Background
Reasons for Extraction: Orthodontic Camouflage
There are two reasons for extracting teeth in orthodontic treatment:
- correction of crowding/protrusion
- camouflage of jaw discrepancy
It is important to keep the difference in mind—which can be confusing because some patients with a skeletal problem (mandibular deficiency, for instance) also have crowded teeth.
This module focuses on the possibilities of extraction of teeth for camouflage of skeletal Class II and Class III malocclusions. Part 1 reviews extraction for crowding/protrusion in skeletal Class I patients.
Possibilities for Treatment of Skeletal Problems: Growth Guidance
Malocclusion caused by jaws that are not aligned correctly is defined as skeletal malocclusion. The term indicates that the problem is the jaw relationship, not the way the teeth are aligned. The most common skeletal malocclusion is Angle’s Class II, in which the upper incisors protrude, usually because of less mandibular than maxillary growth. Skeletal Class III, of course, is just the reverse, and there also are skeletal vertical (open bite/deep bite) and transverse (crossbite) problems.
An important concept: If the jaws are not in a correct relationship, there are three treatment possibilities:
- Guide growth so the deficient jaw catches up, and a normal jaw relationship is produced.
That, of course, is the ideal treatment approach, and it always should be used until there no longer is the possibility of enough correction from differential growth. This patient’s treatment to correct her Class II malocclusion succeeded because her lower jaw grew more than the upper.
 Image 1, pre-tx: Age 11, prior to treatment for a skeletal Class II problem. Image 1, pre-tx: Age 11, prior to treatment for a skeletal Class II problem. |  Image 2, post-tx: Age 14, after two-stage treatment and successful growth modification. Image 2, post-tx: Age 14, after two-stage treatment and successful growth modification. |
 Image 3, comparison: Pre-/posttreatment, successful growth modification. Image 3, comparison: Pre-/posttreatment, successful growth modification. |
Possibilities for Treatment of Skeletal Problems: Camouflage
Treatment possibilities for skeletal problems:
- Growth modification so that the deficient jaw catches up.
- Orthodontic camouflage, which is based on making the teeth fit in spite of the fact that the jaws don’t. This approach carries with it the idea that the jaw discrepancy will not be corrected but will no longer be noticed and will not be a problem, hence the term “camouflage.”
Camouflage treatment usually requires extraction of some teeth, but usually not the extraction of four first premolars, as in the treatment of crowding/protrusion.
For this boy, in whom growth modification was not successful in correcting his Class II malocclusion, extraction of upper first premolars and retraction of the upper incisors gave him both good occlusion and a normal facial appearance. If you look carefully you can see the decrease in prominence of the upper lip. He’s still skeletal Class II, but it really doesn’t show—so it’s successful camouflage.
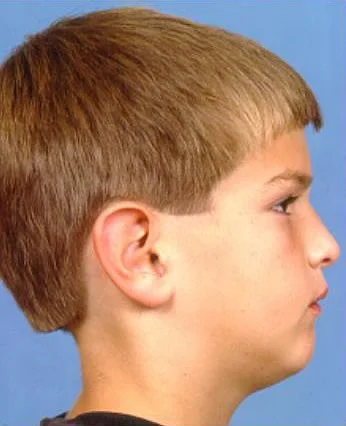 Image 1, pre-tx: Age 11, prior to treatment for a skeletal Class II problem. Image 1, pre-tx: Age 11, prior to treatment for a skeletal Class II problem. | 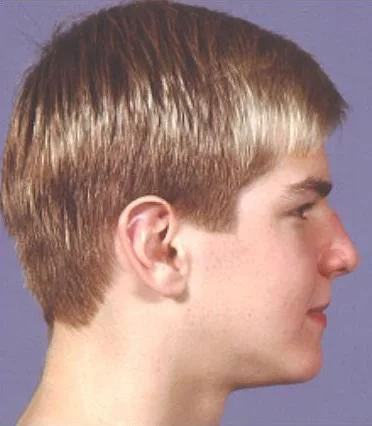 Image 2, post-tx: Age 14, after attempted growth modification failed, with extraction of upper 1st premolars for camouflage. Image 2, post-tx: Age 14, after attempted growth modification failed, with extraction of upper 1st premolars for camouflage. |
 Image 3, comparison: Pre-/post-tx with extractions for Class II camouflage. Image 3, comparison: Pre-/post-tx with extractions for Class II camouflage. |
Possibilities for Treatment of Skeletal Problems: Orthognathic Surgery
Treatment possibilities for skeletal problems:
- Growth modification so the deficient jaw catches up.
- Orthodontic camouflage.
- Orthognathic surgery to place the jaws in the correct position.
The techniques to do this were developed in the second half of the 20th century. At this point surgical correction of even extremely severe problems can be accomplished. The teaching module Indications for Orthognathic Surgery covers this in greater detail.
This girl also did not respond well to growth modification treatment. Her severe mandibular deficiency is apparent. For her, retracting the upper incisors would have made her deficient lower face even more apparent and her large nose look even larger. The result would be a camouflage failure even if the malocclusion were corrected—so surgery to advance the mandible was the appropriate treatment.
 Image 1, pre-surg: Age 13, after attempted growth modification, skeletal Class II persists. Image 1, pre-surg: Age 13, after attempted growth modification, skeletal Class II persists. |  Image 2, post-tx: Age 15, after orthognathic surgery to advance the mandible and correct the skeletal problem. Image 2, post-tx: Age 15, after orthognathic surgery to advance the mandible and correct the skeletal problem. |
 Image 3, comparison: Pre-/post-tx, orthognathic surgery to correct mandibular deficiency. Image 3, comparison: Pre-/post-tx, orthognathic surgery to correct mandibular deficiency. |
Treatment Type as a Function of Age
The type of treatment for jaw discrepancies is affected by the patient’s age.
Common sense tells you that growth modification is possible only when the patient is growing. So this type of treatment must be done prior to the end of the adolescent growth spurt. Usually, it is most effective when carried out during the growth spurt. After early adolescence, camouflage and surgery are the only possibilities. Unfortunately, growth modification does not always succeed, even if the patient cooperates.
Repositioning teeth for camouflage requires reasonably accurate prediction of growth, and the pattern of growth is notoriously unpredictable. If you aren’t sure what the final jaw relationship will be, you don’t know where to put the teeth to compensate for the jaw relationship. So camouflage should not be done until late adolescence, when it is apparent that correction via growth modification no longer is feasible and the final jaw relationship is nearly established.
Surgical correction for nearly all patients is indicated only when growth is complete or nearly complete. This means that with some exceptions for syndromic or exceptionally severe problems, surgery is not done until at or near the end of adolescent growth.

Class II Camouflage
Class II Camouflage
Class II malocclusion is the major indication for orthodontic camouflage. In Class II, the upper incisors protrude. The space to retract them is obtained by extracting the maxillary first premolars.
There are three possible extraction patterns:
- Maxillary first premolars
- Maxillary first and mandibular second premolars
- Maxillary and mandibular first premolars
Why extract in the mandibular arch if the goal is to retract the upper but not the lower incisors? It would be important not to retract the lower incisors—if that happened the overjet could not be reduced. But it also is important not to move the lower incisors more than slightly forward, because then lip pressure would cause them to relapse backward, leading to both incisor crowding and return of excessive overjet.
So extraction in the lower arch is done when Class II elastics will be used during the treatment to help reduce the overjet. These elastics, connected from the lower molars to the upper incisors, pull the upper incisors back and the lower molars forward.
In camouflage treatment when Class II elastics are planned, rather than first premolar extraction in the lower arch, second premolar extraction often is employed to guard against any retraction of the lower incisors. If the lower arch also is somewhat crowded, the combination of elastics and lower first premolar extraction might be needed to maintain the position of the incisors.
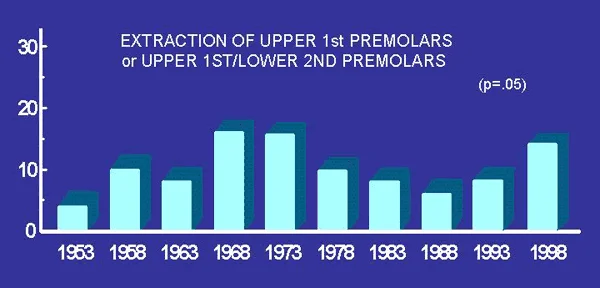
Extraction Percentages over Time
About 40% of the patients seen in a typical American orthodontic practice have Class II malocclusion. Although there have been some fluctuations in the number of patients with the extraction pattern typical for Class II (upper first premolars alone or upper first/lower second premolars), the changes are not nearly as dramatic as those for four first premolars, the typical extraction pattern for Class I crowding/protrusion.
The figure shows the percentage of patients in the orthodontic clinic at UNC with extractions for Class II camouflage over a 45-year period. Although the percentage of patients with this extraction pattern was greater at the height of enthusiasm for premolar extraction in the 1960s, it did not change nearly as much as the extraction percentage for Class I crowding/protrusion patients (see To Extract or Not to Extract, part 1).
It is interesting that the percentage of Class II camouflage extractions increased somewhat in the late 1990s. This probably reflects camouflage for some patients who might have been treated better with orthognathic surgery, after denial of coverage for surgery by insurance companies.
Typical Class II Camouflage Patient
Sometimes it is thought the camouflage always is a compromise, really not the best treatment. But in the right circumstance camouflage can be very effective.
Consider Diana, who was seen initially at age 16. When asked why she had sought treatment, she just smiled (image 1)—and then explained that she tried not to smile because her teeth looked so bad. It’s a significant handicap to spend a lot of your time trying not to smile. That’s a psychosocial handicap, a good example of the reason most patients seek orthodontic treatment.
In profile (image 2), you can see that she has a weak chin, and the cephalometric radiograph (image 3) makes it clear that she has a deficient mandible. This is a skeletal Class II malocclusion, but with crowding rather than protrusion of the upper incisors—Class II division 2, in other words.
If she had been seen earlier, prior to adolescence, growth modification treatment would have been attempted, and if it had been successful, it might have been possible to treat her without extraction. At this point, the only possibilities are camouflage, which would require premolar extraction to provide space to align her upper incisors without protruding them, or surgery to advance her mandible after incisor alignment created excessive overjet.
 Image 1, frontal view: Diana, age 16: “My teeth stick out and are crooked and ugly. Image 1, frontal view: Diana, age 16: “My teeth stick out and are crooked and ugly. | 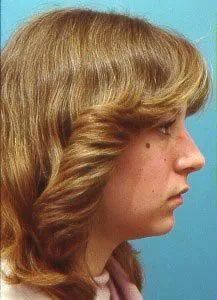 Image 2, profile: Diana, age 16, profile view showing lack of projection of the mandible. Image 2, profile: Diana, age 16, profile view showing lack of projection of the mandible. |
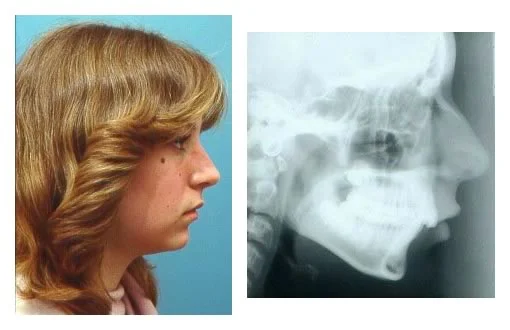 Image 3, profile/ceph: The cephalometric radiograph reveals the extent of the mandibular deficiency. Image 3, profile/ceph: The cephalometric radiograph reveals the extent of the mandibular deficiency. |
Typical Class II Camouflage Patient (cont.)
Diana had the classic dental occlusion of Class II division 2, with the upper incisors crowded and upright and only mild crowding in the lower arch.
When a skeletal Class II relationship exists, the lower lip usually is behind the upper incisors, so they tip facially and overjet is present. This is the classic presentation of Class II division 1. But sometimes the lower lip remains in front of the upper incisors, which tips them lingually and leads to crowding. It’s easier to get your lower lip in front of your upper teeth if your face height is short, so Class II division 2 patients usually have a short face and deep bite.
The greater crowding in the upper than the lower arch that occurs in Class II division 2 is because the upper incisors are tipped lingually by the lower lip pressure. The upper incisors hold the lower lip away from the lower incisors, so crowding is minimized in the lower arch.
 Image 1, frontal view: Diana, age 16, Class II division 2 malocclusion. Image 1, frontal view: Diana, age 16, Class II division 2 malocclusion. |  Image 2, right lateral: Diana, age 16, Class II division 2 malocclusion. Image 2, right lateral: Diana, age 16, Class II division 2 malocclusion. |
 Image 3, left lateral: Diana, age 16, Class II division 2 malocclusion. Image 3, left lateral: Diana, age 16, Class II division 2 malocclusion. |  Image 4, maxillary occlusal: Diana, age 16, Class II division 2 malocclusion. Image 4, maxillary occlusal: Diana, age 16, Class II division 2 malocclusion. |
 Image 5, mandibular occlusal: Diana, age 16, Class II division 2 malocclusion. Image 5, mandibular occlusal: Diana, age 16, Class II division 2 malocclusion. |
Diana: Treatment Options
Diana was told that her treatment options were orthodontics alone or jaw surgery, but she also was told that for her, the orthodontic option could produce a satisfactory result. She and her family chose the orthodontic (camouflage) option.
Diana was treated with extraction of maxillary first premolars only. This meant minimal use of Class II elastics, so a transpalatal lingual arch was used to augment the resistance of upper molars to being moved forward as the extraction space was closed. The extraction space was used largely for retraction of the maxillary canines. Then the upper incisors were aligned and their roots were torqued lingually. This is a classic form of Class II camouflage.
In this cephalometric radiograph taken toward the end of treatment, you can see that overjet and overbite are now normal and the incisor roots are in a much more normal position.

Treatment Outcome: Dentition
Diana’s orthodontic treatment required 24 months. These images show her dental relationships at the completion of treatment.
Note that with upper first premolar extraction, the Class II molar relationship remains, but overjet and overbite now are normal, and the teeth are well aligned. The maxillary premolar extraction spaces were closed by distal movement of the canines.
The malocclusion has been corrected quite satisfactorily.
Is this successful camouflage treatment?
The truth is that just from looking at the dental occlusion, you don’t know.
 Image 1, frontal view: Diana, age 18, at completion of treatment. Image 1, frontal view: Diana, age 18, at completion of treatment. |  Image 2, right lateral: Diana, age 18, at completion of treatment. Image 2, right lateral: Diana, age 18, at completion of treatment. |
 Image 3, left lateral: Diana, age 18, at completion of treatment. Image 3, left lateral: Diana, age 18, at completion of treatment. |  Image 4, maxillary occlusal: Diana, age 18, at completion of treatment. Image 4, maxillary occlusal: Diana, age 18, at completion of treatment. |
 Image 5, mandibular occlusal: Diana, age 18, at completion of treatment. Image 5, mandibular occlusal: Diana, age 18, at completion of treatment. |
Treatment Outcome: Facial
Only when you look at the face can you judge the success of camouflage.
Diana now enjoys displaying her smile (image 1). Successful camouflage requires two things: acceptable dental occlusion and acceptable facial esthetics. After treatment, the smile esthetics are quite acceptable, and the mandibular deficiency is hard to see (so the camouflage is successful).
The post-treatment cephalometric radiograph (image 2) shows that she still is mandibular deficient, so the jaw discrepancy still is present. It’s just that at this point you don’t see it clinically (unless you have x-ray vision!).
It’s easier to follow what happened in treatment by superimposing tracings of the pre- and post-treatment cephalometric radiographs (image 3). Note that, as one would have expected, she didn’t grow. The treatment change was almost totally retraction, torque, and intrusion of the upper incisors.
With the amount of tooth movement that occurred in this case, it is not surprising that there was some shortening of the roots of the upper incisors (note the shortening of root length seen in the superimposition tracing). That, fortunately, is not a long-term problem, but it is necessary to warn camouflage patients that some minor root resorption, especially of the upper incisors, is likely to occur, and that there is a small chance (2-3%) of loss of more than 1/4 of the root length.
Bottom line (image 4): what to the patient was an unacceptable situation now is acceptable—and that’s the definition of successful camouflage.
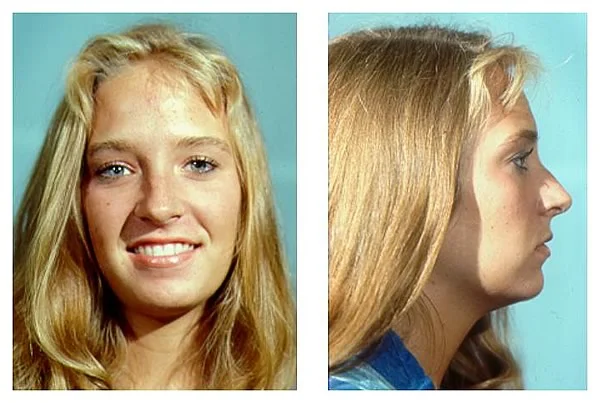 Image 1, post-tx face: Diana, age 18, post-treatment. Smile esthetics are now quite acceptable, and the mandibular deficiency now is hard to see. Image 1, post-tx face: Diana, age 18, post-treatment. Smile esthetics are now quite acceptable, and the mandibular deficiency now is hard to see. | 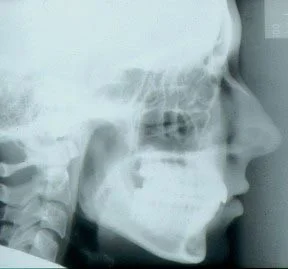 Image 2, post-tx ceph: Post-tx ceph shows that mandibular deficiency still is present. Image 2, post-tx ceph: Post-tx ceph shows that mandibular deficiency still is present. |
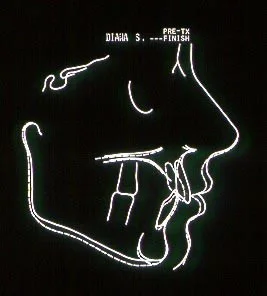 Image 3, superimposition tracing: Superimposition tracing, pre- to post-treatment. Image 3, superimposition tracing: Superimposition tracing, pre- to post-treatment. |  Image 4, smile comparison: Camouflage solved the problem of smile esthetics. Image 4, smile comparison: Camouflage solved the problem of smile esthetics. |
Class II Camouflage Failure
If extensive orthodontic treatment fails to camouflage the underlying jaw discrepancy, an improvement in dental occlusion isn’t much of a consolation prize.
This 18-year-old student sought further orthodontic consultation after going away to college because she was unhappy with the result of her four years of previous orthodontic treatment, first with attempted growth modification, then with extraction of upper and lower premolars. As you can see in the dental casts (image 1), the occlusion is not too bad—about 1/2 cusp Class II, with mildly excessive overjet, and if you only looked at the teeth, you might wonder what she was complaining about.
It’s when you see her face (image 2) that the camouflage failure becomes apparent. She has severe mandibular deficiency. A first stage of growth modification succeeded in restricting the growth of her upper jaw but did not correct the skeletal problem, and in the attempted camouflage, her maxillary incisors were retracted much too far for acceptable esthetics.
She was told that orthognathic surgery to reposition both jaws and her chin was the only way to achieve an esthetically acceptable result. Further orthodontic treatment would be more likely to do harm than good. She had been treated for so long already, she just wasn’t willing to do that. She chose to live with what can only be described as a treatment failure.
Bottom line: If the mandibular deficiency is severe enough, camouflage simply can’t produce an acceptable result.
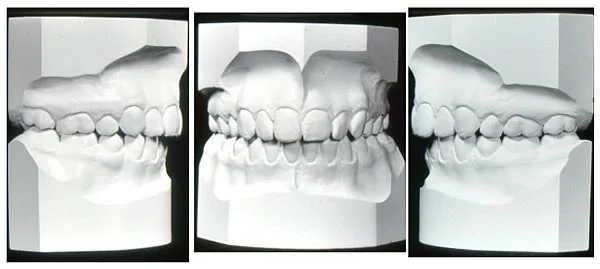 Image 1, dental casts: Age 18, after 4 years of orthodontic treatment, premolar extraction both arches: camouflage failure. Image 1, dental casts: Age 18, after 4 years of orthodontic treatment, premolar extraction both arches: camouflage failure. | 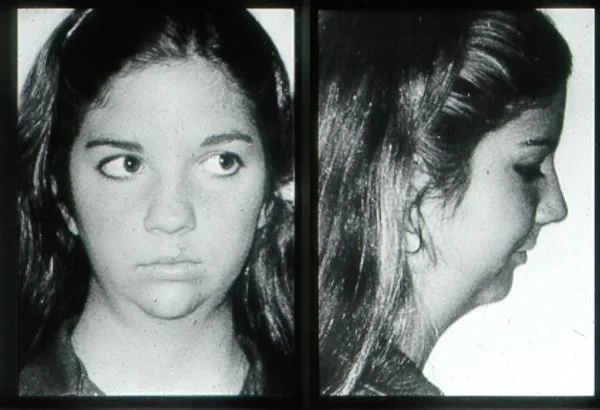 Image 2, facial appearance: Age 18, after 4 years of orthodontic treatment, premolar extraction both arches: camouflage failure. Image 2, facial appearance: Age 18, after 4 years of orthodontic treatment, premolar extraction both arches: camouflage failure. |
Camouflage vs Surgery
Deciding Between Camouflage and Surgery
As usually is the case, there’s a gray area between patients who are clear-cut candidates for camouflage because of relatively mild problems and patients who would require surgery because of very severe problems. How does one decide between these alternatives in a borderline situation?
Consider Adam, age 18, who wants his teeth fixed. Why? Because he doesn’t like his bite and doesn’t like the way things look.
Note that he doesn’t show his teeth when he smiles. Like Diana, whom we saw earlier, he knows his dental appearance detracts, and he really tries not to show his teeth.
From the profile view, a skeletal Class II jaw relationship due to mandibular deficiency is obvious.
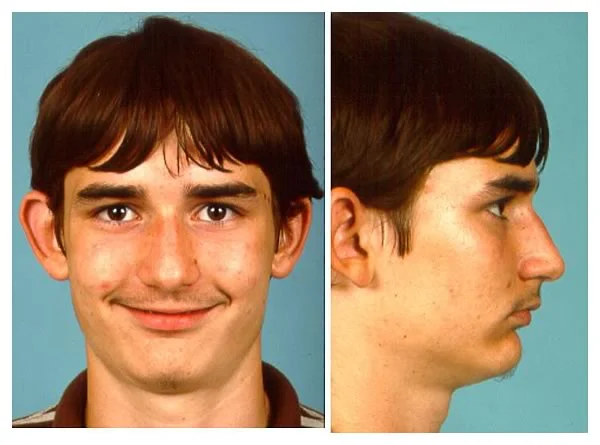
Deciding Between Camouflage and Surgery (cont.)
Also like Diana, Adam has a Class II division 2 malocclusion, with crowded and irregular maxillary incisors and a deep bite.
He has congenitally missing second premolars and retained second primary molars in both arches.
 Image 1, frontal view: Adam, age 18, Class II division 2 malocclusion. Image 1, frontal view: Adam, age 18, Class II division 2 malocclusion. |  Image 2, right lateral: Adam, age 18, Class II division 2 malocclusion. Image 2, right lateral: Adam, age 18, Class II division 2 malocclusion. |
 Image 3, left lateral: Adam, age 18, Class II division 2 malocclusion. Image 3, left lateral: Adam, age 18, Class II division 2 malocclusion. |  Image 4, maxillary occlusal: Adam, age 18, Class II division 2 malocclusion. Image 4, maxillary occlusal: Adam, age 18, Class II division 2 malocclusion. |
 Image 5, mandibular occlusal: Adam, age 18, Class II division 2 malocclusion. Image 5, mandibular occlusal: Adam, age 18, Class II division 2 malocclusion. |
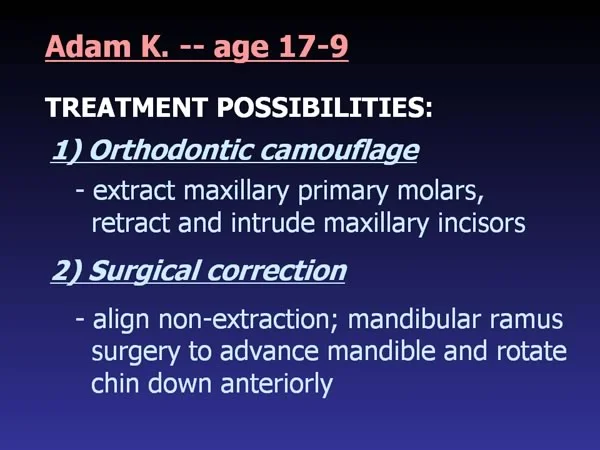
Camouflage and Surgery Possibilities
For Adam, there are two possible treatment approaches:
- Camouflage with extraction of second primary molars and closure of the second premolar spaces. This would be difficult because it would be necessary to retract the maxillary first premolars, then the canines, but it is feasible.
- Orthognathic surgery, with the arches aligned without extraction in preparation for the surgery. Eventually, the second primary molars would have to be replaced, but they would be maintained as long as possible.
If you’re the doctor, how do you make the choice between the alternative treatment plans?
Patient, Not Doctor, Decides
The answer is very simple:
In the modern world, the doctor doesn’t make that choice, the patient does!
The doctor’s role is to give the patient the information needed to make an informed decision. It has been a moral imperative for a long time that alternative treatment possibilities must be presented to the patient. This now is the legal requirement in the United States, and the consequences of no treatment also must be explained.
Computer Simulations
When camouflage or orthognathic surgery are the alternative treatment possibilities, the major difference is likely to be the effect on facial proportions. This, of course, affects facial esthetics. It can be difficult for patients to understand what the difference in the esthetic outcomes might be. Computer simulations of the facial effects of treatment recently have become an important tool in helping patients decide.
It is possible now to use computer algorithms that relate the amount of change in the facial soft tissues to the amount of change in underlying hard tissues. In the absence of growth, these simulations are surprisingly accurate, good enough for patients to understand.
For Adam, as we have noted, one possibility is to correct his malocclusion by retracting his upper incisors, which would leave his facial appearance largely unchanged. The other possibility is surgical advancement of the deficient mandible, which would bring his chin down and forward and give him a “stronger” chin.
It’s one thing to tell him that. It’s something else to show him.
Here are Adam’s cephalometric tracing and soft tissue profile (image 1), and predictions of what he would look like with premolar extraction for camouflage (image 2) and with arch expansion followed by mandibular advancement (image 3). His problem is not too severe for orthodontic correction, at least as far as obtaining reasonably normal occlusion. In the prediction tracings, the dotted lines are pretreatment, solid lines are the prediction.
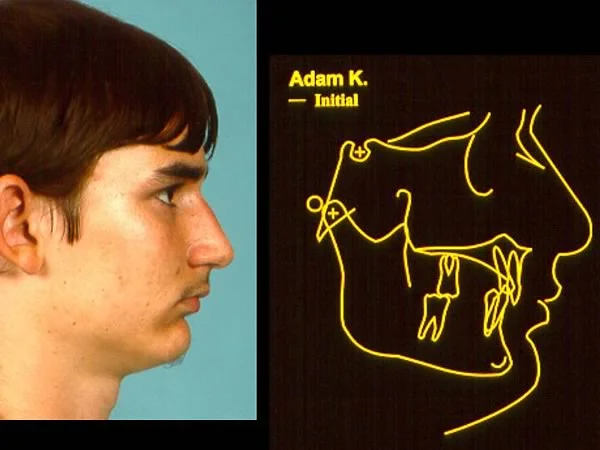 Image 1, pre-treatment: Adam, age 18, profile/cephalometric tracing prior to treatment. Image 1, pre-treatment: Adam, age 18, profile/cephalometric tracing prior to treatment. | 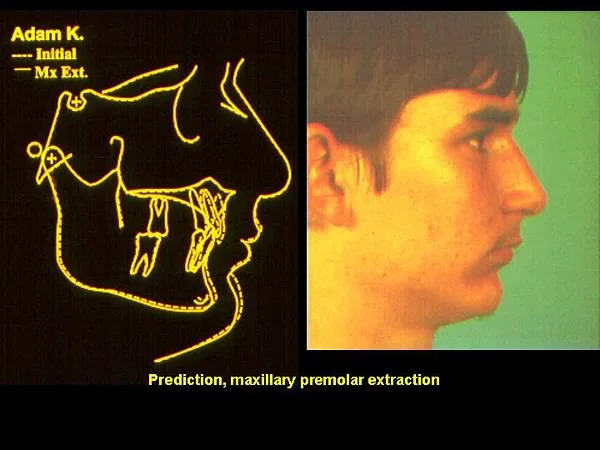 Image 2, camouflage prediction: Cephalometric/profile prediction, premolar extraction for camouflage. Image 2, camouflage prediction: Cephalometric/profile prediction, premolar extraction for camouflage. |
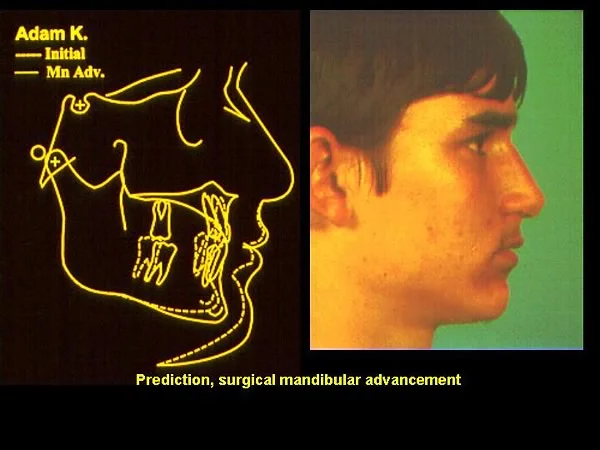 Image 3, surgery prediction: Cephalometric/profile prediction, arch expansion, and surgical mandibular advancement. Image 3, surgery prediction: Cephalometric/profile prediction, arch expansion, and surgical mandibular advancement. |
Computer Simulations (cont.)
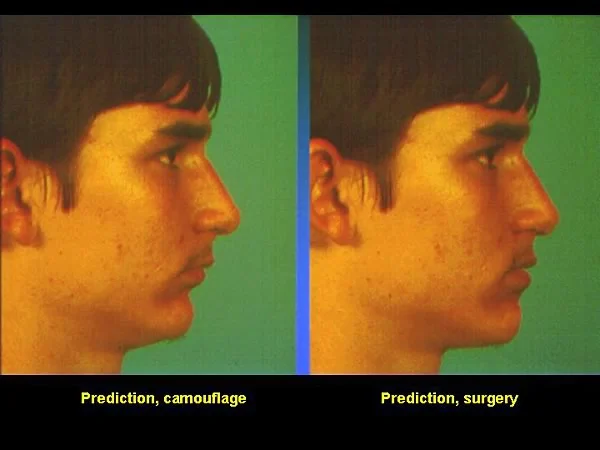
So looking at this image of the predictions side by side, which treatment do you think Adam would choose?
As always, the surgical treatment has the potential to make a greater difference in facial appearance, but would be more costly and would carry a greater risk. Adam and his parents would have to make their choice based on their reaction to the difference.
Somewhat to the doctor’s surprise, Adam was enthusiastic about the change produced by surgery. He had given the impression that he didn’t care very much about how he looked, but both he and his parents had no problem in identifying surgery as the treatment they wanted. He went ahead with orthodontic preparation for surgery that involved aligning his upper incisors and creating overjet, to provide space for mandibular advancement, had the jaw surgery and finishing orthodontics, and was quite happy with the outcome.
But in other cases with similar changes, the reaction was, “I wouldn’t do the surgery for no more change than that.” It’s the patient’s choice. The doctor has no right to play God and make the decision for the patient.
Class III Camouflage
Class III Camouflage
Camouflage of skeletal Class III problems, as a rule, is less successful than Class II camouflage. The problem is that retracting the lower incisors does not make a protruding chin less prominent, and in fact may make it even more obvious.
This means two things:
- a higher percentage of skeletal Class III than Class II patients will require surgery, and
- retracting the lower incisors a long way rarely is indicated, even if it would produce normal dental occlusion. Extracting only upper premolars to camouflage skeletal Class II often is a good idea; extracting only lower premolars to camouflage skeletal Class III usually is a bad idea.
An interesting alternative for Class III camouflage patients is the extraction of one lower incisor. It seems that this would not be compatible with normal occlusion, but if the upper incisors are inclined facially and the lower incisors are upright, often good dental relationships can be obtained with three lower incisors. In fact, you should remember from the previous courses that late mandibular growth is the major cause of the mandibular incisor crowding that happens to most people in their late teens and early 20s. The more the growth pattern tends toward Class III, the greater the chance that normal alignment of the lower anterior teeth would require three (not four) incisors.
Class III Camouflage (cont.)
Consider the situation for Sally, age 13.
She had a moderately severe skeletal Class III malocclusion due to a prominent mandible (image 1), with slight reverse overjet. Mild maxillary spacing was apparent when she smiled, and lower as well as upper incisors were displayed.
Sally’s major concern, and that of her parents, was the appearance of the maxillary incisors, especially the spacing.
She was a quite mature young lady. It was unlikely that she would have a large amount of further (and disproportionate) mandibular growth. Patients of African descent often have a more prominent mandible than Europeans. For her, this was a family characteristic, but there was no history of severe Class III problems.
The teeth in both arches (image 2) were well aligned. She had spacing in the maxillary arch that reduced the tendency toward anterior crossbite, but she still had an end-to-end incisor relationship. The maxillary lateral incisors were small (these teeth are particularly likely to be missing or small in Class III patients).
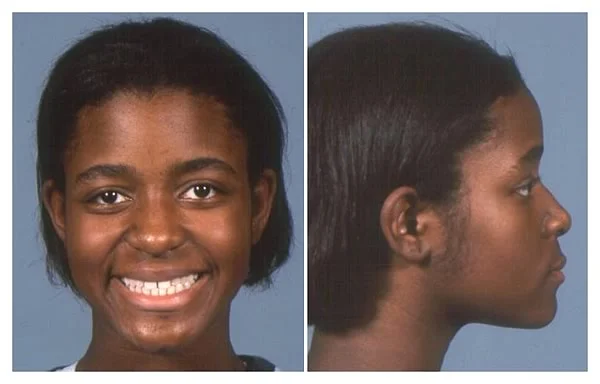 Image 1, face: In general, facial esthetics are acceptable despite the strong chin. Image 1, face: In general, facial esthetics are acceptable despite the strong chin. |  Image 2, teeth: Dental relationships. Image 2, teeth: Dental relationships. |
Orthodontic Treatment Plan
The plan for Sally was to remove one lower incisor and close the extraction space, which would allow moderate retraction of the remaining incisors. Then spaces could be closed in the upper arch while maintaining correct overjet and overbite. The small maxillary lateral incisors would help compensate for the potential tooth-size discrepancy created by the incisor extraction, as would the upright lower and somewhat proclined upper incisors that the jaw relationship made necessary.
Following treatment (image 1), one lower central incisor was exactly in the middle of the mandibular arch, but both overjet/overbite and occlusion of the posterior teeth were nearly ideal. The location of the maxillary dental midline is esthetically important. The location of the mandibular dental midline isn’t. Even dentists sometimes overlook a missing lower incisor unless they are careful to count the teeth—three lower incisors can look perfectly normal.
Successful camouflage? Again, you don’t know until you look at her face.
Although Sally still has a strong chin at the end of treatment (image 2), her facial appearance is within normal variation, and in fact she is quite attractive. For her, Class III camouflage was the appropriate treatment because the jaw discrepancy was mild. Premolar extraction would not have been as satisfactory as the lower incisor extraction—it would have retracted the lower incisors too much.
 Image 1, post-tx teeth: Sally, age 14, retainers in place after extraction of one lower incisor and space closure in both arches. Image 1, post-tx teeth: Sally, age 14, retainers in place after extraction of one lower incisor and space closure in both arches. | 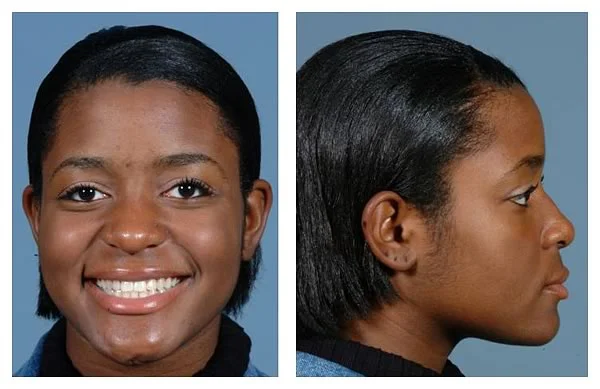 Image 2, post-tx face: Sally, age 14, Class III camouflage. Image 2, post-tx face: Sally, age 14, Class III camouflage. |
Summary/Conclusions
Camouflage of Other Skeletal Problems
Extraction of teeth allows retraction or proclination of incisors, with the movement almost totally in the anteroposterior plane of space. For that reason, extraction is of little or no help in patients with vertical problems—the space is created in the wrong plane of space. This also is true for transverse skeletal problems.
So camouflage is done frequently for Class II patients, especially those who have maxillary dental protrusion and mild or moderate mandibular deficiency. It is done occasionally for Class III patients with mild skeletal problems, and rarely for those who have other types of skeletal problems.
As a treatment plan, camouflage sometimes attracts extreme opinions. It has been highly praised on some occasions as being good enough for almost all patients with skeletal problems (which we can label as the self-serving insurance company fallacy) or condemned as an old-fashioned approach to problems better treated surgically in the modern world (often offered as an excuse for never being willing to extract teeth for orthodontic purposes).
Neither of those extreme views is correct. Mild to moderate problems can be camouflaged, severe ones cannot. Who decides what is too severe for orthodontics alone? The patient, not the doctor.
Appropriate patient selection, with a major role given to the patients who see computer simulations to help them decide, is the key to success with camouflage.
Problems with Camouflage
There are two major potential problems associated with camouflage:
- Worse, not better, facial esthetics. Retracting the incisors too much can make the skeletal problem more apparent, just the opposite of camouflaging it.
- Loss of root length (root resorption) of the maxillary incisors. This is known to occur more frequently in Class II or Class III camouflage than in other types of orthodontic treatment. It reflects the amount of tooth movement that often is required, and the chance that the roots of the teeth (especially the upper incisors) will be thrown against the cortical plates of bone.
Some dentists have been concerned that retracting the upper incisors could lead to development of TM pain/dysfunction. When it was claimed in the early 1990s that upper premolar extraction led to TMD, the rationale was that retracting the incisors led to incisal interferences and that this caused TMD.
Perhaps that is theoretically possible, although retracting the incisors enough to produce interferences would be difficult to accomplish in most Class II patients even if that were the goal. More important, clinical studies have not shown any relationship between upper premolar extraction and TMD. So TMD isn’t a complication of camouflage.
Conclusions
Camouflage of skeletal malocclusion is based on retracting protruding incisors. It usually involves retracting upper incisors in Class II patients after extraction of maxillary first premolars. Ocasionally it is possible to treat mild Class III patients by retracting lower incisors after extraction of one lower incisor or second premolars.
The goals of camouflage treatment are to simultaneously obtain normal dental occlusion and normal facial soft tissue contours. The treatment can be judged as successful only if both these goals are met.
Camouflage rarely is adequate treatment for patients with severe jaw discrepancies. The alternative, orthognathic surgery, must be considered for these patients.
The patient must be involved in the decision for camouflage versus orthognathic surgery. Computer simulations of possible treatment outcomes are a valuable tool in providing information to help patients decide what treatment they want, especially in borderline situations when both camouflage and surgery are reasonable alternatives.
Possible complications of camouflage include unfortunate facial esthetic changes and root resorption of upper incisors, but the evidence shows that despite claims to the contrary, it does not lead to the development of TMD.
Self-Test Referral
The self-test section of this program is designed to help you be sure you have understood the material. Read the assigned material in Contemporary Orthodontics, (5th ed., pp ; 4th ed., pp. ), then take the test, and use it as a guide for further study and review.
Copyright 2013, UNC Dept. of Orthodontics
Self-Test
Question 1
Which of the following would be considered camouflage treatment?
a. Retraction of protruding upper incisors
b. Retraction of protruding lower incisors
c. Retraction of both upper and lower incisors
d. Midpalatal expansion (sutural expansion) of a narrow maxillary arch to treat posterior crossbite
- a and b ✓
- c and d
- a, b, and c
- a, b, and d
- all of the above
Correct
That’s right, retraction of protruding upper incisors is typical camouflage for skeletal Class II problems; retraction of protruding lower incisors could be camouflage for skeletal Class III. Retraction of incisors in both arches implies correction of crowding/protrusion in patients who don’t have a jaw discrepancy, so that isn’t camouflage. Neither is sutural expansion of a narrow maxillary arch, because if the midpalatal suture opens, the maxilla is widened and the skeletal discrepancy is corrected.
Incorrect
No, that’s wrong. Retraction of protruding upper incisors is typical camouflage for skeletal Class II problems; retraction of protruding lower incisors could be camouflage for skeletal Class III. Retraction of incisors in both arches implies correction of crowding/protrusion in patients who don’t have a jaw discrepancy, so that isn’t camouflage. Neither is sutural expandsion of a narrow maxillary arch, because if the midpalatal suture opens, the maxilla becomes wider and the skeletal discrepancy is corrected, not camouflaged.
Question 2
Which of the following are appropriate times for orthodontic camouflage?
a. preadolescence
b. adolescent growth spurt
c. late adolescence
d. early adult life
- a and b
- a and c
- c and d ✓
- a, b, and c
- b, c, and d
Correct
That’s right, camouflage treatment isn’t indicated until after the adolescent growth spurt is over, or nearly over. It’s acceptable in late adolescence and in adults, but not in children who still have a lot of growth left. Growth modification, avoiding the displacement of teeth that is typical of camouflage, should be attempted first in growing children.
Incorrect
No, that’s wrong. Camouflage treatment isn’t indicated until after the adolescent growth spurt. It’s acceptable in late adolescence and in adults, but not in children who still have a lot of growth left. Growth modification, avoiding the displacement of teeth that is typical of camouflage, should be attempted first in growing children.
Question 3
Which of the following are appropriate extraction patterns for Class II camouflage?
a. one lower incisor
b. upper first premolars
c. upper first and lower second premolars
d. upper and lower first premolars
- a only
- a and b
- b and c
- a, b, and c
- b, c, and d ✓
Correct
That’s right, upper first premolar extraction, alone or in combination with lower second premolar extraction (usually) or lower first premolar extraction (occasionally) is used for Class II camouflage. Extraction of one lower incisor implies Class III, not Class II camouflage.
Incorrect
No, that’s wrong. Extraction of one lower incisor implies Class III, not Class II camouflage. Upper first premolar extraction, alone or in combination with lower second premolar extraction (usually) or lower first premolar extraction (occasionally) is used for Class II camouflage.
Question 4
(A) The major reason patients seek correction of Class II or Class III problem is to improve jaw function, because (B) Incisor contact is difficult to achieve in Class II and impossible in Class III.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true ✓
- A and B false
Correct
That’s right, the first statement is false, but the second is true. Some patients seek treatment primarily to improve function, and it’s true that normal incisor function is lacking in Class II and Class III patients. But the great majority who bring their children for treatment or seek it themselves as adults have concerns about their appearance. When protruding upper incisors and a deficient chin cause you to be judged stupid until proved otherwise, and a sunken-in midface and prominent lower jaw makes you a witch, concerns about facial appearance are much more than just vanity.
Incorrect
No, that’s wrong. The first statement is false, but the second is true. Some patients seek treatment primarily to improve function (or at least claim they do), and it’s true that normal incisor function is lacking in Class II and Class III patients. But the great majority who bring their children for treatment or seek it themselves as adults have concerns about their appearance. When protruding upper incisors and a deficient chin cause you to be judged stupid until proved otherwise, and a sunken-in midface and prominent lower jaw makes you a witch, concerns about facial appearance are much more than just vanity.
Question 5
Patients are likely to judge their camouflage treatment as a failure if
a. incisors are retracted too much, affecting facial appearance.
b. incisors are not retracted enough, so that excess overjet remains.
c. extraction spaces are not closed.
d. vertical problems are not corrected.
- a only
- a and d
- a, b, and c
- b, c, and d
- all of the above ✓
Correct
That’s right, all these factors probably would lead patients to judge their camouflage treatment a failure. The most significant ones, however, are those that affect facial appearance. If you sought treatment to improve your appearance and the effect was to improve your dental occlusion while making facial appearance worse, you would be justifiably upset.
Incorrect
No, that’s incorrect. All these factors probably would lead patients to judge their camouflage treatment a failure. The most significant ones, however, are those that affect facial appearance. If you sought treatment to improve your appearance and the effect was to improve your dental occlusion while making facial appearance worse, you would be justifiably upset.
Question 6
Why are computer simulations of treatment outcomes used for postadolescent camouflage and surgery patients, but not for younger patients?
- Growth prediction is almost impossible ✓
- Younger patients are too immature to choose appropriately
- Parents of younger children object to prediction techniques
- Predictions are just as useful in younger patients
Correct
That’s right, computer simulations of treatment effects, in the absence of growth, can be accurate enough to be useful clinically, but in children with skeletal problems, the combination of growth and treatment is almost impossible to predict accurately. If prediction worked for younger patients, it could be quite useful in helping patients and parents choose among alternatives, but simulations have to be at least reasonably accurate or they’re just misleading.
Incorrect
No, that’s wrong. They aren’t used with younger patients because in children with skeletal problems, the combination of growth and treatment is almost impossible to predict accurately. If prediction worked for younger patients, it could be quite useful in helping patients and parents choose among alternatives, but simulations have to be at least reasonably accurate or they’re just misleading.
Question 7
Which of the following are reasons for many fewer Class III than Class II patients treated with extraction for camouflage?
a. Fewer Class III patients in the population
b. Retracting the lower incisors tends to make the chin more prominent
c. Class III patients often have a large nose, and extraction for camouflage may make it look bigger
d. On a percentage basis, as many Class IIIs as Class IIs have camouflage
- a and b ✓
- c and d
- a, b, and c
- b, c, and d
- all of the above
Correct
That’s right, the first 2 items are reasons for the lower number of Class III patients: there are fewer of them, and a large chin is difficult to camouflage. The size of the nose is a factor in Class II camouflage but is not particularly relevant for Class III patients. The percentage of Class III patients who have camouflage is lower than Class II because retracting the incisors often makes the chin look even stronger. A prominent chin is a major concern for Class III patients. They don’t want it made even more prominent by retracting the lower incisors.
Incorrect
No, that’s wrong. Tte first 2 items are reasons for the lower number of Class III patients: there are fewer of them, and a large chin is difficult to camouflage. The size of the nose is a factor in Class II camouflage but is not particularly relevant for Class III patients. The percentage of Class III patients who have camouflage is lower than Class II because retracting the incisors often makes the chin look even stronger. A prominent chin is a major concern for Class III patients. They don’t want it made even more prominent by retracting the lower incisors.
Question 8
Orthodontic camouflage isn’t a good idea for patients with a long face, open bite problem. Why? Which of the following are correct?
a. Elongating the incisors to close the bite often makes facial appearance worse
b. Retracting the incisors does not shorten excessive face height although it may reduce the extent of the open bite
c. Attempts at camouflage may make the nose and chin more prominent
d. No need to try camouflage, open bite often corrects itself spontaneously
- a and b ✓
- c and d
- a, b, and c
- b, c, and d
- all of the above
Correct
That’s right. Elongating the incisors often makes facial appearance worse rather than better by exposing too much of the teeth (and often the gingiva as well) beneath the lips, and changing the a-p position of anterior teeth does not reduce excessive face height. There is little effect on the nose and chin, however. Although open bite tends to correct itself in young children with normal jaw relationships, self-correction almost never occurs in adolescents. For the girl in this image, the upper teeth already are too far below the lip line for good facial esthetics. Elongating them further, with or without extraction, might close her open bite but would damage rather than improve facial esthetics. She is a candidate for surgery.
Incorrect
No, that’s wrong. Elongating the incisors often makes facial appearance worse rather than better by exposing too much of the teeth (and often the gingiva as well) beneath the lips, and changing the a-p position of anterior teeth does not reduce excessive face height. There is little effect on the nose and chin, however. Although open bite tends to correct itself in young children with normal jaw relationships, self-correction almost never occurs in adolescents. For the girl in this image, the upper teeth already are too far below the lip line for good facial esthetics. Elongating them further, with or without extraction, might close her open bite but would damage rather than improve facial esthetics. She is a candidate for surgery.
Question 9
To what extent does camouflage treatment correlate with the development of TMD?
- High positive correlation, increases the chance of TMD
- Low positive correlation, slightly increases the chance of TMD
- Little or no correlation ✓
- Low negative correlation, slightly decreases the chance of TMD
- High negative correlation, decreases the chance of TMD
Correct
That’s right, a number of studies have shown little or no correlation between camouflage treatment and the development of TMD.
The good news is that like most orthodontic treatment, camouflage doesn’t cause TMD. The bad news is that like most orthodontic treatment, camouflage also doesn’t cure TMD.
Incorrect
No, that’s wrong. A number of studies have shown little or no correlation between camouflage treatment and the development of TMD.
The good news is that like most orthodontic treatment, camouflage doesn’t cause TMD. The bad news is that like most orthodontic treatment, camouflage also doesn’t cure TMD.
Question 10
What’s the best advice from the family dentist to a 16-year-old who asks about the possibility of orthodontics to correct her protruding upper incisors?
- You need treatment to try to make your lower jaw grow—it’s not too late.
- At this point, you’ll need braces on all your teeth and will have to have some teeth removed.
- If you really want to look better, you’ll probably have to have an operation on your jaw.
- At this point, you need a complete diagnostic evaluation to decide what type of treatment would be best. ✓
Correct
That’s right, a complete diagnostic evaluation is needed, including photographs and cephalometric radiographs that can be put into a computer program to allow simulation of possible outcomes. At age 16, correcting the problem by modifying growth almost surely wouldn’t work, but there’s no way to know about camouflage versus surgery without further information. If it’s a borderline situation, having the patient and parents view computer simulations to help them make the decision is the modern approach.
Incorrect
No, that’s wrong. A complete diagnostic evaluation is needed, including photographs and cephalometric radiographs that can be put into a computer program to allow simulation of possible outcomes. At age 16, correcting the problem by modifying growth almost surely wouldn’t work, but there’s no way to know about camouflage versus surgery without further information. If it’s a borderline situation, having the patient and parents view computer simulations to help them make the decision is the modern approach.