impeded teeth, and it should be possible to move teeth orthodontically if they didn’t erupt on their own.
For this patient, supernumerary teeth and bone over the unerupted incisors were removed at age 10, and by age 11 the permanent incisors had erupted a considerable distance (image 1). At that point orthodontic attachments were placed on the incisors to bring them into normal position (image 2).
In addition to the eruption problem there was severe crowding in both arches. Note the position of the mandibular canines in image 2. These teeth were removed along with additional supernumerary teeth in the canine-premolar area, and later the maxillary first premolars were removed so there would be room to bring the maxillary canines and 2nd premolars into the arch.
Eventually, the remaining succedaneous teeth were brought into the dental arch except the maxillary right 2nd premolar (image 3), which was extracted after it proved impossible to move, probably because an area of its periodontal ligament was damaged during the surgery to remove other teeth and this led to ankylosis (fusion of cementum to bone).
The concept is important: if a tooth doesn’t erupt because it’s mechanically obstructed, it may do so when the obstruction is removed and can be moved orthodontically if necessary.
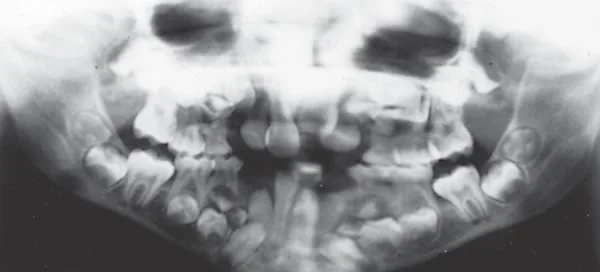 Image 1: Cleidocranial dysplasia, age 11, after surgical exposure of incisors. Image 1: Cleidocranial dysplasia, age 11, after surgical exposure of incisors. | 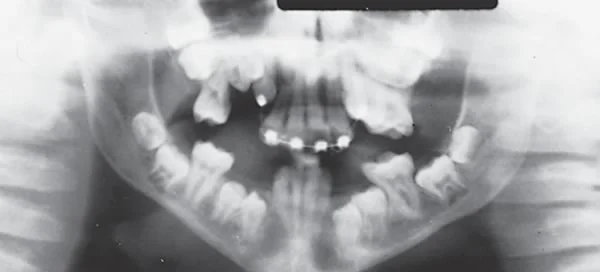 Image 2: Cleidocranial dysplasia, age 12, after alignment of incisors and removal of obstructions in the canine-premolar area. Image 2: Cleidocranial dysplasia, age 12, after alignment of incisors and removal of obstructions in the canine-premolar area. |
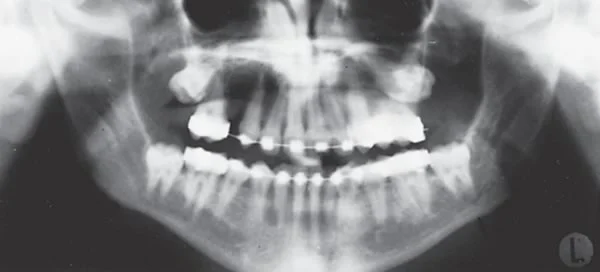 Image 3: Cleidocranial dysplasia, age 16, near end of orthodontic treatment. Image 3: Cleidocranial dysplasia, age 16, near end of orthodontic treatment. |
Primary Molar Ankylosis / Obstructed Permanent Successor
Although most ankylosed primary teeth eventually are exfoliated and the underlying permanent tooth then can erupt, an ankylosed primary tooth can be a formidable mechanical obstruction. If a primary molar becomes ankylosed at an early age, it can disappear as other teeth erupt past it and gingiva covers it over. Then the crown of the primary tooth is retained even if the root resorbs, and resorption of enamel is very slow if it happens at all (image 1). For this patient, note that the roots of the obstructed 2nd premolars have continued to develop. The root of the premolar in the lower right has stopped at the border of the mandible.
The maxillary second premolars and the ankylosed primary molars were extracted, and space was opened between the 1st molar and 1st premolar in the lower left. The 2nd premolar erupted on its own and brought alveolar bone with it (image 2). With the premolar moved orthodontically the rest of the way to its normal position (image 3), alveolar bone height in the premolar area also was normal. Note that the root of the premolar has remained incomplete. A tooth with an incomplete root can still have eruptive potential.
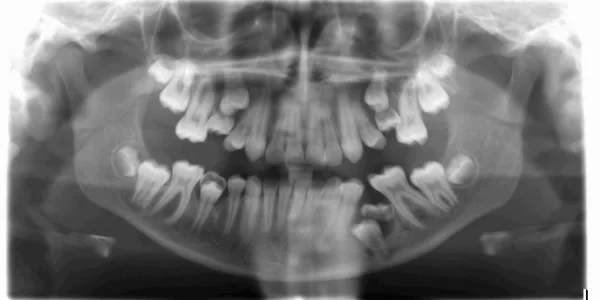 Image 1, Ankylosed primary molars: Primary second molars in all four quadrants were ankylosed and prevented normal eruption of the underlying premolars. Image 1, Ankylosed primary molars: Primary second molars in all four quadrants were ankylosed and prevented normal eruption of the underlying premolars. |  Image 2, Ankylosed primary molars: All four ankylosed primary molars as well as the maxillary second premolars were extracted, and the lower premolars erupted. Image 2, Ankylosed primary molars: All four ankylosed primary molars as well as the maxillary second premolars were extracted, and the lower premolars erupted. |
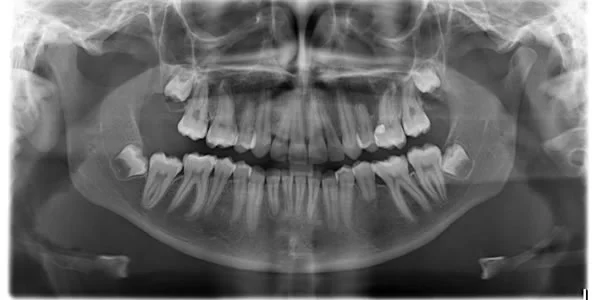 Image 3, Ankylosed primary molars: Despite its short root, the lower left premolar erupted into occlusion. Image 3, Ankylosed primary molars: Despite its short root, the lower left premolar erupted into occlusion. |
Molar Ankylosis vs Primary Failure of Eruption
The usual cause of a posterior open bite is failure of premolars or permanent molars to erupt normally. There are two possibilities when this occurs: isolated ankylosis of one or more first molars (image 1), or primary failure of eruption affecting multiple posterior teeth (images 2 and 3).
Ankylosis can be thought of as the ultimate form of mechanical obstruction—once a tooth fuses to bone, it can’t erupt and can’t be moved unless the ankylosis can be released, which is impossible except for brief periods and then only if the area of ankylosis is small. Primary failure of eruption (PFE) carries that name because the teeth do not erupt even though they are not ankylosed—which indicates a failure of the eruption mechanism.
In both conditions, the problem is first noted when some or all the first permanent molars stop erupting, and in both conditions the prognosis for the affected molar is very poor. If it’s ankylosed but the area of ankylosis is small, sometimes it is possible to gently luxate the tooth to break the ankylosis, and then move it orthodontically—but eventually it becomes ankylosed again.
In PFE the periodontal ligament is abnormal, and the affected teeth do not respond to orthodontic force. They can’t be moved even though they aren’t ankylosed. About the only effect of trying to move these teeth is that they do become ankylosed.
 Image 1: This mandibular first molar became ankylosed soon after it erupted, after an occlusal restoration had been placed. Note the amount that it submerged as the 2nd molar and premolars grew past it. Image 1: This mandibular first molar became ankylosed soon after it erupted, after an occlusal restoration had been placed. Note the amount that it submerged as the 2nd molar and premolars grew past it. |  Image 2: Cephalometric radiograph showing posterior open bite. With so many teeth affected, primary failure of eruption is the likely diagnosis. Image 2: Cephalometric radiograph showing posterior open bite. With so many teeth affected, primary failure of eruption is the likely diagnosis. |
 Image 3: Panoramic radiograph, primary failure of eruption affecting molars in all four quadrants.. Image 3: Panoramic radiograph, primary failure of eruption affecting molars in all four quadrants.. |
Primary Failure of Eruption
The distinction between ankylosis of first permanent molars and primary failure of eruption is important, because it establishes the prognosis for the second molars. In isolated ankylosis of first molars, the second and third molars are likely to respond perfectly normally to orthodontic force—so the second molar can be moved into a first molar extraction site, creating room for the third molar to erupt.
In contrast, in PFE all teeth distal to the most mesial affected tooth are affected (images 1-3). First premolars sometimes are affected but usually are not; 2nd premolars may or may not be affected, as in this patient. Usually the 1st molar is affected but it may be just the 2nd and 3rd molars.
Because the periodontal ligament is abnormal and does not respond to orthodontic force, an attempt to move any of these teeth is guaranteed to fail. You’ll learn more about managing eruption problems later—but at this point you need to understand the significance of failure of a tooth to follow along as its eruption path is cleared. It is difficult to have to say to parents that nothing can be done to bring the affected teeth into the mouth—but at least ineffective treatment can be avoided if the correct diagnosis is made.
 Image 1: Primary failure of eruption affecting both maxillary posterior quadrants, with the left side more affected than the right. Note the cleared eruption path for the maxillary right 2nd premolar. Image 1: Primary failure of eruption affecting both maxillary posterior quadrants, with the left side more affected than the right. Note the cleared eruption path for the maxillary right 2nd premolar. |  Image 2: Primary failure of eruption affecting all 4 quadrants. Image 2: Primary failure of eruption affecting all 4 quadrants. |
 Image 3: Intra-oral photos of the patient in image 2. Image 3: Intra-oral photos of the patient in image 2. |  Image 4: For this patient, an attempt to bring an unerupted 1st molar down into position resulted instead in intrusion of the teeth mesial to it. Image 4: For this patient, an attempt to bring an unerupted 1st molar down into position resulted instead in intrusion of the teeth mesial to it. |
Primary Failure of Eruption: Diagnosis
If a permanent first molar doesn’t erupt, it can be difficult to tell at age 7-8 whether it’s ankylosed or whether it is affected by PFE (image 1). If the second molar erupts normally, it’s an isolated ankylosis of the first molar. If the second molar also doesn’t erupt although its eruption path has been cleared, it’s primary failure, and the second premolar may be affected as well. This means that a definite diagnosis of ankylosis or primary failure cannot be made until it is obvious that the second molar is erupting normally (image 2) or is failing to erupt and also is affected.
When posterior teeth are not erupting normally, caution in proceeding with orthodontic treatment is advised until a definite diagnosis can be made, but early extraction of an abnormal permanent first molar often is better than waiting. For the patient in image 2, the first molar should have been extracted long before this image was taken. If it’s PFE, the early extraction does no harm. If it’s just an ankylosed first molar, the normal second molar can begin drifting mesially as it erupts, and then it brings alveolar bone with it.
You’ll learn more about managing eruption problems later—but at this point you need to understand the significance of failure of a tooth to follow along as its eruption path is cleared.
 Image 1: An 8-year-old with ankylosed primary molars and failure of the maxillary right 1st molar to erupt. This might be PFE, but the 2nd molars are symmetric bilaterally, and a definitive diagnosis cannot be made yet. Image 1: An 8-year-old with ankylosed primary molars and failure of the maxillary right 1st molar to erupt. This might be PFE, but the 2nd molars are symmetric bilaterally, and a definitive diagnosis cannot be made yet. |  Image 2: Obvious ankylosis of a maxillary 1st molar. The 2nd molar and 2nd premolar have erupted past it and the 2nd molar moved mesially over it. Image 2: Obvious ankylosis of a maxillary 1st molar. The 2nd molar and 2nd premolar have erupted past it and the 2nd molar moved mesially over it. |
Hereditary Pattern of PFE
Primary failure of eruption runs in families and is the result, at least in part, of a specific genetic mutation that has been identified.
The PTH1R gene encondes information for a parathyroid hormone receptor protein. A novel mutation in this gene is associated with individuals who have PFE. Studies indicate that it is inherited in an autosomal dominant fashion.
These radiographs of mother (images 1 and 2) and daughter (images 3, 4, 5) show all quadrants affected in both. Sometimes PFE is present in one or two quadrants of the dental arch, while the other quadrants have only an ankylosed first molar, so there is some overlap between isolated ankylosis and PFE.
Eruption disorders like PFE have a complicated etiology, but it is likely that the specific causes will be worked out before too long as genetic studies of these individuals continue.
 Image 1: Mother, all 4 quadrants affected, after extraction of most of the affected teeth. Image 1: Mother, all 4 quadrants affected, after extraction of most of the affected teeth. |  Image 2: Mother, all 4 quadrants affected. Image 2: Mother, all 4 quadrants affected. |
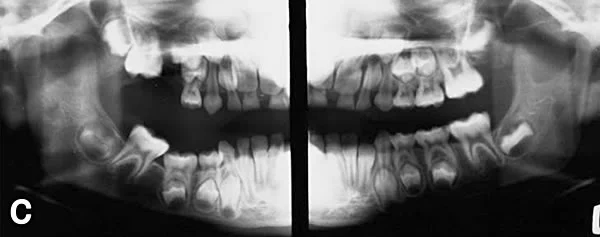 Image 3: Daughter, age 7. Note ankylosed primary teeth and unerupted permanent molars. Image 3: Daughter, age 7. Note ankylosed primary teeth and unerupted permanent molars. |  Image 4: Daughter, age 14. All four quadrants are affected but right side is more severe. Image 4: Daughter, age 14. All four quadrants are affected but right side is more severe. |
 Image 5: Daughter, age 14, bilateral posterior open bite. Image 5: Daughter, age 14, bilateral posterior open bite. |
Summary
Important points to remember:
Pre-emergent eruption
- no eruptive movement until root formation begins
- mechanism: differential blood flow in PDL (?)
- control: resorption over crown
- accelerated if crown is uncovered by loss of primary tooth, delayed if dense bone forms over the crown after very early loss
Post-emergent eruption
- fastest movement during pre-occlusal spurt
- continued slow eruption in concert with vertical jaw growth
- mechanism: blood flow prior to occlusion collagen maturation / shortening afterward
- control: soft tissue pressures, light force, long duration
Clinical application
impaction:
- clearing eruption path often but not always can prevent it
- more likely when teeth are crowded by lack of space
ankylosis:
- created by fusion of an area of cementum to bone
- frequent in primary teeth, rare in permanent teeth
primary failure of eruption:
- abnormal periodontal ligament
- all teeth distal to most mesial affected one are affected
- teeth do not erupt although they are not ankylosed
- teeth do not respond to orthodontic force, cannot be moved
Self-Test Referral
Before you take the self-test, read pages 74-80 in the 5th edition of Contemporary Orthodontics (87-93 in the 4th ed.). Then use the self-test to be sure you have understand the material you have reviewed. It’s important background for treatment of children with eruption problems.
Self-Test
Question 1
Almost all tooth eruption occurs during which stage of tooth development?
- initiation
- histodifferentiation
- morphodifferentiation
- growth ✓
- attrition
Correct
That’s correct. Eruption doesn’t start until the growth stage has been reached. It occurs mostly during the growth stage, but because very slow eruption persists throughout life, a small amount of eruption also occurs during the attrition stage (and occurs to some extent in response to loss of occlusal enamel to attrition).
Incorrect
No, that’s incorrect. Eruption doesn’t start until the growth stage has been reached. It occurs mostly during the growth stage, but because very slow eruption persists throughout life, a small amount of eruption also occurs during the attrition stage (and occurs to some extent in response to loss of occlusal enamel to attrition).
Question 2
How far does a permanent first molar have to erupt after it first comes into occlusion?
- 10 mm or more ✓
- 4-5 mm
- 1-3 mm
- none, eruption ends when the tooth reaches occlusion
Correct
That’s right. Face height normally increases 20 mm or more between age 6, when first molars first come into occlusion, and age 18 when the growth rate declines to the very slow adult level. So both upper and lower first molars each have to erupt 10 mm or more to maintain occlusal contact as the jaws grow. If they didn’t continue to erupt, they would appear to submerge into the gingiva as the other teeth erupted past them—which happens occasionally to a tooth that becomes ankylosed.
Incorrect
No, that’s wrong. Face height normally increases 20 mm or more between age 6, when first molars first come into occlusion, and age 18 when the growth rate declines to the very slow adult level. So both upper and lower first molars each have to erupt 10 mm or more to maintain occlusal contact as the jaws grow. If they didn’t continue to erupt, they would appear to submerge into the gingiva as the other teeth erupted past them—which happens occasionally to a tooth that becomes ankylosed.
Question 3
When a tooth is mechanically blocked from erupting, its root may become distorted in form. What is the descriptive term for such a root?
- macerated
- dilacerated ✓
- encapsulated
- commiserated
- eviscerated
Correct
That’s right. A severely curved tooth root is called dilacerated. This is the result of trauma or a souvenir of mechanically-blocked eruption. Trauma while the root is still forming can displace the apex. When the crown can’t move toward the oral cavity because a path cannot be cleared, root formation continues and the root apex moves away from the mouth. If it hits a bony wall like the wall of the maxillary sinus or the lower border of the mandible, a curve in the root is formed.
Incorrect
No. you’re wrong. A severely curved tooth root is called dilacerated. This is the result of trauma or a souvenir of mechanically-blocked eruption. Trauma while the root is still forming can displace the apex. When the crown can’t move toward the oral cavity because a path cannot be cleared, root formation continues and the root apex moves away from the mouth. If it hits a bony wall like the wall of the maxillary sinus or the lower border of the mandible, a curve in the root is formed.
Question 4
During the post-emergent spurt stage of eruption, when does active eruption occur?
- mostly from early morning to noon
- mostly from noon to late afternoon
- mostly from late afternoon to midnight ✓
- mostly from midnight to early morning
- no influence of time of day
Correct
That’s right. Active eruption occurs mostly in the evening, beginning in late afternoon or early evening and ending around midnight. There is little or no net eruption from early morning until the next evening, and usually the tooth loses some of the ground it gained the previous evening during the next 18 hours—but it starts the next day’s eruption from a higher point, so there’s some net gain each day.
Incorrect
No, that’s wrong. Active eruption occurs mostly in the evening, beginning in late afternoon or early evening and ending around midnight. There is little or no net eruption from early morning until the next evening, and usually the tooth loses some of the ground it gained the previous evening during the next 18 hours—but it starts the next day’s eruption from a higher point, so there’s some net gain each day.
Question 5
How is eruption controlled after a tooth comes into occlusion?
- tongue-lip pressures against the teeth ✓
- biting force
- level of circulating growth hormone
- all the above
- none of the above
Correct
That’s right, the experimental evidence suggests that light force of long duration is the controlling element for post-emergent eruption, and this probably comes from tongue-lip pressures against the teeth while the jaws are separated during sleep. Biting force is heavy force of long duration, so it has the wrong characteristics. The level of growth hormone may play a role indirectly, since it relates to the amount of skeletal growth after a tooth comes into occlusion, but its direct role on blood flow no longer applies.
Incorrect
No, that’s wrong. The experimental evidence suggests that light force of long duration is the controlling element for post-emergent eruption, and this probably comes from tongue-lip pressures against the teeth while the jaws are separated during sleep. Biting force is heavy force of short duration, so it has the wrong characteristics. The level of growth hormone may play a role indirectly, since it relates to the amount of skeletal growth after a tooth comes into occlusion, but its direct role on blood flow no longer applies.
Question 6
What is the most important initial diagnostic sign of primary failure of eruption?
- 1st molars failing to erupt after eruption path is cleared
- 1st and 2nd molars failing to erupt after eruption path is cleared ✓
- failure of the roots to form after crown formation is complete
- failure of the affected teeth to respond to orthodontic force
- submergence of the affected teeth
Correct
That’s correct, the primary diagnostic sign of primary failure of eruption is failure of 1st and 2nd molars to erupt even though an eruption path has been cleared for them. If first molars fail to erupt, the problem may be just ankylosis; if other posterior teeth in the same quadrant also fail to erupt, it’s probably primary failure. In primary failure, second premolars often also are affected. It’s true that the affected teeth may appear to submerge over time, and that they do not respond to orthodontic force, but these are best thought of as confirmatory rather than initial diagnostic signs.
Incorrect
That’s wrong. The primary diagnostic sign of primary failure of eruption is failure of 1st and 2nd molars to erupt even though an eruption path has been cleared for them. If first molars fail to erupt, the problem may be just ankylosis; if other posterior teeth in the same quadrant also fail to erupt, it’s probably primary failure. In primary failure, second premolars often also are affected. It’s true that the affected teeth may appear to submerge over time, and that they do not respond to orthodontic force, but these are best thought of as confirmatory rather than initial diagnostic signs.
Question 7
What controls the rate of pre-emergent eruption?
- the rate of bone resorption over the tooth ✓
- the rate of root formation
- the rate of formation of new tissue at the root apex
- the amount of force generated by the eruption mechanism
Correct
That’s right, the rate at which obstacles to eruption are removed, not the rate at which new tissue forms or the amount of force from the eruption mechanism, is what controls pre-emergent eruption. Normally, an eruption path is formed, and then the eruption mechanism moves the tooth along that path so that the crown stays close to the area where bone, primary tooth roots or gingiva are being resorbed. Failure of a tooth to follow along a cleared eruption path indicates either mechanical failure of eruption (ankylosis) or primary failure of eruption (abnormal PDL, eruption mechanism doesn’t work).
Incorrect
No, that’s wrong. The rate at which obstacles to eruption are removed, not the rate at which new tissue forms or the amount of force from the eruption mechanism, is what controls pre-emergent eruption. Normally, an eruption path is formed, and then the eruption mechanism moves the tooth along that path so that the crown stays close to the area where bone, primary tooth roots or gingiva are being resorbed. Failure of a tooth to follow along a cleared eruption path indicates either mechanical failure of eruption (ankylosis) or primary failure of eruption (abnormal PDL, eruption mechanism doesn’t work).
Question 8
(A) If a tooth becomes ankylosed and fails to erupt, it appears to submerge because (B) the alveolar bone grows past it and may eventually cover it over.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false ✓
- A false, B true
- A and B false
Correct
That’s correct, the first statement is correct but the second is false. Alveolar bone forms in response to eruption of a tooth, so if a tooth becomes ankylosed, no bone forms in that area, and there is likely to be a long-term alveolar defect. If an ankylosed tooth is totally covered over, it’s by soft tissue only.
Incorrect
No, that’s incorrect. The first statement is correct but the second is false. Alveolar bone forms in response to eruption of a tooth, so if a tooth becomes ankylosed, no bone forms in that area, and there is likely to be a long-term alveolar defect. If an ankylosed tooth is totally covered over, it’s by soft tissue only.
Question 9
Which of the following is the major mechanism of post-emergent eruption after a tooth comes into occlusion?
- shortening of collagen fibers in the PDL ✓
- contractile fibroblasts in the PDL
- pressure from proliferating cells at the root apex
- blood pressure / flow in the PDL
Correct
That’s right, maturation and shortening of collagen fibers in the PDL is now thought to be the major mechanism of post-emergent eruption. The other possibilities cannot be totally ruled out but are not supported by experimental evidence.
Incorrect
No, that’s not the best answer. Maturation and shortening of collagen fibers in the PDL is now thought to be the major mechanism of post-emergent eruption. The other possibilities cannot be totally ruled out but are not supported by experimental evidence.
Question 10
During the crown formation stage of tooth eruption, the direction of eruption is:
- anterior
- posterior
- a and c
- no eruptive movements occur ✓
Correct
That’s correct. The tooth enlarges during crown formation, but movement toward the occlusal plane doesn’t start until root formation begins, and there are no anterior or posterior movements during crown formation.
Incorrect
That’s wrong. The tooth enlarges during crown formation, but movement toward the occlusal plane doesn’t start until root formation begins, and there are no anterior or posterior movements during crown formation.
Question 11
The eruption of a mandibular molar is best described relative to the:
- cranial base
- occlusal plane
- core bone of the maxilla
- core bone of the mandible ✓
Correct
That’s right. An erupting mandibular tooth moves relative to the cranial base, occlusal plane and maxilla, but eruption is defined as movement of a tooth relative to its jaw. For a mandibular molar, of course that’s the mandible.
Incorrect
That’s wrong. An erupting mandibular tooth moves relative to the cranial base, occlusal plane and maxilla, but eruption is defined as movement of a tooth relative to its jaw. For a mandibular molar, of course that’s the mandible.
Question 12
How does the prognosis for the unerupted teeth in primary failure of eruption compare to the prognosis for an unerupted tooth that is mechanically obstructed?
- worse ✓
- about the same
- better
- impossible to predict
Correct
That’s right, the prognosis is worse. If a mechanical obstruction is removed, there is a chance that unerupted teeth will erupt on their own, and if not, they can be pulled into position orthodontically. But when the eruption mechanism fails, there is an abnormality of the periodontal ligament that makes teeth impossible to move orthodontically. The only option in primary failure of eruption is to eventually replace the unerupted teeth with some type of prosthesis.
Incorrect
No, that’s wrong, the prognosis is worse. If a mechanical obstruction is removed, there is a chance that unerupted teeth will erupt on their own, and if not, they can be pulled into position orthodontically. But when the eruption mechanism fails, there is an abnormality of the periodontal ligament that makes teeth impossible to move orthodontically. The only option in primary failure of eruption is to eventually replace the unerupted teeth with some type of prosthesis.