Facial Growth Patterns
Purpose of this Program
In this program we discuss facial growth in the context of different growth patterns, their clinical presentations, and their treatment considerations. Read pages 96-103 in the 5th edition of Contemporary Orthodontics (or pages 111-119 in the 4th ed.) in addition to viewing the teaching program. Be sure you are able to:
- describe the normal pattern of facial growth and development, specifying the changes in the cranium, cranial base, maxilla, and mandible
- differentiate skeletal Class I, Class II, and Class III jaw relationships and growth patterns
- describe the interaction between changes in the position of the dentition during growth and the facial growth pattern.
Facial Growth: Patterns and Principles
Before we discuss facial growth patterns, it is important to quickly review the concepts of pattern and growth pattern that you learned in the first part of this course:
- A pattern is defined as the proportional relationships of parts.
- A growth pattern refers to how proportional relationships change, or fail to change over time.
In the context of facial growth, pattern describes how various facial structures relate to each other. Growth patterns refer to how these facial proportional relationships change over time as we grow and mature.
Timing of Facial Growth with General Body Growth
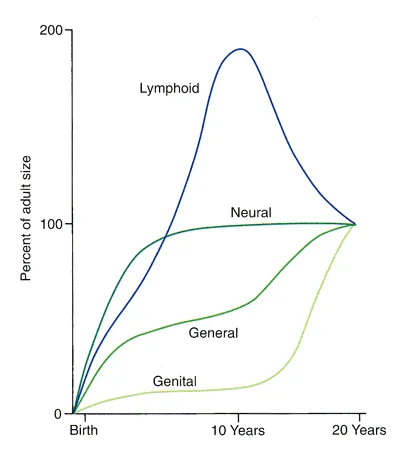
Remember, a major influence on the pattern of facial skeletal growth is the different timing of growth of different body tissues. By now you’re very familiar with Scammon’s curves, but it’s important to keep in mind that not all structures in the body grow at the same rate at the same time.
Craniofacial Skeleton: Functional Units
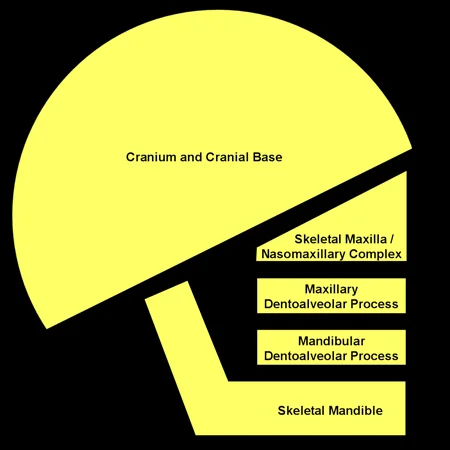
You will recall that it is easiest to understand the facial skeleton as a set of major functional units. The major functional units of the craniofacial complex are:
- Cranium and cranial base
- Maxilla
- Maxillary dentoalveolar process
- Mandibular dentoalveolar process
- Mandible
Let’s review the effect of different growth timing for different types of tissues on the facial growth pattern.
Craniofacial Growth: Cranium and Cranial Base
The cranium and cranial base follow Scammon’s neural curve and complete most of their growth by age 7.
Craniofacial Growth: Maxilla and Mandible
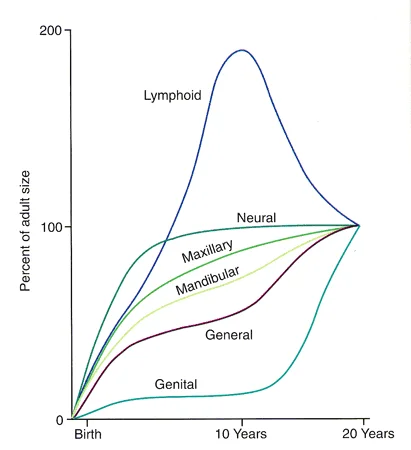
The growth pattern of the face is influenced by an interaction between neural and general body growth. The result is that the facial skeleton grows according to a cephalocaudal gradient—the structures closest to the brain, which follows the neural growth curve, grow faster initially and mature earlier than structures closer to the bottom of the head. At birth, the mandible is relatively underdeveloped relative to the maxilla, and it gradually catches up but really doesn’t do so until the adolescent growth spurt is completed.
Craniofacial Growth: Facial Soft Tissue
It is also important to consider the growth of the facial soft tissues. Of course the soft tissues that cover the cranium have to follow the neural curve. You will not be surprised to hear that the cephalocaudal gradient also can be seen in the nose. The nasal bone completes its growth around age 10, but the cartilage and soft tissues of the nose (which are further from the brain) grow and become more prominent during adolescence. The mandibular musculature grows and becomes stronger during adolescence, as do the lips. The soft tissue chin is something of an exception-it becomes more prominent as the mandible grows forward but the soft tissue itself does not thicken appreciably.
Can you see these changes in the boy pictured in images 1 and 2?
 Image 1: Age 11-10 Image 1: Age 11-10 | 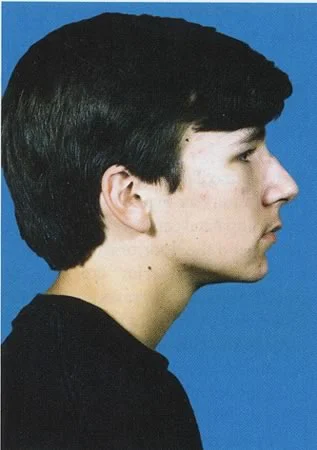 Image 2: Age 14-4 Image 2: Age 14-4 |
Constancy of the Pattern
Although all children more or less follow Scammon’s curves, it is obvious that facial proportions are different in different individuals. For example, some children have a relatively small mandible, some a relatively large nose, etc.
These differences tend to stay relatively constant during growth, which is another way of saying that the facial pattern in childhood tends to stay the same as a person grows and matures. For example, a child with mandibular deficiency is likely to remain mandibular deficient during adolescence and adulthood, while a child with true mandibular excess is likely to exhibit mandibular excess during adolescence and adulthood.
Although constancy of the facial pattern is the rule, there are exceptions. Trauma, hormonal disturbances, and a number of other growth problems can affect and change facial symmetry and proportions.
Assessing Skeletal Growth (cephalometrics)
Cephalometrics
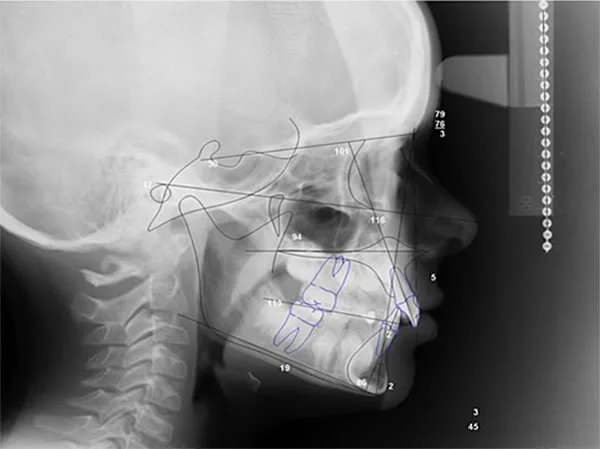
The structural components of the cranium and face can be distinguished well in a lateral projection (image 1). A lateral cephalometric radiograph (image 2) is an excellent way to document and understand the relationships between facial skeletal structures, or facial pattern. Note that you could outline the structural units on the radiograph (which we will call a ceph from now on) just as you could on the anatomic drawing. These radiographs are particularly valuable in evaluating how the five functional units relate to each other.

Cephalometric Tracings
A single cephalometric radiograph provides a snapshot of what the facial pattern and relationships are at any single point of time. In order to analyze facial pattern, it helps to make a tracing of the radiograph that outlines the functional units and other important structures of the facial skeleton. The tracing reduces the amount of information contained on a radiograph to the essential structures, and makes more apparent how these structures relate to each other.
Cephalometric Superimpositions
It is only by carefully comparing radiographs taken at different times that we can truly discover and understand the changes in facial proportions over time, the facial growth pattern.
When two cephalometric tracings from radiographs of the same individual are superimposed on stable structure, areas that do not overlap are areas where changes, typically growth, have occurred. The tracings shown here are superimposed on the cranial base, which completes its growth around age 7, and therefore is stable after that time. This makes the cranial base superimposition ideal for showing the growth of the face after the time that permanent teeth are beginning to erupt.
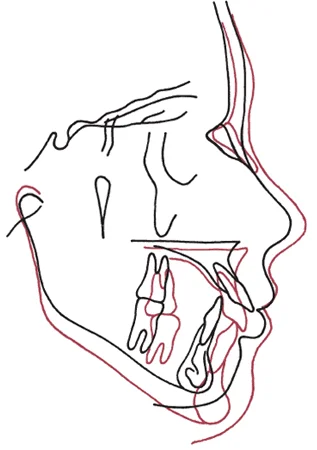
Cephalometrics: Stable Landmarks
This comparison of radiographs shows how facial structures grow—the absolute amount for individual structures, and the relative amount compared to adjacent structures.
The superimposition shows that relative to the cranial base, the facial structures grew downward and forward. Note the somewhat greater growth of the mandible than the maxilla, which you would expect from the cephalocaudal gradient of growth that we discussed previously.
Variations in Skeletal Growth
Maxilla and Mandible
Variation in facial growth affects the relationship between the functional units of the craniofacial complex, and you are used to seeing differing facial patterns all around you.
Some degree of variation is normal, but extreme variation in the growth of one or more of the functional units can cause facial disharmony that creates problems for the affected individual and could be considered abnormal. These growth variations occur in varying degrees and directions. For our purposes, fairly extreme examples help to illustrate this important concept. It is obvious that the girl in image 1 has had less mandibular growth than normal, and that the boy in image 2 has had too much.
Differences in the facial pattern resulting from variations in facial growth are most easily understood when analyzing the functional units in separate planes of space: antero-posterior, vertical, or transverse.
 Image 1: This boy has an obviously deficient mandible, and a Class II profile. Image 1: This boy has an obviously deficient mandible, and a Class II profile. | 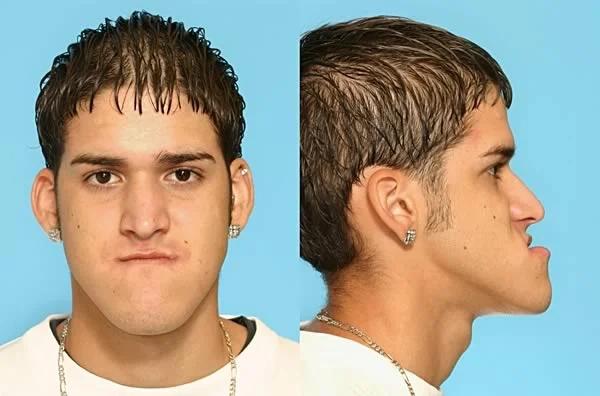 Image 2: This young man has an impressively large mandible, and a Class III profile. Image 2: This young man has an impressively large mandible, and a Class III profile. |
AP Variations in Skeletal Growth: Class II
Antero-posterior growth variations are typically expressed in an altered A-P position of either the maxilla, mandible, or both jaws.
A skeletal Class II jaw relationship occurs when the maxilla is positioned a significant amount anteriorly relative to the mandible or the mandible is significantly posterior to the maxilla. This can have several causes that are illustrated below in block diagrams using the structural components: mandibular deficiency (image 1, image 4); maxillary excess, which also is called maxillary prognathism (image 2); or a combination of both (image 3, image 5). A Class II relationship typically results in increased overjet that is due to the displacement of the jaws, not to displacement of the teeth relative to their own jaw.
By definition, a Class II growth pattern is one that leads to a skeletal Class II jaw relationship.
 Image 1: Normal maxilla, deficient mandible Image 1: Normal maxilla, deficient mandible |  Image 2: Prognathic maxilla, normal mandible Image 2: Prognathic maxilla, normal mandible |
 Image 3: Prognathic maxilla, deficient mandible Image 3: Prognathic maxilla, deficient mandible |  Image 4: Severe Class II, deficient mandible Image 4: Severe Class II, deficient mandible |
 Image 5: Severe Class II, deficient mandible Image 5: Severe Class II, deficient mandible |
A-P Variations in Skeletal Growth: Class III
A skeletal Class III jaw relationship occurs when the maxilla is positioned behind the mandible, and of course a Class III growth pattern leads to this condition.
This A-P relationship in the position of the jaws can have several causes: mandibular excess, which is also called mandibular prognathism (image 1); maxillary deficiency (image 2); or a combination of both (images 3,4,5). These jaw relationships usually result in no overjet (end-to-end incisors) or reverse overjet.
 Image 1: Normal maxilla and prognathic mandible Image 1: Normal maxilla and prognathic mandible |  Image 2: Deficient maxilla and normal mandible Image 2: Deficient maxilla and normal mandible |
 Image 3: Deficient maxilla and prognathic mandible Image 3: Deficient maxilla and prognathic mandible |  Image 4: Deficient maxilla and prognathic mandible Image 4: Deficient maxilla and prognathic mandible |
 Image 5: Deficient maxilla and prognathic mandible Image 5: Deficient maxilla and prognathic mandible |
A-P Variations in Skeletal Growth: Class I (Bimaxillary Protrusion)
Sometimes an individual can have normal skeletal relationship between the maxilla and mandible (image 1), but have both the upper and lower teeth and dentoalveolar processes displaced anteriorly relative to their skeletal bases (images 2,3,4).
In patients like this, the growth pattern of the jaws is normal (which is called a Class I growth pattern). The patient’s condition, strictly speaking, is bimaxillary dentoalveolar protrusion, but it is called bimaxillary protrusion for short (except by anthropologists, who use bimaxillary protrusion to describe protrusion of both jaws relative to the cranium). The dentists’ bimaxillary protrusion is characterized by proclined maxillary and mandibular incisors on normally positioned jaws (see image 2).
 Image 1: Normal skeletal and dental relationships Image 1: Normal skeletal and dental relationships |  Image 2: Bimaxillary dentoalveolar protrusion, normal jaw relationship Image 2: Bimaxillary dentoalveolar protrusion, normal jaw relationship |
 Image 3: Bimaxillary dentoalveolar protrusion, normal jaw relationship Image 3: Bimaxillary dentoalveolar protrusion, normal jaw relationship |  Image 4: Bimaxillary dentoalveolar protrusion, normal jaw relationship Image 4: Bimaxillary dentoalveolar protrusion, normal jaw relationship |
Vertical Variations in Skeletal Growth
For normal jaw relationships, both the a-p and vertical positions of the jaws must be normal (image 1). Variations in vertical growth result in an altered vertical position of either the maxilla, mandible, or both jaws.
The two extremes are skeletal open bite (long face) and skeletal deep bite (short face) patterns (images 2 and 3, respectively). Naturally, the growth patterns that produce these conditions are called the long face (or open bite) and short face (or deep bite) growth patterns.
 Image 1: Normal vertical (and A-P) jaw relationships Image 1: Normal vertical (and A-P) jaw relationships |  Image 2: Long face (skeletal open bite) jaw relationships Image 2: Long face (skeletal open bite) jaw relationships |
Vertical Variations in Skeletal Growth: Open Bite / Long Face
Skeletal open bite, characterized by anterior open bite and a long face (increased vertical face height, see image 1), often is caused by a maxilla that has grown more in the posterior than anterior. This results in a palatal plane that appears tipped down posteriorly and downward-backward rotation of the mandible (image 2).
It can also be caused by a short mandibular ramus, which also leads to downward-backward rotation of the mandible, often with an increased gonial angle and steep mandibular plane (images 3 and 4).
 Image 1: Long face pattern Image 1: Long face pattern |  Image 2: Skeletal open bite, downward-back rotation of mandible Image 2: Skeletal open bite, downward-back rotation of mandible |
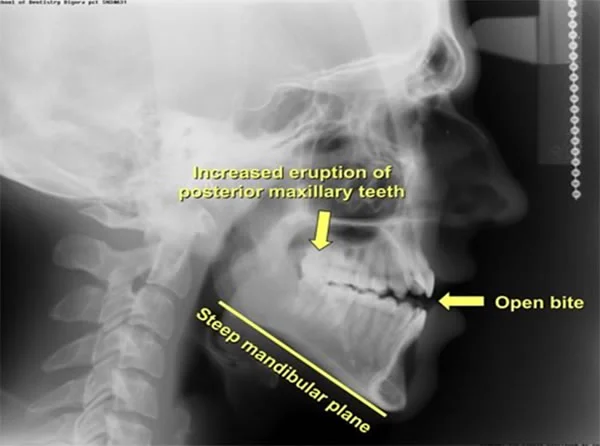 Image 3: Long face pattern, open bite Image 3: Long face pattern, open bite | 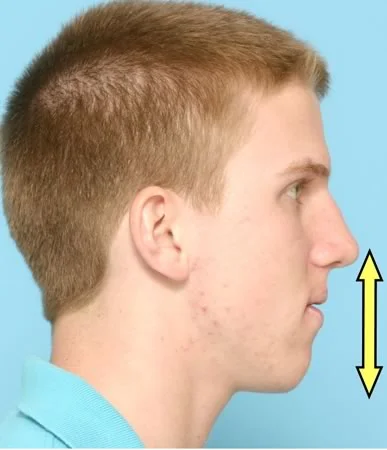 Image 4: Long face pattern; note increased lower face height Image 4: Long face pattern; note increased lower face height |
Vertical Variations in Skeletal Growth: Deep Bite / Short Face
At the other extreme is the skeletal deep bite pattern, characterized by a short face that almost always is accompanied by a deep bite (image 1).
This is often caused by a growth pattern that leads to a long mandibular ramus, decreased gonial angle and flat mandibular plane (images 2,3,4). This boy has maxillary incisors that are tipped forward and are protrusive. That’s not uncommon in patients with a deep bite, but it’s not part of the vertical problem—you can have a short face and deep bite without protrusion of upper incisors.
 Image 1: Short face, deep bite anteriorly (excessive overbite) Image 1: Short face, deep bite anteriorly (excessive overbite) |  Image 2: Short face pattern Image 2: Short face pattern |
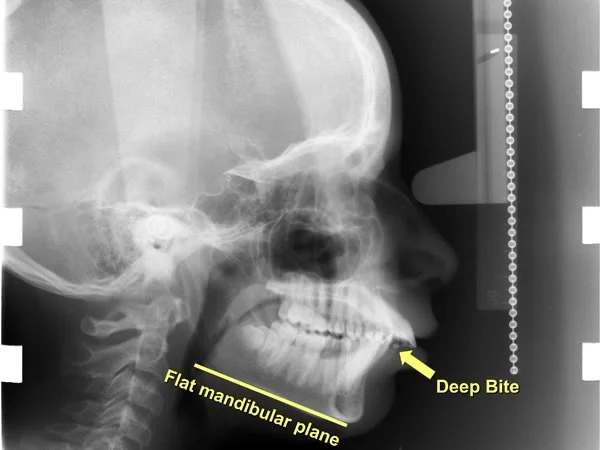 Image 3: Short face pattern (same pt.) Image 3: Short face pattern (same pt.) | 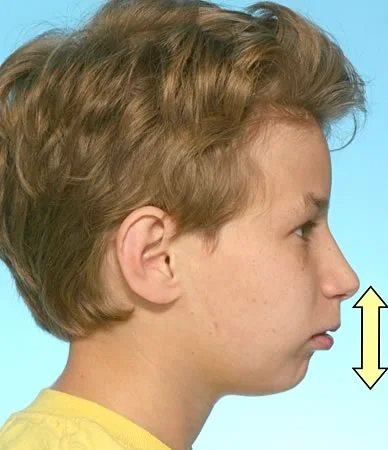 Image 4: Short face pattern (same pt.) Image 4: Short face pattern (same pt.) |
Transverse Variations in Skeletal Growth
Transverse growth variations are typically expressed in an altered transverse position of the mandible. True maxillary asymmetry is rare, but mandibular asymmetry occurs frequently.
A mandibular asymmetry with the chin to the right side can result from excess growth on the left, decreased growth or degeneration on the right, or a combination of both. Conversely, a mandibular asymmetry to the left (as shown here) can result from excess growth on the right, decreased growth or degeneration on the left side, or a combination of both.

Transverse Variations in Skeletal Growth: Patient Example
For this patient (image 1), the deviation of the mandible to her left can be seen even more clearly in a P-A cephalometric radiograph (image 2). She has a corresponding mandibular midline deviation to the left that can be seen in her intraoral photograph (image 3). Examination of her panoramic radiograph reveals a left mandibular condyle that is smaller than the right mandibular condyle (image 4).
Detecting the asymmetry may be easy in a case like this, but understanding the cause of the asymmetry can be much more difficult. Because her face height is abnormally long on the right side, the asymmetric mandibular growth was elongation of the neck of the ramus on the right, which pushed the chin to the left.
| Image 1: Frontal photograph, note chin asymmetry |  Image 2: P-A cephalometric radiograph, same pt. Image 2: P-A cephalometric radiograph, same pt. |
 Image 3: Frontal intraoral photo, note midline deviation Image 3: Frontal intraoral photo, note midline deviation |  Image 4: Panoramic radiograph, note long condylar neck on right Image 4: Panoramic radiograph, note long condylar neck on right |
Complex Variations in Skeletal Growth
Disturbances in facial growth that affect multiple planes of space can create complex deformities. Analyzing facial and facial growth patterns using three distinct planes of space helps you fully analyze and understand the variation.
This patient (image 1), more obviously than the previous one, has hemimandibular hypertrophy (excessive growth of the mandible on one side). Notice how the excess growth of the right condyle and ramus (image 5) has caused problems in all three planes of space, including mandibular asymmetry, a dental midline discrepancy, and lateral open bite (images 2,3). In the lateral cephalometric radiograph (image 4), you can see two distinct mandibular planes because the ramus is longer on the right side. In addition, there is a Class III molar relationship on the right side.
 Image 1: Frontal view, chin off to left Image 1: Frontal view, chin off to left |  Image 2: Note unilateral posterior open bite Image 2: Note unilateral posterior open bite |
 Image 3: P-A cephalometric radiograph (same pt) Image 3: P-A cephalometric radiograph (same pt) |  Image 4: Lateral cephalometric radiograph (same pt) Image 4: Lateral cephalometric radiograph (same pt) |
 Image 5: Panoramic radiograph, note the long condylar process on the right Image 5: Panoramic radiograph, note the long condylar process on the right |
Dental Compensations for Skeletal Discrepancies
Dental Compensations for Skeletal Discrepancies
Now let’s look at the effect these skeletal variations have on the teeth and dentoalveolar processes. The dentition exhibits a remarkable ability to compensate for an unfortunate growth pattern of the jaws. These compensations allow individuals with different facial types to have teeth that fit together reasonably well despite the jaw relationships. Even if a severe malocclusion results from the growth pattern, often the dental compensations mask the severity of the skeletal problem, i.e., the jaw deviations are worse than the dental deviations.
Again, it is easiest to understand these dental compensations by analyzing in three planes of space the dental compensations that accompany different facial patterns.
Dental Compensations for Class II Growth Patterns
Class II patients often have upper incisors that are upright or more lingual relative to the maxilla, and lower incisors that are flared facially relative to the mandible (image 1).
Notice how this patient has a deficient mandible (image 2) but a relatively minimal increase in overjet because of forward movement of the lower teeth relative to the mandible and lingual tipping of upper incisors (image 3). The lower incisors are not as far forward as they would have been if the growth pattern were normal and the mandible were not deficient.
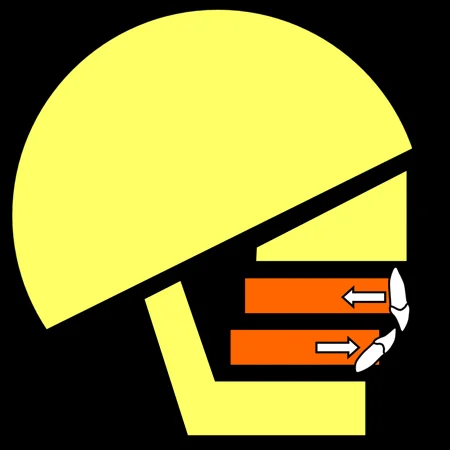 Image 1: Dental compensation for Class II growth Image 1: Dental compensation for Class II growth |  Image 2: Skeletal Class II, mandibular deficiency Image 2: Skeletal Class II, mandibular deficiency |
 Image 3: Forward position of mandibular teeth, decreasing overjet Image 3: Forward position of mandibular teeth, decreasing overjet |
AP Dental Compensations: Skeletal Class III
Class III patients often have upper incisors that are flared facially relative to the maxilla and lower incisors that are upright relative to the mandible (image 1).
Notice how this patient (image 2) has a Class III profile with the typical associated dental compensations. Her Class III skeletal problem (image 3) was so severe that even with the dental compensations she could not maintain a positive overjet. She was treated with surgical repositioning of the jaws.
 Image 1: Dental compensation for Class III growth Image 1: Dental compensation for Class III growth |  Image 2: Severe skeletal Class III Image 2: Severe skeletal Class III |
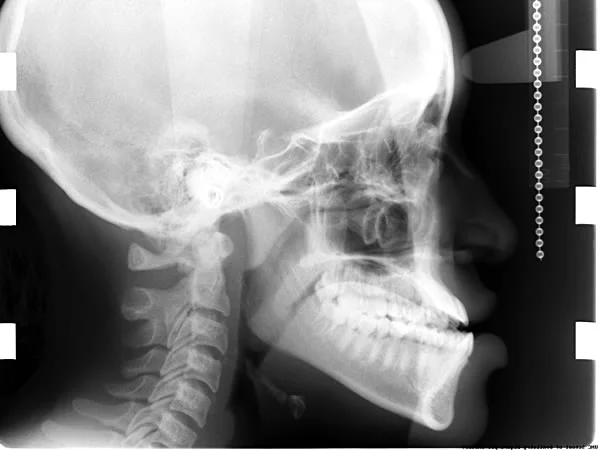 Image 3: Note the proclined upper incisors and upright lower incisors (same pt) Image 3: Note the proclined upper incisors and upright lower incisors (same pt) |
AP Dental Compensations
Many patients with Class II and Class III jaw relationships can have fairly normal overjet, despite the fact that there is a significant discrepancy between the AP position of the maxilla and mandible.
These two patients (images 1,2 and images 3,4) have relatively small differences in overjet and similar dental occlusion, but widely different jaw structures and relationships.
 Image 1: profile view, Class II patient Image 1: profile view, Class II patient |  Image 2: note the upright maxillary incisors and proclined lower incisors Image 2: note the upright maxillary incisors and proclined lower incisors |
 Image 3: profile view, Class III patient Image 3: profile view, Class III patient |  Image 4: note the proclined upper incisors and upright lower incisors Image 4: note the proclined upper incisors and upright lower incisors |
Vertical Dental Compensations: Skeletal Open Bite
Vertical dental compensations are expressed in the vertical position of incisors relative to their skeletal bases (maxilla or mandible). Remember that a skeletal open bite pattern is often associated with a short mandibular ramus and steep mandibular plane.
In order to compensate for this skeletal pattern, more eruption of incisors than normal would decrease the open bite (image 1). Patients with these compensations (images 2,3,4) can have relatively normal overbite relationships, especially when compared to their underlying skeletal pattern. For this girl, incisor eruption almost totally compensated for the downward rotation of the mandible—but she would benefit from correction of her Class III and long face characteristics. This would require surgical repositioning of both jaws.
 Image 1: dental compensation for skeletal open bite Image 1: dental compensation for skeletal open bite |  Image 2: long face, Class III facial pattern Image 2: long face, Class III facial pattern |
 Image 3: long face, Class III facial pattern Image 3: long face, Class III facial pattern |  Image 4: anterior view of dentition: no open bite despite long face Image 4: anterior view of dentition: no open bite despite long face |
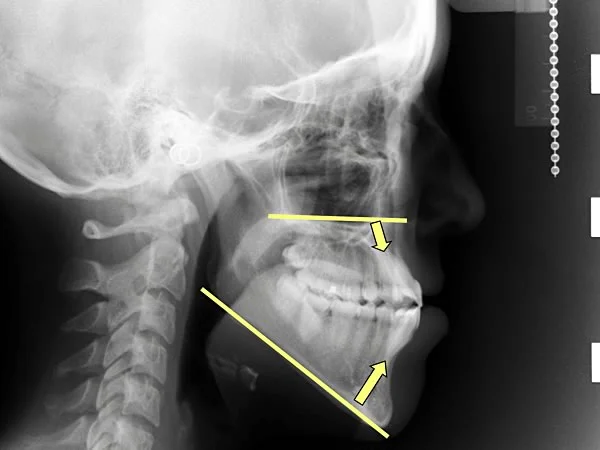 Image 5: note excessive eruption of incisors Image 5: note excessive eruption of incisors |
Vertical Dental Compensations: Skeletal Deep Bite
Remember that patients with a skeletal deep bite pattern typically have a decreased gonial angle and a flat mandibular plane. In order to compensate for this relationship, less than normal eruption of incisors would be required (image 1).
This short-face girl has reasonably normal overbite despite her short face (images 2,3,4,5). Note the facial tipping of the incisors in both arches.
 Image 1: short face height predisposes a patient to anterior deep bite Image 1: short face height predisposes a patient to anterior deep bite |  Image 2: short face patient Image 2: short face patient |
 Image 3: short face patient Image 3: short face patient |  Image 4: minimal overbite despite short face pattern Image 4: minimal overbite despite short face pattern |
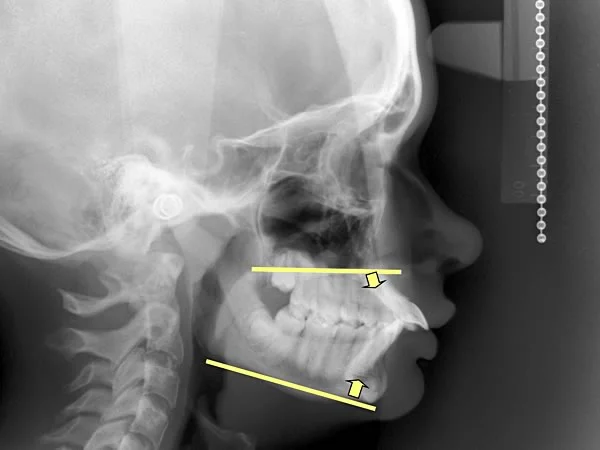 Image 5: minimal overbite, but incisors are severely proclined Image 5: minimal overbite, but incisors are severely proclined |
Transverse Dental Compensations: Skeletal Asymmetry
As with the other planes of space, transverse dental compensations usually accompany asymmetric jaw growth. If the jaw deviates to one side, the teeth shift back toward the midline so that the dental midline discrepancy often is less than the jaw discrepancy.
For this patient the dental compensation is apparent but not nearly enough to create normal dental occlusion, and treatment would have to be surgery to reposition the jaws. In order to get good jaw relationships, however, the dental compensation would have to be removed by presurgical orthodontic treatment.
| PA cephalometric film: Note the mandibular asymmetry with the chin to the patient’s left. | Same patient, intraoral view: The position of the mandibular teeth are compensated to mask the skeletal asymmetry of the mandible. |
Orthodontic Treatment in the Context of Growth
Treatment for Growing Patients
For growing patients, it is important to recognize skeletal malocclusions so they can be treated at the appropriate time. Often this treatment will involve growth modification—trying to alter the position of the skeletal bases and/or dentoalveolar segments while an individual is growing. Of course, you can’t modify growth that isn’t happening, either because the child is in a period of slow growth prior to the adolescent growth spurt, or because an adolescent already is past the growth spurt.
For example, consider the problem presented by failure of the maxilla to grow forward as it should (image 1). This 7 year-old boy presented with the a convex profile and a facial appearance of maxillary deficiency and an anterior crossbite (images 2,3). Cephalometric analysis revealed a component of maxillary deficiency contributing to his Class III skeletal pattern and reverse overjet (image 4).
 Image 1: maxillary deficient Class III Image 1: maxillary deficient Class III |  Image 2: age 7, profile appearance Image 2: age 7, profile appearance |
 Image 3: age 7, cephalometric radiograph Image 3: age 7, cephalometric radiograph |  Image 4: age 7, anterior crossbite Image 4: age 7, anterior crossbite |
Treatment for Growing Patients (cont.)
His treatment involved a reverse pull headgear to protract the maxilla and maxillary dentoalveolar segments (image 1). This resulted in elimination of the anterior crossbite (compare images 2 and 3), and a flattening of the profile convexity as the maxilla moved forward.
This treatment has to be done before the sutures of the maxilla become so interdigitated that the maxilla cannot be moved forward. The ideal time for most children is between ages 6 and 8 (depending on their physiologic maturity rather than chronologic age). If it is delayed beyond about age 10, the skeletal deficiency no longer can be treated without surgery.
 Image 1: growth modification treatment, moving maxilla forward Image 1: growth modification treatment, moving maxilla forward |  Image 2: age 7, before growth modification treatment Image 2: age 7, before growth modification treatment |
 Image 3: age 8, after treatment Image 3: age 8, after treatment |
Treatment for Adults / Non-Growing Patients
In older patients who have completed the vast majority of their growth, there are fewer options for treating a skeletal malocclusion. Sometimes a jaw discrepancy is so great (image 1) that repositioning the jaws through orthognathic surgery is the only way to obtain an acceptable facial appearance (image 2) and get the teeth to fit together normally.
Early diagnosis of the facial pattern and growth pattern, and appropriate treatment at the ideal time are essential for effectively treating skeletal malocclusions. Unfortunately, it is almost impossible to control excessive mandibular growth, and an individual with this growth pattern is quite likely to end up needing surgery, despite efforts to treat it during growth.
Fortunately, as these pre- (image 1) and post-surgery (image 2) images show, it is possible now to correct jaw deformities with surgical repositioning of either or both jaws. Class III problems are more likely to require surgery because of the tendency of the mandible to grow after maxillary growth is nearly completed.
 Image 1, A girl with a Class III skeletal relationship: Her malocclusion was treated with surgical-orthodontics since she was no longer growing. Image 1, A girl with a Class III skeletal relationship: Her malocclusion was treated with surgical-orthodontics since she was no longer growing. |  Image 2, Same girl post-surgery: Her maxilla was moved forward surgically to correct her skeletal and dental Class III relationships. Image 2, Same girl post-surgery: Her maxilla was moved forward surgically to correct her skeletal and dental Class III relationships. |
Summary
In summary:
- The pattern of facial growth reflects an interaction between the neural and general body growth curves, so that growth of the face trails behind growth of the cranium and cranial base, and growth of the mandible trails behind growth of the maxilla
- Some individuals have a pattern of growth with excessive or deficient growth of the maxilla and/or mandible, which leads to what is best described as a skeletal malocclusion (by definition, a skeletal malocclusion means that the jaw position is abnormal and tends to create a dental malocclusion).
- For mild skeletal discrepancies, dental compensation during growth may create normal dental occlusion, and if not dental compensation created by orthodontic treatment can be satisfactory. For moderately severe discrepancies, growth modification can be successful treatment; for the most severe ones, surgery is the only option.
- Mandibular growth that is more downward and less forward leads to a Class II skeletal and dental relationship.
- Mandibular growth that is more forward and less downward leads to a Class III skeletal and dental relationship.
- The pattern of facial growth, whether normal or leading to skeletal malocclusion, is established early and rarely changes spontaneously.
- In children with skeletal malocclusion, dental compensation for the skeletal discrepancy usually occurs so that the dental occlusion is less abnormal than the jaw relationship.
Now take the self-test in the following section. Before you do, be sure you have read pages 96-103 in the 5th edition of Contemporary Orthodontics (or pages 111-119 in the 4th ed.). Then use the self-test to help you understand these concepts of evaluating patients and using that information to plan appropriate treatment.
Self-Test
Question 1
Growth pattern of the face refers to:
- proportional relationships during growth
- changes in proportional relationships during growth ✓
- the rate of growth of the components of the head and face
- all of the above
Correct
That’s right, growth pattern refers to the way proportional relationships in the face change during growth, not to the proportional relationships themselves or to the rate of growth of the components.
Incorrect
That’s incorrect, growth pattern refers to the way proportional relationships in the face change during growth, not to the proportional relationships themselves or to the rate of growth of the components.
Question 2
The major characteristic of a Class I skeletal relationship in a profile view is:
- cranial, facial and dental structures in a nearly straight line ✓
- facial and dental structures straight but prominent to the cranium
- cranial and facial structures in a nearly straight line, teeth can be anywhere
- maxilla forward relative to mandible
- mandible forward relative to maxilla
Correct
That’s correct. In a Class I (normal) relationship, the cranium, maxilla, maxillary teeth, mandibular teeth and mandible are in a nearly straight line.
Incorrect
That’s wrong. In a Class I (normal) relationship, the cranium, maxilla, maxillary teeth, mandibular teeth and mandible are in a nearly straight line.
Question 3
The major characteristic of a Class II skeletal relationship is:
- cranial, facial and dental structures in a nearly straight line
- facial and dental structures straight but prominent to the cranium
- cranial and facial structures in a nearly straight line, teeth can be anywhere
- maxilla forward relative to mandible ✓
- mandible forward relative to maxilla
Correct
That’s right. In a Class II relationship the maxilla is forward relative to the mandible. This can occur because the maxilla grew normally while the mandible grew less than normal, or because the maxilla grew too much, or any combination of deficient mandibular and excess maxillary growth.
Incorrect
No, that’s wrong. In a Class II relationship the maxilla is forward relative to the mandible. This can occur because the maxilla grew normally while the mandible grew less than normal, or because the maxilla grew too much, or any combination of deficient mandibular and excess maxillary growth.
Question 4
The major characteristic of a Class III skeletal relationship is:
- cranial, facial and dental structures in a nearly straight line
- facial and dental structures straight but prominent to the cranium
- cranial and facial structures in a nearly straight line, teeth can be anywhere
- maxilla forward relative to mandible
- mandible forward relative to maxilla ✓
Correct
That’s right. In a Class III relationship the mandible is forward relative to the maxilla. This can occur because the mandible grew normally while the maxilla grew less than normal, because the mandible grew too much, or any combination of deficient maxillary and excess mandibular growth.
Incorrect
That’s incorrect. In a Class III relationship the mandible is forward relative to the maxilla. This can occur because the mandible grew normally while the maxilla grew less than normal, because the mandible grew too much, or any combination of deficient maxillary and excess mandibular growth.
Question 5
For which of the following is the adolescent growth spurt least prominent?
- weight
- height
- lower jaw length
- upper jaw length ✓
Correct
That’s right. Because the maxilla is influenced by the neural growth curve, it has less response to the adolescent growth spurt that particularly affects general body growth than the mandible and weight / height.
Incorrect
That’s wrong. Because the maxilla is influenced by the neural growth curve, it has less response to the adolescent growth spurt that particularly affects general body growth than the mandible and weight / height.
Question 6
What would you expect to happen to the a-p position of the lower incisors in response to a Class II growth pattern?
- forward (facial) movement ✓
- little or no movement
- backward (lingual) movement
- vertical change more probable than a-p change
Correct
That’s correct. If the maxilla grows forward more than the mandible in a Class II growth pattern, often the lower incisors partially compensate by moving forward (facially).
Incorrect
No, that’s wrong. If the maxilla grows forward more than the mandible in a Class II growth pattern, often the lower incisors partially compensate by moving forward (facially).
Question 7
What would you expect to happen to the a-p position of the upper incisors in response to a Class III growth pattern?
- forward (facial) movement ✓
- little or no movement
- backward (lingual) movement
- vertical change more probable than facio-lingual change
Correct
That’s correct. In response to a Class III growth pattern the upper incisors would tend to tip forward, moving facially. In a skeletal Class III patient, the forward movement of the upper incisors and the backward movement of the lower incisors both reduce the relative protrusion of the lower teeth. This is a classic example of dental compensation for a skeletal discrepancy. In Class III or Class II patients, the dental occlusion is often better than the jaw relationship at the end of growth for this reason.
Incorrect
That’s wrong. In response to a Class III growth pattern the upper incisors would tend to tip forward, moving facially. In a skeletal Class III patient, the forward movement of the upper incisors and the backward movement of the lower incisors both reduce the relative protrusion of the lower teeth. This is a classic example of dental compensation for a skeletal discrepancy. In Class III or Class II patients, the dental occlusion is often better than the jaw relationship at the end of growth for this reason.
Question 8
In a child with end-to-end permanent first molars at age 10 and a mild Class II growth pattern, what is the most likely molar relationship at age 12?
- Class I
- end-to-end ✓
- Class II
- Class III
Correct
That’s correct. With a mild Class II growth pattern it is unlikely that the end-to-end permanent molars would make the normal shift to Class I, and most probably they would stay end-to-end. If the Class II growth pattern was really severe, they could move to Class II. Transition to Class III would require a severe Class III growth pattern.
Incorrect
That’s incorrect. With a mild Class II growth pattern it is unlikely that the end-to-end permanent molars would make the normal shift to Class I, and most probably they would stay end-to-end. If the Class II growth pattern was really severe, they could move to Class II. Transition to Class III would require a severe Class III growth pattern.
Question 9
In a child with Class I permanent first molars at age 10 and a Class III growth pattern, what is the most likely molar relationship at age 12?
- Class I
- end-to-end
- Class II
- Class III ✓
Correct
That’s correct. With a Class III growth pattern, molars that were already Class I at age 10 (when many children with a normal growth pattern are still end-to-end) would be carried toward Class III, and that’s the most probable molar relation after 2 more years of Class III growth.
Incorrect
That’s wrong. With a Class III growth pattern, molars that were already Class I at age 10 (when many children with a normal growth pattern are still end-to-end) would be carried toward Class III, and that’s the most probable molar relation after 2 more years of Class III growth.
Question 10
(A) A Class I malocclusion rarely becomes a Class III malocclusion during growth because (B) a Class II growth pattern rarely occurs in a Class I patient.
- A true, B true, A and B related
- A true, B true, A and B not related ✓
- A true, B false
- A false, B true
- A false, B false
Correct
That’s right. Both statements are true but they’re not related. Class I rarely becomes Class III because Class III growth pattern rarely occurs in a Class I patient. A Class II growth pattern would turn Class I into Class II, not III.
Incorrect
That’s incorrect. Both statements are true but they’re not related. Class I rarely becomes Class III because Class III growth pattern rarely occurs in a Class I patient. A Class II growth pattern would turn Class I into Class II, not III.
Question 11
What is the chance that a child with a Class II skeletal pattern would spontaneously grow out of it and become Class I as an adult?
- less than 10% ✓
- 10-20%
- 20-40%
- about 50%
- totally unpredictable - no way to know
Correct
That’s right. Spontaneous correction of a skeletal Class II or Class III pattern rarely occurs. The general rule is “constancy of the pattern”, meaning that whatever the growth pattern is, it’s unlikely to change (but of course unlikely things do happen, they just don’t happen very often). The chance of spontaneous correction of a skeletal Class II or Class III is considerably less than 10%, in fact probably closer to 1%.
Incorrect
That’s wrong. Spontaneous correction of a skeletal Class II or Class III pattern rarely occurs. The general rule is “constancy of the pattern”, meaning that whatever the growth pattern is, it’s unlikely to change (but of course unlikely things do happen, they just don’t happen very often). The chance of spontaneous correction of a skeletal Class II or Class III is considerably less than 10%, in fact probably closer to 1%.
Question 12
(A) In a child with a skeletal open bite growth pattern, positive overbite can be present because (B) increased eruption of incisors would compensate for the open bite tendency.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A false, B false
Correct
That’s right, increased eruption of incisors could compensate for a skeletal open bite growth pattern, maintaining positive overbite even though the mandible was growing downward away from the maxilla.
Incorrect
That’s wrong. Increased eruption of incisors could compensate for a skeletal open bite growth pattern, maintaining positive overbite even though the mandible was growing downward away from the maxilla.