Oral Potentially Malignant Disorders and Oral Cancer
- ==Progression from normal mucosal variations to potentially malignant lesions==
- ==Presentation of squamous cell carcinoma==
Course Presentation1
A/Prof Omar Kujan
BDS DipOPath MSc MFDS RCPS PhD FRCPath
Clinical Focus
This lecture series emphasizes clinical practice, diagnostic judgment, and the dentist's role in early detection, bridging the gap between theoretical pathology and chairside evaluation.
Learning Outcomes
Scope of Study2
- *Oral potentially malignant disorders
- Leukoplakia
- Erythroplakia
- Oral submucous fibrosis
- Palatal lesions in reverse smokers
- Actinic cheilitis
- Lichen planus
- Lupus erythematosus
- Oral cancer
Clinical and Diagnostic Framework3
- Aetiology and pathogenesis
- Clinical features
- Histopathologic features
- Diagnosis
- Treatment
Principles of Clinical Oral Diagnostication
Understanding the baseline of healthy tissue is the fundamental prerequisite for effective clinical oral diagnostication.
A critical component of clinical evaluation is the ability to recognize normal variations and developmental disorders. Without a firm grasp of normal anatomy, a clinician cannot accurately identify abnormal changes.
Importance of Normal Anatomy and Histology4
Requirements for Clinical Assessment5
To effectively recognize changes in normal tissues, the clinical oral diagnostician must possess a thorough and complete knowledge of the following:
- The normal oral cavity.
- Surrounding anatomical regions.
- Visual Inspection: Looking for changes in color, texture, and symmetry.
- Palpation: Checking for consistency (e.g., induration or friability) and lymphadenopathy.
- Holistic View: Integrating the clinical appearance with the patient’s social and medical history.
Recognition of Abnormal Changes
Initial Steps in Differential Diagnosis6
In learning to make a differential diagnosis of soft tissue lesions, the primary step is to identify the presence of abnormal changes during a clinical oral examination. These changes are typically categorized by alterations in:
- Function
- Structure
- Appearance
- Color Changes: Identifying red (erythematous), white (keratotic), or pigmented lesions.
- Texture/Consistency: Noting if a lesion is smooth, corrugated, exophytic (growing outward), or ulcerated.
Nicotine Stomatitis
- Presentation: Red dots (inflamed orifices of minor salivary gland ducts) surrounded by raised white keratotic areas on the hard and soft palate.
- Etiology: Common in heavy smokers due to heat and chemical irritation.
- Diagnostic Key: Correlation between the anatomical location of minor salivary glands and the patient's smoking history.
Epidemiology of Oral Cancer78910
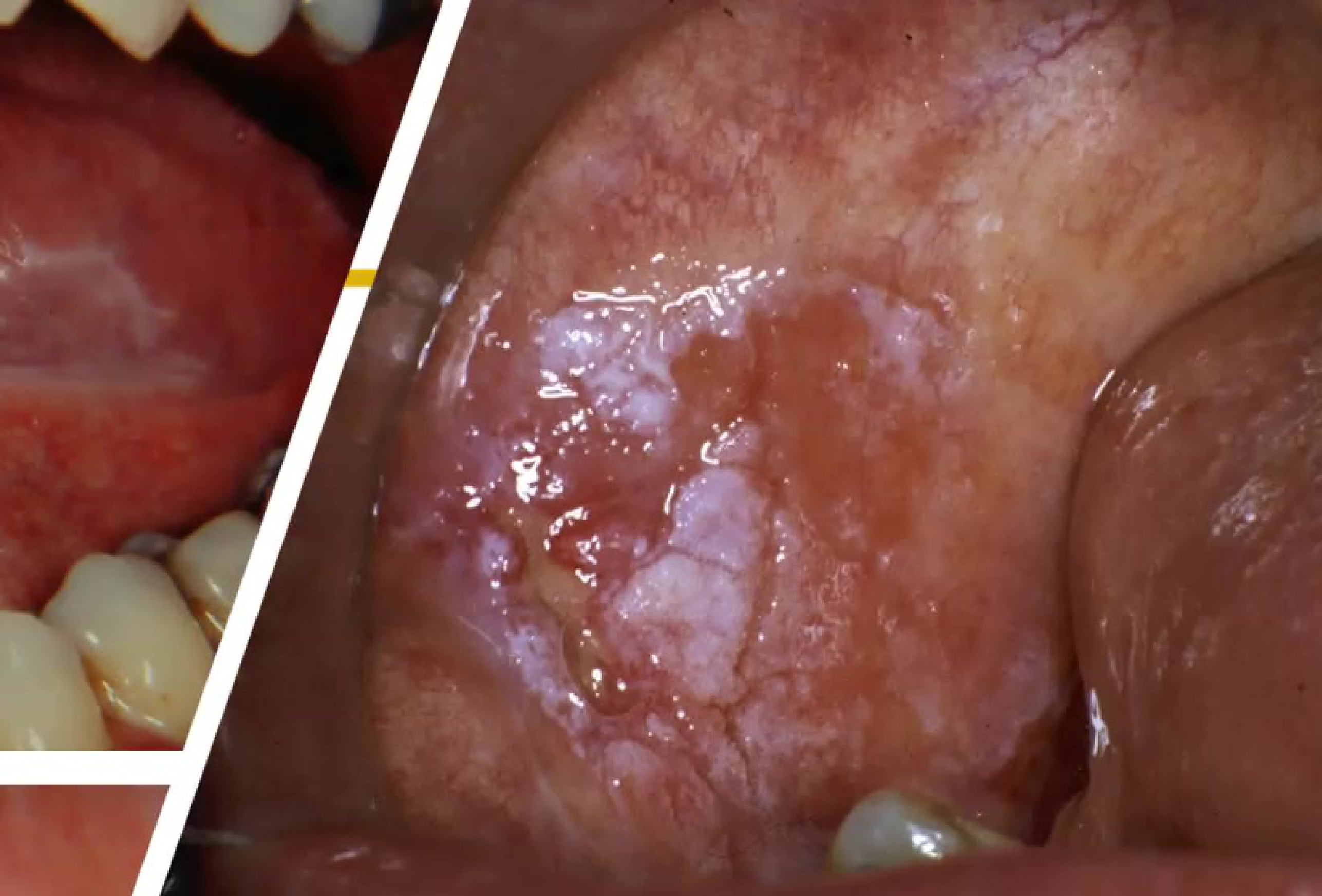
 Ulcer + swelling with surrounding white keratosis; history: non‑healing/persistent → SCC. |  Exophytic, keratotic gingival lesion; tissue very friable → SCC. | 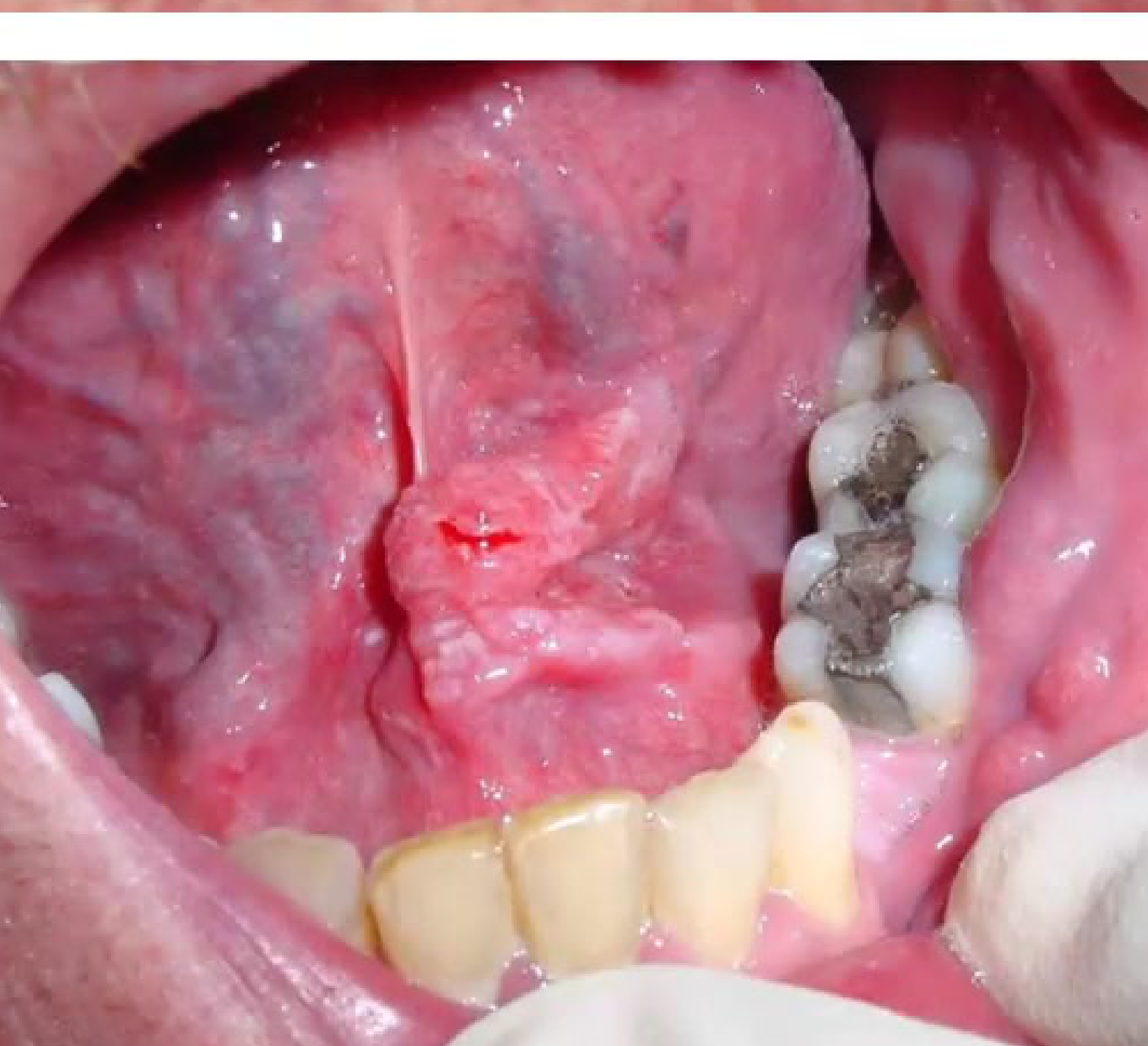 Lesion on floor of mouth and ventral tongue → SCC. |
 Subtle gingival change mimicking periodontitis but malignant on biopsy → SCC. |
Global Incidence and Trends
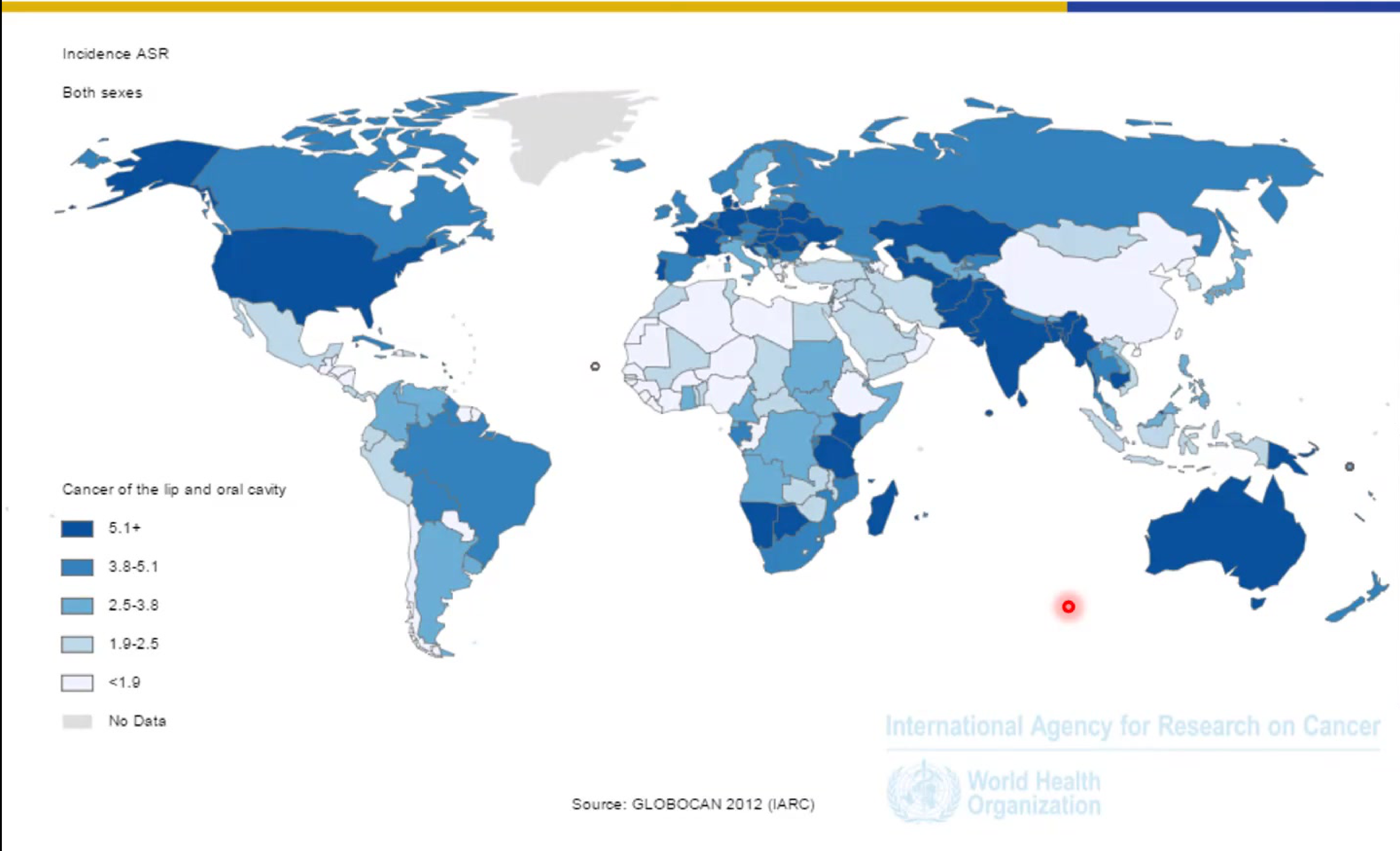
Global Incidence Overview11
Data regarding the global incidence of oral cancer is typically visualized through geographic mapping to identify high-burden regions.
Regional Trends and Statistics12
- India: Over 100,000 cases of oral cancer are diagnosed annually, with numbers currently increasing. (Males are most common)
- France: Reports the highest incidence rate of oropharyngeal cancer.
- Australia: During the period from 1982 to 2008, an annual increase of 3.2% was observed specifically in cancers of the base of the tongue
- Historically high rates of lip carcinoma were noted in Australia prior to the 1980s. but preventative measures helped reduce new cases of lip cancer successfully
Incidence Projections for 2035
 |  |
Global Forecast for Lip and Oral Cavity Cancer13
- Total Projected New Cases (2035): 494,897 (all ages, both sexes).
- Growth Drivers: The increase from 2012 levels is attributed to the demographic effect (population growth and aging
- Projections suggest a total 50% increase in the number of cases between 2012 and 2035.).
Source: GLOBOCAN 2012 (IARC).
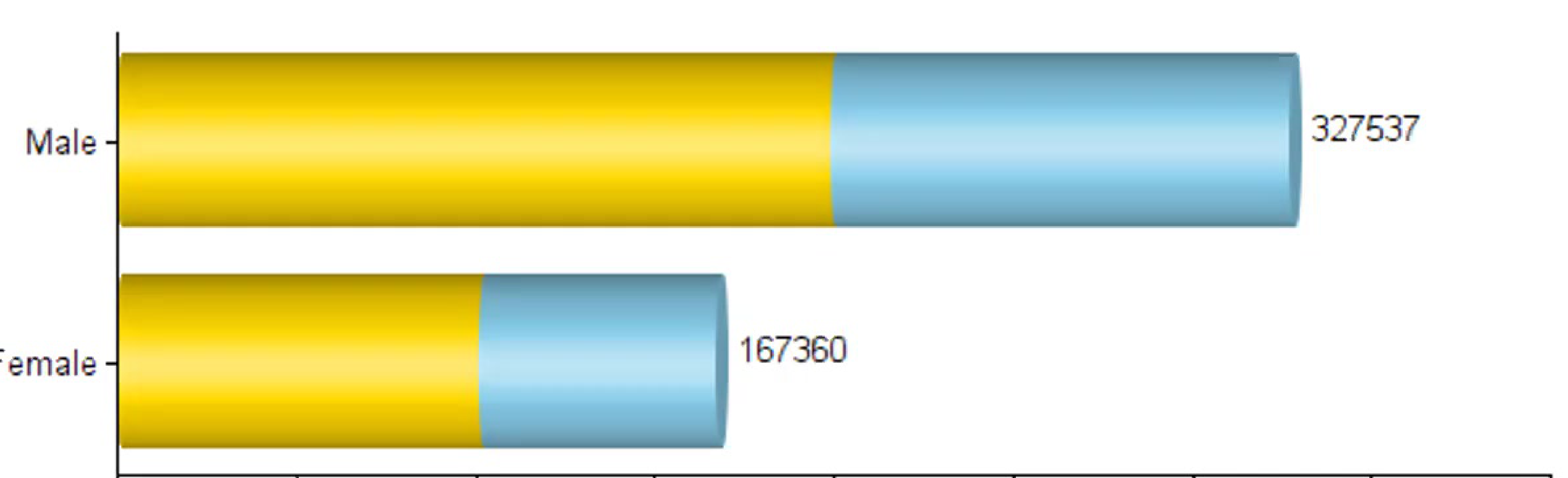
Gender-Specific Incidence Projections14
Projected number of new cases for lip and oral cavity cancers by 2035:
- Male: 327,537 cases
- Female: 167,360 cases
These projections represent the combined total of the baseline incidence recorded in 2012 and the anticipated demographic effect.
Mortality Rates and Projections
 |  |
 |  |
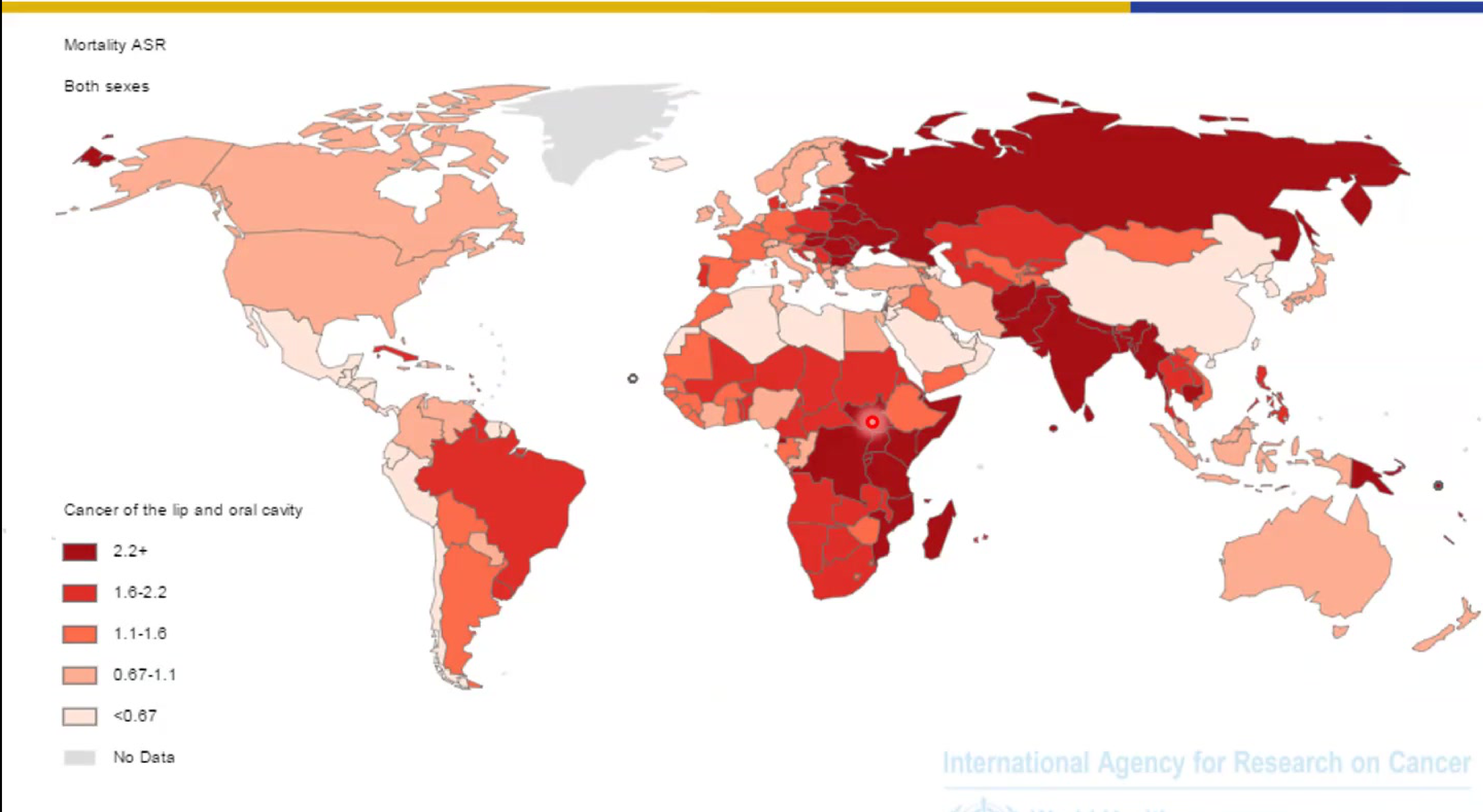
Age-Standardized Mortality Rates (ASR)15
Global mortality rates for cancer of the lip and oral cavity (both sexes) are categorized by the following ASR ranges:
Clinical Impact
Mortality remains high primarily due to late diagnosis; early detection is the most significant factor in improving survival.
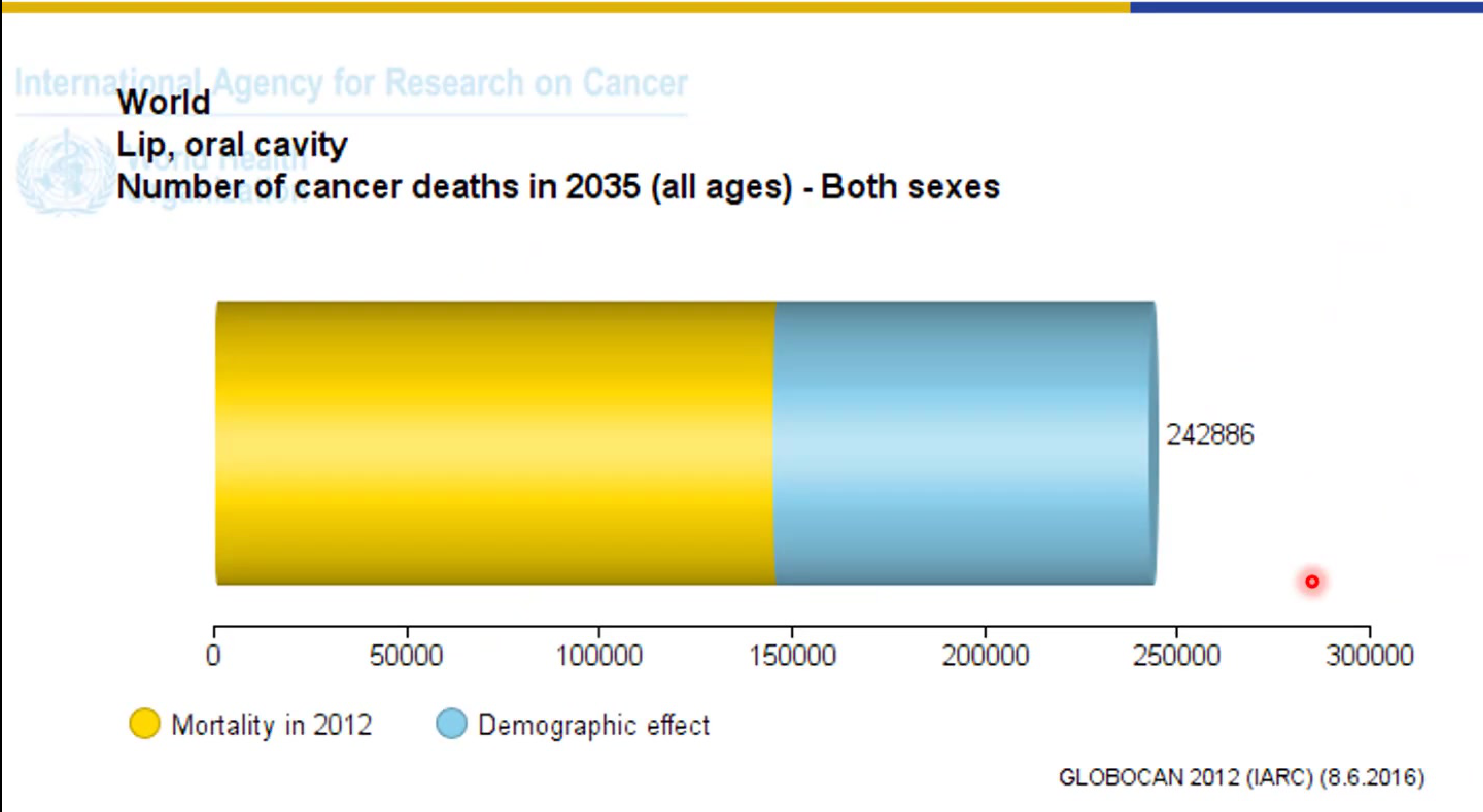
Global Mortality Forecast16
- Total Projected Deaths (2035): 242,886 (all ages, both sexes).
- Components of Change: The total reflects the mortality recorded in 2012 plus the projected demographic effect over the intervening years
- Mortality is expected to increase by approximately 50% by 2035.
- Southeast Asia currently holds the highest mortality rates globally.
- In Australia, the survival rate is approximately 60%, which is considered substandard and highlights the need for better screening..
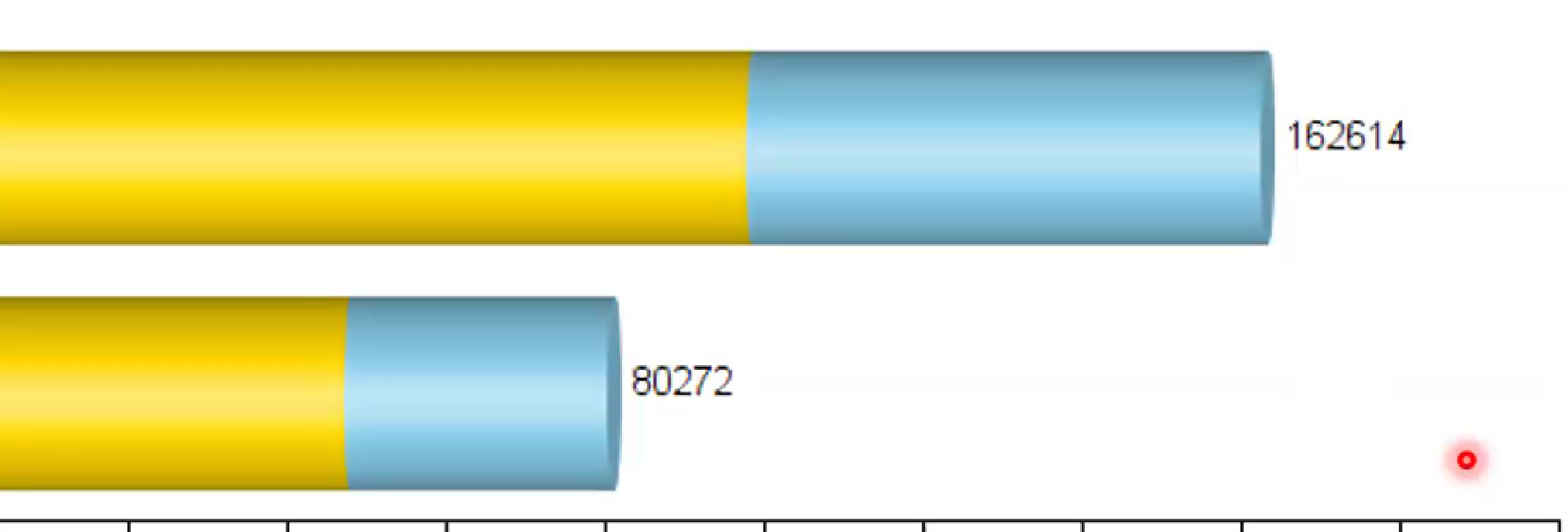
Mortality Projections by Gender (2035)17
| Gender | Mortality in 2012 | Demographic Effect | Total Projected Deaths (2035) |
|---|---|---|---|
| Male | ~97,000 | ~65,614 | 162,614 |
| Female | ~47,000 | ~33,272 | 80,272 |
Age Group Distribution
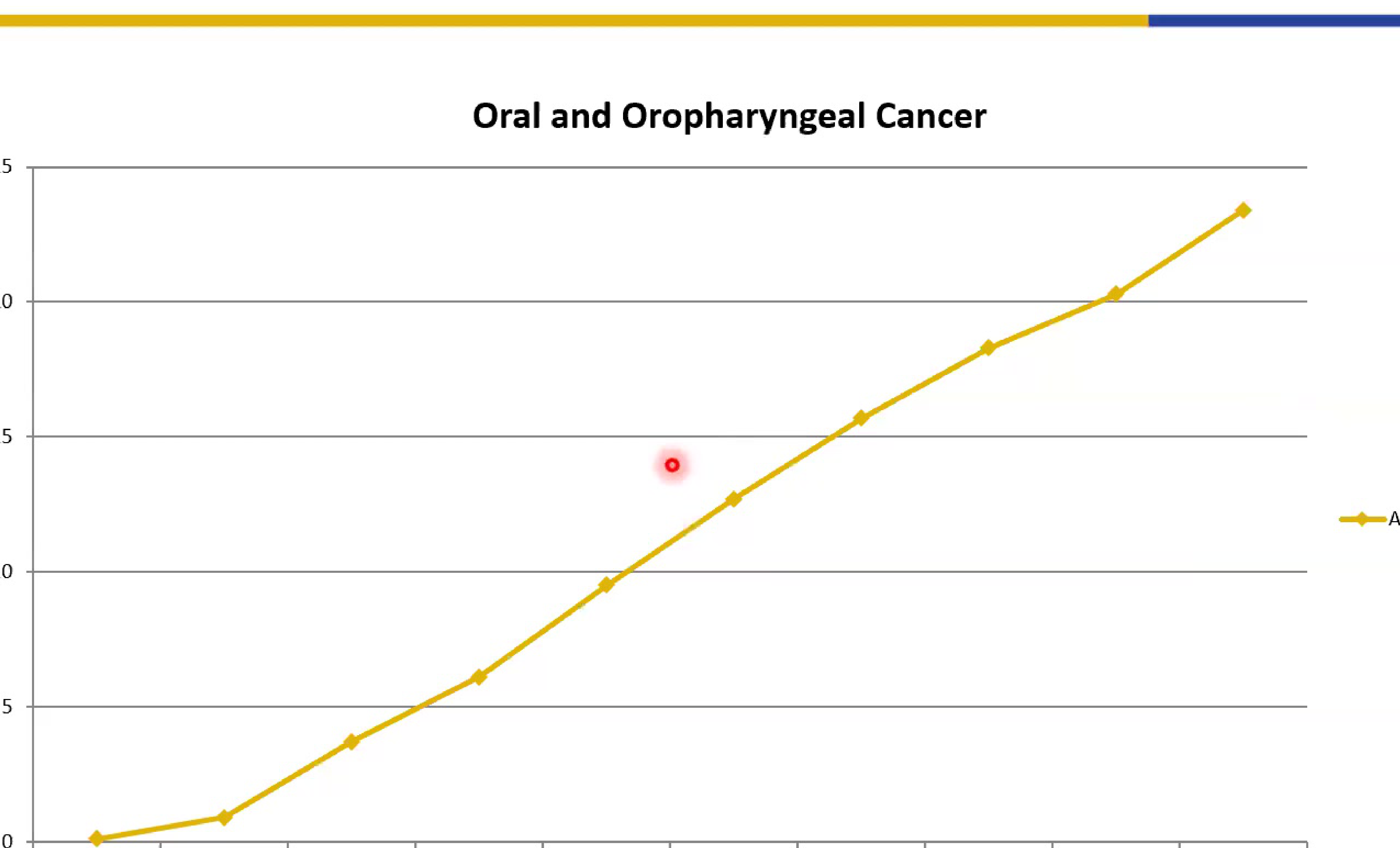
Incidence Rates by Age Group18
Data indicates a clear correlation between age and the incidence of oral and oropharyngeal cancer:
- Trend: Incidence rates show a steady rise as age increases.
- Key Observation: A significant increase in incidence is noted starting in the 55–59 age group.
- Measurement: Data is represented as Age-Standardized Rates (World
Emerging Trend
In Australia, there is a notable increase in oral cancer among females under age 40 who possess no known traditional risk factors.).
Source: GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 (2013).
Nomenclature and Classification19
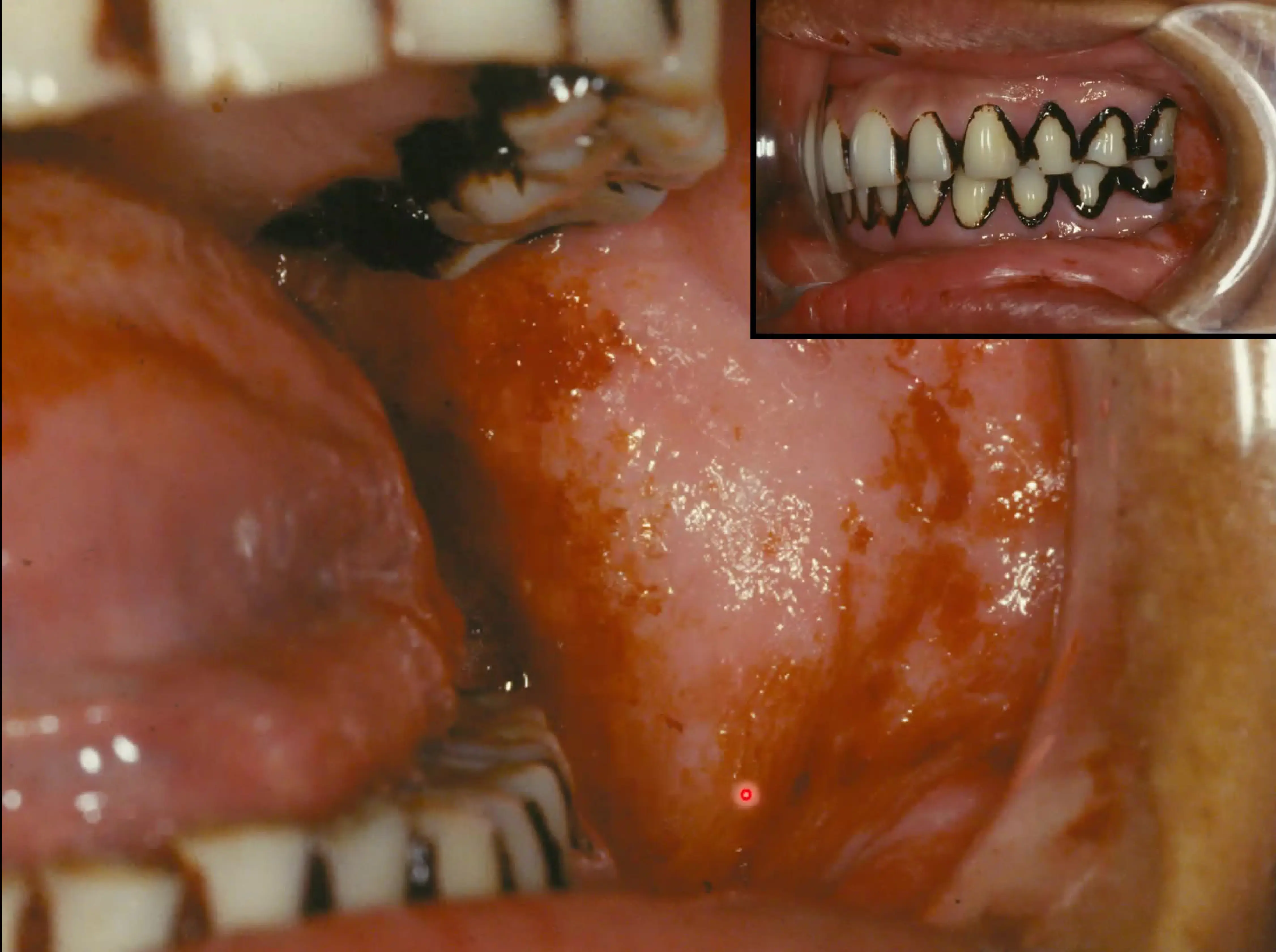
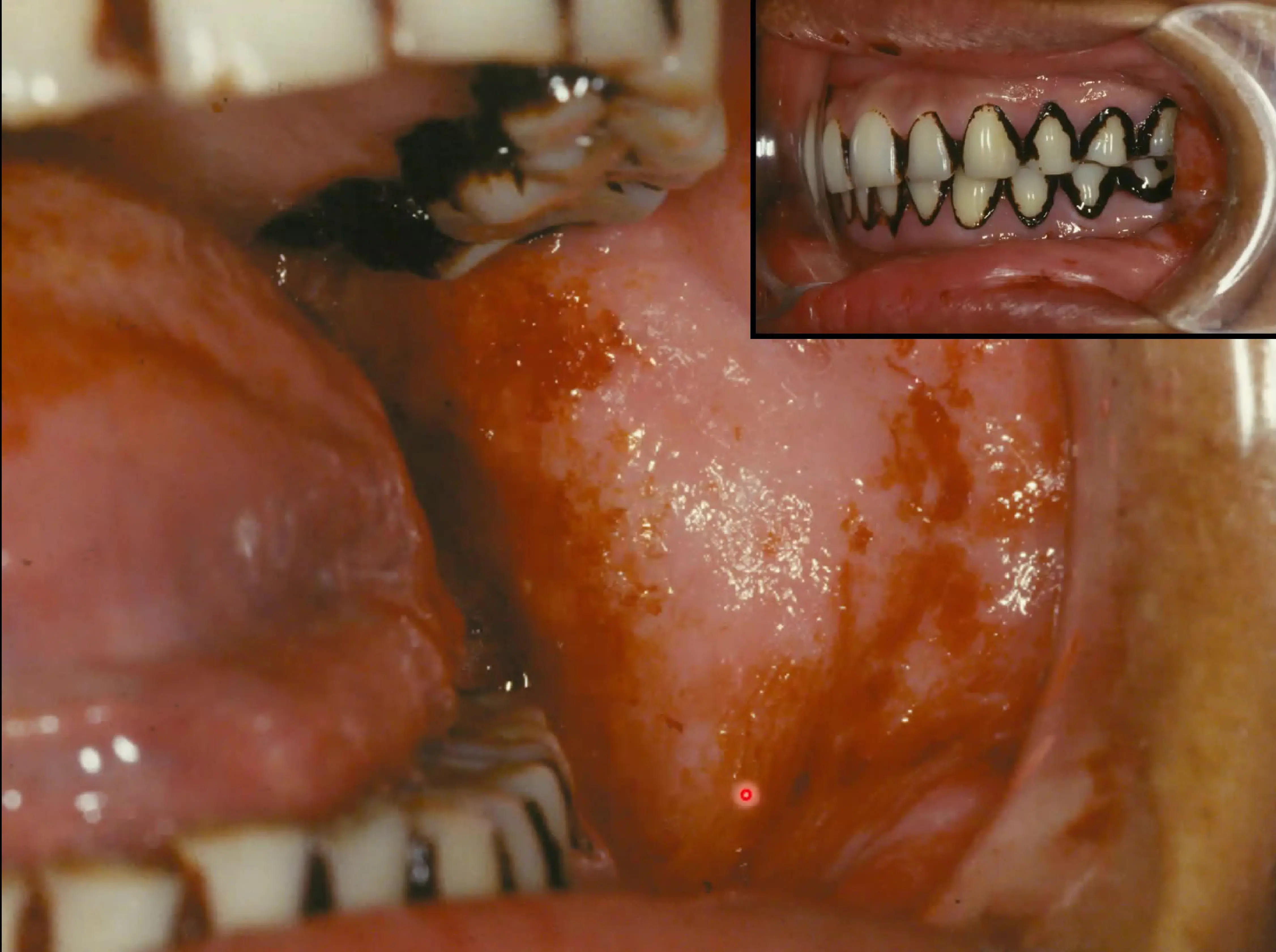
Non-Healing Ulcer (Squamous Cell Carcinoma)
- Presentation: A swelling associated with a non-healing ulcer, surrounded by white keratotic and red (erythematous) areas.
- Patient History: The patient reported the ulcer was persistent despite various self-treatments.
- Outcome: Biopsy confirmed Squamous Cell Carcinoma (SCC).
Definition of Oral Potentially Malignant Disorders20
Clinical Definition and Terminology21
Oral Potentially Malignant Disorders (OPMDs) refer to a group of lesions and conditions characterised by a variably increased risk of developing cancers of the lip (C00) and the oral cavity (C02-C06).
Various terms have been used in international literature to broadly describe clinical presentations that may potentially become cancer, including:
- "Oral Potentially Malignant Disorders" (OPMD) is now the internationally accepted standard term.
- Pre-cancer
- Precursor lesions
- Pre-malignant
- Intraepithelial neoplasia
- Potentially malignant
Clinical Presentation of OPMDs
 |  |
 |  |
OPMDs present with various mucosal changes:
- Leukoplakia: White color changes (can be thick, corrugated, or smooth).
- Erythroplakia: Velvety red changes (these carry the highest risk of malignancy).
- Erythroleukoplakia: Mixed red and white lesions.
Footnotes
-
Original PDF page 1: L10 OPMDs and Oral Cancer I slides, p.1 ↩
-
Original PDF page 2: L10 OPMDs and Oral Cancer I slides, p.2 ↩
-
Original PDF page 3: L10 OPMDs and Oral Cancer I slides, p.3 ↩
-
Original PDF page 4: L10 OPMDs and Oral Cancer I slides, p.4 ↩
-
Original PDF page 5: L10 OPMDs and Oral Cancer I slides, p.5 ↩
-
Original PDF page 6: L10 OPMDs and Oral Cancer I slides, p.6 ↩
-
Original PDF page 7: L10 OPMDs and Oral Cancer I slides, p.7 ↩
-
Original PDF page 8: L10 OPMDs and Oral Cancer I slides, p.8 ↩
-
Original PDF page 9: L10 OPMDs and Oral Cancer I slides, p.9 ↩
-
Original PDF page 10: L10 OPMDs and Oral Cancer I slides, p.10 ↩
-
Original PDF page 11: L10 OPMDs and Oral Cancer I slides, p.11 ↩
-
Original PDF page 12: L10 OPMDs and Oral Cancer I slides, p.12 ↩
-
Original PDF page 13: L10 OPMDs and Oral Cancer I slides, p.13 ↩
-
Original PDF page 14: L10 OPMDs and Oral Cancer I slides, p.14 ↩
-
Original PDF page 15: L10 OPMDs and Oral Cancer I slides, p.15 ↩
-
Original PDF page 16: L10 OPMDs and Oral Cancer I slides, p.16 ↩
-
Original PDF page 17: L10 OPMDs and Oral Cancer I slides, p.17 ↩
-
Original PDF page 18: L10 OPMDs and Oral Cancer I slides, p.18 ↩
-
Original PDF page 19: L10 OPMDs and Oral Cancer I slides, p.19 ↩
-
Original PDF page 21: L10 OPMDs and Oral Cancer I slides, p.21 ↩
-
Original PDF page 20: L10 OPMDs and Oral Cancer I slides, p.20 ↩