Demand for Treatment / Motivation
Demand for Adult Treatment
Adult orthodontics was quite rare in the United States until the 1970s, then became the fastest growing area in orthodontics (image 1). By 1990, 25% of all patients receiving comprehensive treatment were age 19 or older.
Since then, the number of adult patients in the United States has remained relatively constant, but the proportion of adults has dropped to 20% because of growth in the number of children receiving treatment (image 2). For more than two decades now, adults with fixed braces on their teeth have been commonly observed at all levels of American society.
The same trend toward more adult orthodontics occurred somewhat later in Western Europe and Japan, where adult orthodontics now frequently is done. It is happening now in other countries as economic advances occur, for example, in the Eastern European countries formerly behind the Iron Curtain.
Having braces on their teeth is no longer a social problem for most adults. Increasingly, this is accepted as nothing special or even a sign of upward social mobility.
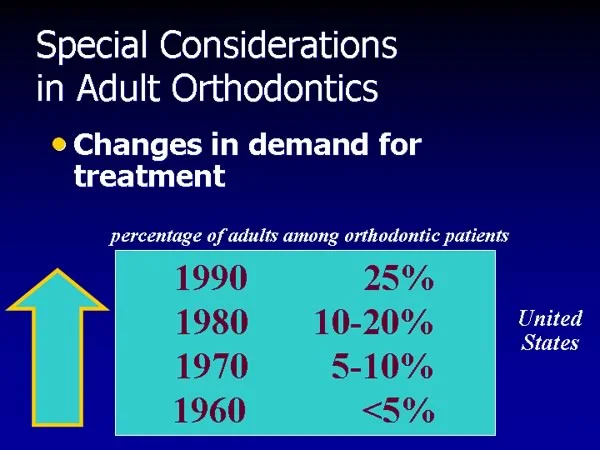 Image 1, 1990 demand Image 1, 1990 demand | 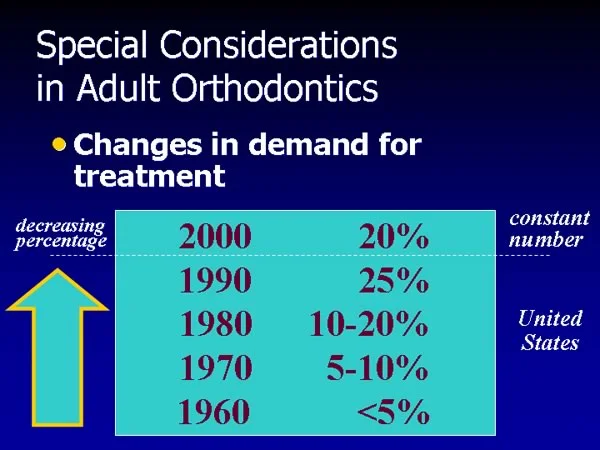 Image 2, current demand Image 2, current demand |
Motivation for Treatment: Improve Present Situation
Adult orthodontic patients can be placed into two groups: those whose motivation is to improve their present situation, and those whose goal is to keep what they have.
The first group often had wanted treatment as adolescents and didn’t get it for some reason. Their motivation almost always includes eliminating the social handicap created by their dental and facial appearance (image 1).
This motivation makes them candidates for comprehensive orthodontic treatment to obtain the best result possible (image 2). It often also makes them candidates for ceramic brackets, lingual orthodontics, or perhaps (if they’re particularly insecure socially) the transparent plastic aligners recently advertised on TV.
For the doctor, a danger with this group is that the real reason they are seeking treatment may be concealed—in other words, there may be a hidden agenda. If treatment does not produce what the patient wanted, he or she will be disappointed—and the doctor, who wasn’t directly told, may not have figured out the patient’s real goal. When esthetic improvement is sought, ascertaining what the patient really wants is an important part of the diagnostic evaluation. That’s true with all types of esthetic dentistry, not just orthodontics.
 Image 1, motivation Image 1, motivation |  Image 2, treatment desired Image 2, treatment desired |
Motivation for Treatment: Maintaining Present Situation
In contrast, the motivation for a second group of adults is not to improve their present situation, but to keep it from getting worse—their goal is to maintain what they have (image 1). The threat typically is loss of teeth and the facial soft tissue/dental appearance changes that accompany tooth loss and aging.
These adults tend to be older (usually age 35 and up, but sometimes younger). Their motivation makes them candidates for treatment involving multiple types of dentistry (image 2). Typically, treatment of periodontal problems and restoration of damaged/missing teeth is required, and the goal of orthodontic treatment is to facilitate the other treatment that the patient needs, not to comprehensively make occlusion and alignment as ideal as possible. The appearance of the orthodontic appliance often is only a minor concern.
Recent experience makes it clear that including orthodontics in the treatment plan for such patients can produce better results than otherwise would have been possible, and in the last decade this has been the fastest growing area in orthodontic treatment. The average age of adult orthodontic patients has increased.
 Image 1, motivation Image 1, motivation |  Image 2, treatment desired Image 2, treatment desired |
Periodontal Considerations
Periodontal Problems by Age
A third important area, which requires even greater emphasis in orthodontics for adults than it does in children, is the health of the periodontium. Several health-related considerations are important.
First (image 1), let’s review the prevalence of periodontitis/periodontal pockets and mucogingival problems (lack of adequate attached tissue) at various ages.
The graph in image 2 is derived from examination of 1000 patients with severe malocclusion who were evaluated through UNC’s Dentofacial Clinic for possible orthognathic surgery.
Note that the prevalence of periodontal pocketing, reflecting bone loss, doubles between age 20 and 26 and doubles again by age 33-39. The odds are that potential orthodontic patients who are over age 30 will have some evidence of periodontal disease. The severity of malocclusion is not a major factor in whether periodontal problems develop, so these prevalence numbers are reasonable estimates for adult orthodontic patients with less severe problems.
Note also that mucogingival problems, typically a lack of attached gingiva, are much more prevalent than pocketing in the 10-19 age group who are the more frequent candidates for orthodontics—but this peaks in the early 20s and actually declines thereafter.
The bottom line: It’s critically important to be sure that periodontal disease is under control before any orthodontics begins—and periodontal problems, though perhaps of different types, are likely to be present in both younger and older adults.
 Image 1, outline Image 1, outline | 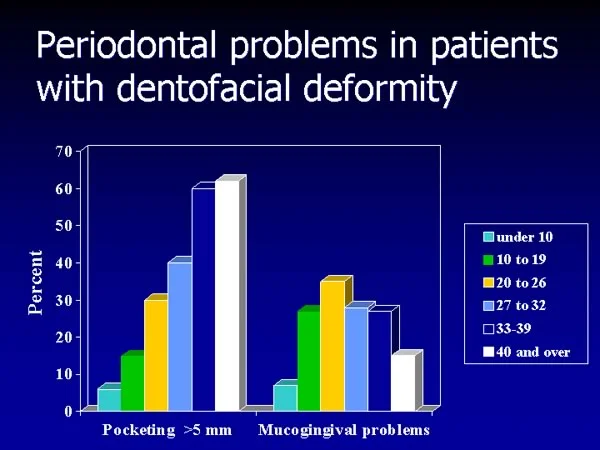 Image 2, prevalence graph: Periodontal pocketing and mucogingival problems in patients seeking treatment for severe malocclusion. Image 2, prevalence graph: Periodontal pocketing and mucogingival problems in patients seeking treatment for severe malocclusion. |
Detection of Periodontal Problems
A second important aspect of periodontal health in adults who are candidates for orthodontic treatment is the detection of periodontal problems (image 1).
The guideline for any sort of orthodontics is simple: Orthodontic treatment is quite feasible for patients who have had periodontal disease and bone loss—but tooth movement cannot begin until active disease is brought under control.
Of course the best indicator of active disease is bleeding on gentle probing (image 2).
It is equally important to remember that expansion of the dental arches stresses the gingival attachment and can lead to further loss of gingival tissue. The primary trouble area is the lower incisor region, where alignment of crowded incisors tends to move them facially (image 3). Arch expansion in other areas, however, also stresses the gingival attachment.
Tooth movement that stresses the attachment is risky in children who do not have good gingival attachment before treatment starts—and it’s even riskier in adults. Areas of reduced attachment must be evaluated carefully when tooth movement is planned.
Measuring the amount of attached tissue, and noting areas that already are at risk, are important steps in detecting potential mucogingival problems. Repositioning frenum attachments and/or placing a gingival graft before orthodontics begins may be needed.
 Image 1, outline Image 1, outline | 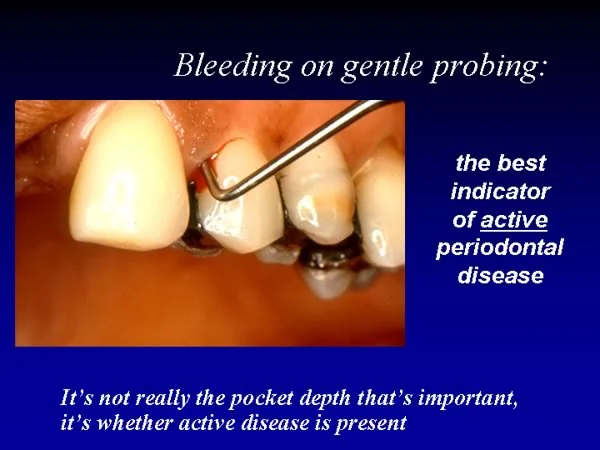 Image 2, active disease Image 2, active disease |
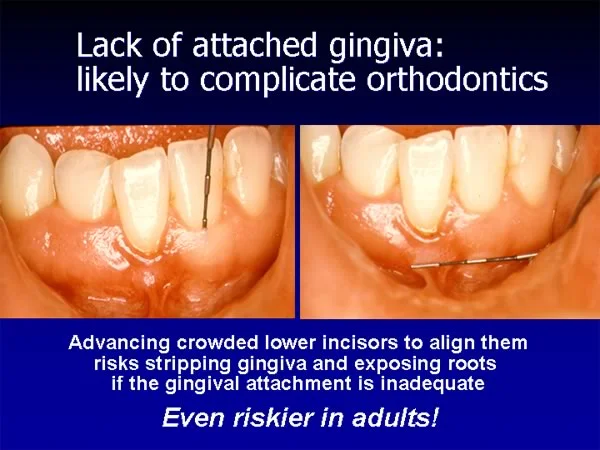 Image 3, mucogingival Image 3, mucogingival |
Orthodontics and Periodontal Health (cont.)
A third important periodontal consideration in adult orthodontics is the effect of bone loss on the amount of force for orthodontic tooth movement (image 1). If bone loss has occurred in an adult patient, both the amount of force and the magnitude of the moment to control root position must be adjusted.
By now you are quite familiar with the optimal force for various types of tooth movement, as shown in image 2. Remember that there is only one optimal pressure in the PDL. The amount of force for the various tooth movements varies because the force distribution in the PDL varies, hence the force variation keeps the pressure at the optimum.
But these forces are based on the assumption that the amount of periodontal ligament area is normal, i.e., that the amount of root supported by alveolar bone is normal.
 Image 1, outline Image 1, outline | 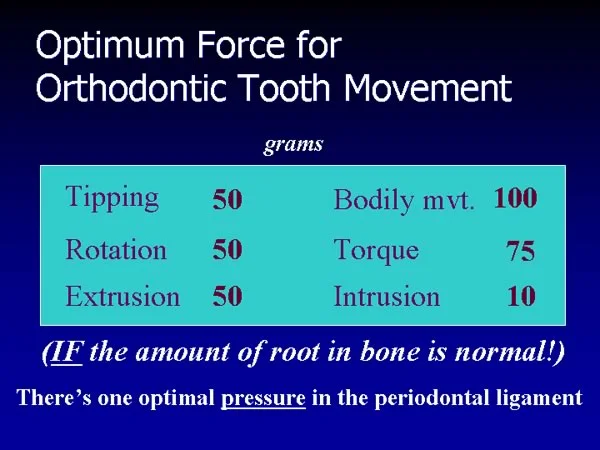 Image 2, orthodontic force Image 2, orthodontic force |
Effect of Bone Loss on Orthodontic Force (cont.)
Consider the force system to move a premolar bodily (image 1). For bodily movement, a force of 100 grams is appropriate. If this force is applied against the crown, however, the tooth will tip, because force against the crown is at a distance from the center of resistance, which is about the midpoint of the part of the root supported by bone. Typically, that distance is about 10 mm, so a 100-gm force against the crown creates a 1000 gm-mm moment (moment of the force, MF). To obtain bodily movement, a moment in the opposite direction with a magnitude of 1000 gm-mm must be created, by applying a couple on the bracket (moment of the couple, MC).
Now look at the situation when significant bone loss has occurred (image 2). If the bone level is halfway down the root, the area of the periodontal ligament over which the force will be expressed is half what it would be normally, so now 100 grams would produce twice the optimal pressure. Further, the center of resistance now would be 15 mm from the bracket, not 10, so the moment of the force would be 1500 gm-mm, and a 1000 gm-mm moment from the couple on the bracket would not be enough to prevent tipping.
For bodily movement of a premolar with loss of half the alveolar bone, the optimal force would be 50 gm, not 100 gm (image 3). Since the moment of this force would be 750 gm-mm (50 gm x 15 mm to the center of resistance), the moment of the couple on the bracket would have to be 750 gm-mm. The force was reduced by half, but the moment of the couple only decreased 25%.
You might have thought that since adults have harder heads, it would take more force to move their teeth. It’s just the opposite. Successful tooth movement in adults, especially those who have had bone loss, requires careful use of light forces and relatively larger moments to control root position.
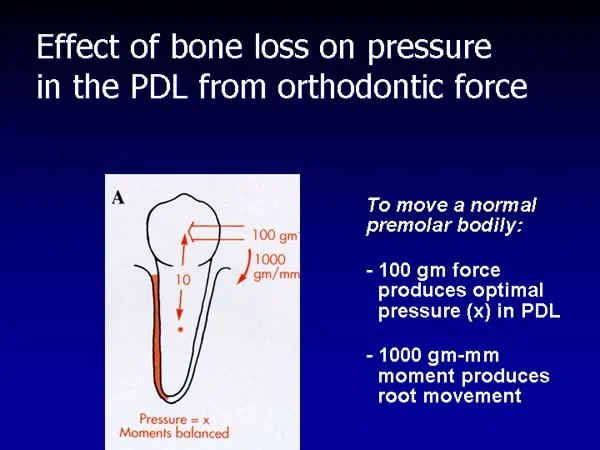 Image 1, normal Image 1, normal | 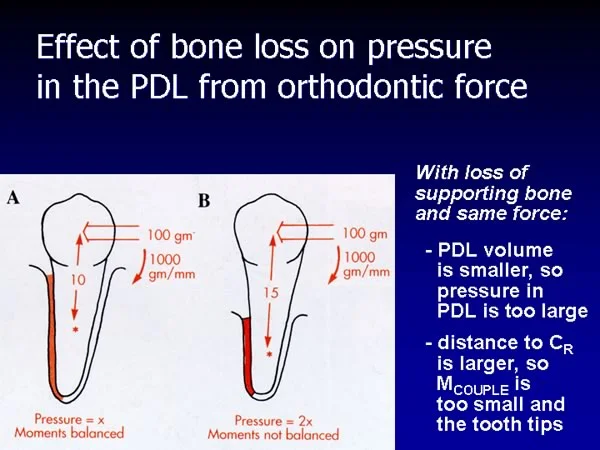 Image 2, bone loss Image 2, bone loss |
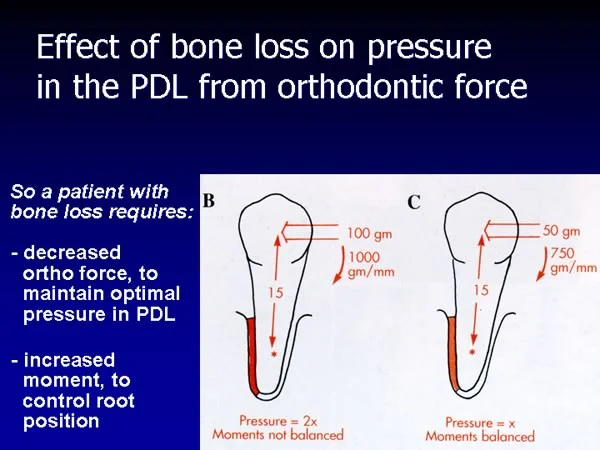 Image 3, corrected for bone loss Image 3, corrected for bone loss |
Patient Management
Patient Management
As people get older, lots of things aren’t as easy as they once were. Tolerating orthodontic treatment definitely falls into that category (image 1). If you’re the family dentist and one of your adult patients has orthodontic treatment, you’re very likely to hear about how difficult it was to get through the first couple of weeks.
Don’t tell adults, “Oh, there’s nothing to it really—you’ll do just fine.” Tell them there will be all kinds of things that are problems during those first 2 weeks, but fortunately after that it gets better. Expectations affect the reaction to most treatment. Often it’s not so much that things are good or bad that determines your reaction, it’s the extent to which the reality matches what you expected.
It’s important to provide medication for pain control (image 2). Adults have sore teeth initially to an extent that children don’t, and also are more likely to complain about mucosal lesions where some part of the appliance touches the lips or cheek.
Reminding patients to keep wax on any irritating part of the appliance until they get used to it, and giving them a small tube of a topical anesthetic, can prevent “emergency” appointments during those first 2 weeks.
Ibuprofen, on balance, probably is the best choice for pain control. The new COX-2 inhibitors have the potential advantage for adults that they reduce stomach irritation and require only one tablet per day, but their safety still is questionable for long-term use and at present their cost is considerably higher.
 Image 1, difficulties Image 1, difficulties |  Image 2, pain control Image 2, pain control |
Reassurance and Explanation
Finally, children and adolescents often are somewhat indifferent about their orthodontic treatment. That doesn’t happen with adults. They’re intensely interested, and the clinician has to be prepared for questions and discussion about how the treatment is going.
As one adult orthodontic patient put it, “You might as well go ahead and tell me all about it while you’re doing the treatment, because if you don’t I’m going to ask you before I leave.”
- What has happened since last time? How am I doing?
- What are you doing today? Why?
- What’s going to happen between now and next time?
- Will I have any special difficulty?
If you’re the family dentist and your patient now is seeing an orthodontist, be prepared. The patient is going to tell you all about it, ask if you think things are going well, and seek your opinion about whether the orthodontist will finish the treatment on time.
It’s just part of patient management—easier to handle if you expect it.
Case #1: Incisor Intrusion / Build-Ups
Case #1: Incisor Intrusion, Incisor Build-Ups
Now let’s consider three patients who illustrate specific areas of interest for adult orthodontics, beginning with a young adult who needs intrusion of maxillary incisors and build-ups for small incisors.
Steve’s chief complaint (image 1) was the appearance of his upper incisors. He said, “I try never to smile showing my front teeth.” After graduation from college, he was working as a research technician in the orthodontic department and became aware that this could be corrected.
Facial proportions generally were normal (images 2 and 3), but note that there is a mild mandibular asymmetry, with the chin off to the left. This isn’t a problem, but it is something that should be observed. It explains why the dental midline also is slightly off in the same direction.
 Image 1, smile: Steve, age 22, prior to treatment. Image 1, smile: Steve, age 22, prior to treatment. | 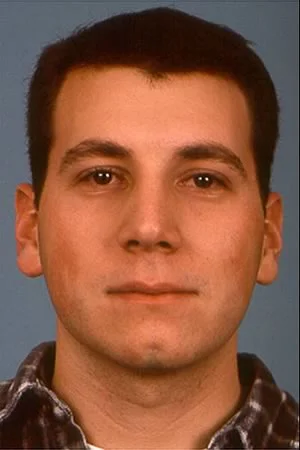 Image 2, frontal: Steve, age 22, prior to treatment. Image 2, frontal: Steve, age 22, prior to treatment. |
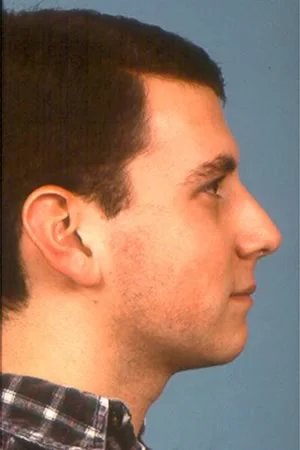 Image 3, profile: Steve, age 22, prior to treatment. Image 3, profile: Steve, age 22, prior to treatment. |
Case #1: Initial Records
In the frontal view of the dentition (image 1), note the elongation of the maxillary central incisors, deep overbite, and incisor spacing.
The molar relationship is normal (Class I), but the maxillary incisors are very upright, almost in a Class II, division 2 pattern (images 2 and 3).
The upper and lower teeth are well aligned (images 4 and 5), but spacing around the small maxillary incisors is apparent. Tooth size analysis confirmed that both the maxillary central and lateral incisors were small relative to the other teeth.
 Image 1, frontal view: Steve, age 22, prior to treatment. Image 1, frontal view: Steve, age 22, prior to treatment. |  Image 2, right lateral: Steve, age 22, prior to treatment. Image 2, right lateral: Steve, age 22, prior to treatment. |
 Image 3, left lateral: Steve, age 22, prior to treatment. Image 3, left lateral: Steve, age 22, prior to treatment. |  Image 4, maxillary occlusal: Steve, age 22, prior to treatment. Image 4, maxillary occlusal: Steve, age 22, prior to treatment. |
 Image 5, mandibular occlusal: Steve, age 22, prior to treatment. Image 5, mandibular occlusal: Steve, age 22, prior to treatment. |
Case #1: Initial Records
On the panoramic radiograph (image 1), it is apparent that the dentition is generally healthy, with no restorations and no evidence of alveolar bone loss.
Note the elongated maxillary left third molar. A tooth in this position can be the cause of a mandibular shift on closure. As a general rule, removal of third molars is indicated before comprehensive orthodontics for adults begins.
The cephalometric radiograph and tracing (images 2 and 3) confirm the upright/elongated position of the maxillary central incisors. The anteroposterior jaw relationships are normal, and lower face height is slightly decreased.
 Image 1, pan: Steve, age 22. Note the elongated maxillary 3rd molar. Image 1, pan: Steve, age 22. Note the elongated maxillary 3rd molar. |  Image 2, ceph: Normal jaw relationships, upright/elongated maxillary incisors. Image 2, ceph: Normal jaw relationships, upright/elongated maxillary incisors. |
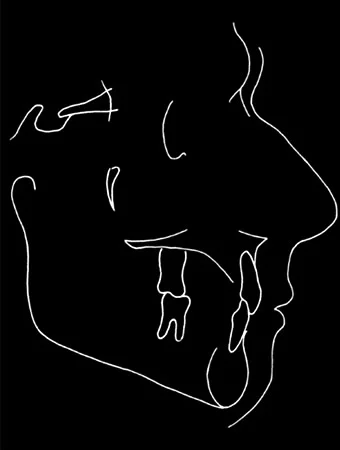 Image 3, tracing: Normal jaw relationships, upright/elongated maxillary incisors. Image 3, tracing: Normal jaw relationships, upright/elongated maxillary incisors. |
Case #1: Treatment Plan
The plan for Steve was to address his primary problem of elongated/spaced maxillary incisors and excessive overbite, using segmented arch mechanics to intrude the central incisors (this is the only way to obtain the very light force necessary for intrusion), then build-ups of the small incisors with composite resin to bring them to normal size and eliminate spacing.
The first step in treatment would be to remove the elongated maxillary left third molar. A tooth in this position creates a potential occlusal interference, and even if it is tolerated prior to treatment, it can become a problem during treatment.
When arch segments are created, and especially when intrusion of maxillary incisors is desired, a transpalatal lingual arch becomes an important stabilizing/anchorage part of the orthodontic appliance.
Because of the deep bite anteriorly, it would not be possible to place brackets on the lower incisors until the upper incisors had been repositioned, so treatment for the upper arch would have to start first.
Case #1: Incisor Intrusion
The first step in the orthodontic treatment was to align the teeth within segments. In this case, the two central incisors were one segment, and the molar-lateral incisor portions of the arch on either side were separate segments.
Intrusion of upper incisors requires a lingual arch. At the first appointment, mandibular and maxillary molar bands were fitted, and the upper molar bands were sent to the lab for fabrication of the lingual arch. These bands and the lingual arch were placed at the next appointment.
A continuous arch wire must not be used when the goal is intrusion. Such arch wires always are extrusive, not intrusive, because when steps are placed in the arch wire to change the vertical relationship of brackets, the force is far above the amount needed for intrusion. The relationship of the teeth changes, but the tooth movment is extrusion of the presumed anchor teeth, not intrusion of the ones where this was desired.
 Image 1, frontal view: First appointment, begin alignment within segments. Image 1, frontal view: First appointment, begin alignment within segments. |  Image 2, right lateral: First appointment, begin alignment within segments. Image 2, right lateral: First appointment, begin alignment within segments. |
 Image 3, right lateral: First appointment, begin alignment within segments. Image 3, right lateral: First appointment, begin alignment within segments. |
Case #1: Incisor Intrusion (cont.)
After initial alignment, an intrusion arch was used, first to deliver a precisely measured 20 grams (10 grams/tooth) to the maxillary central incisors. Intrusion requires light force to obtain the optimal pressure in the small PDL area around the apex of the tooth. If the force is too heavy, cells in the periapical area of the PDL become necrotic, recruitment of osteoclasts is slow, and the bone remodeling necessary for intrusion does not occur.
The intrusion arch fits into auxiliary rectangular tubes on the first molar bands and is tied to the wire segment in the incisor segment. The position of the intrusion arch in the anterior vestibule (images 1 and 2) is adjusted until bending it downward to the level of the teeth produces 20 gm force (images 3 and 4). A force gauge is used to measure the force created by deflecting the wire.
Intrusion of maxillary incisors requires the use of a transpalatal lingual arch to control the position of the upper molars (image 5).
Note that in this case, the intrusion arch is tied in the midline (image 3). The point of attachment of the intrusion arch to the segment wire can be varied, depending on what change in tooth position in addition to intrusion is desired.
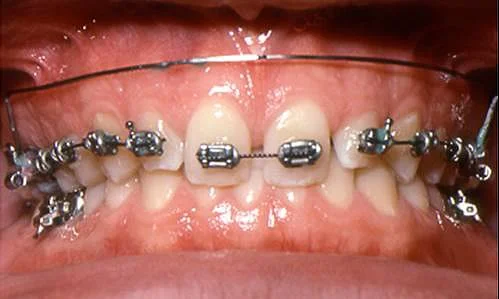 Image 1, frontal view: Intrusion arch prior to activation. Image 1, frontal view: Intrusion arch prior to activation. |  Image 2, frontal view, activated: Intrusion arch tied to incisor segment, to deliver 20 grams force. Image 2, frontal view, activated: Intrusion arch tied to incisor segment, to deliver 20 grams force. |
 Image 3, lateral view: Intrusion arch prior to activation. Image 3, lateral view: Intrusion arch prior to activation. |  Image 4, lateral view, intrusion arch activated: Intrusion arch tied to incisor segment, to deliver 20 grams force. Image 4, lateral view, intrusion arch activated: Intrusion arch tied to incisor segment, to deliver 20 grams force. |
 Image 5, occlusal view: Transpalatal lingual arch for stabilization, intrusion arch tied in midline. Image 5, occlusal view: Transpalatal lingual arch for stabilization, intrusion arch tied in midline. |
Case #1: Intrusion Progress
Two months later (image 1), the maxillary centrals had been intruded somewhat and tipped facially. Compare the pretreatment and progress vertical position of these teeth (image 2).
Tying an intrusion arch in the midline places the point of force application anterior to the center of resistance of the incisors, so they would tip facially as they intrude unless the intrusion arch were tied back against the molars to prevent this. In Steve’s case, facial movement of the incisors was desired, so the intrusion arch was left free to slip forward as the teeth responded to the force system.
This tooth movement allowed enough space to place brackets on the lower arch without occlusal interferences, and treatment for the lower arch began soon thereafter.
 Image 1, progress: Frontal view, prior to treatment. Image 1, progress: Frontal view, prior to treatment. |  Image 2, comparison: Pretreatment vs progress: note the vertical position of the maxillary central incisors. Image 2, comparison: Pretreatment vs progress: note the vertical position of the maxillary central incisors. |
Case #1: Extrusive Leveling, Lower Arch
Later in treatment, leveling of the lower arch was needed to complete correction of the deep overbite. Because a slight increase in face height was desired, this was done with a continuous arch wire and an auxiliary leveling arch that delivered 150 grams, so that the lower molars would be extruded.
An important concept: Intrusion of incisors requires the use of segmented arch wires and light force. Continuous arch wires and heavier force produce extrusion of posterior teeth, not intrusion of incisors.
Steve had intrusive mechanics in the upper arch, extrusive mechanics in the lower arch. The important differences:
- Arch wire segments tied into the brackets in the upper arch, continuous arch wire tied into the brackets in the lower arch
- Light (20 gm) force from the auxiliary wire in the upper arch, heavier (150 gm) force from the auxiliary wire in the lower arch
 Image 1, not activated: Auxiliary leveling arch, not activated. Image 1, not activated: Auxiliary leveling arch, not activated. |  Image 2, activated: Auxiliary leveling arch, activated by tying to main arch wire. Image 2, activated: Auxiliary leveling arch, activated by tying to main arch wire. |
Case #1: Maxillary Incisor Torque/Spacing
Then active torque was placed in a rectangular maxillary arch wire to bring the roots of the incisors to the lingual, and space was distributed around the upper incisors to allow build-up of these teeth to normal size (images 1-3).
Note that space between the maxillary incisors is being adjusted by coil springs that were slipped over the arch wire before it was inserted.
A cephalometric radiograph near the end of treatment (image 4) shows the change in incisor position, and the cephalometric superimposition (image 5) documents both intrusion and torque of the maxillary central incisors. The lower incisors were tipped facially slightly as the lower arch was leveled.
Now he is ready for the incisor build-ups, which must be coordinated with the completion of the orthodontic treatment.
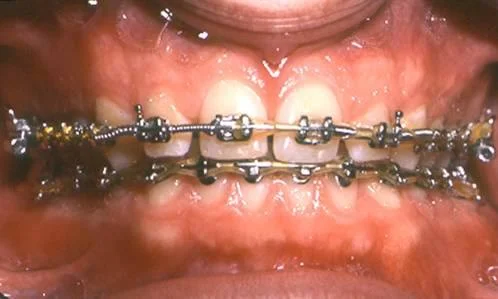 Image 1, frontal view: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. Image 1, frontal view: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. |  Image 2, right lateral: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. Image 2, right lateral: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. |
 Image 3, right lateral: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. Image 3, right lateral: Progress: rectangular arch wire for torque, coil springs to adjust incisor position. |  Image 4, ceph: Cephalometric radiograph near end of treatment. Image 4, ceph: Cephalometric radiograph near end of treatment. |
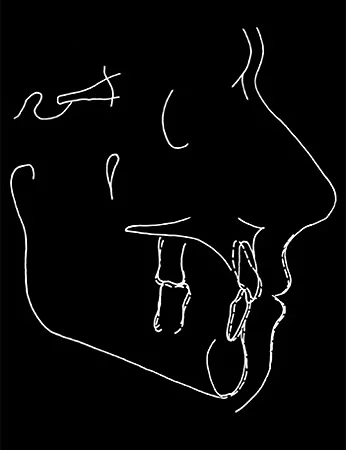 Image 5, superimp tracing: Cephalometric superimposition tracing—note the changes in incisor position. Image 5, superimp tracing: Cephalometric superimposition tracing—note the changes in incisor position. |
Case #1: Incisor Build-Ups
In order to allow the best restorative dentistry, the orthodontist provides slightly excessive space before incisor build-ups are done. The ideal sequence is:
- the brackets are removed from the upper incisors,
- the patient goes immediately to the restorative dentist, and
- the brackets are reapplied after the restorations are completed, so that the excess space can be closed with complete control of tooth positions.
A less satisfactory alternative is to position the teeth to be built up as precisely as possible as the orthodontic treatment is completed and provide a retainer until the restorations are completed. Any excess space then would have to be closed with a modified retainer—which is possible but more difficult and less precise.
Steve’s maxillary incisor brackets were removed early in the morning, the restorations were done the same morning (by Dr. Harald Heymann), and the brackets were replaced that afternoon so that closure of the remaining space could begin.
 Image 1, pre-buildup: 9 AM, just prior to removal of the arch wire and incisor brackets. Image 1, pre-buildup: 9 AM, just prior to removal of the arch wire and incisor brackets. |  Image 2, buildups completed: 1:30 PM same day, back to orthodontist after build-ups. Image 2, buildups completed: 1:30 PM same day, back to orthodontist after build-ups. |
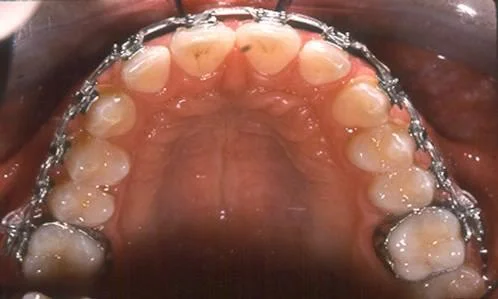 Image 3, continuation: 2 PM same day, brackets and arch wire replaced. Image 3, continuation: 2 PM same day, brackets and arch wire replaced. |
Case #1: Incisor Build-Ups (cont.)
Image 1 shows the appearance of the teeth at 1:30 PM, after completion of the restorations, just before the brackets and arch wire were replaced.
Note that as planned, there is still some space in the incisor segment. The last step in the orthodontics is final space closure and positioning of the teeth.
Image 2 shows the appearance of the teeth at 2 PM the same afternoon, with brackets reapplied, the arch wire replaced, and the appliance activated for closure of the residual space.
Close coordination of the restorative and orthodontic treatment at this stage is important for best results. Any delay between removal of the arch wire and brackets and the build-ups is an opportunity for uncontrolled shifting of the teeth, which can compromise the quality of the restorations. A delay in reapplying the orthodontic appliance is not as critical, but orthodontic finishing should proceed as rapidly as possible.
 Image 1, build-ups: After completion of build-ups, before the arch wire and brackets were replaced. Image 1, build-ups: After completion of build-ups, before the arch wire and brackets were replaced. | 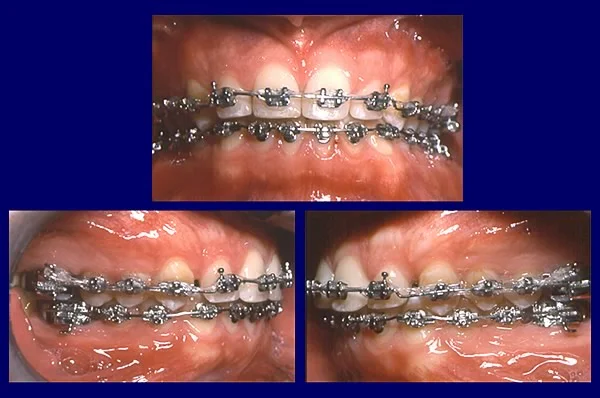 Image 2, treatment continuation: Same day, continuation of orthodontics. Image 2, treatment continuation: Same day, continuation of orthodontics. |
Case #1: Treatment Completed
Images 1-3 show the appearance of the dentition at the removal of the orthodontic appliance five months later. After completion of the incisor build-ups, the residual spaces were closed and the teeth were put into their final position.
When a space between maxillary central incisors has been closed, long-term retention usually is needed. Like most adults, Steve did not like wearing a removable retainer that covered the palate. Children tolerate these much better than adults.
A fixed retainer, contoured to allow easy flossing and with vertical stops to control overbite, was used instead (image 4). After correction of excessive overbite, the retainer must maintain the correct bite depth as well as alignment. It would be expected to remain in place at least for a time equal to the duration of active treatment.
 Image 1, post-tx frontal view: 5 months after build-ups, just after removal of the orthodontic appliance. Image 1, post-tx frontal view: 5 months after build-ups, just after removal of the orthodontic appliance. |  Image 2, right lateral: 5 months after build-ups, just after removal of the orthodontic appliance. Image 2, right lateral: 5 months after build-ups, just after removal of the orthodontic appliance. |
 Image 3, left lateral: 5 months after build-ups, just after removal of the orthodontic appliance. Image 3, left lateral: 5 months after build-ups, just after removal of the orthodontic appliance. | 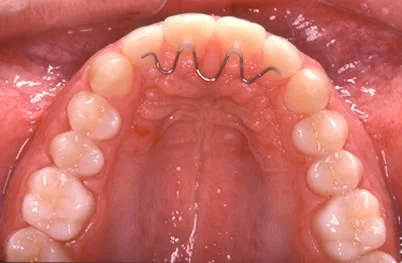 Image 4, fixed retainer: Bonded maxillary retainer. Image 4, fixed retainer: Bonded maxillary retainer. |
Case #1: Treatment Completed
Facial proportions were essentially unchanged during the nearly 2 years of treatment (image 1). The mild mandibular asymmetry was not corrected, because it was not a problem to the patient, and indeed is noticed only on careful examination.
A comparison of the smile appearance before and after treatment (image 2) shows the esthetic effect of this combination of orthodontic and restorative treatment.
Cephalometric radiographs before and after treatment (image 3) show the changes in incisor position and overbite that were obtained. Note that the roots of the maxillary incisors were torqued lingually, improving the inclination of these teeth.
The effect of this tooth movement on the position of the teeth can be seen in the comparison views of before and after treatment (images 4 and 5).
Total treatment time was just over 2 years.
 Image 1, post-tx face: Posttreatment facial proportions. Image 1, post-tx face: Posttreatment facial proportions. |  Image 2, smile comparison: Smile comparisons pre- to posttreatment. Image 2, smile comparison: Smile comparisons pre- to posttreatment. |
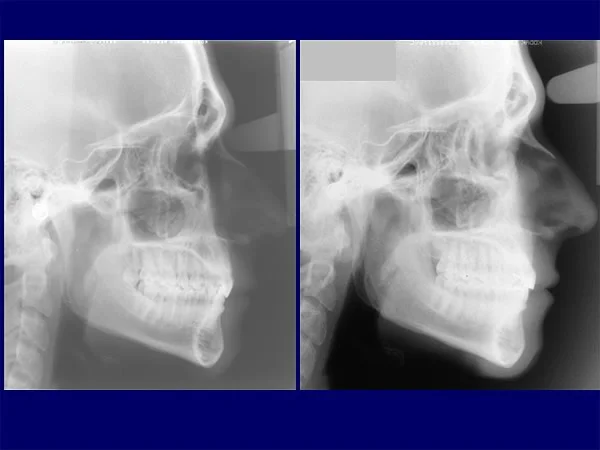 Image 3, cephalometrics: Pre- and posttreatment cephalometric radiographs. Image 3, cephalometrics: Pre- and posttreatment cephalometric radiographs. |  Image 4, frontal change: Pre- and posttreatment occlusion, frontal view. Image 4, frontal change: Pre- and posttreatment occlusion, frontal view. |
 Image 5, lateral change: Pre- and posttreatment occlusion, lateral view. Image 5, lateral change: Pre- and posttreatment occlusion, lateral view. |
Case #2: Severe Perio / Fiber Section
Case #2: Severe Perio/Fiber Section Surgery
Now let’s look at a second case, a young adult whose main reason for treatment was the control of severe periodontal problems and who had an adjunctive periodontal surgical procedure to facilitate orthodontic retention.
Nancy was only in her 20s when she developed severe periodontal disease. After treatment brought the disease under control, she was referred for orthodontics by her periodontist, who felt that maintaining control would be more likely if her severe crowding were corrected.
Nancy would not have sought orthodontic treatment otherwise, but said she would appreciate the dental esthetic improvement from aligning her upper incisors, which detracted from her smile (image 2). On profile examination, no disproportions were apparent (images 3, 4).
 Image 1, outline Image 1, outline |  Image 2, frontal view: Irregular maxillary incisors were apparent on smile. Image 2, frontal view: Irregular maxillary incisors were apparent on smile. |
 Image 3, profile: Normal jaw proportions are seen in the profile view. Image 3, profile: Normal jaw proportions are seen in the profile view. |  Image 4, combined: Esthetics: a consideration but not the main reason for treatment. Image 4, combined: Esthetics: a consideration but not the main reason for treatment. |
Case #2: Initial Records
Although her molar relationship was Class II bilaterally, Nancy had minimal overjet with severe crowding and rotation of the maxillary incisors. There was only moderate crowding in the lower arch.
The upper lateral incisors were very large, and the central incisors were each rotated 45 degrees. The severe crowding in the maxillary arch, therefore, had two causes: (1) the Class II molar relationship with minimal overjet, and (2) the tooth-size discrepancy created by the large lateral incisors.
 Image 1, frontal view: Nancy, age 27, prior to orthodontics. Image 1, frontal view: Nancy, age 27, prior to orthodontics. |  Image 2, right lateral: Nancy, age 27, prior to orthodontics. Image 2, right lateral: Nancy, age 27, prior to orthodontics. |
 Image 3, left lateral: Nancy, age 27, prior to orthodontics. Image 3, left lateral: Nancy, age 27, prior to orthodontics. |  Image 4, maxillary occlusal: Nancy, age 27, prior to orthodontics. Image 4, maxillary occlusal: Nancy, age 27, prior to orthodontics. |
 Image 5, mandibular occlusal: Nancy, age 27, prior to orthodontics. Image 5, mandibular occlusal: Nancy, age 27, prior to orthodontics. |
Case #2: Initial Records (cont.)
The intraoral radiographs (image 1) showed the extent of bone loss in multiple areas. Note particularly the extensive pocketing on the distal of the upper right 2nd premolar.
A major indication for a full series of periapical radiographs is the presence of widespread periodontal disease. For a patient like Nancy, a panoramic radiograph prior to orthodontic treatment is not sufficient. Detailed images of areas with potential disease are necessary.
The cephalometric radiograph and tracing (image 2) confirmed a dental but not a skeletal Class II malocclusion, i.e., the Class II molar relationship was due to a forward position of the upper molars.
For an adult patient, cephalometric analysis has two purposes: (1) to allow a more refined diagnosis (for example, in Nancy’s case, so that the cause of the Class II malocclusion could be described more precisely), and (2) to make it possible to use superimposition tracings to follow the course of treatment.
The second reason is the compelling one for cephalometric radiology in most orthodontic treatment. You often can make the diagnosis accurately enough for appropriate treatment planning without cephalometric analysis, but it is impossible to know exactly what is happening in treatment without serial radiographs that can be superimposed.
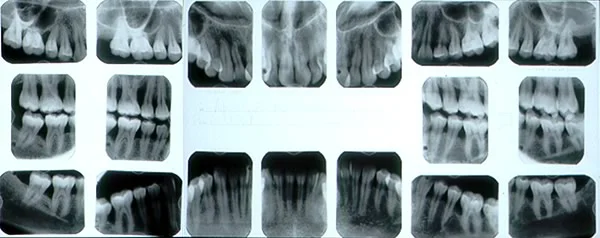 Image 1, intraoral radiographs: Nancy, age 27, intraoral radiographs. Image 1, intraoral radiographs: Nancy, age 27, intraoral radiographs. |  Image 2, ceph: Nancy, age 27, cephalometric radiograph. Image 2, ceph: Nancy, age 27, cephalometric radiograph. |
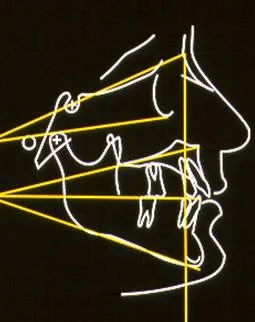 Image 3, ceph tracing: Nancy, age 27, dental but not skeletal Class II. Image 3, ceph tracing: Nancy, age 27, dental but not skeletal Class II. |
Case #2: Treatment Plan
The treatment plan for Nancy emphasized continued treatment to keep periodontal disease under control. A patient like this who has orthodontic treatment needs frequent recall for periodontal maintenance, perhaps as frequently as she sees the orthodontist, certainly at not more than 2-3-month intervals.
The plan was to extract the maxillary right 1st premolar and the maxillary left 2nd premolar, which was selected for extraction because of its poor periodontal prognosis (see the intraoral radiographs, previous screen) even though the orthodontic treatment would have been easier if both first premolars could have been removed.
Because of the limited posterior anchorage, a maxillary transpalatal arch to stabilize the position of the upper molars was planned, and the canines were to be retracted separately before the incisors were aligned, which would also reduce the strain on the posterior teeth.
Gingival surgery to section the gingival elastic fibers was planned because it would be critically important in maintaining the rotation correction for the maxillary central incisors. The fiber section procedure is most effective if it is done after the teeth are in their final position (i.e., rotations have been corrected) but before the orthodontic appliance is removed, so that the teeth can be held in position while healing occurs.
Case #2: Progress, 18 Months Treatment
After 18 months, the maxillary incisors had been aligned and the extraction spaces were closed. The improved alignment was apparent on smile (image 1). On the maxillary occlusal view, note that the transpalatal lingual arch has been removed after completion of closure of the extraction space. The large maxillary lateral incisors were reduced in width as much as feasible without going all the way through the proximal enamel (image 2), and the mild mandibular incisor crowding was corrected by slight expansion of the arch (image 3).
At this point (image 4), she was ready for the fiber section surgery, to release the tension in the gingival elastic fibers created by correcting the rotation of the incisors.
 Image 1, progress smile: Nancy, age 28, after incisor alignment and space closure in the upper arch. Image 1, progress smile: Nancy, age 28, after incisor alignment and space closure in the upper arch. |  Image 2, maxillary occlusal: Incisor alignment and space closure in the upper arch. Image 2, maxillary occlusal: Incisor alignment and space closure in the upper arch. |
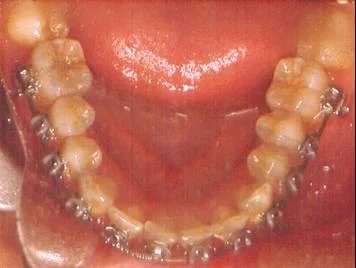 Image 3, mandibular occlusal: Nonextraction alignment of lower arch. Image 3, mandibular occlusal: Nonextraction alignment of lower arch. |  Image 4, frontal: Progress, ready for fiber section surgery. Image 4, frontal: Progress, ready for fiber section surgery. |
Case #2: Fiber Section Surgery
With the orthodontic appliance in place, the periodontist (Dr. Ray Williams) carried out the gingival surgery.
The first step was facial (image 1) and lingual (image 2) incisions within the gingival sulcus to section gingival fibers and allow repositioning of the frenum.
Then the gingival papillae were sectioned almost but not quite to the tip (image 3) and sutured into position (image 4), to minimize shrinkage of the papillae during healing.
Two weeks later, healing was essentially complete (image 5).
 Image 1, facial incisions: Facial incisions, for repositioning of the frenum. Image 1, facial incisions: Facial incisions, for repositioning of the frenum. |  Image 2, lingual incisions: Lingual incisions to base of gingival sulcus. Image 2, lingual incisions: Lingual incisions to base of gingival sulcus. |
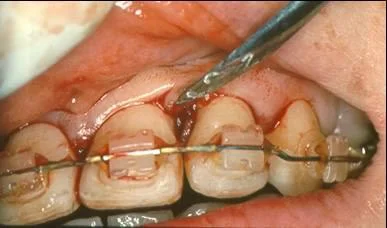 Image 3, papilla split: Incisions in gingival papillae to section gingival elastic fibers. Image 3, papilla split: Incisions in gingival papillae to section gingival elastic fibers. |  Image 4, papillae sutured: Papillae sutured after incisions. Image 4, papillae sutured: Papillae sutured after incisions. |
 Image 5, healing at 2 weeks: Healing at 2 weeks. Image 5, healing at 2 weeks: Healing at 2 weeks. |
Case #2: Completion of Treatment
Treatment was completed and orthodontic appliances were removed at 24 months. Periodontal control had been maintained successfully, and the fiber section procedure also succeeded in maintaining papilla height, which is important in esthetically sensitive areas like the maxillary incisor region. She liked the change in her dental and facial appearance (images 1, 2). The change in smile esthetics was particularly pleasing (image 3).
The maxillary premolar extraction spaces were closed largely by retraction of the canines, so that the Class II molar relationship was maintained and overjet did not develop (image 4). Note the improved contours and color of the gingiva, reflecting an improvement in periodontal health even though significant bone loss still is present.
At this point the teeth were well aligned in both arches, but retention would be important. In patients who have had bone loss, deep undercuts around the teeth make palate-covering retainers impractical. Like most adult patients, Nancy had thermoplastic suckdown retainers for both arches, made with undercuts waxed out. These were worn full-time initially, then on a decreasing part-time basis after the first 4 months.
 Image 1, post-tx frontal: Nancy, age 29, at completion of treatment. Image 1, post-tx frontal: Nancy, age 29, at completion of treatment. |  Image 2, post-tx profile: Nancy, age 29, at completion of treatment. Image 2, post-tx profile: Nancy, age 29, at completion of treatment. |
 Image 3, smile comparison: Smile before and after treatment. Image 3, smile comparison: Smile before and after treatment. |  Image 4, dental relationships: Dental relationships after treatment. Image 4, dental relationships: Dental relationships after treatment. |
Case #2: Completion of Treatment (cont.)
In the posttreatment panoramic radiograph (image 1), areas of bone loss related to the original periodontal disease can be seen, but there has been no progression during the orthodontic treatment, and some improvement can be observed especially in the maxillary right premolar area.
Comparison with the pretreatment radiographs (image 2) shows that extraction of the maxillary right 2nd premolar and closure of the extraction space eliminated one of the worst periodontal defects. Note the bone fill-in in the old 2nd premolar extraction site.
Fortunate results of this type can occur if the area of a periodontal defect is curetted regularly as the orthodontics proceeds, but cannot be expected routinely. On the other hand, with good periodontal maintenance, the periodontal condition should not become worse during even extensive orthodontic treatment.
 Image 1, post-tx pan: Posttreatment panoramic radiograph. Image 1, post-tx pan: Posttreatment panoramic radiograph. |  Image 2, x-ray comparison: Pre- and posttreatment radiographs showing improvement in 2nd premolar area. Image 2, x-ray comparison: Pre- and posttreatment radiographs showing improvement in 2nd premolar area. |
Case #2: Two-Year Recall
On 2-year recall, Nancy was wearing retainers only at night, and her periodontal condition was being maintained quite nicely. Her smile esthetics remained good (image 1).
The alignment and occlusion of the teeth were well maintained after 2 years (image 2). Although she admitted that her retainer wear had become sporadic after the first year, the severely rotated maxillary incisors were still well aligned.
Almost surely, that would not have been the case without the fiber section surgery. Sectioning stretched gingival fibers after rotated teeth have been corrected is critically important for long-term retention. Teeth that have been severely rotated, like Nancy’s upper central and lateral incisors, simply will not stay aligned without surgical release of the pull of gingival elastic fibers.
In this case, perio surgery was needed not only before orthodontics to help bring disease under control but also as an adjunct to successful orthodontics.
Given the severity of bone loss in several areas, Nancy will need to be followed carefully long term—but her periodontal prognosis is significantly better after the orthodontics.
 Image 1, 2 year facial: Nancy, age 31, 2-year recall. Image 1, 2 year facial: Nancy, age 31, 2-year recall. |  Image 2, 2 year dental: Nancy, age 31, 2-year recall. Image 2, 2 year dental: Nancy, age 31, 2-year recall. |
Case #3: Adjunctive Cosmetic Surgery
Case #3: Adjunctive Cosmetic Surgery
Now let’s look at a third adult patient, for whom adjunctive facial cosmetic surgery was an important part of the treatment plan.
Ronald (image 2) inquired at age 48 about the possibility of cosmetic bonding of his incisor teeth to improve their appearance. His motivation definitely was to improve his facial and dental appearance—and though it was not said in so many words, to improve his social image and interactions.
His mustache took attention away from what in novels often is described as a “weak chin.” He had poor throat form, with a quite obtuse lip-chin-throat angle (the ideal is near 90 degrees) and minimal throat length.
His chief concern was the appearance of his maxillary incisors (image 3). The left lateral incisor was congenitally missing, and the midline was shifted severely to that side.
Despite the missing maxillary lateral incisor, the maxillary incisors were crowded and malaligned. There was severe crowding in the mandibular arch, with a malformed mandibular right second molar (image 4).
 Image 1, outline Image 1, outline | 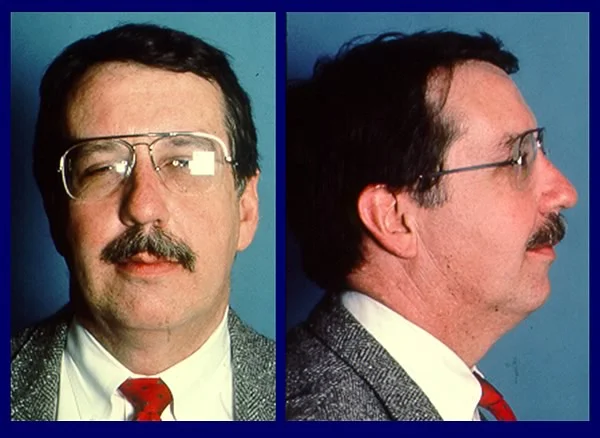 Image 2, pre-tx face: Ronald, age 48, prior to treatment. Image 2, pre-tx face: Ronald, age 48, prior to treatment. |
 Image 3, front teeth: Maxillary incisor crowding, left lateral incisor missing, midline off. Image 3, front teeth: Maxillary incisor crowding, left lateral incisor missing, midline off. | 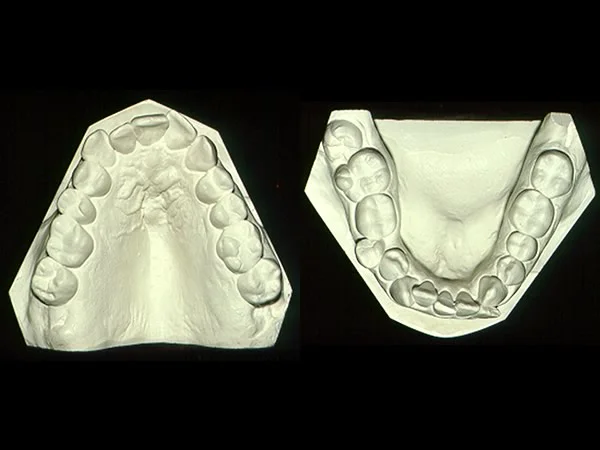 Image 4, occlusal views: Moderate maxillary, severe mandibular crowding. Image 4, occlusal views: Moderate maxillary, severe mandibular crowding. |
Case #3: Initial Records
His periodontal condition generally was good, except for bone loss and pocketing on the distal of the mandibular right second molar, where a partially impacted third molar still was present (image 1).
Current research has shown that the chance of periodontal breakdown adjacent to a third molar in this position is quite high. A partially erupted mandibular third molar is a greater risk for long-term problems than a completely impacted one.
Multiple restorations were present, and the mandibular left second premolar had a root canal filling. An endo-treated tooth can be moved, but its poorer long-term prognosis must be considered in treatment planning.
Cephalometric analysis (image 2) showed a skeletal Class II jaw relationship, with chin deficiency and somewhat increased face height. The relationship of the upper incisors to the maxilla is reasonably normal; the lower incisors are severely protrusive relative to the deficient chin. For this reason, overjet was normal.
The rotation of the palatal plane (which should be tipped in the other direction, intermediate between the occlusal plane below and true horizontal line above) indicates a skeletal open bite tendency.
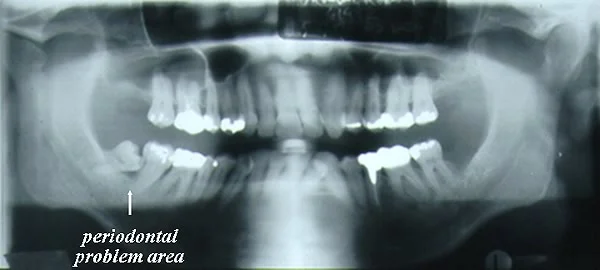 Image 1, panoramic radiograph: Note the periodontal problem area distal to the mandibular right second molar. Image 1, panoramic radiograph: Note the periodontal problem area distal to the mandibular right second molar. | 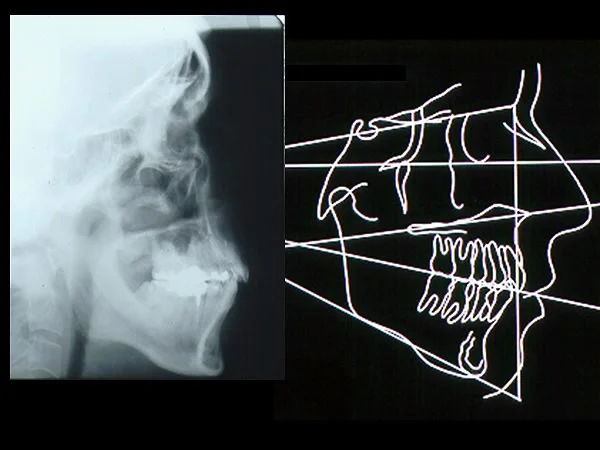 Image 2, ceph/tracing: Chin deficiency, prominent lower incisors, rotated palatal plane. Image 2, ceph/tracing: Chin deficiency, prominent lower incisors, rotated palatal plane. |
Case #3: Treatment Plan
Aligning the maxillary incisors and correcting the midline would require space to bring the central incisors around to the right, and extracting the right lateral incisor would allow the greatest improvement in the midline. The major esthetic problem with using canines to replace missing lateral incisors is their greater crown height, but Ronald’s low lip line meant that the gingival margins were not visible even on smile, and the cusp tips could be reshaped. The decision, therefore, was to extract the right maxillary lateral incisor and substitute the canines for the laterals.
The goal in the lower arch was to align the teeth without retracting the lower incisors, which would create excessive overjet, so extraction of mandibular second premolars was chosen. Extraction of the remaining third molar was an important aspect of bringing periodontal disease under control.
Because of the deficient chin and poor throat form, a lower border osteotomy of the mandible to bring the chin forward (a type of genioplasty) was suggested. He agreed to consider this as the orthodontic treatment came to a close.
Case #3: Progress
After 16 months of orthodontic treatment, the teeth were aligned. In the maxillary arch, there was still a small amount of space to bring the maxillary central incisors around to the right to improve the midline discrepancy, and the mandibular second premolar extraction sites were not quite closed. The cusp tips of the maxillary canines had not yet been flattened to make them look more like lateral incisors.
Ceramic brackets were used on the maxillary incisors to reduce the esthetic impact of the orthodontic appliance. Although these brackets are more esthetic, they make treatment more difficult, and their use is limited to highly visible teeth only.
 Image 1, frontal view: Age 49, 16 months progress, teeth aligned, space nearly closed. Image 1, frontal view: Age 49, 16 months progress, teeth aligned, space nearly closed. |  Image 2, right lateral: Age 49, 16 months progress, teeth aligned, space nearly closed. Image 2, right lateral: Age 49, 16 months progress, teeth aligned, space nearly closed. |
 Image 3, left lateral: Age 49, 16 months progress, teeth aligned, space nearly closed. Image 3, left lateral: Age 49, 16 months progress, teeth aligned, space nearly closed. |  Image 4, maxillary occlusal: Age 49, 16 months progress, teeth aligned, space nearly closed. Image 4, maxillary occlusal: Age 49, 16 months progress, teeth aligned, space nearly closed. |
 Image 5, mandibular occlusal: Age 49, 16 months progress, teeth aligned, space nearly closed. Image 5, mandibular occlusal: Age 49, 16 months progress, teeth aligned, space nearly closed. |
Case #3: Progress (cont.)
At that point, the issue of genioplasty was brought up again. His appearance on smile was significantly improved (image 1), but he was now aware that chin deficiency was a major part of his esthetic problem.
The cephalometric radiograph (image 2) clearly shows the protrusion of the lower incisors relative to the chin. Cephalometric superimposition (image 2, right) shows that the alignment in both arches was done with little change in incisor position—the incisors in both arches had been retracted very slightly. In this tracing, the pretreatment position is the solid line.
Ronald requested further information about surgical repositioning of his chin.
 Image 1, progress, face: Improved smile, obvious chin deficiency, and poor throat form on profile view. Image 1, progress, face: Improved smile, obvious chin deficiency, and poor throat form on profile view. | 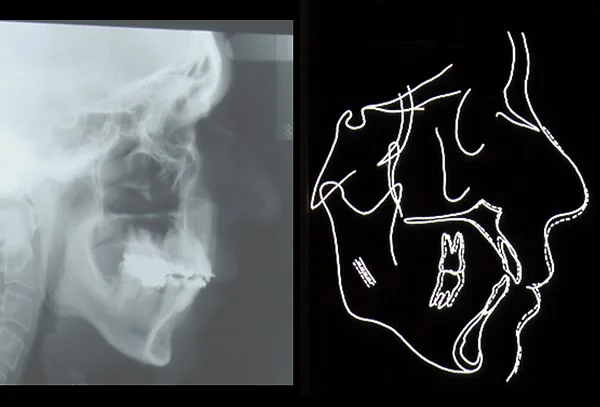 Image 2, ceph / tracing: Protrusive lower incisors, little change in incisor position during treatment. Image 2, ceph / tracing: Protrusive lower incisors, little change in incisor position during treatment. |
Case #3: Computer Image Prediction
It is possible now to use computer technology to show patients the probable outcome of a procedure like moving one of the jaws or the chin. The prediction is based on making the bony change on the cephalometric tracing and using algorithms that relate soft tissue to hard tissue change to create the predicted soft tissue image.
For Ronald, a cephalometric prediction tracing was prepared in a computer imaging software program (Dolphin Imaging) (image 1). Note that the chin has been moved forward. Then the prediction algorithms were used to produce the soft tissue profile change (image 2). At the chin, the soft tissue moves forward almost 1:1 with the hard tissue—note the corresponding amount of change in the bony and soft tissue chin created within the computer program. In the absence of growth, the predictions are quite accurate for chin position and reasonably accurate for lip changes.
Ronald was pleased with the orthodontic progress, and when he was shown the predicted effect of repositioning his chin (image 3), he liked it, so a lower border osteotomy to augment the chin was planned.
Research has shown that showing patients computer image predictions of this type greatly improves their ability to understand the esthetic implications of orthognathic surgery procedures. The research also shows that (if the predictions are realistic) there is little or no risk of raising expectations that cannot be met.
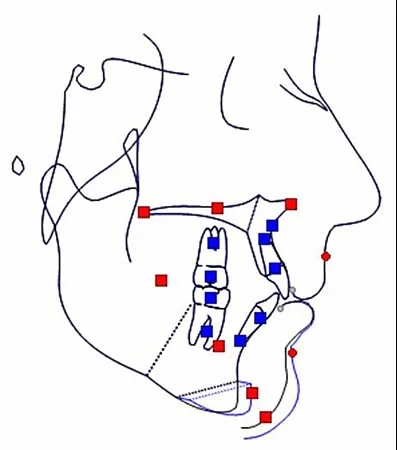 Image 1, ceph prediction: Cephalometric prediction of chin augmentation. Image 1, ceph prediction: Cephalometric prediction of chin augmentation. | 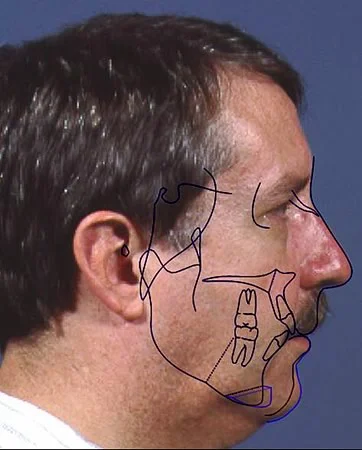 Image 2, profile prediction: Ceph / soft tissue profile predictions. Image 2, profile prediction: Ceph / soft tissue profile predictions. |
 Image 3, profiles compared: Present profile compared to prediction. Image 3, profiles compared: Present profile compared to prediction. |
Case #3: Lower Border Osteotomy
These radiographs show the cut in the lower border of the mandible that is used to slide the bony chin forward. This improves both the projection of the soft tissue chin and throat form. The angle of the cut controls the extent to which the chin also moves upward as it is advanced.
The surgery is done under general anesthesia, working intraorally from an incision in the depth of the mandibular vestibule. It does not require overnight hospitalization, and morbidity is equivalent to extracting premolars or molars bilaterally. If desired, submental fat can be removed at the same time to improve throat form—that was not done in this case.
In the superimposition tracing, note the change in the position of the bony chin and in the profile. With a lower border osteotomy to reposition the bony chin, the soft tissue chin is augmented quite predictably.
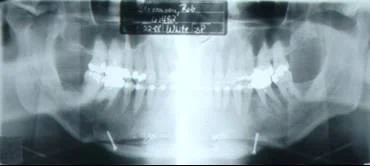 Image 1, post-surg pan: Age 49, after lower border osteotomy to augment chin. Image 1, post-surg pan: Age 49, after lower border osteotomy to augment chin. | 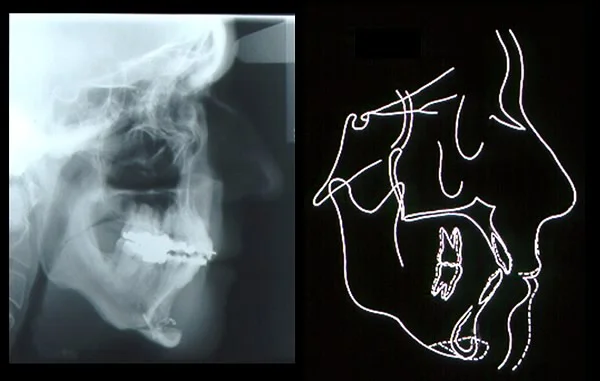 Image 2, ceph/tracing: Cephalometric radiograph and superimposition tracing after chin augmentation. Image 2, ceph/tracing: Cephalometric radiograph and superimposition tracing after chin augmentation. |
Case #3: Treatment Outcome
Treatment was completed and the orthodontic appliances were removed 5 months after the genioplasty, with a total treatment time of 19 months. With the canines in the lateral incisor positions, the midline was almost completely corrected (image 1). Because the lower incisors were not appreciably retracted, overjet remained nearly ideal (image 2).
Toward the end of the orthodontic treatment, the canines were recontoured to make them look more like lateral incisors. Note that the high gingival margin of the canines is noticeably different from what would be expected for lateral incisors—but Ronald does not show the gingival margins when he smiles, so only the morphology of the lower two-thirds of the crown is important in his smile esthetics.
 Image 1, frontal intraoral: Age 50, completion of treatment. Image 1, frontal intraoral: Age 50, completion of treatment. |  Image 2, profile intraoral: Age 50, completion of treatment. Image 2, profile intraoral: Age 50, completion of treatment. |
 Image 3, right lateral view: Age 50, completion of treatment. Image 3, right lateral view: Age 50, completion of treatment. |  Image 4, left lateral view: Age 50, completion of treatment. Image 4, left lateral view: Age 50, completion of treatment. |
 Image 5, composite views: Age 50, completion of treatment. Image 5, composite views: Age 50, completion of treatment. |
Case #3: Treatment Outcome (cont.)
These images show the facial change at age 49, from just prior to the genioplasty to 5 months later.
Because the gingival margins of the upper teeth are not seen on smile (image 1), even on a broad smile beyond what is pictured here, the canine substitution for the lateral incisors is esthetically acceptable, and the midline deviation has been corrected to the point that it is no longer immediately noticeable.
The three-quarter view (image 2) shows the increased chin projection and the tightening of skin contours created by moving the chin forward, which contributes to a younger look after the genioplasty.
On the profile view (image 3), greater chin prominence and improved throat form are apparent. Although dentists often do not consider the esthetics of the throat area, it is an important factor in overall facial esthetics.
The presurgery profile, computer prediction and actual outcome are shown in image 4. The presurgery profile is on the left, the computer image prediction in the center, and the actual profile on the right. Patients usually consider, as Ronald did, that the actual result looks better than the computer image prediction. He was pleased with the outcome in terms of both his dental and facial appearance.
Did the treatment affect his life adjustment? After treatment, he left his previous job and started his own English-language newspaper in a European city. It is reported to be quite successful.
 Image 1, frontal view: Frontal view before/after genioplasty. Image 1, frontal view: Frontal view before/after genioplasty. |  Image 2, oblique view: Oblique view before/after genioplasty. Image 2, oblique view: Oblique view before/after genioplasty. |
 Image 3, profile view: Profile view before/after genioplasty. Image 3, profile view: Profile view before/after genioplasty. |  Image 4, prediction / result: Prediction compared to actual result. Image 4, prediction / result: Prediction compared to actual result. |
Summary/Conclusions
Orthodontics for adults makes up about 20% of specialty practice now. The motivation for adults is different, and sometimes difficult to ascertain. There are two distinct groups of adult orthodontic patients:
1) Those who want to improve their situation
They are: younger; motivated primary by psychosocial considerations (want to get ahead in the world); candidates for comprehensive rather than adjunctive treatment; and interested in the appearance of the orthodontic appliance, so are candidates for clear brackets, lingual orthodontics, or Invisalign.
2) Those who want to keep what they have
They are: older; motivated primarily by concerns about their oral health and jaw function; candidates for adjunctive rather than comprehensive treatment; and not particularly concerned about the appearance of the appliance (bonded metal brackets are just fine).
Periodontal considerations always are important:
- Pocketing/mucogingival problems are likely to be present
- Bone loss affects orthodontic forces/moments
Patient management can be more difficult:
- Adults don’t adapt as well to orthodontic treatment
- Pain control requires medication, with Vioxx 50 mg a good choice
- Explanation and reassurance take additional time
But orthodontics for adults can be a highly gratifying part of all types of dental practice. It brings dentists in family practice and specialty practice into treatment teams, in a way that is stimulating to the practitioners and beneficial to the patients. Better dentistry is the result.
Self-Test Referral
The self-test section of this program is designed to help you be sure you have understood the material. Take it now, and use it as a guide for further study and review.
Copyright 2003, UNC Dept. of Orthodontics
Self-Test
Question 1
What is the percentage of adults in the orthodontic patient pool in the United States at present?
- 5%
- 10%
- 15%
- 20% ✓
- 25%
Correct
That’s right, as of 2000 about 20% of all orthodontic patients were adults. The percentage was down from the 25% of 1995, but the absolute number of adults seeking treatment has remained at the 1995 level, so it’s still a significant proportion of the total orthodontic treatment pool.
Incorrect
No, that’s wrong. As of 2000 about 20% of all orthodontic patients were adults. The percentage was down from the 25% of 1995, but the absolute number of adults seeking treatment has remained at the 1995 level, so it’s still a significant proportion of the total orthodontic treatment pool.
Question 2
Which of the following are characteristics of the group of adults who seek treatment to improve their present situation?
a. Younger, usually between 20 and 40
b. Want comprehensive treatment
c. Motivation usually is psychosocial
d. Often concerned about visibility of braces
- a and b
- b and c
- a, b, and c
- b, c, and d
- all of the above ✓
Correct
That’s right, all these are characteristics of the group of adults who seek treatment to improve their present situation. They tend to be younger, want comprehensive treatment, have a primarily psychosocial motivation, and often are willing to pay extra for braces that are less visible, such as ceramic brackets, lingual brackets, or the clear plastic aligners advertised as “invisible braces.”
Incorrect
No, that’s wrong. all these are characteristics of the group of adults who seek treatment to improve their present situation. They tend to be younger, want comprehensive treatment, have a primarily psychosocial motivation, and often are willing to pay extra for braces that are less visible, such as ceramic brackets, lingual brackets, or the clear plastic aligners advertised as “invisible braces.”
Question 3
Which of the following are characteristics of the group of adults who seek treatment to maintain their teeth and their dental health?
a. Older, usually over 30
b. Want treatment for specific problems
c. Motivation usually is psychosocial
d. Often concerned about visibility of braces
- a and b ✓
- b and c
- a, b, and c
- b, c, and d
- all of the above
Correct
That’s right, the first two statements describe the patients whose goal is to maintain their dentition, but the last two do not. These patients tend to be older and want treatment for specific problems that require a multidisciplinary dental approach rather than comprehensive orthodontic treatment. They are motivated by health concerns more than psychosocial ones and usually are not concerned about the visibility of orthodontic appliances once they decide they need treatment.
Incorrect
No, that’s wrong. The first two statements describe the patients whose goal is to maintain their dentition, but the last two do not. These patients tend to be older and want treatment for specific problems that require a multidisciplinary dental approach rather than comprehensive orthodontic treatment. They are motivated by health concerns more than psychosocial ones and usually are not concerned about the visibility of orthodontic appliances once they decide they need treatment.
Question 4
Which of the following statements accurately describe the prevalence of perio problems in patients with severe malocclusion?
a. Periodontal pocketing is more prevalent than mucogingival problems at all ages.
b. The prevalence of mucogingival problems peaks at about age 40, then declines.
c. By age 25, the majority of patients with severe malocclusion have evidence of mucogingival problems.
d. For patients with severe malocclusion, the prevalence of periodontal pocketing doubles between the early 30s and the early 40s.
- none of the above ✓
- a and b
- a, b, and c
- b, c, and d
- all of the above
Correct
That’s right, for patients seen in the dentofacial clinic where those with very severe malocclusion are evaluated, none of these statements are correct. The data show that mucogingival problems are more prevalent than pocketing below age 25. The prevalence of mucogingival problems peaks in the early 20s, not at age 40, and declines in the late 20s. At age 25, about one-third of dentofacial patients have evidence of mucogingival problems, but it never becomes a majority. The prevalence of pocketing is about the same (nearly two-thirds of the patients) in the age 33-39 and over 40 age groups—the rapid increase in perio problems is over by the mid-30s.
Incorrect
No, that’s wrong. For patients seen in the dentofacial clinic where those with very severe malocclusion are evaluated, none of these statements are correct. The data show that mucogingival problems are more prevalent than pocketing below age 25. The prevalence of mucogingival problems peaks in the early 20s, not at age 40, and declines in the late 20s. At age 25, about one-third of dentofacial patients have evidence of mucogingival problems, but it never becomes a majority. The prevalence of pocketing is about the same (nearly two-thirds of the patients) in the age 33-39 and over 40 age groups—the rapid increase in perio problems is over by the mid-30s.
Question 5
(A) Stripping of gingival tissues away from the facial surface of incisors is a particular risk when nonextraction orthodontic treatment is performed because (B) Expansion of the arches to obtain space moves the teeth facially and stresses the gingival attachment.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false
Correct
That’s correct, these statements are true and related. When the arches are expanded in nonextraction treatment, the teeth have to be moved facially. Then stripping of the gingival tissues is a risk, even more in adults than in children. This is a major limitation of how much the dental arches can be expanded to bring teeth into alignment.
Incorrect
No, that’s wrong. These statements are true and related. When the arches are expanded in nonextraction treatment, the teeth have to be moved facially. Then stripping of the gingival tissues is a risk, even more in adults than in children. This is a major limitation of how much the dental arches can be expanded to bring teeth into alignment.
Question 6
What is optimal force for tipping a tooth to a new position when half the alveolar bone support has been lost?
- 10 grams
- 25 grams ✓
- 50 grams
- 75 grams
- 100 grams
Correct
That’s right, when half the alveolar bone has been lost, half the periodontal ligament area over which force would be distributed has also been lost, so the optimal force would be half the amount for tipping with normal bone support (50 grams), or 25 grams.
Incorrect
No, that’s wrong. When half the alveolar bone has been lost, half the periodontal ligament area over which force would be distributed has also been lost, so the optimal force would be half the amount for tipping with normal bone support (50 grams), or 25 grams.
Question 7
For a premolar to be moved bodily after half the alveolar bone support had been lost, how would the ratio between the force to move the tooth and the moment to control root position be affected?
- No effect on this ratio
- Increased force relative to the moment
- Increased moment relative to the force ✓
- Necessary to double the moment, otherwise the tooth would tip
- Effect unpredictable, would depend on the shape of the root
Correct
That’s correct. The force would need to be reduced from what would be used with normal bone support, but because bone loss increase the distance from the point of force application to the center of resistance of the root, the moment would have to be increased relative to the force.
Incorrect
No, that’s wrong. The force would need to be reduced from what would be used with normal bone support, but because bone loss increase the distance from the point of force application to the center of resistance of the root, the moment would have to be increased relative to the force.
Question 8
(A) Adults tend to tolerate the irritations of orthodontic treatment better than children because (B) Almost all adults have a higher pain tolerance.
- A true, B true, A and B related
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false ✓
Correct
That’s right, both of these statements are false. As a rule, adults don’t tolerate the irritations of orthodontic treatment as well as children, and it’s not true that older patients necessarily have a higher tolerance for orthodontic pain. One of the modern pain-relieving agents is needed routinely for adults at the beginning of treatment, and the addition of a mild tranquilizer can help some of the more severely affected adults—something that’s almost never needed with children.
Incorrect
That’s wrong. Both of these statements are false. Adults don’t tolerate the irritations of orthodontic treatment as well as children, as a rule, and it’s not true that older patients necessarily have a higher tolerance for orthodontic pain. One of the modern pain-relieving agents is needed routinely for adults at the beginning of treatment, and the addition of a mild tranquilizer can help some of the more severely affected adults—something that’s almost never needed with children.
Question 9
What amount of force would be required to intrude a pair of elongated maxillary central incisors?
- 10 grams
- 20 grams ✓
- 50 grams
- 75 grams
- 100 grams
Correct
That’s right, the correct force for intrusion of a single tooth would be 10 grams, so for two central incisors 20 grams would be needed. The only way to obtain the precisely calibrated force necessary for this type of tooth movement is to use an auxiliary spring to deliver the force just to those two teeth. A continuous arch wire must not be used.
Incorrect
No, that’s wrong. The correct force for intrusion of a single tooth would be 10 grams, so for two central incisors 20 grams would be needed. The only way to obtain the precisely calibrated force necessary for this type of tooth movement is to use an auxiliary spring to deliver the force just to those two teeth. A continuous arch wire must not be used.
Question 10
Why should an elongated maxillary third molar be extracted before orthodontic treatment begins?
- Probable periodontal disease around such a tooth
- Periodontal breakdown likely to develop during orthodontics
- Occlusal interference from its position likely to complicate treatment ✓
- No reason to extract it if it’s healthy
Correct
That’s right, an elongated maxillary third molar, even if healthy, is likely to cause occlusal interferences as tooth movement proceeds. That would be the major reason for removing it, especially in the maxillary arch where retained third molars are less likely to lead to periodontal problems. But in the orthodontic treatment of adults, removal of upper and lower third molars before the orthodontics begins usually is needed to minimize the chance of problems of some type.
Incorrect
No, that’s not the best answer. An elongated third molar, even if healthy, is likely to cause occlusal interferences as tooth movement proceeds. That would be the major reason for removing it, especially in the maxillary arch where retained third molars are less likely to lead to periodontal problems. But in the orthodontic treatment of adults, removal of upper and lower third molars before the orthodontics begins usually is needed to minimize the chance of problems of some type.
Question 11
Which of the following characteristics would be needed in a bracket/wire appliance to torque the roots of central incisors lingually?
a. Rectangular arch wire that nearly fills the bracket slots
b. Torsional force of 75 grams per tooth
c. Precious metal wire material
d. Ceramic, not metal, brackets
- a and b ✓
- b and c
- a, b, and c
- b, c, and d
- all of the above
Correct
That’s right, the first two statements describe a torquing arch wire, but precious metal is not necessary and is obsolete in modern usage, and metal rather than ceramic brackets would be preferred. Depending on the size of the bracket and therefore the dimensions of the wire to fill the bracket slot, a modern torquing wire would be either stainless steel or beta-titanium (nearly pure titanium). Ceramic brackets look better, but everything else about them is a disadvantage, not an advantage. That’s why metal brackets are preferred when torque is needed.
Incorrect
No, that’s wrong. The first two statements describe a torquing arch wire, but precious metal is not necessary and is obsolete in modern usage, and metal rather than ceramic brackets would be preferred. Depending on the size of the bracket and therefore the dimensions of the wire to fill the bracket slot, a modern torquing wire would be either stainless steel or beta-titanium (nearly pure titanium). Ceramic brackets look better, but everything else about them is a disadvantage. That’s why metal brackets are preferred when torque is needed.
Question 12
When restorative build-ups of incisors are needed in an adult patient to bring small teeth to normal size and allow proper alignment/occlusion, at what point in treatment should this be done?
- Before any orthodontics begins
- Immediately after initial alignment is obtained
- Near the end of orthodontics, with slightly excessive space provided ✓
- Immediately after the orthodontic treatment is completed
Correct
That’s right, the best integration of the orthodontic and restorative phases of treatment is obtained by doing the build-ups near the end of the orthodontic treatment, with the teeth close to their final position but with slightly excessive space provided for the convenience of the restorative dentist. This allows ideal contouring of the restorations, and then the residual space can be closed in the final months of the orthodontic treatment. The alternative is to wait until the orthodontics is completed, but it can be difficult to have just the right amount of space available in that circumstance.
Incorrect
No, that’s wrong. The best integration of the orthodontic and restorative phases of treatment is obtained by doing the build-ups near the end of the orthodontic treatment, with the teeth close to their final position but with slightly excessive space provided for the convenience of the restorative dentist. This allows ideal contouring of the restorations, and then the residual space can be closed in the final months of the orthodontic treatment. The alternative is to wait until the orthodontics is completed, but it can be difficult to have just the right amount of space available in that circumstance.
Question 13
For a patient with severe malocclusion and periodontal disease, at what point would orthodontic treatment be indicated?
- As soon as possible, to facilitate the perio treatment
- As soon as initial perio treatment is completed
- When active disease has been eliminated
- When perio control has been established and can be maintained ✓
- Not until at least one year after periodontal disease has been eliminated
Correct
That’s correct, orthodontics should not begin until perio control has been established and can be maintained. Control of the perio problems must be maintained throughout any orthodontic treatment. Beginning orthodontics before that time risks exacerbation of periodontal breakdown—but there is no need to wait for a year after control has been established.
Incorrect
No, that’s wrong. Orthodontics should not begin until perio control has been established and can be maintained. Control of the perio problems must be maintained throughout any orthodontic treatment. Beginning orthodontics before that time risks exacerbation of periodontal breakdown—but there is no need to wait for a year after control has been established.
Question 14
(A) Gingival surgery to section the elastic gingival fibers is important in maintaining the correction of severe rotations because (B) These fibers are the major cause of relapse after rotation correction.
- A true, B true, A and B related ✓
- A true, B true, A and B not related
- A true, B false
- A false, B true
- A and B false
Correct
That’s right, these statements are both true and related. Stretched elastic gingival fibers cause relapse after correction of rotations unless they are sectioned and allowed to heal with the tooth in the correct position, so this adjunctive perio surgical procedure is important when rotations have been corrected.
Incorrect
No, that’s incorrect. These statements are both true and related. Stretched elastic gingival fibers cause relapse after correction of rotations unless they are sectioned and allowed to heal with the tooth in the correct position, so this adjunctive perio surgical procedure is important when rotations have been corrected.
Question 15
What is the relation of exposure of gingiva on smile to the decision to use canines as replacements for missing lateral incisors?
- Exposure of gingiva on smile is acceptable, but not exposure with lips relaxed.
- Successful canine substitution requires reshaping the crown.
- Gingival surgery to change the contours often is needed for canine substitution.
- Canines look more like laterals if their greater crown height is not observed. ✓
- There is no relationship, shape of crown is the key.
Correct
That’s correct. Because of their greater crown height, it is very difficult to make canines look like laterals if the entire crown height is observed on smile. But if the lip line is low and only part of the crown is seen even on smile, that makes canine substitution more esthetic. Dental esthetics are particularly important on smile, and exposure during smiling, not at rest, is the important criterion.
Incorrect
No, that’s wrong. Because of their greater crown height, it is very difficult to make canines look like laterals if the entire crown height is observed on smile. But if the lip line is low and only part of the crown is seen even on smile, that makes canine substitution more esthetic. Dental esthetics are particularly important on smile, and exposure during smiling, not at rest, is the important criterion.
Question 16
Surgery to move the chin forward improves facial esthetics in which of the following ways?
a. Decreases the appearance of a weak chin
b. Improves throat form and throat length
c. Decreases the amount of wrinkles in the lower face
d. Makes the nose look less prominent in the face
- a and b
- b and c
- a, c, and d
- b, c, and d
- all of the above ✓
Correct
That’s right, moving the chin forward improves facial esthetics in all these ways. Not only does it make the chin itself more prominent, it improves throat form and throat length and stretches the skin in that area so that the amount of wrinkles in the lower face decreases. The nose always is viewed in relation to the chin, so making the chin more prominent decreases the relative prominence of the nose.
Incorrect
No, that’s incorrect. Moving the chin forward improves facial esthetics in all these ways. Not only does it make the chin itself more prominent, it improves throat form and throat length and stretches the skin in that area so that the amount of wrinkles in the lower face decreases. The nose always is viewed in relation to the chin, so making the chin more prominent decreases the relative prominence of the nose.