Treatment Outcomes, Persistent Radiolucencies, Options for Management1
W/Prof. Paul V. Abbott AO
That root-filled tooth now has a periapical area … What next ???
Case Example
When a root-filled tooth presents with a periapical radiolucency, a practitioner must diagnose the cause and determine the next steps. For example, a tooth with both periapical and lateral radiolucencies was successfully retreated. The healing of both areas suggested the cause was an infected root canal system, including an infected lateral canal, rather than a crack or perforation. This illustrates the core principle: successful outcomes are achieved by correctly diagnosing the problem (the cause), removing that cause (e.g., bacteria), and preventing reinfection.
- Why was there healing?
- Diagnosis
- Provisional
- infected root canal system and apical periodontitis
- Investigated
- crown and post removed, nothing found
- Confirmed
- retreated tooth and area healed
- Provisional
- Cause(s)
- Identified
- Removed
- Diagnosis
Evaluation of Endodontic Treatment2
- the outcome of treatment is what determines success and failure in endodontic treatment
Info
Evaluating the outcome of root canal treatment is crucial for both the patient and the practitioner. It helps determine if the treatment has worked and if the tooth remains stable over time. A root-filled tooth is still susceptible to long-term issues like restoration breakdown and bacterial reinfection, similar to a vital tooth.
-
its difficult to assess the outcome of treatment if patients don’t return
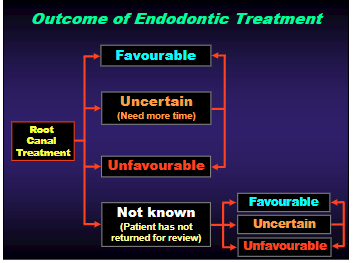
Outcome of Endodontic Treatment345
Criteria for Assessment
- A combination of criteria can be used for outcome assessment
- Histological
- Clinical
- Radiographic
- Functional
- Patient’s perceptions
Use a combination of these criteria
Histological Criteria
- No inflammatory cells
- No scar tissue
- Hard tissue repair
- Bone
- Cementum
- No resorption
- Tooth
- Bone
The IDEAL results !!! BUT … We can NOT assess these criteria in the clinical situation with our patients !!!
However … These criteria MUST be used to evaluate endodontic treatment during RESEARCH Results of research can then be used clinically to provide more predictable treatment outcomes
CRITERIA for a Favourable Outcome:67
-
Lack of symptoms
- But a lack of symptoms does not imply the lack of disease
-
Lack of evidence of ongoing pathosis
- There is no swelling, draining sinus tract, or other soft tissue abnormalities.
-
Radiographic signs of bone repair
- Or no new radiolucency developing
-
No radiographic signs of resorption
-
Function maintained
-
Patient - comfortable tooth, no complaints
The “Toronto study” - JoE 2003
- 95% of cases had no symptoms … but:
- Only 85% had repair evident radiographically
Info
This large study highlighted the discrepancy between symptoms and disease. This reinforces that many dental conditions, including chronic apical periodontitis, are asymptomatic.
WHEN should we assess the outcome?8
Info
There is no single ideal time interval for assessment, as healing rates vary significantly between patients. A Swedish study showed that large lesions could heal in 6 months, while smaller ones could take up to 5 years.
- 6 months - initial indication of how the repair process is going
- 1 - 3 years - more accurate assessment
- 5 years - generally considered the time required to accurately assess outcome of the endodontic treatment
- > 5 years - now really assessing the restoration rather than the RCF
Info
The root filling has done its job; the longevity of the tooth now depends on preventing reinfection.
CRITERIA for an Unfavourable Outcome:9
→ Anything that does not achieve the desired results for a favourable outcome
- Usually because of either: → Bacteria persisting in canals → New bacteria entering the canals → Ongoing periapical disease → true cyst, extra-radicular infection, FBR
Info
Unfavourable outcomes are often evident earlier than favourable ones, as the radiolucency may fail to decrease in size or may even enlarge.
Criteria for Uncertain / Surviving cases10
→ When at least one of the criteria for a favourable outcome has not been achieved but the other criteria have been achieved - for example:
- The pre-operative radiolucency has not healed completely or has not healed at all
- The patient has no symptoms
- There are no other clinical signs
- The patient can function normally on the tooth
- Typically noted at a review appointment
Info
This may indicate the presence of periapical scar tissue.
Considering Root-Filled Teeth with Periapical Radiolucencies11
A new way to consider root-filled teeth with periapical radiolucencies is based on WHEN the radiolucency occurs:
① Early - occur soon after treatment
Note
==(Persistent Radiolucency < 5 years post-treatment)==
→ May be a true “failure” of the endodontic treatment - or the operator!!! → OR: may be due to a true cyst, an extra-radicular infection, a foreign body reaction or a periapical scar
② Late - occur many years later
Note
==(New Radiolucency > 5 years post-treatment)==
→ A “new disease” - rather than a “failure” of endodontic treatment
Unfavourable Endodontic Outcomes12
True “failures” of endodontic treatment
- Occur a short time after treatment
- Due to bacteria being left behind at the time of the previous treatment
- Up to 5 years after treatment
- Probably due to:
- Inadequate treatment techniques
- Inadequate asepsis during treatment
- Inadequate temporaries during treatment
- Inadequate restoration after the RCF
- The patient failing to have a permanent restoration placed
Time Since Previous Endodontic Treatment until Re-Treatment Required13
Info
==The study found that 73% of cases required retreatment within 5 years of the original procedure. This data supports the concept that early radiolucencies are often linked to shortcomings in the initial treatment.==
Info
==The speaker’s own practice data showed a similar trend, with approximately 60% of retreatments occurring within 5 years.==
“Infected Canal Disease Cycle”
Info
==When a small number of bacteria are left in the canal or enter during treatment, they typically cause asymptomatic chronic apical periodontitis. Over months or years, the bacteria multiply, and the periapical lesion grows. Symptoms (an acute exacerbation or
- Small number of bacteria in the canal
- Left at time of treatment
- Gradual proliferation / increase in numbers - Chronic situation for some time
- Periapical response develops - No symptoms until response well established
- Gradual increase in periapical involvement
- Acute phase when conditions suitable
- Many factors can affect the “balance” situation - e.g. Other illness, treatment, stress, tiredness, etc
- This cycle can take 3 mths - 5 yrs
**Late Occurrences: A
Info
==When a radiolucency develops on a tooth more than 5 years after a root canal treatment that was previously deemed healed, it should be considered a new disease process, not a failure of the original endodontic therapy.==
“New Disease”**
- A radiolucency may occur many years after endodontic treatment.
- This occurs when Bacteria re-enter the tooth through:
- Broken down restorations
- Caries
- Cracks
- Trauma - fractures
Restoration Breakdown141516
- All restorations have a finite life span
Info
Bacteria can penetrate through failing margins long before there are any clinical or symptomatic signs of failure.
- Bacterial penetration may be occurring for a long time before:
- Symptoms
- Clinical signs
- Caries
- Fracture
- Dislodgment
- etc, etc…
Bacterial Migration1718
Info
Even under clinically and radiographically sound restorations, micro-gaps can allow fluid and bacteria to penetrate towards the pulp space. An experimental model demonstrated this process.
- Many studies have demonstrated that various bacteria can migrate along the entire length of a root canal filling. Coronal → Apical
- Time for penetration varies
- e.g. 2 days, 3 days,
- 20 days, 30 days,
- 60 days, 90 days,
- etc.
Concepts of Dentine
Dentine – Pulp complex1920
Info
The dentine is not a solid barrier. It is a highly complex, porous structure. Scanning electron microscopy (SEM) reveals that dentinal tubules are not just simple parallel tubes but form an intricate, interconnected network.
The presence and distribution of bacteria in dentinal tubules of root-filled teeth
Kwang S, Abbott PV. Int Endo J - 2014: 47, 600 - 610.
Info
SEM studies on teeth from the bacterial leakage model showed that bacteria do not just stay in the main canal. They migrate extensively through the interconnected dentinal tubule network, eventually reaching the periapical tissues to cause a new lesion.
Experimental Model21222324
Effect of Coronal Restorations2526
Treatment Outcome - Favourable
| RCF’s: | Restorations: Good | Restorations: Poor |
|---|---|---|
| Good | 91.4 % | 44.1 % |
| Poor | 69.6 % | 18.1 % |
Concluded: “… The quality of the coronal restoration was more important than the quality of the RCF for apical periodontal healing …”
Success
This underscores that the long-term longevity of a root-filled tooth is primarily dependent on the seal provided by the final restoration.
Summary of Treatment Outcomes27
- High quality endodontic treatment, based on sound biological principles, will improve the number of favourable outcomes.
- By removing intra-radicular bacteria
- with accurate diagnosis, removal of the cause, aseptic techniques, mechanical cleaning, disinfection via irrigation and medication, interim and temporary restorations, good RCF’s, final restoration, etc
- By reducing the extrusion of foreign bodies into the periapical tissues
- By removing intra-radicular bacteria
- BUT: there will be an upper ceiling to the number of favourable outcomes that can be achieved by conventional endodontic treatment.
- Due to the role played by true cysts and extra-radicular bacteria
- The highest possible number of favourable outcomes will be limited by the incidence of these pathological entities.
Persistent Radiolucencies: Causes28
Due to:
- Intra-Radicular Infection
- Extra-Radicular Infection
- Foreign Body Reaction
- Periapical True Cyst
- Periapical Scar
Guidelines for considering periapical radiolucencies associated with root-filled teeth
| Due to: | Initial Management |
|---|---|
| Intra-Radicular Infection | Endodontic Re-treatment |
| Extra-Radicular Infection | Periapical Surgery |
| Foreign Body Reaction | Periapical Surgery |
| Periapical True Cyst | Periapical Surgery |
| Periapical Scar | Observe and Reassess |
BUT the problem is that we can not clinically differentiate between all these conditions
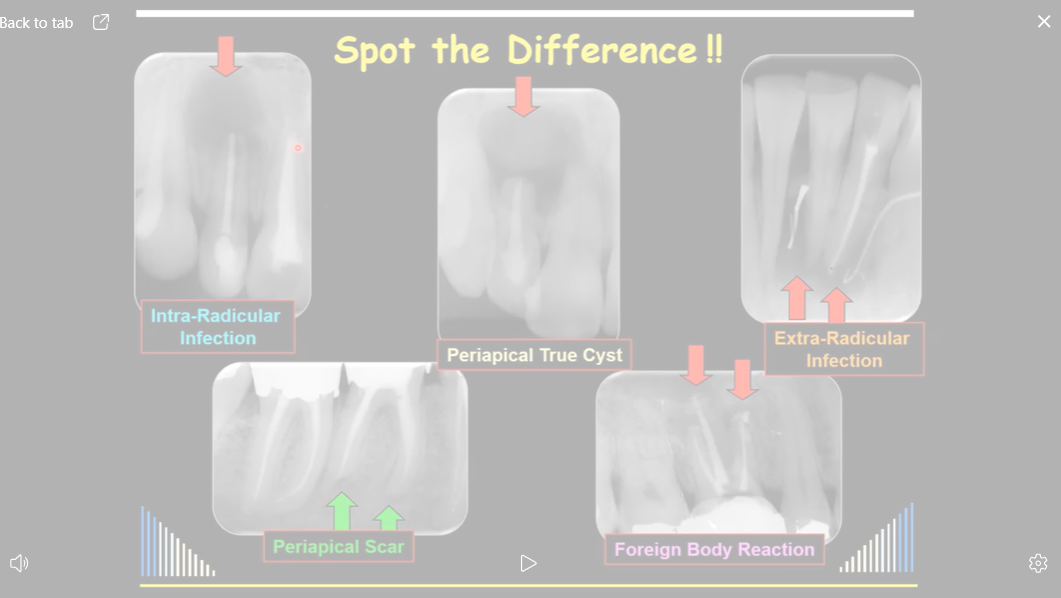
Spot the Difference!!29
Question
An exercise with five different radiographs demonstrated that it is often impossible to differentiate between these five causes based on radiographic appearance alone. While some clues may exist (e.g., extruded material suggesting a foreign body reaction, or draining sinuses suggesting extra-radicular infection), the presentation is often ambiguous.
How common are each of these?30
Incidence of Radicular Cysts
- theres a large variation of the number of cysts found Cysts: 6 - 55% Granuloma: 0 - 94% “Others”: 0 - 81%
Total: 18,026 lesions
Interpreting Historical Data
==Older biopsy studies reported a wide and often high incidence of cysts (6-55%). However, these studies were flawed because they did not use complete serial sectioning. The landmark work by Nair used meticulous serial sectioning and found that in his specific sample of 256 lesions, only 9% were true cysts and 6% were pocket cysts. 50% were abscesses and 35% were granulomas. It is crucial to note this is 9% of his specific sample, not 9% of all periapical lesions in the general population.==
Biopsy Reports – Various Studies3132
Notes on Studies:
Summary
The key takeaway from comparing various clinical biopsy studies is that the reported incidence of cysts and other conditions varies widely depending on the sample population and diagnostic criteria.
Implications for Treatment Outcome33
- BUT: even with high quality “intracanal treatment”, there will still be an upper limit to the number of favourable outcomes that can be achieved by conventional endodontic treatment. Largely determined by the incidence of:
- Residual intracanal bacteria → 35 - 83 %
- Extra-radicular infection → 2 %
- Peri-radicular true cysts → 9 %
- Foreign body reactions → 20 - 25 %
- Periapical scars → 1 - 3 %
Clinical Takeaway
==The relatively low incidence of true cysts and extra-radicular infections means that the vast majority of periapical radiolucencies are caused by intra-radicular infections (granulomas or abscesses) and are therefore treatable with non-surgical root canal retreatment.==
Biopsy studies - limited value - only the % of the biopsies examined, not the % in all patients
Specialist Endodontic Practice Service Mix - Surgical Cases
- 1986 - 1990
- 10.6% of all cases treated
- 1995 - 1999
- 1% of cases
- 2005 - 2010
- 0.1% of cases
Info
This reflects a better understanding in the profession that most cases can and should be managed non-surgically first.
Management Guidelines for Persistent Radiolucencies34
- The causes of persistent radiolucencies often include an infected root canal system, which is frequently the primary problem.
- Intra-Radicular Infection
- Extra-Radicular Infection
- Foreign Body Reaction
- Periapical True Cyst
- Periapical Scar
Info
==Intra-radicular Infection (bacteria inside the canal system) is the most common cause. The management depends entirely on the diagnosis, but all five conditions can appear as a radiolucency on an x-ray.==
- Ideally: do endodontic re-treatment first since most periapical radiolucencies are caused by, or are associated with, intra-radicular bacteria.
- Then the treatment will be more predictable and the rate of favourable outcomes will be higher. → Since the cause of the radiolucency is addressed
- **If still no healing, consider periapical surgery.
Fundamental Principle
==The fundamental principle is to retreat the root canal system first. Surgery is only considered if non-surgical retreatment fails to lead to healing.==
**
- If re-treatment before surgery: 24% higher rate of healing than when surgery done alone (Grung et al - 1990)
Differential Diagnoses for Periapical Radiolucencies on Root-Filled Teeth35
- A lesion that mimics a periapical radiolucency but is not endodontic in origin.
- A persistent radiolucency on a recently root-filled tooth (< 5 years ago) due to one of the following:
- An intra-radicular infection
- An extra-radicular infection
- A foreign body reaction
- A periapical true cyst, or
- A periapical scar
- A new radiolucency due to:
- Any of the above presenting as a new lesion on a tooth that had the RCF done > 5 years ago.
1. Non-Endodontic Origin36
A lesion that mimics a periapical radiolucency but is not endodontic in origin.
Info
Examples include a lateral periodontal cyst, benign or malignant tumor, or an anatomical variation. If the tooth tests vital and there is no other evidence of an endodontic problem, the patient should be referred to the appropriate specialist (e.g., oral surgeon) for diagnosis and management.
flowchart TD A[Root-filled Tooth with a Periapical Radiolucency] --> B[Non-Endodontic Origin] B --> C[See Table] C --> D[Refer patient to appropriate dental and/or medical specialist] D --> E[Review to confirm diagnosis and to ensure healing with no dental problems]
2. Persistent Radiolucency (< 5 years post-RCF)37
A persistent radiolucency on a recently root-filled tooth (< 5 years ago) due to: A. An intra-radicular infection B. An extra-radicular infection C. A foreign body reaction D. A periapical true cyst, or E. A periapical scar
Info
==Since the most likely cause is an intra-radicular infection, the primary management is non-surgical retreatment.==
3. New Radiolucency (> 5 years post-RCF)38
A new radiolucency on a tooth that had the RCF done > 5 years ago, due to:
- A. Apical Periodontitis → 2º Acute Apical Periodontitis → Chronic Apical Periodontitis → Foreign Body reaction
- B. Infection → 2º Acute Apical Abscess → Chronic Apical Abscess → Extra-Radicular Infection
- C. Periapical Cyst → Pocket Cyst → True Cyst
- D. Periapical Scar
Most common + due to an infected root canal system
Info
==This represents a new disease due to reinfection, almost always from a failing coronal restoration. The management is the same as for a primary infection: non-surgical retreatment.==
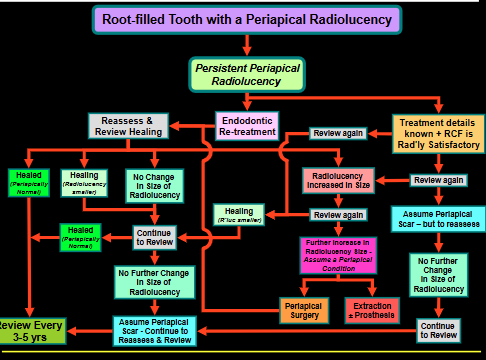
graph TD A[Root-filled Tooth with a Periapical Radiolucency] --> B[Healed Periapically Normal] A --> C[No Change in Size of Radiolucency] A --> D[Radiolucency Increased in Size] B --> E[Review Every 3-5 yrs] C --> F[Assume Periapical Scar - Continue to Reassess & Review] D --> G[Further Increase in Radiolucency Size - Assume a Periapical Condition] G --> H[Continue to Review] D --> I[Endodontic Re-treatment] D --> J[Periapical Surgery] D --> K[Extraction ± Prosthesis] I --> L[No Further Change in Size of Radiolucency] L --> M[Continue to Review] I --> N[Healing Radiolucency smaller] N --> O[Reassess & Review Healing] I --> P[Healed Periapically Normal] P --> Q[Review Every 3-5 yrs]
SUMMARY39
- Do endodontic re-treatment first !!!
Managing Persistent Radiolucencies
A systematic, review-based approach should be followed:
- ==Perform non-surgical retreatment.==
- ==Review at 6 months.==
- ==Assess the outcome: - Healed: Place the patient on a long-term (3-5 year) recall schedule. - Smaller / Unchanged: Continue to review annually. If the lesion stabilizes but does not fully resolve, it may be a periapical scar, which only requires monitoring. - Larger: If the lesion has increased in size, review again in 6 months. If it continues to enlarge, this suggests a true cyst, extra-radicular infection, or foreign body reaction. At this point, periapical surgery or extraction should be considered.==
- Ideally: do endodontic re-treatment first since most periapical radiolucencies are caused by, or are associated with, intra-radicular bacteria.
- Therefore the rate of favourable outcomes will be higher.
- As shown by Grung et al (1990):
→ If re-treatment before surgery
- 24% higher rate of healing than when surgery was done alone
Case Examples: Conservative Treatment of Large Periapical Lesions40
Example
These cases debunk the common misconception that large, well-defined lesions are always cysts that require surgery. The size and border of a lesion are not reliable predictors of its histology.
-
Case studies demonstrate that large periapical lesions can heal with conservative endodontic re-treatment.
-
One case showed healing one year after re-treatment with GP + AH26.
-
Another case showed healing one year after re-treatment. Courtesy Dr Geoff Heithersay – Adelaide
-
A further case showed healing after using Calcium Hydroxide for 13 months before final root filling. Courtesy Dr Geoff Heithersay – Adelaide
-
Another case showed healing over a 2-year period using MTA in the apical half and GP/sealer in the coronal half. Courtesy Dr George Bogen – Calif, USA
Management Options4142
- What are the options?
- No treatment
- Extraction
- Surgery
- Re-treatment
It depends on the DIAGNOSIS !!!
e-treatment first !!!**
Managing Persistent Radiolucencies
- Ideally: do endodontic re-treatment first since most periapical radiolucencies are caused by, or are associated with, intra-radicular bacteria
- Therefore the rate of favourable outcomes will be higher
- As shown by Grung et al (1990):
- If re-treatment before surgery
- 24% higher rate of healing than when surgery was done alone
- If re-treatment before surgery
Management Options42
It depends on the DIAGNOSIS !!!
- ==No Treatment / Monitor: Appropriate for a suspected periapical scar in an asymptomatic, functional tooth.==
- ==Extraction: If the tooth is non-restorable or the patient declines other options.==
- ==Periapical Surgery: Reserved for cases that do not heal after adequate non-surgical retreatment or where retreatment is not feasible.==
- ==Non-Surgical Retreatment: The primary and initial treatment of choice for the vast majority of cases, as they are caused by intra-radicular infection.==
Footnotes
-
Original PDF page 1: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.1 ↩
-
Original PDF page 2: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.2 ↩
-
Original PDF page 3: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.3 ↩
-
Original PDF page 4: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.4 ↩
-
Original PDF page 5: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.5 ↩
-
Original PDF page 6: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.6 ↩
-
Original PDF page 7: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.7 ↩
-
Original PDF page 8: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.8 ↩
-
Original PDF page 9: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.9 ↩
-
Original PDF page 10: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.10 ↩
-
Original PDF page 11: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.11 ↩
-
Original PDF page 12: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.12 ↩
-
Original PDF page 13: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.13 ↩
-
Original PDF page 14: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.14 ↩
-
Original PDF page 15: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.15 ↩
-
Original PDF page 16: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.16 ↩
-
Original PDF page 17: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.17 ↩
-
Original PDF page 18: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.18 ↩
-
Original PDF page 19: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.19 ↩
-
Original PDF page 20: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.20 ↩
-
Original PDF page 21: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.21 ↩
-
Original PDF page 22: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.22 ↩
-
Original PDF page 23: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.23 ↩
-
Original PDF page 24: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.24 ↩
-
Original PDF page 25: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.25 ↩
-
Original PDF page 26: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.26 ↩
-
Original PDF page 27: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.27 ↩
-
Original PDF page 28: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.28 ↩
-
Original PDF page 29: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.29 ↩
-
Original PDF page 30: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.30 ↩
-
Original PDF page 31: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.31 ↩
-
Original PDF page 32: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.32 ↩
-
Original PDF page 33: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.33 ↩
-
Original PDF page 34: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.34 ↩
-
Original PDF page 35: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.35 ↩
-
Original PDF page 36: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.36 ↩
-
Original PDF page 37: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.37 ↩
-
Original PDF page 38: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.38 ↩
-
Original PDF page 39: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.39 ↩
-
Original PDF page 40: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.40 ↩
-
Original PDF page 41: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.41 ↩
-
Original PDF page 42: O3 Treatment Outcomes, Persistent Radiolucencies, Options for Management, p.42 ↩ ↩2