Retention: Why?
Overview of Retention
Why, even if you’re not treating complex orthodontic problems, do you need to know something about orthodontic retainers? Because you will be seeing patients in your family practice or specialty practice who are wearing them—or should be. When a retainer is lost or broken, often you’re the first dentist who is asked what to do next. And you will have to counsel patients about what would be required to get teeth back into alignment after relapse when a retainer was not replaced.
Did you have orthodontic treatment? If so you have already had some experience with retainers, so you can share personal experience, maybe even use yourself as an example. And if you didn’t have treatment yourself, you undoubtedly have had friends complaining to you about what happened with their retainers. So you already know at least a little about retention and retainers. The goals of this module are to
- Explain why retainers are necessary
- Describe the schedule and timing of retention
- Discuss the indications for and management of removable vs. fixed retainers
- Put retention in the perspective of interaction with orthodontists about patients that you have in common.
Why Are Retainers Necessary?
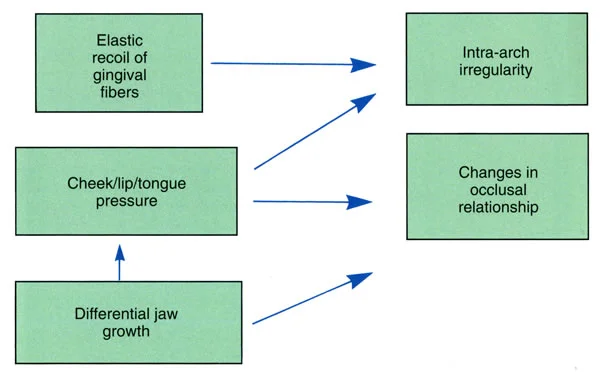
Retainers are necessary because orthodontic treatment outcomes are potentially unstable for three reasons:
- The periodontal and gingival tissues are affected by tooth movement, and even in the best case they require time for reorganization after an active orthodontic appliance is removed.
- Pressure by the tongue and lips / cheeks provides force against teeth that can result in tooth movement (the equilibrium effects that you have learned about previously).
- Growth after treatment is likely to lead to adaptive changes in tooth position—which means potential instability until growth is completed even in patients who had no skeletal problem.
Reorganization of PDL After Treatment
You will remember from Level III that widening of the periodontal ligament space and disruption of the collagen fiber bundles that connect the tooth to the adjacent bone is an essential part of tooth movement. Tooth mobility increases as the alveolar bone around them is remodeled. At the end of treatment, reattachment of the fibers to a new layer of bone is required.
Something you should remember but may have forgotten: the PDL plays an “active stabilization” role in equilibrium. Remember that soft tissue pressures against the teeth are not perfectly balanced (Image 1), and even very light but prolonged pressure can cause tooth movement. The PDL can compensate for an imbalance of a few grams but not more than that. An orthodontic appliance overcomes this stabilization—but until the PDL reorganizes after treatment, active stabilization doesn’t work, and the teeth are very sensitive to pressure imbalances that could be tolerated when reorganization is complete (Image 2).
An important concept: reorganization of the periodontal ligament does not begin until orthodontic archwires are removed and teeth can move relative to each other during function. Independent movement of teeth is impossible when they are splinted together, as they are during the finishing stage of treatment when stiff archwires are being used to obtain torque and precise positioning. So it simply isn’t true that if passive archwires were left in place for a few months after active tooth movement ended, PDL reorganization would be complete when they were finally removed.
Once displacement of a tooth relative to the one next to it can occur, i.e., once alveolar bone bending during function is back to normal, it takes 3-4 months for PDL reorganization to be completed. The slight mobility that is present when an orthodontic appliance is removed disappears over that period of time.
The bottom line: every orthodontic patient is going to need something to maintain tooth position for a few months while the PDL is undergoing reorganization (Image 3).
 Image 1 Image 1 |  Image 2 Image 2 |
 Image 3 Image 3 |
Reorganization of the Gingival Tissues
The soft tissues of the gingiva also are disturbed by orthodontic tooth movement, and remodeling of these tissues is needed as part of the adaptation to treatment. The gingiva contains both collagenous and elastic fibers, which reorganize more slowly than the PDL. At one year after alignment of the teeth the supracrestal elastic fibers still are stretched, particularly after a tooth has been rotated, and they exert enough force to cause immediate relapse.
In orthodontic treatment, the first step is to align the teeth, and after that they are held in alignment. Unlike the PDL, gingival remodeling does start while an orthodontic appliance is in place (Image 1), so it helps that typical treatment takes another year or so after alignment is completed. But if the teeth were severely crowded and malaligned, at least another year of retention is likely to be needed (Image 2).
Severely rotated teeth can be almost impossible to retain unless the stretched gingival elastic fibers are relaxed by fiberotomy. That is a relatively simple surgical procedure which should be done before the active appliance is removed. It makes all the difference in maintaining a rotated tooth in its new position (Images 3, 4).
 Image 1 Image 1 |  Image 2 Image 2 |
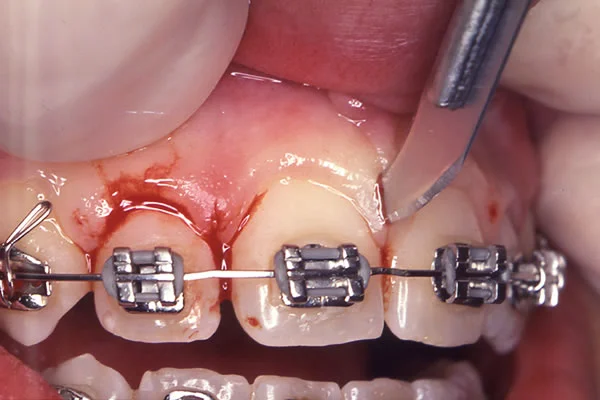 Image 3, Fiberotomy surgery: Sectioning stretched gingival elastic fibers to prevent re-rotation is needed after correction of severe rotation. It is particularly important for maxillary incisors, where relapse is obvious every time the lips are separated. For these teeth, the surgical technique should be modified to maintain papilla height. Image 3, Fiberotomy surgery: Sectioning stretched gingival elastic fibers to prevent re-rotation is needed after correction of severe rotation. It is particularly important for maxillary incisors, where relapse is obvious every time the lips are separated. For these teeth, the surgical technique should be modified to maintain papilla height. | 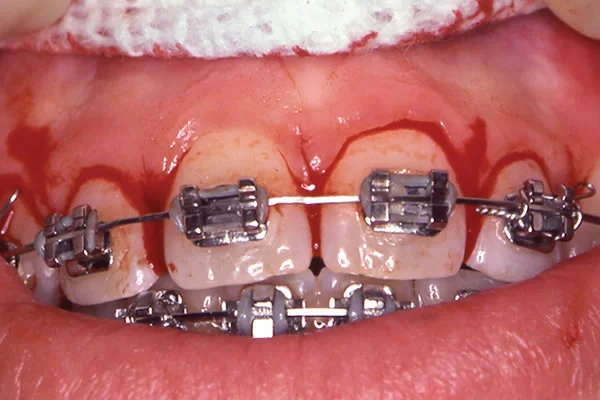 Image 4, Fiberotomy incisions before suturing: Note that the fiberotomy incisions do not go completely through the tip of the interdental papillae, to control loss of papilla height. Cuts on the lingual also are required. Image 4, Fiberotomy incisions before suturing: Note that the fiberotomy incisions do not go completely through the tip of the interdental papillae, to control loss of papilla height. Cuts on the lingual also are required. |
Wisdom Teeth?
From previous discussions of equilibrium, you already know that mandibular third molars are erupting, or attempting to erupt, at the same time in late adolescence that lower incisor crowding tends to develop even in patients who never had orthodontic treatment. And you already know that the culprit usually is some late mandibular growth that is not matched by maxillary growth.
You’re going to have to discuss third molars with all your adolescent and young adult patients. Should they be removed to prevent lower incisor crowding. No. Should they be removed for other reasons? For many of them, yes. Just be careful about blaming incisor crowding on third molars and using that as a reason for early extraction.
 Image 1 Image 1 |  Image 2 Image 2 |
Growth: Class II / Deep Bite Patients
For skeletal Class II and deep bite problems, comprehensive treatment is done during adolescence, for two reasons: the response to attempted growth modification is better then, and treatment often ends just as the adolescent growth spurt is coming to an end. The more a patient grows after the braces come off, the greater the chance that the original skeletal problem will reappear, as overjet develops and the deep bite returns (Image 1). That means that retention to maintain the jaw relationship and prevent eruption of lower incisors will be needed until growth subsides (Image 2).
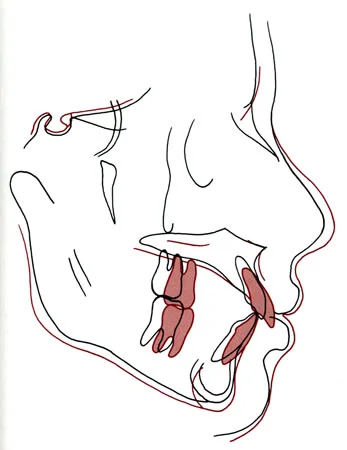 Image 1, Post-treatment growth, Class II patient: Cephalometric superimposition. Black, immediately after correction of a Class II problem, age 13; red, recall, age 17. Note the post-treatment growth of the mid-face and maxilla, with minimal growth of the mandible, which led to a return of relative mandibular deficiency, overjet and deep bite. Image 1, Post-treatment growth, Class II patient: Cephalometric superimposition. Black, immediately after correction of a Class II problem, age 13; red, recall, age 17. Note the post-treatment growth of the mid-face and maxilla, with minimal growth of the mandible, which led to a return of relative mandibular deficiency, overjet and deep bite. |  Image 2 Image 2 |
Growth: Class III Patients
Relapse due to late growth is even more of a problem for skeletal Class III and open bite problems. If a Class III patient has continued mandibular growth in late adolescence, as often occurs, not only will the lower incisors be tipped lingually at the expense of alignment, the increasingly prominent chin will become more of an esthetic problem (Images 1-4). As you already know, preadolescent treatment for Class III patients with maxillary deficiency is the modern recommendation, but if excessive mandibular growth occurs during adolescence, retention is very difficult, almost impossible, and orthognathic surgery at the end of the growth period may be required (image 5).
The same is true for severe anterior open bite, which is largely caused by vertical growth of the maxilla that is not matched by vertical growth of the mandibular ramus. Treatment during adolescence can lead to temporary correction of the open bite—and if further vertical growth of the maxilla occurs, as it often does, intraoral appliances can’t control it. So delaying treatment until growth is complete or nearly complete is the best plan.
 Image 1: Age 7, prior to treatment for developing Class III problem. Image 1: Age 7, prior to treatment for developing Class III problem. |  Image 2: Age 8, after facemask (reverse-pull headgear) treatment. Image 2: Age 8, after facemask (reverse-pull headgear) treatment. |
 Image 3: Age 13, after adolescent growth. Note the increased prominence of the chin. Image 3: Age 13, after adolescent growth. Note the increased prominence of the chin. | 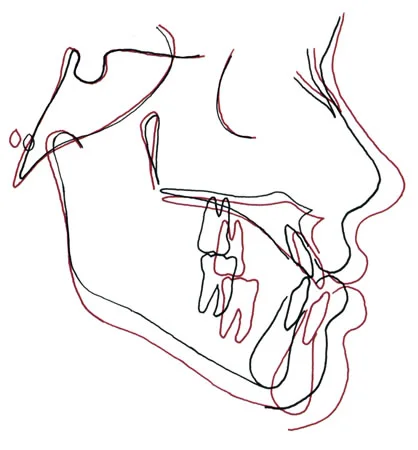 Image 4: Ceph superimposition ages 8 (black) and 13 (red). During that time the maxilla grew a little and the mandible grew a lot, and the Class III correction was lost. Image 4: Ceph superimposition ages 8 (black) and 13 (red). During that time the maxilla grew a little and the mandible grew a lot, and the Class III correction was lost. |
 Image 5: Age 19, after orthognathic surgery. Image 5: Age 19, after orthognathic surgery. |
Summary
Based on what you just read, you should now understand that all patients who have had significant orthodontic tooth movement require retention. In a sense, you’re now seeing clinical application of things that you learned about growth all the way back in Level I, and that you learned about soft tissues and equilibrium in Level III.
It has been said repeatedly by some clinicians that “My method corrects malocclusion so perfectly that no retainers are necessary”. The thought—the fantasy—is that perfect dental occlusion would generate the forces necessary to keep the teeth where treatment put them. You already know better than that, because you know that patients rarely bring their teeth into the occlusion except when clenching or grinding. For better or worse, occlusion is not a retainer.
Should all patients get the same set of retainers? That makes no sense when you take a broader view of retention. Clearly, retainers should be designed to control the type of relapse would be expected for that individual patient. The guideline is that teeth tend to move back toward their original relationships within the dental arch and original occlusal relationship.
Retention: When?
The Retention Schedule: Function as an Influence
Occlusion as seen on an articulator may not be a factor in retention, but occlusal function certainly is. We have described what it takes to obtain reorganization of the PDL: movement of the teeth relative to each other during chewing, and the bending of alveolar bone that accompanies mastication. Your teeth, of course, rarely come into occlusion when you’re eating.
What does that mean relative to retention? Should the patient be wearing a retainer all the time as soon as the braces are removed? The interesting, and perhaps surprising, answer is No.
Why not? Because the retainer would prevent the movement of teeth in function that is necessary for PDL reorganization. So during the first 3-4 months after treatment, removable retainers should be taken out to eat, and worn all the rest of the time. And if a fixed retainer is used, it must be made so that it is flexible enough to allow the desired tooth movement during function.
![]()
The Retention Schedule: Gingival Elastic Fibers
Gingival elastic fibers remodel slowly. How does that fit into the retention schedule?
For a typical patient who had crowded and malaligned teeth, even if the teeth were held in alignment for most of the orthodontic treatment time, the elastic fibers will still be at least somewhat active by the time PDL reorganization is complete. Fortunately, part-time retainer wear is adequate to control this, but wearing the retainer 10-12 hours per day for the rest of the first post-treatment year is needed. Does it make any difference which hours it is worn? Fortunately, evening and night hours (when patients are more likely to be compliant) are as good, perhaps even better, than daytime hours.
![]()
The Retention Schedule: Tongue vs. Lip / Cheek Pressures
What about tongue pressure versus lip and cheek pressures against the teeth? We have already talked about active stabilization by the PDL after its reorganization is complete—but remember that the PDL’s capacity to stabilize is limited to overcoming a few grams of pressure.
What does that mean for retention? Simply that if the teeth have been put in a position where the soft tissue pressures are too great for PDL stabilization, retention will be needed long-term. If the dental arches were over-expanded, that’s the obvious conclusion—and many current orthodontic patients are being put into that situation.
![]()
Typical Retention Schedule
So where does that leave us relative to a typical retention schedule? It usually looks like the attached figure. Would that ever be modified? Of course it would, if the patient was exposed to things that this retention plan would not control, or if he or she were not exposed to things that it does control.
The goal, of course, is to retain what is likely to change without retention.
![]()
Retention: How?
Maintaining Alignment
Now let’s look at how retention is done. The principle: How you do it is primarily determined by what you’re trying to control, then secondarily by practical considerations like the difficulty of fabricating what is needed and the acceptability of the retention device to patients.
A primary goal for patients who have treatment to correct crowding and malalignment of the teeth is to maintain alignment (Image 1). Sounds obvious, doesn’t it? But that leads directly to an important consideration: this requires two-point contact on each tooth. If you don’t have that, just as with an appliance to move teeth, you don’t have control.
How do you get two-point contact? A retainer wire has to be contoured so that it follows the surface of the tooth. That’s easier on the facial than the lingual, so a fixed retainer to maintain lower incisor alignment needs to be against the flat portion of the lingual surface, above the rounded cingulum where only one point of contact would be made (Image 2).
If the retainer is made with heavy wire, it should be bonded only on the canines? Why? So the teeth can move relative to each other in function. Remember, you don’t want to splint them so they can’t move in function.
So what would be needed if you did want to attach the retainer wire to each incisor? The wire would have to be small and flexible, so that the teeth could still move in function (Image 3). A retainer of that design gives more positive control of the incisors, but has a significant disadvantage: the bond to an incisor can break without the patient knowing it, and then tooth decay under the loose bonding material can develop rapidly. If you’re the dentist seeing a recall patient with a retainer like this, it’s important to check carefully to be sure everything is bonded correctly.
 Image 1 Image 1 | 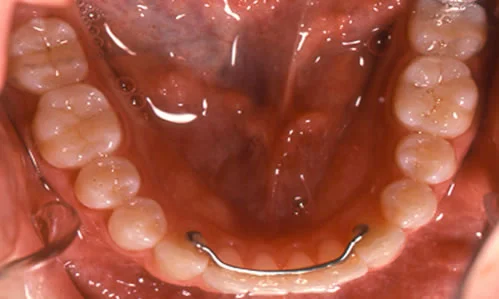 Image 2: Note that the wire is contoured so that it contacts the flat lingual area above the cingumlum, and that it is bonded only to the canines. Image 2: Note that the wire is contoured so that it contacts the flat lingual area above the cingumlum, and that it is bonded only to the canines. |
 Image 3: If each tooth is to be bonded to the retainer wire, it must be light and quite flexible, like this small diameter multi-stranded (twist) wire. Image 3: If each tooth is to be bonded to the retainer wire, it must be light and quite flexible, like this small diameter multi-stranded (twist) wire. |
Maintaining Alignment (cont.)
A removable retainer to maintain alignment must satisfy the same requirement: two point contact is required. Note the use of acrylic around the wire in this “clip-on” retainer, so that it fits tightly and compactly against the facial and lingual surfaces of the anterior teeth (Images 1,2). It is so small that it’s lost down the drain if you drop it in the sink. A retainer with this type of anterior component could be extended posteriorly against the lingual surfaces of the premolars and molar, if those teeth had been rotated or otherwise repositioned during treatment (Image 3). That modification also makes it easier to keep up with.
Maxillary fixed or removable retainers would have to meet the same criterion for effectiveness in maintaining alignment: two-point contact on the teeth. It is easier to obtain 2-point contact on the wider facial surface of maxillary incisors with wire than on teeth with more curved or smaller facial surfaces. Note in image 4 the modification to place tightly-fitting wires against the facial surface of the canine. For this patient, the maxillary canines had been rotated slightly and moved lingually into position, so it was important to keep them from drifting facially and rotating toward their original orientation.
Another aspect of maintaining alignment is keeping spaces closed or open, as desired. Also in Image 5, note the wires mesial and distal to the small maxillary lateral incisors to keep space open until a restorative dentist can build up the crown width with a composite bonding material.
 Image 1, Clip-on retainer, frontal view: The retainer is made on a laboratory model, with a wire fitted around the canines and incisors, and acrylic added to give good (2-point) contact with the facial and lingual surfaces. Image 1, Clip-on retainer, frontal view: The retainer is made on a laboratory model, with a wire fitted around the canines and incisors, and acrylic added to give good (2-point) contact with the facial and lingual surfaces. |  Image 2, Clip-on retainer, occlusal view: It’s called a clip-on retainer because that’s exactly what it does, grasping the teeth tightly as it is pushed to position. Image 2, Clip-on retainer, occlusal view: It’s called a clip-on retainer because that’s exactly what it does, grasping the teeth tightly as it is pushed to position. |
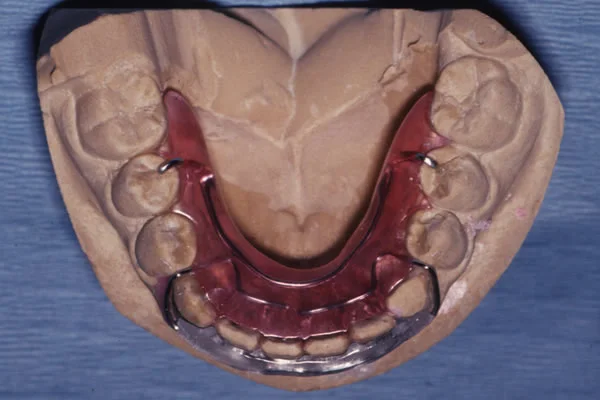 Image 3, Clip-on retainer with distal extension: The distal extension would be used to maintain arch form and prevent rotation of premolars or molar(s). Image 3, Clip-on retainer with distal extension: The distal extension would be used to maintain arch form and prevent rotation of premolars or molar(s). |  Image 4, Maxillary removable retainer: For the upper retainer, the anterior bow has been modified to allow better control of the canines. Image 4, Maxillary removable retainer: For the upper retainer, the anterior bow has been modified to allow better control of the canines. |
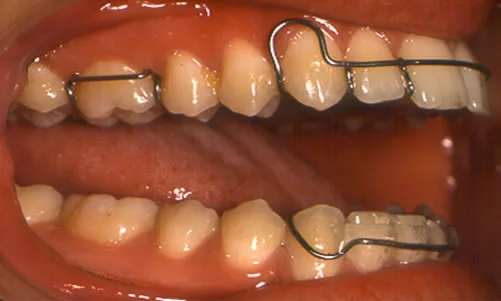 Image 5, Maxillary removable retainer: This maxillary removable retainer has been modified to maintain space mesial and distal to the lateral incisors, using wire segments into the space. Image 5, Maxillary removable retainer: This maxillary removable retainer has been modified to maintain space mesial and distal to the lateral incisors, using wire segments into the space. |
Thermoplastic Retainers
Another possible retainer for maintenance of alignment is a “suckdown” clear plastic device made from a thermoplastic material that was vacuum-formed to fit over the dental arch. As the cost of the equipment to do this dropped in the late 1980s, the Essix company offered it to orthodontists, and retainers of this type became popular. One can be quickly fabricated in the office on a dental cast taken just after the active appliance was removed, so that the patient goes home with a retainer the same day.
Their advantage is that the clear material makes them almost invisible—and this technology was extended to treatment in the development of Invisalign as a treatment method. Most patients like them, especially for the maxillary arch. Although they work in the lower arch, they are less comfortable there, and one thickness of the plastic material between the teeth is more acceptable than two thicknesses. When alignment is the only problem, a maxillary suck-down retainer and a bonded wire or clip-on retainer for the mandibular arch is a good combination.
Keeping Spaces Closed
When teeth are missing and one of the goals of orthodontic treatment is to close space, an important objective of retention is to keep those spaces closed. Note that this patient (Images 1, 2) has had closure of the space of missing laterals, with further space closure on the right side where a second premolar also was missing.
The wrap-around outer bow provides a force to keep the teeth from moving apart, while the acrylic lingual portion provides two-point contact, as does the wire across the flat central incisors. Two-point contact on the facial of the canines, premolars and molars is difficult but unnecessary if the lingual acrylic is configured tightly against that surface.
Another way to keep extraction spaces closed is to solder the outer bow of a removable retainer to clasps on the molar teeth, which extends the bow across a premolar extraction site (Image 3).
Thermoplastic retainers also are a good choice for keeping spaces closed.
 Image 1, Maxillary wrap-around retainer: The outer bow is activated by closing the loops slightly, so that it provides a light force against the teeth. Image 1, Maxillary wrap-around retainer: The outer bow is activated by closing the loops slightly, so that it provides a light force against the teeth. | 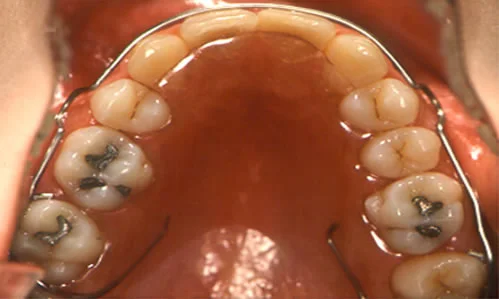 Image 2, Wrap-around retainer in the mouth: Note the two-point contact on the lingual and on the facial of the central incisors. Image 2, Wrap-around retainer in the mouth: Note the two-point contact on the lingual and on the facial of the central incisors. |
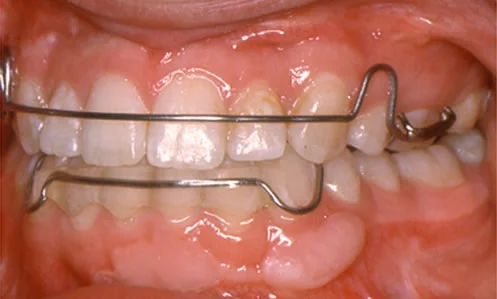 Image 3, Outer bow extended to first molar: To keep a maxillary extraction space closed, the outer bow can be extended posteriorly to the first molar and soldered to the clasp on it. Image 3, Outer bow extended to first molar: To keep a maxillary extraction space closed, the outer bow can be extended posteriorly to the first molar and soldered to the clasp on it. |
Retaining a Maxillary Central DiastemaRetaining a Maxillary Central Diastema
A maxillary central diastema poses a special retention problem, because usually there’s a defect in the bone between these teeth that prevents gingival elastic fibers from crossing the midline. The result is that, unlike every other location in the dental arches, there is nothing to keep the teeth together after the central incisors have been brought together.
The solution is a flexible wire bonded on the lingual (Image 1). The space pops open as soon as there is nothing holding the teeth together, so a bonded flexible wire is by far the best retainer. A removable retainer moves the teeth back and forth a little every time it is placed or removed, and that leads to continuing mobility and risks both periodontal breakdown and root resorption.
The wire is contoured to be passive on a dental cast (Image 2). To bond the retainer so that it keeps the space closed, it is necessary to pull the teeth tightly together (Image 3), and then bond it in position (Image 4). A flexible wire allows the teeth to move slightly in function, and is compatible with long-term periodontal health; a heavy stiff wire splints the teeth and prevents movement in function. The flexible wire also is much more likely to remain in place. This is a definite indication for a retainer that will be needed indefinitely.
 Image 1, Maxillary central diastema: A wide separation of the teeth like this usually is due to a cleft in the interdental bone, with excessive fibrous tissue in the area. Image 1, Maxillary central diastema: A wide separation of the teeth like this usually is due to a cleft in the interdental bone, with excessive fibrous tissue in the area. |  Image 2, Laboratory preparation: The flexible wire must be formed in the laboratory to be sure that it will fit passively when it is bonded intra-orally. Image 2, Laboratory preparation: The flexible wire must be formed in the laboratory to be sure that it will fit passively when it is bonded intra-orally. |
 Image 3, Tying teeth together for bonding: If the retainer is bonded before the orthodontic appliance is removed, the brackets on the central incisors can be used to hold the space tightly closed during bonding. If brackets have been removed, a wire ligature can be looped over the crowns to hold the space closed. Image 3, Tying teeth together for bonding: If the retainer is bonded before the orthodontic appliance is removed, the brackets on the central incisors can be used to hold the space tightly closed during bonding. If brackets have been removed, a wire ligature can be looped over the crowns to hold the space closed. |  Image 4, Bonding completed: The flexible wire retainer has two advantages over a heavier wire: it allows better periodontal health and is more likely to be maintained long-term. Image 4, Bonding completed: The flexible wire retainer has two advantages over a heavier wire: it allows better periodontal health and is more likely to be maintained long-term. |
 Image 5: Tying the teeth together while bonding them ensures that they will not move apart during the bonding process - a prudent step since a diastema can re-open remarkably quickly. Image 5: Tying the teeth together while bonding them ensures that they will not move apart during the bonding process - a prudent step since a diastema can re-open remarkably quickly. |
Maintaining Overbite Correction
Many patients with excessive overjet (the typical Class II division 1) also have a deep bite anteriorly, because the lack of incisor contact allows the lower incisors to over-erupt. For these patients, retaining the overbite correction is as important as keeping the upper incisors in alignment.
How do you retain overbite? If it was due to over-eruption of lower incisors, you block further eruption of those teeth. This requires a bite plate behind the upper incisors. It is easy to contour the anterior palatal portion of an acrylic retainer so that the lower incisors just touch it, and the wire outer bow of the retainer can be activated to keep a light force against the upper incisors. If the overbite was due to over-eruption of the maxillary incisors, a mandibular clip-on retainer can provide a surface that prevents re-eruption after treatment.
For the patient shown in these photos (Images 1 and 2), contact of the incisors with the retainer in the other arch is controlling re-eruption in both arches.
Suck-down retainers are not a good choice for a patient who had excessive overbite, because the light contact of the plastic material with the facial and lingual surfaces of the teeth may not be enough to keep incisors from erupting.
 Image 1, Overbite retention: For this patient, the lower incisors contact the palatal portion of the maxillary retainer when the teeth are brought together, and the upper incisors contact the upper surface of a lower clip-on retainer. This keeps the incisors in both arches from re-erupting. Image 1, Overbite retention: For this patient, the lower incisors contact the palatal portion of the maxillary retainer when the teeth are brought together, and the upper incisors contact the upper surface of a lower clip-on retainer. This keeps the incisors in both arches from re-erupting. | 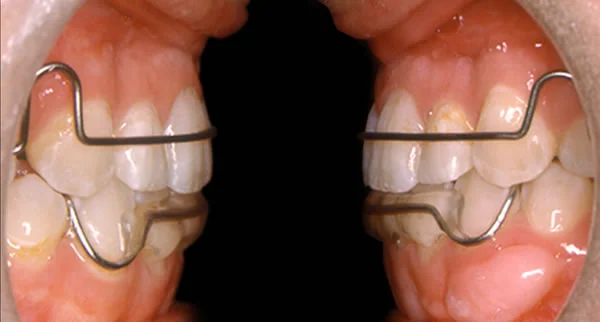 Image 2, Overbite retention: The wire bow of the upper (Hawley) retainer controls the a-p position of the upper incisors, while contact of their incisal edges with the lower clip-on retainer controls their vertical position. Image 2, Overbite retention: The wire bow of the upper (Hawley) retainer controls the a-p position of the upper incisors, while contact of their incisal edges with the lower clip-on retainer controls their vertical position. |
Maintaining Open Bite Correction
Anterior open bite usually is due to excessive eruption of maxillary posterior teeth, not to infra-eruption of maxillary incisors. If that is the case, force to oppose eruption of those teeth would be an important component of a retainer.
The easiest way to generate such a force is to extend the acrylic of a maxillary retainer over the occlusal surface (Image 1), so that the mandible is forced downward a little more than the freeway space (Image 2). So the retainer should look as if it makes the open bite worse? In a word, yes. It may be counter-intuitive but it does give control of posterior eruption.
This can be effective for mild open bite problems, but not for patients with a severe long face / open bite growth pattern. As we have noted, those patients may require re-treatment after growth stops.
 Image 1, Open bite retainer: To control eruption of posterior teeth, the acrylic of a palate-covering retainer can be brought over the occlusal surface. Image 1, Open bite retainer: To control eruption of posterior teeth, the acrylic of a palate-covering retainer can be brought over the occlusal surface. |  Image 2, Open bite retainer: The patient is held open enough to generate light force opposing eruption of both maxillary and mandibular posterior teeth. The idea, of course, is to maintain an ideal 1-2 mm overbite anteriorly. Image 2, Open bite retainer: The patient is held open enough to generate light force opposing eruption of both maxillary and mandibular posterior teeth. The idea, of course, is to maintain an ideal 1-2 mm overbite anteriorly. |
Maintaining Class I Occlusion
As we have noted, after correction of a skeletal Class II problem, growth in the original pattern of more maxillary than mandibular growth can recreate the malocclusion. That’s why treatment should end at about the time adolescent growth subsides to the very slow levels of adult life.
How do you retain an occlusal relationship? For Class II patients, a functional appliance like the one shown here is the best way to do that. Think about it: this appliance, into which the patient bites into a predetermined position, is rather like maxillary and mandibular retainers bonded together. If the Class II patient is still growing, it makes no sense to have retainers that maintain alignment and tooth position in each arch but do not retain the occlusal relationship. From the patient’s point of view, wearing retainers that are joined together is not appreciably different from wearing separate upper and lower retainers, and they need to wear it only at night. An appliance like this during the last part of post-treatment growth is the only way to keep some patients from slipping back toward Class II. It isn’t exactly active treatment, it’s just a way to control an unfortunate growth pattern.
For mandibular prognathic Class III patients, unfortunately, this doesn’t work. We have already discussed the difficulty of controlling that growth pattern. Like severe open bite patients, re-treatment after mandibular growth subsides in the late teens, is required, and orthognathic surgery may be the best treatment.

Summary
How is retention accomplished? With procedures aimed at the specific problem(s) of individual patients:
Alignment: successful appliances include
- vacuum-formed thermoplastic “suck-down” retainer
- maxillary palate-covering retainers with wire outer bow (Hawley retainer)
- mandibular clip-on retainers with wire-reinforced plastic in contact with the teeth
- mandibular lingual bonded wires
- heavy wire, bonded only to canines
- light wire, bonded to each tooth
- maxillary lingual light wires, bonded to central incisors only or centrals and laterals
Space closure:
- wrap-around facial wire
- wire soldered to molar clasps
- suck-down retainer
Deep bite: contact with surface of retainer in other arch
Anterior open bite: occlusal coverage posteriorly
Class II: modified functional appliance
Referral to Self-test
At this point, review the assigned reading for this module (Chapter 18, pages 606-616, Contemporary Orthodontics, 5th edition; Chapter 17, pages 617-628, 4th edition). Then take the self-test and use it to direct your re-examination of parts of the teaching module and the reading.
Copyright 2013, UNC Department of Orthodontics.
Self-Test
Question 1
Which of the following are major reasons for orthodontic retainers after the end of active treatment?
- Imperfect occlusion
- PDL reorganization incomplete
- gingival fiber reorganization incomplete
- unfavorable growth
- a and b
- c and d
- a, b and c
- b, c and d ✓
- all are major reasons
Correct
That’s correct; b, c and d is the right answer. Imperfect occlusion is not a reason for orthodontic retention (thought it might be a reason for more thorough treatment), because the occlusal relationships have little to do with post-treatment stability. Despite what some clinicians have claimed, a patient who has a perfect result needs retainers just as much as one whose occlusion is improved but not perfect. The other things on the list are the major reasons for retention.
Incorrect
No, that’s incorrect. The correct answer is b, c and d. Imperfect occlusion is not a reason for orthodontic retention (thought it might be a reason for more thorough treatment), because the occlusal relationships have little to do with post-treatment stability. Despite what some clinicians have claimed, a patient who has a perfect result needs retainers just as much as one whose occlusion is improved but not perfect. The other things on the list are the major reasons for retention.
Question 2
When passive arch wires are left in place as retainers after active tooth movement has stopped, how long does it take for the PDL to reorganize?
- 2-3 months
- 4-6 months
- 7-9 months
- at least a year
- an indefinitely long time ✓
Correct
That’s right. The time would be indefinitely long, because PDL reorganization proceed very far as long as teeth are splinted together by archwires, and it is incomplete when the braces are removed no matter how long passive archwires have been in place. Reorganization of the PDL requires that a tooth can be displaced in function relative to the ones next to it, which is what happens during normal function.
Incorrect
No, that’s wrong. The time would be indefinitely long, because PDL reorganization proceed very far as long as teeth are splinted together by archwires, and it is incomplete when the braces are removed no matter how long passive archwires have been in place. Reorganization of the PDL requires that a tooth can be displaced in function relative to the ones next to it, which is what happens during normal function.
Question 3
How long does it take for gingival elastic fibers to completely remodel after a severely rotated tooth has been repositioned?
- 2-3 months
- 4-6 months
- 7-9 months
- at least a year
- an indefinitely long time ✓
Correct
That’s right, #5 is the correct answer. Gingival elastic fibers take a long time to remodel when they have been stretched a lot, and the greatest amount of stretching of those fibers occurs when a severe rotation is corrected. Remodeling of gingival fibers does begin while archwires are holding the teeth in position, but it isn’t complete even after a year of archwire retention and another year of being held by a retainer. For that reason, a surgical fiberotomy procedure often is needed to prevent re-rotation.
Incorrect
No, that’s wrong. #5 is the correct answer. Gingival elastic fibers take a long time to remodel when they have been stretched a lot, and the greatest amount of stretching of those fibers occurs when a severe rotation is corrected. Remodeling of gingival fibers does begin while archwires are holding the teeth in position, but often it isn’t complete even after a year of archwire retention and another year of being held by a retainer. For that reason, a surgical fiberotomy procedure often is needed to prevent re-rotation.
Question 4
(A) Mandibular wisdom teeth routinely should be removed at the end of orthodontic treatment, because (B) pressure on the other teeth as they try to erupt is a major cause of lower incisor crowding.
- A true, B true, related
- A true, B true, not related
- A true, B false
- A false, B true
- A and B false ✓
Correct
That’s right, both statements are false. There are indications for removal of third molars, but that doesn’t have to be done routinely, and pressure from third molars is not the main reason for crowding of lower incisors in the late teens.
Incorrect
No, that’s wrong. Both statements are false. There are indications for removal of third molars, but that doesn’t have to be done routinely, and pressure from third molars is not the main reason for crowding of lower incisors in the late teens.
Question 5
Which of the following are ways in which growth in the late teens affects the stability of a corrected malocclusion?
- forward mandibular growth
- downward rotation of the mandible
- decrease of the mandibular plane angle
- downward growth of the maxilla
- a and b
- a, b and c
- b, c and d
- a, b and d ✓
- all are major reasons
Correct
That’s right, the correct answer is #4, a, b and d. A small decrease of the mandibular plane angle usually occurs during normal adolescent growth, but this has little or no effect on the stability of the corrected malocclusion, especially if the treatment ended at the end of the adolescent growth spurt. In contrast, downward growth of the maxilla that causes downward rotation of the mandible is a major cause of anterior open bite, and forward growth of the mandible is the major cause of late incisor crowding, and if extreme leads to mandibular prognathism and a severe Class III malocclusion.
Incorrect
No, that’s wrong, the correct answer is #4, a, b and d. A small decrease of the mandibular plane angle usually occurs during normal adolescent growth, but this has little or no effect on the stability of the corrected malocclusion, especially if the treatment ended at the end of the adolescent growth spurt. In contrast, downward growth of the maxilla that causes downward rotation of the mandible is a major cause of anterior open bite, and forward growth of the mandible is the major cause of late incisor crowding, and if extreme leads to mandibular prognathism and a severe Class III malocclusion.
Question 6
What is the minimum length of time for full-time (except while eating) retainer wear after correction of alignment problems?
- 3 months ✓
- 6 months
- 7-12 months
- one year
- an indefinitely long time
Correct
That’s correct. 3 months is the minimum time, because PDL reorganization takes that long. Beyond 3 months, gingival elastic fibers are the main threat to alignment, and their effect can be controlled with part-time wear. But of course that schedule presumes that the dental arches have not been over-expanded and incisors have not been moved too far labially—if that’s not the case, permanent retention will be needed.
Incorrect
No, that’s incorrect. 3 months is the minimum time, because PDL reorganization takes that long. Beyond 3 months, gingival elastic fibers are the main threat to alignment, and their effect can be controlled with part-time wear. But of course that schedule presumes that the dental arches have not been over-expanded and incisors have not been moved too far labially—if that’s not the case, permanent retention will be needed.
Question 7
(A) Retention time for adults often can be shorter than it is for adolescents because (B) adults take their treatment more seriously and are more compliant with the retainer schedule.
- A true, B true, related
- A true, B true, not related ✓
- A true, B false
- A false, B true
- A and B false
Correct
That’s right. Both statements are true but they have no cause-effect relationship. The major reason that adults often have shorter retention times than adolescents is that they do not need prolonged retention to control growth, while adolescents do. Compliance with retainer wear has nothing to do with the speed of reorganization of tissues. Age does—the older you are, the slower you recover from most things, so PDL reorganization probably is a bit slower in adults.
Incorrect
No, that’s incorrect. Both statements are true but they have no cause-effect relationship. The major reason that adults often have shorter retention times than adolescents is that they do not need prolonged retention to control growth, while adolescents do. Compliance with retainer wear has nothing to do with the speed of reorganization of tissues. Age does—the older you are, the slower you get recover from most things, so PDL reorganization probably is a bit slower in adults.
Question 8
For which of the following do you need 2-point contact of the retainer with the tooth to maintain tooth position? Correction of …
- rotation
- a-p alignment
- vertical alignment
- space closure
- a and b
- a, b and c
- b, c and d
- a, b and d
- a, b, c and d ✓
Correct
That’s right, a retainer needs at least 2-point contact for all of these. One-point contact allows tooth position to change in all of these ways even if a retainer is worn.
Incorrect
No, that’s wrong. A retainer needs at least 2-point contact for all of these. One-point contact allows tooth position to change in all of these ways even if a retainer is worn.
Question 9
What is the greatest problem in using a suck-down lower retainer to maintain incisor alignment?
- compliance ✓
- poor control of rotations
- poor control of vertical alignment
- poor control of facio-lingual alignment
- poor control of space closure
Correct
That’s right, the greatest problem is compliance. A lower suckdown is less comfortable than an upper one, and patients don’t wear them as well for that reason. It’s true that suckdowns do not control vertical position as well as facio-lingual position, but vertical control is adequate if the patient wears it, and control of both rotations and space closure is good.
Incorrect
No, that’s incorrect. The greatest problem is compliance. A lower suckdown is less comfortable than an upper one, and patients don’t wear them as well for that reason. It’s true that suckdowns do not control vertical position as well as facio-lingual position, but vertical control is adequate if the patient wears it, and control of both rotations and space closure is good.
Question 10
What is the greatest disadvantage of a suckdown retainer for the maxillary arch?
- compliance
- poor control of rotations
- poor control of vertical alignment ✓
- poor control of facio-lingual alignment
- poor control of space closure
Correct
That’s correct, the answer is #3. A maxillary retainer often needs to control both alignment and overbite. An acrylic palate-covering retainer makes it easy to arrange a bite plate lingual to the upper incisors to keep the lower incisors from erupting, while a suckdown retainer maintains alignment but does not offer the same control of lower incisor eruption. If maintenance of alignment is all that needed, a suckdown retainer is a good choice.
Incorrect
No, that’s incorrect. The answer is #3. A maxillary retainer often needs to control both alignment and overbite. An acrylic palate-covering retainer makes it easy to arrange a bite plate lingual to the upper incisors to keep the lower incisors from erupting, while a suckdown retainer maintains alignment but does not offer the same control of lower incisor eruption. If maintenance of alignment is all that needed, a suckdown retainer is a good choice.
Question 11
(A) When a heavy wire is used as a fixed retainer for the lower incisors, it is important to bond it to every tooth because (B) If it’s bonded to multiple teeth, it won’t come off if the bond breaks on one tooth.
- A true, B true, related
- A true, B true, not related
- A true, B false
- A false, B true ✓
- A and B false
Correct
That’s right, the first statement is false and the second statement is true. When a heavy wire is used as a fixed lower canine-to-canine retainer, it should be bonded only to the canines so that the incisors are not splinted together and can function normally. It’s true that if a fixed retainer is bonded to all the incisors, it won’t come off if the bond to one incisor breaks—but that’s a major disadvantage of bonding to multiple teeth, because tooth decay under a broken bond can develop quickly.
Incorrect
No, that’s incorrect. The first statement is false and the second statement is true. When a heavy wire is used as a fixed lower canine-to-canine retainer, it should be bonded only to the canines so that the incisors are not splinted together and can function normally. It’s true that if a fixed retainer is bonded to all the incisors, it won’t come off if the bond to one incisor breaks—but that’s a major disadvantage of bonding to multiple teeth, because tooth decay under a broken bond can develop quickly.
Question 12
Which of these characteristics are the major disadvantages of a canine-to-canine clip-on retainer?
- So small it’s easy to lose
- So small it’s easy to bend out of shape
- Poor control of vertical alignment
- Poor control of space closure
- a only ✓
- b only
- a and b
- c and d
- a, c and d
Correct
That’s correct, the small size that makes it so easy to lose is a major disadvantage of a canine-to-canine clip-on; the other characteristics are strengths rather than weaknesses. The clip-on design resists distortion well, gives good a-p and vertical control of incisor position, and excellent control of space closure.
Incorrect
No, that’s incorrect. The small size that makes it so easy to lose is a major disadvantage of a canine-to-canine clip-on; the other characteristics are strengths rather than weaknesses. The clip-on design resists distortion well, gives good a-p and vertical control of incisor position, and excellent closure of space closure.
Question 13
Which of these characteristics is the most important cause of the difficulty in keeping a maxillary central diastema closed?
- large width of the space
- excessive fibrous tissue between the teeth
- abnormal contour of the teeth
- abnormal elastic fiber arrangement ✓
- abnormal root structure of the teeth
Correct
That’s right, the biggest problem is an abnormal elastic fiber arrangement—the elastic fibers do not cross the midline as they normally do, so there is nothing to keep the space closed. It is true that there often is a wide space and usually there is excessive fibrous tissue between the teeth that needs surgical removal, but the space can be closed without great difficulty. Both the crowns and roots of the teeth are normal and do not affect treatment and retention.
Incorrect
No, that’s wrong. The biggest problem is an abnormal elastic fiber arrangement—the elastic fibers do not cross the midline as they normally do, so there is nothing to keep the space closed. It is true that there often is a wide space and usually there is excessive fibrous tissue between the teeth that needs surgical removal, but the space can be closed without great difficulty. Both the crowns and roots of the teeth are normal and do not affect treatment and retention.
Question 14
(A) After a maxillary central diastema is closed, a bonded lingual retainer is the best choice because (B) a removable retainer clips the teeth tightly.
- A true, B true, related
- A true, B true, not related ✓
- A true, B false
- A false, B true
- A and B false
Correct
That’s correct. Both statements are true, but the second statement is not why a bonded retainer is the best choice. The space between the maxillary incisors after a central diastema has been closed usually pops open a little every time a removable retainer is removed, and then the teeth are pushed back together when the retainer is re-inserted. That means the teeth are continually jiggled back and forth. This keeps them from tightening up as the PDL is reorganized and may lead to root resorption—so a fixed retainer is more physiologic as well as more esthetic.
Incorrect
No, that’s wrong, both statements are true, but the second statement is not why a bonded retainer is the best choice. The space between the maxillary incisors after a central diastema has been closed usually pops open a little every time a removable retainer is removed, and then the teeth are pushed back together when the retainer is re-inserted. That means the teeth are continually jiggled back and forth. This keeps them from tightening up as the PDL is reorganized and may lead to root resorption—so a fixed retainer is more physiologic as well as more esthetic.
Question 15
(A) The most likely mechanism by which high-intensity light accelerates tooth movement (if it does) is increased blood flow because (B) light chills the tissues it affects and cold is known to facilitate healing. These statements are:
- A true, B true, related
- A true, B true, not related
- A true, B false ✓
- A false, B true
- A and B false
Correct
That’s right, A is true and B is false. Light energy is known to heat tissues, heating tissues is known to increase blood flow, and increased blood flow seems to facilitate tooth movement, so A is the most likely mechanism at present—though the mechanism is not understood.. Even though correctly-timed cold can facilitate healing after injury, light doesn’t chill tissues, so B is incorrect. What is the real mechanism for tissue-penetrating light? That’s still unknown.
Incorrect
No, that’s incorrect. A is true and B is false. Light energy is known to heat tissues, heating tissues is known to increase blood flow, and increased blood flow seems to facilitate tooth movement, so A is the most likely mechanism at present—though the mechanism is not understood. Even though correctly-timed cold can facilitate healing after injury, light doesn’t chill tissues, so B is incorrect. What is the real mechanism for tissue-penetrating light? That’s still unknown.