- Infection of the Teeth and Jaws July 11, 2025 4:56 PM
Oral Pathology module
Infections of Teeth and Jaws
Infections
- Microorganisms cause infectious diseases.
- Microorganisms:
- bacteria
- Viruses
- Fungi
- Prions
- Protozoa
- Helminthes
- arthropods.
- Not all microorganisms are pathogenic
- The most common infectious agents in the oral cavity are periodontal pathogens and cariogenic microorganisms.
Opportunistic Infection
- Opportunistic infection is caused by microorganisms that usually do not produce disease in a person with a healthy immune system. When the immune system is compromised in some way, and the host’s natural defenses against the pathogen are reduced or eliminated, these microorganisms may cause disease.
- Opportunistic infections are especially common in patients with immunosuppressive conditions such as AIDS. A classic example is Candida (a fungal infection), which often becomes opportunistic in patients who are immunocompromised or whose oral microflora has been altered by broad-spectrum antibiotic therapy. Antibiotics can decrease the immune system’s function to some degree and disrupt the microbial balance, allowing Candida to proliferate.
Types of Microorganisms
- Bacteria
- Cocci
- Bacilli
- Spirochetes
- Viruses
- Envelope proteins (for attaching to specific cell surfaces)
- Capsid
- Genetic material (DNA or RNA)
- Lipid envelope
- Fungi
- Fungal hyphae
- Fruiting body
- Spores
- Spore germination
Variables affecting outcome of exposure to infectious agent
| Organism | Host defenses | Local environment | Outcome |
|---|---|---|---|
| Quantity of exposure | Skin (physical barrier, fatty acids) | pH | |
| Virulence | Mucous membranes (enzymes) | Temperature | |
| Production of toxins | Respiratory tract (mucociliary clearance) | Wet or dry | |
| Enzymes | Gastrointestinal tract (acids, bile detergents, resident microflora) | Denture wearing | |
| Immune system | Recent antibiotic use |
- Integrity of Skin and Mucosa: A break in the epithelium, such as an ulcer, removes the physical barrier and predisposes the host to infection
- . - Saliva: Saliva provides a protective layer and contains antibodies that defend against microorganisms.
-
- pH: Changes in oral pH, often due to diet, can create an environment conducive to certain pathogens. For example, an acidic environment promotes dental caries.
-
- Temperature: Body temperature fluctuations, such as a fever during a systemic infection, can alter the oral environment and sometimes trigger oral pain.
-
- Moisture: Conditions like xerostomia (dry mouth) due to a lack of saliva increase susceptibility to fungal infections like Candida .
Pathways from Periodontal Oral Cavity to Pulmonary Infections
graph TD A["Periodontal oral cavity (10^9 bacteria/mm^3 dental plaque)"] --> B["Oral bacteria form biofilm on ventilation tubing and inoculate the respiratory tract"] B --> C1["Cytokines and enzymes transferred into lungs"] C1 --> D1["Local inflammation, colonization of pathogens, and lung infection"] D1 --> E1["Chronic obstructive pulmonary infections:\nInhalation pneumonia, Bacterial pneumonia"] B --> C2["Aspiration of oral pharyngeal bacteria"] C2 --> D2["Respiratory pathogens in tracheobronchial tract colonize the oral and pharyngeal tissues"] D2 --> B
Infections and inflammation in the mouth, particularly from periodontitis, have established links to systemic conditions.
- Mechanism: Bacteria in dental plaque secrete cytokines and enzymes that can enter the bloodstream and affect other parts of the body.
- Systemic Links:
- Diabetes: There is a bidirectional relationship. Poorly controlled diabetes can worsen periodontal health, and poor periodontal health can make it harder to control diabetes.
- Alzheimer’s Disease: Recent research has linked specific oral bacteria to Alzheimer’s disease, with researchers at Melbourne University developing a vaccine to target these species.
Oral dysbiosis and autoimmunity
https://www.frontiersin.org/articles/10.3389/fimmu.2020.591255/full
Clinical Signs and Symptoms of Infection
- Signs and symptoms of infection may be caused by the organism directly or by the host response to being infected.
- Infections may be localized, systemic, or disseminated.
- Localized infections tend to cause pain in a specific body part. For example, if a cut on the skin is infected with bacteria, pain will occur at the site of the infection. The lesion will show redness, swelling, heat, edema, possibly a foul odor, and some form of exudate, such as pus.
- Systemic and disseminated infections tend to show extreme fatigue, weight loss, low-grade or spiking fever, night sweats and chills, and generalized body aches.
Bacterial infections
Dental caries
- Prevalence: The most common disease in humans.
- Etiology: A multifactorial disease requiring four key elements:
- A susceptible host (dental hard tissue).
- Cariogenic microorganisms (bacteria).
- A suitable substrate (fermentable carbohydrates).
- Sufficient time.
- Pathology: Dental caries is associated with progressive tissue damage. Bacterial toxins dissolve minerals from the tooth structure (demineralization) and cause the subsequent collapse of the organic matrix. Carious dentin feels soft because it has lost its mineralization. In its later stages, when the organic matrix has collapsed, the lesion is irreversible and requires removal and restoration.
| Patient’s level risk factors | Intraoral level risk factors |
|---|---|
| Current hypo-salivation | Active caries lesions |
| Oral hygiene practices | PUFA |
| Sugary drinks & snacks | Thick plaque |
| Social-economical status | Appliances |
| Head & neck radiation | Dry mouth |
| Topical fluoride exposure | Caries experience |
| Dental attendance | Exposed root surfaces |
| Mothers’ caries experience |
Pulpitis
Causes of pulpitis
- Dental caries
- Traumatic exposure of the pulp
- Fracture of a crown or cusp
- Cracked tooth
- Thermal or chemical irritation
Types of pulpitis
- Acute closed pulpitis
- Chronic closed pulpitis
- Open pulpitis
- Chronic hyperplastic pulpitis
PERIAPICAL PERIODONTITIS, ABSCESS AND GRANULOMA
- Periapical inflammation is due to spread of infection, bacterial products or other irritants through the apex into the periodontal ligament following death of the pulp. The specific outcome---be it periodontitis, an abscess, or a granuloma---depends on the intensity and duration of the infection.
Causes of apical periodontitis
- Infection
- Trauma
- Chemical irritation
- The first step in inflmmatoin is the “call for neutrophils”, these then go on to release prostaglandins as the primary mediators for inflamattion
Sequelae of Pulpitis
graph TD Rare resolution / polyp (side note) A["Very rarely pulp remains viable and inflammation resolves. Only if pulp open to mouth and root apices open; resorption or incomplete. Pulp polyp forms"] B -. "rare/alternative" .-> A C -. "rare/alternative" .-> A Granuloma (central hub) D --> F["Periapical granuloma: chronic persistent inflammation, usually asymptomatic or with periods of exacerbation"] E --> F Infected cyst branch H --> J["Infected cyst caused by virulent organism from pulp or by communication with antrum, oral or nasal cavity"] Three branches from abscess I --> K["Drainage of pus (intraoral or extraoral) → symptoms reduce; leads to chronic persistent infection with periods of exacerbation unless treated"] I --> L["Acute soft tissue or fascial space infection: abscess, cellulitis, or combination"] I --> M["Inadequate or inappropriate antibiotic treatment → persistent infection"] %% Complications K --> N["Rare but severe complications of low-grade infection: infectious endocarditis; osteomyelitis"] L --> O["Rare but severe complications of virulent infection: Ludwig’s angina, cavernous sinus thrombosis, septicaemia; death"] M --> P["Rare but severe complications of virulent infection: Clostridium difficile infection, necrotising fasciitis, etc.; risk of death"]
- Acute Phase: The initial inflammatory response is dominated by neutrophils , which are the first cells to arrive at the site of injury. They release inflammatory mediators like prostaglandins .
- Chronic Phase: If the infection is not resolved, macrophages arrive after approximately 48 hours, marking the transition to a chronic inflammatory state.
Differential Diagnosis of Toothache pulpbiology endodontics
| Toothache or pain felt in teeth or alveolus | |||||||
|---|---|---|---|---|---|---|---|
| Pain of pulpal origin Sensitivity to sweet, hot or cold; poorly localised | Pain of periodontal ligament origin Pain on biting/pressure, usually well localised | Neurological or vascular pain | Neuralgic or psychogenic pain | ||||
| Dentine hypersensitivity | Pulpitis | Cracked tooth / cusp | Periapical periodontitis | Periodontal abscess | Sinusitis | ||
|
Reversible pulpitis
Irreversible pulpitis
|
|
|
|
|
|
|
Referral Process for Non-Odontogenic Pain 1. The first step is to rule out an odontogenic cause, as this is within the dentist’s scope. 2. If the cause is determined to be non-odontogenic, referral is necessary. In the Australian health system, patients are often referred to their General Practitioner (GP), who may then refer them to a medical or dental specialist (e.g., an oral and maxillofacial surgeon). 3. To save time, a dentist can refer a patient directly to a dental specialist while also copying the patient’s GP into the communication.
CHRONIC APICAL PERIODONTITIS AND PERIAPICAL GRANULOMA
- Chronic periapical granuloma is the most frequent outcome of necrotic pulp.
- Most develop without symptoms.
- They can also arise from acute apical periodontitis
- A periapical granuloma is caused by frustrated healing.
- The granuloma itself is sterile in almost all cases, but bacteria and irritants from necrotic tissue remain in the pulp chamber, inaccessible to the host response. A fistula (sinus tract) may form, creating a passage for pus to drain from the apex to the oral mucosa or skin.
- The tooth is non-vital and may be slightly tender to percussion; otherwise, symptoms may be minimal.
**Periapical granuloma
- A periapical granuloma is a typical focus of chronic inflammation characterised by lymphocytes, macrophages and plasma cells in loose edematous fibrous tissue.
Histologically, it is composed of[[Granulation Tissue| granulation tissue]] , which is primitive tissue characterized by:
- Numerous new, leaky blood vessels (proliferation of endothelial cells).
- A large number of chronic inflammatory cells ( lymphocytes, plasma cells, macrophages ).
- A scant amount of collagen fibers and fibroblasts. Due to its high vascularity, granulation tissue bleeds easily upon manipulation.
Possible outcomes of chronic apical periodontitis
- Periapical granuloma formation
- Radicular cyst formation
- Mechanism: Chronic inflammation stimulates the proliferation of the epithelial rests of Malassez , which are dormant epithelial cell remnants in the periodontal ligament.
- Cystogenesis: As these epithelial cells proliferate into a mass, the central cells move further from their blood supply in the surrounding connective tissue. This leads to central ischemia, necrosis, and liquefaction, forming a fluid-filled, epithelium-lined pathologic cavity---the cyst .
- Appearance: Radicular cysts typically appear as well-defined, circular radiolucencies on radiographs due to their consistent, slow growth pattern.
- Suppuration, sinus formation or spread
- Periodic acute exacerbations of inflammation of infection Spontaneous resolution does not occur.
Gingivitis and periodontitis periodontitis
Pathological processes in chronic periodontitis
- Chronic inflammation
- Destruction of periodontal ligament fibres
- Resorption of alveolar bone
- Migration of the epithelial attachment to the apex
- Formation of pockets around the teeth
- Formation of subgingival plaque and calculus
Acute pericoronitis
- Pericoronitis is a localized, intraoral soft tissue infection most commonly associated with erupting lower third molars.
- The microflora of pericoronitis is diverse and differs from pathogens that cause periodontitis.
- In a study of microbiota of pericoronitis, Actinomyces oris , Eikenella corrodens , Eubacterium nodatum , Fusobacterium nucleatum , Treponema denticola , and Eubacterium saburreum were present in high levels
- Usually is triggered by trauma from the opposing dentition A flap of mucosal tissue, the operculum , covers part of the occlusal surface. This flap can be traumatized by the opposing tooth and can trap food debris and plaque, leading to a bacterial infection, severe pain, and swelling.
Acute pericoronitis: Differential diagnosis
- Foreign body impaction
- Pyogenic granuloma
- Peripheral ossifying fibroma
- Dental caries
- Periodontitis
- Periapical abscess or granuloma
Gingival inflammatory swellings
- Orofacial granulomatosis
- Sarcoidosis
- Acute leukaemia
- Wegener’s granulomatosis
- Scurvy
Alveolar osteitis
Key features
- The most common painful complication of dental extractions
- Commonly known as dry socket
- Loss of clot normally filling extraction socket
- The blood clot is essential for protecting the underlying bone and facilitating healing.
- Loss of clot may be due to excessive local fibrinolytic action or bacterial enzymes or both
- Bare, whitish lamina dura exposed in socket.
- Pain relieved by irrigation and repeated dressing of socket
- Dead bone usually shed as crumblike fragments
- Eventual healing of socket from its base by granulation
- Alveolar osteitis develops more frequently after 1%—2% of extractions for lower-third molar extractions.
Predisposing factors for alveolar osteitis
- Excessive extraction trauma
- Limited local blood supply
- Gingival infection such as acute ulcerative gingivitis, pericoronitis or abscess
- Local anaesthesia with vasoconstrictor
- Smoking
- Oral contraceptives
- Osteosclerotic disease: Paget’s disease, cemento-osseous dysplasia
- Radiotherapy
- History of previous dry socket
ACUTE OSTEOMYELITIS
- In acute osteomyelitis bacteria and inflammation spread through the medullary bone from a focus of infection.
- The most common cause is spread of infection from a periapical infection.
- Adult males who have more dental infections than females are mostly affected.
- Almost all cases affect the mandible, which is less vascular than the maxilla.
- Early complaints are severe, throbbing, deep-seated pain and swelling with external swelling due to inflammatory edema. Later, distension of the periosteum with pus and, finally, subperiosteal bone formation cause the swelling to become firm. The overlying gingiva and mucosa is red, swollen and tender. Associated teeth are tender.
Important predisposing conditions for osteomyelitis
Local damage to or disease of the jaws
- Radiation damage
- Causes of osteosclerosis
- Paget’s disease
- Fibro-osseous lesions, particularly cemento-osseous dysplasia
- Osteopetrosis
Impaired immune defences
- Poorly controlled diabetes mellitus
- Sickle cell anaemia
- Chronic alcoholism or malnutrition
- Drug abuse
- Tobacco smoking
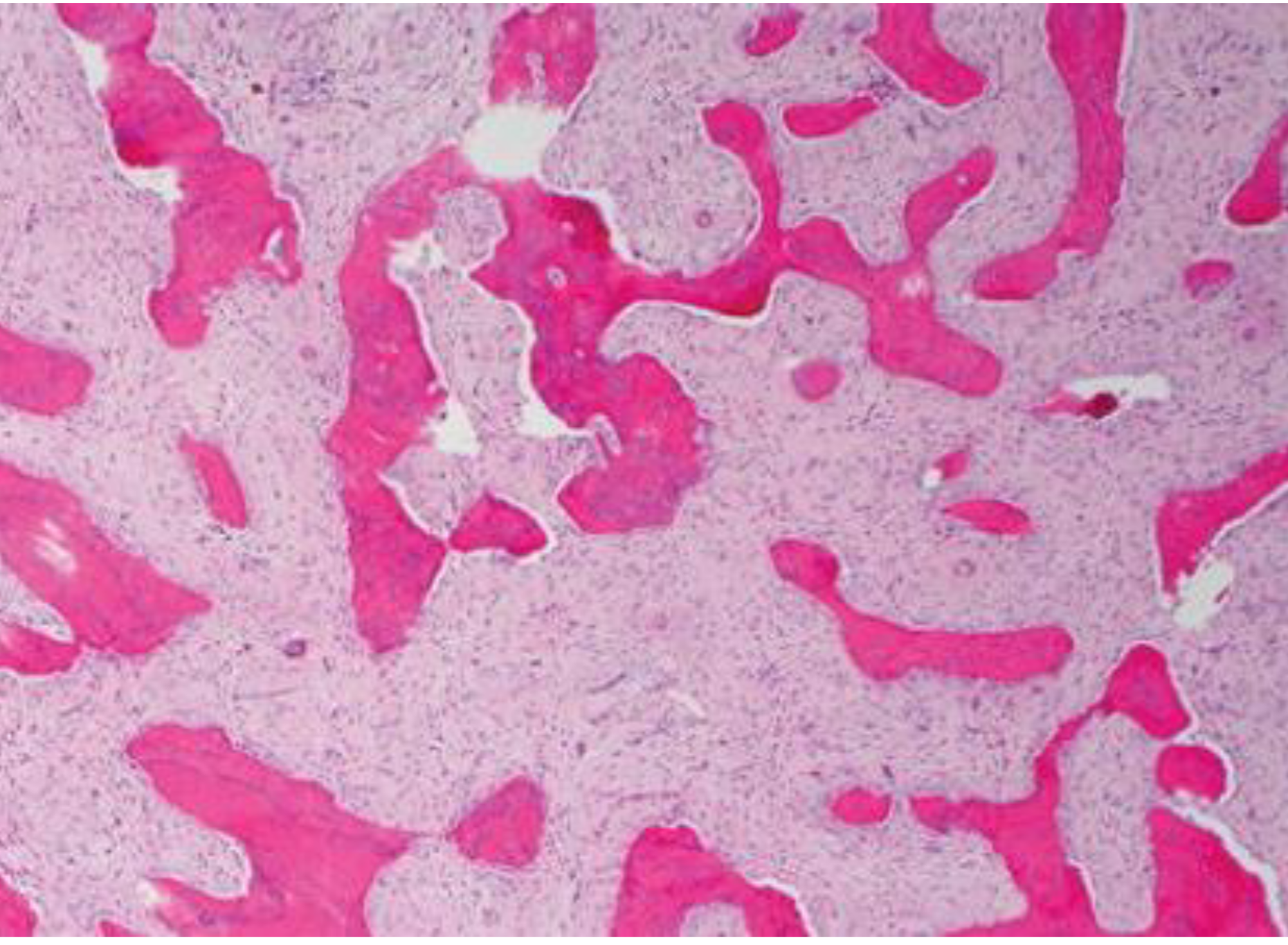
- Malignant neoplasms and their treatment Pathology - Sequestrum: The hallmark of osteomyelitis is the formation of a sequestrum , which is an island of non-vital (dead) bone that has become separated from the surrounding living bone. It is characterized by empty lacunae (loss of osteocytes) and a lack of osteoblasts on its surface.
- Inflammation: The surrounding area shows a mixed bacterial flora and a massive infiltration of neutrophils , characteristic of an acute infection.
- Suppuration (Pus Formation): The infection is often suppurative, meaning it produces pus. Pus is composed of liquefied necrotic tissue and dead inflammatory cells (mainly neutrophils). Pus accumulation can lead to further bone resorption and the formation of subcutaneous or submucosal abscesses.
Histological image of acute osteomyelitis showing inflammatory infiltration in bone tissue.

L3 Infections Teeth and Jaws, p.29
CHRONIC OSTEOMYELITIS
- More common than acute osteomyelitis and arises from infection by weakly virulent bacteria or in avascular bone.
- Most cases develop without a prior acute phase and only rarely does acute osteomyelitis lead to chronic osteomyelitis
Key features
- Mandible mainly affected
- Infection of dental origin
- Low-grade pain
- Associated with a persistent, low-grade, dull pain
- Sclerosis or avascular bone is often a predisposing factor
- Resistant to treatment
- Prolonged antibiotic treatment required
- Role for surgery to remove sequestra and sclerotic bone
L3 Infections Teeth and Jaws, p.31
Stages of Osteomyelitis
- Stage I (Medullary osteomyelitis)
- Necrosis limited to medullary contents and endosteal surfaces.
- Etiology: Hematogenous
- Treatment:
- Early: Antibiotics/host alteration
- Late: Unroofing, intramedullary reaming
- Stage II (Superficial osteomyelitis)
- Necrosis limited to exposed surfaces.
- Etiology: Contiguous soft tissue infection
- Treatment:
- Early: Antibiotics/host alteration
- Late: Superficial debridement/coverage
- Possible ablation
- Stage III (Localized osteomyelitis)
- Well marginated and stable before and after debridement.
- Etiology: Trauma, evolving stages I and II, Iatrogenic
- Treatment:
- Antibiotics/host alteration
- Debridement, dead space management
- Temporary stabilization, bone graft optional
- Stage IV (Diffuse osteomyelitis)
- Circumferential and/or permeative.
- Unstable prior to or after debridement
- Etiology: Trauma, evolving stages I, II, and III, Iatrogenic
- Treatment:
- Antibiotics/host alteration
- Stabilization - ORIF, external fixation (Ilizarov)
- Debridement, dead space management
- Possible ablation
DIFFUSE SCLEROSING OSTEOMYELITIS
L3 Infections Teeth and Jaws, p.33
Key features
- Affects adults
- No sex predilection
- Affects mandible almost exclusively
- Patchy diffuse sclerosis in the alveolar process
- Changes more marked around sites of periapical or periodontal chronic inflammation
- Persistent ache or pain but no swelling
- Radiographically resembles but is distinct from florid cemento-osseous dysplasia
Pathology
- Bone sclerosis and remodelling
- Scanty marrow spaces and little or no inflammatory infiltrate, although adjacent to areas of inflammation Clinical photographs and radiographic images of a dental case (frontal facial view, intraoral view, and radiographs).
Focal sclerosing osteomyelitis
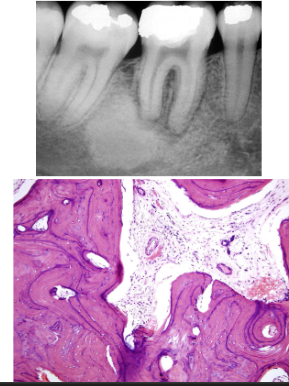
Key features
- Bony reaction to low-grade periapical infection
- Children and young adults affected
- Premolar or molar region of mandible affected
- Bone sclerosis associated with a non-vital tooth
- Localised but uniform radiodensity related to tooth with widened periodontal ligament space or periapical area
- No expansion of the jaw
Pathology
- Dense sclerotic bone with scanty connective tissue or inflammatory cells DIFFUSE SCLEROSING OSTEOMYELITIS