Case 1 White Sponge Nevus
🔬 Corrected Microscopic Features: White Sponge Nevus
White Sponge Nevus is a genetic disorder caused by mutations in the genes that produce specific keratin proteins ( and
). This leads to a defect in the normal maturation of the oral mucosa, resulting in the following characteristic microscopic appearance.
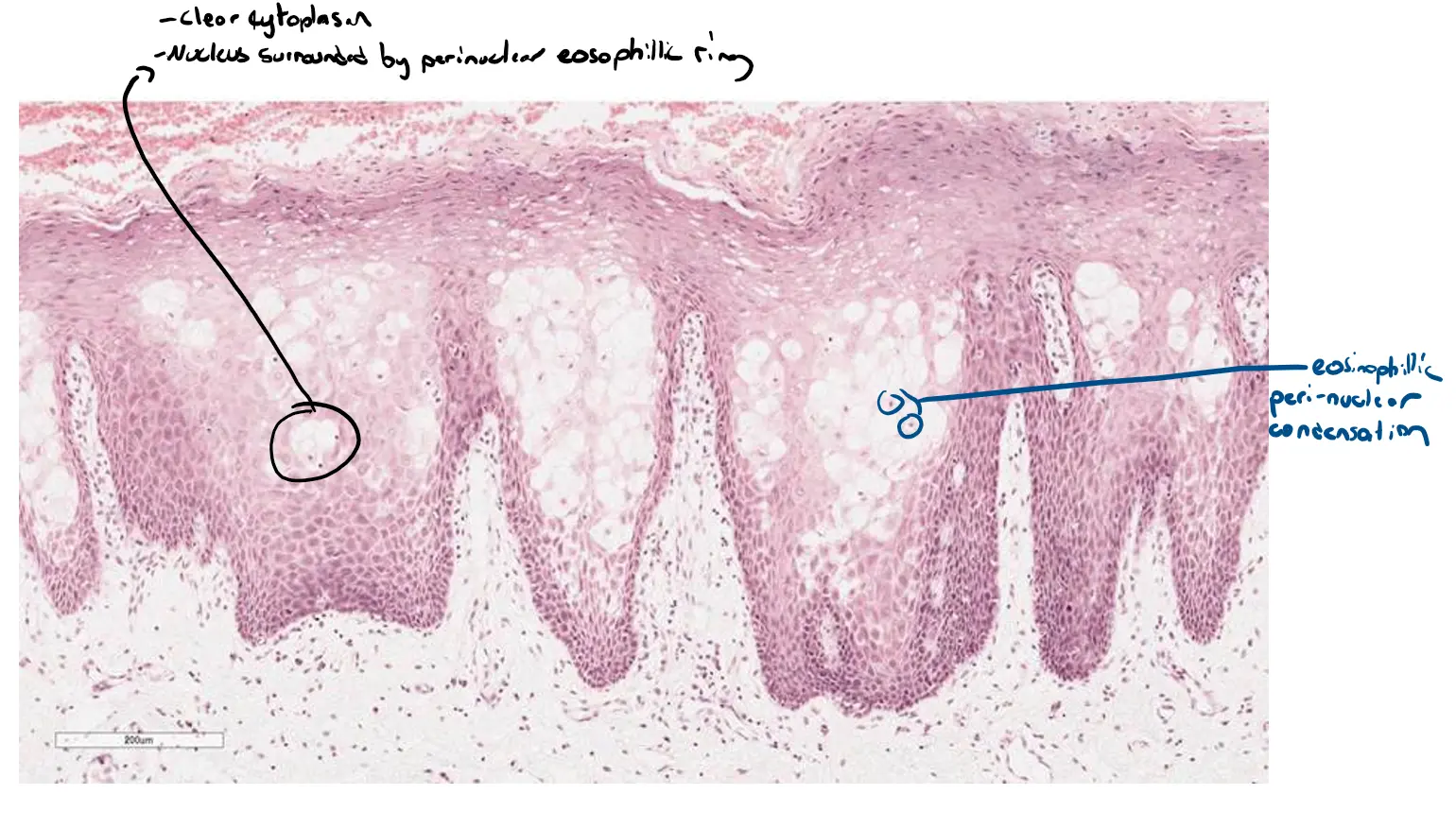
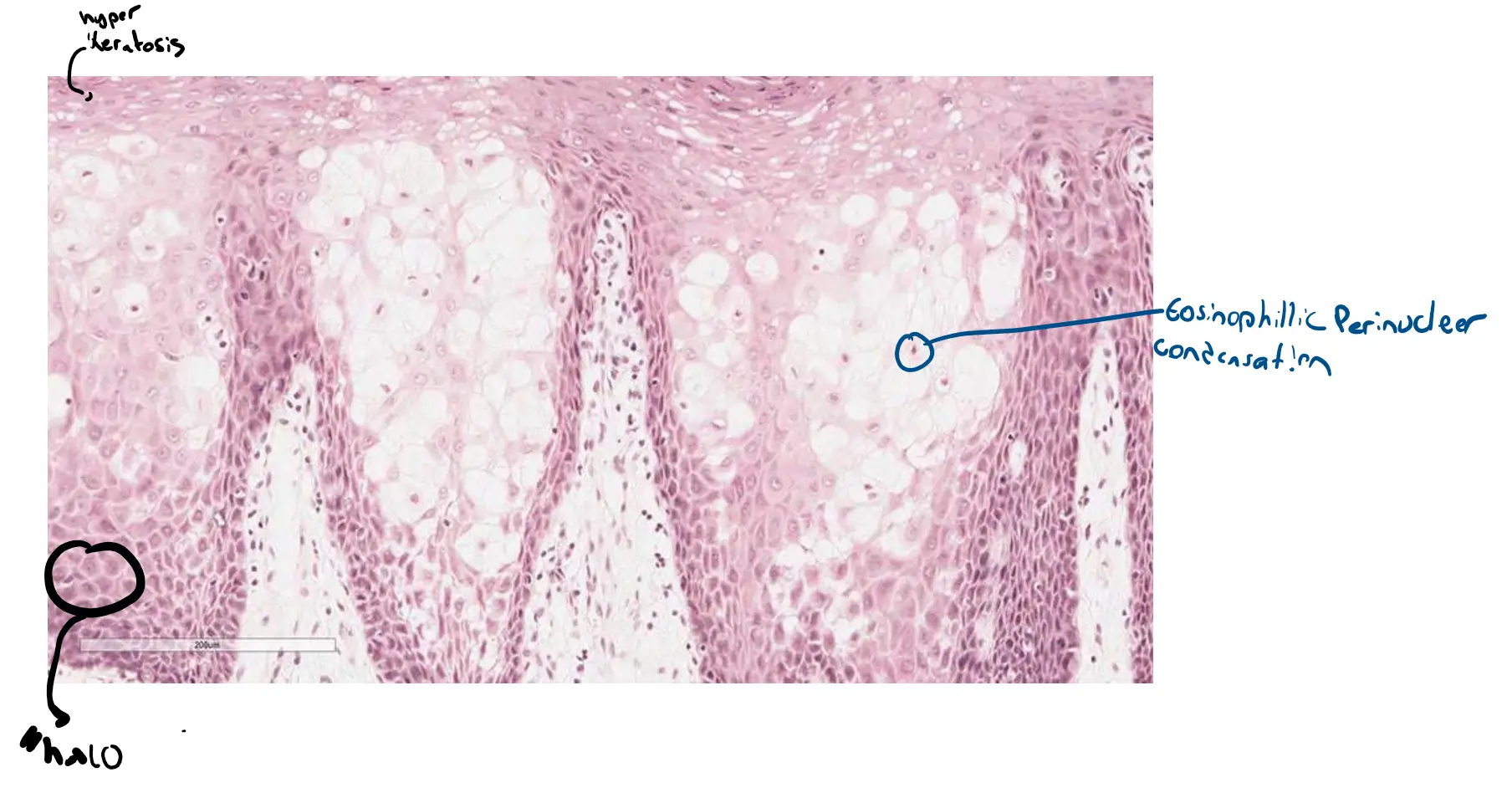
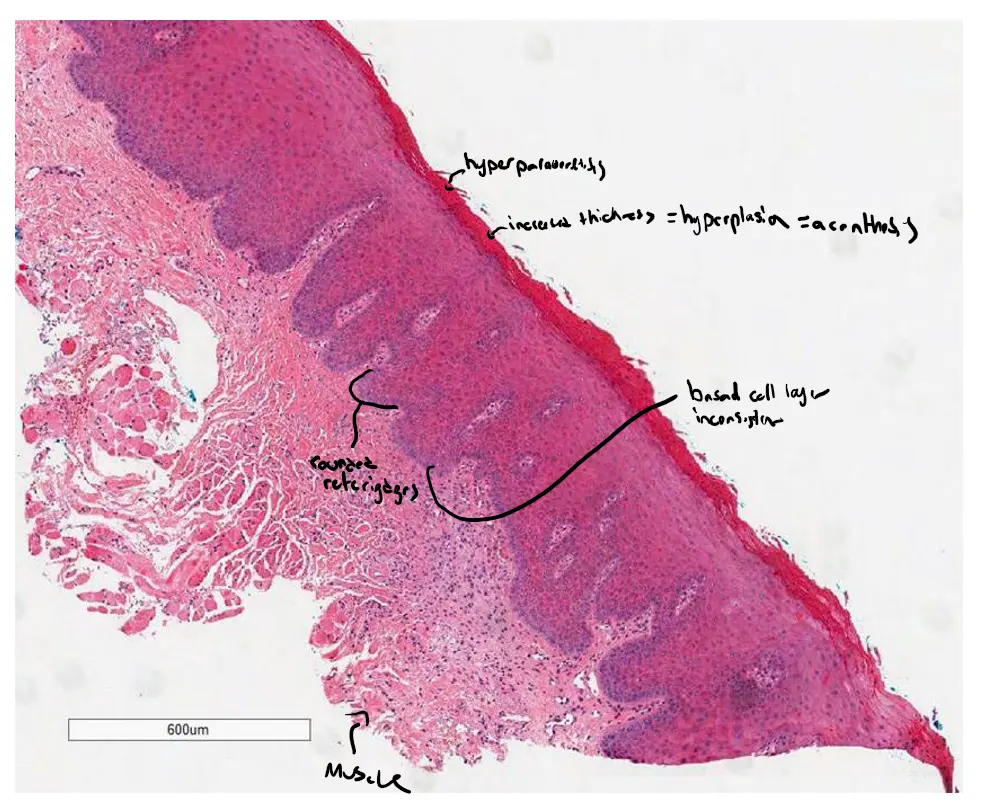
Hyperparakeratosis and Acanthosis
This part of the description remains visually the same, but the cause is different.
-
Prominent hyperparakeratosis: The outermost layer of the mucosa (the stratum corneum) is significantly thickened, and the cells improperly retain their nuclei.
-
Marked acanthosis: The spinous layer is much thicker than normal, leading to the elongated and broadened epithelial projections.
Why this happens in WSN: The faulty keratin genes disrupt the normal, orderly shedding of epithelial cells, causing them to pile up and leading to the thick, white, “spongy” plaques seen clinically.
Cytoplasmic Clearing and Perinuclear Halos
-
Clearing of the cytoplasm: The cells in the spinous layer appear large, pale, and empty. This is due to extensive intracellular edema (excess water in the cells) and the disorganization of the internal keratin network. This creates the “spongy” texture that gives the condition its name.
-
The “Halo” Effect: The clearing of the cytoplasm creates a large, pale space around the nucleus, which appears as a “halo.” In WSN, this is a direct result of the defective keratin structure, not a viral-induced effect.
Eosinophilic Perinuclear Condensation
-
This is a key diagnostic feature of White Sponge Nevus.
-
Within the cleared cytoplasm of many cells, you can see a distinct, dense, pink-staining (
eosinophilic) ring or condensation immediately surrounding the nucleus. -
This material represents the tangled, aggregated, and collapsed abnormal keratin filaments that result from the underlying genetic mutation. While the clearing effect can look similar to other conditions, this specific feature is highly characteristic of WSN.
In summary, the combination of a thickened, spongy epithelium with cleared cells and, most importantly, the presence of these perinuclear eosinophilic condensations, confirms the diagnosis of White Sponge Nevus.
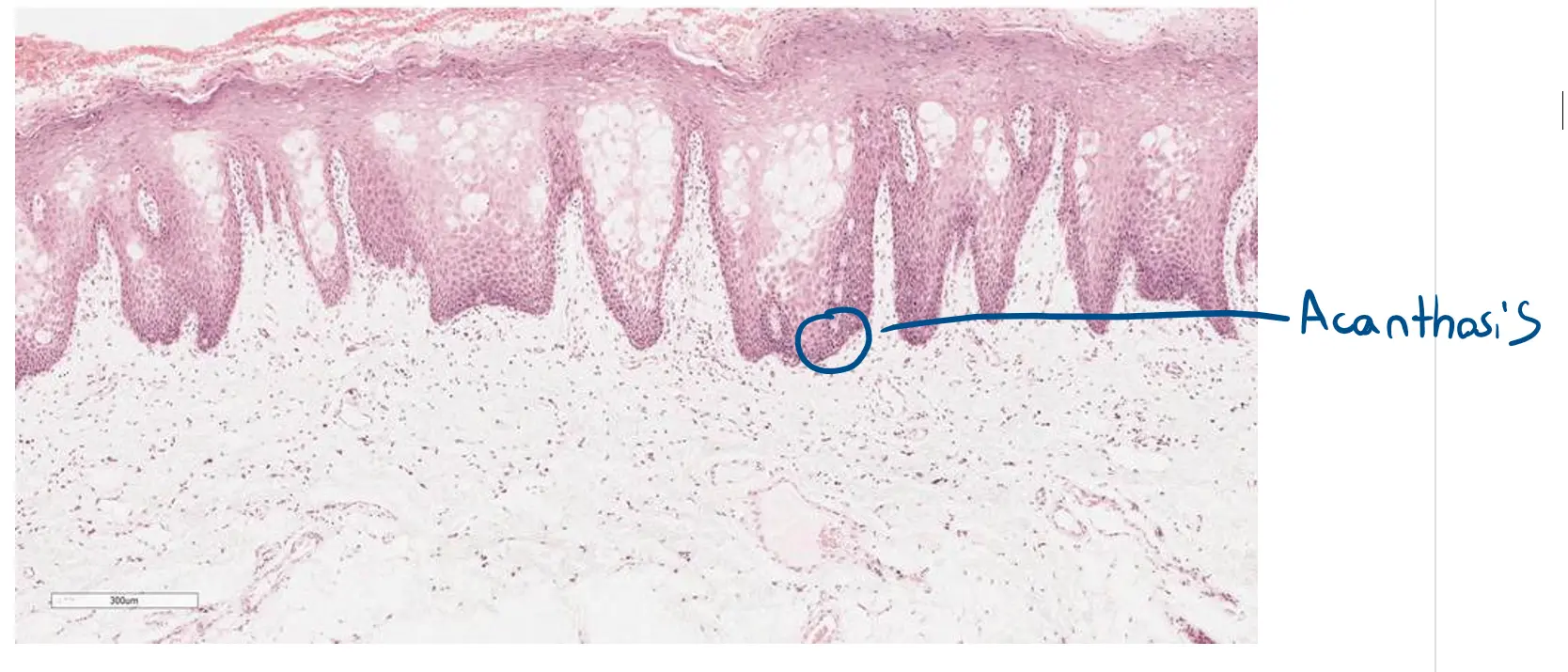
Case2: Squamous Papilloma

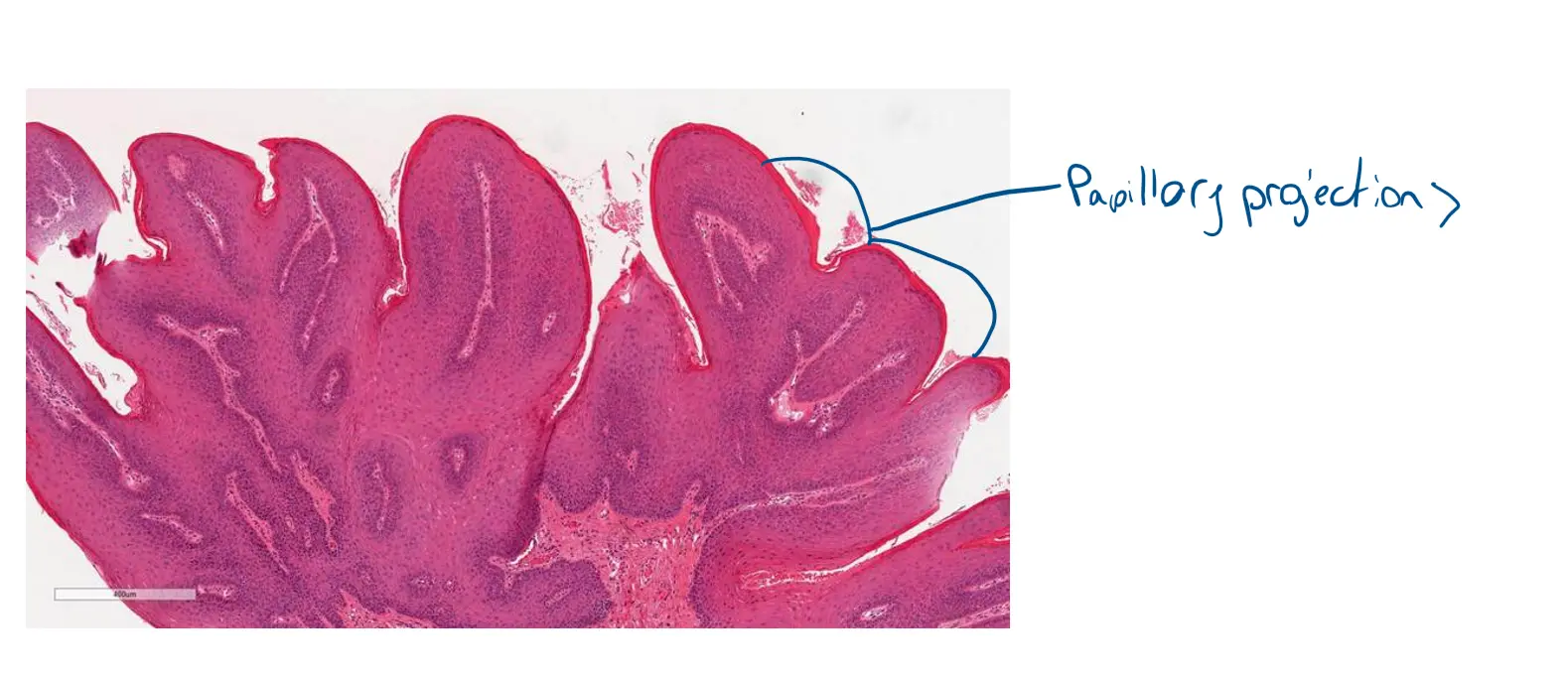

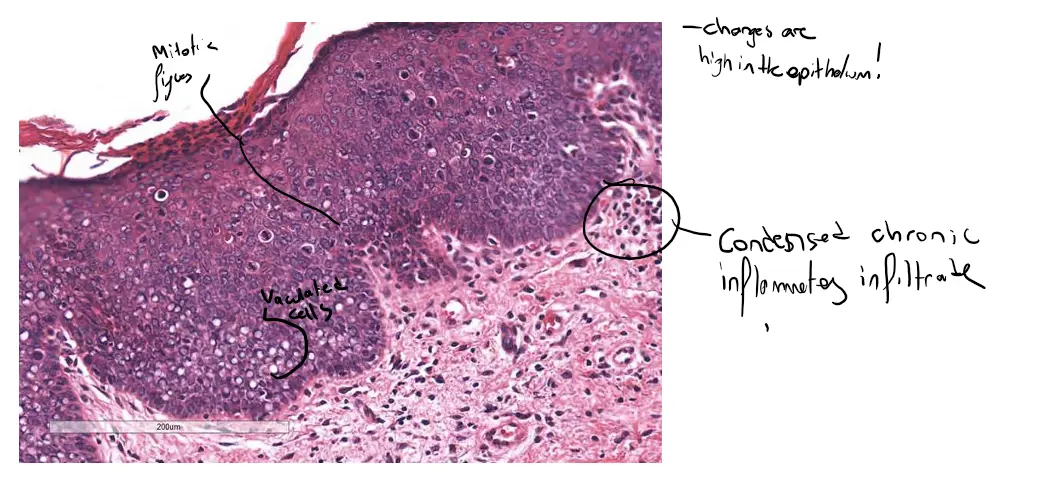
Excellent. This high-magnification image beautifully illustrates all the features we’ve discussed. Here is a comprehensive analysis of this image, integrating all the points to confirm the diagnosis of a squamous papilloma.
🔬 Comprehensive Analysis: Squamous Papilloma
This image provides a detailed view of the lesion’s cross-section, confirming the diagnosis by showcasing both its unique architecture and the specific cellular changes caused by the Human Papillomavirus (HPV).
Architectural Features
The overall structure seen here is the foundation of the papilloma.
-
Papillary Structure: You are looking at a cross-section of the “finger-like projections.” Instead of a flat surface, the epithelium grows in complex, swirling folds. The structure on the right shows a single projection cut at an angle, while the multiple structures on the left represent several adjacent projections that have been cross-sectioned.
-
Fibrovascular Cores: At the center of each epithelial fold, you can clearly see a lighter-staining connective tissue core. Crucially, within these cores are small blood vessels (capillaries), which are visible as small, circular structures. These fibrovascular cores act as a scaffold and provide the blood supply needed to nourish the thickened, proliferating epithelium.
-
Acanthosis: The layers of squamous epithelium surrounding the cores are markedly thickened, with an increased number of cells. This is known as acanthosis and is responsible for the bulk of the lesion.
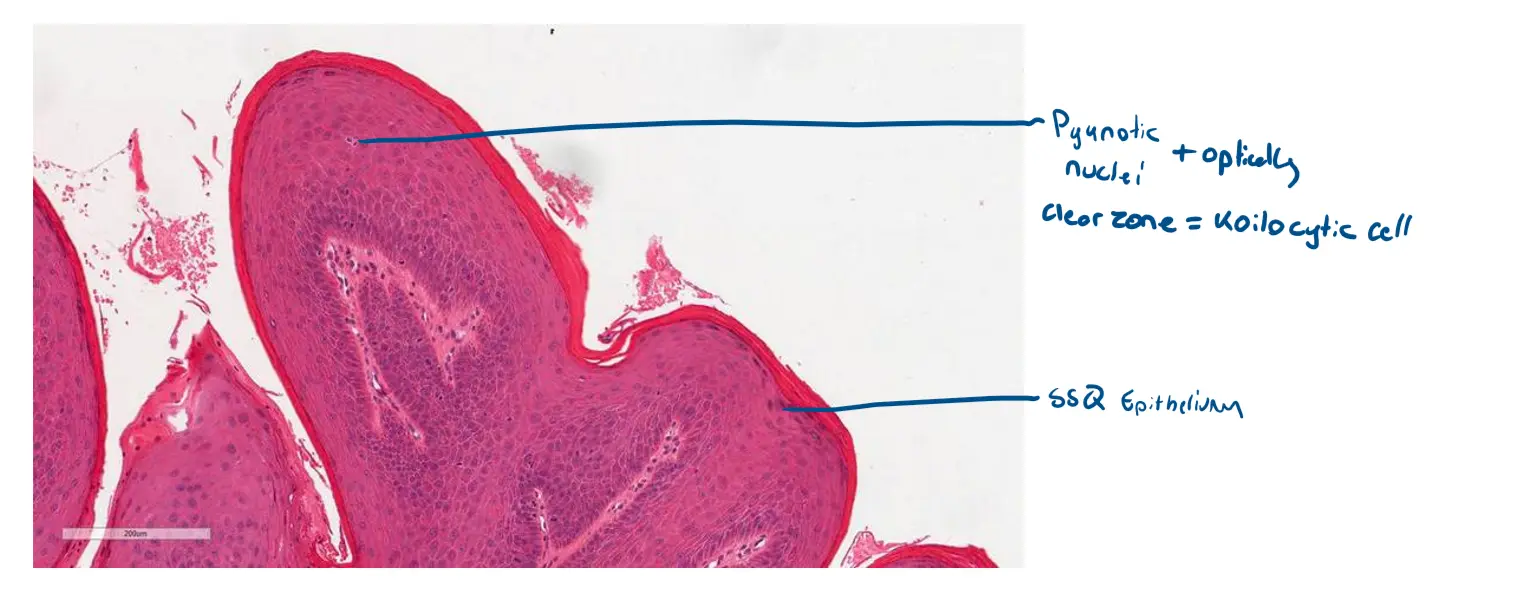
Cellular Features (The Hallmark of HPV)
This is where we see the direct effect of the virus on the individual cells.
-
Koilocytic Atypia: This image clearly displays koilocytes, the cells pathognomonic for HPV infection. They are most prominent in the upper-middle layers of the epithelium (the upper stratum spinosum and granulosum). These cells exhibit two key features:
-
Pyknotic Nuclei: The nuclei of the infected cells are shrunken, irregular in shape, and intensely dark (hyperchromatic). They look like small, dark “raisins” instead of the larger, rounder nuclei of the healthy cells in the lower layers.
-
Perinuclear Halo: Surrounding these dark nuclei is a clear, empty-looking zone or “halo.” This is the optically clear zone created by the viral proteins disrupting the cell’s internal structure.
-
Summary
This image perfectly captures the essence of a squamous papilloma. We can see:
-
A papillary growth pattern.
-
Supported by central fibrovascular cores.
-
Composed of thickened squamous epithelium showing clear evidence of koilocytes.
These features together create the complete microscopic picture of a benign, HPV-induced squamous papilloma.
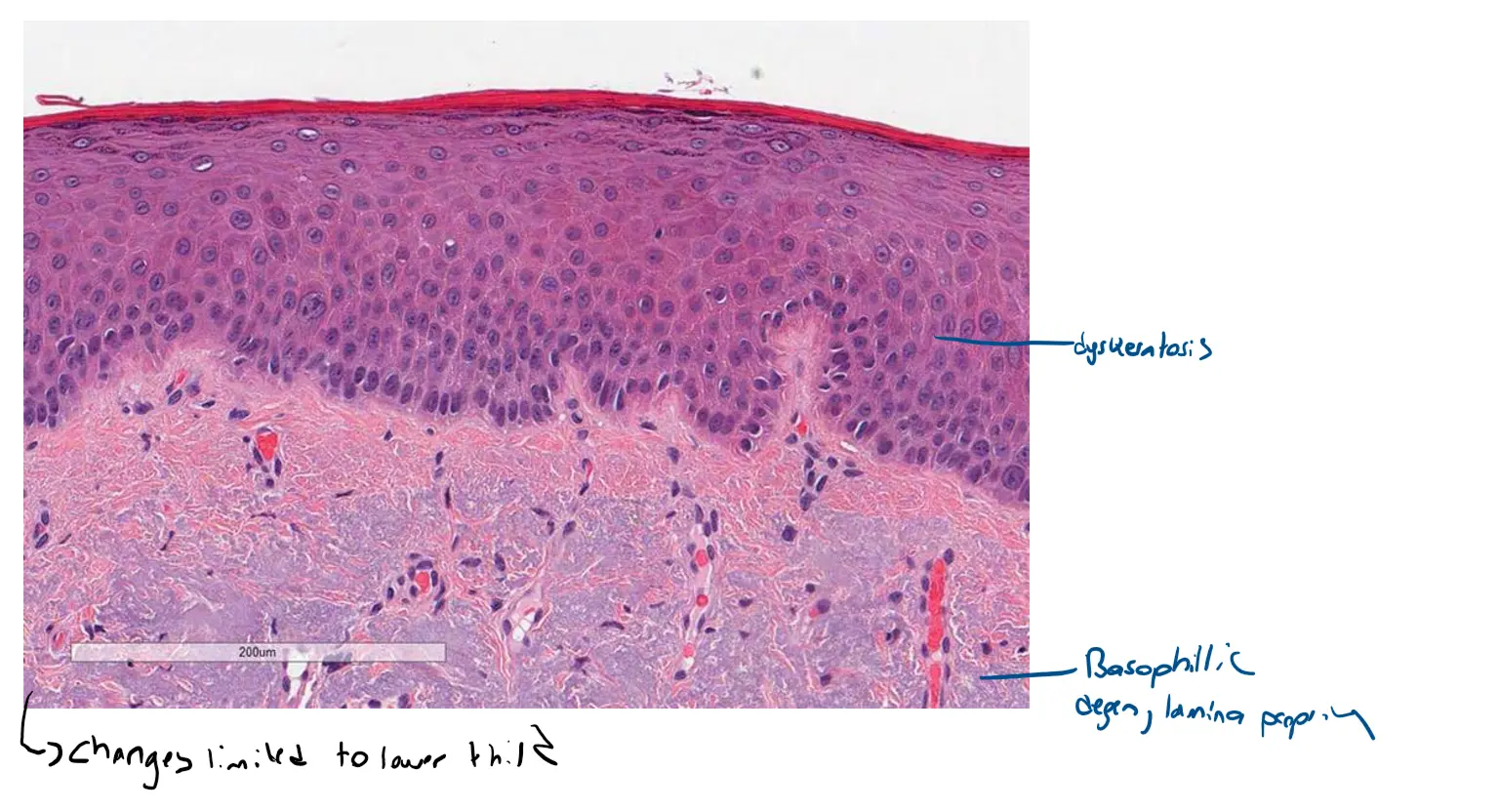
Case 3 Mild Epithelial Dysplasia
Of course. That’s an excellent question. Understanding the difference between mild and severe epithelial dysplasia comes down to assessing the extent and severity of specific architectural and cellular changes.
The primary difference is how far the disordered cells extend up the thickness of the epithelium.
Using your image as a reference for mild dysplasia, let’s break down the key differences.
🔬 Grading Dysplasia: From Mild to Severe
Epithelial dysplasia is graded based on a combination of disordered architecture and abnormal cell features (atypia). The most critical factor for grading is the vertical involvement of the epithelium.
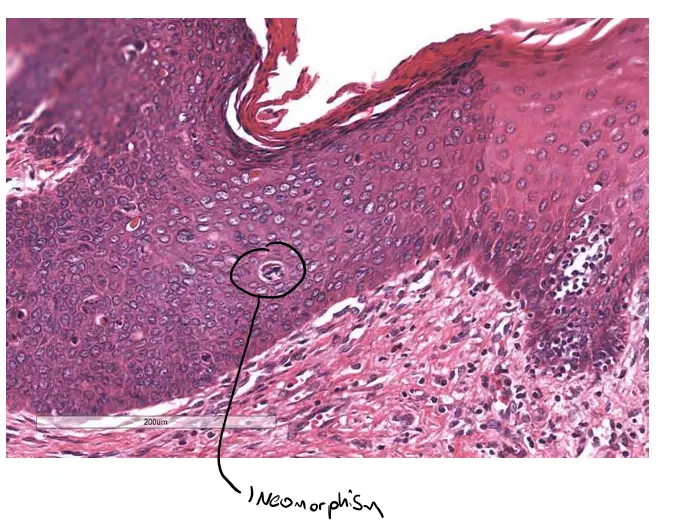
Mild Epithelial Dysplasia (As seen in your image)
In mild dysplasia, the abnormal changes are confined to the basal and parabasal layers, which is the lower one-third of the epithelium.
-
Architectural Changes: There is some loss of the normal, orderly maturation. You can see basal cells that are more crowded and disorganized than usual.
-
Cellular Changes: Some cells may have slightly larger, darker nuclei (hyperchromasia) and a higher nuclear-to-cytoplasmic ratio.
-
Key Feature: The upper two-thirds of the epithelium still show evidence of maturation. Notice in your image how the cells near the top surface are flatter and more organized, resembling normal tissue.
In your image, you can see the cellular crowding and darker nuclei are concentrated at the bottom of the rete ridges (the downward-pointing epithelial projections). The cells mature and flatten as they approach the top surface.
Severe Epithelial Dysplasia / Carcinoma in Situ
In severe dysplasia, the abnormal changes are much more pronounced and extend into the upper one-third of the epithelium. When the full thickness is involved, it is called Carcinoma in Situ (CIS).
-
Architectural Changes: There is a near-complete loss of maturation. Cells at the top surface may still be large and round with prominent nuclei instead of being flat and condensed. Mitotic figures (dividing cells), which should only be at the very bottom, can be found in the middle or even upper layers.
-
Cellular Changes: The abnormalities are much more significant. There is marked variation in nuclear size and shape (pleomorphism), prominent and dark nuclei, and a very high nuclear-to-cytoplasmic ratio.
-
Key Feature: The disordered, immature-looking cells occupy most, if not all, of the epithelial thickness.
Comparison Table
| Feature | Mild Dysplasia | Severe Dysplasia / Carcinoma in Situ (CIS) |
|---|---|---|
| Primary Location | Lower 1/3 of epithelium | Upper 1/3 to Full Thickness |
| Cellular Maturation | Present in the upper layers | Largely absent; loss of stratification |
| Nuclear Atypia | Mild changes in size and color | Marked variation (pleomorphism) and darkness |
| Mitotic Figures | Few, confined to the basal layer | More numerous, may be found in upper layers |
In essence, you can tell the difference by looking at how far up the “ladder” of the epithelium the disordered, basal-like cells have climbed. In your image, they are at the bottom. In severe cases, they have climbed nearly to the top.
Would you like me to explain the risk of progression from mild and severe dysplasia to invasive cancer?
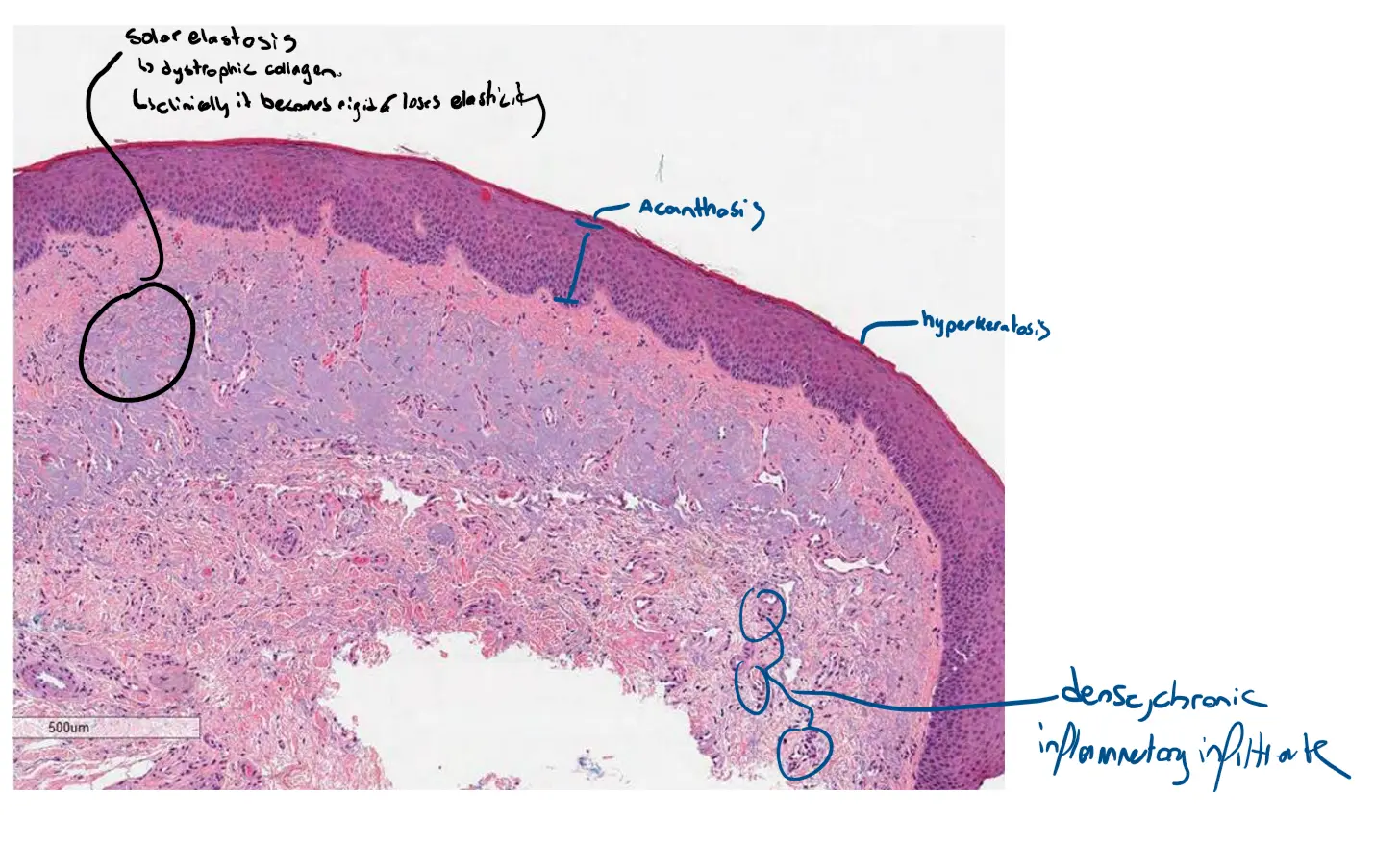
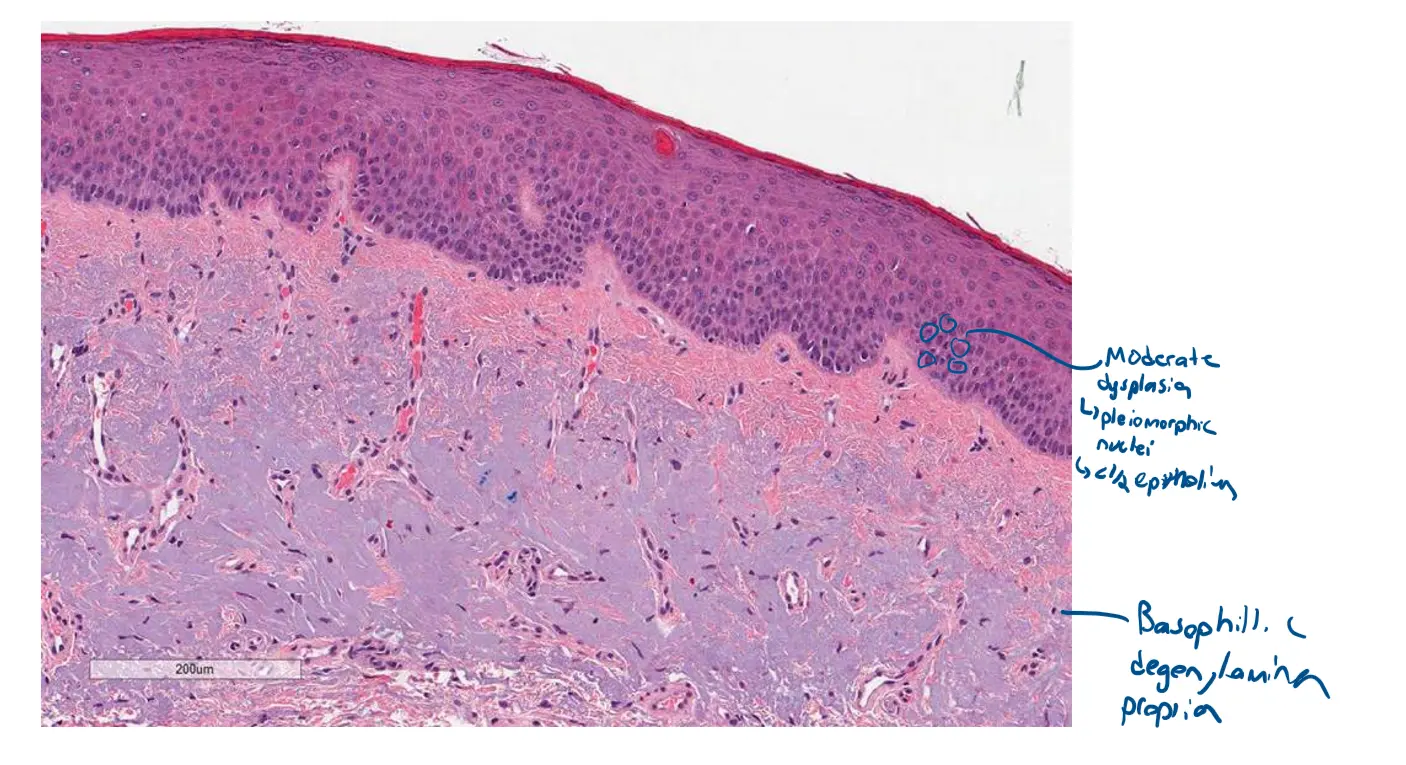
Case 4 Severe Epithelial Dysplasia
Case 5 : Actinic Cheilitis