Overview
Definition of Orthodontic Problem
In modern health care, diagnosis and treatment planning is built around the problem-oriented approach. The question in diagnosis is: “What is the problem?” Its answer is a description of the problem and its cause. The question in treatment planning, of course, is what to do about it.
The problem-oriented approach to orthodontics is particularly valuable because it forces the doctor to focus on what difference it makes to the patient if the teeth aren’t correctly aligned or if the occlusion is imperfect. The evolution of thoughts about the goal of orthodontic treatment is covered in some detail in the module titled “Why Orthodontics?”
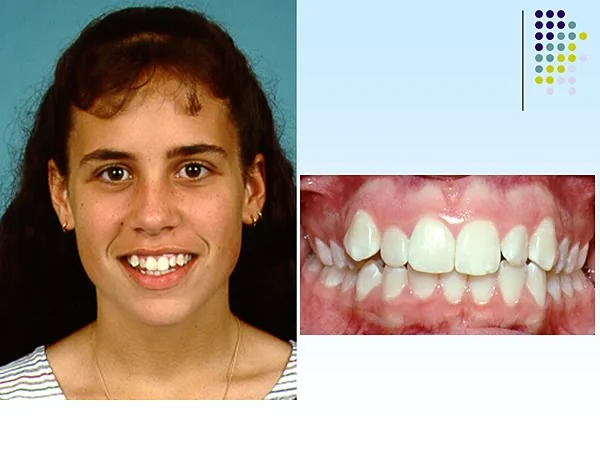
What is an orthodontic problem? The simplest definition: A condition characterized by alterations from normal alignment and occlusion of the teeth which causes problems for the patient. Does this girl have an orthodontic problem? To evaluate that, you will have to examine her teeth and facial appearance, and you’ll have to ask her what she thinks.
Definition of Orthodontic Problem (cont.)
In fact, Katherine and her mother agreed that they didn’t like the appearance of her teeth. This caused some problems for her now and had the potential to affect social interactions in the future.
It’s obvious that she has a malocclusion, that is, her teeth don’t fit properly. But saying she has a problem isn’t a diagnosis—it’s a reason for doing a diagnostic evaluation, to obtain a complete list of the problems that constitutes a diagnosis.
An important concept: The goal of diagnosis is the truth about the patient. So pulling together the facts about the patient is a scientific procedure. At this stage the doctor’s opinion needs to be kept out of the picture as much as possible—don’t jump to conclusions.
 Image 1, profile: Katherine, age 12, initial examination. Image 1, profile: Katherine, age 12, initial examination. |  Image 2, occlusion right: Katherine, age 12, initial examination. Image 2, occlusion right: Katherine, age 12, initial examination. |
 Image 3, occlusion left: Katherine, age 12, initial examination. Image 3, occlusion left: Katherine, age 12, initial examination. |
Diagnostic Process
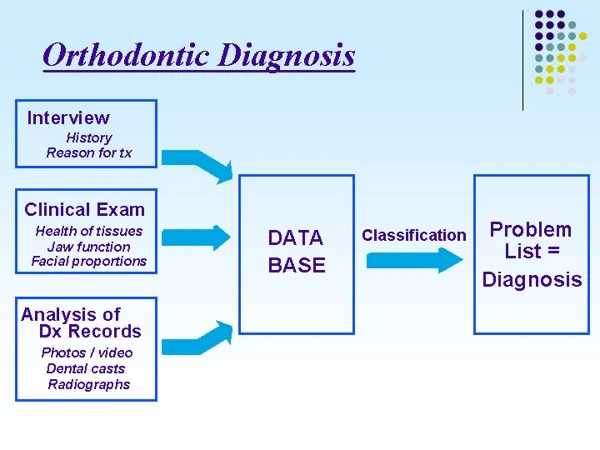
What’s needed is a systematic approach to gathering and analyzing the necessary diagnostic data. The process calls for, first:
- development of a diagnostic data base, derived from interview clinical examination analysis of records
then
- systematic description, often called classification, to produce the problem list that is the diagnosis
Interview
Interview Process
Let’s follow the diagnostic process with Anna, who was 12 years, 6 months of age when she was evaluated for orthodontic problems. Her problems aren’t quite so obvious, but she illustrates the general approach reasonably well.
The diagnostic work-up begins with collection of data from an interview, which typically includes review of a form that the patient filled out in advance and some follow-up questions.
 Image 1, smile: Anna, age 12-6, initial evaluation. Image 1, smile: Anna, age 12-6, initial evaluation. |  Image 2, dentition: Anna, age 12-6, initial evaluation. Image 2, dentition: Anna, age 12-6, initial evaluation. |
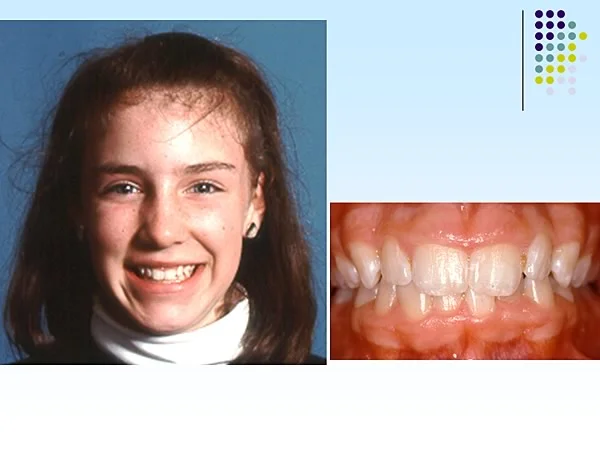 Image 3, combined: Anna, age 12-6, initial evaluation. Image 3, combined: Anna, age 12-6, initial evaluation. |
Interview Data
The goal of the interview is to answer four major questions:
- Why is this patient seeking treatment, and why now?
The intent is to understand her concerns and motivation. For a child, this often is straightforward, but children occasionally and adults often tell the doctor what they think he or she wants to hear. If you don’t understand why the patient is seeking treatment, you have no chance of determining what the real problem is.
For Anna, she and her family simply want to have her dental problems corrected. The motivation is to detect anything that is abnormal and get it corrected in the optimal way.
Anna’s mother had several congenitally missing teeth, and she is concerned that Anna may have a similar problem.

Interview Data (cont.)
- How did things get to be the way they are?
That, of course, involves understanding the pertinent medical and dental history, and (to the extent possible) the etiology of any abnormalities.
Anna has had normal physical development, with no pertinent medical history of any serious illnesses.
- What, if anything, is likely to change in the near future?
That requires considering two important things: (1) the progression of any medical condition, which is not pertinent for Anna; and (2) probable growth changes, which is highly pertinent.
Anna has not yet reached sexual maturity but recently has begun to grow rapidly. Since the adolescent growth spurt is the ideal time for most orthodontic treatment, it is important to establish where she is in development.
Interview Data (cont.)
- What do the patient and parents expect as a result?
The important thing here is to establish whether what they expect is realistic or not. This relates to motivation for treatment but isn’t quite the same thing. Sometimes patients correctly identify problems but have unrealistic expectations. For example, if Anna’s mother is worried about a possible congenitally missing tooth and thinks the dentist can stimulate one to grow, it is important to know about this unrealistic expectation from the beginning.
In fact, the expectations are realistic. Anna and her parents simply think that if there is a problem, the dentist will find it and offer appropriate treatment.
It only takes a minute or two to review the history form and ask the questions. The bottom line from this interview: No special problems with this patient. But sometimes a red flag goes up—it can be critically important to get the answers to these questions.
Clinical Exam
Steps in Clinical Examination
The second step in the diagnostic evaluation is to take a good look at the patient. This includes examining the mouth but certainly is not limited to that.
The clinical exam has four goals:
- Evaluate facial proportions and tooth-lip relationships.
- Evaluate the health of oral hard and soft tissues.
- Evaluate jaw function.
- Determine what diagnostic records are required.
Let’s take these one at time, starting with facial proportions and tooth-lip relationships. This evaluation, of course, is the facial form analysis with which you already have had some experience.
Facial Examination
In the facial examination, it is important to look at three things:
- First, in the full face view, symmetry and proportion. Anna has a symmetric face, with no right-left or up-down disproportions, so there is no skeletal problem in these planes of space.
- Second, in the profile view, a-p and vertical jaw relationships. Anna has mild mandibular deficiency, but the jaw relationships are within normal limits.
- Third, in the smile and profile views, lip-tooth relationships and lip support. Anna’s display of incisor teeth on smile is normal. In the profile view, her lip profile is normal. She has no evidence of lip strain to close her lips over protruding teeth and does not have excessive lip separation at rest.
The bottom line: No skeletal or dentofacial problems.
 Image 1, frontal relaxed: Anna, age 12, frontal view with lips relaxed. Image 1, frontal relaxed: Anna, age 12, frontal view with lips relaxed. |  Image 2, profile relaxed: Anna, age 12, profile view with lips relaxed. Image 2, profile relaxed: Anna, age 12, profile view with lips relaxed. |
 Image 3, smile: Anna, age 12, smile view; note normal display of all the incisors but no gingiva. Image 3, smile: Anna, age 12, smile view; note normal display of all the incisors but no gingiva. |
Intraoral Exam, Health of Tissues
Now we can look at the teeth—but the focus should be first on the health of the tissues and on jaw function, not the details of the occlusion.
Anna has healthy-appearing teeth, with all primary teeth exfoliated except the lower second primary molars, and with permanent teeth erupting.
In the examination of the soft tissues, it is important to examine the amount of attached gingival tissue, in addition to looking for areas of gingivitis/bleeding on probing.
Anna has mild gingivitis around upper central incisors but has normal attached gingiva, no evidence of periodontitis, and no clinical caries or restorations.
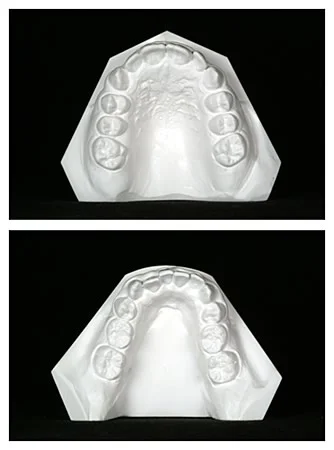
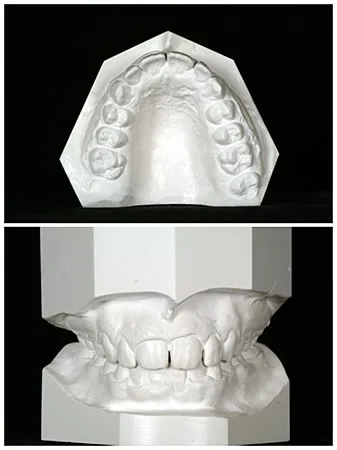
 Image 1, frontal view: Anna, age 12-6. Image 1, frontal view: Anna, age 12-6. |  Image 2, right lateral view: Anna, age 12-6. Image 2, right lateral view: Anna, age 12-6. |
 Image 3, left lateral view: Anna, age 12-6. Image 3, left lateral view: Anna, age 12-6. |  Image 4, maxillary occlusal: Anna, age 12-6. Image 4, maxillary occlusal: Anna, age 12-6. |
 Image 5, mandibular occlusal: Anna, age 12-6. Image 5, mandibular occlusal: Anna, age 12-6. |
Intraoral Exam, Jaw Function
The third important step in clinical examination is evaluation of jaw function. If a malocclusion is so severe that the patient has difficulty eating, of course that would be noted. Anna is the other extreme. But TM joint function/dysfunction must be considered.
The best single indicator of whether the TM joint is normal is whether the patient can open normally and move the jaw laterally and forward. The general guideline is simple: If a joint moves normally, almost surely there isn’t a problem with function. If it doesn’t move normally, at least to some extent, there is a problem.
Anna had normal opening for a girl her age of 42 mm, with normal lateral and forward movements, and no deviation on opening. There were no joint sounds or pain on palpation.
This girl, unlike Anna, deviates to the left on opening, although she can open almost the normal distance. She moves laterally more on one side than the other. Both these findings are consistent with a problem with the left TM joint.

Clinical Exam: What Diagnostic Records?
The final part of the clinical examination is to determine what diagnostic records are needed.
For a patient with a potential orthodontic problem, a panoramic radiograph always is indicated. It should be supplemented with bitewings if caries is noted on clinical examination or if restorations are present, and with periapical radiographs in specific areas if there is evidence of pulpal pathology or periodontal disease.
Anna’s panoramic radiograph shows that formation of one mandibular second primary molar is very delayed, and the other is missing.

Diagnostic Records (cont.)
Other essential orthodontic diagnostic records are:
- Dental castsThese are necessary to allow the measurements in space analysis and to provide a record of the pretreatment alignment and occlusion.
- Intraoral and facial photographsThese are primarily a record to allow evaluation of change. It is important to photograph areas of soft tissue problems, for instance, lack of gingival attachment in the lower incisor area.
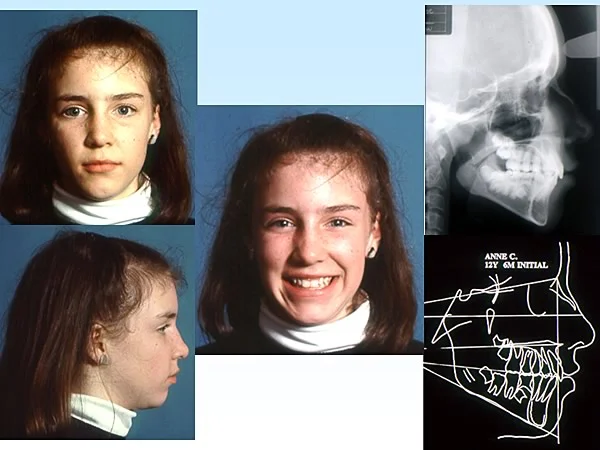
- Lateral cephalometric radiograph/tracingThe ceph is essential to allow evaluation of the response to treatment, and it allows greater precision in evaluating jaw and tooth-jaw relationships. The cephalometric radiograph and tracing for Anna confirm mild mandibular deficiency and otherwise normal relationships.
 Image 1, pre-tx ceph: Anna, age 12-6. Image 1, pre-tx ceph: Anna, age 12-6. | 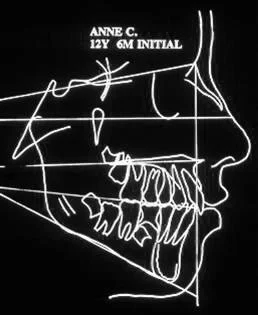 Image 2, pre-tx tracing: Anna, age 12-6. Image 2, pre-tx tracing: Anna, age 12-6. |
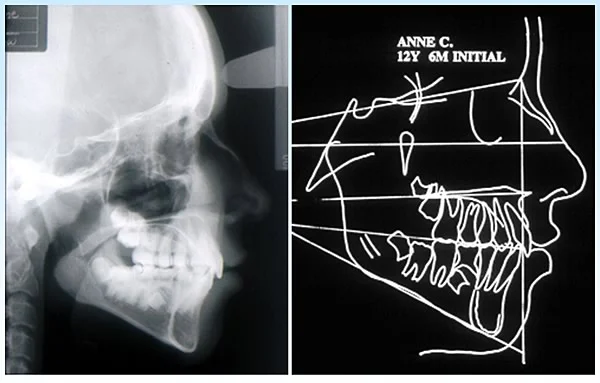 Image 3, combined: Anna, age 12-6. Image 3, combined: Anna, age 12-6. |
Diagnostic Records (cont.)
Three important questions about typical orthodontic diagnostic records:
1. Is there any advantage in having the dental casts mounted on an articulator? That depends on the individual case. If extensive restorative treatment or maxillary surgery must be planned as part of comprehensive evaluation in an adult, then yes, articulator mounting is indicated. But as a general rule for orthodontics and especially for children, the answer is no. In a growing child, because the relationship of the dentition to the TM joint changes rapidly, the articulated casts quickly become only a historical artifact.
2. Is a cephalometric radiograph necessary for orthodontic diagnosis? The cephalometric radiograph makes it easier to define skeletal and dental relationships, but it is not strictly necessary for diagnosis. Problems in jaw relationships and lip support can be detected on careful clinical examination. Yet modern orthodontic treatment almost always requires cephalometric analysis. It’s malpractice to do comprehensive treatment without cephalometrics. Why? Because it is impossible to determine the progress of treatment without being able to superimpose serial cephalometric tracings. You can easily be fooled on clinical examination as to what really is happening. If you didn’t take a pretreatment ceph, a progress ceph is of minimal value.
3. What is the indication for a P-A cephalometric radiograph in addition to the lateral ceph? The primary indication for a P-A ceph is jaw asymmetry noted on clinical examination. A P-A ceph is not taken routinely for two reasons: (a) symmetric transverse relationships can be evaluated from clinical records and dental casts, and (b) in contrast to the lateral ceph, evaluating growth and treatment response from serial superimpositions is difficult and inaccurate.
The bottom line:
- Articulator-mounted casts are indicated primarily as an aid in planning treatment that involves extensive restorative dentistry and/or orthognathic surgery.
- Lateral cephalometric radiographs are essential for evaluating treatment and quite helpful (but not essential) for diagnosis.
- P-A cephs are indicated primarily for asymmetry and not obtained routinely.
3D Imaging?
The ability of obtain 3D images and use them in evaluation of orthodontic patients has developed rapidly in the last few years. In fact, 3D images of three types now can obtained if desired:
- 3D photographs or 3D video
- MRI (magnetic resonance imaging)
- CT (computed tomography)
Let’s consider these in turn.
3D Photography
Several systems for obtaining 3D facial photographs that allow precise evaluation of facial soft tissue proportions and dimensions now are available. This can be a valuable research tool, particularly when the dynamics of facial soft tissue change are evaluated (which requires video, not just still images). This type of evaluation is valuable, for instance, when the effects of plastic surgery to correct a cleft lip are being considered, or when the amount of lip support provided by a fixed orthodontic appliance is to be determined.
In these superimposed images from a 3dMD camera system, one can precisely measure the amount of change in lip support created by removing a fixed orthodontic appliance (image 1). The color map shows the amount of change: the blue color indicates a change in lip posture moving into the background, green is minimal change, and red indicates forward change—so for this patient, the lips moved back about 2 mm in most areas immediately after braces were removed. In a series of 9 patients (image 2), the superimposed images show that a 2 mm change occurred in most of them, with an extension of change beyond the corners of the mouth in 3 of the group. With a 4-camera 3dMD version that allows video recording, the rapid pattern of change in facial expressions can be detected.
It is unlikely that this high-definition 3D photography will be widely used in evaluation of most orthodontic patients, however, simply because it is expensive and does not add valuable diagnostic information beyond what can obtained from the type of facial form analysis that you have already learned how to do.
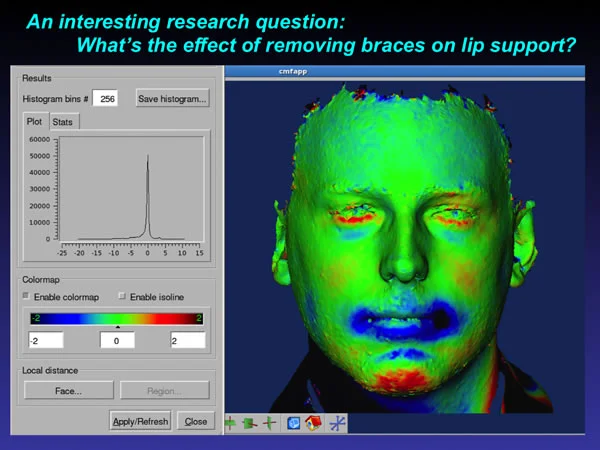 3dMD research image: Using special software to evaluate changes between superimposed 3D camera images, it is possible to precisely measure change in lip position. The color shows the direction of change (blue moving back, into the screen; red moving forward), the color intensity shows the magnitude. 3dMD research image: Using special software to evaluate changes between superimposed 3D camera images, it is possible to precisely measure change in lip position. The color shows the direction of change (blue moving back, into the screen; red moving forward), the color intensity shows the magnitude. | 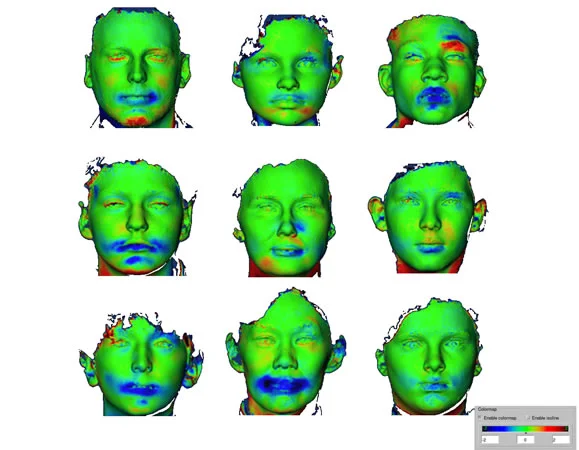 3dMD research image sequence: Note that for most of these patients, the lips moved back about 2 mm, with a decrease in soft tissue prominence extending into the cheeks for three of them. 3dMD research image sequence: Note that for most of these patients, the lips moved back about 2 mm, with a decrease in soft tissue prominence extending into the cheeks for three of them. |
Magnetic Resonance Imaging
Magnetic resonance imaging, like photography, has the advantage that no ionizing radiation is used to obtain the images. In contrast to radiographs, internal soft tissues are revealed more clearly than hard tissues, and in dentistry MRI can be quite valuable in evaluation of TM joint problems like disk displacement (image 1) or soft tissue pathologic changes in or near the joint (image 2).
For an individual in whom a problem internal to the TM joint has been detected during the clinical examination, MRI, not radiography, now is the diagnostic procedure of choice. Fortunately, most orthodontic patients do not have TM joint pproblems—but referral for MRI of those in those who do is important.
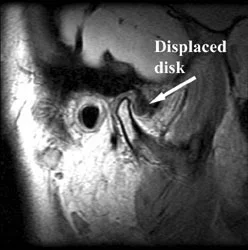 MRI image of TM joint: The MRI image shows clearly that disk has been displaced from its normal position over the head of the condyle. MRI image of TM joint: The MRI image shows clearly that disk has been displaced from its normal position over the head of the condyle. | 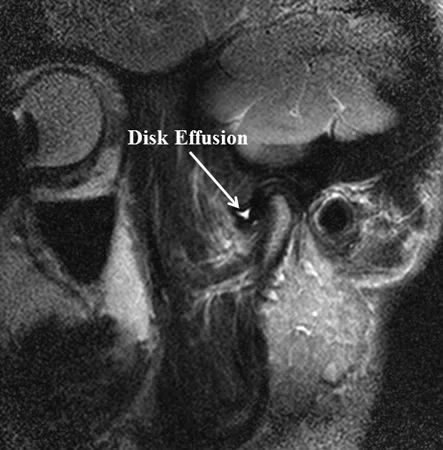 MRI image of TM joint: In this image, pathologic changes in the disc can be visualized. MRI image of TM joint: In this image, pathologic changes in the disc can be visualized. |
Computed Tomography
Computed tomography (CT) imaging has become an important part of medical diagnosis despite its relatively high radiation dose and the expensive equipment. In recent years cone-beam CT (CBCT) has been developed as a method for obtaining 3D images of the head and face, at both lower radiation levels and lower economic cost. It is rapidly becoming an important part of orthodontic evaluation.
There are two concerns about the use of CBCT in dental and orthodontic practice. The first is that its ability to reveal unexpected pathology. Does one need additional expertise to evaluate pathologic changes revealed by these images? The answer to that is a clear-cut yes—which means that a radiologist needs to view them to screen for pathology.
The other concern is the amount of radiation exposure with CBCT, which is a factor in deciding whether to use it. The larger the field of view with CBCT, the higher the radiation dose. The table in image 1 shows the relative radiation dose with modern technology for periapical, panographic and cephalometric images in comparison to the radiation from medium- and large-field CBCT. It is apparent that the radiation to image a small area, such as you would find around an unerupted maxillary canine, is similar to what would be generated from a panographic radiograph, while the radiation from a large-field CBCT image of the face and jaws is considerably larger than the radiation from a cephalometric radiograph. Logically, one would choose the higher cost and higher radiation exposure when, and only when, the value of the additional diagnostic information it would provide would benefit the patient. As a general guideline, CBCT of the area of impacted teeth now is indicated for most patients, and full-face CBCT is indicated for skeletal asymmetry. Other potential reasons for obtaining CBCT are not (yet?) supported by evidence.
The analysis of CBCT images is discussed in the following section of this module.
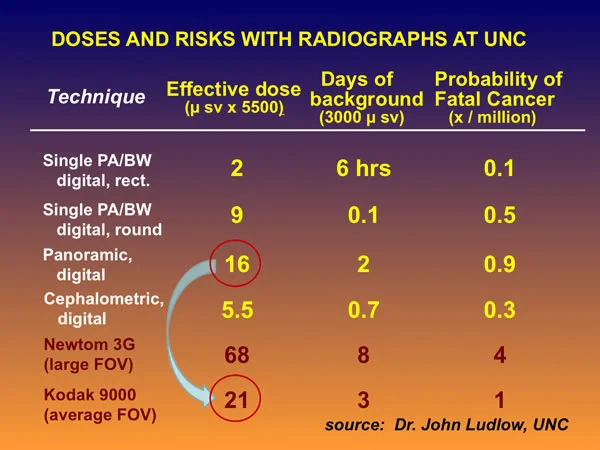 Digital pan vs. small FOV CBCT: The comparative radiation dose for a digital panoramic radiograph vs. small field-of-view CBCT. Digital pan vs. small FOV CBCT: The comparative radiation dose for a digital panoramic radiograph vs. small field-of-view CBCT. | 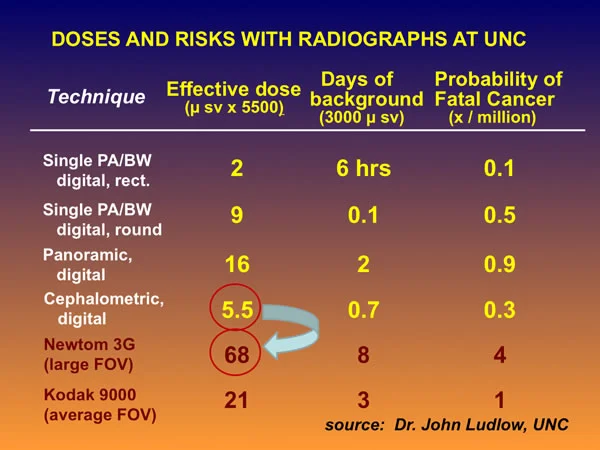 Digital ceph vs. large FOV CBCT: The comparative radiation dose for a digital cephalometic radiograph vs. large field-of-view CBCT. Digital ceph vs. large FOV CBCT: The comparative radiation dose for a digital cephalometic radiograph vs. large field-of-view CBCT. |
Analysis of Records
Photo/Video Records
The diagnostic records for an orthodontic patient typically consist of:
- photographs (and/or digital video clips)
- dental casts
- radiographs
Occasionally, articulator-mounted casts, CT scans, MRI images, or other data are added. Almost always, this occurs in children with severe (syndromic) problems or in adults with multiple dental problems, including missing teeth (see the modules on Adult Orthodontics and Adjunctive Treatment).
Photographs primarily provide confirmation and documentation of what was observed clinically. Facial animation, especially on smile, is an important part of evaluating esthetics. Short video clips (as seen in the accompanying image) can be obtained with almost any modern digital camera and incorporated into digital records, and are likely to become a routine part of orthodontic evaluations in the future. The video clips can provide facial views in multiple dimensions as well as a record of lip-tooth relationships on smiling. Careful observation, not frame-by-frame measurement, is the primary method of analysis.
Digital video clip: A digital video that shows both soft tissue animation and views from multiple orientations provides a record of facial proportions that cannot be obtained from a series of still images.
Cast Analysis
Analysis of dental casts is primarily space analysis, the calculation of space available versus space required for alignment of the permanent teeth (image 1). The use of this form is shown in detail in the Level 2 module on space analysis. Space analysis now can be carried out using a computerized version of this form (image 2), and in your future practice you probably will have that available—but doing it manually now so that you understand the steps in the procedure is a better learning experience.
If the patient is in the mixed dentition, careful analysis to indicate the extent of potential crowding is important, but quantification of actual crowding also is important for patients in the permanent dentition.
If a posterior crossbite exists, measuring arch widths can provide insight into whether the upper arch is unusually narrow because of a skeletal problem (narrow palatal vault) or a dental problem (alveolar processes tipped lingually), or the lower arch is unusually wide.
These measurements become part of the diagnostic database. They provide an important guideline for treatment planning.
 Image 1, space analysis: Mixed dentition space analysis form. Image 1, space analysis: Mixed dentition space analysis form. | 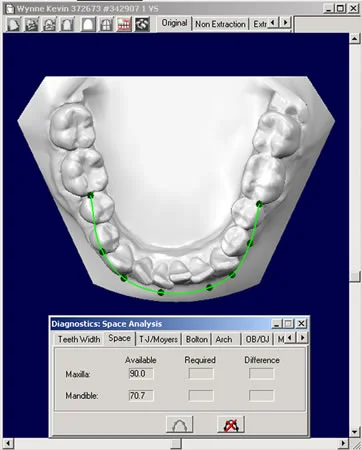 Space analysis, virtual models: Space analysis using digitized casts can be done with accuracy equal to manual measurements of space available vs. space required. Space analysis, virtual models: Space analysis using digitized casts can be done with accuracy equal to manual measurements of space available vs. space required. |
Cast Analysis (cont.)
Space analysis for Anna was done using maxillary and mandibular casts (image 1) and the UNC form for this purpose. Measurements for space available in the upper and lower arches are shown in images 2 and 3. The results of space analysis for the two arches are shown in image 4, and the other things that must be taken into consideration when space analysis is done are shown in image 5.
The data show that in the mandibular arch, if normal 2nd premolars were present in the arch, she would have enough space. With missing 2nd premolars, of course, there is a large excess of space. Space analysis predicts mild crowding in the upper arch.
 Image 1, dental casts: Anna, age 12, maxillary and mandibular casts. Image 1, dental casts: Anna, age 12, maxillary and mandibular casts. | 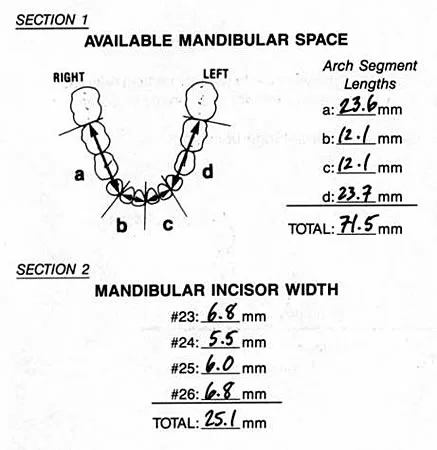 Image 2, mand. space available: Anna, age 12, measurements of space available and incisor widths, mandibular arch. Image 2, mand. space available: Anna, age 12, measurements of space available and incisor widths, mandibular arch. |
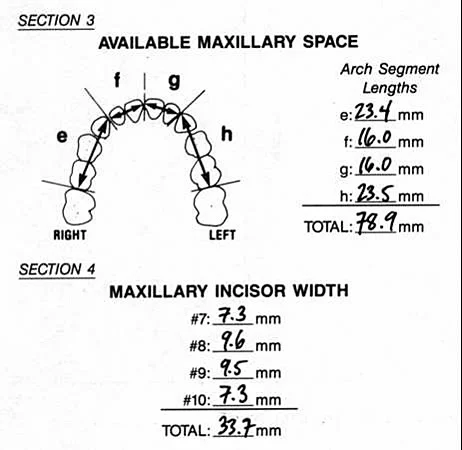 Image 3, max. space available: Anna, age 12, space available and incisor widths, maxillary arch. Image 3, max. space available: Anna, age 12, space available and incisor widths, maxillary arch. | 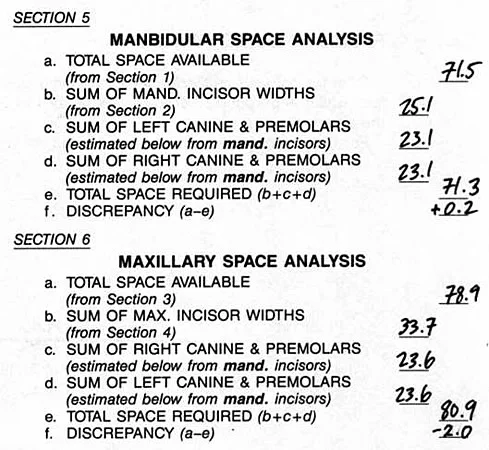 Image 4, space analysis results: Anna, space analysis results, assuming normal 2nd premolars. Image 4, space analysis results: Anna, space analysis results, assuming normal 2nd premolars. |
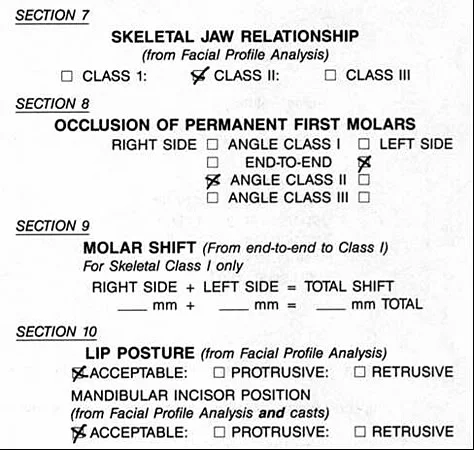 Image 5, other considerations: Anna, other considerations in space analysis. Image 5, other considerations: Anna, other considerations in space analysis. |
Cephalometric Analysis
Cephalometric analysis can be complex and difficult to understand. All the measurements and calculations, however, are indicators of critical relationships that were already evaluated less precisely on clinical examination.
The critical relationships are:
- How the jaws relate to the cranial base
- How the jaws relate to each other
- How the teeth of each jaw relate to the supporting bone of the jaw itself
These relationships must be judged in both the anteroposterior and vertical planes of space. The key is to understand the relationships. Any set of measurements is a means to an end, not the end in itself. For example, the ANB angle often is used to evaluate the relationship of the maxilla to the mandible—but the value of the angle must be interpreted. No individual measurement or calculation can give the big picture of the important relationships.
Cephalometric Analysis, Anna
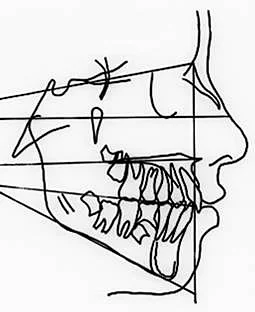
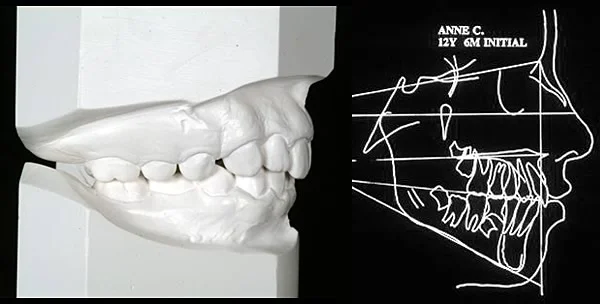
For Anna, we can see the important things just from inspection of the tracing, with a true vertical line dropped from nasion and the important horizontal planes drawn in.
First, look at the relationship of the anterior maxilla and mandible to the nasion vertical line. Note that point A is almost on the line, while the chin is about 6 mm behind it. So the a-p relationship of the maxilla is normal. Then look at the relationship of the S-N (cranial base), true horizontal and palatal planes. The palatal plane is slightly tipped down posteriorly, indicating slightly excessive maxillary posterior vertical growth.
Then look similarly at the mandible. The chin is about 6 mm behind the true vertical line, and the mandibular plane angle is a little large.
Then look at the teeth relative to each jaw, using the true vertical line moved to points A and B, respectively.
The bottom line: Anna has mild skeletal deviations from ideal, compensated by mild displacement of the position of the teeth so that dental relationships are normal.
CBCT for Impacted Teeth
Although Anna has one missing lower second premolar and one slowly-developing one, she does not have impacted teeth and so had no indication for CBCT as part of her diagnostic records. This, however, is the logical place to briefly discuss analysis of CBCT images to evaluate impacted teeth.
As we have noted above, impacted teeth—usually but certainly not always maxillary canines—are an indication now for CBCT of that area, but not CBCT of the whole head. CBCT is indicated simply because it is likely to change the treatment plan over what probably would have been done using 2D images. The relationship of the impacted tooth to the bone and other teeth around it can be seen clearly in the 3D image, which can be rotated so that a view from any direction is possible (image 1), and sequential slices through any area at any orientation are possible (image 2).
The 3D images often show that the impacted tooth needs to moved away from the root of another permanent tooth (for an impacted canine, away from the root of a lateral or central incisor) before then being brought toward the oral cavity. Otherwise, the impacted tooth may be pulled directly into the adjacent tooth root, further damaging it. Analysis is just a matter of observing how the impacted tooth should be moved in order to minimize damage to other teeth.
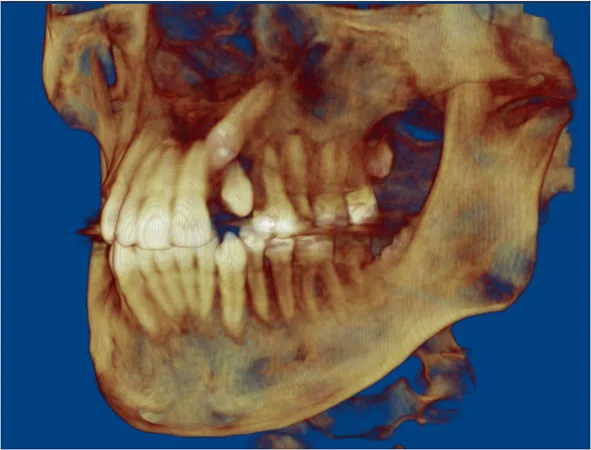 Image 1, Composite view: In this oblique view, the tip of the crown of the impacted canine can be seen to be behind the root of the central incisor—which may already have been damaged, and would need to be avoided as the impacted tooth was brought toward the oral cavity. A view of this type can be rotated to be seen at any angle on the computer screen. Image 1, Composite view: In this oblique view, the tip of the crown of the impacted canine can be seen to be behind the root of the central incisor—which may already have been damaged, and would need to be avoided as the impacted tooth was brought toward the oral cavity. A view of this type can be rotated to be seen at any angle on the computer screen. | 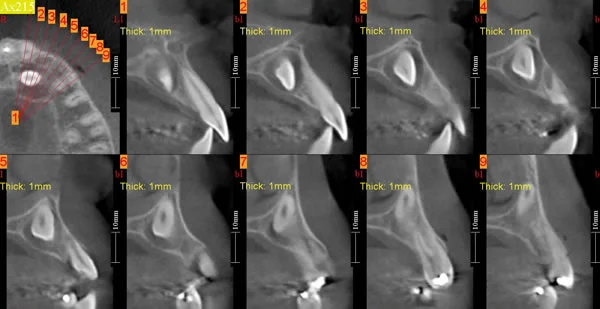 Image 2, Series of slices: A series of slices, moving along the dental arch, provides more detail. This impacted canine is behind and below the root of the central and lateral, both of which could be damaged by moving the canine directly facially. Image 2, Series of slices: A series of slices, moving along the dental arch, provides more detail. This impacted canine is behind and below the root of the central and lateral, both of which could be damaged by moving the canine directly facially. |
Skeletal Asymmetry
The second major indication for CBCT, and the major reason to use a large field of view, is skeletal facial asymmetry. Planning treatment for these patients using information from CBCT is much more straightforward than using a combination of frontal and lateral cephalometric radiographs, and of course the CBCT is increasingly valuable as the degree of asymmetry increases. A composite rendering of the CBCT (image 1) can be rotated on the computer screen so that the extent and location of the asymmetry can be viewed from any perspective. Slices (images 2-4) at any plane reveal details of the normal and affected sides. This allows both a more precise evaluation of the patient’s condition and more precise planning of both the orthodontic and surgical treatment that is likely to be needed.
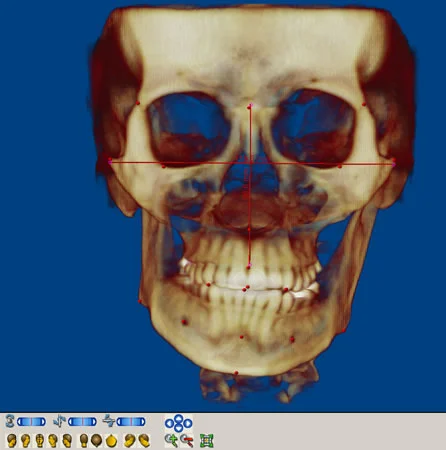 Image 1, Jaw asymmetry, frontal composite Image 1, Jaw asymmetry, frontal composite | 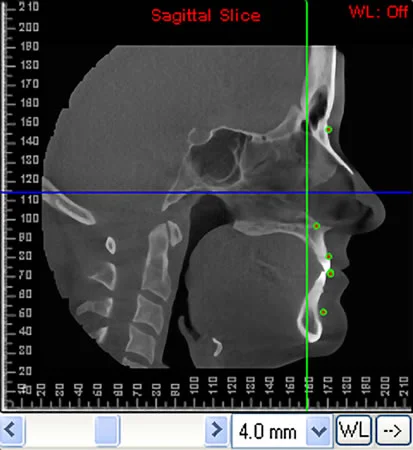 Image 2, Same patient, sagittal midline slice Image 2, Same patient, sagittal midline slice |
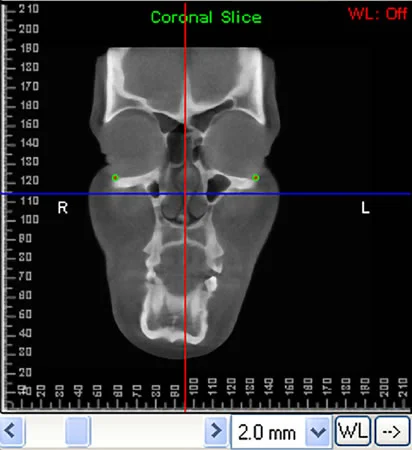 Image 3, Same patient, coronal slice, molar region Image 3, Same patient, coronal slice, molar region | 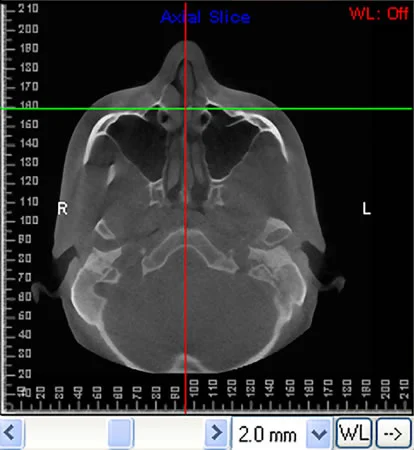 Image 4, Same patient, axial slice, molar region Image 4, Same patient, axial slice, molar region |
Detailed Evaluation of Treatment Outcomes
The third major use of CBCT is the use of superimposed sequential images to obtain a more detailed evaluation of treatment outcomes, which makes it a valuable research tool. Cephalometric radiographs are important in orthodontic diagnosis, but their most important use is to determine the effect of treatment on both the teeth and jaw relationships, which is difficult to detect just from clinical examination. Superimposition of CBCT images is difficult but provides much more information about the location and amount of change.
A good illustration of this use is the evaluation of changes following orthognathic surgery. It is possible to superimpose CBCT images on the surface of the cranial base, and then to display changes created by surgically repositioning the jaws as color maps. Image 1 shows changes in the position of the maxilla and mandible created by 2-jaw surgery for correction of a severe Class III problem that included a mandibular asymmetry. The red color shows the forward movement of the maxilla that included a forward rotation, so that the paranasal area was brought forward more than the incisor teeth. The blue color shows the backward movement of the mandible, with more setback on the right than the left side. It is impossible to get a similar sense of the surgical movements from lateral and PA cephalograms. Movements can be seen from other views, as shown in image 2.
It also is possible to view changes in the position and orientation of the mandibular condyles, as the ramus segments are rotated several degrees as the mandible is set back (image 3). Color maps of the condyles from immediate postsurgery to follow-up allow a better understanding of the adaptive changes to the surgical rotation.
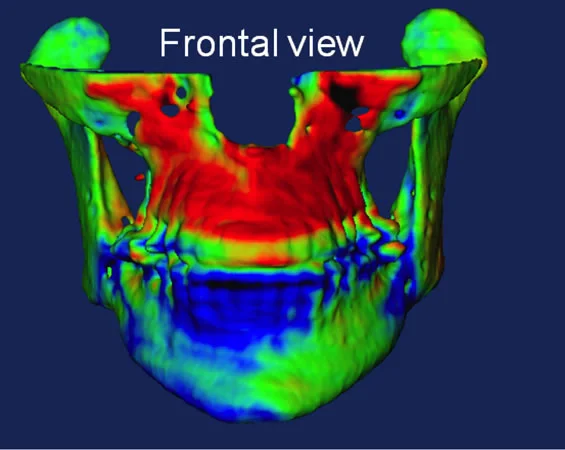 Image 1, Superimposition color map, 2-jaw surgery: This patient underwent maxillary advancement and asymmetric mandibular setback. The red color shows the location and magnitude of the advancement; the blue shows the setback. Image 1, Superimposition color map, 2-jaw surgery: This patient underwent maxillary advancement and asymmetric mandibular setback. The red color shows the location and magnitude of the advancement; the blue shows the setback. | 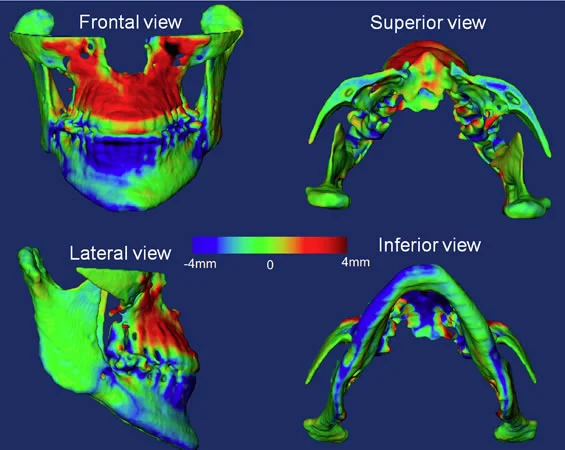 Image 2, Same patient, multiple views: CBCT superimposition (on the cranial base for all views) allows changes to be evaluated from any perspective. Image 2, Same patient, multiple views: CBCT superimposition (on the cranial base for all views) allows changes to be evaluated from any perspective. |
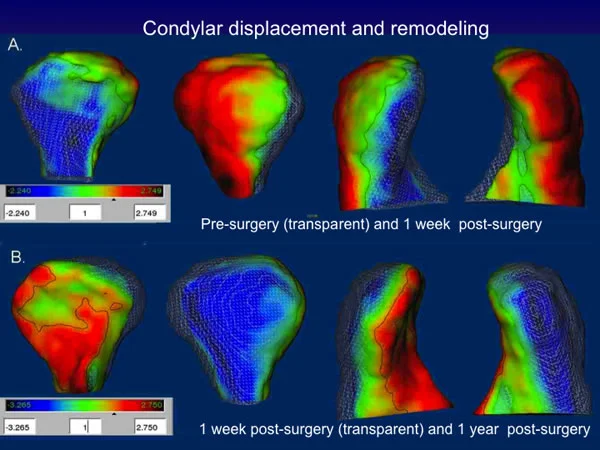 Image 3, Surgical changes, condyle/ramus close-up: Close-up views of changes in the orientation / position of the ramus segment and condyles allow observation of the amount of surgical change, and remodeling can be observed directly with postsurgery to follow-up superimpositions. Image 3, Surgical changes, condyle/ramus close-up: Close-up views of changes in the orientation / position of the ramus segment and condyles allow observation of the amount of surgical change, and remodeling can be observed directly with postsurgery to follow-up superimpositions. |
Classification, Problem List
Classification = Systematic Description
At this point, with the diagnostic database assembled, the next step is to generate the problem list that constitutes diagnosis. The approach:
- First, note any pathologic problems separately. These receive priority for treatment, not because they are more important but because they must be brought under control before other treatment starts.
- Then, classify the diagnostic findings of developmental problems to develop the rest of the problem list using systematic description.
The systematic description approach (Ackerman-Proffit classification) is designed to ensure that important aspects of the patient’s orthodontic problems are not overlooked, while minimizing the size and complexity of the resulting problem list. You already have learned how to use this method—now let’s review it in the context of applying it to Anna’s diagnosis and treatment plan.
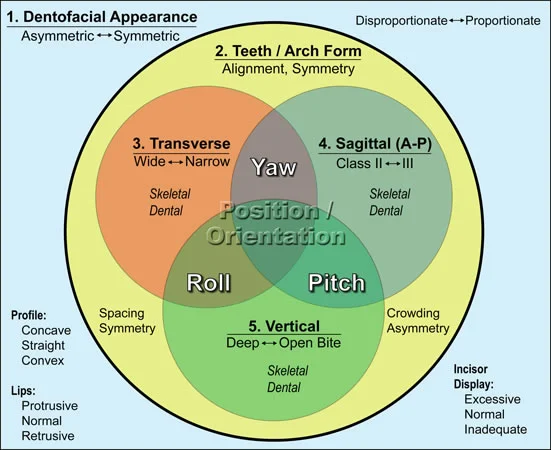
Systematic description has 5 steps:
- Alignment/symmetry of the dental arches
- Evaluation of dental protrusion/esthetics
- Transverse skeletal/dental relationships
- A-P skeletal/dental relationships
- Vertical skeletal/dental relationships
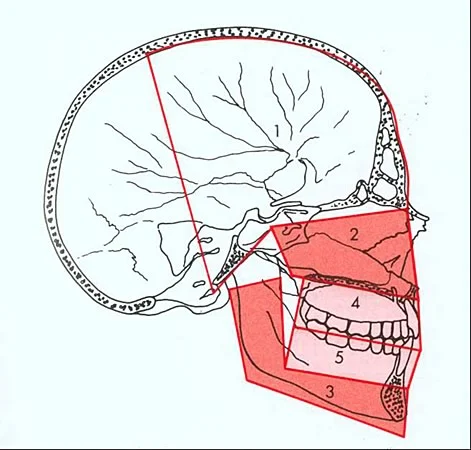
The classification scheme can be expressed as a Venn diagram, as shown in image 1. This emphasizes the possibility for different sets of problems and for interactions in multiple planes of space—but the key is simply to look at the 5 characteristics in order and note any problems related to each characteristic.
Step 1. Alignment/Symmetry
The first step is to look at the alignment and symmetry within the dental arches, considered separately, with the results of space analysis and other measurements available, and with the panoramic radiograph and any other dental radiographs available. Only positive findings (problems) will be carried forward to the problem list.
For Anna, the arches are symmetric and there is adequate space in the maxillary arch. The mandibular arch is mildly crowded, one second premolar is missing, and the other is severely delayed. These items go to the problem list.
Step 2. Esthetic Impact of Malocclusion
The second step in classification is to evaluate the impact on facial esthetics of the tooth and jaw positions. It requires looking at the notes from clinical examination of tooth-lip relationships and facial proportions, photographs, and cephalometric analysis.
Anna has normal tooth-lip relationships as seen clinically, in the photos, and on the cephalometric radiograph. Her tooth-jaw relationships and soft tissue profile are normal.
Bottom line: no esthetic problem.
Step 3. Transverse Relationships
The next step is to put the dental casts together and evaluate skeletal and dental relationships in all 3 planes of space, beginning with the transverse plane.
Anna has normal transverse relationships of the teeth (no posterior crossbite), and there is no evidence of any skeletal transverse problem. If an asymmetry had been noted on clinical examination, a P-A cephalometric radiograph or (and better) CBCT would have been included in the diagnostic records.
Step 4. A-P Relationships
Now the dental and skeletal relationships in the antero-posterior plane of space are evaluated, using the dental casts and the cephalometric analysis.
The Angle classification is used to describe the molar relationship, and its extended version is used to describe the skeletal relationship.
It is important to note that although the dental and skeletal relationships usually match, they may not. For individual patients, an accurate description might be “skeletal Class II with Class I molars” or “Class II molars with Class I skeletal relationship.”
For Anna, the description is “mild skeletal Class II with Class I molars,” and that’s not really a problem.
Step 5. Vertical Relationships
The final step is to look at the dental casts and the cephalometric analysis to evaluate dental and skeletal relationships in the vertical plane of space.
Dental vertical problems are excessive overbite, anterior open bite, or posterior open bite. Skeletal vertical problems are excessive or deficient mid- or lower face height, often related to rotation of either or both jaws. Excessive or deficient eruption of teeth also can be noted on the ceph.
Cephalometric analysis often puts more emphasis on A-P than vertical relationships. Particularly, many published analyses that are a set of prescribed measurements often do not reveal skeletal vertical problems.
For Anna, there is a mild tendency toward skeletal open bite, shown by the rotated palatal plane and increased mandibular plane angle. This is compensated by slightly increased eruption of the lower incisors, and overbite is normal.
Problem List
Anna’s orthodontic diagnosis is the list of problems derived from this procedure.
Should the missing/delayed mandibular second premolars be considered a pathologic or developmental problem? In this case, the structure of the problem list would not really be affected whichever way you did it: The missing teeth are the major problem. As a rule, however, missing teeth are dealt with most effectively if they’re considered a developmental problem, and pathology is reserved for disease entities.
The final problem list:
- missing mandibular right 2nd premolar, severely delayed mandibular left 2nd premolar
- mild crowding of mandibular incisors
A major advantage of having the diagnosis in this form is that attention is immediately directed toward the treatment that will be needed—which is a giant step toward developing an appropriate treatment plan. In Anna’s case, the orthodontic diagnosis has served largely to rule out problems other than the missing teeth that would have complicated treatment. But you have to know whether other problems exist before you can develop the correct treatment plan. The problem list for a patient with a more severe malocclusion would be longer. Note, however, that there would be a maximum of 5 developmental problems (each of which might have several characteristics).
Experience has shown that this grouping of problems makes it easier to keep up with the treatment possibilities for patients with severe problems—and the same diagnostic method is applicable to all potential orthodontic patients, however simple or complex their problems may be. In the apparently simple cases, it’s important not to overlook something important. In the complex ones, it’s important to be thorough and pick up all the problems, not just the most obvious ones.
The development of a treatment plan for Anna, and the outcome of that treatment, are shown in the Concepts of Treatment Planning module.
Self-Test Referral
The self-test section of this program is designed to help you be sure you have understood the material.
Now that you have gone through the module, do the assigned reading in Contemporary Orthodontics(pages 147-184 in 5th ed.; pages 163-201, 4th ed.) Then take the self-test, and use it as a guide for further study and review.
Copyright 2013, UNC Dept. of Orthodontics
Self-Test
Question 1
Which of the following must be evaluated during orthodontic diagnosis?
a. Dental alignment
b. Dental occlusion
c. Facial proportions
d. Patient attitude toward dental condition
- a and b
- a and c
- a, b, and c
- a, b, and d
- all of the above ✓
Correct
That’s right, all must be evaluated. Whether dental alignment and occlusion and/or facial proportions are a problem depends to a considerable extent on whether the patient thinks they are a problem. Some patients tolerate conditions that are not tolerable for others—a fact that is recognized in problem-oriented diagnosis. One way to look at it is that if the patient thinks he or she has a problem related to the dentition and facial proportions, that is a reason for an orthodontic diagnostic evaluation.
Incorrect
That’s wrong. All these factors must be evaluated. Whether dental alignment and occlusion and/or facial proportions are a problem depends to a considerable extent on whether the patient thinks they are a problem. Some patients tolerate conditions that are not tolerable for others—a fact that is recognized in problem-oriented diagnosis. One way to look at it is that if the patient thinks he or she has a problem related to the dentition and facial proportions, that is a reason for an orthodontic diagnostic evaluation.
Question 2
At what point in orthodontic diagnosis is the process of classification used?
- As soon as problems are detected, typically during the interview
- In clinical examination, when the occlusion is evaluated
- When diagnostic records are ordered
- After the database is completed ✓
Correct
That’s right, classification (systematic description) is used to organize the information collected in the database after the interview and clinical examination have been completed and diagnostic records have been ordered and analyzed. The goal of modern classification is to obtain a list of the patient’s problems, taking everything into account. The classic Angle classification of malocclusion, therefore, is just one aspect of the larger process.
Incorrect
No, that’s wrong. Classification (systematic description) is used to organize the information collected in the database after the interview and clinical examination have been completed and diagnostic records have been ordered and analyzed. The goal of modern classification is to obtain a list of the patient’s problems, taking everything into account. The classic Angle classification of malocclusion, therefore, is just one aspect of the larger process.
Question 3
Which of the following are appropriate questions to be answered in the interview part of an orthodontic diagnostic evaluation?
a. Why are you seeking treatment, and why now?
b. How did things get to be the way they are now?
c. What is likely to change in the near future?
d. What do you (your parents) expect as a result of treatment?
- a and b
- b and c
- c and d
- a, b, and d
- all of the above ✓
Correct
That’s right, all these questions need to be answered during an orthodontic diagnostic evaluation. It’s important to know why the patient is seeking treatment, how things came to be as they are from the perspective of both medical/dental history and etiology, what is likely to change from the perspective of both pathology and growth, and what the patient expects as a result of treatment.
Incorrect
No, that’s wrong. All these questions need to be answered during an orthodontic diagnostic evaluation. It’s important to know why the patient is seeking treatment, how things came to be as they are from the perspective of both medical/dental history and etiology, what is likely to change from the perspective of both pathology and growth, and what the patient expects as a result of treatment.
Question 4
Which of the following are not goals of the clinical examination in an orthodontic diagnostic evaluation?
a. Evaluation of the alignment of the teeth b. Evaluation of the dental occlusion c. Evaluation of gingival/periodontal health d. Evaluation of TM joint function
- a and b ✓
- b and c
- c and d
- c only
- none of the above
Correct
That’s right. The dental alignment and occlusion can be evaluated better from the diagnostic records, so the clinical examination does not focus on these characteristics. Its goals are to evaluate facial proportions and tooth-lip relationships, the health of oral hard and soft tissues, and jaw function, and to determine what diagnostic records are needed, so the last two items are important goals of the clinical examination.
Incorrect
No, that’s wrong. The dental alignment and occlusion can be evaluated better from the diagnostic records, so the clinical examination does not focus on these characteristics. Its goals are to evaluate facial proportions and tooth-lip relationships, the health of oral hard and soft tissues, and jaw function, and to determine what diagnostic records are needed, so the last two items are important goals of the clinical examination.
Question 5
Which of the following is it important to look for in the frontal examination of the face?
a. Symmetry
b. Vertical facial proportions
c. Tooth-lip relationships
d. Lip protrusion
- a and b
- b and c
- a, b, and c ✓
- a, c, and d
- all of the above
Correct
That’s correct. Lip protrusion is better evaluated from the profile than the frontal view, so it is not included as a major goal of the frontal examination, whereas the other characteristics are examined in the frontal view. In the clinical examination, it is particularly important to examine tooth-lip relationships on smile and at rest, because these are difficult to capture completely in the diagnostic records.
Incorrect
No, that’s wrong. Lip protrusion is better evaluated from the profile than the frontal view, so it is not included as a major goal of the frontal examination, whereas the other characteristics are examined in the frontal view. In the clinical examination, it is particularly important to examine tooth-lip relationships on smile and at rest, because these are difficult to capture completely in the diagnostic records.
Question 6
On orthodontic clinical examination, what is the most important single indicator of whether TM joint function is within normal limits?
- Extent of maximal opening ✓
- Deviation on maximal opening
- Limited lateral excursion
- Limited protrusive movement
- TM joint sounds on opening
Correct
That’s right, all these characteristics could indicate a potential problem with the TM joint, but the most important single indicator of TM joint function is the extent of maximal opening. If any of the other findings like deviation on opening were present, the extent of maximal opening almost surely would be affected, so limited opening indicates particular care in examining other aspects of TM joint function.
Incorrect
No, that’s wrong. All these characteristics could indicate a potential problem with the TM joint, but the most important single indicator of TM joint function is the extent of maximal opening. If any of the other findings like deviation on opening were present, the extent of maximal opening almost surely would be affected, so limited opening indicates particular care in examining other aspects of TM joint function.
Question 7
Which of the following diagnostic records is least likely to be included in an orthodontic diagnostic evaluation?
- Panoramic radiograph
- Bitewing radiographs
- Lateral cephalometric radiograph
- P-A cephalometric radiograph ✓
- Facial photographs
Correct
That’s correct. The primary indication for a P-A cephalometric radiograph is clinically apparent facial asymmetry, which is relatively rare. The other records are taken routinely except for bitewing radiographs, which are included if there is clinical evidence of caries or if restorations are present. Bitewings are more likely to be needed than a P-A ceph.
Incorrect
No, that’s wrong. The primary indication for a P-A cephalometric radiograph is clinically apparent facial asymmetry, which is relatively rare. The other records are taken routinely except for bitewing radiographs, which are included if there is clinical evidence of caries or if restorations are present. Bitewings are more likely to be needed than a P-A ceph.
Question 8
Which of the following are important aspects of dental cast analysis?
a. Space analysis
b. Dental arch symmetry
c. Palatal width evaluation
d. Dental protrusion
- a and b
- b and c
- a, b, and c ✓
- a, c, and d
- all of the above
Correct
That’s right, dental protrusion cannot be evaluated from the dental casts and is not part of cast analysis, but space analysis, dental arch symmetry, and palatal width evaluation all are parts of cast analysis. The width of the palate is a skeletal dimension that can be seen on the dental casts, and if a posterior crossbite is present, it is particularly important to check whether the palate is narrow or whether the alveolar processes are tipped lingually.
Incorrect
That’s wrong. dental protrusion cannot be evaluated from the dental casts and is not part of cast analysis, but space analysis, dental arch symmetry, and palatal width evaluation all are parts of cast analysis. The width of the palate is a skeletal dimension that can be seen on the dental casts, and if a posterior crossbite is present, it is particularly important to check whether the palate is narrow or whether the alveolar processes are tipped lingually.
Question 9
On inspection of a cephalometric tracing, which of the following would indicate the prominence of the upper incisors?
a. Point A relative to N vertical line
b. Upper incisor relative to N vertical line
c. Inclination of upper incisor relative to SN
d. ANB angle
- a only
- b only ✓
- a and b
- a, b, and c
- all of the above
Correct
That’s right, the prominence of the upper incisor would be indicated by its position relative to a true vertical line dropped from nasion, but not by the other measurements. The inclination of the upper incisor to SN can be suggestive of incisor prominence, but the incisor can be tipped without being protrusive, so its inclination is only part of the picture. What counts is how far forward the incisal edge is. The position of point A relative to that line indicates the position of the maxilla, and the ANB angle indicates the relative position of the jaws—neither indicate tooth position.
Incorrect
That’s wrong. The prominence of the upper incisor would be indicated by its position relative to a true vertical line dropped from nasion, but not by the other measurements. The inclination of the upper incisor to SN can be suggestive of incisor prominence, but the incisor can be tipped without being protrusive, so its inclination is only part of the picture. What counts is how far forward the incisal edge is. The position of point A relative to that line indicates the position of the maxilla, and the ANB angle indicates the relative position of the jaws—neither indicate tooth position.
Question 10
Which of the following is not one of the five steps in systematic description of orthodontic problems?
- Patient’s reaction to the dental condition ✓
- Dental alignment/symmetry
- Dental protrusion/facial esthetics
- Transverse/posterior crossbite relationships
- Vertical/open-deep bite relationships
Correct
That’s right, the patient’s reaction to the dental condition is important in helping establish the need for treatment of orthodontic problems, but it is not part of systematic description. The other items are part of this 5-step process. Experience has shown that this grouping of problems makes it easier to keep up with the treatment possibilities for patients with severe problems—and the same diagnostic method is applicable to all potential orthodontic patients, however simple or complex their problems may be.
Incorrect
No, that’s incorrect. The patient’s reaction to the dental condition is important in helping establish the need for treatment of orthodontic problems, but it is not part of systematic description. The other items are part of this 5-step process. Experience has shown that this grouping of problems makes it easier to keep up with the treatment possibilities for patients with severe problems—and the same diagnostic method is applicable to all potential orthodontic patients, however simple or complex their problems may be.
Question 11
Which of the following are examined to evaluate the impact on facial esthetics of tooth and jaw positions?
a. Interview data
b. Clinical examination notes
c. Photographs
d. Cephalometric radiograph
- a, b, and c
- a, b, and d
- b, c, and d ✓
- all of the above
- none of the above, done in clinic
Correct
That’s right, clinical examination notes, photographs, and the cephalometric radiograph all are used to evaluate esthetic considerations—but interview data as to what the patient thinks are used later, not in this objective part of the evaluation.
Incorrect
No, that’s wrong. Clinical examination notes, photographs, and the cephalometric radiograph all are used to evaluate esthetic considerations—but interview data as to what the patient thinks are used later, not in this objective part of the evaluation.
Question 12
Which of the following would be noted during the last step in systematic description?
a. Anterior open bite
b. Posterior open bite
c. Deep bite
d. Mandibular asymmetry
- a, b, and c ✓
- a, b, and d
- b, c, and d
- all of the above
- none of the above, done in clinic
Correct
That’s right, the last step in systematic description is to evaluate vertical dental and skeletal relationships, using the dental casts, photographs, and lateral cephalometric radiograph. So open bite/deep bite are examined at this stage—but asymmetry is examined earlier, because it primarily affects the transverse plane of space.
Incorrect
No, that’s wrong. The last step in systematic description is to evaluate vertical dental and skeletal relationships, using the dental casts, photographs, and lateral cephalometric radiograph. So open bite/deep bite are examined at this stage—but asymmetry is examined earlier, because it primarily affects the transverse plane of space.
Question 13
Which of the following uses of cone-beam CT requires a large field of view?
- Analysis of skeletal asymmetry ✓
- Locating an impacted tooth
- Evaluation of an edentulous site to be restored with an implant
- 1 and 3
- 1 and 2
Correct
That’s correct. Analysis of skeletal asymmetry is a major indication for the use of CBCT in orthodontics and requires a field of view large enough to capture all of the craniofacial skeletal units. While CBCT is indicated for the localization of impacted teeth and implant planning, only a field of view large enough to visualize the teeth or site in question is needed.
Incorrect
No, that’s wrong. Analysis of skeletal asymmetry is a major indication for the use of CBCT in orthodontics and requires a field of view large enough to capture all of the craniofacial skeletal units. While CBCT is indicated for the localization of impacted teeth and implant planning, only a field of view large enough to visualize the teeth or site in question is needed.
Question 14
In examination of patients with temporomandibular pain and dysfunction (TMD), which of the following are advantages of MRI over cone-beam CT?
a. lower radiation dose b. no radiation dose c. better visualization of condyle and glenoid fossa d. better visualization of TM disk e. better visualization of cranial base
- all the above
- b, c, and d
- a, d, and e
- a and c
- b and d ✓
Correct
That’s right, MRI has no radiation dose and provides much better visualization of soft tissues, so both of those characteristics are better than CBCT in determining the extent of soft tissue problems (like a displaced disk) in patients with TMD. But it gives inferior views of hard tissues like the mandibular condyle and the glenoid fossa, and it costs more.
Incorrect
No, that’s incorrect. The correct answer is #5. MRI has no radiation dose and provides much better visualization of soft tissues, so both of those characteristics are better than CBCT in determining the extent of soft tissue problems (like a displaced disk) in patients with tempormandibular pain and dysfunction. But it gives inferior views of hard tissues like the mandibular condyle and the glenoid fossa, and it costs more.