Orthodontic Anchorage
Learning Objectives
An important aspect of carrying out orthodontic treatment is that the goal almost always is to move some of the teeth (perhaps a lot) while maintaining other teeth in their original position (or at least as close to it as possible). How do you do that? The answer is “With some difficulty, because this requires consideration of orthodontic anchorage”.
The objectives of this module are to help you understand anchorage, how it traditionally has been controlled, and how temporary skeletal anchorage is used in contemporary treatment.
In addition to going through the module, read pp. 328-346 and pp. 667-683 in the 5th edition of Contemporary Orthodontics, or pp. 377-393 and pp. 674-683 in the 4th edition**.
Orthodontic Anchorage: What Is It?
Anchorage usually refers to how a ship is held in place by an anchor that grasps the bottom beneath it, and is generalized to to how other structures are held in place against forces that would displace them.
Orthodontic anchorage is a special use of the term. It is best defined as “resistance to unwanted tooth movement”, which contains a reference to what the dentist desires. That seems a strange way to put it, but it’s the clearest way to understand what happens in typical orthodontic treatment. The dentist or orthodontist activates an orthodontic appliance to produce certain desired tooth movements. For every action, there’s an equal and opposite reaction, and the anchorage is the resistance to reaction forces. Usually it is provided by other teeth, occasionally by the palate, head or neck, and increasingly now by anchors screwed into the bone.
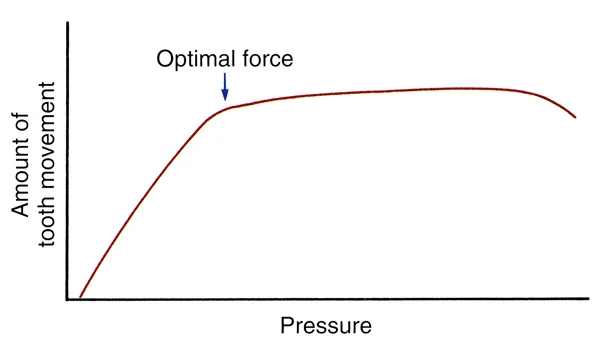
Let’s begin with other teeth as anchor units. The essence of anchorage is its use to produce differential tooth movement, which is more movement of the teeth you’re trying to move than of the teeth that you don’t want to move. That’s done by taking advantage of the relationship of tooth movement to pressure in the periodontal ligament (PDL), as shown in this graph. What’s the optimal force for moving a tooth? It’s the lightest force (and resulting pressure in the PDL) that will produce tooth movement at a near-maximum rate. Why is that the optimal force? Because of anchorage considerations that we need to discuss.
Pressure in the PDL and Differential Tooth Movement
How can you arrange things with dental anchorage so that differential tooth movement occurs? The slope of the curve gives the answer: that could occur only if the pressure in the PDL of the anchor teeth was less than the pressure in the PDL of the tooth you’re trying to move, and if you were on the vertical leg of the graph.
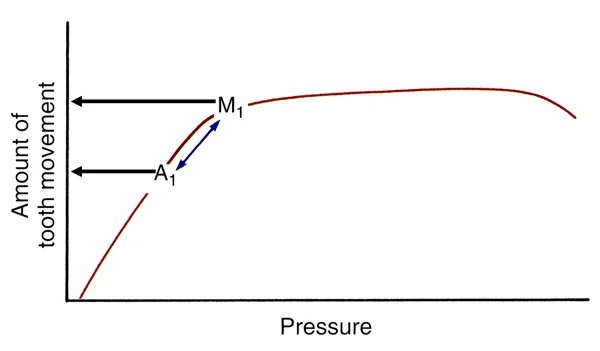
Consider the situation when the reaction force for movement of one tooth (M1 on the graph) is spread over two or more teeth that serve as anchors (A1). The reaction force is equal and opposite, but because it is distributed over a larger PDL volume, PDL pressure would be lower for the anchor teeth. They would move less than the tooth on which the force was concentrated. The larger the PDL volume over which the reaction force was distributed relative to the tooth we’re trying to move, the greater the relative movement would be.
As a general guideline, the ratio between PDL pressures for the movement tooth and anchor teeth should be at least 3:1. The larger the ratio, the better the anchorage, and vice versa.
Pressure in the PDL and Differential Tooth Movement (cont.)
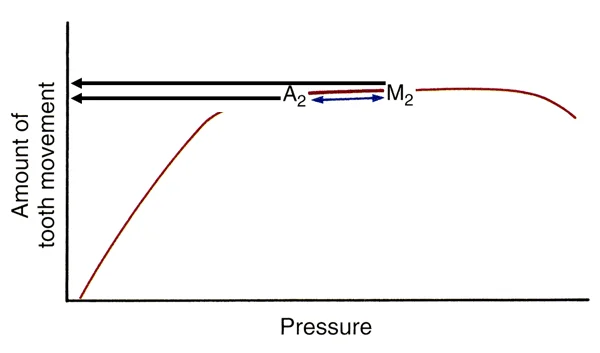
What would happen if you increased the force against the tooth you’re trying to move, so that it was greater than the optimal force? Dentists often act as if they believe the old adage that “if a little bit is good, more must be better”. Increasing the force against the movement tooth would equally increase the reaction force. The effect would be to move M2 and A2 further along the response curve.
Note the unintended effect: now the movement tooth moves only a little more than it did with the optimal force, while the anchor teeth move a lot more. The heavier force was meant to increase the desired tooth movement. What it really did was increase the undesired tooth movement. This is referred to as “burning the anchorage”, or perhaps as “blowing or “slipping” it. Whatever you call it, using more than the optimal force destroys the anchorage value of the teeth that were meant to provide anchorage.
The important principle is that light forces allow control of anchorage and heavy forces make anchorage control impossible.
Anchorage Value of Different Teeth
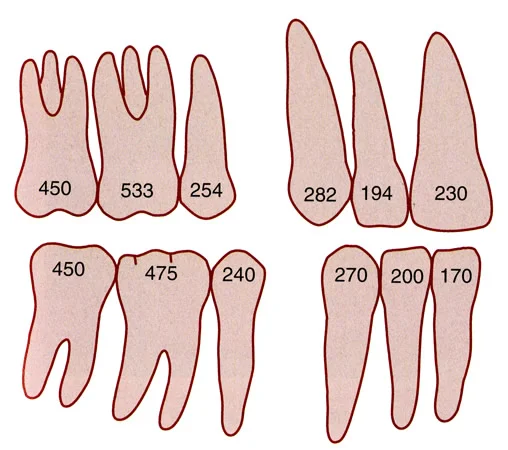
It should be apparent now that all teeth are not created equal from an anchorage perspective. The bigger the tooth and the larger its PDL volume, the greater its anchorage value should be.
It’s hard to calculate the PDL volume, but because only one part of the total volume is loaded at any one time, a two-dimensional representation of PDL area actually is more useful in determining the anchorage value of a given tooth. It’s certainly true that the anchorage value of a canine is greater than that of an incisor, and the anchorage value of a molar is greater than that of a canine. You can turn that around. If a canine is to be moved, more force will be needed to do so, and there would be more stress on the anchor teeth than if an incisor was being moved.
This image shows the calculated anchorage value of various teeth. The relative values, not the absolute numbers, are what we’re interested in.
Types of Anchorage
Reciprocal Anchorage
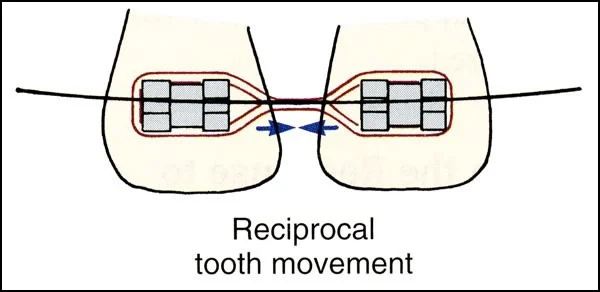
The simplest type of anchorage is called reciprocal anchorage. It would occur when movement of one tooth (like a maxillary central incisor) was pitted against one exactly like it (the other central incisor). That could easily occur in the closure of a maxillary central diastema. Not surprisingly, the result would be that both teeth would have the same pressure in the PDL, and they would move toward each other equally.
The same thing would happen if one group of teeth were pitted against another group with equal anchorage value. Suppose the first molar and second premolar were the anchorage unit for retraction of the canine and two incisors after first premolar extraction. If you look back at the previous figure, you’ll see that the anchorage values of those teeth are close to the same. All other things being equal, the tooth movement would be reciprocal or close to it.
Reinforced Anchorage
Suppose the goal was to close a first premolar extraction space by retracting the incisors and canine more than the premolar and molar moved forward. One strategy would be to add the second molar to the posterior anchorage unit. That would increase the anchorage value of the posterior unit. Now you would have to be sure that the force was optimal for moving the anterior teeth. If so, the force against the posterior anchor unit would produce a PDL pressure below the optimal level, and those teeth would not move forward as much (image 1). Adding the extra molar to the anchorage unit is described as “reinforcing the anchorage”.
The principle of reinforcement of anchorage can be generalized to refer to anchorage outside the dental arch. One example is the use of extra-oral force (headgear) to reinforce anchorage. Could you control forward movement of posterior anchorage by having your patient wear headgear to the upper first molars (image 2)? The answer would have to be yes, because the headgear force would counteract some of the reaction force from the anterior teeth.
Unfortunately neither the magnitude nor the duration of headgear force is conducive to reinforcing anchorage. Ideally, the amount of force would be light and its duration would be very long if not continuous. Headgear force tends to be heavy, and even the most conscientious patient doesn’t come close to wearing it all the time. Headgear for growth modification is more successful than headgear for anchorage reinforcement. The wrong force and duration for tooth movement explain why.
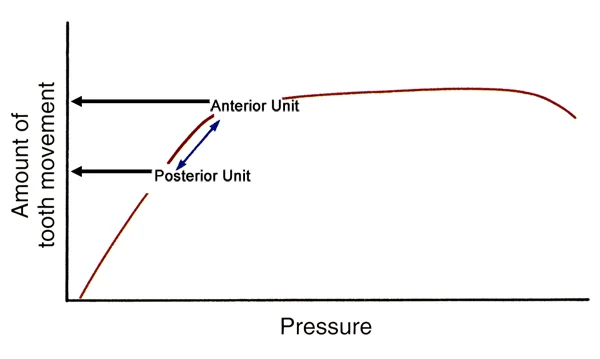 Image 1 Image 1 |  Image 2: Headgear like this is ineffective as reinforcement of posterior anchorage. Image 2: Headgear like this is ineffective as reinforcement of posterior anchorage. |
Stationary Anchorage
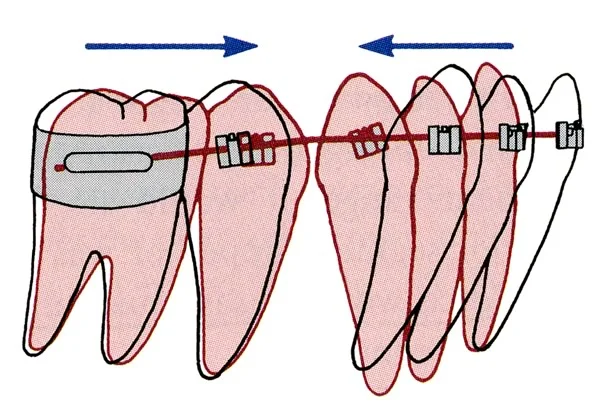
Another strategy to increase the anchorage value is to take advantage of the different loading of the PDL for bodily movement vs. tipping. Since a force is distributed over twice as much PDL area for bodily movement as for tipping, you would move a tooth twice as much as its anchor if the anchor could only move bodily while the movement tooth was allowed to tip. Arranging the force and moments on the anchor unit so those teeth can only move bodily is called “stationary anchorage”.
This strategy applies very well to the situation when an anterior unit (canine plus incisors) is to be retracted more than its posterior anchor unit moves forward. If the incisors are allowed to tip while the posterior teeth have to move bodily, the optimum pressure for the anterior unit would be produced by about half as much force as if those teeth were to be moved bodily. The reaction force over the posterior unit would be only half the amount for optimal bodily movement, and then the anterior teeth would be retracted twice as much. This image shows the outcome.
That’s not a total net gain because the roots of the anterior teeth would have to be repositioned later, but two-stage movement of a unit to be moved often is used to reduce the strain on anchorage. Again, note that this works only if the force is kept below the optimum for movement of the anchor unit. Using too much force would totally destroy this method of anchorage control.
Cortical Anchorage
It is obvious that anchorage could be both reinforced and stationary, and the combination of more teeth in the anchor unit and allowing the anchor teeth only to move bodily is frequently used clinically.
Another aspect of anchorage is seen in the different remodeling response of cortical and medullary bone. Teeth normally are in medullary bone, which remodels relatively quickly adjacent to a stressed PDL. Cortical bone can and does remodel, but it does so much more slowly. You can say that cortical bone has a higher anchorage value, but usually when it’s a factor in anchorage, it opposes the desired tooth movement, so it creates greater resistance to tooth movement rather than contributing to the anchorage.
A good example is seen in the area where a tooth was lost years previously (images 1 and 2). Almost always the alveolar process has become narrower and shorter. Closing a space like that requires remodeling of cortical bone, and that puts great stress on anchor teeth. An old extraction site, particularly in adults, can be so difficult to close that often it is not good judgment to try to do it.
 Image 1: Early loss of 2nd primary molars in a patient with congenital absence of 2nd premolars has led to narrowing of the alveolar ridge. Closing the space will require remodeling of cortical bone. Image 1: Early loss of 2nd primary molars in a patient with congenital absence of 2nd premolars has led to narrowing of the alveolar ridge. Closing the space will require remodeling of cortical bone. |  Image 2: Early loss of 1st molars in this adult, with loss of alveolar ridge width and height, has created a space that will be very difficult to close orthodontically. Image 2: Early loss of 1st molars in this adult, with loss of alveolar ridge width and height, has created a space that will be very difficult to close orthodontically. |
Resistance to Sliding and Anchorage Control Strategies
In our previous discussion of modern fixed appliances, we have already touched on resistance to sliding, which cannot be avoided in patients (though it can in a laboratory where brackets are moved along a wire without the inconvenience of having roots on teeth). Laboratory data of that type can look good in an advertising brochure but are irrelevant to clinical treatment.
Let’s consider the impact of resistance to sliding (RS) on anchorage, using the familiar setting of closure of an extraction space when retraction of protruding incisor teeth is desired. A 60-40 ratio of anterior to posterior movement (image 1) often is all that is needed. Too much retraction of the anterior teeth can have an adverse effect on lip support and facial appearance.
If you wanted to retract the anterior segment further than that, what would you do? Reinforce the anchorage, of course, or make it stationary while allowing the anterior teeth to tip. It’s possible to use the teeth in the opposite arch for anchorage reinforcement (image 2), and there’s also an exciting new possibility that we’ll discuss at the end of this module.
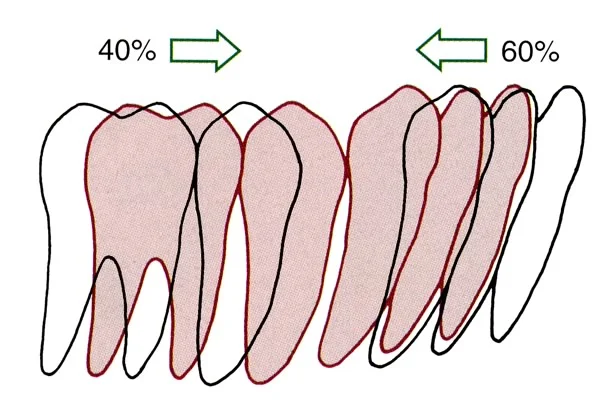 Image 1: After first premolar extraction, retracting the canine and 2 incisors creates about a 60:40 ratio—which often is as much incisor retraction as is desired. Image 1: After first premolar extraction, retracting the canine and 2 incisors creates about a 60:40 ratio—which often is as much incisor retraction as is desired. | 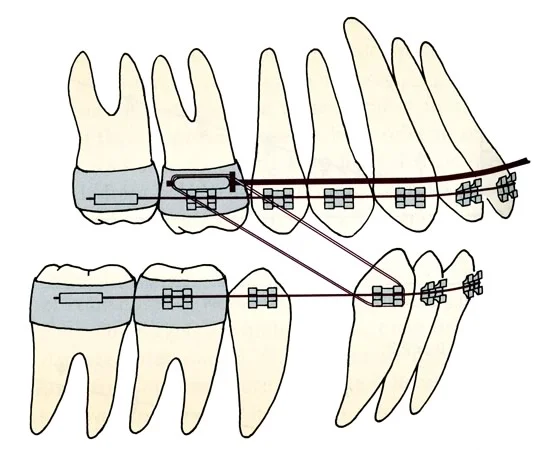 Image 2: Anchorage can be reinforced is several ways, including elastics from the other arch. Image 2: Anchorage can be reinforced is several ways, including elastics from the other arch. |
Resistance to Sliding and Anchorage Control Strategies (cont.)
How much force does it take to move the canine and 2 incisors (on each side) posteriorly? The canine will need to move bodily (100 gm), the incisors can be allowed to tip back somewhat (~75 gm each), with a total of about 250 gm per side. But if an archwire has to slide through brackets on the posterior teeth, at least 100 gm has to be added to overcome the RS. The result will be force levels on the posterior teeth that pull them up toward if not onto the plateau of the force / response curve, decreasing their anchorage value.
The problem is aggravated because RS cannot be known precisely, and the clinician is tempted to be sure there’s enough force to close the space—so the amount of force is likely to be moved up. Even if the anchorage is reinforced by adding the second molars, the posterior teeth are likely to move forward as much as the anterior ones move back.
What to do? If space closure by sliding is planned, the space closure almost has to be done in two stages, first retracting the canine (100 gm + RS), then adding it to the posterior anchorage unit as the incisors are retracted (image 1). There still will be forward movement of the posterior anchor teeth, but this two-stage method allows more retraction of the incisors.
The alternative is to move segments of wire with the teeth attached, so that there is no sliding of brackets along a wire (image 2). This can be accomplished with loops that form the retraction spring. Then the typical incisor retraction could be achieved in one step, pitting the entire anterior segment against the posterior anchorage. The price of resistance to sliding then becomes clearer: the difficulty of controlling anchorage as teeth slide along an archwire increases treatment time to achieve the desired result.
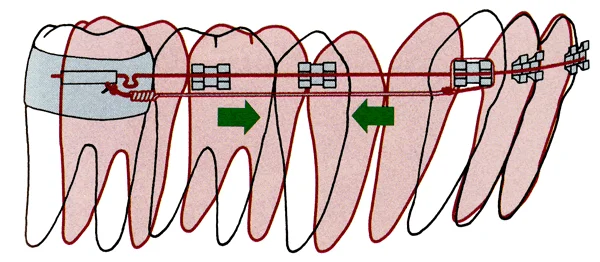 Image 1: Two-stage space closure, retracting the canine by itself initially, then retracting the incisors, decreases the strain on posterior anchorage. Image 1: Two-stage space closure, retracting the canine by itself initially, then retracting the incisors, decreases the strain on posterior anchorage. |  Image 2: Closing loops of this type eliminate strain on anchorage from resistance to sliding, and allow one-step space closure (which reduces treatment time). Image 2: Closing loops of this type eliminate strain on anchorage from resistance to sliding, and allow one-step space closure (which reduces treatment time). |
Complex Force Systems
Determinate vs. Indeterminate Force Systems
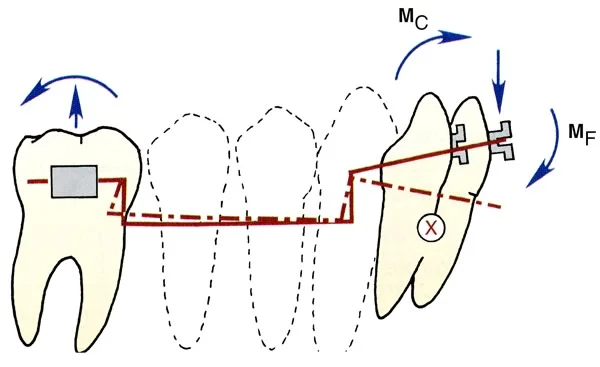
By now you should be convinced that in order to control tooth movement, it’s necessary to be careful to use the right amount of force and use couples appropriately to obtain the desired MF / MC ratio. Otherwise, it’s easy to destroy the value of dental anchorage. It can be surprisingly difficult to be sure what forces and moments are produced by an orthodontic appliance because as the force system becomes more complex, it also is likely to become indeterminate.
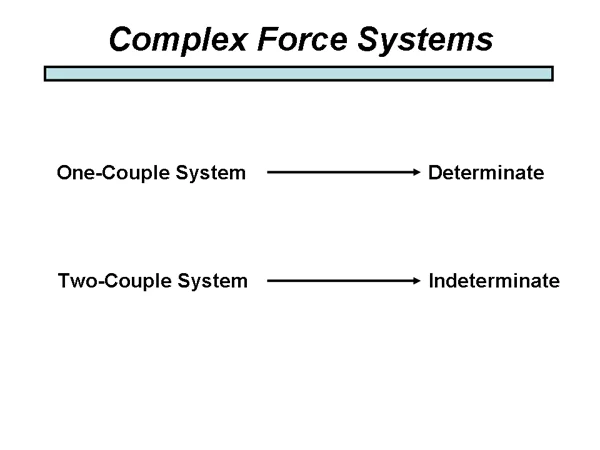
A determinate force system means that you can measure, and therefore determine, the force and moments felt by all teeth. An indeterminate force system means that it is impossible to know exactly what forces and moments are produced.
What makes a force system indeterminate? The answer is that a one-couple system is determinate, while two-couple systems are indeterminate. What’s a one-couple system? Simply a system in which a couple is present at only one place, and a force or forces without a couple are felt elsewhere. Two-couple systems have forces and couples present in at least two places.
Determinate vs. Indeterminate Force Systems (cont.)
Removable appliances rarely become two-couple systems—they have enough trouble producing one moment, much less two. So although they are not very efficient, you can at least know what forces and moments are being delivered.
Multi-bracketed fixed appliances with a continuous arch wire easily become two-couple systems. A two-couple system is guaranteed if you place a continuous rectangular wire in more than one rectangular bracket. The rectangular wire creates a couple within the bracket in the torque plane of space if there is any twist when it is inserted (image 1), and the wire also can create couples across the bracket in the mesio-distal inclination plane of space if it is not passive when it is inserted. A round wire also can produce couples across a bracket if the wire is flexed as it goes into the bracket (image 2). You can picture that with this wire, the root of the maxillary right central incisor would be moved mesially as the teeth are aligned because of the inclination of the wire across the bracket. The result is that with a typical fixed appliance, it’s impossible to know exactly what the forces and moments on individual teeth are.
Up to this point you’ve probably thought about orthodontic tooth movement being a smooth continuous action. With a fixed appliance it’s not, it’s more like a dance of the teeth. When the wire is inserted, a complex force system (almost surely a two-couple system) is established. As tooth movement begins, one tooth moves a little, which changes the force system and produces a response by another tooth, and so on. If you made a movie from images taken every 10 minutes over several days, you’d have something like one you’ve probably seen that shows a flower unfolding as the blossom opens. The dance is tolerable because the form of the arch wire limits how far teeth can move, and so the outcome is predictable although the steps to get there are not.
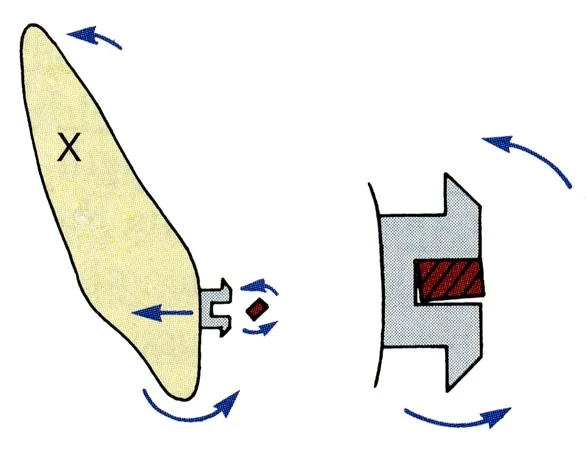 Image 1: A rectangular wire in a rectangular bracket produces a torque couple unless its orientation precisely matches that of the bracket. Image 1: A rectangular wire in a rectangular bracket produces a torque couple unless its orientation precisely matches that of the bracket. |  Image 2: A round wire like this produces couples across brackets, so the force system becomes indeterminate. Image 2: A round wire like this produces couples across brackets, so the force system becomes indeterminate. |
Intrusion: A Major Indication for a One-Couple System
You will remember that intrusion requires very light force, on the order of 10 gm / tooth. With even the springiest superelastic NiTi wire, the force between brackets on adjacent teeth will be about 50 gm, which is perfect for tipping teeth into alignment. But if the brackets are not vertically aligned, there also will be a extrusive force of 50 gm on one tooth and a 50 gm intrusive force on the somewhat elongated one next to it. That’s also perfect for extrusion, but the 50 gm intrusive force has no effect until undermining resorption can take place, and that’s particularly slow because of the dense bone beneath the teeth.
The result is that a continuous arch wire is extrusive. It aligns the brackets much more by extruding a relatively depressed tooth than by intruding an elongated one.
How do you set up an appliance for intrusion? This requires two things: a long span of wire that bypasses some teeth (so that it will deliver the necessary light force), and the absence of a couple where it attaches to the incisor teeth. A light round steel wire from bands on first molars to brackets only on the incisors (image 1) can meet both of these requirements. It’s often called a 2 x 4 appliance: 2 molar bands, 4 incisor brackets. It can generate a light vertical force at the incisors, and it produces a couple across the molar tube but doesn’t create a couple anteriorly. The problem is that the two molars aren’t much anchorage, and the reaction force from the incisors tends to tip the molars distally.
Better control is obtained by creating a multi-tooth anchorage segment, and using a one-couple intrusion arch formed from a rectangular wire. It inserts into an auxiliary tube on the molar but bypasses the brackets on other teeth, and is tied to a segment of wire in the teeth to be intruded (image 2). Tying it to the wire rather than placing it into the brackets keeps it a one-couple system, so that the intrusion force can be measured precisely. For two teeth to be intruded, it should deliver 20 gm.
 Image 1: 2 x 4 appliance. The long span from molar to incisor allows the light force necessary for intrusion. Image 1: 2 x 4 appliance. The long span from molar to incisor allows the light force necessary for intrusion. | 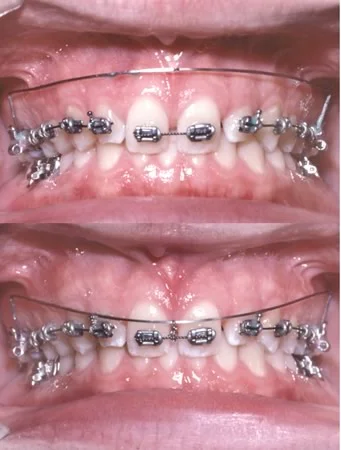 Image 2: Auxiliary intrusion arch to intrude two maxillary central incisors. The intrusion arch is formed from rectangular wire but is tied anteriorly so that there is no couple. Image 2: Auxiliary intrusion arch to intrude two maxillary central incisors. The intrusion arch is formed from rectangular wire but is tied anteriorly so that there is no couple. |
Intrusion: Where Force Magnitudes Are Really Important
An easy way to see the effect of changing from a one-couple to a two-couple system is to tie a rectangular intrusion arch into the brackets on incisors. This creates one couple at the molar, another couple anteriorly. The clinical observation is that such an auxiliary intrusion arch is unpredictable in its effects. Sometimes excellent intrusion is obtained. Sometimes there is little intrusion, with reaction forces strongly expressed at the molars. Why? Because even though the wire is adjusted so that it would deliver a 30-40 gm intrusion force (appropriate for 4 lower incisors) when it’s deflected up to the level of the bracket, as soon as it’s tied into the anterior brackets, the actual intrusion force is unknown.
The bottom line: you can’t intrude teeth with a continuous arch wire, and for all practical purposes you can’t do it with a two-couple system even if it bypasses brackets to reduce the force it delivers. You can do it predictably with a one-couple system.
Applications of Temporary Skeletal Anchorage
Ankylosed Teeth: Perfect Anchorage
Suppose you had to deal with an ankylosed tooth that needed to be repositioned. What would happen if you pulled against it? Once even a small part of the tooth root is fused to the bone (no PDL in that area), the tooth can’t move no matter how hard you pull on it. Any tooth movement would occur in what was meant to be the anchorage unit.
That unfortunate situation occurs sometimes during efforts to bring a badly impacted maxillary canine into the arch. If the canine ankyloses before it reaches its normal position in the arch and efforts to move it continue, there can be major displacements of the other maxillary teeth. The only way to move an ankylosed tooth is to create a bony segment that includes it, and move the segment by distraction osteogenesis. Although that’s possible, it’s rarely feasible. Usually it’s better to extract such a tooth—especially now that an implant to replace it is quite possible.
On the other hand, an ankylosed tooth would be perfect anchorage if it was in the right place. Since an implant is the equivalent of an ankylosed tooth, could it serve as an anchor for tooth movement? Yes, it can. Implants easily withstand the light forces needed to move other teeth. An implant that was placed to support a restoration can also serve as an orthodontic anchor, as these images show.
 Image 1: The edentulous space behind the lower second premolar is to be restored with an implant that also can serve as an anchor for reduction of the patient’s overjet. Image 1: The edentulous space behind the lower second premolar is to be restored with an implant that also can serve as an anchor for reduction of the patient’s overjet. | 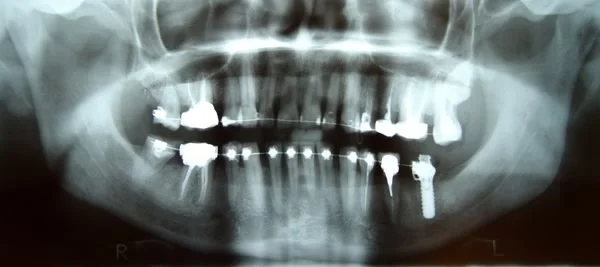 Image 2: The implant has been incorporated into the orthodontic appliance, to serve as anchorage for retraction of the anterior teeth. Image 2: The implant has been incorporated into the orthodontic appliance, to serve as anchorage for retraction of the anterior teeth. |
 Image 3: The implant serves as perfect anchorage as Class II elastics are used during the pre-prosthetic orthodontic treatment. Image 3: The implant serves as perfect anchorage as Class II elastics are used during the pre-prosthetic orthodontic treatment. |
Temporary Skeletal Anchorage
Would it be possible to place a skeletal anchor that, unlike a typical implant for restorative purposes, would be easily removable after its orthodontic use? The answer to that also is yes. Temporary anchorage devices (TADs) now are coming into widespread use in orthodontics, especially in adults but also in adolescents. The lower age limit for TADs is about age 11. In children younger than that, the bone is not mature enough to maintain a bone anchor.
TADs take two forms: bone screws placed in alveolar bone, and mini-plates that are attached to basal bone beneath the teeth by multiple bone screws. Bone screws work very well when they serve as the anchorage for repositioning specific teeth. Mini-plates are advantageous when more extensive tooth movement is needed.
A typical application of a bone screw as an anchor for tooth movement is shown in the attached images. The goal for this patient, who had lost almost all her posterior teeth, was to align the remaining lower anterior teeth without protruding them. There weren’t any posterior teeth to serve as anchorage. A single bone screw was placed into the remaining alveolar bone on the right side. It provided the anchorage to retract the first premolar so that the canine could be rotated into proper position. Then comprehensive prosthodontic treatment could be done without concern for the occlusal interference posed by the displaced canine or any need to adapt the partial denture (whether fixed or removable) to the irregular anterior teeth.
 Image 1: Canine crossbite and interference prior to treatment Image 1: Canine crossbite and interference prior to treatment |  Image 2: Pre-treatment occlusal view Image 2: Pre-treatment occlusal view |
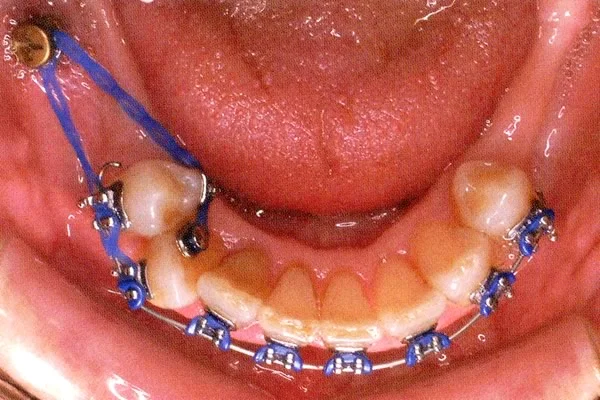 Image 3: Retraction of the first premolar Image 3: Retraction of the first premolar |  Image 4: Rotation of the canine (with a superelastic wire segment) Image 4: Rotation of the canine (with a superelastic wire segment) |
 Image 5: Alignment completed, ready for comprehensive prosthodontics Image 5: Alignment completed, ready for comprehensive prosthodontics |
Uses of Temporary Skeletal Anchorage
There are now four major applications of temporary skeletal anchorage in adults:
- positioning individual teeth when no other satisfactory anchorage is available (as shown on the previous screen)
- intrusion of posterior teeth to close an anterior open bite
- retraction and intrusion of protruding maxillary incisors
- distal movement of molars (and the entire maxillary or mandibular arch if needed)
It now is possible also to use skeletal anchorage in growth modification treatment for young adolescents.
The above list shows an increasing need for mini-plates as opposed to isolated alveolar bone screws.
Protruding Maxillary Incisors
Retraction of maxillary incisors with TADs can be done in three ways: using bone screws in the palate to stabilize a lingual arch that holds the posterior anchor teeth in position (image 1); using bone screws in the alveolar process posteriorly (image 2); or using mini-plates placed at the base of the zygomatic arch, with an arm projecting into the vestibule (images 3 and 4).
Bone screws provide excellent anchorage, but their position determines the vertical aspect of force against them. Often it is desirable to intrude severely protruding incisors as they are retracted, because tipping them to produce a more normal orientation brings the incisal edges down. Palatal anchorage makes this very difficult. The vertical position of bone screws can be adjusted to some extent, but screws need to be placed in attached gingiva rather than alveolar mucosa, which can make it difficult to obtain a vertical direction of force.
Mini-plates have the great advantage that a wire can be attached to the arm that extends into the oral cavity, so that the point of force application can be almost anywhere.
 Image 1: A palatal bone screw stabilizes a premolar-to-premolar lingual arch, to provide anchorage to retract the protruding and spaced upper incisors. Image 1: A palatal bone screw stabilizes a premolar-to-premolar lingual arch, to provide anchorage to retract the protruding and spaced upper incisors. |  Image 2: A bone screw in alveolar bone between the premolars provides anchorage to retract the incisors without forward movement of the posterior teeth. Image 2: A bone screw in alveolar bone between the premolars provides anchorage to retract the incisors without forward movement of the posterior teeth. |
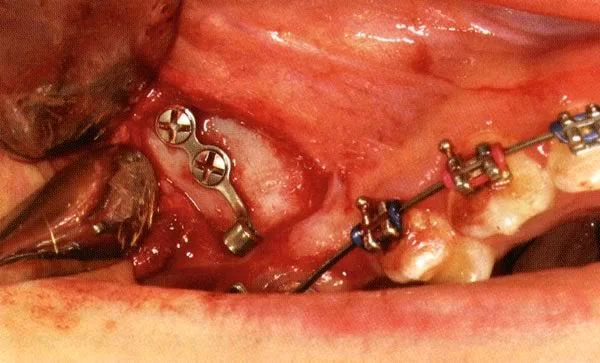 Image 3: Mini-plates usually are placed at the base of the zygomatic arch above the roots of the teeth and are held by multiple screws. Image 3: Mini-plates usually are placed at the base of the zygomatic arch above the roots of the teeth and are held by multiple screws. |  Image 4: A wire segment can be extended from the tube at the end of the mini-plate. This allows the anchor point to be adapted as needed, so that a straight posterior pull as shown here (or any other force direction) can be obtained. Image 4: A wire segment can be extended from the tube at the end of the mini-plate. This allows the anchor point to be adapted as needed, so that a straight posterior pull as shown here (or any other force direction) can be obtained. |
Protruding Maxillary Incisors (cont.)
The young adult seen in these images had protruding maxillary incisors, and was treatment-planned for retracting the incisors into a first premolar extraction site. For him, skeletal anchorage was particularly indicated because he needed space closure with maximum incisor retraction—and he had posterior bone loss from previous periodontal disease that decreased the anchorage value of the posterior teeth. The lower arch would be treated without extraction, bringing the lower incisors forward.
 Image 1: Maxillary incisor protrusion and deep bite anteriorly, prior to treatment. Image 1: Maxillary incisor protrusion and deep bite anteriorly, prior to treatment. |  Image 2: The pre-treatment molar relationship was nearly a full Class II, and the goal was to maintain the posterior segment in that relationship. Image 2: The pre-treatment molar relationship was nearly a full Class II, and the goal was to maintain the posterior segment in that relationship. |
 Image 3: The extent of incisor protrusion can be seen in the pre-treatment ceph. Image 3: The extent of incisor protrusion can be seen in the pre-treatment ceph. |
Retraction of Maxillary Incisors
Miniplates were placed bilaterally at the base of the zygomatic arch, and a superelastic NiTi spring delivering 200 gm was attached to the mini-plate and used to begin retraction of the incisors with an upward and posterior direction of force (image 1). This is termed direct anchorage, i.e., the spring is attached directly to the TAD. Then, to obtain a more directly posterior force direction, an arm was fastened to the mini-plate’s intra-oral attachment to stabilize the maxillary molar. This use of TADs is termed indirect anchorage (image 2).
The dental occlusion at the completion of treatment (which required 18 months) is shown in images 3 and 4, and cephalometric superimposition from before to after treatment is shown in image 5. Note the lack of movement of the upper molar as the maxillary incisors were retracted.
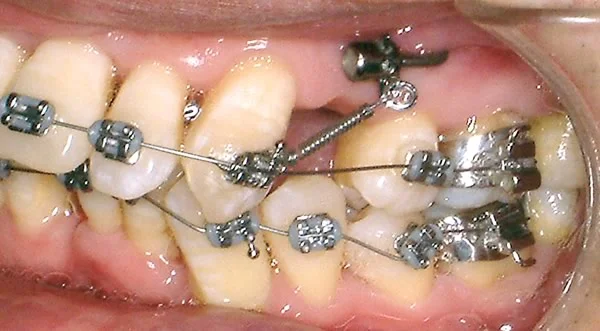 Image 1: NiTi spring attached to end of arm from mini-plate. Image 1: NiTi spring attached to end of arm from mini-plate. | 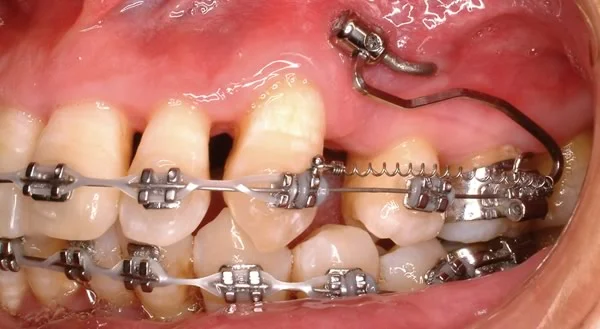 Image 2: An auxiliary arm from the miniplate attachment, stabilizing the molar to allow horizontal direction of retraction force. Image 2: An auxiliary arm from the miniplate attachment, stabilizing the molar to allow horizontal direction of retraction force. |
 Image 3: Post-treatment occlusion, overjet and overbite corrected. Image 3: Post-treatment occlusion, overjet and overbite corrected. |  Image 4: Posterior occlusion, Class II molar relationship with good interdigitation. Image 4: Posterior occlusion, Class II molar relationship with good interdigitation. |
 Image 5: Superimposition tracings on cranial base, maxilla and mandible. Image 5: Superimposition tracings on cranial base, maxilla and mandible. |
Distal Movement of Maxillary Arch
Placing a bone screw between teeth makes it impossible to move all the teeth posteriorly. With mini-plate anchorage against the zygomatic buttress, above the roots of the teeth, it is possible to move the entire maxillary arch posteriorly—but there has to be space available, so extraction of third molars is necessary before this can be done. For some patients, second molar extraction may be needed so that the rest of the teeth can be moved back.
For this patient, orthognathic surgery to advance the mandible was one possible treatment; distalization of the maxillary arch was an alternative because it also would give acceptable facial appearance. Moving the upper teeth back, of course, is a form of camouflage—which is satisfactory only if the facial appearance is satisfactory after treatment.
As the facial images and ceph show, her maxillary incisors were already crowded and tipped lingually, so she already had a form of Class II camouflage. The upper incisors could end up almost in their initial position if they were retracted after being aligned.
 Image 1: Pre-treatment frontal view Image 1: Pre-treatment frontal view |  Image 2: Pre-treatment profile Image 2: Pre-treatment profile |
 Image 3: Pre-treatment right lateral view: note the Class II molar relationship Image 3: Pre-treatment right lateral view: note the Class II molar relationship |  Image 4: Pre-treatment maxillary occlusal view: note the incisor crowding Image 4: Pre-treatment maxillary occlusal view: note the incisor crowding |
 Image 5: Pre-treatment ceph. In essence, the maxillary incisors have already been retracted naturally as they crowded - so minimal further retraction is needed. Image 5: Pre-treatment ceph. In essence, the maxillary incisors have already been retracted naturally as they crowded - so minimal further retraction is needed. |
Distal Movement of Maxillary Arch (cont.)
Initial alignment of the upper incisors created overjet (image 1). At that point 150 gm retraction force was employed (image 2), and after 3 months it was increased to 300 gm (image 3). At 14 months, the molar relationship was Class I (image 4), the maxillary incisors were in their planned position, and a lower fixed appliance was added.
In the cephalometric superimposition from pre-treatment to 14 months (image 5), note the distal movement of the molar and the position of the upper incisors (which were tipped forward into alignment, then retracted along with the rest of the maxillary arch).
 Image 1: Note the incisor protrusion after initial alignment Image 1: Note the incisor protrusion after initial alignment |  Image 2: NiTi coil spring to stabilize the canine position during alignment of the incisors. Image 2: NiTi coil spring to stabilize the canine position during alignment of the incisors. |
 Image 3: Heavier coil spring force for distalization of entire arch Image 3: Heavier coil spring force for distalization of entire arch |  Image 4: Progress, molar relationship now Class I Image 4: Progress, molar relationship now Class I |
 Image 5: Superimposition tracings at completion of distalization Image 5: Superimposition tracings at completion of distalization |
Distal Movement of Maxillary Arch (cont.)
The post-treatment smile and profile (images 1 and 2) were quite satisfactory, as was the dental occlusion and alignment (images 3 and 4). Treatment time was 26 months. Note that the mini-plates are still present in the final photographs—they were removed soon thereafter.
The cephalometric superimposition for the total treatment is shown in image 5. Note that the mandible was rotated down and back somewhat in the final stage of treatment, giving her greater anterior face height at the cost of decreased chin prominence.
 Image 1: Post-treatment smile Image 1: Post-treatment smile |  Image 2: Post-treatment profile Image 2: Post-treatment profile |
 Image 3: Post-treatment occlusion: Class I molar relationship achieved Image 3: Post-treatment occlusion: Class I molar relationship achieved |  Image 4: Post-treatment alignment of maxillary incisors Image 4: Post-treatment alignment of maxillary incisors |
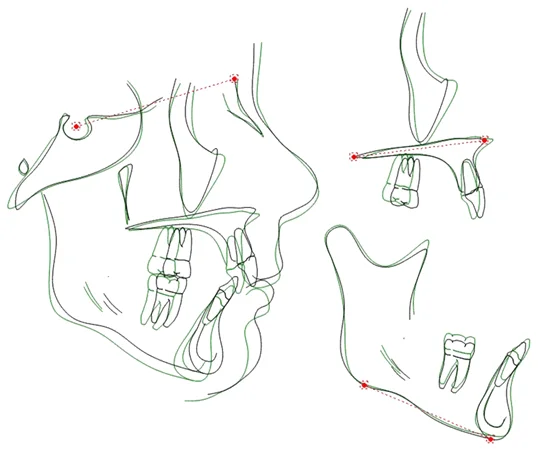 Image 5: Post-treatment superimposition tracings: note the alignment of the maxillary incisors without protrusion Image 5: Post-treatment superimposition tracings: note the alignment of the maxillary incisors without protrusion |
Posterior Intrusion to Correct Anterior Open Bite
Mini-plates above the maxillary posterior teeth also allow a vertical force for intrusion. For many years there was a joke about intruding those teeth, which often are elongated in anterior open bite patients: “If only there was a sky hook over the patient’s head…”. Now mini-plates can provide the sky hook.
Not all open bite patients, of course, need intrusion of maxillary posterior teeth, but usually an anterior open bite is caused by posterior teeth that are elongated rather than incisors that haven’t erupted enough. Often the vertical position of the posterior teeth is influenced by downward rotation of the maxilla during growth, and the more severe the skeletal problem, the more likely that the patient would need orthognathic surgery. But for patients with a mild to moderate open bite, intrusion of maxillary posterior teeth now offers an alternative to the maxillary surgery that was the only treatment until quite recently.
The patient shown in these images had a 6 mm open bite and mild elongation of her lower face. Intruding the maxillary posterior teeth would allow the mandible to rotate upward and forward, closing the anterior open bite and improving her facial proportions.
 Image 1: Pre-treatment: note the display of the maxillary incisors, which is good—so elongation of these teeth to correct her anterior open bite would be unesthetic. Image 1: Pre-treatment: note the display of the maxillary incisors, which is good—so elongation of these teeth to correct her anterior open bite would be unesthetic. |  Image 2: This degree of anterior open bite had developed as she experienced vertical growth after orthodontic treatment in early adolescence. Image 2: This degree of anterior open bite had developed as she experienced vertical growth after orthodontic treatment in early adolescence. |
 Image 3: Anterior open bite from canine to canine. Image 3: Anterior open bite from canine to canine. |  Image 4: Class II tendency in posterior occlusion. Image 4: Class II tendency in posterior occlusion. |
 Image 5: Pre-treatment ceph, showing mild downward-back rotation of the mandible and increased anterior face height. Image 5: Pre-treatment ceph, showing mild downward-back rotation of the mandible and increased anterior face height. |
Posterior Intrusion Treatment
The plan for this patient was intrusion of the maxillary posterior segments initially, and then a complete orthodontic appliance after the bite was closed.
Rather than a miniplate, a long bone screw was placed into the base of the zygomatic arch, after the roots of the 1st molars and 2nd premolars had been diverged to make space for it (image 1). A splint with lingual arches off the palate was bonded (image 2), and vertical force was applied against the maxillary segments via NiTi springs to the splint from the bone screw (image 3). Note that there is a spring anterior and posterior from the arm, giving a largely vertical pull.
After 6 months, the open bite was closed, the splint was removed, and a complete orthodontic appliance was placed. The archwire was tied to the bone screws to control re-elongation of the intruded teeth during the fixed appliance treatment (image 4).
Total treatment time was 15 months, with closure of the open bite (image 5) and successful maintenance of appropriate display of maxillary incisors (image 6). The result was stable at 2 years post-treatment, but 5 year follow-up is required to adequately evaluate long-term stability.
 Image 1: Separation of the 2nd premolar and 1st molar roots was accomplished with bonded brackets and a segmental wire, so there would be space between them for placement of a long bone screw as anchorage. Image 1: Separation of the 2nd premolar and 1st molar roots was accomplished with bonded brackets and a segmental wire, so there would be space between them for placement of a long bone screw as anchorage. |  Image 2: A bonded splint with trans-palatal connectors is an effective way of preventing the posterior teeth from being tipped facially by force applied on the facial side. Image 2: A bonded splint with trans-palatal connectors is an effective way of preventing the posterior teeth from being tipped facially by force applied on the facial side. |
 Image 3: The splint also helps to prevent the lower molars from erupting as the upper ones are intruded. Image 3: The splint also helps to prevent the lower molars from erupting as the upper ones are intruded. |  Image 4: During post-intrusion fixed appliance treatment, the molar tube is tied to the bone screw with a wire ligature, to maintain the intrusion. Image 4: During post-intrusion fixed appliance treatment, the molar tube is tied to the bone screw with a wire ligature, to maintain the intrusion. |
 Image 5: Open bite closed at completion of treatment; at least one year in retention is required. Image 5: Open bite closed at completion of treatment; at least one year in retention is required. |  Image 6: In this post-treatment facial photo, note the decrease in lower face height that improves facial proportions without change in maxillary incisor display. Image 6: In this post-treatment facial photo, note the decrease in lower face height that improves facial proportions without change in maxillary incisor display. |
Posterior Intrusion Stability
A key question, of course, is whether posterior intrusion will be stable, or whether the intruded teeth will re-erupt so that the open bite recurs. Follow-up data are not yet extensive enough to be sure about long-term stability. It is known that moving the maxilla up is one of the most stable surgical movements. Perhaps this is an encouraging sign that intruding the teeth also will be stable—but 5-year follow-up on a reasonably large sample of patients is needed to know.
All that can be said now is that preliminary results are encouraging. For the patient whose treatment you just saw, cephalometric superimpositions at the end of intrusion (image 1) show the change in tooth positions during treatment. From that point to the end of treatment (image 2) the changes were maintained, and at 29 months post-treatment there still was no relapse (image 3). What it will look like at 5 years? We still do not have enough data (as of early 2013) to be sure about that. Results from a sequence of at least 25 consecutive cases with 5 year recall is needed.
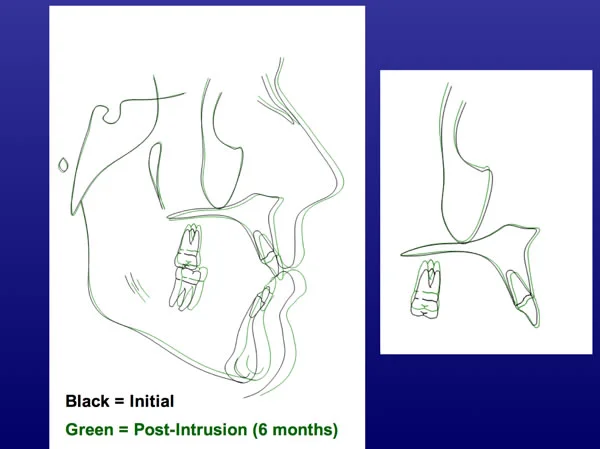 Image 1 Image 1 | 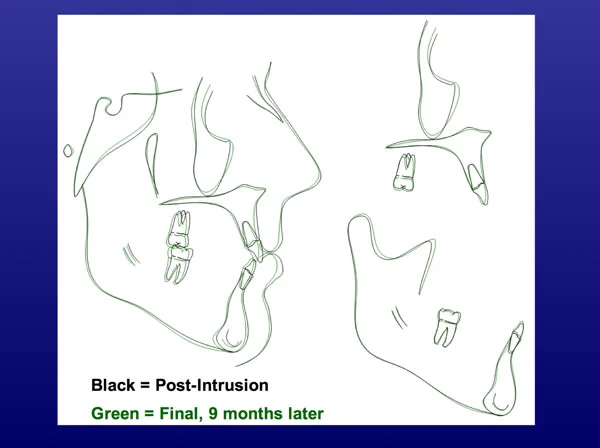 Image 2 Image 2 |
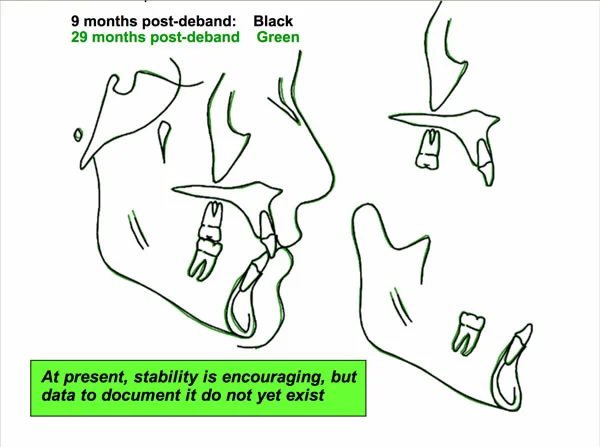 Image 3 Image 3 |
TADs vs. Orthognathic Surgery
As we discussed in a previous module, Class III elastics to bone plates can modify the pattern of growth in children with maxillary deficiency and have some potential to alter the pattern of mandibular growth as well. In this module, we have discussed using TADs for intrusion of maxillary posterior teeth as a way to decrease anterior face height in patients with a long-face/open bite problem—which previously could be accomplished only with surgery to superiorly reposition the maxilla. Moving the entire maxillary or mandibular arch posteriorly now can be accomplished with skeletal anchorage, and this is a way to correct Class II or Class III malocclusion, respectively.
Does this mean that many fewer patients now will need orthognathic surgery? It is difficult to answer that question at this point, because using TADs to correct or camouflage skeletal problems is so new that there are no good data for long-term outcomes. It has been observed many times that jaw relationships apparently corrected by growth modification in children tend to recur during adolescence. Will that be the case with the new TAD-supported approach? We won’t know for sure until these patients have been followed all the way through their teen years.
Intrusion of maxillary posterior teeth is done primarily for patients who have little or no growth left, so post-treatment growth would not be a major reason for relapse—but intruding posterior teeth beyond 4 mm is very difficult, and most patients experience 1 mm re-eruption of the intruded teeth despite efforts at retention. So a net intrusion of 3 mm is about as much as can be hoped for. Two mm closure of anterior open bite is achieved for each mm of posterior intrusion—which means that closing an open bite of more than 6 mm probably is not feasible with this method. The more severe long face patients will continue to need surgery.
Correcting Class II problems by moving the maxillary teeth posteriorly, or Class III by moving the mandibular teeth posteriorly, does not correct the jaw relationship. This succeeds only if protrusion of the upper or lower incisors was a significant part of the problem. Moving the anterior teeth back too much makes the facial appearance worse, and that is particularly a limit in Class III patients with a prominent chin because retracting the lower incisors makes the chin even more prominent.
The probable effect of TADs as a replacement for orthognathic surgery is summarized in image 4. The greatest effect is likely to be on treatment of long face patients; there will be some effect on treatment of skeletal Class III problems from a combination of growth modification and camouflage, with the magnitude of the effect still in doubt; there will be perhaps some, but not much, effect on treatment of skeletal Class II problems. With extraction of upper premolars, we already can camouflage Class II patients, and the limitations of doing that are not changed by extracting more posteriorly and retracting the whole dental arch.
Impact of TADs on Patients and Treatment Difficulty
What’s it like to be the patient who receives TADs? Placing bone screws requires anesthesia (a potent topical usually is enough)—then the patient feels pressure as it is inserted, but minimal pain. There is some tissue irritation during the next few days. Mini-plates require more potent anesthesia, a flap to expose the bone, then sutures while it heals. Some swelling occurs that peaks at 2 days, and tissue irritation persists for another few days.
Despite the reaction to this amount of surgery, experience with both types of TADs shows that patients tolerate them quite well. The amount of pain and swelling reported in a group of 97 mini-plate patients is shown in image 1. This is acceptable to patients if they expect it.
The effect of mini-plates on the subsequent orthodontic treatment also is interesting. The 30 orthodontists who treated the same group of 97 patients expected the treatment to be difficult, usually very difficult (image 2, blue bars) because of the type of malocclusion and the treatment plan. They found it to be much easier than they expected. The majority of the cases were judged to be moderately easy (green bars), and none were judged to be very difficult.
The bottom line: TADs of both types are well tolerated by patients, and make tooth movement possible that couldn’t be done any other way. Skeletal anchorage won’t revolutionize orthodontics, but it certainly will be widely used to overcome anchorage problems.
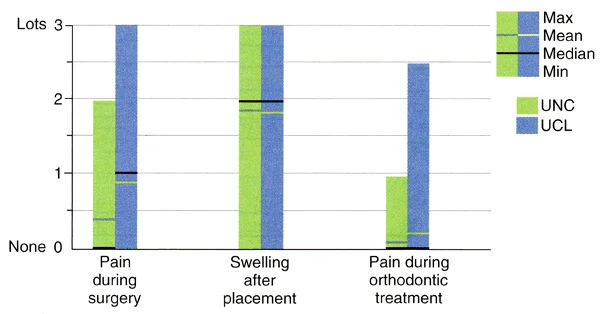 Image 1: Patient reports of pain and swelling after placement of mini-plates, in patients treated in Belgium (UCL) and NC. Note that pain during surgery to place the mini-plates and during orthodontic treatment was quite low for the great majority of patients, while post-surgical swelling was experienced by almost all. Image 1: Patient reports of pain and swelling after placement of mini-plates, in patients treated in Belgium (UCL) and NC. Note that pain during surgery to place the mini-plates and during orthodontic treatment was quite low for the great majority of patients, while post-surgical swelling was experienced by almost all. | 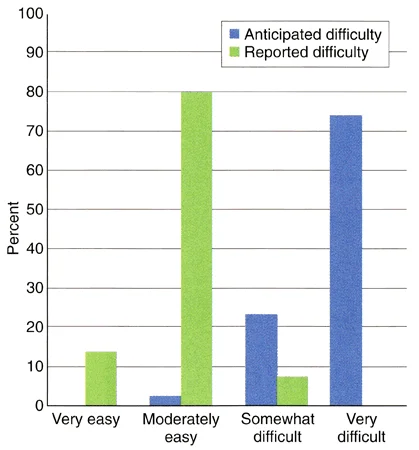 Image 2: Orthodontist expectations of treatment difficulty in patients with mini-plates compared to their actual experience. The orthodontists judged that treatment of 75% of the patients would be very difficult without TADs; with TADs over 90% of the actual treatment was judged to be moderately easy or very easy. Image 2: Orthodontist expectations of treatment difficulty in patients with mini-plates compared to their actual experience. The orthodontists judged that treatment of 75% of the patients would be very difficult without TADs; with TADs over 90% of the actual treatment was judged to be moderately easy or very easy. |
Self-Test Referral
The self-test section of this program is designed to help you be sure you have understood the material.
Now that you have gone through the module, be sure you also have done the assigned reading in Contemporary Orthodontics(pages 383-388 in 5th ed.; pages 382-383, 4th ed.) Then take the self-test, and use it as a guide for further study and review.
Copyright 2013, UNC Dept. of Orthodontics
Self-Test
Question 1
Regarding heavy vs. light orthodontic force: which of the following statements are correct?
- heavy force tends to cause more pain
- heavy force tends to burn anchorage
- heavy force requires more effort to conserve anchorage
- 1 and 2
- 1 and 3
- 2 and 3
- none are correct
- all are correct ✓
Correct
That’s right, all these statements are correct. With heavy force, not only is there more pain, it is more difficult to control anchorage and anchorage is more likely to be lost.
Incorrect
No, that’s wrong. All these statements are correct. With heavy force, not only is there more pain, it is more difficult to control anchorage and anchorage is more likely to be lost.
Question 2
Which of the following are examples of reinforced anchorage in retraction of protruding incisors?
- adding 2nd molars to the posterior anchorage unit
- adding teeth from the other arch to the anchorage unit
- adding bone screws to anchorage unit
- allowing the incisors to tip distally while anchor teeth move bodily
- 1 and 3
- 2 and 4
- 1, 2, and 3 ✓
- 1, 2, and 4
- all the above
Correct
That’s right, the first 3 items are examples of reinforcement of anchorage, the fourth isn’t. Reinforcement can be done by adding more teeth in the same arch to the anchorage unit, by adding teeth in the other arch, or by adding temporary anchorage devices. Pitting tipping of the teeth to be moved against bodily movement of the anchor teeth is an example of stationary anchorage.
Incorrect
No, that’s wrong. The first 3 items are examples of reinforcement of anchorage, the fourth isn’t.Reinforcement can be done by adding more teeth in the same arch to the anchorage unit, by adding teeth in the other arch, or by adding temporary anchorage devices. Pitting tipping of the teeth to be moved against bodily movement of the anchor teeth is an example of stationary anchorage.
Question 3
(A) In orthodontics, the anchorage unit is what the dentist says it is because (B) the amount and distribution of pressure in the PDL that a tooth experiences is a critical variable in how it responds.
- A true, B true, A and B related
- A true, B true, A and B not related ✓
- A true, B false
- A false, B true
- A and B false
Correct
That’s right, both statements are true but there’s no cause-effect relationship between them. Orthodontic anchorage is defined by how the orthodontic appliance is set up, and the anchorage is what the dentist thinks it is as he connects one tooth or group of teeth to others. Whether the anchorage concept produces the desired tooth movement is determined by the way the teeth respond. In an important sense, you have to think rationally about anchorage as tooth movement is planned, because wishful thinking about the response of the teeth isn’t the way to get what you’d like to happen.
Incorrect
No, that’s wrong. Both statements are true but there’s no cause-effect relationship between them. Orthodontic anchorage is defined by how the orthodontic appliance is set up, and the anchorage is what the dentist thinks it is as he connects one tooth or group of teeth to others. Whether the anchorage concept produces the desired tooth movement is determined by the way the teeth respond. In an important sense, you have to think rationally about anchorage as tooth movement is planned, because wishful thinking about the response of the teeth isn’t the way to get what you’d like to happen.
Question 4
With reciprocal anchorage for closing a maxillary midline diastema, what would be the effect on the speed of tooth movement if you increased the amount of force from 50 to 150 grams?
- much more rapid tooth movement
- more rapid tooth movement
- little or no effect ✓
- slower tooth movement
- much slower tooth movement
Correct
That’s right, in a reciprocal situation there would be little or no effect. Since each tooth (or group of teeth) is both an anchor and a movement tooth, they’d move toward each other at the same rate, almost independent of the force. The difference with heavier force would be much more in decreased patient comfort than speed of movement.
Incorrect
No, that’s incorrect. In a reciprocal situation there would be little or no effect. Since each tooth (or group of teeth) is both an anchor and a movement tooth, they’d move toward each other at the same rate, almost independent of the force. The difference with heavier force would be much more in decreased patient comfort (a nice way of saying more pain) than speed of movement.
Question 5
(A) Heavy force in orthodontic treatment makes it difficult to control anchorage because (B) it compromises the anchorage value of all the teeth in the anchorage unit.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false
Correct
That’s correct, both statements are true and related. Heavy force compromises the anchorage value of all the teeth in the anchorage unit by moving them closer to the plateau in the force / response curve, where there is little differential tooth movement. Heavy force creates two problems: not only does it increase the amount of pain for the patient, it makes it more difficult to control anchorage.
Incorrect
No, that’s incorrect, both statements are true and related. Heavy force compromises the anchorage value of all the teeth in the anchorage unit by moving them closer to the plateau in the force / response curve, where there is little differential tooth movement. Heavy force creates two problems: not only does it increase the amount of pain for the patient, it makes it more difficult to control anchorage.
Question 6
(A) Headgear is a particularly effective way to reinforce posterior anchorage because (B) it provides heavy interrupted force against the posterior teeth to which it is attached.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true ✓
- A and B false
Correct
That’s correct, the first statement is false but the second one is true. Headgear is a rather poor way to reinforce posterior anchorage, because it provides interrupted rather than continuous force (it’s never worn all the time) and the force tends to be too heavy when it is present.
Incorrect
No, that’s incorrect. The first statement is false but the second one is true. Headgear is a rather poor way to reinforce posterior anchorage, because it provides interrupted rather than continuous force (it’s never worn all the time) and the force tends to be too heavy when it is present.
Question 7
Why is two-stage space closure more likely to be needed when teeth are pulled along an archwire with a spring than when a loop in the wire is used as a spring?
- anchorage control is more difficult
- with the loop, teeth tip into position
- sliding makes it possible to control force more precisely
- there’s no resistance to sliding with the loop
- 1 and 2
- 2 and 3
- 3 and 4
- 1 and 3
- 1 and 4 ✓
Correct
That’s right, when you pull a tooth or teeth along an archwire so that brackets on the teeth slide on the wire, two-stage space closure is more likely to be needed for two reasons. First, anchorage control is more difficult when you slide teeth along an archwire because additional force beyond what is needed for tooth movement has to be used to also overcome the resistance to sliding. Second, there’s no resistance to sliding with the loop (the teeth are tied to the wire and segments of wire with teeth attached are moved). Bodily tooth movement is quite possible when a loop is used, and force control can be managed about equally well with loops vs. sliding.
Incorrect
That’s wrong. When you pull a tooth or teeth along an archwire so that brackets on the teeth slide on the wire, two-stage space closure is more likely to be needed for two reasons. First, anchorage control is more difficult when you slide teeth along an archwire because additional force beyond what is needed for tooth movement has to be used to also overcome the resistance to sliding. Second, there’s no resistance to sliding with the loop (the teeth are tied to the wire and segments of wire with teeth attached are moved). Tipping can be controlled when loops are used, and it’s more rather than less difficult to precisely control force during sliding. Bodily tooth movement is quite possible when a loop is used, and force control can be managed about equally well with loops vs. sliding.
Question 8
(A) Complex force systems with more than one couple present within the system make it difficult to determine forces and moments because (B) one-couple systems are indeterminate while two-couple systems are determinate.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false ✓
- A false, B true
- A and B false
Correct
That’s right, the first statement is true but the second one is false. For (B), it’s the other way around: one couple systems are determinate and the forces and moments can be determined precisely, while two-couple systems are indeterminate and the forces and moments cannot be known precisely. That’s particularly important when light forces for intrusion are needed. If you can’t determine the force, there’s no way to know whether you’re using the right force magnitude, so a one-couple force system is needed.
Incorrect
No, that’s wrong. The first statement is true but the second one is false. For (B), it’s the other way around: one couple systems are determinate and the forces and moments can be determined precisely, while two-couple systems are indeterminate and the forces and moments cannot be known precisely. That’s particularly important when light forces for intrusion are needed. If you can’t determine the force, there’s no way to know whether you’re using the right force magnitude, so a one-couple force system is needed.
Question 9
Which of the following are reasons that a multi-bracketed orthodontic appliance becomes a complex two-couple system?
- couples are created across multiple brackets
- with rectangular wire, couples are created within multiple brackets
- wires are ligated into multiple brackets
- 1 only
- 2 only
- 1 and 3
- 2 and 3
- 1, 2, and 3 ✓
Correct
That’s right, all these are reasons why a multi-bracketed orthodontic appliance becomes a complex two-couple system. When a wire is ligated into a bracket, a couple across the bracket is created as soon as tooth movement begins, even if it’s a round wire, and a rectangular wire with any degree of twist produces a couple within each bracket as soon as it’s inserted.
Incorrect
No, that’s wrong. All these are reasons why a multi-bracketed orthodontic appliance becomes a complex two-couple system. When a wire is ligated into a bracket, a couple across the bracket is created as soon as tooth movement begins, even if it’s a round wire, and a rectangular wire with any degree of twist produces a couple within each bracket as soon as it’s inserted.
Question 10
Which of the following can provide perfect anchorage for orthodontic tooth movement?
- ankylosed maxillary canine
- tooth with fusion of a small area of the root to alveolar bone
- osseointergrated implant
- alveolar bone screw
- 1 and 2
- 3 and 4
- 1, 3, and 4
- 2, 3, and 4
- all the above ✓
Correct
That’s right, all of these situations can provide perfect anchorage. It takes only a small area of fusion of the root to bone to produce ankylosis, and an ankylosed tooth can’t be moved unless that area of fusion can be released. Osseointegrated implants and alveolar bone screws lack a periodontal ligament, and therefore can’t be moved like teeth. They may become loose and fall out, but they don’t move through the bone—that takes an intact PDL.
Incorrect
No, that’s wrong. If anterior face height is increased, it is likely that the patient will have anterior open bite. An increased distance from nose to upper incisor, indicating excessive eruption of the maxillary anterior teeth, would decrease the chance of open bite. The other two are not related to open bite.
Question 11
Which of the following are advantages of miniplates placed at the base of the zygomatic arch versus alveolar bone screws?
Miniplates
- become osseointegrated, bone screws don’t
- are held by multiple screws
- allow a change in force direction
- use flap surgery in the mucosa for insertion
- 1 and 2
- 2 and 3 ✓
- 1, 2, and 3
- 1, 2, and 4
- all the above
Correct
That’s right, statements 2 and 3 are advantages of miniplates, while statement 4 (although true) is a disadvantage rather than an advantage. Neither miniplates nor alveolar bone screws become osseointegrated, at least not in the way that restorative implants do. That’s more of an advantage than a disadvantage because it makes them easier to remove after orthodontic treatment is completed.
Incorrect
No, that’s incorrect. Statements 2 and 3 are advantages of miniplates, while statement 4 (although true) is a disadvantage rather than an advantage. Neither miniplates nor alveolar bone screws become osseointegrated, at least not in the way that restorative implants do. That’s more of an advantage than a disadvantage because it makes them easier to remove after orthodontic treatment is completed.
Question 12
Which of the following is the type of tooth movement that most requires miniplate rather than alveolar bone screw anchorage?
- positioning individual teeth
- retraction and intrusion of protruding maxillary incisors
- distal movement of the entire maxillary dental arch ✓
- intrusion of maxillary posterior teeth
- intrusion of maxillary anterior teeth
Correct
That’s right. You can’t move the entire maxillary arch distally with bone screws between the tooth roots as anchorage, because the teeth would quickly run into a bone screw as they were moved distally. Bone screws can be used to produce the other movements, although miniplates may make it easier because they allow changes in the force direction.
Incorrect
No, that’s wrong. You can’t move the entire maxillary arch distally with bone screws between the tooth roots as anchorage, because the teeth would quickly run into a bone screw as they were moved distally. Bone screws can be used to produce the other movements, although miniplates may make it easier because they allow changes in the force direction.