Occlusion: Keys for Optimal Occlusion12
Occlusion3
Significance
Dental treatments inevitably affect the occlusion:
- Tooth restoration
- Tooth extraction
- Tooth movement
- Tooth adjustment
Post-Extraction Changes
Following an extraction, it is important to inform the patient that adjacent teeth may drift into the edentulous space and opposing teeth may supra-erupt. This explains the need for prosthetic replacements like bridges or dentures.
Many patients present with a form of occlusal problems:
- Tooth wear (attrition, erosion, abrasion, abfraction)
- Overloading
- Fractured cusp or restoration
- Cracked tooth Significance of occlusal problems
- Little evidence suggesting that a change in occlusion will precipitate morphological changes within TMJs
- The most likely adaptation occur in teeth and their supporting structures
For example: tooth wear, tooth movement and fracture
Pathological adaptations45
Attrition
Incisors wear
Info
Severe wear of the anterior teeth is often a result of a lack of posterior support, which concentrates forces on the front. This is exacerbated when combined with bruxism and erosion.
Possible causes:
- Lack of posterior tooth support
- Abrasive restorative material
- Bruxism
Generalized attrition6
- Severe wear, fractured teeth
- Dentoalveolar compensation: limits vertical space for dental restoration
Compensatory Mechanism
In cases of long-term grinding, a compensatory mechanism can occur where cementum and bone are deposited at the apex of the tooth socket. This leads to a gradual super-eruption of the teeth, maintaining the vertical dimension of occlusion (VDO) despite significant wear of the occlusal surfaces. Restoring these cases is complex because simply “opening the bite” is not an option, as the VDO is already correct. Treatment may require elective endodontics and crown lengthening to create space for restorations.
Splayed teeth7
Possible causes:
- Loss of posterior teeth combined with periodontal problems (reduced periodontal support)
- Over contouring of palatal surface of maxillary incisors or incisal/labial surfaces of mandibular incisors.
- anterior teeth will usually be sore before they move!
Sore teeth8
Overcompression of periodontal ligament can cause considerable pain on biting
Clinical Application
It is critical to perform a thorough occlusal adjustment after placing a restoration, especially while the patient is numb and cannot provide accurate feedback.
- ==Articulating Paper Interpretation: A heavy contact will often appear as a ring or perforation in the paper, not just a small dot. These heavy marks must be adjusted until the contacts are even across all teeth. Removing all marks would take the tooth out of occlusion.==
Causes:
- Premature occlusal contacts (occlusal overload)
- Occlusal interferences
Sensitive teeth9
Hypersensitivity might result from occlusal overload
Info
Occlusal overload can also lead to pulp hypersensitivity, causing the patient to experience sensitivity to temperature changes (e.g., cold). Before assuming a filling is leaking or has recurrent decay, the occlusion should always be checked and adjusted, as this can often resolve the symptoms.
Causes:
- restoration causing occlusal interferences
Hypermobility10
Pathological adaptation
Causes:
- Restoration causing occlusal interferences
- All mobile teeth should be assessed to rule out deflective contacts or occlusal overload as a factor in the cause of the mobility
Info
This is a mid- to long-term consequence of excessive occlusal stress, particularly from lateral interferences. The tooth becomes “wobbly” as a protective mechanism. Radiographically, a widening of the PDL space may be visible. Treatment involves a precise occlusal adjustment to eliminate interferences, often by establishing proper canine guidance.
Tooth cracks11
- Crack lines routinely develop when a cusp is loaded with heavy occlusal forces
Warning
Cracked tooth syndrome often presents as sharp pain specifically on biting down. It is essential to investigate the cause (e.g., occlusal overload, failing restoration) and consider preventative treatment, such as a crown or onlay, to protect the tooth from fracturing.
- Can precedes tooth fracture
Cracked tooth syndrome
Prosthetic Reconstruction
Many patients require prosthetic treatment due to conditions like:
- ==Occlusal Overload: Lack of posterior support can put excessive stress on remaining teeth, leading to abfractions, cusp fractures, and cracked tooth syndrome.==
Painful musculature12
Cause:
- Deflective occlusal interferences that cause jaw joints to displace
- Unbalanced muscle contraction
Mechanism
The brain subconsciously directs the mandible to shift away from the interference, creating a new habitual bite position. This results in an imbalanced contraction of the masticatory muscles, which over time causes soreness and fatigue. Treatment involves correcting the occlusion, sometimes after deprogramming the muscles with an occlusal splint.
Masticatory system13
Components
- Teeth
- Periodontal tissues
- Articulatory apparatus
Function of each component14
- TMJs: guiding system
- Dental occlusion: guiding system
- Masticatory muscle: moving system
TMJ15
Movements16
-
Hinge movement:
- Rotation around the intra-condylar axis
- Within the glenoid fossa
- < 2 cm of movement
-
Translation movement:
- Gliding against articular eminence
-
2 cm
Bilaminar Zone
This is a highly vascular and innervated area posterior to the condyle. In a healthy joint, it is not compressed. In cases of anterior disc displacement, the condyle can compress this zone, causing pain.
Movement directions17
- Protrusive movement
- Both condyles are in similar gliding motion
- Lateral movement
- Working side: rotational movement around the vertical axis without leaving the glenoid fossa
- Non-working side: gliding movement against the articular eminence
Excursive movements18
- During a lateral excursion of the mandible, the major movement within the TMJs occurs on the non-working side:
- The head of the condyle on the nonworking side moves forward, downward and medially
- The angle of downwards movement is established by the ‘condylar angle’
- The angle of medial movement is known as the ‘Bennet angle’
Condylar guidance19
Info
The downward path of the condyle during protrusive and lateral movements is dictated by the steepness of the articular eminence. On a semi-adjustable articulator, this is typically set to an average of 30 degrees. A steeper condylar guidance results in more immediate disocclusion (separation) of the posterior teeth during movement.
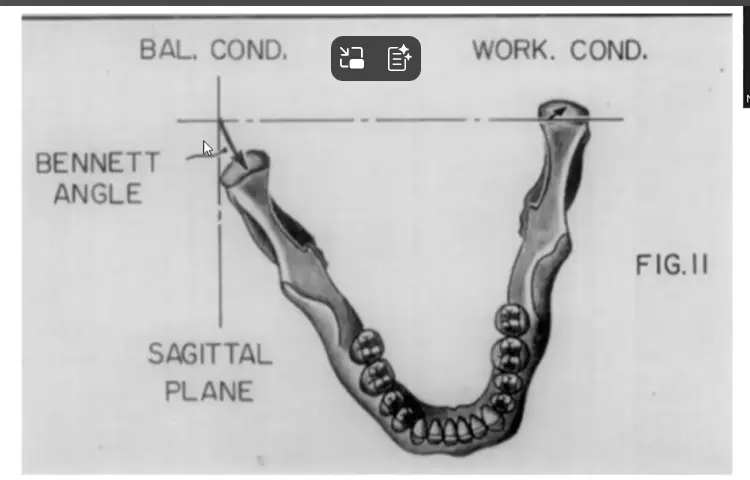
Bennett angle2021
Bennett angle: formed between the sagittal plane and the average path of the advancing non-working side condyle as viewed in horizontal plane during lateral mandibular movement.
- the first line is simply a line perpendicular to the coronal plane of the mandible (i.e. a straight line along the long axis)
- The second line is a line drawn through the midpoints of the condylar head before and after movement this
- the angle between those two lines causes the bennett angle
-  -
-
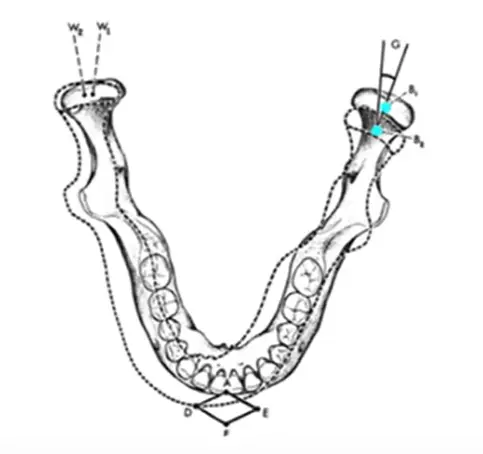 Bennett movement = LATEROTRUSION
Bennett movement = LATEROTRUSION
- in the below the bennet movement is the difference between w1 and w2
Bennett angle
- the Average bennett angle is 15 degrees
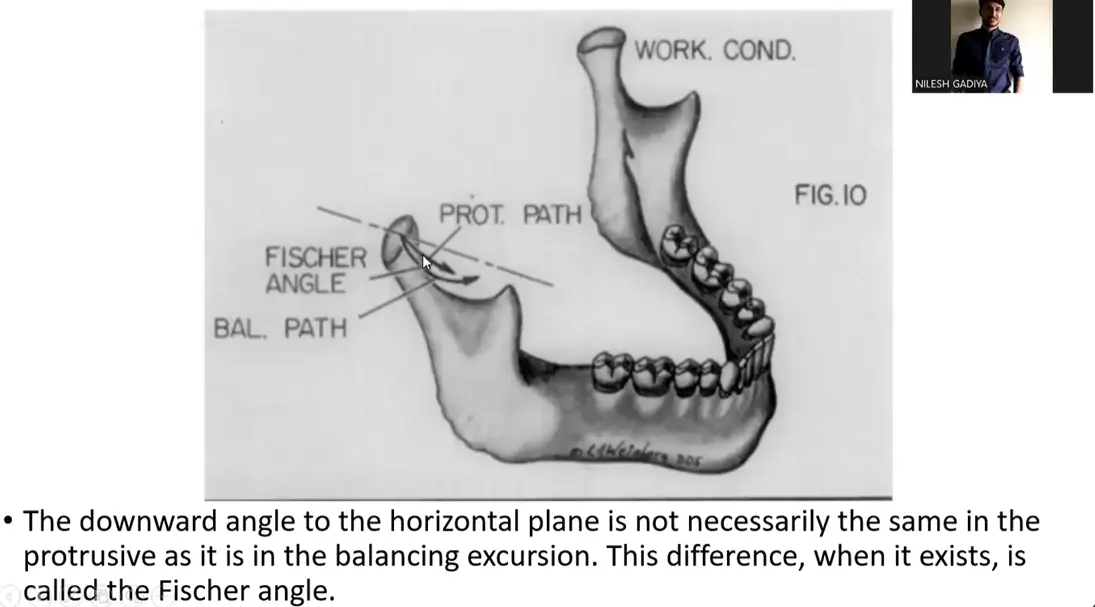
Note on Fischer Angle
The same movement of the non-working condyle, when viewed from the sagittal plane, creates the Fischer angle). This angle exists because the roof of the glenoid fossa is concave both antero-posteriorly and medio-laterally.
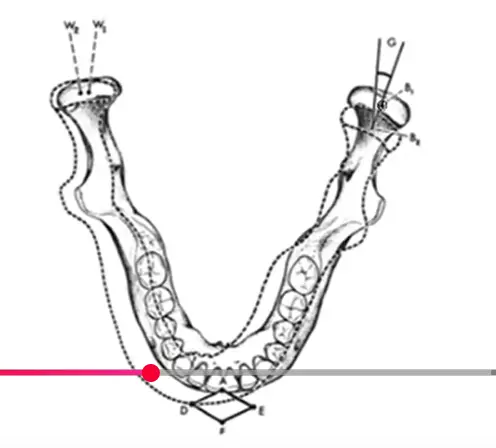
Bennett side shift22
Bennett side shift (mandibular lateral translation): the medio-lateral movement of the mandible when viewed in the frontal plane during Bennett movement
Info
The movement on the working side is not pure rotation. The entire mandible also shifts laterally towards the working side. This bodily side-shift is called the[ Bennett side shift](Immediate and Progressive Side Shift| Bennet Movement - YouTube) or lateral translation.
- immediate Bennett side shift : rapid, straight medial movement of the non-working condyle that occurs at the very start of lateral jaw movement
- progressive Bennett side shift is a gradual angled movement that happens after the initial shift
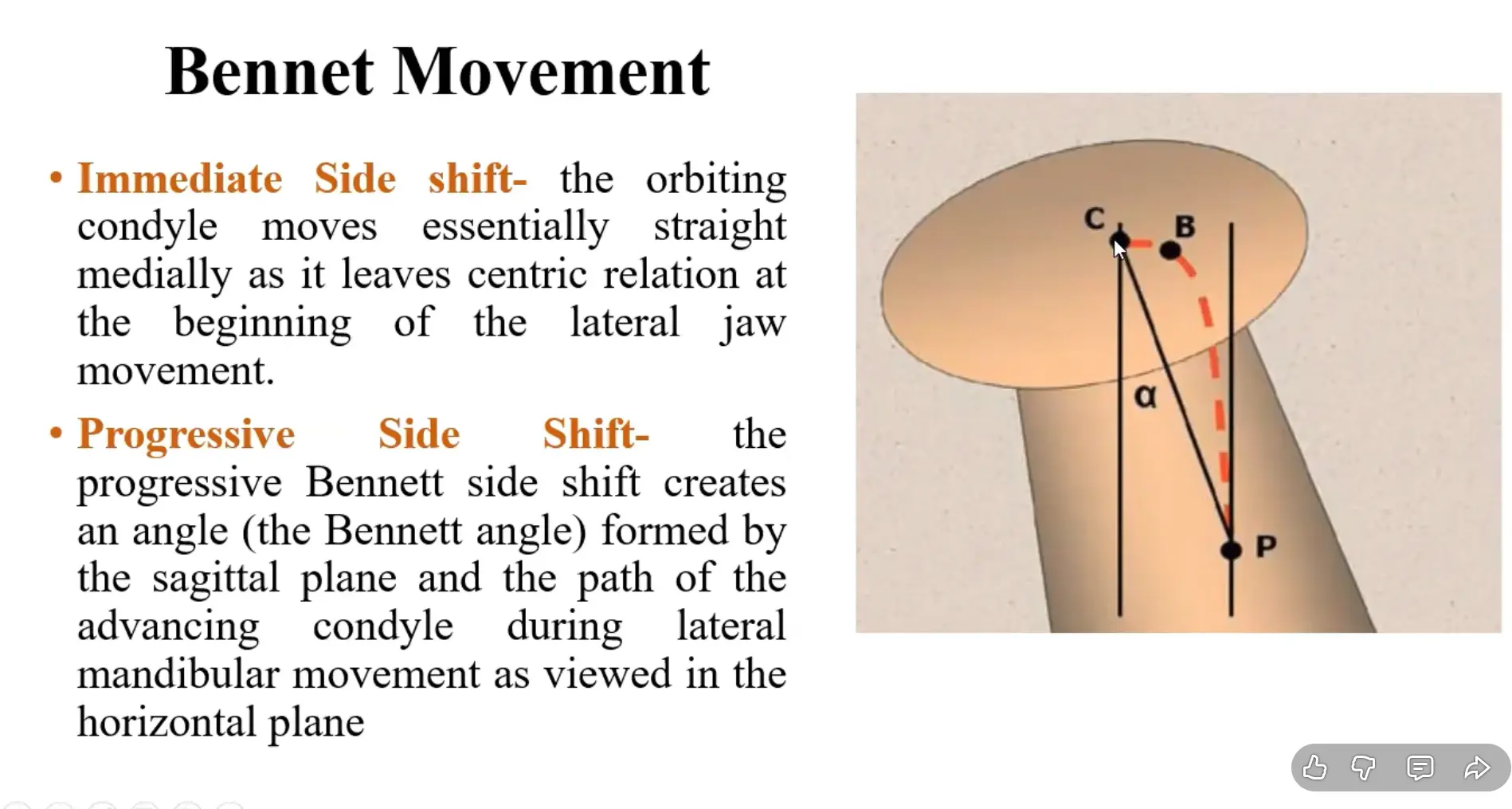
NOTE
- C-B is immediate bennett side shift
- B-P is the progressive side shift
Dental occlusion2324
Provided by whichever teeth touching the opposing teeth or analogs
- Static occlusion
- Dynamic occlusion
Overview of occlusal concepts25
Static occlusion
- Maximal intercuspation
- Centric relation/Centric occlusion
- Freedom in centric
- Extent of posterior tooth support
- Overbite and overjet
Dynamic occlusion
- Protrusion
- Lateral occlusion guidance
- Canine guidance
- Group function
- Balanced occlusion (complete dentures)
- Working and non-working sides interferences
Static occlusion26
Centric relation
A maxillomandibular relationship in which the condyles articulate in the anterior-superior position against the posterior slopes of the articular eminences.
- This position is independent of tooth contact
- centric relation is highly reproducible
Clinical Significance
It is the primary reference point for mounting casts and fabricating prostheses for edentulous patients, as they lack a repeatable tooth-guided position.
Maximum intercuspal position (MIP)27
The complete intercuspation of the opposing teeth independent of condylar position
- Bite of convenience
- Habitual bite (position)
Info
It is the most stable position for a dentate patient.
Centric occlusion
The occlusion of opposing teeth when the mandible is in centric relation
- In 90% of population MIP ≠ CO
Info
There is typically a small anterior-posterior slide from the initial contact in CO to the full bite in MIP.
Freedom in centric28
Freedom in centric occlusion occurs when the mandible is able to move anteriorly for a short distance in the same horizontal and sagittal plane while maintaining tooth contact.
There is a flat region in the central fossa where opposing cusps contact that gives to the mandible freedom in eccentric movements (no interference).
Tip
Restorations should be designed to allow for this freedom to avoid occlusal stress.
Dynamic occlusion29
Refers to occlusal contacts that are made whilst the mandible is moving relative to the maxilla.
- The mandible is moved by the muscles of mastication
- The pathways along which its moves are determined by two guidance systems (TMJ and dental occlusion)
Anterior Guidance
The contact of the lower incisors against the palatal surfaces of the upper incisors during protrusive and lateral movements.
Relationship to Condylar Guidance: A steep anterior guidance can compensate for a flat condylar guidance by creating more separation (disocclusion) of the posterior teeth during movement. This is a key principle in denture construction but is less modifiable in fixed prosthodontics.
- As the head of the condyle moves downwards and forwards, the mandible moves along a guidance pathway which is determined by the intraarticular disc and the articulatory surfaces of the glenoid fossa;
- If teeth are touching during a protrusive or lateral movement of the mandible then those (touching) teeth are also providing guidance to mandibular movement;
- Tooth contacts dictate the mandibular movement in occlusion.
Criteria for optimal occlusion3031
1) Mandibular stability: contact of inferior and superior teeth must stabilize the mandible in centric
- Condyles are positioned within the glenoid cavity without stretching or compressing the ligament or articular disc
- Bilateral and simultaneous occlusal contacts in centric (CR/MIP)
2) Axial load: The occlusal load should be parallel to the long axis of the tooth
- Load is distributed equally throughout the periodontal ligament
3) During lateral excursions of the mandible, there is no interference on the working side
Types of guidance3233
- Canine guidance - dentate
- Group function (total or partial) – dentate
- Balanced occlusion (bilaterally balanced occlusion) – edentate
Lateral occlusion guidance34
Canine guided (protected) occlusion
- A form of articulation in which the vertical and horizontal overlap of canine teeth disengage posterior teeth in excursive movements of the mandible
- Complete disocclusion of posterior teeth during lateral movement
Advantages
The canine is structurally suited to withstand heavy lateral forces. This scheme is considered ideal for the natural dentition and is simpler to achieve in restorative dentistry.
- Most widely accepted concept in restorative dentistry
- Easier to reproduce
- Canines are ideal guiding teeth
Canine guided Occlusion is Not indicated if the canines are compromised:
- Periodontally
- Endodontically
Group function occlusion (unilaterally balanced occlusion)3536
- Distribution of lateral forces to a group of teeth
- Multiple contacts between the maxillary and mandibular teeth in lateral movements on the working side whereby simultaneous contact of several teeth acts as a group to distribute occlusal forces
- On lateral movements, the contacts are on the buccal cusps of the working side
Distinction from Interference
True group function involves a smooth, sequential contact of multiple teeth. If only the canine and a single posterior tooth (e.g., a second molar) are in contact, the molar contact is considered an interference, not group function.
- Non-working (balancing) side - no contacts
- Widely accepted
- May cause excessive load on posterior teeth
- Difficult to establish
in group function occlusion, During lateral excursions of the mandible, there is disocclusion in the non-working side**
Interferences373839
Types of Interferences
- ==Working Side Interference: A posterior contact on the working side that prevents the desired canine guidance or disrupts a smooth group function.==
- ==Non-Working Side (Balancing) Interference: Any tooth contact on the non-working side. These are particularly destructive as they place oblique, harmful forces on the teeth.==
- ==Protrusive Interference: A posterior tooth contact during a forward movement of the mandible.==
- Can be observed clinically
- Increase patient awareness of the restoration
- Excessive horizontal and oblique forces will be applied on the restoration or natural teeth
Lateral occlusion guidance34
Balanced occlusion (bilaterally balanced occlusion)40
- Bilateral, simultaneous, anterior and posterior occlusal contact of teeth in centric and eccentric positions
- At least 3 contact points: 2 posterior and 1 anterior
Purpose
The bilateral contacts provide stability to the denture bases, preventing them from tipping or losing suction during function. This scheme is destructive to natural teeth and should not be created in a dentate patient.
- Useful for complete denture cases to prevent tipping of the denture
- Cross arch balanced occlusion is not indicated for natural dentition
REASONS:
- Excessive wear was observed
- Presence of balancing contacts can apply horizontal and oblique destructive forces on posterior teeth
- Destructive effects on the non working side
Protrusive or Anterior guidance
Mutually protected articulation4142
- An occlusal scheme in which the posterior teeth prevent excessive contact of the anterior teeth in MIP; and anterior teeth disengage the posterior teeth in all mandibular excursive movements
In simpler terms:
- ==In maximum intercuspation (MIP), the posterior teeth are in firm, even contact to absorb the heavy vertical forces of chewing, thus protecting the anterior teeth.==
- ==In all excursive movements (protrusive and lateral), the anterior teeth (incisors and canines) contact and guide the mandible, causing the posterior teeth to disocclude. This protects the posterior teeth from harmful off-axis (oblique) forces.==
Summary: Criteria for optimal occlusion434445
- Mandibular stability
- Axial occlusal load
- During lateral excursions: no interference in the working side
- During lateral excursions: disocclusion in the non-working side
- During protrusion: disocclusion of posterior teeth
Footnotes
-
Original PDF page 1: MR4 OptimalOcclusion, p.1 ↩
-
Original PDF page 2: MR4 OptimalOcclusion, p.2 ↩
-
Original PDF page 3: MR4 OptimalOcclusion, p.3 ↩
-
Original PDF page 4: MR4 OptimalOcclusion, p.4 ↩
-
Original PDF page 5: MR4 OptimalOcclusion, p.5 ↩
-
Original PDF page 6: MR4 OptimalOcclusion, p.6 ↩
-
Original PDF page 7: MR4 OptimalOcclusion, p.7 ↩
-
Original PDF page 8: MR4 OptimalOcclusion, p.8 ↩
-
Original PDF page 9: MR4 OptimalOcclusion, p.9 ↩
-
Original PDF page 10: MR4 OptimalOcclusion, p.10 ↩
-
Original PDF page 11: MR4 OptimalOcclusion, p.11 ↩
-
Original PDF page 12: MR4 OptimalOcclusion, p.12 ↩
-
Original PDF page 13: MR4 OptimalOcclusion, p.13 ↩
-
Original PDF page 14: MR4 OptimalOcclusion, p.14 ↩
-
Original PDF page 15: MR4 OptimalOcclusion, p.15 ↩
-
Original PDF page 16: MR4 OptimalOcclusion, p.16 ↩
-
Original PDF page 17: MR4 OptimalOcclusion, p.17 ↩
-
Original PDF page 18: MR4 OptimalOcclusion, p.18 ↩
-
Original PDF page 19: MR4 OptimalOcclusion, p.19 ↩
-
Original PDF page 20: MR4 OptimalOcclusion, p.20 ↩
-
Original PDF page 21: MR4 OptimalOcclusion, p.21 ↩
-
Original PDF page 22: MR4 OptimalOcclusion, p.22 ↩
-
Original PDF page 23: MR4 OptimalOcclusion, p.23 ↩
-
Original PDF page 24: MR4 OptimalOcclusion, p.24 ↩
-
Original PDF page 25: MR4 OptimalOcclusion, p.25 ↩
-
Original PDF page 26: MR4 OptimalOcclusion, p.26 ↩
-
Original PDF page 27: MR4 OptimalOcclusion, p.27 ↩
-
Original PDF page 28: MR4 OptimalOcclusion, p.28 ↩
-
Original PDF page 29: MR4 OptimalOcclusion, p.29 ↩
-
Original PDF page 30: MR4 OptimalOcclusion, p.30 ↩
-
Original PDF page 31: MR4 OptimalOcclusion, p.31 ↩
-
Original PDF page 32: MR4 OptimalOcclusion, p.32 ↩
-
Original PDF page 33: MR4 OptimalOcclusion, p.33 ↩
-
Original PDF page 34: MR4 OptimalOcclusion, p.34 ↩ ↩2
-
Original PDF page 35: MR4 OptimalOcclusion, p.35 ↩
-
Original PDF page 36: MR4 OptimalOcclusion, p.36 ↩
-
Original PDF page 37: MR4 OptimalOcclusion, p.37 ↩
-
Original PDF page 38: MR4 OptimalOcclusion, p.38 ↩
-
Original PDF page 39: MR4 OptimalOcclusion, p.39 ↩
-
Original PDF page 41: MR4 OptimalOcclusion, p.41 ↩
-
Original PDF page 42: MR4 OptimalOcclusion, p.42 ↩
-
Original PDF page 43: MR4 OptimalOcclusion, p.43 ↩
-
Original PDF page 44: MR4 OptimalOcclusion, p.44 ↩
-
Original PDF page 45: MR4 OptimalOcclusion, p.45 ↩
-
Original PDF page 46: MR4 OptimalOcclusion, p.46 ↩