Oral Pathology module: Odontogenic and non-odontogenic cysts
Definition
A cyst is a pathological cavity filled with fluid, semi-fluid or gaseous contents and is not created by an accumulation of pus.
Aetiology and pathogenesis
- Epithelial proliferation
- Hydrostatic or osmotic factors
- Keratin formation
- Bone resorbing factors (prostaglandins, collagenase)
Clinical features
- Noticeable swelling
- Discharge into the mouth
- Pain due to secondary infection
Diagnosis
- Combination of adequate history, clinical examination and selected investigation (radiographs)
CLASSIFICATION: Cysts of the Jaws
- EPITHELIAL CYSTS
- Odontogenic
- Inflammatory
- Radicular (dental) cyst (periapical, lateral, residual)
- Paradental cyst
- Developmental
- Dentigerous cyst
- Eruption cyst
- Odontogenic keratocyst (primordial cyst)
- Gingival-infants
- Gingival-adults
- Lateral periodontal
- “Odontogenic cysts are lined by odontogenic epithelium derived from the dental lamina
- Inflammatory
- Non-odontogenic
- Nasopalatine duct cyst
- Nasolabial (naso-alveolar) cyst
- Odontogenic
- NON-EPITHELIAL CYSTS (Primary Bone Cysts)
- Solitary Bone Cyst
- Aneurysmal Bone Cyst
Inflammatory Odontogenic Cysts
RADICULAR CYSTS
Clinical Features
- 60-75% of all jaw cysts (Most Common)
- Peak in 4th and 5th decades
- Non-vital tooth
- Upper lateral incisor - most common tooth
- Rare in deciduous teeth
- Asymptomatic or expansion → springy → egg-shell crackling → fluctuation
- Infection → pain
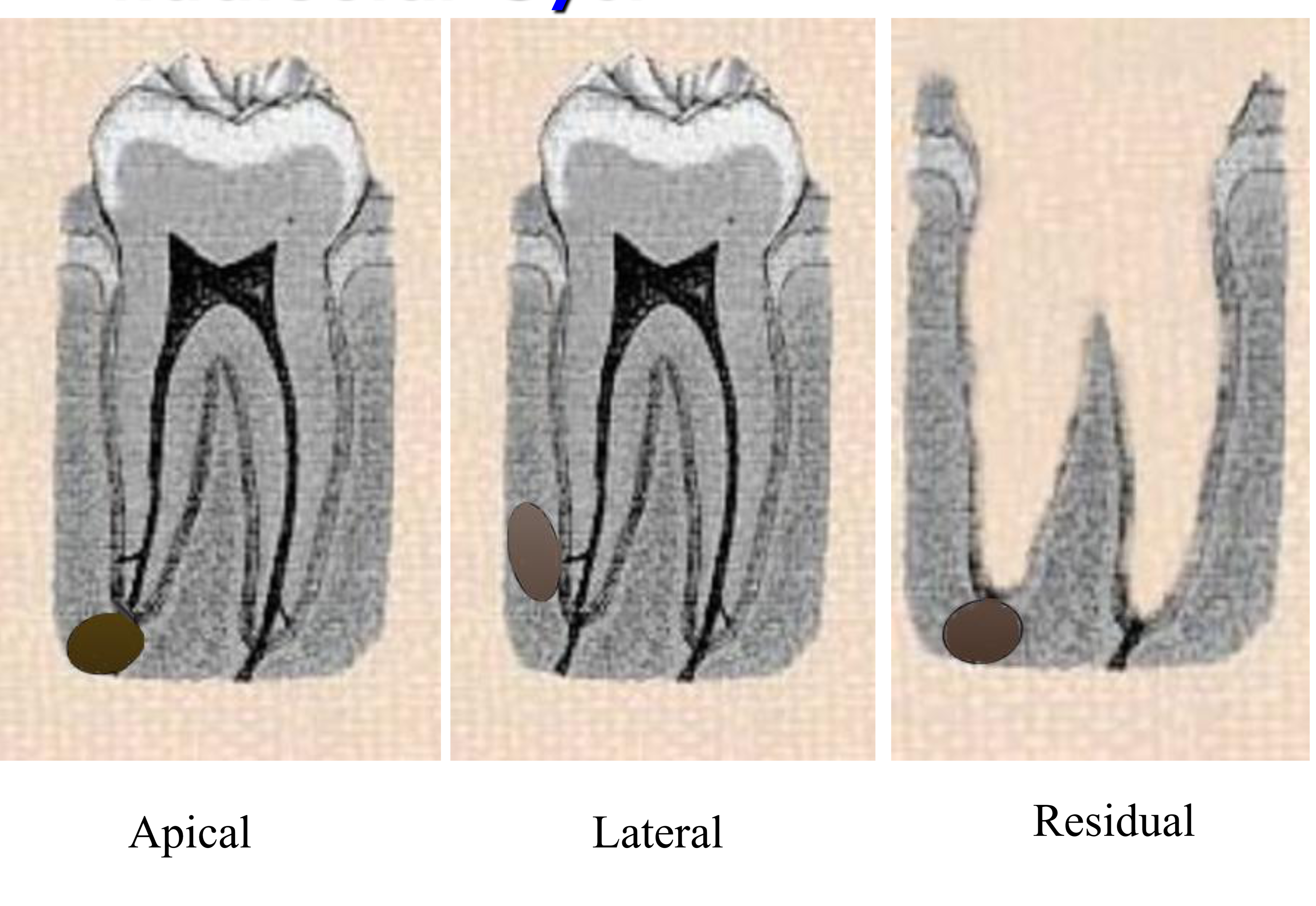
- Radicular Cyst can be:
- Apical
- Lateral
- Residual
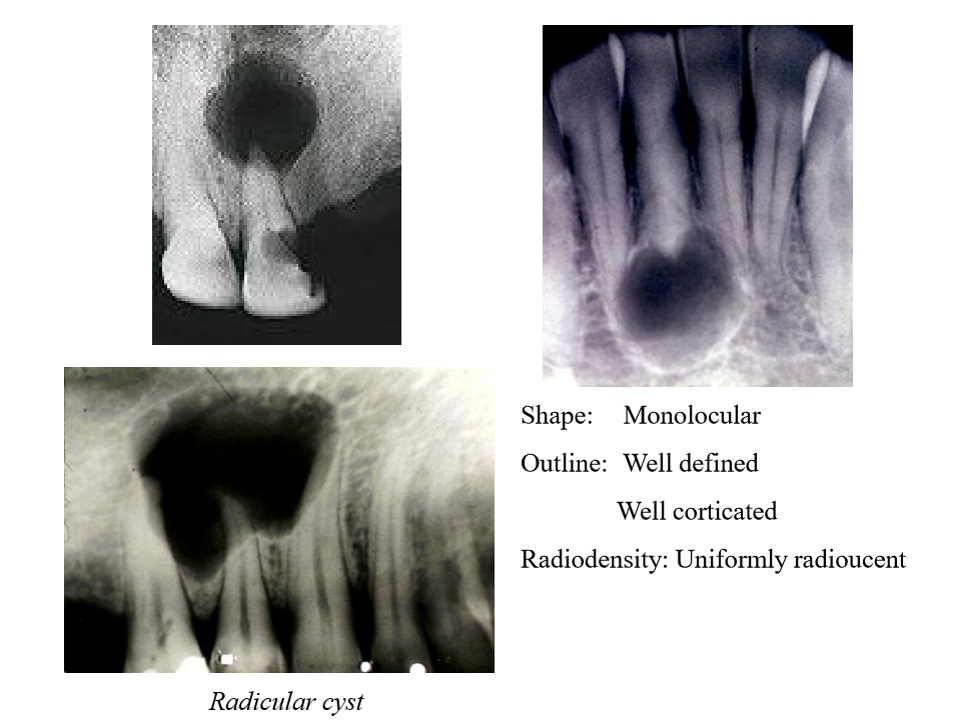
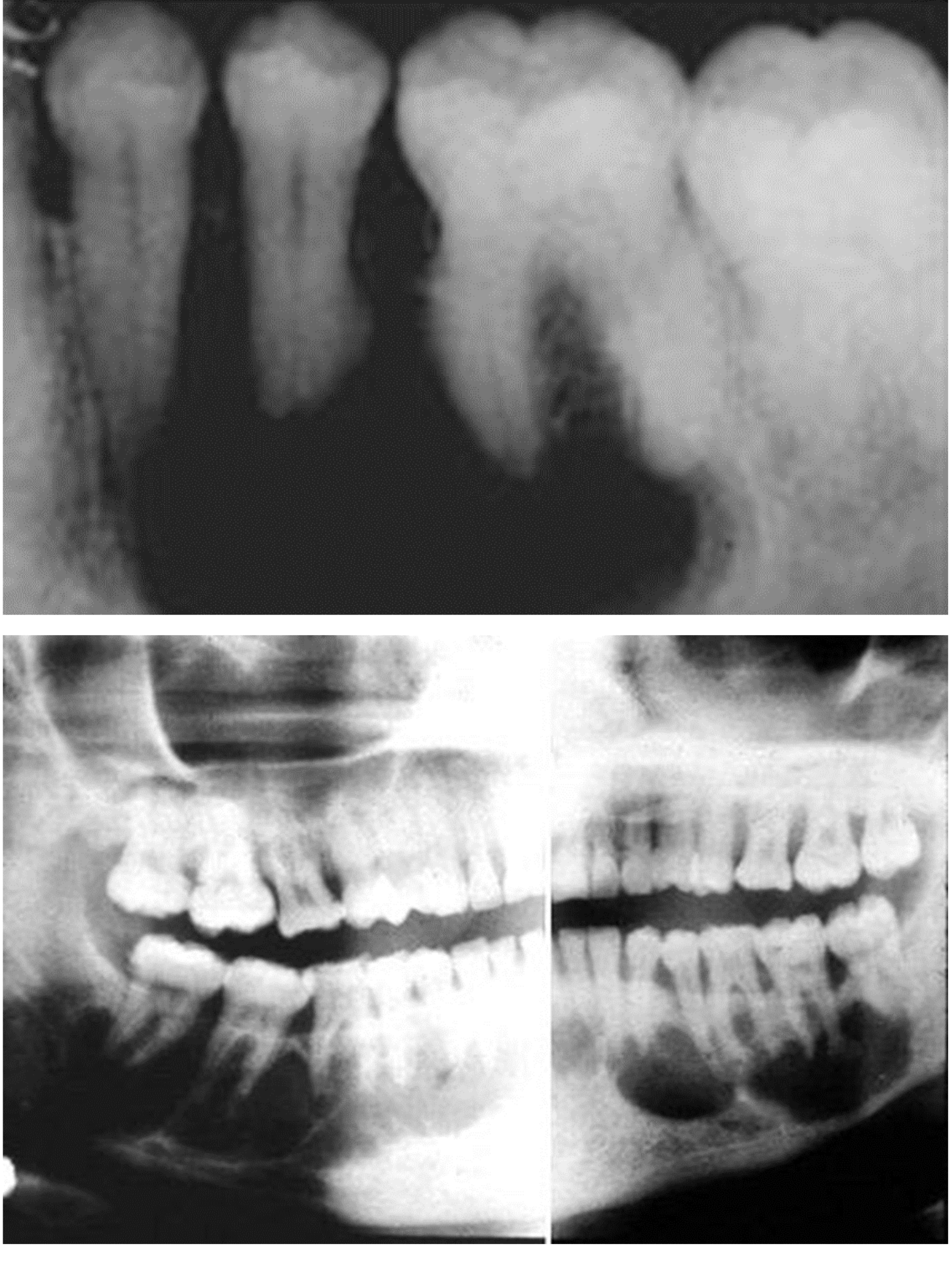
Radicular Cyst
**Radiographic Features
- Shape: Monolocular
- Outline: Well defined, Well corticated
- Radiodensity: Uniformly radiolucent
- Vitality : teeth usually become non-vital
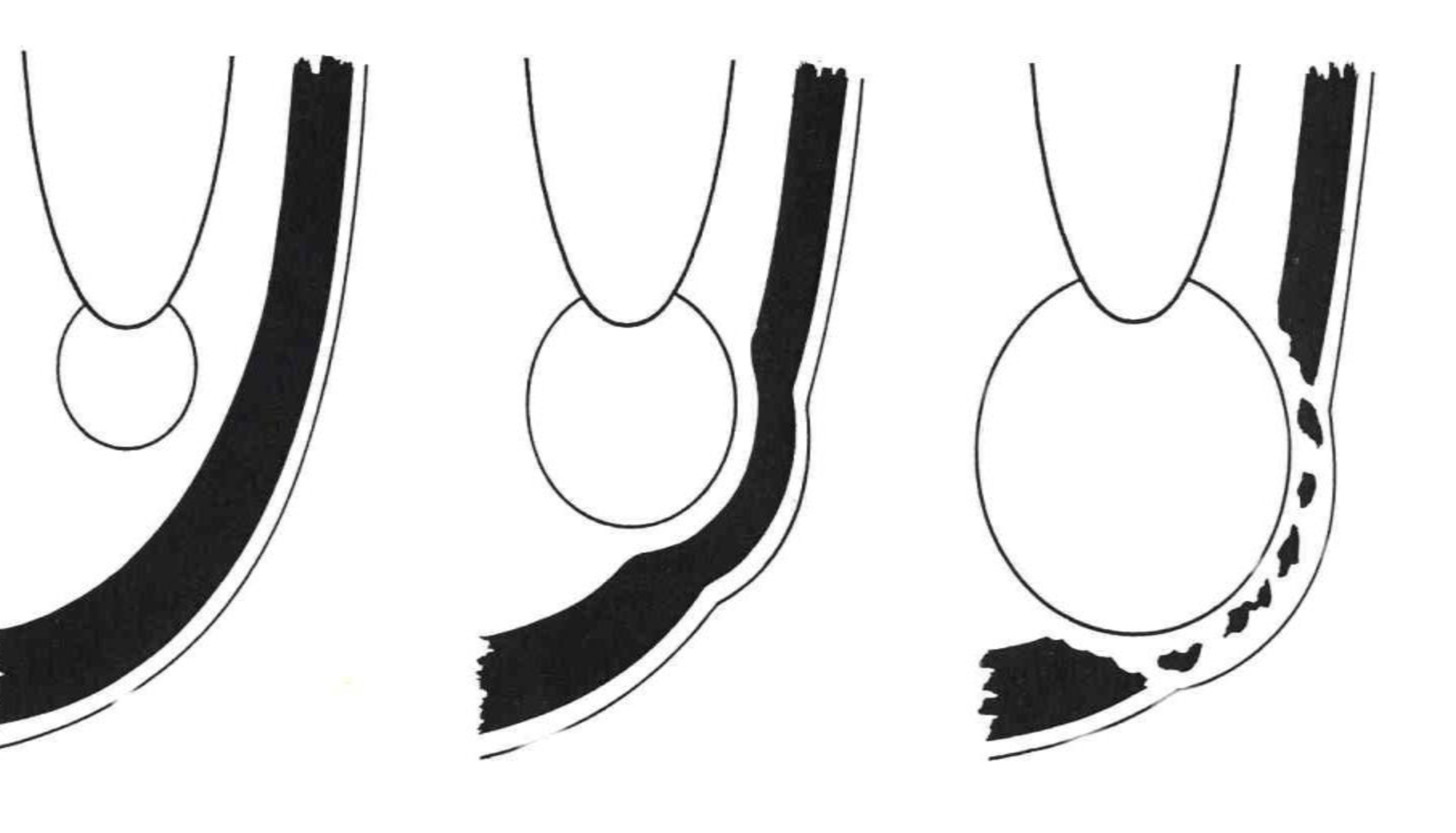
Pathogenesis
- **INITIATION
- Cell rest of Malassez activated
- Activated by products of necrotic pulp
- CYST FORMATION
- Degeneration and death of central cells leads to cavitation
- CYST ENLARGEMENT
- increased osmolality due to breakdown products becoming smaller and more osmotically active
- wall acts as semi-permeable membrane
Cysts Contents
- Breakdown products of cells
- Serum proteins
- Water and electrolytes
- Cholesterol crystals
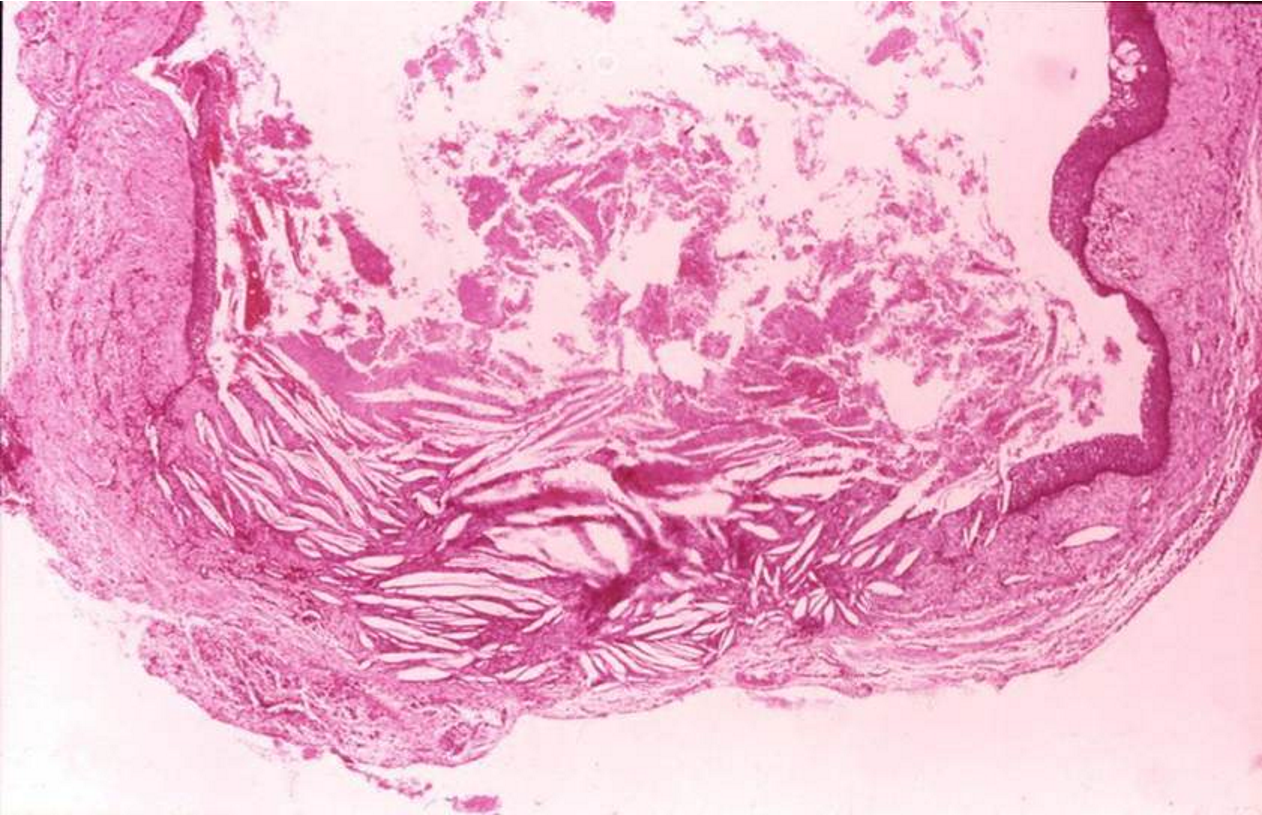
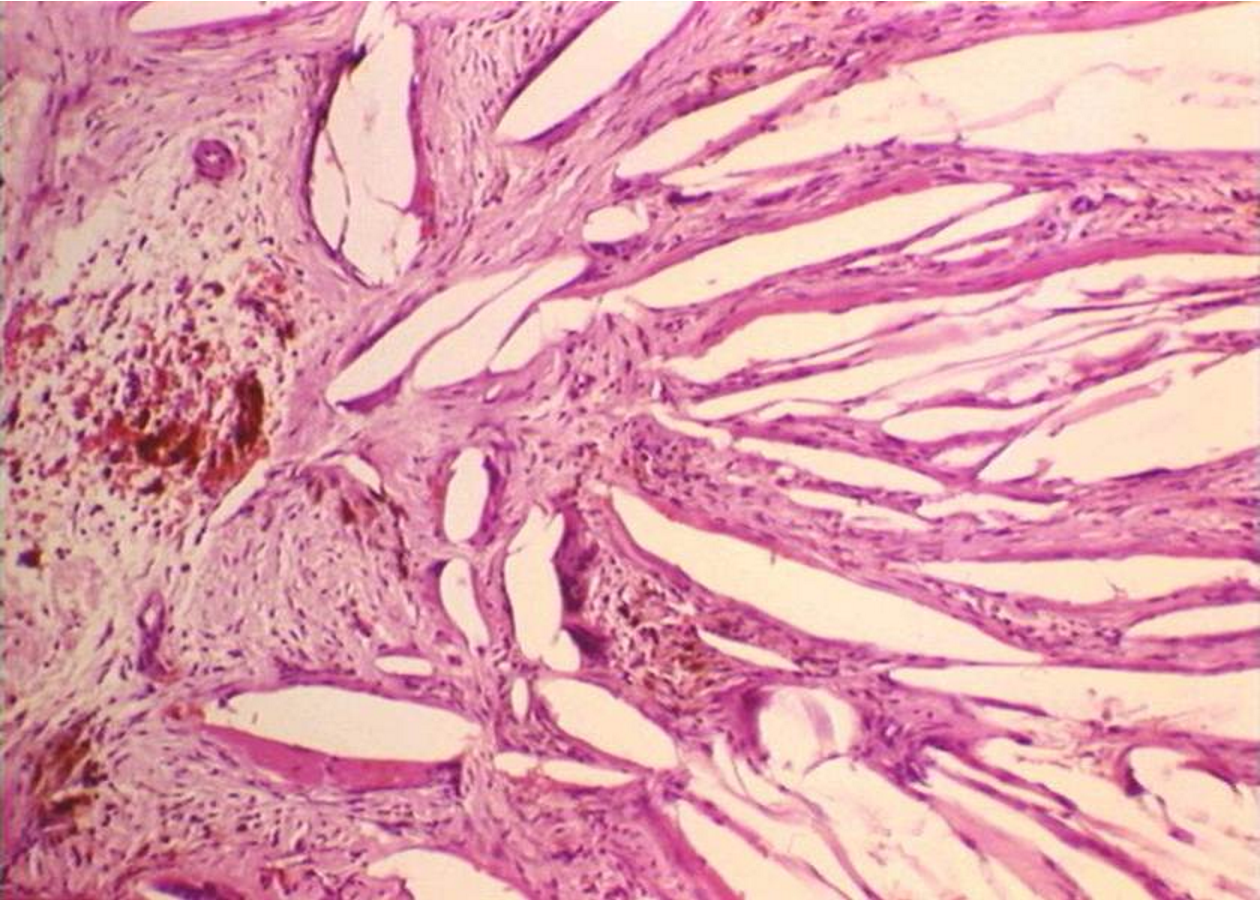
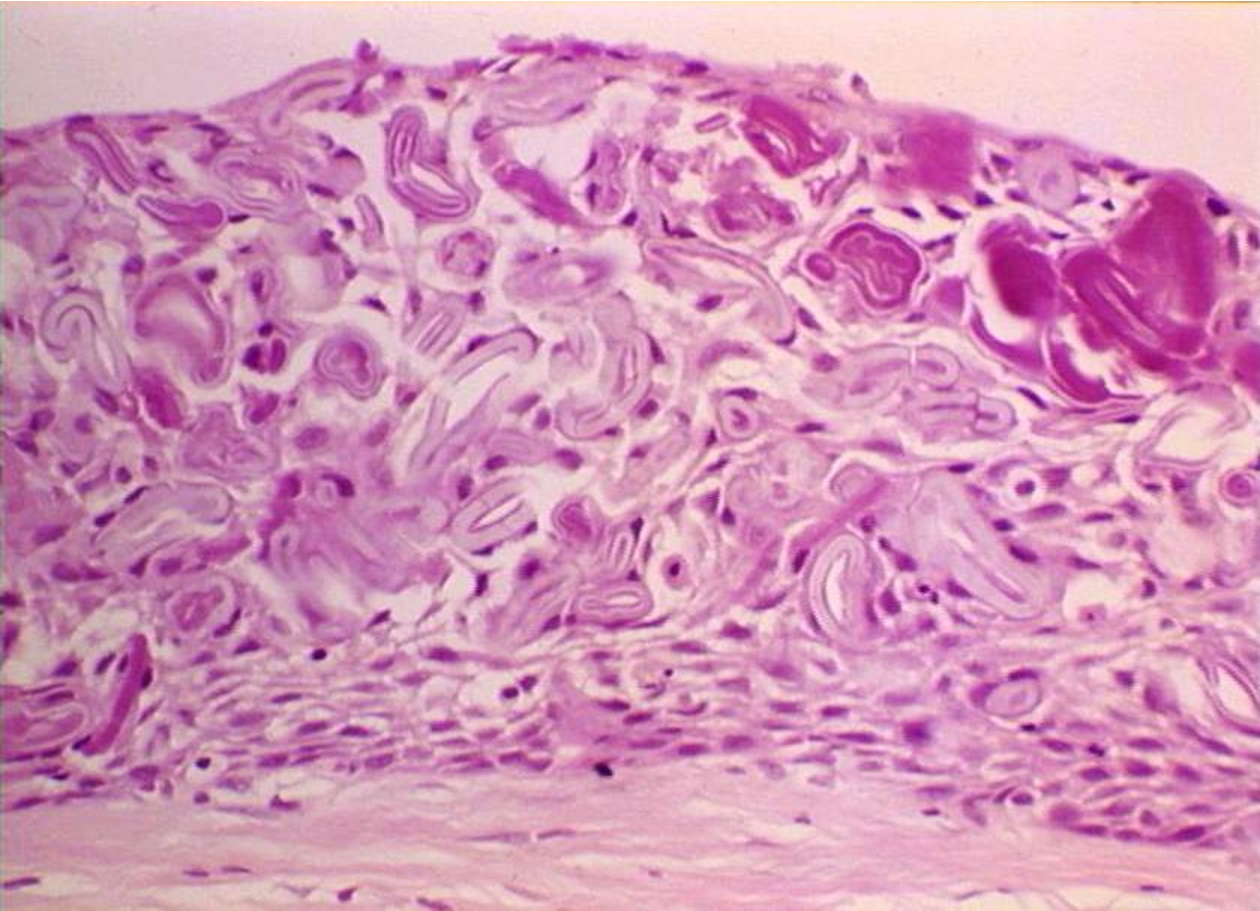
**Histopathology
-
Periapical granuloma with epithelial proliferation - polymorphs in epithelium Granulation tissue = endothelial cells from new blood vessels and a little amount of collagen fibers from fibroblasts
-
Cyst lined by irregular, non-keratinised stratified squamous epithelium
-
Foam cells, lymphocytes, plasma cells, cholesterol clefts, surrounding fibrosis
- Foam cells = macrophages
- They are called foam cells because the macrophages become enlarged and have cloudy cytoplasm
- Foam cells = macrophages
-
Lining becomes thinner and less inflamed
-
10% contain hyaline (Rushton) bodies
-
Cholesterol dissolves in alcohol, during preparation of the ssmaple it will dissolve, leaving the clefts
-
-
Image shows “Hematosomes”:
-
Rushton bodies:
**PARADENTAL CYST
- Partially erupted lower 3rd molar usually with pericoronitis
- Buccal/Disto-buccal aspect
- Enamel spur from bucco-cervical margin of root furcation
- Histologically resembles radicular cyst
- Derived from reduced enamel epithelium
- Paradental cysts are usually attached to the Neck of the tooth
Developmental Odontogenic Cysts
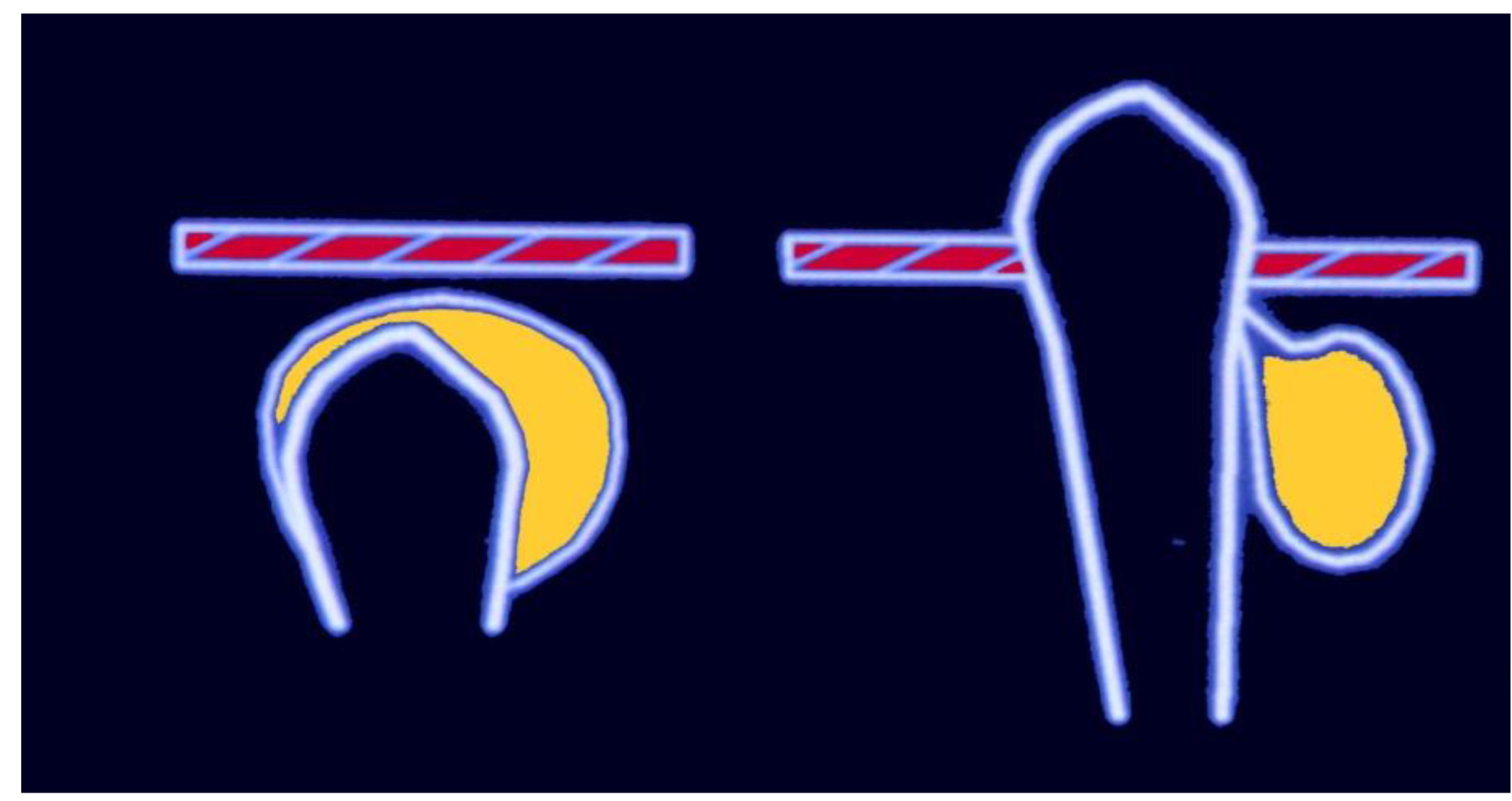
DENTIGEROUS CYST
- Cyst enclosing crown of an unerupted tooth
- Attached to cemento-enamel junction
- Follicular cyst is another name
- Often used because its related to the dental follicle
- We can never see a dentigerous cyst in an unerupted tooth
PATHOGENESIS
- Intrafollicular fluid accumulates between Reduced enamel epithelium and enamel
- Pressure of tooth on impacted follicle causes
- Obstruction of venous outflow
- Serum transudation
- Exudation
CLINICAL FEATURES
- 10-15% of cyst
- Children and young adults
- Permanent teeth
- Upper canine and lower 3rd molar — teeth likely to be impacted
- M:F 1.6:1
- Males are more affected
- Painless enlargement — missing tooth
- Tilting of tooth
- Root resorption
- Radicular cysts usually happen in middle age, but dentigerous cysts happen at younger ages
PATHOLOGY
- Clear yellow fluid — cholesterol
- Purulent if infected
- Lined by flattened, non-keratinised stratified squamous epithelium
- Continuous with reduced enamel epithelium
- Mucous and ciliated columnar metaplasia
- Fibrous wall with variable inflammation
ERUPTION CYST
- Extra-alveolar dentigerous cyst
- Deciduous tooth or permanent molar
- Fluctuant bluish swelling
- Haemorrhage into cyst common
- Most spontaneously resolve
- Better to make an incision that allows the tooth to erupt to help it laong
Relative Frequency of Cysts
| Odontogenic (90%) | Non-odontogenic (10%) |
|---|---|
| Radicular 60-75% | Nasopalatine 5-10% |
| Dentigerous 10-15% | Others 1% |
| Keratocyst 5-10% | |
| Paradental 3-5% | |
| Gingival 1% | |
| Lateral periodontal 1% |
- There are some genetic disruptions that occur specifically keratocytes
- Sometimes they have a high recurrence and can come back in an aggressive form
ODONTOGENIC KERATOCYST
- “The name of this cyst indicates that its epithelial lining keratinises, but this alone is not specific. Another less common cyst, the orthokeratinising odontogenic cyst, also has this feature, and minor focal keratinisation can be seen in other odontogenic cysts.” (Odell, 2017, p. 149)
- “Definition The odontogenic keratocyst is a developmental odontogenic cyst with a tendency to recur, characterised by a histological appearance of parakeratinised lining epithelium with palisaded ameloblast-like basal cells.” (Odell, 2017, p. 149)
CLINICAL
- 5-10% of all jaw cysts
- SITE
- 70-80% mandible
- Most frequent in the posterior mandible
- 50% angle/ramus
- 70-80% mandible
- Often asymptomatic
- M>F
- Swelling, discharge, pain, pathological fracture, tooth displacement, rarely buccal expansion
- Can cause fracture of the mandible when it becomes very large
- 10% of cases of keratocysts have multiple cysts
- High recurrence rate
PATHOGENESIS
- Derived from the dental lamina or it’s remnants - cell rests of Serres
- Originate from enamel organ (tooth primordium) of a tooth before hard tissues develop:
- normal tooth
- supernumerary
RADIOLOGICAL APPEARANCE
- Well demarcated radiolucency
- Pseudolocular or multilocular, often with scalloped periphery
- Root or tooth displacement
[[L5 cysts.pdf#page=44&selection=0,0,0,14&color=yellow|HISTOPATHOLOGY]]
- Regular stratified squamous epithelium
- Thin epithelial layer (5-8 cells thick)
- Palisaded basal layer
- The basal cells have a hypertraumatic blue nuclues
- Slightly columnar appearance
- Aligned in a consistent way
- Palisaded Basal Cells = looks like a fence
- Corrugated surface which can be parakeratinised or orthokeratininsed
- Thin, friable fibrous capsule - little inflammation
- Satellite (daughter) cysts
- The daughter cysts in the cyst wall is what causes the recurrence rates !
Enlargement
- Cancellous enlargement antero-posteriorly
- Little or no bucco-lingual expansion → large, especially in angle and ramus of mandible
RECURRENCE
- Up to 60%
- Size and infiltrative nature
- Tendency to multiplicity and satellite cysts
- Intrinsic growth potential
- Thin, friable capsule
- Genetic - multiple basal cell naevus syndrome (Gorlin-Goltz)
GORLIN - GOLTZ SYNDROME
- Multiple keratocystsis the main defining feature of Gorlin-Goltz syndrome
- Multiple basal cell naevi which can develop into basal cell carcinomas
- Patient may also have Skeletal abnormalities
- bifid ribs
- spine defects
- Frontal bossing and hypertelorism
- Calcification of the falx cerebri
LATERAL PERIODONTAL CYST
CLINICAL FEATURES
- Canine/premolar area
- Rare < 20 years
- Adjacent teeth vital
- NB - Differential diagnosis
**RADIOGRAPHY
- Well defined radiolucent area lateral to tooth
HISTOPATHOLOGY
- Derived from reduced enamel epithelium or cell rests of Malassez
- NKSSE 2-6 cells thick
- Periodic thickening in luminal surface of epithelium
GINGIVAL CYSTS
INFANTS
- Bohn’s nodules, Eptein’s pearls
- Common in newborns and up to 3 months
- Usually rupture or spontaneously involute
- 2-3 mm keratinising stratified squamous epithelium
- Arise from the cell rests of Serres
ADULT
- Slow -growing, usually < 1cm diameter
- Cause a large swelling
- Free or attached gingiva or interdental papilla
- Tooth vital
- Pathogenesis
- odontogenic
- implantation
Non-Odontogenic Developmental Cysts
- The non odontogenic cysts are called Nasoplatlaine duct cysts and nasolabial(naso-alveolar cysts)
- The old classifications of median cysts and globulomaxillary cyst have been removed
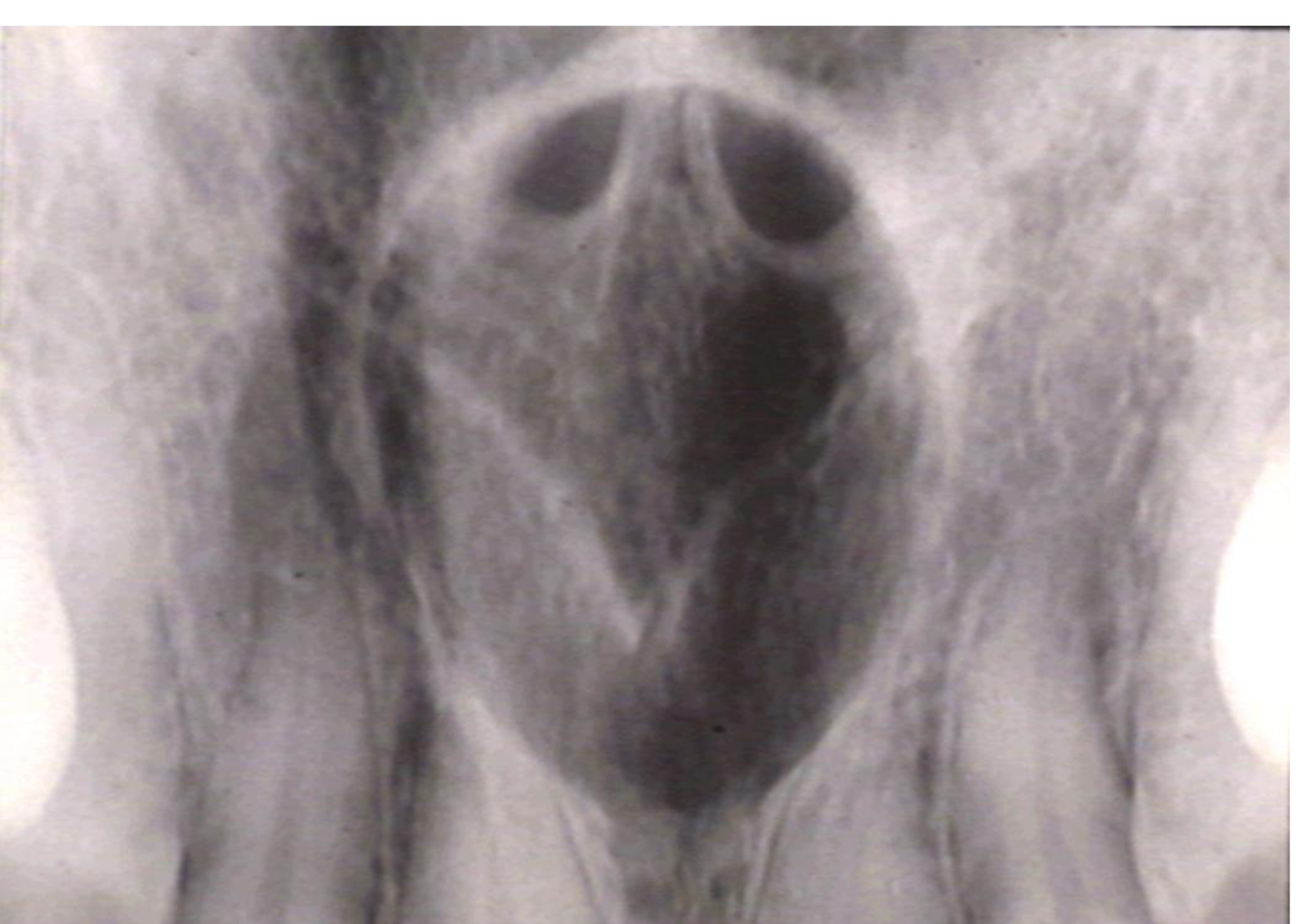
NASO-PALATINE DUCT CYST
- Incisive canal cyst
- Remnants of nasopalatine duct
- M:F 4:1
- 30-60 years
- Swelling of midline of anterior hard palata
- Pain and discharge
- Mucoid and salty
- Anterior Teeth are vital
- No source of infection
RADIOLOGY
- Well defined radiolucency between roots of central incisors
- Roots may diverge
- Intact lamina dura
**HISTOPATHOLOGY
- Respiratory type epithelium
- Stratified squamous epithelium
- Blood vessels and nerves in wall Histological image of pseudostratified columnar epithelium with cilia.
NASOLABIAL CYST
- Swelling in nasolabial fold below alae and leading to loss of fold
- Sometimes bilateral
- Swelling, pain, difficulty in nasal breathing
- Nasolabial cysts are soft tissue lesions
PATHOGENESIS
- epithelium enclosed at a site of ‘fusion’ of globular, lateral nasal and maxillary processes — unlikely
- remnants of embryonic nasolacrimal rod or duct
HISTOPATHOLOGY
- Non-ciliated columnar, respiratory type or stratified squamous epithelium
Non-Epithelial (Primary Bone) Cysts
- Also called simple, haemorrhagic, traumatic bone cysts
- Rare
- Mandible, usually in second decade
- Radiolucent area extending between roots (scalloping), usually without expansion
- Resolves with minimal intervention
**HISTOPATHOLOGY
- No epithelium
- Vascular fibrous tissue in the cyst wall Radiographic and histological images of a Solitary Bone Cyst.
ANEURYSMAL BONE CYST
- Radiolucent area bulging into adjacent soft tissue
- Mostly in children and young adults
- Blood filled spaces - non endothelial lined
- Giant cells, haemorrhage, osteoid
- Giant cell lesion
- Very aggressive type of cysts Cyst wall Sometimes the cyst linig isn’t consistent, some areas are thick while othes are then Cyst lining Needs are: cholesterol clefts