Goals of Adjunctive Treatment
Definition of Adjunctive Treatment
Adjunctive orthodontic treatment, by definition, is “tooth movement carried out to facilitate other dental procedures that are aimed at controlling disease and restoring function.”
Although adjunctive treatment could be needed in children, for all practical purposes it is treatment for adults who have lost teeth and/or supporting bone to dental disease. Some tooth positions and dental relationships are not conducive to long-term oral health, so that occlusal function contributes to destruction of the occlusion. This is referred to as “pathologic occlusion.” An example would be the loss of gingival tissues lingual to the upper incisors from a deep, impinging overbite.
If signs of pathologic occlusion exist, or if restorations needed for other problems would compromise the maintenance of oral hygiene or overly stress the periodontal support apparatus, tooth movement should become part of an overall treatment plan.
For this patient, there are two possibilities for replacement of the missing mandibular first molars. One is a complete orthodontic fixed appliance supported by bone plates or screws to bring the second and third molars mesially and close the space; the other is opening the space for replacement of the first molars (with implants or bridges), which requires repositioning the tipped mandibular second molars, to both improve the periodontal health of the second molars and provide space for adequate restorations.
The problem with closing the space is that it requires complex and prolonged orthodontic treatment, probably over more than 2 years, because remodeling of cortical bone would be required and the roots of the molars would have to be brought mesially further than the crowns. In the lower arch, leaving the molars tipped mesially creates a periodontal situation that is difficult to manage.
In contrast, the orthodontic component of a replacement treatment plan is straightforward and reasonably quick. What is needed is distal tipping of the second molars. The replacement plan, therefore, usually is the more practical and better choice.
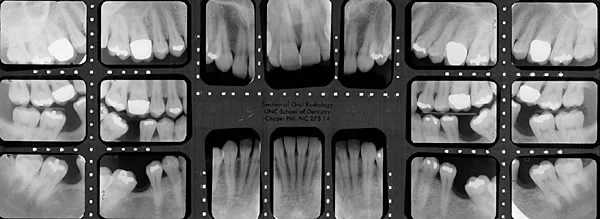 Image 1, full series: Pretreatment, missing lower molars, evidence of periodontal disease. Image 1, full series: Pretreatment, missing lower molars, evidence of periodontal disease. |  Image 2, panoramic: Pretreatment, panoramic overview. Image 2, panoramic: Pretreatment, panoramic overview. |
Goals of Adjunctive Treatment
Adjunctive treatment implies limited orthodontic goals, improving a particular aspect of the occlusion rather than comprehensively altering it.
The goals of adjunctive treatment are to
- facilitate restorative treatment by positioning the teeth so more ideal and conservative techniques (including implants) can be used.
- improve periodontal health by eliminating plaque-harboring areas and improving the alveolar ridge contour adjacent to the teeth.
- establish favorable crown-root ratios and position the teeth so that occlusal forces are transmitted along the long axes of the teeth.
- do this while maintaining or improving dental and facial esthetics.
The treatment methods discussed in this module and presented in more detail in the Adjunctive Treatment Procedures module, typically involve a partial fixed appliance and are completed in less than 6 months. Such treatment can be (and often is) carried out in the context of family/restorative practice.

Adjunctive Treatment: Types of Tooth Movement
Possible tooth movements in adjunctive treatment include
- mesial or distal movements of specific crowns, roots, or both
- correction of the axial inclination of drifted teeth
- correction of the buccolingual position of certain teeth
- correction of rotations
- extrusion of selected teeth
Although intrusion of teeth can be an important part of comprehensive treatment for adults, it should be avoided as part of adjunctive treatment because of its technical difficulty and the possibility of root resorption and/or loss of control of tooth positions. As a general rule for adjunctive treatment, teeth that are excessively elongated are best treated by reduction of crown height, which has the added advantage of improving the crown-root ratio in patients who have experienced loss of alveolar bone.
For example, when a mandibular molar is to be uprighted (image 1), it is usually necessary to reduce its occlusal surface to avoid occlusal interferences (image 2). Reducing the crown also changes the crown-root ratio in a favorable direction (image 3).
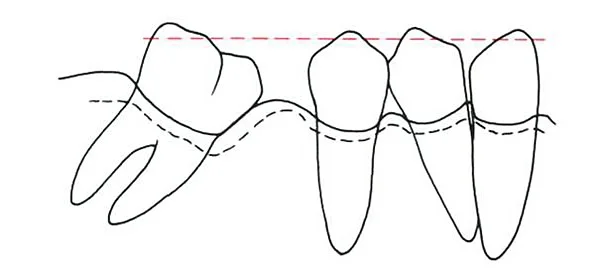 Image 1, pre-uprighting: Uprighting a tipped molar increases the crown height while it reduces the depth of the mesial periodontal pocket. Image 1, pre-uprighting: Uprighting a tipped molar increases the crown height while it reduces the depth of the mesial periodontal pocket. | 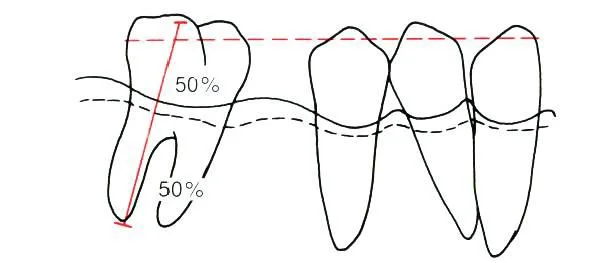 Image 2, progress: Reducing the height of the crown usually is necessary to avoid occlusal interferences and allow the uprighting to occur. Image 2, progress: Reducing the height of the crown usually is necessary to avoid occlusal interferences and allow the uprighting to occur. |
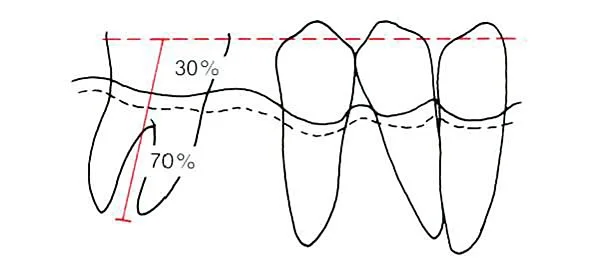 Image 3, crown height reduction: Reduction of crown height is particularly desirable if bone support is lacking, because it improves the crown-root ratio. Image 3, crown height reduction: Reduction of crown height is particularly desirable if bone support is lacking, because it improves the crown-root ratio. |
Adjunctive vs Comprehensive/Complex Treatment
In this patient (image 1), a fractured lower incisor created an esthetic problem because it was obvious when she smiled, and the malpositioned tooth was difficult to restore properly. Five months of adjunctive orthodontic treatment aligned the upper and lower incisors, and then an ideal restoration was placed (treatment details are shown in the module Adjunct Treatment Procedures). To her, the orthodontics was an important part of solving an esthetic problem that the fractured tooth created. Adjunctive treatment can be indicated to improve dental esthetics as well as to improve function and/or control health problems.
In adults with periodontal and restorative problems that are complex enough to require more than 6 months for the orthodontic phase of therapy, coordinated ortho/perio/restorative treatment by a team of dentists usually is needed.
Whether one or several practitioners are involved, adjunctive orthodontics must be coordinated carefully with the periodontal and restorative treatment. Orthodontic treatment for TM dysfunction should not be considered adjunctive. Complex adjunctive treatment is considered in more detail in the Level IV module with that title.

Diagnosis / Treatment Planning
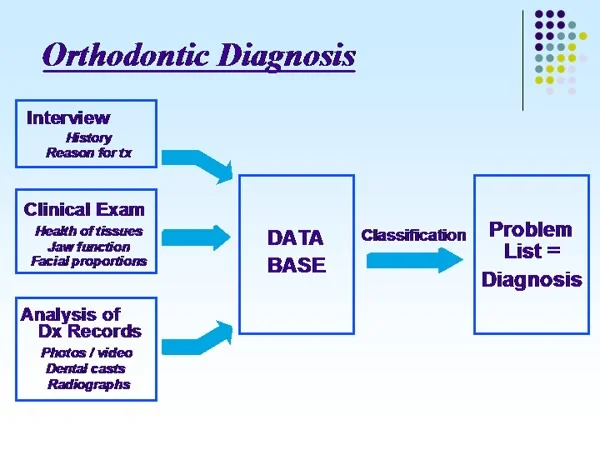
Diagnosis: Data Base—Problem List
Any treatment plan must be based on adequate diagnosis. Planning for adjunctive treatment requires two diagnostic steps:
- Collecting an adequate data base of information
- Developing a comprehensive but clearly stated list of the patient’s problems
These are precisely the same steps needed in evaluation of any potential orthodontic patient (see the modules Essentials of Orthodontic Diagnosis, and Concepts of Treatment Planning).
The problem list, of course, includes all the patient’s problems, not just those directly related to orthodontics. Comprehensive diagnosis, in the sense that no problems have been overlooked, is the key to developing appropriate solutions to problems that may involve several branches of dentistry.
Diagnosis: Data Base—Problem List (cont.)
The interview and clinical examination parts of the diagnostic evaluation are the same, whatever the type of orthodontic treatment. Diagnostic records for adjunctive orthodontic patients, however, differ from those for children in several ways:
- Individual intraoral radiographs usually are needed to supplement the panoramic radiograph (image 1).
The U.S. Public Health Service guidelines for radiographic evaluation of dental pathology should be followed in determining exactly what radiographs are needed (click on image 2 to see the summary of these recommendations).
- Cephalometric radiographs may not be needed.
The guideline is that serial cephalometric evaluation is required to evaluate changes due to growth or to major changes in tooth position. Nongrowing adults whose treatment will involve repositioning of only some teeth, therefore, do not require a cephalometric radiograph.
- Articulator-mounted casts are more likely to be needed.
This is the case if extensive restorative procedures are planned, or if there are signs of pathologic occlusion.
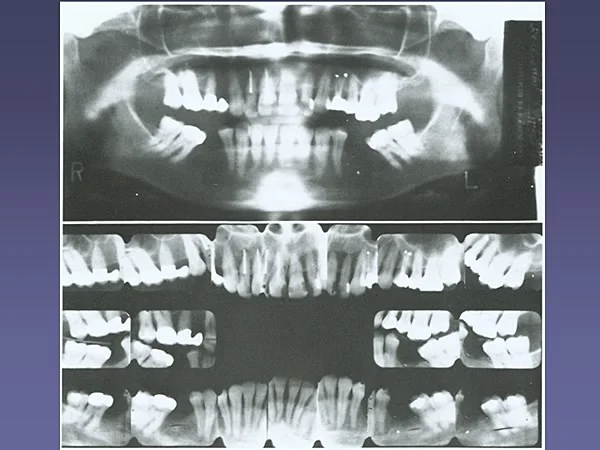 Image 1, radiographs: For patients with periodontal disease, additional intraoral detail radiographs are required. Image 1, radiographs: For patients with periodontal disease, additional intraoral detail radiographs are required. | 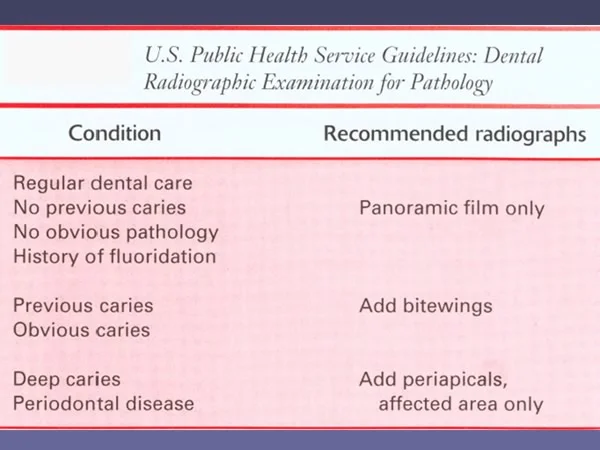 Image 2, radiographic examination: USPHS guidelines, radiographic examination for dental pathology. Image 2, radiographic examination: USPHS guidelines, radiographic examination for dental pathology. |
Treatment Planning
For patients receiving adjunctive orthodontic treatment, the treatment plan must specify the solutions to the patient’s various problems and the sequence in which treatment procedures will be carried out.
The sequence of treatment is guided by two principles:
- Pathologic problems must be brought under control before the orthodontic phase of treatment begins (image 1).
- Permanent restorations and definitive perio procedures should be deferred until after the final occlusion has been developed (image 2).
The first step in treatment planning, therefore, is to separate pathologic problems from occlusal problems.
Once these problems have been identified, they are brought under control. The sequence of treatment then is orthodontic tooth movement to establish the occlusion and finally the definitive perio/restorative treatment. Maintenance of the restorations and continued disease control is required long term.
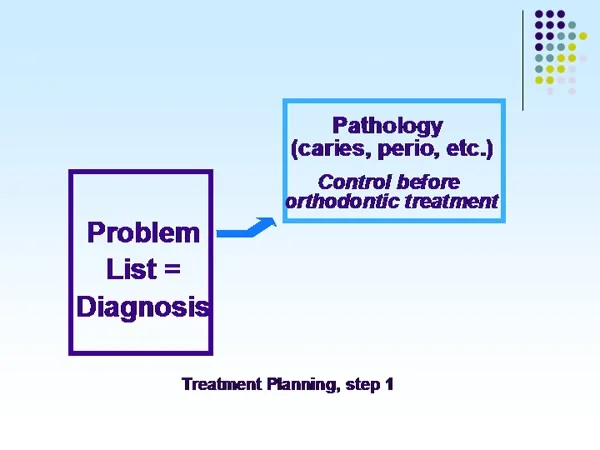 Image 1, first step: The first step in treatment planning: separate pathologic from occlusal problems. Image 1, first step: The first step in treatment planning: separate pathologic from occlusal problems. | 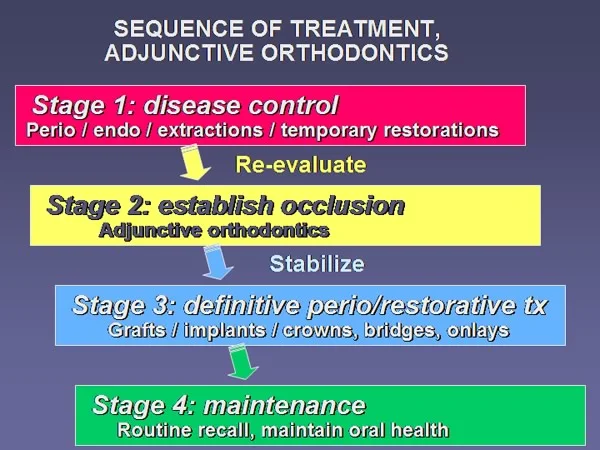 Image 2, treatment sequence: Treatment sequence, adjunctive orthodontics. Image 2, treatment sequence: Treatment sequence, adjunctive orthodontics. |
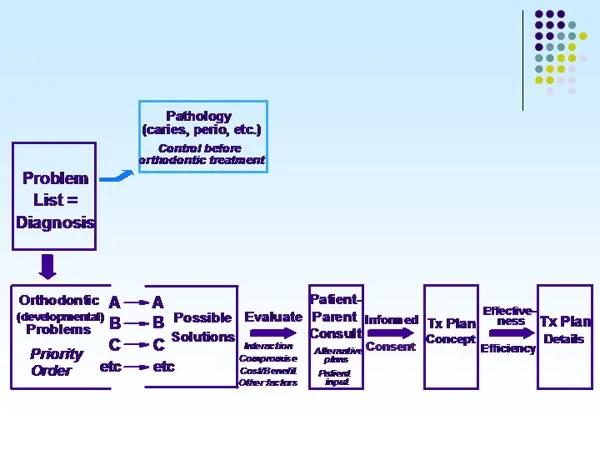
Patient Consultation
The same scheme used for comprehensive orthodontic treatment applies also to adjunctive patients. The approach is best described as an organized way to seek the plan that provides optimal benefit to the patient.
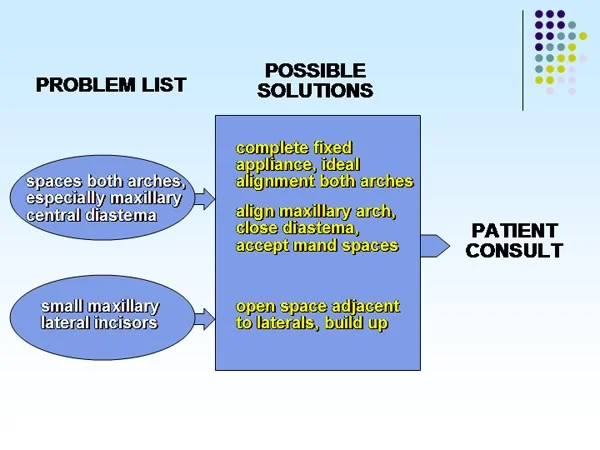
Possible solutions to the various problems are considered, starting with the most important one, interactions and practical considerations are reviewed, and alternative treatment possibilities are outlined.
At a meeting with the patient, the doctor’s role is to evaluate the alternative treatment possibilities and present them as clearly and objectively as possible. The goal is to get the patient to understand the alternatives.
After the patient and doctor agree on the treatment plan concept, its details are established.
Diagnostic Evaluation, Adjunctive Ortho Patient
Let’s examine this process in the context of a specific patient.
Fred, age 30, was concerned primarily about the appearance of his maxillary incisors, because of the midline space (central diastema) and the small size of the laterals (image 1). He particularly didn’t like “the gap in my smile.”
Fred had spaces in both the upper and lower arches. Three first premolars and the mandibular left canine had been extracted previously. Overjet was slightly excessive, but the posterior occlusion was essentially normal (image 2).
The panoramic radiograph showed good dental health despite the spacing in the arches, so there was no indication for intraoral radiographs (image 3).
Did you notice the facial asymmetry, with the nose somewhat off to the left and the chin off to the right? Note in the pan that the right condyle is smaller than the right one and there is a more pronounced antegonial notch on the right side, indicating a lack of condylar growth on that side. Both those findings suggest an old condylar fracture that healed well. The deviation of the nose probably also is the result of old trauma. Is the asymmetry a problem? Not unless he is aware of it as a problem, and he was not. Is further loss of the smaller condyle likely? Probably not, unless he has experienced early signs of degenerative arthritis—and he had not.
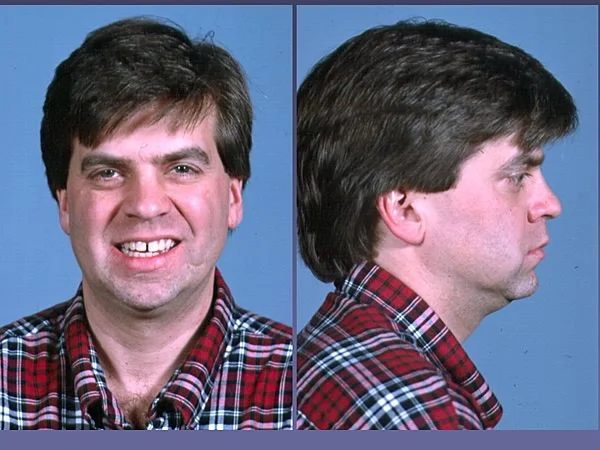 Image 1, facial photos: Fred, age 30, prior to treatment. Image 1, facial photos: Fred, age 30, prior to treatment. |  Image 2, intraoral: Fred, age 30, prior to treatment. Image 2, intraoral: Fred, age 30, prior to treatment. |
 Image 3, panoramic: Fred, age 30, prior to treatment. Image 3, panoramic: Fred, age 30, prior to treatment. |
Diagnostic Evaluation, Adjunctive Ortho Patient (cont.)
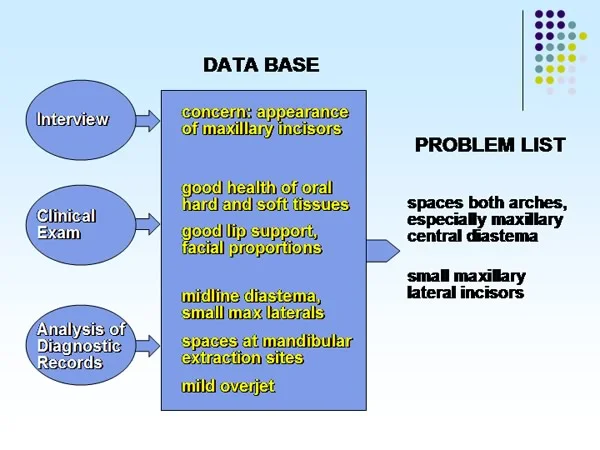
As with all patients, the diagnostic data base is derived from three sources:
- Interview—which made it clear that his concern was almost entirely the appearance of his maxillary incisors
- Clinical examination—which revealed no problems with oral health, jaw function, or facial esthetics (despite the mild mandibular and nasal asymmetry, which were not perceived as problems by the patient)
- Analysis of diagnostic records—in this case, primarily the dental casts, which revealed small lateral incisors midline diastema mildly excessive overjet dental midlines not coincident
The mild overjet was not really a problem—but it would have to be considered when correction of the diastema and small lateral incisors was planned. It would be important to keep the maxillary dental midline coincident with the middle of the face, rather than focusing on making it coincident with the mandibular dental midline.
Possible Solutions / Patient Conference
There were two possible solutions to the problem of spacing in both arches:
- Comprehensive orthodontics to close spaces and obtain alignment in both arches that was as ideal as possible
- Treatment of the maxillary arch only, accepting the spaces in the mandibular arch
For the problem of the small maxillary lateral incisors, the only treatment would be restorations to build up them up to normal size (or choose not to correct the problem, which would leave him with compromised dental esthetics).
How do you choose between the possibilities?
Remember, you don’t, the patient does. It is the doctor’s role to present the possible solutions and discuss their pros and cons with the patient so that he can make an informed decision.
In this case, Fred chose the shorter and less expensive approach of treating the maxillary arch only, but wanted the small laterals built up as part of the overall approach.
Treatment Plan Concept / Details
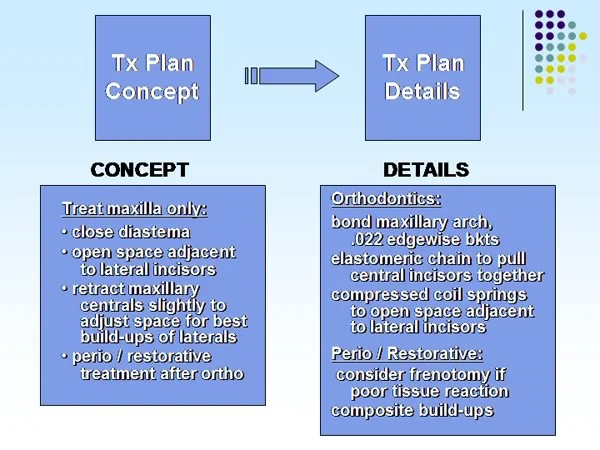
At this point, the treatment plan concept should be clear. For Fred, it was treatment for the maxillary arch only, to close the maxillary central diastema, keeping the maxillary dental midline about where it was, and open space so that the lateral incisors could be built up. The essence of informed consent is that the patient and the doctor(s) agree at this point.
The treatment plan details are for the doctor(s) and show how the concept is to be implemented:
- bonding of edgewise .022 slot brackets for the maxillary arch, back to 2nd premolars only
- elastomeric chains to close the central diastema, then compressed coil springs to open space for build-ups of the lateral incisors
- slight retraction of the central incisors as needed to get the space correct for ideal proportions of the lateral incisors
- removal of excessive gingival tissue in the maxillary midline, and repositioning of the frenum, if needed
- composite build-ups of the lateral incisors
- maxillary retainer
Treatment Progress
Treatment was implemented as planned. The maxillary arch was bonded, but only to the 2nd premolars (which simplified the appliance and avoided the problem of attachments to the crown on one maxillary first molar) (image 1).
Elastomeric chain on an steel arch wire that provided 0.003-inch clearance between the wire and the bracket, so that the teeth could slide along the wire, was used to close the excess space, slightly retracting the upper incisors as this was done (image 2). Note the use of multiple segments of the chain, with a 2-unit segment initially from the mesial bracket of one central incisor to the mesial bracket of the other. A continuous chain would have produced too much force. There was no attempt to correct the dental midline, which might have made the facial asymmetry more apparent.
After the diastema was closed, compressed coil springs were used to open space for build-ups of the lateral incisors (image 3). When a maxillary central diastema is closed, tissue reaction in the midline is possible, and the patient should be told that a frenotomy procedure may be needed. In this case, it was not.
Composite build-ups were done immediately after the orthodontic appliance was removed (image 4), and a retainer was placed. Treatment time, as planned, was 6 months.
 Image 1, pre-treatment: Age 30, prior to treatment. Image 1, pre-treatment: Age 30, prior to treatment. |  Image 2, space closure: Space closure with elastomeric chains. Image 2, space closure: Space closure with elastomeric chains. |
 Image 3, positioning laterals: Positioning laterals with compressed coil springs. Image 3, positioning laterals: Positioning laterals with compressed coil springs. |  Image 4, treatment completed: Restorations completed. Image 4, treatment completed: Restorations completed. |
 Image 5, treatment sequence: Overview of steps in treatment. Image 5, treatment sequence: Overview of steps in treatment. |
Treatment Progress (cont.)
Fred was pleased with the improvement in his smile esthetics (image 1), and lip support was unchanged (image 2). To a trained eye the facial asymmetry is still noticeable, but all faces have some asymmetry, and if Fred remained more asymmetric than most people, neither he was not even aware of it, and almost certainly his friends and associates also had never noticed it. Although the comprehensive treatment that would have been required for ideal occlusion was not done, the treatment solved his problem.
Should the lower arch have been treated? There was no esthetic problem related to the spaces there, his oral health was good despite the spaces, and there was no problem with functional occlusion. So the judgment was that there was no compelling reason to treat the lower arch.
It often is the case that adjunctive orthodontics focuses—quite appropriately—on a specific aspect of the dental occlusion rather than comprehensive correction of a malocclusion.
 Image 1, smile change: Change in smile esthetics with treatment. Image 1, smile change: Change in smile esthetics with treatment. | 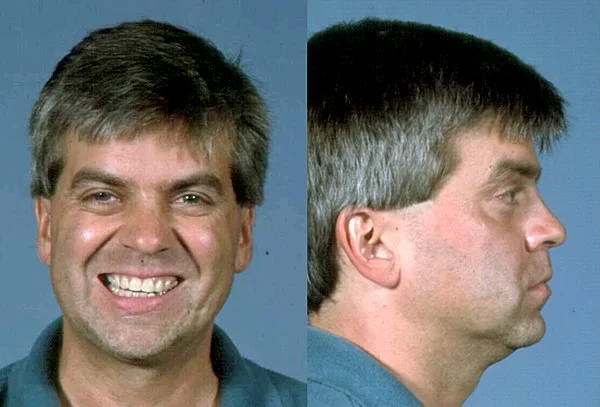 Image 2, post-treatment facial: Fred, age 31, at completion of treatment. Image 2, post-treatment facial: Fred, age 31, at completion of treatment. |
Biomechanical Considerations
Effects of Reduced Periodontal Support
Because adjunctive treatment often involves adults who have experienced periodontal disease, an important consideration in developing the detailed plan for adjunctive orthodontic treatment is the amount of bone support for the teeth.
When bone loss has occurred, a periodontally involved tooth differs from a normally supported tooth in two important ways:
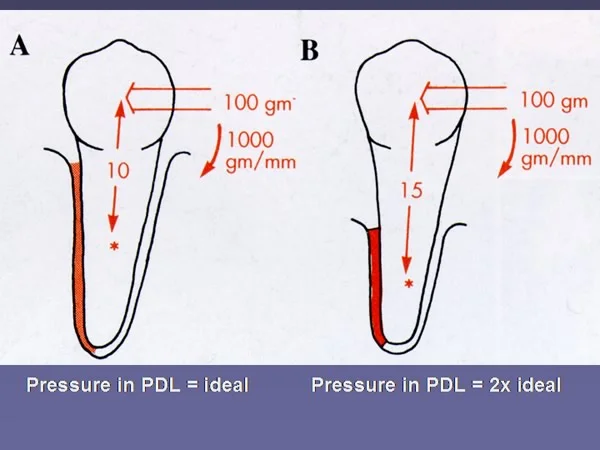
- **A decrease in the volume of the periodontal ligament also occurs (image 1).**This means that the normal force against the crown produces greater pressure in the PDL—so lighter forces are required when bone loss has occurred.
Remember that it’s the pressure in the PDL that affects blood flow and leads to the biologic responses that allow tooth movement. The goal, obviously, is to use whatever force is needed to produce the optimal pressure. For example, suppose you were trying to move a premolar bodily. The typical force to do that, producing close to the ideal pressure in the PDL, is 100 grams. But if half the alveolar bone support has been lost, 100 grams would produce twice the ideal pressure, because the force is being expressed over half the PDL volume.
If bone loss has occurred, the force has to be reduced from what it would have been with a normal tooth. Otherwise pressure in the PDL would be too large.
Effects of Reduced Periodontal Support (cont.)
When bone loss has occurred, a periodontally involved tooth differs from a normally supported tooth in two important ways:
- A decrease in the volume of the periodontal ligament also occurs
- When force is applied, the center of resistance of the root will be further from the crown—so relatively larger moments are needed to control root position.
Remember that a force against the crown of a tooth creates a moment (MF), because the force on the crown is at a distance from the center of resistance, which is near the midpoint of the part of the root that is within supporting bone. For our typical normal premolar, a 100-gm force creates a 1000 gm-mm moment because it is 10 mm to the center of resistance.
To control root position, a couple (two forces equal in magnitude and opposite in direction) must be applied to the crown, creating a moment (MC) that counteracts the moment of the force. A couple creates a pure moment—no net force to move the tooth, just a moment to rotate it. The couple usually is created by a wire that crosses a bracket on the crown at an angle, so that one corner of the bracket is lifted up while the other is pushed down. In the normal condition, a 1000 gm-mm MC is needed to cancel out the 1000 gm-mm MF, and then bodily movement will occur.
But when half the bone support has been lost, the distance to the center of resistance increases to 15 mm, and with 100 gm force, a 1000 gm-mm MC would be inadequate and the tooth would tip (image 1). After loss of half the supporting bone, therefore, bodily movement would require a 50-gm force and a 750 gm-mm moment of the couple, to balance the 750 gm-mm moment of the force (image 2).
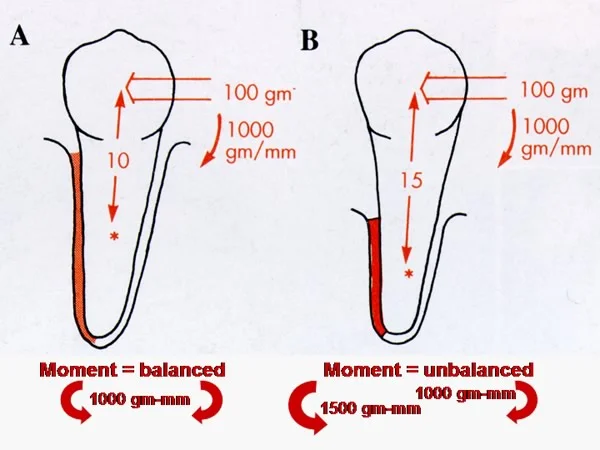 Image 1, moments: Bone loss increases the distance from the crown (and an orthodontic force on it) to the center of resistance. Image 1, moments: Bone loss increases the distance from the crown (and an orthodontic force on it) to the center of resistance. | 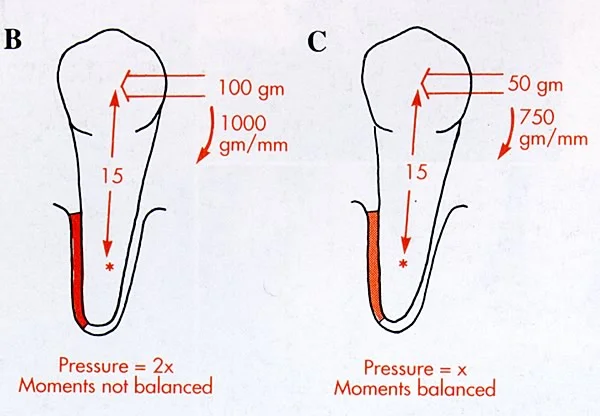 Image 2, corrected for bone loss: With loss of half the bone, half the force and a relatively larger moment are required. Image 2, corrected for bone loss: With loss of half the bone, half the force and a relatively larger moment are required. |
Appliance Considerations: Fixed vs Removable
Can you use a removable appliance for adjunctive orthodontics, or is a fixed appliance required?
For adults receiving adjunctive orthodontics, as a general rule, removable appliances rarely are satisfactory, for four reasons. With acrylic removable appliances that incorporate springs for tooth movement:
- It is impossible to obtain both a force, which generates a moment, and the moment of a couple to counteract the moment of the force, with a single spring (image 1), so control of root position is lacking. A couple is much easier when you can pull as well as push. That requires a fixed attachment.
- It is difficult to correct rotations at the same time a crown is repositioned, for the same reasons: two points of contact are needed to rotate a tooth without displacing it (image 2). The direction of tooth movement is always at right angles to the initial contact of a fingerspring on a removable appliance. Applying a fingerspring to the mesiolingual angle so that the rotation of the premolar would improve also carries the tooth buccally, whether or not that is desirable.
- At best, the removable appliance is worn only part of the time. Interrupted forces, those that are there when the appliance is in place but drop to zero when it is removed, can move teeth but are not as effective as continuous forces.
- Discomfort and interference with speech and mastication are greater than with a carefully designed and placed fixed appliance.
Do the same limitations apply to clear aligners, like those used with Invisalign? The top 3 items in the above list apply in the same way. With Invisalign you can not rotate teeth or move them bodily unless you bond fixed attachments to the teeth so the aligner can get a better grip (image 3), and the aligners are not worn all the time. Clear aligners are easier for adults to tolerate than acrylic plates, however.
 Image 1, spring for distal tipping: With a finger spring from a removable appliance, the tooth would tip distally, because there is no moment to control root position. Image 1, spring for distal tipping: With a finger spring from a removable appliance, the tooth would tip distally, because there is no moment to control root position. | 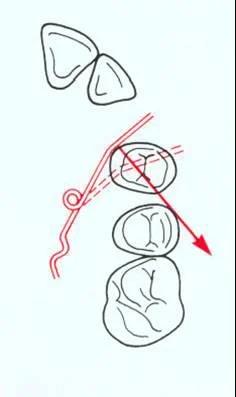 Image 2, spring for attempted rotation: Adjusting the point of application of the spring could produce some rotation, but the tooth also would be displaced facially. Image 2, spring for attempted rotation: Adjusting the point of application of the spring could produce some rotation, but the tooth also would be displaced facially. |
 Image 3, Clear aligner over fixed attachment: For rotation, extrusion or bodily movement of teeth, clear aligners require fixed attachments on the teeth. Image 3, Clear aligner over fixed attachment: For rotation, extrusion or bodily movement of teeth, clear aligners require fixed attachments on the teeth. |
Appliance Considerations: Fixed vs Removable (cont.)
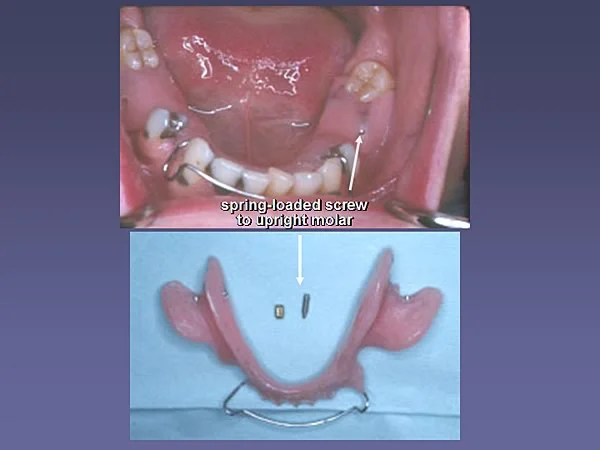
One situation in which an acrylic removable appliance may have an advantage is in a patient with multiple missing teeth. With a fixed appliance that has long unsupported spans of wire between teeth, distortion of the arch wire can become a problem, and irritation of the cheek can also occur. These problems are avoided with a removable appliance that has acrylic between separated teeth.
In addition, with a removable appliance, some reaction forces from tooth movement can be spread over adjacent supporting tissues, such as the palatal vault and alveolar mucosa. Major tooth movements, however, will still be very difficult with a removable appliance. The anchorage value of supporting tissues is minimal.
In the patient shown here, a removable appliance was preferred to reposition the second molar before fabrication of a removable partial denture, because of thethe multiple missing teeth and the long span between the incisors and the molar. A spring-loaded screw against the molar was used instead of a fingerspring to provide better control of the amount of activation.
Fixed Appliance Considerations: Bracket Placement
The position of fixed appliance brackets, like the twin edgewise brackets typically employed in adjunctive orthodontics, affects the type of movement that will occur for each tooth when a wire connecting the brackets is placed.
Often the primary goal of adjunctive treatment is to upright a molar, using the premolars and canine as anchorage. If the anchor teeth are not perfectly aligned, and brackets are placed on the anchor teeth in the ideal position near the center of the crown, a straight piece of wire connecting the brackets creates forces and moments to ideally position these teeth, which can decrease their anchorage value (image 1).
If the goal is to upright a molar but to use the premolars and canines just as anchorage without repositioning them, it would be better to place the brackets on the anchor teeth so that a straight segment of wire would not displace them (image 2). The effect on the anchor teeth with the different bracket positions is compared in image 3.
Where do you put the brackets for adjunctive orthodontics with a partial fixed appliance? It depends on exactly what tooth movement you’re trying to accomplish.
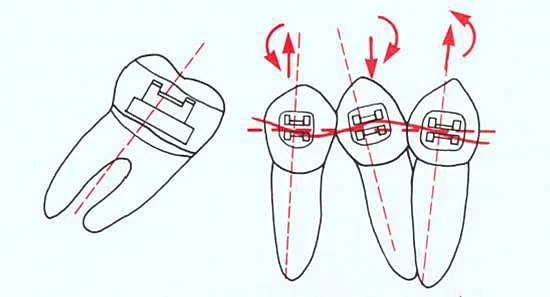 Image 1, ideal bracket position: With ideal bracket positions on malaligned anchor teeth, a straight wire creates forces and moments to reposition the anchor teeth, whether or not it was intended to move them. Image 1, ideal bracket position: With ideal bracket positions on malaligned anchor teeth, a straight wire creates forces and moments to reposition the anchor teeth, whether or not it was intended to move them. | 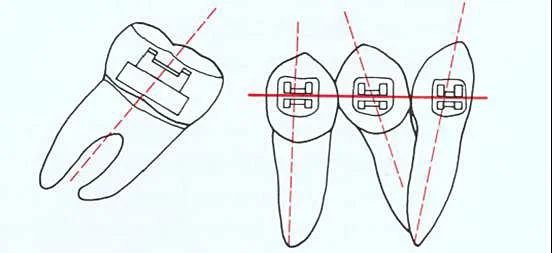 Image 2, compensatory bracket position: Positioning the brackets so that a straight wire fits passively can prevent unwanted movement of anchor teeth. Image 2, compensatory bracket position: Positioning the brackets so that a straight wire fits passively can prevent unwanted movement of anchor teeth. |
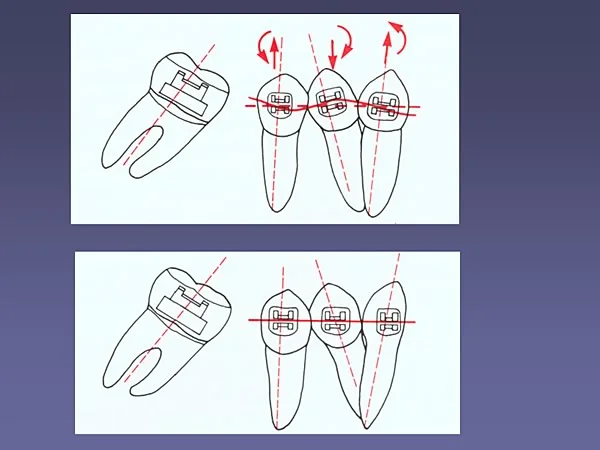 Image 3, comparison: Comparison of effect of ideal versus compensatory bracket positions. Image 3, comparison: Comparison of effect of ideal versus compensatory bracket positions. |
Summary, Adjunctive Orthodontic Concepts
Adjunctive orthodontics differs from comprehensive/complex orthodontics in several important ways:
- The goals of treatment are to solve specific problems for the patient, usually related to control of periodontal disease and long-term maintenance of the teeth or positioning teeth to facilitate restorative and prosthodontic treatment, not to produce ideal dental occlusion.
- Diagnostic records are likely to include additional radiographs, and articulator-mounted dental casts are needed more frequently.
- Treatment usually involves only part of the dentition and is completed in 6 months or less.
- Fixed appliances are preferred but often the brackets are placed to limit the movement of anchor teeth instead of repositioning them to an ideal position.
Self-Test Referral
The self-test section of this program is designed to help you be sure you have understood the material. Read pages 362-369, 621-627 in *Contemporary Orthodontics,*5th ed, (or pages 411-417, 633-639, 4th ed) then take the test, and use it as a guide for further study and review.
Copyright 2013, UNC Dept. of Orthodontics
Self-Test
Question 1
Which of the following are not goals of typical adjunctive treatment?
a. Improve the periodontal prognosis for a second molar
b. Improve smile esthetics
c. Concentrate the costs of treatment on the problem most important to the patient
d. Allow treatment with a removable rather than a fixed appliance
- c only
- d only ✓
- c and d
- b, c, and d
- all of the above
Correct
That’s correct, the first three statements are true, but the last one is false. Adjunctive treatment isoften used to improve smile esthetics, and when costs and treatment time for more extensive orthodontics are a factor, to focus the financial resources on the patient’s most important problem. Eliminating fixed appliances isn’t a goal, however. Successful adjunctive treatment often requires a fixed appliance simply because removable appliances are neither as effective nor as efficient.
Incorrect
No, that’s wrong. The first three statements are true, but the last one is false. Adjunctive treatment is often used to improve smile esthetics, and when costs and treatment time for more extensive orthodontics are a factor, to focus the financial resources on the patient’s most important problem. Eliminating fixed appliances isn’t a goal, however. Successful adjunctive treatment often requires a fixed appliance simply because removable appliances are neither as effective nor as efficient.
Question 2
Which of the following are reasons that intrusive tooth movement is rarely part of an adjunctive orthodontic treatment in general dental practice?
a. Risk of creating a periodontal problem around the tooth being intruded
b. Greater technical difficulty in creating and maintaining the necessary force system
c. Possibility of facial or lingual displacement of the tooth
d. Increased chance of root resorption
- a and b
- b and c
- c and d
- a, b, and c
- b, c, and d ✓
Correct
That’s right, the first statement isn’t a reason for avoiding intrusion in adjunctive treatment, but the other three are. Periodontal problems rarely occur when intrusion is carried out, but doing it requires a complex fixed appliance so that forces are kept very light and force directions are carefully controlled. Otherwise root resorption and unexpected displacement of teeth can occur. As a general rule, intrusion isn’t recommended in adjunctive orthodontics.
Incorrect
No, that’s wrong. The first statement isn’t a reason for avoiding intrusion in adjunctive treatment, but the other three are. Periodontal problems rarely occur when intrusion is carried out, but doing it requires a complex fixed appliance so that forces are kept very light and force directions are carefully controlled. Otherwise root resorption and unexpected displacement of teeth can occur. As a general rule, intrusion isn’t recommended in adjunctive orthodontics.
Question 3
Which of the following are advantages of reducing the crown height of a tooth that is deliberately being extruded during adjunctive treatment?
a. Facilitates subgingival extension of restoration margins
b. Improves the crown-root ratio
c. Eliminates occlusal interferences to the tooth movement
d. Makes it easier and more effective to use a removable appliance
- a and b
- b and c ✓
- c and d
- a and d
- b, c, and d
Correct
That’s right, reducing the height of the crown of a tooth that is being extruded often is necessary to eliminate occlusal interferences that would prevent the desired tooth movement, as for instance when a molar is being uprighted before a bridge or implant is placed. It also improves the crown-root ratio, which can be important in improving the periodontal prognosis when bone loss has occurred. Extrusion does not make it easier to place margins subgingivally, and this type of tooth movement is very difficult to accomplish with a removable appliance, so it does not make using removables easier or more effective.
Incorrect
No, that’s wrong. Reducing the height of the crown of a tooth that is being extruded often is necessary to eliminate occlusal interferences that would prevent the desired tooth movement, as for instance when a molar is being uprighted before a bridge or implant is placed. It also improves the crown-root ratio, which can be important in improving the periodontal prognosis when bone loss has occurred. Extrusion does not make it easier to place margins subgingivally, and this type of tooth movement is very difficult to accomplish with a removable appliance, so it does not make using removables easier or more effective.
Question 4
Which statement most correctly describes the place of adjunctive orthodontics in the treatment of temporomandibular dysfunction? For such a patient, adjunctive orthodontics is
- often the key to success.
- frequently an important aid in managing the patient’s problems.
- largely irrelevant to TMD, as a cause or cure. ✓
- as likely to make things worse as better.
- almost always to be avoided because of the chance of making TMD symptoms worse.
Correct
That’s right, orthodontic treatment is best described as having little relationship to TMD, either as a cure or as a cause of additional/worsening symptoms. Certainly neither the first nor last statement, the extreme view on either side, is correct. Sometimes adjunctive treatment can aid on controlling TMD, but that isn’t predictable. There are a number of valid reasons for adjunctive orthodontic treatment. Correcting TMD isn’t one of them.
Incorrect
No, that’s incorrect. Orthodontic treatment is best described as having little relationship to TMD, either as a cure for it or as a cause of additional/worsening symptoms. Certainly neither the first nor last statement, the extreme view on either side, is correct. Sometimes adjunctive treatment can aid on controlling TMD, but that isn’t predictable. There are a number of valid reasons for adjunctive orthodontic treatment. Correcting TMD isn’t one of them.
Question 5
Which of the following are differences in the diagnostic records needed for adjunctive orthodontics in adults as compared to treatment for children? In adults who are candidates for adjunctive orthodontics,
a. cephalometric analysis is more likely to be needed.
b. articulator-mounted models are less important.
c. periapical radiographs are more likely to be required.
d. evaluation of periodontal disease status is even more important.
- a and b
- b and c
- c and d ✓
- a, b, and c
- all of the above
Correct
That’s right. The second and third statements are correct, the other two are not. In adults who are candidates for adjunctive orthodontics, periapical radiographs are more likely to be required because evaluation of periodontal disease status is even more important than it is in children. In adults who will have limited rather than comprehensive orthodontics, however, cephalometric analysis is less, not more, likely to be needed than in children. The articulator-mounted models that are of little use in growing children—because growth changes the relationship of the condyles to the dentition, making the articulator relationship wrong quite quickly—can be important in adults in planning the restorative and/or surgical treatment.
Incorrect
No, that’s wrong. The second and third statements are correct, the other two are not. In adults who are candidates for adjunctive orthodontics, periapical radiographs are more likely to be required because evaluation of periodontal disease status is even more important than it is in children. In adults who will have limited rather than comprehensive orthodontics, however, cephalometric analysis is less, not more, likely to be needed than in children. The articulator-mounted models that are of little use in growing children—because growth changes the relationship of the condyles to the dentition, making the articulator relationship wrong quite quickly—can be important in adults in planning the restorative and/or surgical treatment.
Question 6
(A) At the doctor-patient conference in which a treatment plan is presented, a major role for the doctor is to be sure the patient accepts the total package of perio-ortho-restorative treatment that has been worked out, because (B) There is nothing to be gained from correcting only some, not all of the patient’s problems.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false ✓
Correct
That’s right, both these statements are false. The doctor’s role at the conference is to outline the patient’s problems, evaluate the alternative treatment possibilities, and present the alternatives as clearly and objectively as possible. The goal is to get the patient to understand the alternatives. That’s the heart of informed consent to treatment. It’s the patient’s choice, not the doctor’s, as to what treatment is to be done—but of course the doctor does not have to provide treatment that he or she does not think is in the patient’s best interest.
Incorrect
No, that’s incorrect. Both these statements are false. The doctor’s role at the conference is to outline the patient’s problems, evaluate the alternative treatment possibilities, and present the alternatives as clearly and objectively as possible. The goal is to get the patient to understand the alternatives. That’s the heart of informed consent to treatment. It’s the patient’s choice, not the doctor’s, as to what treatment is to be done—but of course the doctor does not have to provide treatment that he or she does not think is in the patient’s best interest.
Question 7
For a patient with spacing of maxillary incisors that he wants you to correct, who has no major restorations, no clinical evidence of periodontal disease or caries, and no symptoms indicating pulpal pathology, what radiographs would you order beyond a panoramic radiograph?
- Full periapical series, always needed for adult orthodontics
- Periapicals of the maxillary incisors that would be moved orthodontically
- Bitewings only
- Incisor periapicals, bitewings, and lateral ceph
- No other radiographs indicated in this situation ✓
Correct
That’s correct. For this patient, there is no indication for periapicals (no evidence of pulpal pathology or periodontal breakdown), no indication for bitewings (no caries or previous restorations), and no indication for a lateral ceph (no major change in tooth position or jaw relationships expected). Taking too many radiographs, of course, is as much a clinical error as taking too few.
Incorrect
No, that’s wrong. For this patient, there is no indication for periapicals (no evidence of pulpal pathology or periodontal breakdown), no indication for bitewings (no caries or previous restorations), and no indication for a lateral ceph (no major change in tooth position or jaw relationships expected). Taking too many radiographs, of course, is as much a clinical error as taking too few.
Question 8
If your goal in adjunctive treatment is to slide teeth along an archwire to obtain proper positioning for restorations, which of the following are important parts of an appropriate fixed appliance?
a. Flexible undersized archwire
b. Full-dimension rectangular archwire
c. Rigid archwire with clearance in the bracket slots
d. Tightly tied ligatures to hold the archwire in place
- a only
- b only
- c only ✓
- a and d
- c and d
Correct
That’s right, a rigid archwire with clearance in the bracket slots is needed if your goal is to slide teeth along it. It needs to be rigid so the wire doesn’t distort as the teeth slide, undersized relative to the bracket so that there is enough clearance to allow the teeth to slide, and tied loosely to reduce frictional resistance to sliding. So a flexible wire wouldn’t be a good choice, a full-dimension wire with no clearance wouldn’t work, and using tightly tied ligatures would all but prevent the teeth from moving along the archwire.
Incorrect
No, that’s wrong. The only correct answer is the third one. A rigid archwire with clearance in the bracket slots is needed if your goal is to slide teeth along it. It needs to be rigid so the wire doesn’t distort as the teeth slide, undersized relative to the bracket so that there is enough clearance to allow the teeth to slide, and tied loosely to reduce frictional resistance to sliding. So a flexible wire wouldn’t be a good choice, a full-dimension wire with no clearance wouldn’t work, and using tightly tied ligatures would all but prevent the teeth from moving along the archwire.
Question 9
When half the bone support for a tooth has been lost, and you need to move that tooth so you can restore the area properly, what adjustment must be made in the orthodontic force?
- Twice as much force needed in this situation to activate the cells
- Half again more force needed
- Movement stays the same, so does the force
- Half the regular force is needed ✓
- Force must reduce to one-fourth the regular amount
Correct
That’s right, pressure in the PDL is the key to producing the tooth movement, so if half the volume of the ligament has been lost, the force must be cut in half to obtain the correct pressure.
Incorrect
No, that’s wrong. Pressure in the PDL is the key to producing the tooth movement, so if half the volume of the ligament has been lost, the force must be cut in half to obtain the correct pressure.
Question 10
Which of the following are potential problems in the use of a removable appliance in adjunctive orthodontics for adults?
a. Much easier to obtain the moment of a couple than the moment of a force
b. Almost impossible to correct rotations
c. Interrupted force rather than continuous force
d. Increased difficulties with speech
- a and b
- b and c
- a, b, and c
- b, c, and d ✓
- all of the above
Correct
That’s right, the last three statements are correct, but the first one isn’t. With a removable appliance and springs against the surface of a tooth, you get not only a force but a moment that tips the tooth—whether you wanted it or not. The problem is that without a fixed attachment, it’s very difficult to generate the moment of a couple so that root position can be controlled and almost impossible to correct rotations. If an orthodontic appliance can be removed, it will be, so the force is interrupted rather than continuous, and removable appliances are more likely to generate speech problems (because they extend into tongue space). Fixed lingual appliances, occasionally used for comprehensive but not for adjunctive orthodontics, also create speech problems for many patients.
Incorrect
No, that’s wrong. The last three statements are correct, but the first one isn’t. With a removable appliance and springs against the surface of a tooth, you get not only a force but a moment that tips the tooth—whether you wanted it or not. The problem is that without a fixed attachment, it’s very difficult to generate the moment of a couple so that root position can be controlled and almost impossible to correct rotations. If an orthodontic appliance can be removed, it will be, so the force is interrupted rather than continuous, and removable appliances are more likely to generate speech problems (because they extend into tongue space). Fixed lingual appliances, occasionally used for comprehensive but not for adjunctive orthodontics, also create speech problems for many patients.
Question 11
If your goal is to upright a mesially tipped lower second molar without changing the position of the premolars and canine that serve as anchorage, how should you place the brackets on the anchor teeth?
- In a straight line along the crowns, so that a flat wire segment will fit ✓
- In the center of the crowns
- As recommended by the manufacturer, at variable distances from the cusp tips
- At any convenient place, since these teeth won’t move anyway
Correct
That’s right, it’s most efficient to place the brackets in a straight line along the crowns of the anchor teeth, so you won’t have to put bends in the wire to get it to fit passively. If you position them in the center of the crown, or relative to the cusp tips, or in some other apparently convenient way, it will be difficult to contour a wire so that it fits passively—but it has to be passive to prevent movement of these teeth in addition to movement of the molar. Of course, if you want to reposition the premolars as well as the molar—and often you will—the brackets need to be positioned so that a straight wire will fit when they’re in the ideal position, not when they’re misaligned as they are initially.
Incorrect
No, that’s wrong. It’s most efficient to place the brackets in a straight line along the crowns of the anchor teeth, so you won’t have to put bends in the wire to get it to fit passively. If you position them in the center of the crown, or relative to the cusp tips, or in some other apparently convenient way, it will be difficult to contour a wire so that it fits passively—but it has to be passive to prevent movement of these teeth in addition to movement of the molar. Of course, if you want to reposition the premolars as well as the molar—and often you will—the brackets need to be positioned so that a straight wire will fit when they’re in the ideal position, not when they’re misaligned as they are initially.
Question 12
(A) Adjunctive orthodontics is often the most important part of orthodontics in general practice because (B) Both the duration and complexity of treatment are less than in children.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false
Correct
That’s correct, both these statements are true and they have a cause-effect relationship. Adjunctive orthodontics in adults allows a better outcome of much perio/pros/restorative treatment. It is inherently more predictable than most orthodontic treatment in children, because the variables of growth and cooperation are all but eliminated. Technical skill in using fixed appliances is required, and with proper technique, excellent results can be obtained—which is not necessarily the case in children, no matter who does the treatment.
Incorrect
That’s wrong. Both these statements are true and they have a cause-effect relationship. Adjunctive orthodontics in adults allows a better outcome of much perio/pros/restorative treatment. It is inherently more predictable than most orthodontic treatment in children, because the variables of growth and cooperation are all but eliminated. Technical skill in using fixed appliances is required, and with proper technique, excellent results can be obtained—which is not necessarily the case in children, no matter who does the treatment.