Introduction
Learning Objectives
Malocclusion is the result of a complex process of growth and development. For that reason, often it is difficult to precisely specify the cause. But it is important to understand the possible causes, and to know how specific events can influence the development of malocclusion.
The purpose of this program is to outline what is known about specific possible causes of malocclusion, and to put these specific causes in perspective. In a minority of the patients with severe malocclusion that you will meet in the future, you will be able to say that one of these causes was the etiology. In the majority, more than one of these causes may have played a role, so that the etiology would not be known clearly. Even so, you need to know what the possible causes might have been, and how important any of them might have been in your specific patient.
After viewing this program, you should be able to discuss the role of four major factors in the etiology of malocclusion and recognize the etiology of the clinical problem presented by patients affected by them:
- Hereditary factors
- Interference with normal development
- Trauma
- Disturbance in normal function
Effect of Malocclusion on Function
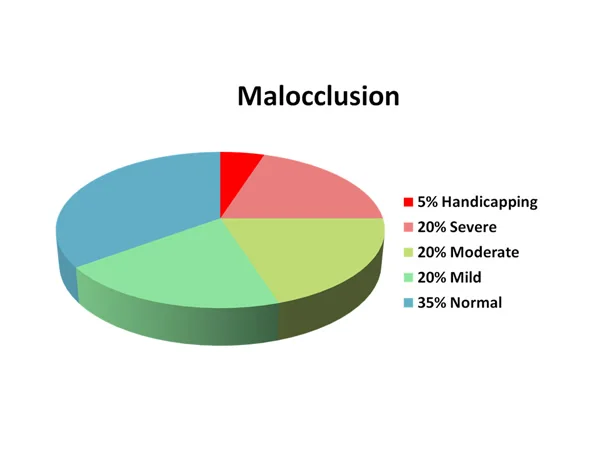
As we discussed in the first unit of this module, malocclusion is so prevalent in contemporary populations that only about 35% of the US population have occlusion that would be classified as normal. Another way to look at it is to consider the effect on function, both physiologic and social. In essence, this combines the functional and aesthetic IOTN grades that you learned about in a previous module.
The worst 5% of the population have a malocclusion so severe that they are handicapped in their ability to function both physiologically and socially. About 20% have a severe problem, another 20% are moderately affected, and another 20% are mildly affected.
The severe and handicapping problems usually have a skeletal component, that is, the position or size of the jaws makes it impossible for the teeth to fit together correctly even if the teeth are well aligned. Moderate and mild problems usually are just displacement of teeth relative to well-proportioned jaws.
Etiology: Overview
Malocclusion almost always is the result of a distortion of normal development, and it can be very difficult to precisely specify the cause.
As a result, the etiology of most malocclusions is not well understood. In some situations, however, we can identify a specific cause of malocclusion, and when that is possible it is important to do so. At present only about 5% of patients fall into that category (image 1).
The 5% with known etiology overlap with the 5% with handicapping malocclusion, but they are not exactly the same group (image 2). A known etiology does not necessarily produce a handicapping problem.
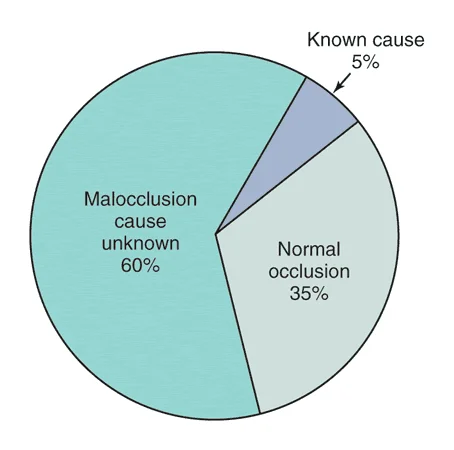 image 1: US population percentages for known / unknown etiology of malocclusion. image 1: US population percentages for known / unknown etiology of malocclusion. | 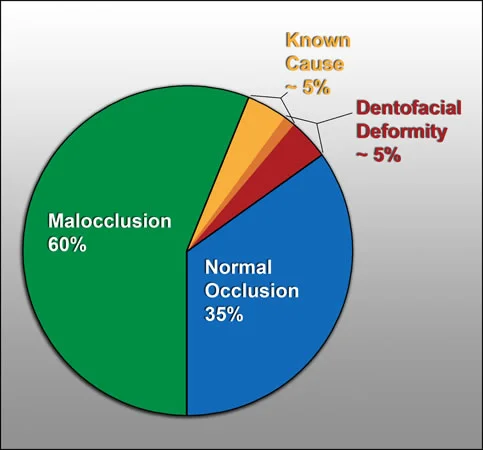 image 2: For some patients with a handicapping malocclusion, the cause is known. For most, there is no single known cause. Does the 5% overlap between known cause and handicapping malocclusion mean it’s 2.5% each. No—it’s not that simple. image 2: For some patients with a handicapping malocclusion, the cause is known. For most, there is no single known cause. Does the 5% overlap between known cause and handicapping malocclusion mean it’s 2.5% each. No—it’s not that simple. |
Interaction Between Genetic and Environmental Influences
For the patients whose malocclusion cannot be attributed to a specific cause, a complex interaction between genetic and environmental factors is involved.
As progress is made in future years, it should become possible to specify more clearly both the genetic or environmental factors and how they interact. In turn, that would greatly improve our ability to predict the outcome and stability of treatment.
Let’s examine some possible specific causes, beginning with hereditary factors.
Hereditary Factors
Evolution?
Certainly it is possible that inheritance of mismatched teeth and jaws could be a major cause of malocclusion, and at one time most malocclusion was thought to be related genetically determined.
Under primitive conditions where populations were genetically quite homogenous and presumably everyone carried the same information for tooth size and jaw size, malocclusion occurred but was much less prevalent than it is now.
In image 1, note the excellent alignment of teeth in this jaw fragment from 100,000 years ago, which is typical of skeletal remains from times up until quite recently. Crowding and malalignment did occur long ago, however (image 2). This individual had the largest teeth of any of the 80 specimens from the same source as image 1.
 Fig. 1: Well-aligned teeth are observed in most jaws taken from ancient archeologic excavations. Fig. 1: Well-aligned teeth are observed in most jaws taken from ancient archeologic excavations. | 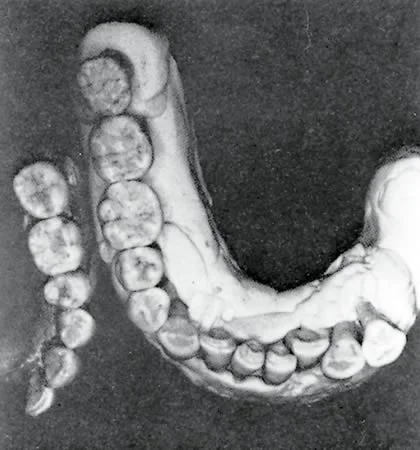 Fig. 2: Irregular teeth in an ancient jaw fragment—so this problem did occur at that time. Fig. 2: Irregular teeth in an ancient jaw fragment—so this problem did occur at that time. |
Evolution? (cont.)
There are several possible causes for increased malocclusion that could relate to changes over a long period of time.
An interesting one is the evolutionary trend toward a decrease in the size of the jaws and the individual teeth, as well as a decrease in the number of teeth. If the reduction in the size of the jaws did not match the reduction in tooth size and number, then malocclusion probably would be the result.
Note the decrease in the size of human teeth from the Qafzeh anthropological site 100,000 years ago, to Neanderthal man 10,000 years ago, to a modern (English) population (image 1).
In image 2, look at how the number of teeth decreases as we follow the primate evolutionary path from basic mammalian to man. Four premolars and three incisors per side has been reduced to two premolars and two incisors. In man, third molars are so often missing now that the trend toward only two molars is apparent, and upper second (lateral) incisors and both upper and lower second premolars seem to be under some pressure.
Over the same time span, jaws also have been reduced in size.
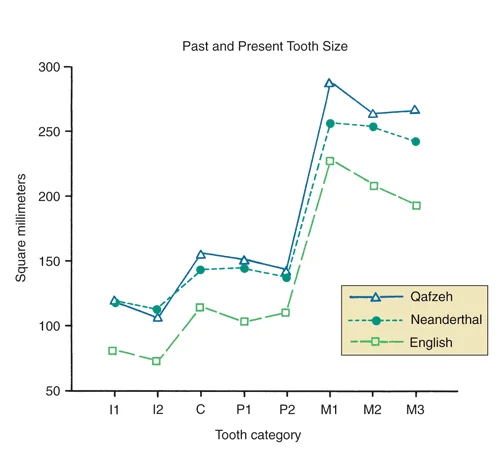 Image 1: Tooth sizes 100,000 years ago (Qafzeh), 10,000 years ago (Neanderthal), and recently. Image 1: Tooth sizes 100,000 years ago (Qafzeh), 10,000 years ago (Neanderthal), and recently. | 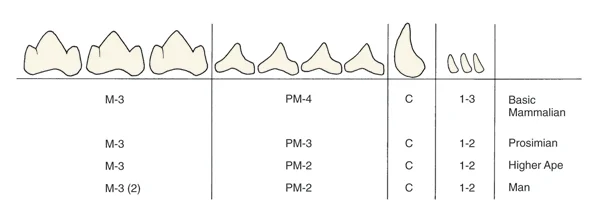 Image 2: Note that man has fewer premolars and incisors than his basic mammalian precursors—and it is obvious that the human third molar is on the way out, because so many people now are congenitally missing these teeth. Image 2: Note that man has fewer premolars and incisors than his basic mammalian precursors—and it is obvious that the human third molar is on the way out, because so many people now are congenitally missing these teeth. |
Genetic Drift
However, this slow genetic drift over many generations and tens of thousands of years cannot explain the recent increase in malocclusion.
It has been only in the last thousand years, perhaps even less, that significant human malocclusion has appeared on the scene, and there simply has not been enough time for evolutionary pressures to act. You could argue that malocclusion has appeared along with urbanization and population growth.
We know of other “diseases of civilization” that have appeared on the same timetable, atherosclerotic heart disease being a prominent example. Is there something about the development of civilization that could contribute to the inherited aspects of malocclusion? Although recent research has shown that the expression of genes can change more quickly than was previously believed, this explains only a small amount, if any, of the recent increase in malocclusion. A recent sensationalist book called “Jaws” says the whole cause of malocclusion is decreased biting force that leads to small jaws, but that makes no sense in the context of major change in so few years—and in fact the jaws of 500 years ago are the same size as they are now.
Hereditary Factors: Outbreeding?
Some day as you point out a child’s deficient chin and tell mother that’s why his upper teeth protrude, she’ll say “But he looks just like his father”.
We have all observed familial tendencies in facial features, and there is no doubt that jaw proportions leading to malocclusion can be passed on from one generation to the next.
Could the recent increase in malocclusion be the result of greater problems because mother’s small jaws matched up with dad’s large teeth, or the child inherited dad’s large upper jaw and mom’s small lower jaw? You could argue that malocclusion should be one result of marriage between different racial and ethnic groups.
Indeed, the US is proud to be a genetic melting pot (and the fact that people from different racial backgrounds come together is good), and we also have one of the highest rates of malocclusion in the world. Modern mobility has created a much more heterogenous gene pool than primitive populations had. Does that mean that the child of parents of different racial backgrounds (i.e. those who were previously geographically separated) is at greater risk of severe malocclusion? No, it’s not that simple.

Hereditary Factors: Outbreeding? (cont.)
Observation of the effects of outbreeding indicate that there are no independently inherited tooth and jaw characteristics that could produce malocclusion when mixed. It’s simply not the case that dental characteristics and jaw characteristics are inherited independently.
Although it’s attractive to think that kids can inherit mom’s jaws and dad’s teeth, it doesn’t work that way. Multiple gene effects and linkage between characteristics keep it from being so simple.
Let’s look at some of the evidence for that contention.
Heriditary Factors: Animal Experiments
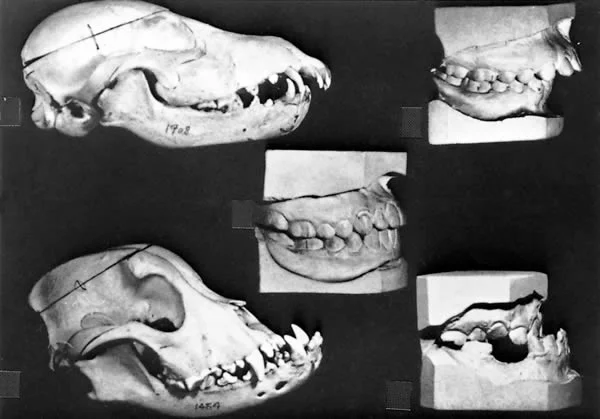
The temptation to blame malocclusion on mixing mom’s jaws and dad’s teeth, or mom’s upper jaw with dad’s lower jaw, was reinforced at first by the results of breeding experiments with dogs.
Crossing various breeds of dogs resulted in striking dentofacial malformations that seemed analogous to human malocclusions, and this illustration from an influential textbook published in 1941 makes the connection explicit. If you cross a small breed of dog with a large one, you can get jaw combinations that look a lot like human Class II or Class III jaw relationships.
Hereditary Factors: Animal Experiments (cont.)
What the early researchers didn’t realize, however, is that many of the involved breeds of dogs carry the gene for achondroplasia.
You will remember from Level 1 that this condition is characterized by deficient growth of primary cartilage, which causes midface deficiency and short limbs. It’s a dominant trait with variable penetrance in dogs. If you cross a Bassett hound like the one shown here, who is quite achondroplastic, with another breed of dog (a collie, for instance) who isn’t achondroplastic, you’re likely to get strangely-proportioned puppies with a malocclusion, but it turns out that the malocclusions are not a true reflection of the mixing of various dentofacial characteristics. Instead, this reflects the variable penetrance of achondroplasia.

Hereditary Factors: Human Data
If breeding experiments in dogs are not a good model, why not look directly at humans?
Chung et. al. did just that by conducting a study of the prevalence of malocclusion in Hawaii, whose population probably shows the greatest degree of interracial mixing in the world.
What they found was that interracial mixes do not produce a major increase in malocclusion. Severe malocclusions are no more frequent in Hawaii than anywhere else, and no extreme combinations of parental characteristics are observed.
So, tempting as it might be, we really can’t blame the recent increase in malocclusion on interbreeding among different human groups.
Hereditary Factors: Familial Characteristics
Nevertheless, children tend to look like their parents. Studying family members by observing similarities between parent and child and between siblings can provide a clue as to the amount of genetic influence on malocclusion.
Among family members, the correlation is higher for skeletal than for dental characteristics, which seems reasonable since tooth position should be more easily changed by environmental influences like habits.
Occasionally, inheritance of a specific pattern of malocclusion is observed. The most apparent is the familial tendency toward mandibular prognathism, well documented in many circumstances including the Hapsburgs, the European royal family.Note the very prominent chins of the members of the Spanish royal family over a period of more than 200 years. But most types of malocclusion aren’t inherited within families in that clear-cut way.
 Image 1: Phillip II and Prince Ferdinand, 1575 Image 1: Phillip II and Prince Ferdinand, 1575 |  Image 2: Phillip IV, 1638 Image 2: Phillip IV, 1638 |
 Image 3: Charles IV, 1800. Note that his mother on the left has a strong chin, and so does his infant son. But his wife (right) has normal facial proportions. Image 3: Charles IV, 1800. Note that his mother on the left has a strong chin, and so does his infant son. But his wife (right) has normal facial proportions. |
Twin Studies
To separate genetic from environmental contributions to a malocclusion, researchers have looked at twins. Since identical twins share essentially the same DNA composition, differences between them are thought to be mostly of environmental origin, while differences in fraternal twins who share only part of their DNA can be of genetic or environmental origin. Comparing identical vs. fraternal twins gives a way to estimate how much variation is hereditary and how much is environmental.
At age 11, as you would expect, these identical twins have remarkably similar facial proportions (images 1 and 2). They’re distinguishing themselves by having different hair styles and clothes. They show a finding, however, that illustrates the extent to which genetic controls affect things that you might think were just random variation. Almost always during the transition from the mixed to the permanent dentition, there is a left-right asymmetry, with the teeth on one side erupting a little ahead of those on the other side. In identical twins, the dental arches will be a mirror image at that point—the teeth on one side ahead in one of the twins, the other side ahead in the other.
Note that for Tom, the maxillary right canine is erupting ahead of the maxillary left one, while for Chris the reverse is true (images 3 and 4). The photos of both boys were made on the same day.
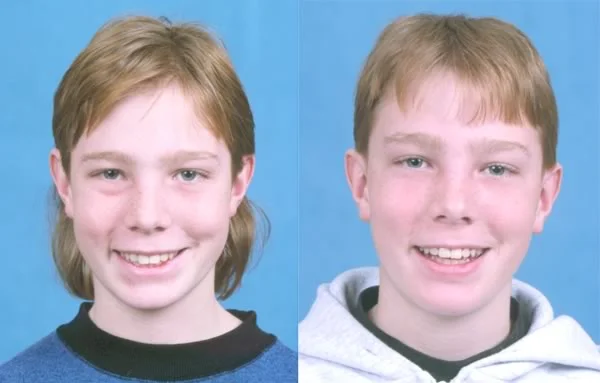 Image 1: Identical twins, Tom (left) and Chris (right), age 11 Image 1: Identical twins, Tom (left) and Chris (right), age 11 |  Image 2: Identical twins, Tom (left) and Chris (right), age 11 Image 2: Identical twins, Tom (left) and Chris (right), age 11 |
 Image 3: Note that on the right side Tom’s teeth are further along in eruption that Chris’ teeth. Image 3: Note that on the right side Tom’s teeth are further along in eruption that Chris’ teeth. |  Image 4: On the left side it’s the reverse, Chris ahead of Tom. Image 4: On the left side it’s the reverse, Chris ahead of Tom. |
Twin Studies (cont.)
The proportion of variation in a given characteristic that is attributed to genetic rather than environmental factors is called heritability.
Twin studies are, indeed, useful in estimating heritability of traits which is expressed as a quotient that varies from 1 to 0. If the heritability quotient is 1, then 100% of the variability in the trait is due to genetic influences. Conversely, if the heritability is zero, then variation in the trait is purely due to environmental influences.
One of the problems with twin studies is that they’re usually living in the same family at the same time, and therefore they have a very similar environment as well as similar genomes. It’s important in twin studies to try to control for similar environments because it places the subjects under similar non-genetic influences.
Contribution of Hereditability to Malocclusion
There are currently opposing views on the contribution of heritability to malocclusion.
One end of the spectrum is occupied by Lundstrom, a well known European orthodontic professor who reviewed his years of research in this area in the 1980’s. The other end is represented well by Corrucini, a professor of physical anthropology who worked with the geneticist Rose Potter at the University of Indiana in the 1990s.
By comparing dentofacial variables in identical twins, especially skeletal and dental overjet, Lundstrom concluded that up to 50% of malocclusions have their origin in hereditary factors. Corrucini and Potter, using a different statistical approach to the same material, came up with essentially no genetic contribution at all. Each group questions the other’s methodology, especially how well they controlled for similarity of environment.
But the data indicate that 50% may be the maximum contribution to malocclusion by hereditary factors, and that the environmental contribution is likely to be significantly higher than the genetic one. The skeletal component of malocclusion seems more influenced by heredity than the dental component—you’re more likely to inherit mismatched jaws than crooked teeth.
Interferences with Pre-Natal Development
Interferences During Pre-Natal Development: FAS
What are the environmental influences that can cause malocclusion? In this sense, everything that isn’t clearly genetic is environmental, which means that there are many possible environmental factors.
One clear-cut example of facial distortion and malocclusion due to interference with normal development during embryonic life is the fetal alcohol syndrome (FAS). Exposure to high levels of alcohol during the first trimester of pregnancy (often, before the mother knows she’s pregnant) produces the characteristic facial features of FAS.
Compare the drawing of the FAS facial features (image 1) with the face of this 7-year-old boy (image 2). The child’s problems, of course, are much bigger than his facial appearance. Mental retardation and decreased neuromuscular coordination are common.
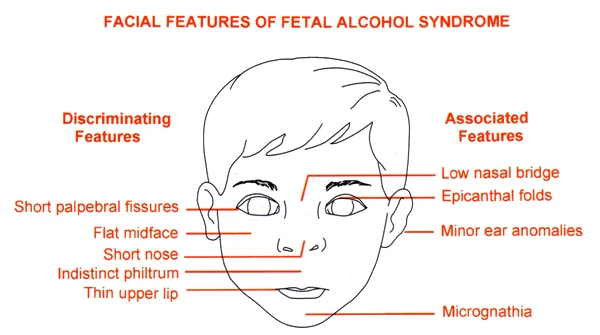 Image 1: FAS facial features Image 1: FAS facial features |  Image 2: Fetal Alcohol Syndrome in a 7-year old boy Image 2: Fetal Alcohol Syndrome in a 7-year old boy |
Craniofacial Microsomia
Another example of interference with normal growth during embryologic life is craniofacial microsomia (formerly referred to as “hemifacial microsomia”), which is caused by early loss of neural crest cells at the stage of origin and migration.
The result is a characteristic underdevelopment of the affected side of the face, as seen in the facial views of this girl who is only mildly affected (images 1 and 2). In a more severely affected child, the ramus of the mandible and the TM joint area may be missing (image 3).
 Image 1: 12-year-old girl with craniofacial microsomia. Note the underdevelopment of the left side of the face. Image 1: 12-year-old girl with craniofacial microsomia. Note the underdevelopment of the left side of the face. |  Image 2: Moderate distortion of the left ear is present. Image 2: Moderate distortion of the left ear is present. |
 Image 3: CT image of a patient with severe craniofacial microsomia shows the loss of hard and soft tissue in the area of the TM joint. Image 3: CT image of a patient with severe craniofacial microsomia shows the loss of hard and soft tissue in the area of the TM joint. |
Intra-Uterine Molding
Pressure against the developing face can significantly interfere with normal development. Image 1 shows the severe maxillary deficiency in a young girl that was produced by a forearm positioned across the mid-face during intra-uterine development.
Pressure against the lower jaw because the head is flexed tightly against the chest produces extreme mandibular deficiency at birth. This occurs when there is a deficiency in the volume of amniotic fluid, which can arise from multiple causes. The condition is called the Pierre Robin sequence or anomolad. When the pressure against the mandible is released after birth, some affected children have normal growth and a complete or nearly complete recovery, while in others the mandible never catches up (image 2).
 Image 1: Mid-face deficiency from mechanical interference with intra-uterine development of the mid-face Image 1: Mid-face deficiency from mechanical interference with intra-uterine development of the mid-face |  Image 2: Severe mandibular deficiency from the Pierre Robin sequence Image 2: Severe mandibular deficiency from the Pierre Robin sequence |
Pre-Natal Interferences with the Dentition
While disturbances of embryologic development are unlikely to produce skeletal malocclusions without any other associated defects, pre-natal disturbances of dental development frequently occur as isolated defects. These can contribute to Class I malocclusions where jaw size and proportions are normal but the teeth are malaligned and irregular.
The best examples are supernumerary (extra) teeth, congenitally missing teeth and distortions of tooth form. An extra tooth occurs relatively frequently in modern populations. The most frequent location is in the maxillary midline, and a supernumerary tooth in that location is called a mesiodens (images 1, 2). Its presence either keeps the maxillary central incisors from erupting, or displaces them to produce an obvious and unsightly malocclusion. Two, or perhaps three, supernumeraries occasionally occur in otherwise-normal children. A supernumerary tooth bud sometimes fuses with the developing crown of a normal tooth, distorting it (images 3 and 4).
Multiple supernumerary teeth are unlikely in children who are not affected by some congenital syndrome, but are a characteristic of cleidocranial dysplasia (image 5).
 Image 1: Midline supernumerary (mesiodens) Image 1: Midline supernumerary (mesiodens) | 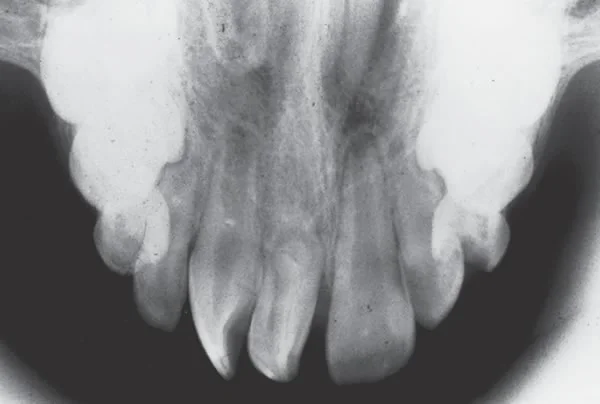 Image 2: Radiographic view of mesiodens Image 2: Radiographic view of mesiodens |
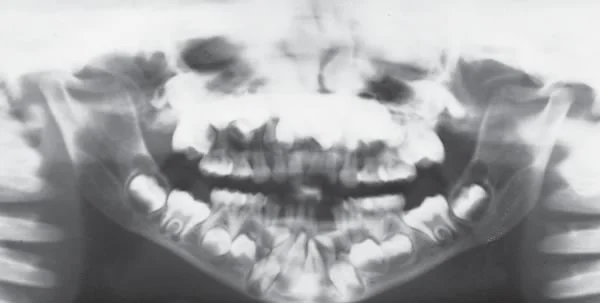 Image 3: Multiple supernumerary teeth in a child with cleidocranial dyslpasia Image 3: Multiple supernumerary teeth in a child with cleidocranial dyslpasia |  Image 4: Note the distortion of the lower right 2nd molar, which fused with a supernumerary tooth at an early stage of development Image 4: Note the distortion of the lower right 2nd molar, which fused with a supernumerary tooth at an early stage of development |
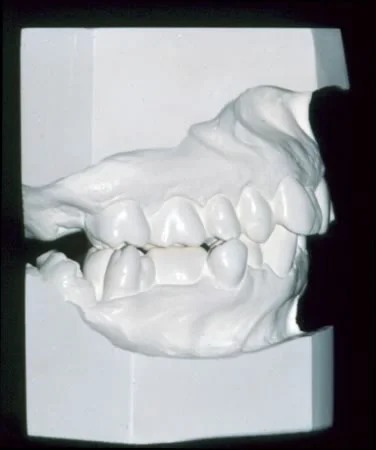 Image 5: Lateral view of distorted lower 2nd molar Image 5: Lateral view of distorted lower 2nd molar |
Pre-Natal Interferences with the Dentition (cont.)
A congenitally missing tooth or teeth also occurs relatively frequently, with the maxillary lateral incisors and/or mandibular 2nd premolars most likely to be affected (but any tooth can be missing in an otherwise-normal individual).
Multiple congenitally missing teeth, like multiple supernumeraries, usually occur only in children with a syndrome of some type. One frequent cause of multiple missing teeth is ectodermal dysplasia, which should be suspected when a patient with a dentition like this one is seen, even if the diagnosis has not previously been made.

Birth Injuries (?)
An injury during birth that leads to interference with growth is possible, but this is the cause of a facial anomaly only rarely—though many parents are convinced that if something is wrong with their child’s face, a birth injury was the cause. As the family dentist, you may have to explain that no matter how convinced the parents are that a birth injury occurred, craniofacial microsomia, severe mandibular deficiency or a malformed incisor was present long before birth and was not caused by something that happened at that time.
Trauma as an Interference with Post-Natal Development
Soft Tissue vs Hard Tissue Injuries
The effect of trauma to the face and jaws as a cause of malocclusion is understood best from the perspective of the functional matrix theory of growth. In most instances, facial growth is affected more by the extent and healing of facial and soft tissue injuries than the amount of hard tissue injury. In particular, scarring of the soft tissues around the facial skeleton and dentition can have marked effects on bone growth and tooth positions.
The unfortunate boy seen in images 1 and 2 experienced trauma to his mid-face in an automobile accident in early childhood, and his severe maxillary deficiency in adolescence is a direct result of the scarring of soft tissues that prevented the normal downward-forward growth of the naso-maxillary area. The deformity became progressively worse as the affected areas did not grow and the adjacent areas did. Surgery to reposition his jaws improved his situation, but the soft tissue scarring could not be completely corrected (images 3 and 4). Fractures of the nose and maxilla usually do not produce this much effect on growth, and in fact may have very little effect—if extensive soft tissue scarring did not occur.
 Image 1: Frontal view, mid-face deficiency 8 years after an automobile accident with maxillary fractures and soft tissue injuries Image 1: Frontal view, mid-face deficiency 8 years after an automobile accident with maxillary fractures and soft tissue injuries |  Image 2: Profile view shows the marked mid-face deficiency, created by scarring that prevented the normal downward-forward growth of the maxilla that should have matched the mandibular growth. Image 2: Profile view shows the marked mid-face deficiency, created by scarring that prevented the normal downward-forward growth of the maxilla that should have matched the mandibular growth. |
 Image 3: Frontal views before / after surgery to move the maxilla down and forward, and reconstruct the nasal bridge Image 3: Frontal views before / after surgery to move the maxilla down and forward, and reconstruct the nasal bridge |  Image 4: Profile view before / after surgery. Note the major advancement of the mid-face and projection of the bridge of the nose. Image 4: Profile view before / after surgery. Note the major advancement of the mid-face and projection of the bridge of the nose. |
Soft Tissue vs Hard Tissue Injuries (cont.)
At age 4, this boy fell from a tractor that then ran over his head. Although the soft ground helped, he had almost too many fractures to count (image 1), but after a month in critical condition, he survived. At that point forward traction in the orthodontic clinic succeeded in moving his displaced maxilla forward 3-4 mm (image 2), and no further treatment was done.
When he returned to the orthodontic department at age 12, the healing of the fractures and the extent of normal growth was remarkable (images 3, 4, 5). In his case, despite the severity of the hard tissue injuries, extensive scarring of the soft tissues did not occur. If you didn’t know his history, you wouldn’t believe that he had experienced trauma of that extent.
He’s an exellent example of how facial growth can continue reasonably normally in the absence of soft tissue scarring.
 Image 1: Facial x-ray post-injury, showing the extensive fracturing of facial bones Image 1: Facial x-ray post-injury, showing the extensive fracturing of facial bones |  Image 2: After his survival was no longer in doubt 2 months later, the maxilla still was displaced posteriorly. Image 2: After his survival was no longer in doubt 2 months later, the maxilla still was displaced posteriorly. |
 Image 3: At 2-4 months post-injury, a facemask (reverse pull headgear) to a splint over the maxillary arch was used to move the maxilla forward 3-4 mm. No other orthodontic treatment was done after that. Image 3: At 2-4 months post-injury, a facemask (reverse pull headgear) to a splint over the maxillary arch was used to move the maxilla forward 3-4 mm. No other orthodontic treatment was done after that. |  Image 4: Age 12. Note the normal facial proportions and jaw relationships. Image 4: Age 12. Note the normal facial proportions and jaw relationships. |
 Image 5: Age 12. The teeth were mildly crowded and irregular, but the malocclusion was only moderately severe. Image 5: Age 12. The teeth were mildly crowded and irregular, but the malocclusion was only moderately severe. |
Soft Tissue vs Hard Tissue Injuries (cont.)
You already know that after a fracture of the condylar process of the mandible, there is a 75% chance of normal growth, and a 25% chance that an asymmetry will develop due to an interference with growth. What’s the difference between the children who subsequently grow normally and those who do not? That’s right, it’s largely whether there was enough soft tissue injury to create scarring around the TM joint that inhibited translation of the mandible as facial growth continued.
 Image 1: Mandibular asymmetry following fracture of the condylar process several years previously Image 1: Mandibular asymmetry following fracture of the condylar process several years previously |  Image 2: The asymmetric mandibular deficiency is the result of soft tissue trauma that eventually restricted mandibular growth. Image 2: The asymmetric mandibular deficiency is the result of soft tissue trauma that eventually restricted mandibular growth. |
Effects of Trauma on the Dentition
If a young child crawling around on the floor bites down on an electrical cord, the result is likely to be a severe burn at the corner of the mouth, as in the girl shown in image 1. As it heals and scars down, pressure against the teeth creates a marked asymmetry in the mandibular dental arch, and makes normal arch form almost impossible to maintain.
The reverse effect is seen when cheek tissues are lost (image 2). Then unopposed pressure by the tongue tips the teeth facially.
In both cases, the soft tissue injury led directly to displacement of the teeth.
 Image 1: Scarring as this burn heals will distort dental arch form Image 1: Scarring as this burn heals will distort dental arch form |  Image 2: Loss of cheek tissue to a tropical infection has led to buccal displacement of the teeth Image 2: Loss of cheek tissue to a tropical infection has led to buccal displacement of the teeth |
Effects of Trauma on the Dentition (cont.)
Direct trauma to the teeth also can lead to malocclusion. If a tooth is lost, the adjacent teeth will tend to drift into its space, and normal alignment and position of the teeth will be lost unless the space is maintained until the lost tooth is replaced. Premature loss of a primary tooth can lead to loss of space for its permanent successor. Loss of a permanent tooth has the same potential for the development of malocclusion.
If a tooth is displaced but not lost as a result of trauma (image 1), the extent of soft tissue injury again becomes a key factor in the long-term outcome. In this situation the soft tissue is the periodontal ligament. If it is severely damaged, the displaced tooth will become ankylosed as the cementum of the root fuses with the alveolar bone. Then neither further eruption of the tooth nor orthodontic tooth movement is possible.
If the PDL is not severely injured, abnormal development of the root (dilaceration) can occur (image 2), but a tooth with a dilacerated root can continue to erupt and may end up in normal position in the dental arch. A displaced tooth with an intact PDL can be moved orthodontically if necessary (image 3).
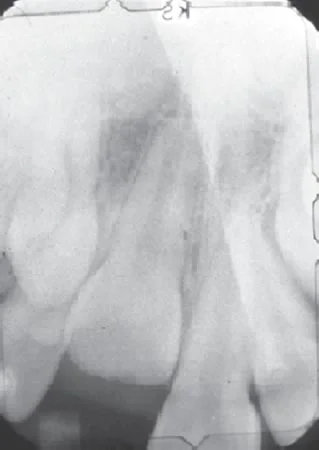 Image 1: Displacement of a central incisor from trauma. Ankylosis is likely with this amount of displacement; if the tooth is to be repositioned orthodontically, this must be done soon after the injury. Image 1: Displacement of a central incisor from trauma. Ankylosis is likely with this amount of displacement; if the tooth is to be repositioned orthodontically, this must be done soon after the injury. |  Image 2: Distortion of the root of this lateral incisor resulted from trauma at an earlier age that displaced the crown of the tooth relative to the developing root. Image 2: Distortion of the root of this lateral incisor resulted from trauma at an earlier age that displaced the crown of the tooth relative to the developing root. |
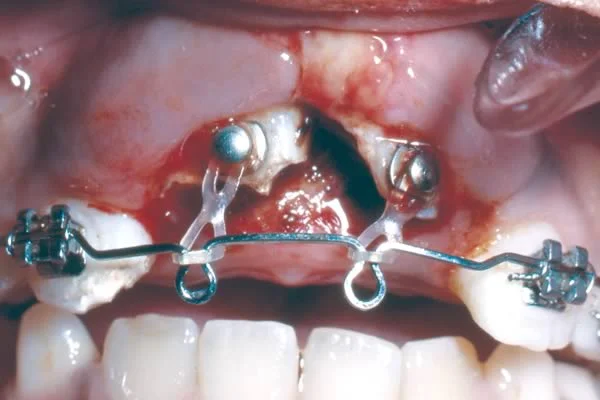 Image 3: Bringing displaced teeth back into the dental arch can be done with orthodontic tooth movement (if the PDL is intact). Image 3: Bringing displaced teeth back into the dental arch can be done with orthodontic tooth movement (if the PDL is intact). |
Disturbance in Normal Function
Habits: Thumbsucking
The final specific potential cause for the development of malocclusion is a disturbance in function.
The dentition is always subject to forces from its environment, such as masticatory forces or pressure from cheeks, lips and tongue just resting against the teeth. Yet tooth position in most people is stable, which indicates that these forces must be somehow in balance or equilibrium. How could normal function be disrupted to result in malocclusion?
One of the more obvious examples of interference with normal function is a thumb habit. Most likely, you have already seen a thumbsucking child who shows the classic side effects of this habit: protruding upper incisors, anterior open bite, and maxillary constriction causing the child to shift into a unilateral posterior crossbite. For the child in image 2 (not the same one as image 1), you can see just where he places the thumb between the teeth.
 Image 1: Thumbsucking child Image 1: Thumbsucking child |  Image 2: For this thumbsucker, it’s obvious where the thumb goes. Image 2: For this thumbsucker, it’s obvious where the thumb goes. |
Habits: Thumbsucking (cont.)
Let’s look more carefully at what thumbsucking does, and how it does it. Why are protruding upper incisors often seen in a thumbsucker? The answer is that the child often puts upward-forward pressure on the upper teeth. If the sucking habit is maintained for enough hours each day, this can displace the teeth and even lead to more forward growth of the upper jaw.
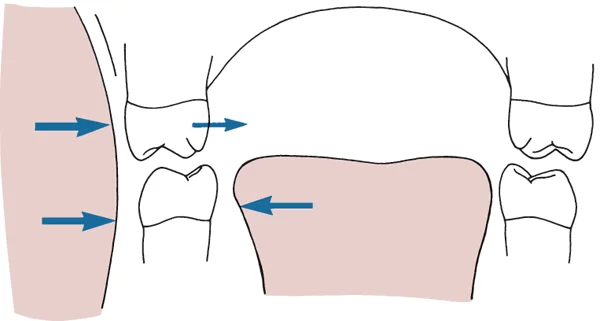
Images 1 and 2 show identical twins, one of whom sucked his thumb but the other did not. In the dental casts you can see the increased overjet in the thumbsucker, with protrusion of the upper incisors. In the superimposed cephalometric tracings, note the remarkable similarity of the cranial and facial structures. This is characteristic for identical twins, and would not be seen in any other pair of individuals. For this thumbsucking child, the effect was a little more forward growth of the maxilla and major protrusion of the upper incisors. Unlike what happened in this child, the position of both the upper and lower incisors often is affected by thumbsucking: the lower incisors are likely to be displaced lingually as the upper incisors are tipped facially.
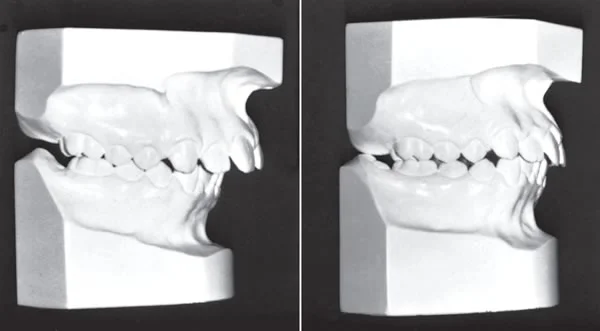 Image 1: Dental casts of identical twins with those of the thumb-sucker on the left. Image 1: Dental casts of identical twins with those of the thumb-sucker on the left. | 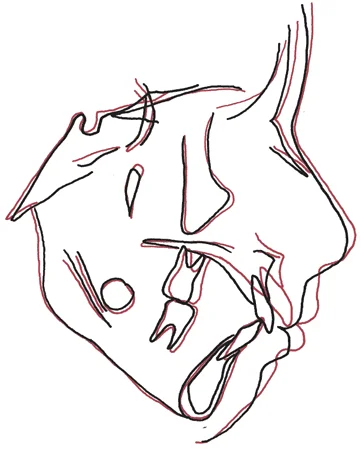 Image 2: Cephalometric tracings of the same twins shown above, superimposed on the cranial base, with the thumbsucker in red. Image 2: Cephalometric tracings of the same twins shown above, superimposed on the cranial base, with the thumbsucker in red. |
Thumbsucking Effect on Arch Width
Probably it’s not obvious to you how thumbsucking could lead to a narrower, V-shaped maxillary arch. This is due to two related factors: increased pressure against the teeth as the cheeks are tightened during sucking, and a lowered tongue posture.
This diagrammatic representation shows how the pressure balance against the teeth is altered during sucking, as cheek pressure increases while the tongue is displaced downward. The effect is a lingual movement of the upper but not the lower teeth, which are stabilized by the tongue. The change toward a V-shaped maxillary arch form occurs because the cheek pressure is highest at the corners of the mouth, so the canines (and first premolars to a lesser extent) are displaced lingually more than the posterior teeth.
Other Oral Habits? Tongue Thrusting? Mouth Breathing?
Although thumbsucking is a clear-cut cause of malocclusion, some other “oral habits” are not. It is easy to conclude that if pressure from a thumb can displace maxillary incisors upward and forward, pressure from the tongue could do the same thing. A “tongue thrust swallow habit” often is blamed for the maintenance or worsening of a malocclusion that relates back to thumbsucking. In these patients, the position of the tongue probably is more an adaptation to the position of the teeth than the cause of their displacement. As you are going to learn in more detail, teeth are displaced by light force of long duration, not by intermittent force like the brief contact of the tongue with the teeth during swallowing.
Mouth breathing because of nasal obstruction also often is considered the cause of open bite, long face malocclusions. There is evidence that in some cases, nasal obstruction is an etiologic factor—but in other patients with the same dental and skeletal morphology, it is not.
The question of the etiology of malocclusion in these situations is difficult, and the answer is complex. This can be understood best in the context of equilibrium between opposing soft tissue pressures as they affect jaw position and tooth position, We have already noted some equilibrium effects, and equilibrium theory will be the subject of the teaching module that follows this one.
Summary
Summary, Inherited Tendencies
Let’s summarize what we have learned about inherited tendencies toward malocclusion:
- Neither genetic drift during evolution nor increased outbreeding explains the recent increase in malocclusion.
- Certain types of malocclusion, especially Class III mandibular prognathism, seem to be inherited—but most are not.
- The heritability of jaw relationships and malocclusion characteristics is not more than 50% and probably less. Heredity can explain some malocclusions, but it cannot explain all or even most of them.
Summary, Interferences with Pre-Natal Development
Interferences with pre-natal development as specific causes of malocclusion include:
Facial Development
- Fetal alcohol syndrome
- Hemifacial microsomia
- Intra-uterine molding
The first two interferences occur early in the first trimester of pregnancy. Alcohol is the most frequent, but not the only drug that can produce problems during the critical events of early stages of development.
Craniofacial microsomia is an example of an accident in development that is not due to an external agent, and is not the only mis-step in development that can affect the face.
Intra-uterine molding, in contrast, affects the growth that occurs in the third trimester. It has an environmental, not a heritable etiology—even though the problem arose before birth.
Dental Development
- Supernumerary teeth
- Congenitally missing teeth
- Fusion of tooth buds
These problems arise at the stage when the dental lamina is formed, late in the first trimester of pregnancy. Can they be due to external influences like drugs? Certainly some drugs, like tetracycline, can affect mineralization, but most problems of dental development do not seem to be due to the intra-uterine environment.
Summary, Interferences with Post-Natal Development
Facial Development
- Facial trauma
- Condylar fracture
The effects of trauma on growth are due much more to the extent of soft tissue injury than the direct injury to the jaws, because the formation of scar tissue that restricts growth of the bones is the key element in affecting post-injury growth.
Dental Development
- Tooth loss
- Tooth displacement: ankylosis?
- Dilaceration
Tooth loss leads to failure of development of alveolar bone. Ankylosis and dilaceration can be considered a reflection of injury to the periodontal ligament, so soft tissue injury is also a factor in problems of dental development.
Disturbance in Function
- Sucking habits
- Other habits?
How much pressure does it take to affect jaw growth and tooth eruption, and how much of the time does it have to be applied to have an effect? We will consider those important questions in the next module.
Referral to Self-Test
Before you proceed to the self-test, be sure to do the assigned reading in Contemporary Orthodontics (5th ed., pages 122-133; 6th ed., pages ). Then use the self-test as a guide to further study. If you didn’t get all the questions right, be sure you understand why you were incorrect.
Self-Test
Question 1
What is the most frequent location for a supernumerary tooth?
- Maxillary midline ✓
- Maxillary lateral incisor area
- Maxillary posterior quadrants
- Mandibular anterior area
- Mandibular posterior area
Correct
That’s right, a supernumerary tooth can appear almost anywhere, but this occurs most frequently in the maxillary midline. A tooth in that location is called a mesiodens.
Incorrect
No, that’s wrong. A supernumerary tooth can appear almost anywhere, but this occurs most frequently in the maxillary midline. A tooth in that location is called a mesiodens.
Question 2
What has happened to the number and size of teeth during primate evolution?
- both have decreased ✓
- size has decreased but number has remained the same
- number has decreased but size has remained the same
- in the human lineage, both have stayed the same
Correct
That’s correct. Both the number and size of the teeth have decreased. At present, the variability and frequent absence of third molars and upper lateral incisors suggests that from an evolutionary perspective, these teeth may be on their way out.
Incorrect
No, that’s wrong. Both the number and size of the teeth have decreased. At present, the variability and frequent absence of third molars and upper lateral incisors suggests that from an evolutionary perspective, these teeth may be on their way out.
Question 3
(A) A scar of the lip after an injury is likely to lead to protrusion of the incisors because (B) the scar changes the pattern of soft tissue pressure against the incisor teeth.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true ✓
- A and B false
Correct
That’s right, the first statement is false but the second is true. A lip scar would tend to increase lip tightness and push the incisors lingually, not make them more protrusive.
Incorrect
No, that’s wrong. the first statement is false but the second is true. A lip scar would tend to increase lip tightness and upright the incisors, not make them more protrusive.
Question 4
Which of the following are characteristic of fetal alcohol syndrome, caused by exposure to high levels of alcohol during embryonic development?
- underdeveloped maxilla and midface
- Class III malocclusion
- long and abnormally shaped upper lip
- 1 only
- 1 and 2
- 1 and 3
- 2 and 3
- 1, 2, and 3 ✓
Correct
That’s right, all of these are facial characteristics of FAS. It leads to an underdeveloped maxilla and midface, Class III malocclusion, and a long and abnormally shaped upper lip.
Incorrect
No, that’s incorrect. All of these are facial characteristics of FAS. It leads to an underdeveloped maxilla and midface, Class III malocclusion, and a long and abnormally shaped upper lip.
Question 5
Which of the following types of malocclusion is most likely to be an inherited problem?
- severe incisor crowding
- maxillary and midface deficiency
- maxillary protrusion
- mandibular and chin deficiency
- mandibular and chin protrusion ✓
Correct
That’s correct. Mandibular protrusion (prognathism) has a strong inherited component, much more than the other conditions listed. The protruding “Hapsburg jaw” of the European royal family has persisted for hundreds of years, but mandibular prognathism is characteristic of many other families as well.
Incorrect
No, that’s incorrect. Mandibular protrusion (prognathism) has a strong inherited component, much more than the other conditions listed. The protruding “Hapsburg jaw” of the European royal family has persisted for hundreds of years, but mandibular prognathism is characteristic of many other families as well.
Question 6
(A) The highest rate of malocclusion is found in modern cities because (B) the mixture of populations in these genetic melting pots leads to inheritance of mismatched jaws and teeth.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false ✓
- A false, B true
- A and B false
Correct
That’s correct. The first statement is true but the second one is false, not the correct explanation. Independently inherited tooth and jaw characteristics do not account for the increase in malocclusion as populations have become more urban.
Incorrect
That’s wrong. The first statement is true but the second one is false, not the correct explanation. Independently inherited tooth and jaw characteristics do not account for the increase in malocclusion as populations have become more urban.
Question 7
Which of the following is not a possible outcome of trauma that displaces a primary maxillary central incisor at age 6?
- an enamel defect in the middle of the crown of the permanent central ✓
- dilaceration of the root of the permanent central
- drift and partial space closure when the primary tooth is lost and the permanent tooth fails to erupt
- ankylosis of the permanent central
Correct
That’s right. The other items are possible, but the crown of the permanent central has formed by age 6, so an enamel defect in the middle of the crown isn’t a possible outcome (although that could happen with trauma at an early age).
Incorrect
That’s wrong. The other items are possible, but the crown of the permanent central has formed by age 6, so an enamel defect in the middle of the crown isn’t a possible outcome (although that could happen with trauma at an early age).
Question 8
How strong is the relationship between ankylosis of a primary molar and the development of malocclusion?
- very strong, usually happens
- strong, often happens
- weak, rarely happens ✓
- not at all, never happens
Correct
That’s right, ankylosis of a primary molar rarely leads to the development of malocclusion, but sometimes a problem arises because of drift of the permanent teeth in the vicinity—so there’s a weak relationship.
Incorrect
No, that’s wrong, ankylosis of a primary molar rarely leads to the development of malocclusion, but sometimes a problem arises because of drift of the permanent teeth in the vicinity—so there’s a weak relationship.
Question 9
In modern urban populations, what percentage have such severe malocclusion that it can be considered handicapping?
- <0.5%
- 1%
- 5% ✓
- 10%
- 25%
Correct
That’s right, about 5% of modern urban populations have malocclusion that is considered handicapping because of its effect on normal function and/or social interactions.
Incorrect
No, that’s wrong. About 5% of modern urban populations have malocclusion that is considered handicapping because of its effect on normal function and/or social interactions.
Question 10
Which of the following conditions is most frequently associated with multiple congenitally missing teeth?
- fetal alcohol syndrome
- ectodermal dysplasia ✓
- cleft lip and palate
- hemifacial microsomia
- all are frequently associated with this problem
Correct
That’s right. Ectodermal dysplasis is so strongly associated with multiple congenitally missing teeth that a child who is missing most of the teeth should be evaluated for ectodermal dysplasia even if that diagnosis has not been made previously.
Incorrect
No, that’s wrong. Ectodermal dysplasis is so strongly associated with multiple congenitally missing teeth that a child who is missing most of the teeth should be diagnostically evaluated for ectodermal dysplasia even if that diagnosis has not been made previously. The other conditions are not characterized by multiple congenitally missing teeth.
Question 11
Modern research suggests that at least what percentage of malocclusion is due to environment rather than inherited factors?
- <10%
- 25%
- 50% ✓
- 75%
-
90%
Correct
That’s right, twin studies show that at least 50% of malocclusion cannot be explained by inherited factors, and some researchers suggest that the figure for environment causation is considerably higher.
Incorrect
No, that’s not the best answer. Twin studies show that at least 50% of malocclusion cannot be explained by inherited factors, and some researchers suggest that the figure for environment causation is considerably higher.
Question 12
What is the most likely cause of a unilateral posterior crossbite in a child?
- hereditary factors
- trauma to one condyle leading to reduced growth on that side
- overgrowth of the condyle on one side
- bilateral narrowing of the maxilla related to thumb sucking ✓
Correct
That’s right, the great majority of apparent unilateral crossbites in children are due to bilateral narrowing of the maxilla due to thumb sucking, and a functional shift so the teeth are in normal occlusion on one side and crossbite on the other.
Incorrect
That’s incorrect. The great majority of apparent unilateral crossbites in children are due to bilateral narrowing of the maxilla due to thumb sucking, and a functional shift so the teeth are in normal occlusion on one side and crossbite on the other.