Pain Control During Endodontic Treatment1
Importance of Pain Control During Treatment2
- Pain during treatment significantly impacts on the amount of post-op. pain
Info
==The more pain a patient feels during treatment, the more pain they will experience after treatment.==
Local Anaesthesia3
- Three goals of local anaesthesia:
- Anaesthesia during treatment
- Haemostasis during treatment
- Prolonged post-operative pain control
Local Anaesthesia3
Mechanisms of Pain Control
- Pain control from local anaesthetics - two mechanisms:
- Direct: Block discharges from peripheral nerves
- Duration: Minutes → Hours
- Indirect: Prolonged blocking of peripheral input reduces central sensitization
- Duration: Hours → Days
- Direct: Block discharges from peripheral nerves
Inadequate Local Anaesthesia
- Pain during treatment
- More post-operative pain
- Since prolonged exposure to sensory input increases allodynia and hyperalgesia
- ==Allodynia: Pain resulting from a stimulus that would not normally be painful.==
- ==Hyperalgesia: An exaggerated pain response to a stimulus.==
Anaesthetic efficacy of the supplemental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irreversible pulpitis4
25 Maxillary Teeth
Nusstein et al JoE 1998
graph TD A[Bu Infiltration Injection<br>Lignocaine + 1:100,000 Adr] --> B[No Response to PT's 92 %] A --> C[Responded to PT's 8 %] B --> D[No Pain 68 %] B --> E[Pain in Dentine 4 %] B --> F[Pain in Pulp 20 %] C --> G[Need supplementary LA techniques] F --> G
Conclusion
Even with a successful buccal infiltration in the maxilla, a significant portion of patients (24%) still experience pain during treatment for irreversible pulpitis.
26 Mandibular Teeth5
IAN Block Injection Lignocaine + 1:100,000 Adr
- No Response to PT’s — 38 %
- Responded to PT’s — 62 %
- No Pain — 7 %
- Pain in Dentine — 12 %
- Pain in Pulp — 19 %
- Need supplementary LA techniques
Conclusion
The IAN block has a very high failure rate for mandibular molars with irreversible pulpitis.
Why Does Local Anaesthesia Not Work with Acute Irreversible Pulpitis?
- Various theories proposed — none proven
- Most commonly discussed:
- Inflammation activates nociceptors (pain receptors) and associated central pain mechanisms
- Inflammatory mediators reduce threshold of nociceptor activation → So minor stimuli fire the neurons
- Mediated by prostaglandins → Produced by arachidonic acid metabolism
- Prostaglandins sensitize nerve endings → Enhances pain and inflammation
- Inflamed pulps have high levels of both prostaglandins and arachidonic acid
Warning
==However, most of these theories focus on local factors around the tooth and fail to adequately explain why a block injection, administered several centimetres away from the site of inflammation, would fail.==
- LA unable to block conduction of all nerve impulses → When pain present - have more impulses than normal
- pH is more acidic in the presence of inflammation so LA is less effective
- Spread of inflammation along myelin sheaths may restrict absorption of the LA solution
- Increased vascularity increases blood flow and removes the LA more rapidly
- Periapically, there may be stasis - reduced blood flow
- Pain can neutralise the effects of LA in the CNS
Other Possible Causes
- Insufficient dose
- Incorrect injection site
- Incorrect technique
- Intravascular injection
- Individual variation - anatomy, dosage, etc.
- Variation in pain threshold and perceptions
- Inadequate time for LA to work
- ==This is a major factor. Dentists often wait only 3-5 minutes, but a block injection for a “hot” tooth may require up to 15 minutes to become fully effective.==
Continued Pain After LA Injection6
- Three stages when pain may be felt:
- Pre-operative
- Dentine
- Pulp
**Strategies to Manage Acute Irreversible Pulpitis in a Lower Molar steps 1-3 out of 8 **7
- Pre-empt the difficult situation - i.e. Diagnosis !!
- Consider pre-medication with ibuprofen → Assuming no contra-indication
- Test tooth : triplex air + percussion during exam
The Effect of Premedication with Ibuprofen and Indomethacin on the Success of Inferior Alveolar Nerve Block for Teeth with Irreversible Pulpitis8
A randomized double-blind clinical trial investigated ibuprofen and indomethacin pre-medication for acute irreversible pulpitis in mandibular molars, focusing on an earlier stage of the condition.
Findings:
- Cold sensibility tests were not perfect predictors of anesthesia effectiveness.
- Ibuprofen and indomethacin significantly improved treatment success compared to placebo.
Discussion:
- NSAID pre-medication aids in pain control, with ibuprofen being more effective and safer than indomethacin.
- Efficacy hinges on the stage of pulpitis, with better results in earlier, less inflamed cases.
Acute Irreversible Pulpitis9
graph TD A[May or may not have pain to bite and percussion] --> B[?] B --> C[± Pain is spontaneous] B --> D[± Pain lying down] B --> E[± Pain wakes patient] B --> F[± Primary acute apical periodontitis] C --> G[Intense throbbing / aching pain; continuous or may come and go] D --> G E --> G F --> H[Pain to bite & tender to percussion] I[Pain with cold stimuli] --> J[Short, very sharp pain then lingering ache / throb] K[± Pain with heat] --> J
Conclusion of Premedication Study
- Pre-medication with a single dose of Ibuprofen can help with pain control during treatment of acute irreversible pulpitis in mandibular molars → If there is no spontaneous pain
- Highlights the need for a thorough history and diagnosis of the presenting complaint
Practical Challenge
The main practical challenge is scheduling the one-hour wait time for the premedication to take effect in a busy practice.
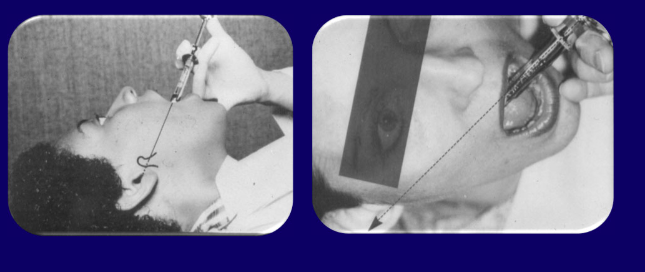
**Step 4: Gow Gates Block
The Gow-Gates Mandibular Block
Technique and Landmarks10
Target site: Lateral region of the neck of the condyle, just below the insertion point of the lateral pterygoid muscle
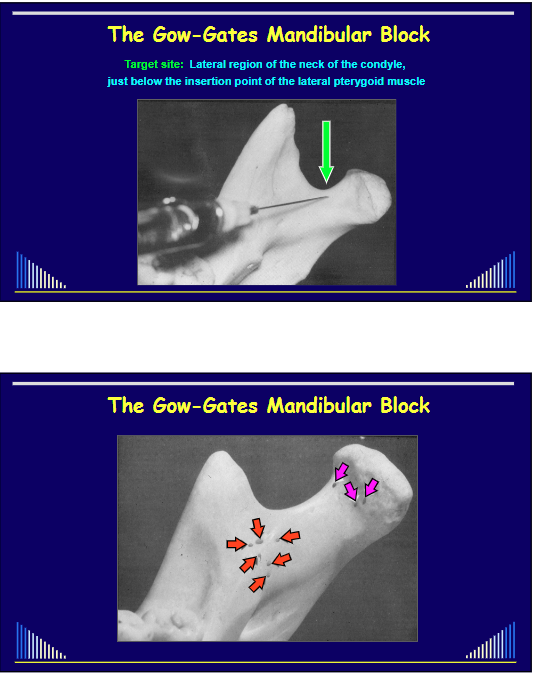
Goal
==To anaesthetise the entire mandibular nerve trunk after it exits the foramen ovale. This includes accessory branches that are often missed by a standard IAN block, which is why it is more effective.==
Entry point: Medial to the deep tendon of the temporalis muscle and slightly below the Palatal cusp of the UPPER 2nd molar

External landmarks: Apex of the intertragic notch and the lower border of the tragus through to opposite corner of the mouth
Advantages of the Gow-Gates Block1112
-
High success rate
- GG: 92 - 99 % vs - IAN: 65 - 85 %
-
No supplementary injections needed
- i.e. Do not need Long Buccal or Lingual nerve injections
-
Less muscle involved
-
Less painful
- Even though larger needle used!
-
==Requires about 15 minutes to take full effect==
- This waiting time can be productively used for patient consultation.
-
A safer technique
-
Less blood vessels at injection site
- Positive aspiration rate - negligible
-
No vaso-constrictor required
- Use plain Prilocaine (e.g. Citanest 4%)
- Only 1 carpule required (i.e. 2.2 ml)
Incidence of Grade “A” anaesthesia1314
Prilocaine , felyrpressin or just plain are all highly successful when doing a gow gates
**Step 5: Retesting after gow-gates block
- Re-test with triplex air and percussion → If no pain: place rubber dam and re-test !! → If still pain: Give IAN Block + Buccal Infiltration
Inferior Alveolar Nerve Block Hints15
Technique Tip
==The most frequent mistake in the gg-block is placing the needle too far distally. Using a short needle with a slight bend can improve control and help target the correct area. The historical fear of needle breakage at the hub is obsolete with modern, single-piece needle manufacturing.==
Efficacy of combining a buccal infiltration with an inferior alveolar nerve block for mandibular molars with irreversible pulpitis1617
Info
This indicates that adding a buccal infiltration is more effective than simply increasing the volume at the IAN block site. However, a 35% failure rate still exists.
Articaine vs. Lidocaine
==A review of the literature shows no significant advantage in using 4% articaine over 2% lidocaine for block anaesthesia in these situations. While some studies show a benefit for infiltration, its use for IAN blocks is discouraged due to its higher concentration (4% vs 2%) and the associated, albeit debated, increased risk of lingual nerve paraesthesia.==
** Gow-gates block Conclusions:**18
- More effective LA for acute irreversible pulpitis in lower molars when an IAN block is combined with a Bu infiltration
- However, some patients will still have pain !!
Supplementary Injections - Other Teeth19
-
Labial infiltration for lower anterior teeth
-
Palatal infiltration for upper molars
- This is a highly effective supplement to a buccal infiltration because it directly anaesthetises the palatal root, which is often missed by buccal-only approaches.
-
Palatal for upper premolars and anterior teeth
- Anterior middle superior alveolar (AMSA) nerve block
**step 8: re-test with triplex air and percussion
- 8. Re-test again with triplex air and percussion → If no pain: proceed with treatment
- Turn the H/S handpiece water off !! → If pain: give PDL injection and test again
- Can then normally cut enamel or restoration
Rubber Dam Cuff Technique20
Advantages:
- Enables PDL injections if required
- Full access to the entire tooth
- Better vision
Periodontal Ligament Injection21
Mechanism
==The PDL injection is effectively an intraosseous injection that works very quickly (20-30 seconds). The anaesthetic is not intended to track down the ligament space. Instead, high pressure forces the solution through the porous cancellous bone of the socket wall to reach the apex.==
Technique
- Place the needle into the gingival sulcus, angled into the PDL space.
- ==The bevel of the needle must face the bone, not the tooth root.==
- Inject with firm, steady pressure at 4-6 points around the tooth (e.g., mesiobuccal, distobuccal, mesiolingual, distolingual corners).
- Only a very small amount of solution can be injected at each site.
Intra-osseous Injections22
Warning
While dedicated systems exist for direct intraosseous injection, they are less practical. They are difficult to use, cannot be administered with a rubber dam in place, and carry a risk of iatrogenic damage to the tooth root. The PDL injection is a simpler and safer alternative.
**Step 10 if pain is felt upon reaching pulp **
→ Intra-pulp injection
Intra-Pulp Injection23
Technique
==This injection is most effective when administered through a very small pulp exposure. The small opening allows for the creation of back-pressure, which forces the anaesthetic solution into the pulp tissue, achieving profound anaesthesia. It is recommended to give an intra-pulp injection proactively as soon as a pinpoint exposure is made. If the pulp chamber is widely opened, the lack of back-pressure renders the technique ineffective.==
**Step 11 : If patient is still in pain
→ Pulpotomy only - CS-AB dressing
-
==The goal should shift from complete instrumentation to pain relief. Place a corticosteroid-antibiotic paste (e.g., Leder mix paste) over the canal orifices to control inflammation.==
→ Re-appoint - 3-4 weeks later
Pain Relief after Pulpotomy24
Success
A pulpotomy is highly effective for pain relief. One study found that it can reduce pre-operative pain by an average of 82% (from 100% down to 18%).
Acute Irreversible Pulpitis - Lower Molar Tooth (Flowchart)
flowchart TD A[Discuss Diagnosis, Treatment Plan, etc] --> B[TEST - Cold, Percussion] B --> C[Gow-Gates Mandibular Block] C --> D[TEST - Cold, Percussion] D --> E[Inferior Alveolar Nerve Block + Buccal Infiltration] E --> F[TEST - Cold, Percussion] F --> G[Periodontal Ligament Injection] G --> H[TEST - Cold, Percussion] H --> I[Intra-Pulp Injection] I --> J[Pulpotomy + CS-AB Dressing]
And …25
❌ Do NOT prescribe antibiotics !!!
- AB’s are unnecessary and contra-indicated
- AB’s are not pain relieving medications
- AB’s do not help treat inflammation
- Pulpitis is an INFLAMMATORY condition
- Even though it is caused by the presence of bacteria in the tooth
- And a systemically-administered AB will not reach the bacteria in in the caries, crack, restoration/tooth interface, etc.
Danger
==Prescribing antibiotics in this situation is inappropriate, ineffective (acting only as a placebo), and contributes to antibiotic resistance. Pain should be managed with analgesics and NSAIDs, not antibiotics.==
Summary26
- Achieving adequate pain control is difficult, and unpredictable, when treating acute irreversible pulpitis
- Dentists need various strategies to ensure good pain control for their patients
- Before treatment
- During treatment
- After treatment
Summary of Management Strategy27
- Pre-empt the difficult situation
- Consider pre-medication
- Test tooth pre-op: → Triplex air + percussion
- Gow-Gates Block → Discuss treatment, etc.
- Re-test: triplex air + percussion → If no pain: proceed with treatm → Turn water off H/S handpiece → If still pain: Give IAN Block + Buccal Infiltration
- Allow more time for LA to work
- Place rubber dam - cuff tech.
- Re-test again: air + percussion → If no pain: proceed with treatm → Turn water off H/S handpiece → If pain: give PDL injection
- If pain felt on reaching dentine → PDL injection
- If pain felt on reaching the pulp → Intra-pulp injection
- If still pain → Pulpotomy - CS-AB dressing → Re-appoint - 3-4 weeks later
Post-Operative Follow-up
Timeline
- 3-4 weeks later
Additional Instructions
- ==Patients should be prescribed appropriate analgesics or anti-inflammatory agents (e.g., ibuprofen) for post-operative pain management.==
- ==Patients should be explicitly told that antibiotics are not necessary or helpful for this condition.==
Footnotes
-
Original PDF page 1: O1A Pain control During retreatment, p.1 ↩
-
Original PDF page 2: O1A Pain control During retreatment, p.2 ↩
-
Original PDF page 3: O1A Pain control During retreatment, p.3 ↩ ↩2
-
Original PDF page 4: O1A Pain control During retreatment, p.4 ↩
-
Original PDF page 5: O1A Pain control During retreatment, p.5 ↩
-
Original PDF page 7: O1A Pain control During retreatment, p.7 ↩
-
Original PDF page 14: O1A Pain control During retreatment, p.14 ↩
-
Original PDF page 8: O1A Pain control During retreatment, p.8 ↩
-
Original PDF page 13: O1A Pain control During retreatment, p.13 ↩
-
Original PDF page 15: O1A Pain control During retreatment, p.15 ↩
-
Original PDF page 16: O1A Pain control During retreatment, p.16 ↩
-
Original PDF page 17: O1A Pain control During retreatment, p.17 ↩
-
Original PDF page 18: O1A Pain control During retreatment, p.18 ↩
-
Original PDF page 19: O1A Pain control During retreatment, p.19 ↩
-
Original PDF page 20: O1A Pain control During retreatment, p.20 ↩
-
Original PDF page 21: O1A Pain control During retreatment, p.21 ↩
-
Original PDF page 22: O1A Pain control During retreatment, p.22 ↩
-
Original PDF page 28: O1A Pain control During retreatment, p.28 ↩
-
Original PDF page 29: O1A Pain control During retreatment, p.29 ↩
-
Original PDF page 30: O1A Pain control During retreatment, p.30 ↩
-
Original PDF page 31: O1A Pain control During retreatment, p.31 ↩
-
Original PDF page 35: O1A Pain control During retreatment, p.35 ↩
-
Original PDF page 36: O1A Pain control During retreatment, p.36 ↩
-
Original PDF page 37: O1A Pain control During retreatment, p.37 ↩
-
Original PDF page 38: O1A Pain control During retreatment, p.38 ↩
-
Original PDF page 39: O1A Pain control During retreatment, p.39 ↩
-
Original PDF page 40: O1A Pain control During retreatment, p.40 ↩