Oral Potentially Malignant Disorders
Oral Cancer Statistics
- 2/3 of oral cancers are detected at advanced stage
- 5-year survival rate is 50%
- Early detection can lead to high survival rate

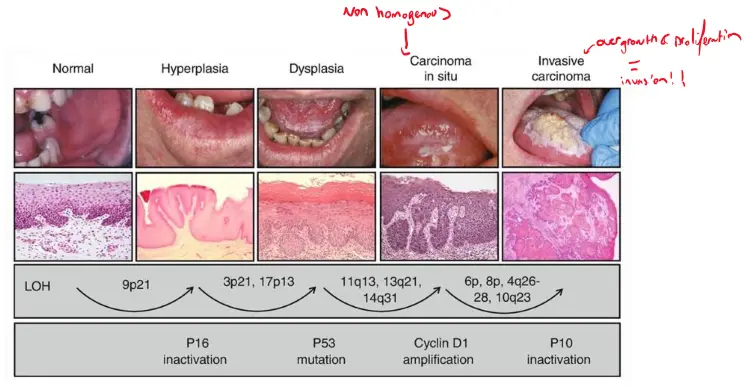
Pathogenesis Pathway
Normal → Hyperplasia → Dysplasia → Carcinoma in situ → Invasive carcinoma
- For oral cancer to occur you need to have at least 6-8 genetic mutations
- Some of these can be related to chromosomal (i.e.e P16, P53, CyclinD1, P10)
- Some of these can be related to chromosomal (i.e.e P16, P53, CyclinD1, P10)
Nomenclature and Classification
Definition
- OPMDs refer to a group of lesions and conditions characterised by a variably increased risk of developing cancers of the lip (C00) and the oral cavity (C02-C06)
- ‘pre-cancer’, ‘precursor lesions’, ‘pre-malignant’, ‘intra epithelial neoplasia’ and ‘potentially malignant’ have been used in the international literature to broadly describe clinical presentations that may potentially become cancer.
- Lesion vs condition:
- Lesions are localized whereas conditions are found in multiple parts of the body
History of terminology
- 1805: Precancer term proposed by European physicians (Baillie & Simms)
- 1978: Oral Precancerous lesions and conditions (WHO Collaborating Center)
- 2003: Oral Precursor Lesions (Oral epithelial dysplasia workshop, Oxford 2003)
- 2005: Potentially Malignant Disorders (WHO Collaborating Center)
- 2020: Oral Potentially Malignant Disorders (WHO Collaborating Center)
Supporting Literature: Nomenclature and Classification (2007)
Summary: Nomenclature and Classification of Oral Potentially Malignant Disorders (Warnakulasuriya et al., 2007) 1. Terminology Shift
- The term “potentially malignant disorders” (PMDs) was recommended over “precancer” to reflect that not all such lesions inevitably progress to cancer.
- This terminology better aligns with the concept of multi-step carcinogenesis in the oral mucosa and encourages more precise clinical communication. 2. Definition of Oral Leukoplakia
- The Working Group proposed a refined definition: leukoplakia refers to “white plaques of questionable risk, having excluded other known diseases or disorders that carry no increased risk for cancer.”
- This definition is exclusion-based, aiming to prevent misclassification of benign white lesions. 3. Diagnostic Guidelines
- A diagnostic outline was proposed to help clinicians distinguish leukoplakia from other white oral lesions such as lichen planus or frictional keratosis.
- The emphasis is on improving diagnostic accuracy and reducing overdiagnosis. 4. Classification Challenges
- The article highlights inconsistencies and deficiencies in existing classification systems for PMDs.
- It calls for standardization to improve research comparability and clinical decision-making. 5. WHO Workshop Consensus
- The recommendations stem from a WHO-coordinated expert workshop, lending international credibility.
- The consensus reflects decades of evolving understanding of oral carcinogenesis and aims to unify terminology and classification practices.
WHO classification 2005
| Classification of precancerous lesions and conditions | |
|---|---|
| Precancerous lesions | Precancerous conditions |
| Leukoplakia | Submucous fibrosis |
| Erythroplakia | Actinic keratosis |
| Palatal lesions in reverse smokers | Lichen planus |
| Discoid lupus erythematosus | |
| Hereditary disorders with increased risk: dyskeratosis congenita and epidermolysis bullosa |
Classification of oral potentially malignant disorders
- Leukoplakia
- Proliferative verrucous leukoplakia
- Erythroplakia
- Oral submucous fibrosis
- Oral lichen planus
- Actinic Keratosis (Actinic Cheilitis)
- Palatal changes in reverse smoking
- Oral Lupus Erythematosus
- Dyskeratosis Congenita
Newly included in 2021 classification
- Oral Lichenoid Lesion
- Oral Graft versus Host Disease
Remove from the 2021 classification due to limited evidence
- Oral Epidermolysis Bullosa
- Chronic hyperplastic candidosis
- Exophytic verrucous hyperplasia/verrucous hyperplasia
OPMD Epidemiology
- A recent systematic review included 22 epidemiological surveys that estimated a global prevalence of OPMDs at 4.47%
- It was noted that prevalence may vary between populations and was generally higher in Asians and males.
Risk factors
- nicotine products Smokers are also at 10 times higher risk for oral cancer compared to non-smokers.
Alcohol
Moderate drinkers have 1.8-fold higher risks of oral cavity and pharynx cancers and 1.4-fold higher risks of larynx cancers than non-drinkers, and heavy drinkers have 5-fold higher risks of oral cavity and pharynx cancers and 2.6-fold higher risks of larynx cancers.
Smoking and Drinking Combined
- The combination of smoking and drinking is the most important aetiological factor for oral cancer and OPMDs
- Many patients smoke and drink heavily (>5 standard drinks/day)
- Both of these account for up to 75% of all OPMD cases
Betel quid/Areca nut
- Areca nut
- Abundant copper and flavonoids
- Stabilize and enhance cross-linking of collagen
- Fibrosis
- Stabilize and enhance cross-linking of collagen
- Alkaloids (arecoline)
- Stimulate collagen synthesis and reduce collagen degradation
- Can be converted to carcinogenic nitrosamines
- Abundant copper and flavonoids
- Gutka
- Powdered tobacco, slaked lime, and spices wrapped in Piper betle leaf, also referred to as “betel leaf”
- more rapid development of oral lesions
HPV
HPV is thought to cause 70% of oropharyngeal cancers in the United States.
Clinical types
Leukoplakia
Persistent white patch that cannot be rubbed off. Generally asymptomatic.
- 1-4% in Western countries
- Higher prevalence in SE Asia
- Global prevalence: 2-3%
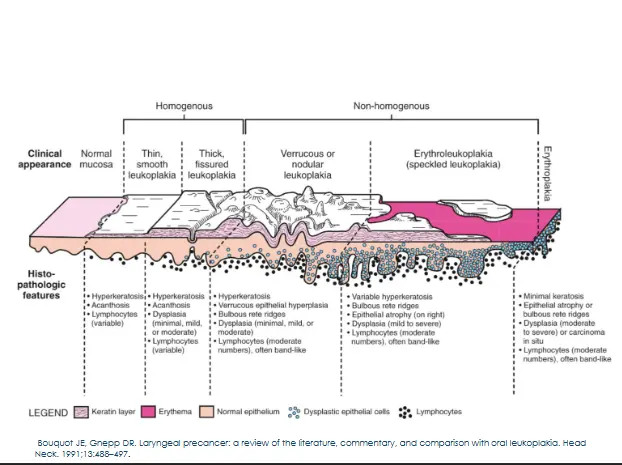
- Homogeneous leukoplakia: Uniformly white, flat and thin, have a smooth surface and may exhibit shallow cracks.
- Nodular leukoplakia: Small polypoid or rounded outgrowths, red or white excrescences.
- Verrucous leukoplakia: The surface is raised, exophytic, wrinkled or corrugated.
Leukoplakia: Clinical and Histopathologic Features
Leukoplakia Diagnostic Pathway
- White patch → Provisional clinical diagnosis of leukoplakia
- Excluded other known conditions/disorders/diseases based on history and examination
- White sponge naevus,
- Frictional keratosis,
- Alveolar ridge keratosis,
- Chemical injury,
- Acute pseudomembranous candidosis,
- Leukoedema,
- Fordyce’s spots/ condition,
- Skin graft,
- Hairy leukoplakia,
- Leukokeratosis nicotina palate (Smoker’s palate)
- BIOPSY
- If other known disorder confirmed: Revise diagnosis to other disease/disorder
- If other known disorder excluded:
- Revise diagnosis to Leukoplakia with dysplasia
- Revise diagnosis to Leukoplakia without dysplasia
Erythroplakia
- Defined as “A predominantly fiery red patch that cannot be characterised clinically or pathologically as any other definable disease”
- Discomfort, tingling and sensitivity to touch, hot beverages or spicy foods
- Velvety
- Granular
- Red plaque
- Usually painless
- Flat or indurated
Erythroplakia: Conditions to Exclude
Clinical conditions to exclude in the diagnosis:
- Erythematous candidiasis,
- Denture-associated stomatitis on palate,
- Erythema migrans.
- Erosive and inflammatory / infective disorders, Desquamative gingivitis,
- Discoid lupus,
- Erosive lichen planus,
- Pemphigoid
Proliferative verrucous leukoplakia
- Multiple, thick, white patches in more than two different oral sites, frequently found on the gingiva, alveolar processes, and palate.
- Majority present with a verrucous pattern.
- Lesions spread and coalesce during development.
- Recurrence in a previously treated area
- Lesion starts on a small spot and keeps growing
- Can only make a PVL diagnosis retrospectively , based on the clinical course
Oral submucous fibrosis
- Diffuse, pale, marble-like, and keratotic areas
- Makes it difficult to open the mouth
- Sites
- Buccal mucosa
- Soft palate
- Tongue
- Symptoms
- Burning
- Increasing trismus
- Clinical presentation
- Blanching of oral mucosa
- Marked loss of tongue papillae
- Leathery mucosa
- Fibrous bands
- Limited mobility of tongue (rigidity)
- Shrunken or deformed uvula
- Limitation of mouth opening
- Can go down all the way to 10mm
- Sunken cheeks
Actinic cheilitis
- UV light exposure
- Aetiopathogenesis similar to that of actinic keratosis of the skin
- Early
- Atrophy (smooth, blotchy, pale areas)
- Dryness
- Fissuring
- Blurring of the vermilion border
- Late
- Rough, scaly areas
- May develop leukoplakia
Lichen Planus
- Immune mediated
- T lymphocytes mainly
- Idiopathic vs drug induced
- Prevalence
- 0.22-5% worldwide
- 30-80 year
- Approximately 15% have cutaneous disease as well
- Females > Males
Lichen Planus Diagnostic Criteria
| Criteria Type | Details |
|---|---|
| Clinical criteria | - Presence of bilateral, more or less symmetrical white lesions affecting buccal mucosa, and/or tongue, and/or lip, and/or gingiva |
| - Presence of a white papular lesions and lace-like network of slightly raised white lines (reticular, annular, or linear pattern) with or without erosions and ulcerations | |
| - Sometimes presents as desquamative gingivitis | |
| Histopathological criteria | - Presence of a well-defined band-like predominantly lymphocytic infiltrate that is confined to the superficial part of the connective tissue |
| - Signs of vacuolar degeneration of the basal and/or supra basal cell layers with keratinocyte apoptosis | |
| - In the atrophic type, there is epithelial thinning and sometimes ulceration caused by failure of epithelial regeneration as a result of basal cell destruction. A mixed inflammatory infiltrate may be found |
Disorders with insufficient epidemiological evidence
- Chronic hyperplastic candidosis
- Exophytic verrucous hyperplasia/Oral verrucous hyperplasia
Oral Epithelial Dysplasia
Summary: Oral Epithelial Dysplasia — Recognition, Grading and Clinical Significance (Odell et al., 2021) 1. Role in OPMDs
- Histopathological grading of oral epithelial dysplasia remains the main laboratory method to assess malignant transformation risk in OPMDs.
- The grading provides essential prognostic information and guides clinical management. 2. Pathogenesis and Histology
- Reviews current understanding of molecular pathogenesis in dysplastic change.
- Details how histological interpretation links cellular and architectural abnormalities to cancer risk. 3. WHO Diagnostic Criteria
- Proposes revisions to the 2017 WHO criteria, placing greater emphasis on architectural features over purely cytological ones in diagnosing epithelial dysplasia. 4. Grading Systems
- Summarises the predictive values of three‑grade systems (mild, moderate, severe) and binary systems (low‑risk vs high‑risk).
- Discusses their relative strengths, limitations, and implications for reproducibility between pathologists. 5. Categories of Dysplasia Reviewed
- Lichenoid and verrucous lesions
- Keratosis of unknown significance
- HPV‑associated dysplasia
- Differentiated epithelial dysplasia
- Basaloid epithelial dysplasia 6. Clinical Management Implications
- The detection of epithelial dysplasia in a biopsy requires careful consideration of follow‑up, surveillance intervals, and possible intervention.
- The article reflects the pathologist’s perspective on integrating histopathological findings into treatment planning.
WHO Classification 2022: Diagnostic Criteria
| Architectural Features | Cytological Features |
|---|---|
| Irregular stratification | Abnormal variation in nuclear size |
| Loss of polarity or disorganisation of basal cells | Abnormal variation in nuclear shape |
| Drop shaped rete processes | Abnormal variation in cell size |
| Basal cell clustering/nesting | Abnormal variation in cell shape |
| Expanded proliferative compartment | Increased mitotic activity |
| Mitoses high in epithelium | Increased nuclear size |
| Mitoses in maturing cells | Increased nucleus:cytoplasm ratio |
| Generalized premature keratinization | Atypical mitotic figures |
| Keratin pearls in rete processes | Increased number and size of nucleoli |
| Reduced keratinocyte cohesion | Single cell keratinisation |
| Altered keratin pattern for oral sub-site | Nuclear hyperchromasia |
| Verrucous or papillary architecture | Apoptotic mitoses |
| Extension of changes along minor gland ducts | |
| Sharply defined margin to changes | |
| Multiple different patterns of dysplasia | |
| Multifocal or skip lesions | |
| Hyperkeratosis and epithelial hyperplasia with no dysplasia (x100). |

OPMD Malignant transformation
- [A systematic review of 92 studies indicated the overall malignant transformation rate across all OPMD groups was **7.9% **]{.underline}
- [Proliferative verrucous leukoplakia **49.5% **]{.underline}
- [Erythroplakia 33.1%]{.underline}
- [Leukoplakia **9.5 **]{.underline}
- Oral Submucous Fibrosis 5.2%
- Oral Lichenoid Lesions 3.8%
- Lichen planus 1.4%
Supporting Literature: Risk of Progression
Oral potentially malignant disorders (OPMDs) have a statistically increased risk of progressing to cancer, but the risk varies according to a range of patient- or lesion-related factors. It is difficult to predict the risk of progression in any individual patient, and the clinician must make a judgment based on assessment of each case. The most commonly encountered OPMD is leukoplakia , but others, including lichen planus, oral submucous fibrosis and erythroplakia may also be seen. Factors
Features Associated with Increased Risk of Malignant Transformation
Need to know!
| Feature | Parameter | Association | |
|---|---|---|---|
| Clinical features | Size of lesion | >200mm² | Strong |
| Texture | Nonhomogeneous | Strong | |
| Colour | Red (Speckled) | Strong | |
| Site | Tongue or floor of mouth | Strong | |
| Sex | Female | Medium | |
| Age | >50 years | Medium | |
| Habits | Nonsmoker | weak | |
| Histological and molecular features | Dysplasia | Severe | Strong |
| High-grade | Strong | ||
| HPV | HPV +16 | Medium | |
| DNA content | Aneuploidy | Medium | |
| LOH | Many genes involved | Medium |
Predictors of Malignant Transformation and Recurrence A recent systematic review revealed:
- a higher rate of MT for non-homogeneous OL, affecting the tongue or the FOM, measuring >200mm², in patients without smoking habits.
- non-homogeneous OL have a higher chance of recurrence after treatment compared with homogeneous ones.
- PVL, we found a significantly higher risk of MT associated with the female sex.
Clinical tips
Differential diagnosis of mucosal lesions in the mouth
- History of current illness
- Onset, location, intensity, frequency, duration
- Aggravating and/or relieving variables
- Better, unchanged or worse over time
- Medical, tobacco and alcohol history
- Medical conditions
- Medications and allergies
- Tobacco and alcohol (type, frequency, duration)
- Clinical examination
- Extraoral
- Intraoral
- Lesion inspection (adjunct tools)
- Differential diagnosis
- Diagnostic tests
- biopsy
- Definitive diagnosis
- Suggested management
Considerations in Differential Diagnosis
- Number of possibilities
- High frequency of insignificant lesions
- Occasional very significant lesions
Lesion Categories for Differential Diagnosis
- Not really an OPMD
- Normal
- Developmental
- Traumatic
- Infectious
- Idiopathic
How to differentiate lesions
- Carcinoma?
- Is it normal?
- Evidence for a developmental condition?
- Habits and causes of friction?
- Does site help - CHC, OHL, SN
- Any striae?
- Risk features for dysplasia or malignancy?
- Smear it
- Biopsy it
Clinical Pathway for the Evaluation of Potentially Malignant Disorders in the Oral Cavity
Clinicians^ should obtain or update a patient history and perform an intraoral and extraoral conventional visual and tactile examination in all adult patients.
| A. No clinically evident lesion or symptoms | B. A clinically evident, seemingly Innocuous lesion (not suspected to be malignant) | C. A clinically evident, suspicious lesion (suspected to be either a PMD or malignant disorder) |
|---|---|---|
| Periodically follow up with patient to determine the need for further evaluation. | Lesion resolves (either spontaneously or after treatment). → No further action is necessary at this time. | Perform a biopsy of lesion or provide Immediate referral to a specialist. |
| Lesion persists or progresses or clinical diagnosis of PMD cannot be ruled out. → Use cytologic adjunct to triage patient and provide additional lesion assessment. | Should a patient decline a biopsy or referral | |
| Cytologic Adjunct Result: | Definitive diagnosis of PMD or malignancy | |
| - Positive or atypical test result: → Perform a biopsy of lesion or provide Immediate referral to a specialist. | ||
| - Negative test result: → Periodically follow up with patient to determine the need for further evaluation. |
Summary
- Oral cancer is a preventable disease
- Early detection can improve survival rates and quality of life
- Dentists and other dental team members play a significant role in detecting OPMDs
- For patients with a clinically evident oral mucosal lesion considered to be suspicious of an OPMD, clinicians should perform a biopsy of the lesion or provide immediate referral to a specialist.
- Cancer may arise during the natural history of an OPMD, patient follow-up at appropriate intervals is strongly recommended. The follow-up interval should be decided based on the individual’s risk assessment and patient compliance