Diseases of the Salivary Glands1
Presented by:
Dr. Lalima Tiwari BDSC (UWA), DClinDent (OralMed) (UWA), MRACDS (OralMed), FOMAA
- Oral Medicine Specialist
- Clinical Senior Lecturer
Learning Outcomes
This section covers knowledge of diseases of the salivary glands, including localized salivary gland disorders, iatrogenic salivary gland disorders, and diseases with extra-oral manifestations that present with salivary gland disorders.
Developmental and Inflammatory Disorders2
- Discuss the clinical features, diagnosis, and treatment of salivary gland aplasia.
- Describe the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of:
- Mucoceles
- Sialolithiasis
- Sialadenitis
- Sjogren syndrome
- Sialadenosis
- Necrotizing sialometaplasia
Salivary Gland Neoplasms
Discuss the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of the following salivary gland neoplasms:
- Pleomorphic adenoma
- Warthin’s tumour
- Oncocytoma
- Mucoepidermoid carcinoma
- Acinic cell carcinoma
- Adenoid cystic carcinoma
- Polymorphous low grade adenocarcinoma
Xerostomia
Discuss the aetiology, clinical features, diagnosis, and management of dry mouth.
Clinical Assessment
The lecture emphasizes the importance of clinical assessment in the diagnosis of xerostomia, ensuring a comprehensive evaluation of the patient’s symptoms and salivary flow.
Anatomical and Physiological Review
Review of Anatomy
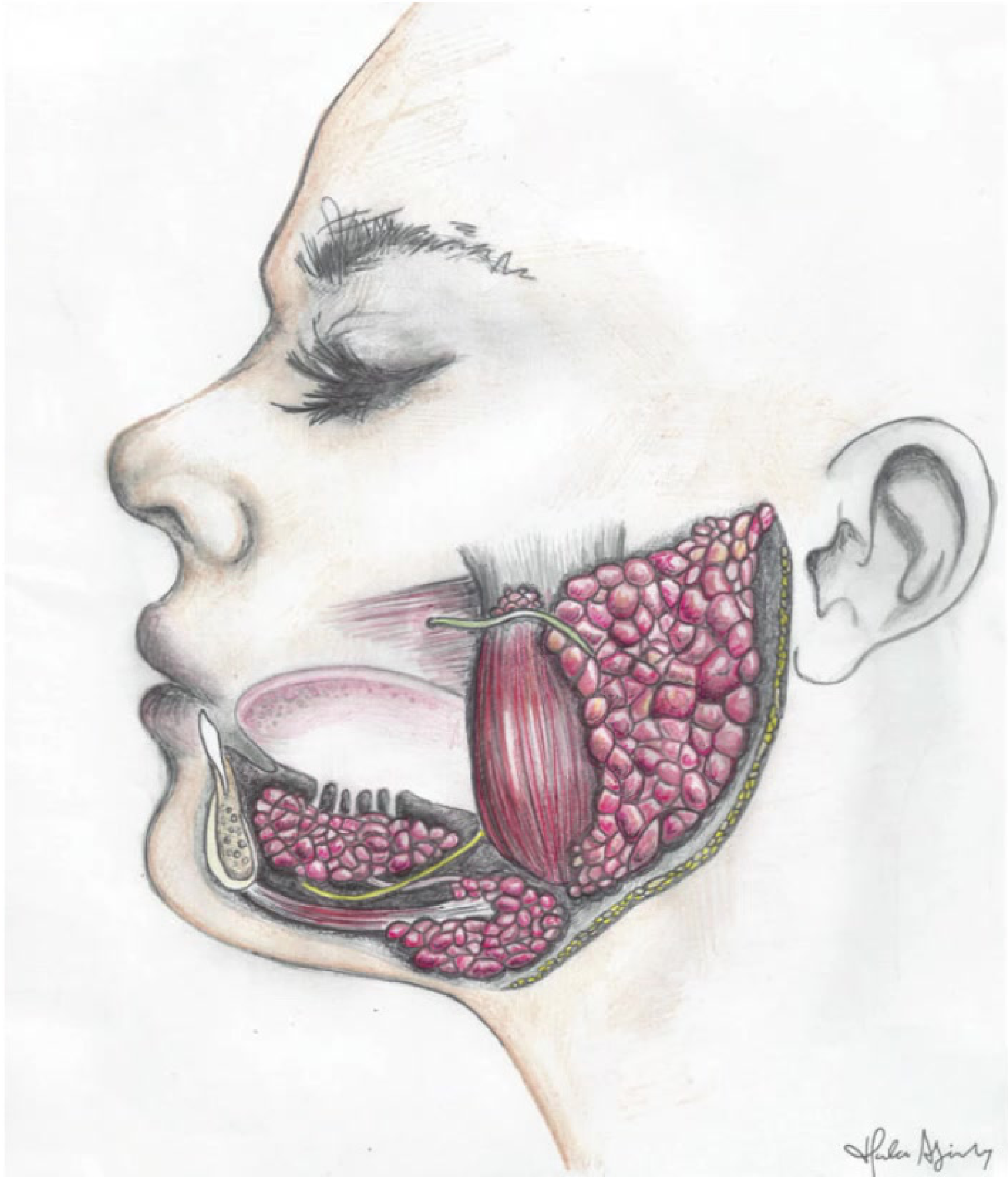
Major Salivary Glands3
The human anatomy includes three paired major salivary glands:
- ==Parotid Gland: The largest gland, located anterior to the ear and posterior to the mandibular ramus. The parotid duct (Stensen’s duct) passes through the masseter and opens near the maxillary second molar.==
- ==Submandibular Gland: Located in the floor of the mouth, folding around the mylohyoid muscle. Wharton’s duct opens at the anterior floor of the mouth.==
- ==Sublingual Gland: The smallest major gland, positioned anterior to the submandibular gland.==
Minor Salivary Glands
There are between 600 and 1000 minor salivary glands located throughout the oral cavity, including:
- Buccal, lingual, palatal, and labial mucosa
- Floor of mouth
Review of Histology
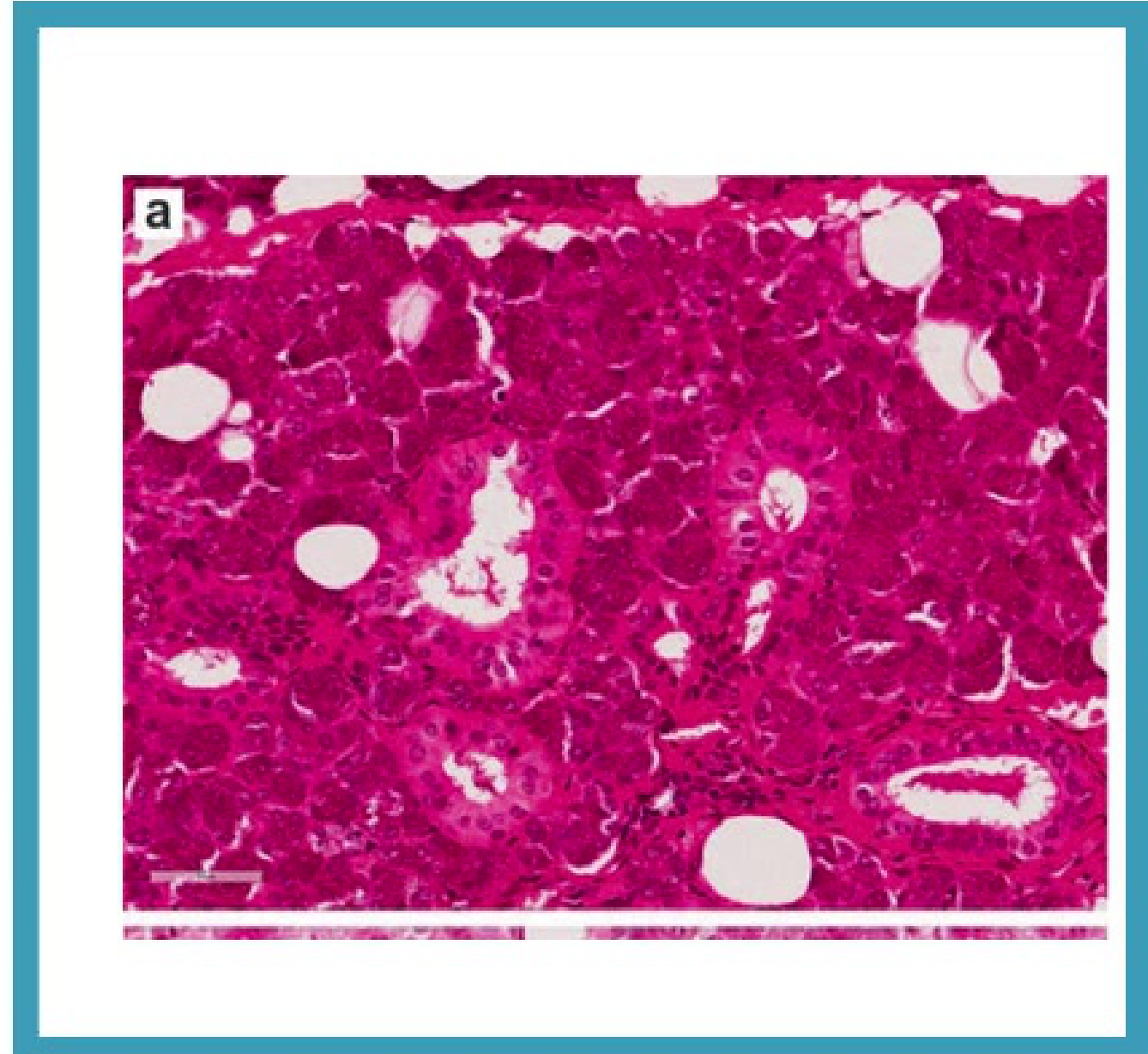
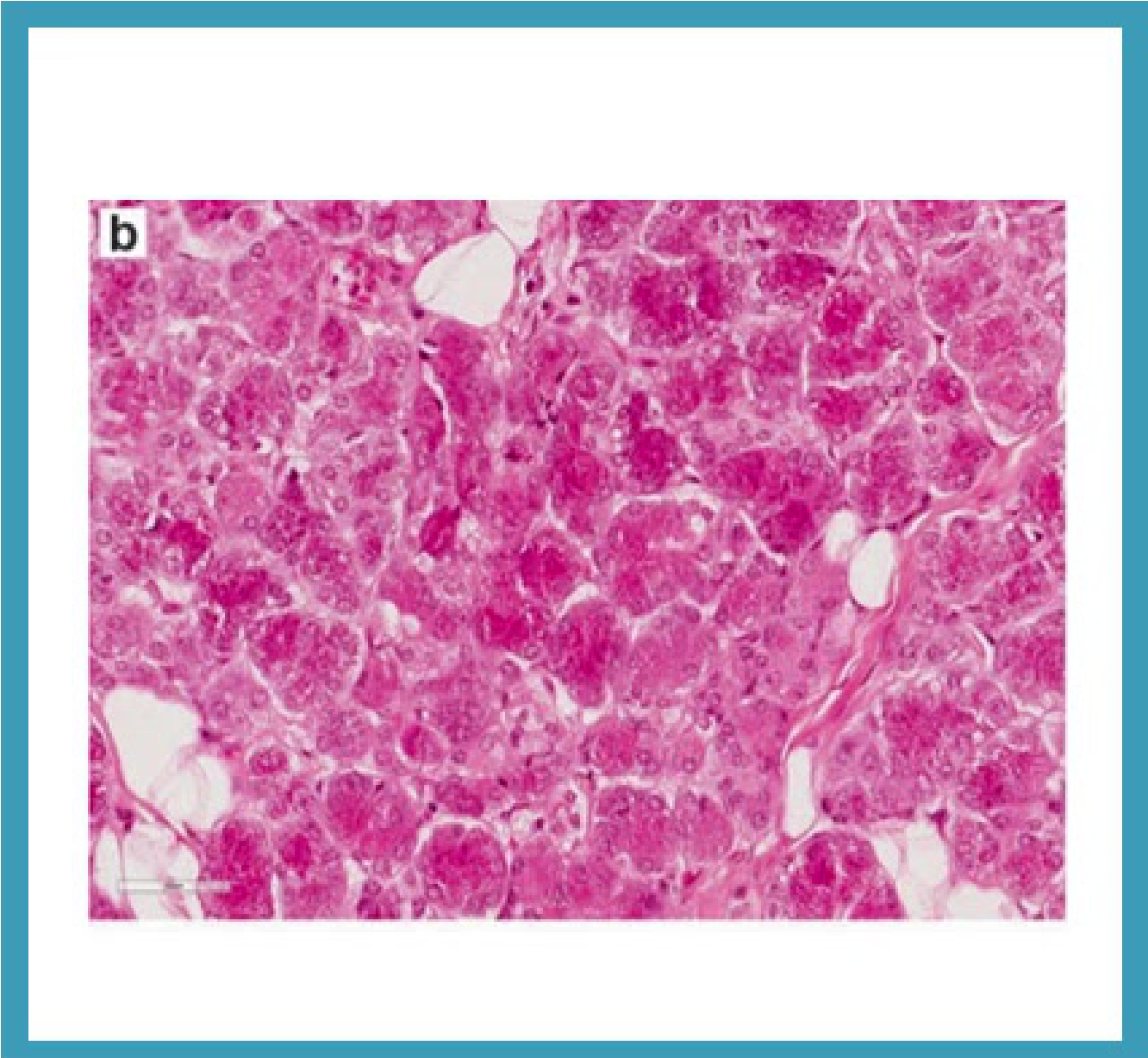
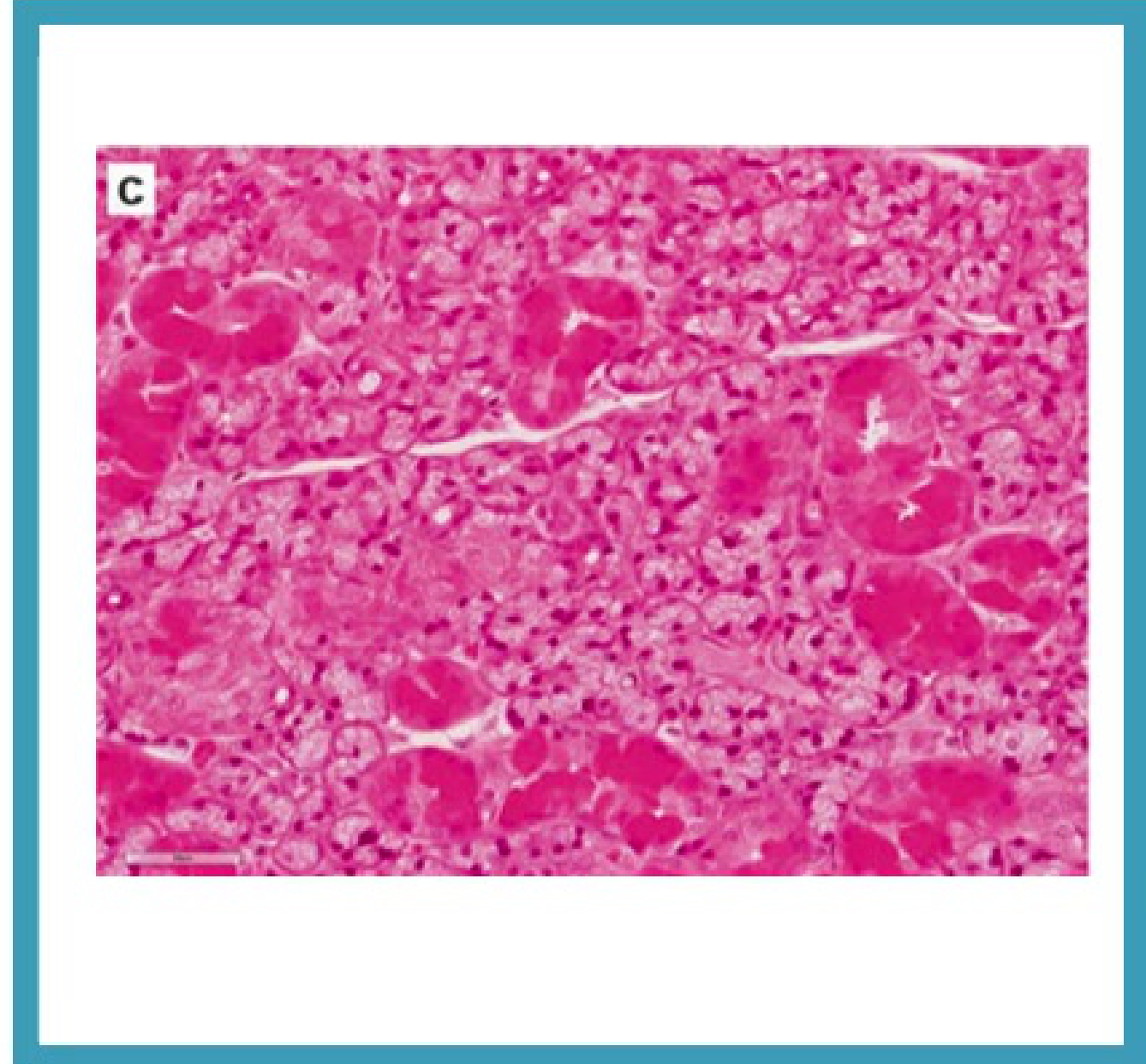
Glandular Composition4
- Parotid gland: Comprised of serous acini with pyramidal-shaped cells that have a basophilic appearance.
- Submandibular and Sublingual glands: Comprised of mixed mucous and serous acini.
- ==Minor Glands: Primarily mucous acini.==
- Structural Organization: Lobules of acini are separated by fibrous connective tissue septa and adipose tissue.
 |  |
 | 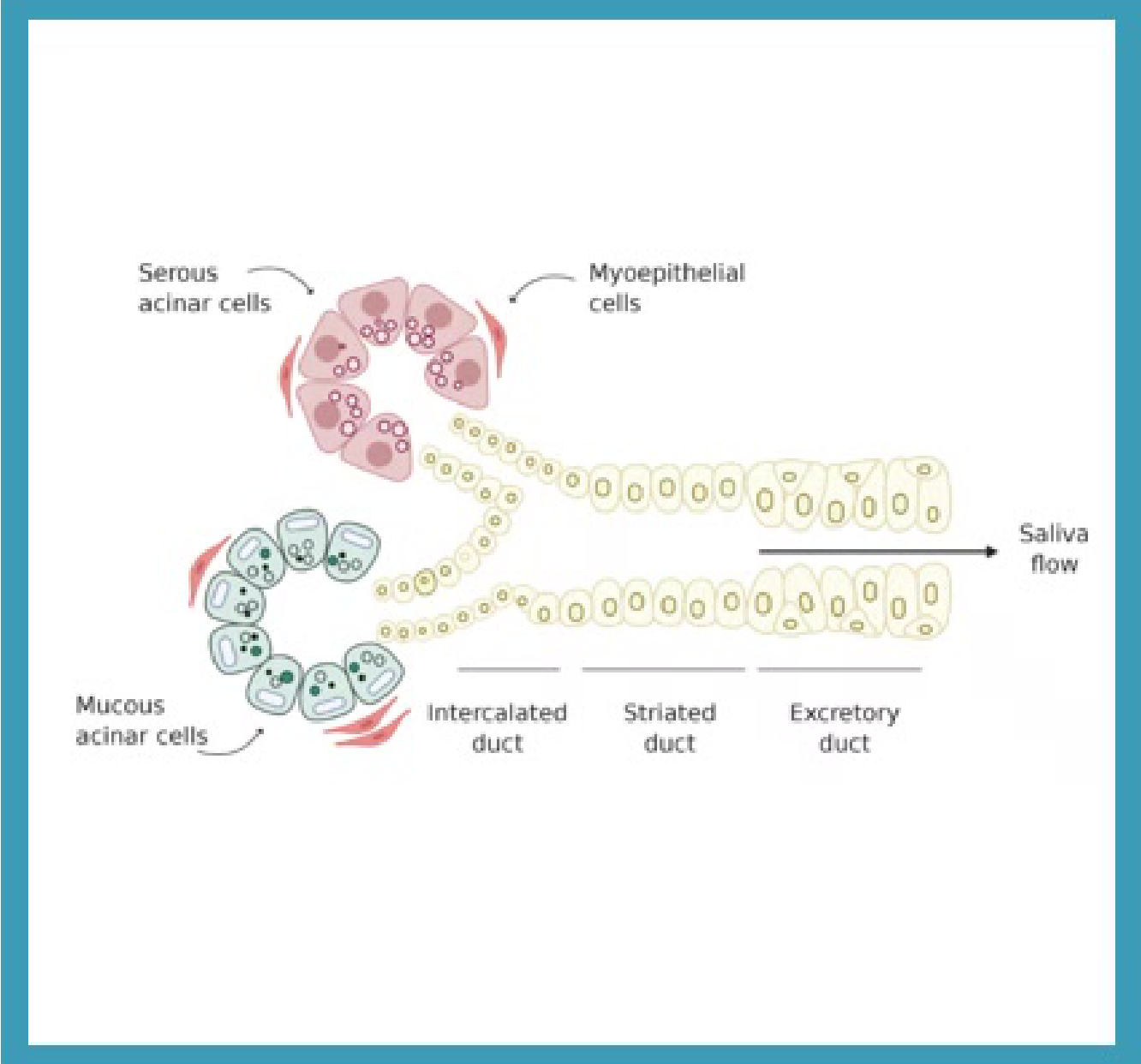 |
Ductal System
The ductal system is organized into specific functional units:
-
Intercalated ducts: Secretory function.
-
Striated ducts: Secretory function.
- Specifically responsible for modifying the ionic composition of saliva.==
-
Interlobular ducts: Excretory function.
Cellular Components
- Myoepithelial cells: Surround the acini and intercalated ducts to facilitate secretion.
- Basal cells: Associated with the striated and excretory ducts.
Review of Salivary Gland Physiology
Saliva Production and Flow Rates5
- Production Distribution:
- Major salivary glands account for 90% of saliva production.
- Minor salivary glands account for 10% of saliva production.
- 60% of unstimulated whole saliva is produced by the submandibular glands.
- Flow Rates:
- Unstimulated whole saliva: 0.2 – 0.5 ml/min.
- Stimulated whole saliva: 1.0 – 2.0 ml/min.
- Flow rates follow a circadian variation, peaking in the late afternoon.
- Flow reaches a minimum at night.
 |  |
 |
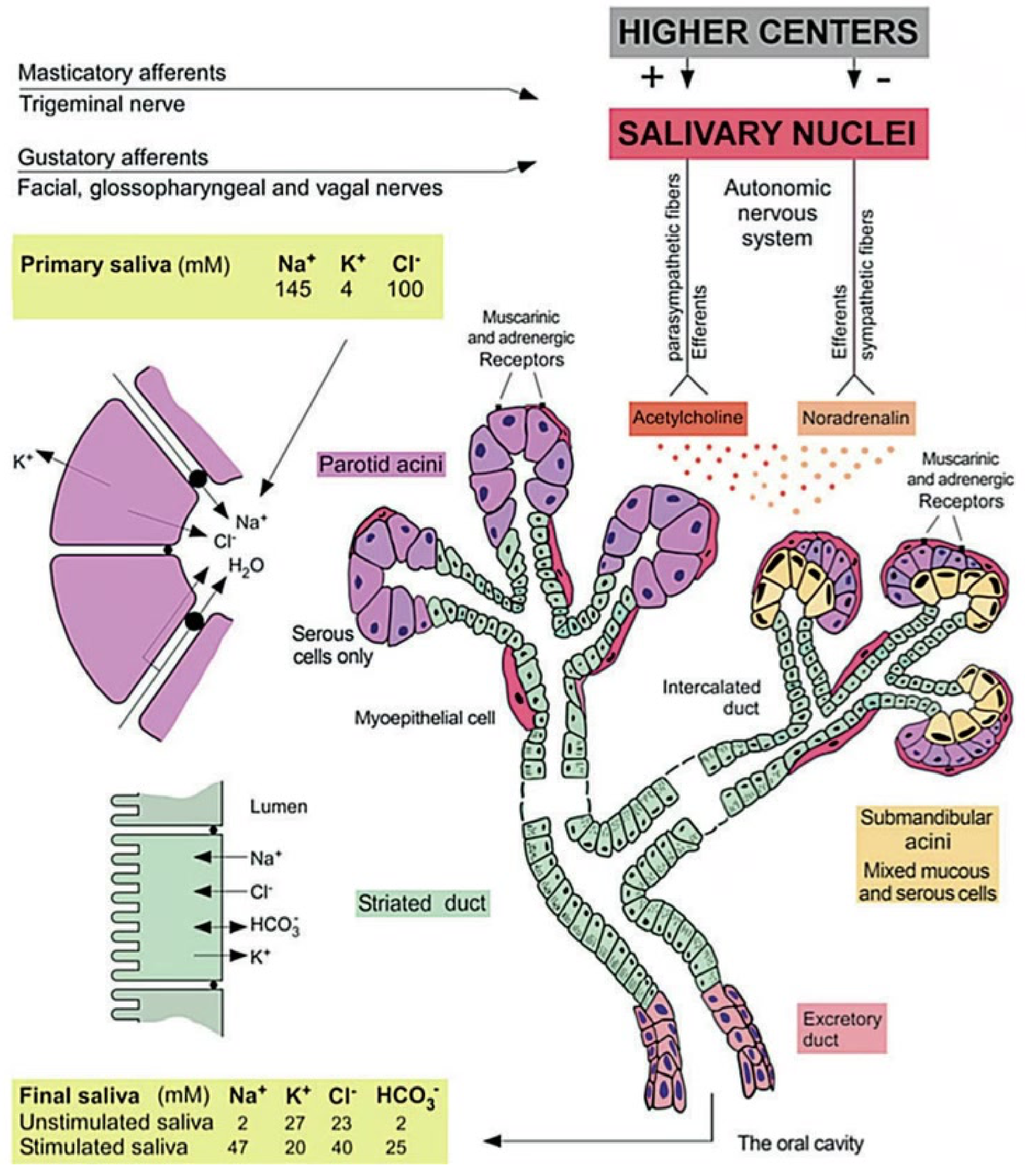
Mechanism of Secretion
- Primary Saliva: Produced by acinar cells.
- Modification: Ion composition is modified during transport through striated ducts.
- Sodium and chloride are reabsorbed.
- Bicarbonate and potassium are secreted by ductal cells.
- Transport: Myoepithelial cells help move saliva through the ducts.
- Final Product: Results in hypotonic saliva delivered to the oral cavity.
Neural Control and Regulation
Excretion is controlled by the autonomic nervous system via muscarinic and adrenergic receptors:
- Parasympathetic fibers: Release Acetylcholine.
- Sympathetic fibers: Release Noradrenalin.
- Afferent Pathways:
- Masticatory afferents: Trigeminal nerve.
- Gustatory afferents: Facial, glossopharyngeal, and vagal nerves.
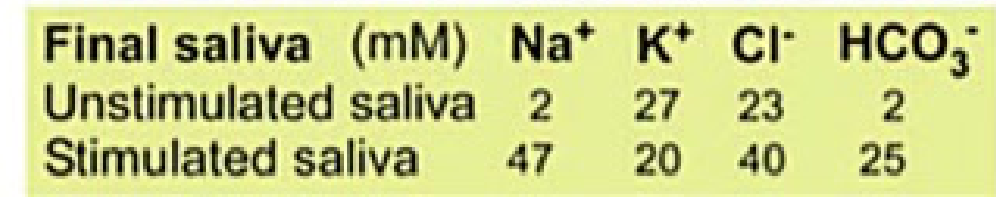
Saliva Ion Composition (mM)
| Saliva Type | Na⁺ | K⁺ | Cl⁻ | HCO₃⁻ |
|---|---|---|---|---|
| Primary Saliva | 145 | 4 | 100 | - |
| Final (Unstimulated) | 2 | 27 | 23 | 2 |
| Final (Stimulated) | 47 | 20 | 40 | 25 |
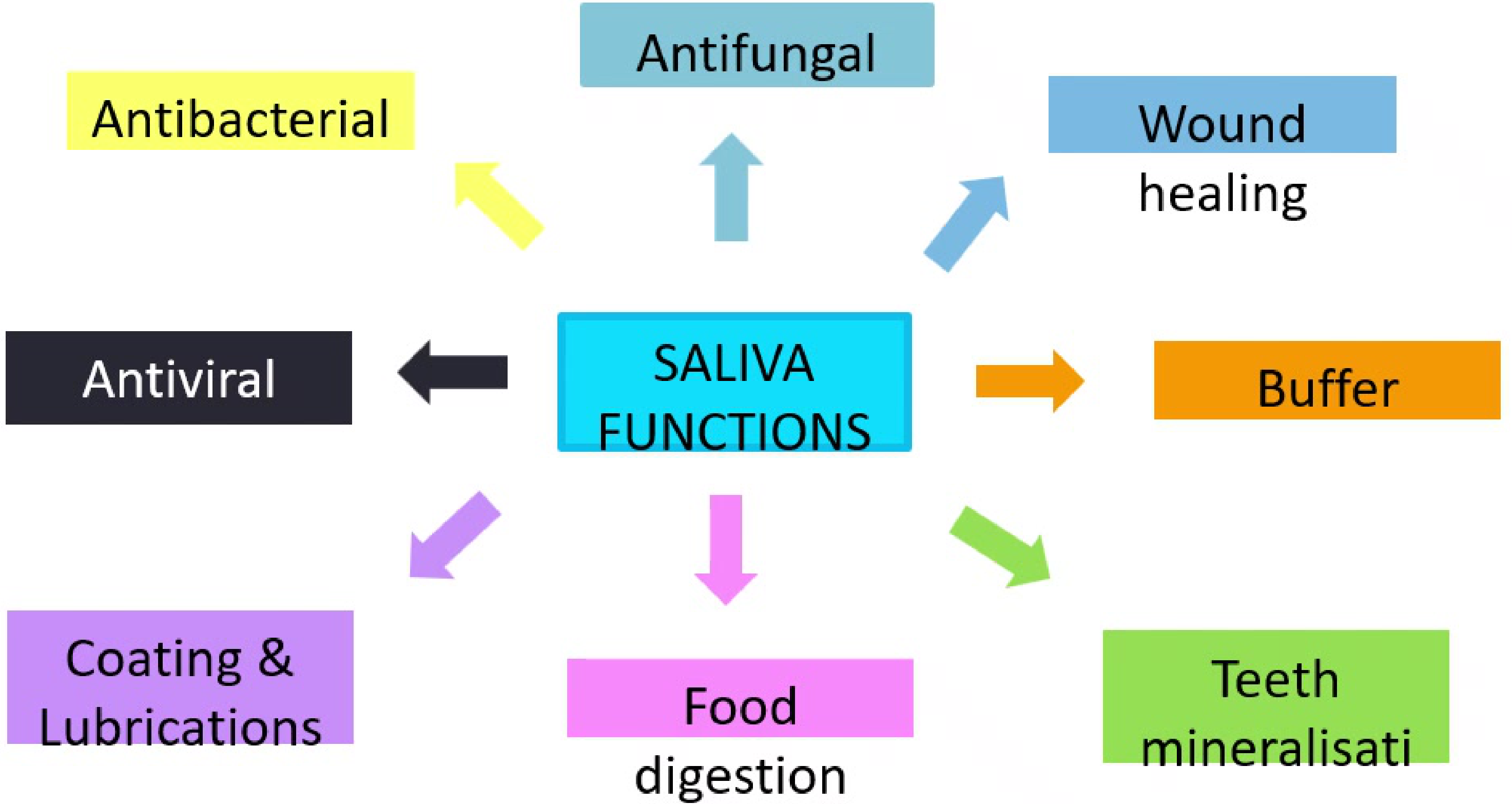
Functions of Saliva6
Saliva serves multiple critical roles in oral and systemic health:
- Protection and Defense:
- Antibacterial
- Antiviral
- Antifungal
- Oral Maintenance:
- Buffer (pH regulation)
- Teeth mineralization
- Coating and lubrication
- Wound healing
- Digestion:
- Food digestion
Salivary Gland Aplasia7
Salivary gland aplasia refers to the congenital absence of salivary glands. It is a rare condition that can be unilateral or bilateral and may occur as an isolated finding or as part of a hereditary syndrome.
Etiology and Incidence8
- Parotid gland aplasia has an estimated incidence of 1:5,000 live births.
- The higher frequency of parotid involvement is related to its earlier morphogenesis compared to other salivary glands.
Associated Syndromes of Ectodermal Tissues
- Ectodermal dysplasia
- Mandibulofacial dysostosis
- Hemifacial microsomia
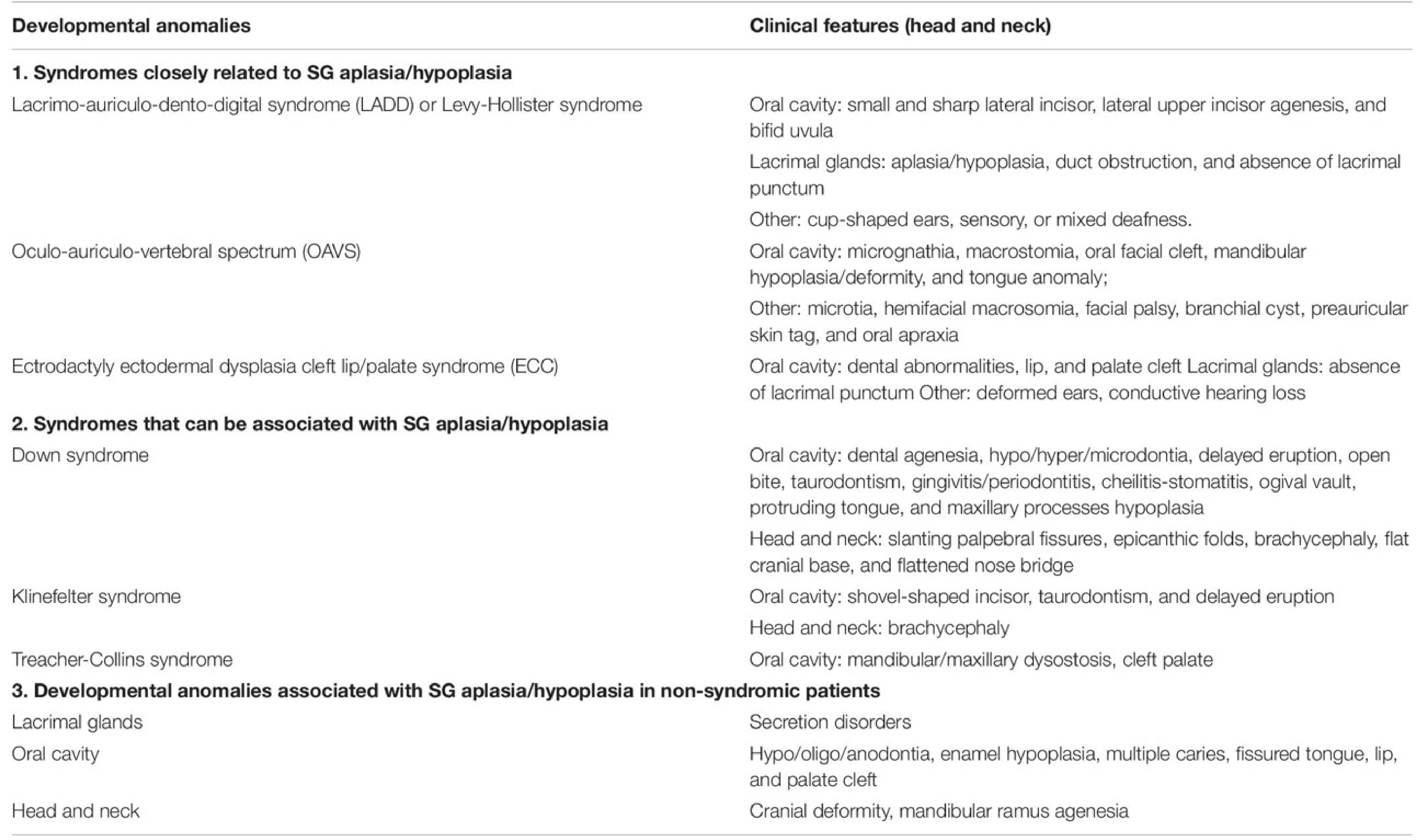
| Developmental Anomalies | Clinical Features (Head and Neck) |
|---|---|
| 1. Syndromes closely related to SG aplasia/hypoplasia | |
| Lacrimo-auriculo-dento-digital syndrome (LADD) or Levy-Hollister syndrome | Oral cavity: small and sharp lateral incisor, lateral upper incisor agenesis, and bifid uvula. Lacrimal glands: aplasia/hypoplasia, duct obstruction, and absence of lacrimal punctum. Other: cup-shaped ears, sensory, or mixed deafness. |
| Oculo-auriculo-vertebral spectrum (OAVS) | Oral cavity: micrognathia, macrostomia, oral facial cleft, mandibular hypoplasia/deformity, and tongue anomaly. Other: microtia, hemifacial macrosomia, facial palsy, branchial cyst, preauricular skin tag, and oral apraxia. |
| Ectrodactyly ectodermal dysplasia cleft lip/palate syndrome (ECC) | Oral cavity: dental abnormalities, lip, and palate cleft. Lacrimal glands: absence of lacrimal punctum. Other: deformed ears, conductive hearing loss. |
| 2. Syndromes that can be associated with SG aplasia/hypoplasia | |
| Down syndrome | Oral cavity: dental agenesis, hypo/hyper/microdontia, delayed eruption, open bite, taurodontism, gingivitis/periodontitis, cheilitis-stomatitis, ogival vault, protruding tongue, and maxillary processes hypoplasia. Head and neck: slanting palpebral fissures, epicanthic folds, brachycephaly, flat cranial base, and flattened nose bridge. |
| Klinefelter syndrome | Oral cavity: shovel-shaped incisor, taurodontism, and delayed eruption. Head and neck: brachycephaly. |
| Treacher-Collins syndrome | Oral cavity: mandibular/maxillary dysostosis, cleft palate. |
| 3. Developmental anomalies in non-syndromic patients | |
| Lacrimal glands | Secretion disorders. |
| Oral cavity | Hypo/oligo/anodontia, enamel hypoplasia, multiple caries, fissured tongue, lip, and palate cleft. |
| Head and neck | Cranial deformity, mandibular ramus agenesis. |
SG: salivary gland.
Clinical Features of Aplasia9
The clinical presentation of salivary gland aplasia is dependent on the number of missing glands. While some patients can be asymptomatic, others experience variable degrees of xerostomia and oral dryness.
 |  |
Oral Mucosal and Dental Impact10
- Erythematous oral mucosa
- Glossitis and tongue papillary atrophy
- Cheilitis and exfoliative lips
- Chronic erythematous candidiasis
- Oral ulcers
- Increased risk of dental caries, teeth erosion, and periodontal disease
Functional and Physical Signs
- Hoarseness and dysphagia
- Oropharyngeal symptoms
- Absence of parotid papillae or submandibular orifices
- Lack of saliva production upon palpation
- Halitosis (bad breath) resulting from reduced salivary flow
- Facial asymmetry
Clinical documentation and literature reviews highlight unusual patterns of dental damage associated with salivary gland aplasia and hypoplasia, particularly in cases involving systemic conditions such as Down syndrome.
Major Salivary Gland Aplasia in Down Syndrome
A clinical case of aplastic salivary glands associated with Down Syndrome. Intraoral findings included a lack of parotid duct openings, a fissured tongue with depapillation, and significant dental erosion.
Diagnosis and Management of Aplasia11
Diagnostic Methods12
- History: Comprehensive patient medical and dental history.
- Examination findings: Clinical assessment of oral dryness and ductal orifices.
- Imaging:
- Ultrasonography
- Computed tomography (CT)
- Magnetic resonance imaging (MRI)
Management Strategies
- Symptom Relief: Use of saliva substitutes.
- Lifestyle Changes:
- Increase water intake
- Limit irritating foods
- Maintain a low-sugar diet
- Preventative Care:
- Regular dental examinations
- Use of fluoride-based dental products
- High-fluoride products (e.g., NeutraFluor 5000) to prevent rampant decay
This section covers the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of the following conditions:
- Mucoceles
- Sialolithiasis
- Sialadenitis
- Sjogren syndrome
- Sialadenosis
- Necrotizing sialometaplasia
Non-Neoplastic Salivary Gland Diseases
Mucoceles and Ranulas
Overview13
- Mucoceles: Cavities filled with mucus that present as benign soft tissue masses in the oral cavity (mucous extravasation cyst).
- Ranula: A mucocele located specifically in the floor of the mouth (mucous retention cyst).
Epidemiology
- Very common occurrence.
- Young persons are the most frequently affected demographic.
- The high incidence in children and young adults is primarily due to higher rates of local trauma.
Aetiopathogenesis14
- Mucoceles: Often associated with a history of trauma, resulting in the leakage of fluid from the ducts or acini into the surrounding tissue.
- Mucous Retention Cysts (Ranula): Typically caused by the obstruction of a duct rather than direct trauma.

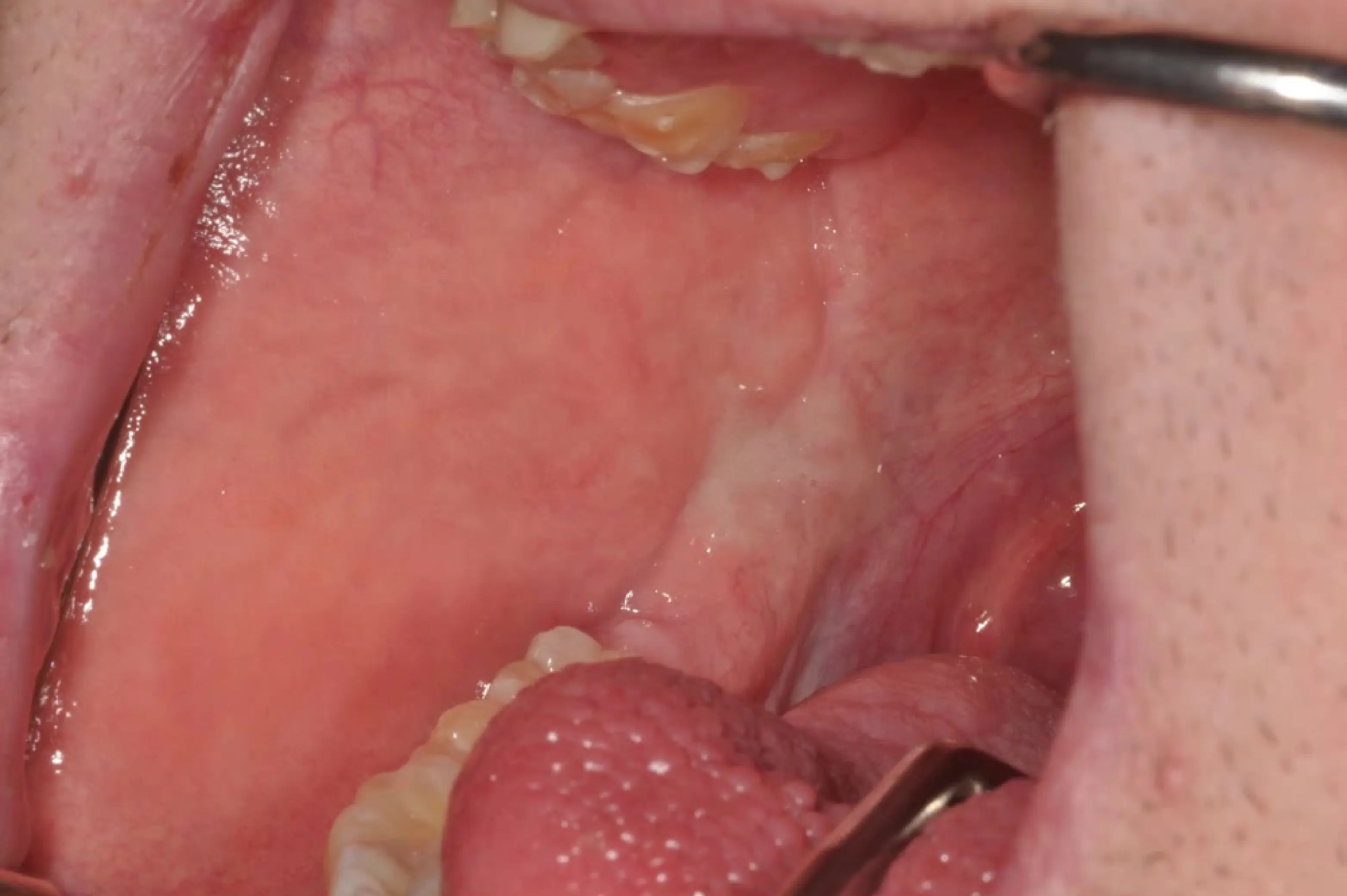
Clinical Presentation
- Commonly present as soft, painless swellings.
- Color ranges from deep blue to normal pink.
- The swelling may also appear translucent, and the size often fluctuates over time.
- Frequent locations include the mucosa or vermilion of the lower lip, though they can occur at other intraoral sites.
- Duration is variable and often depends on the level of inconvenience caused to the patient.
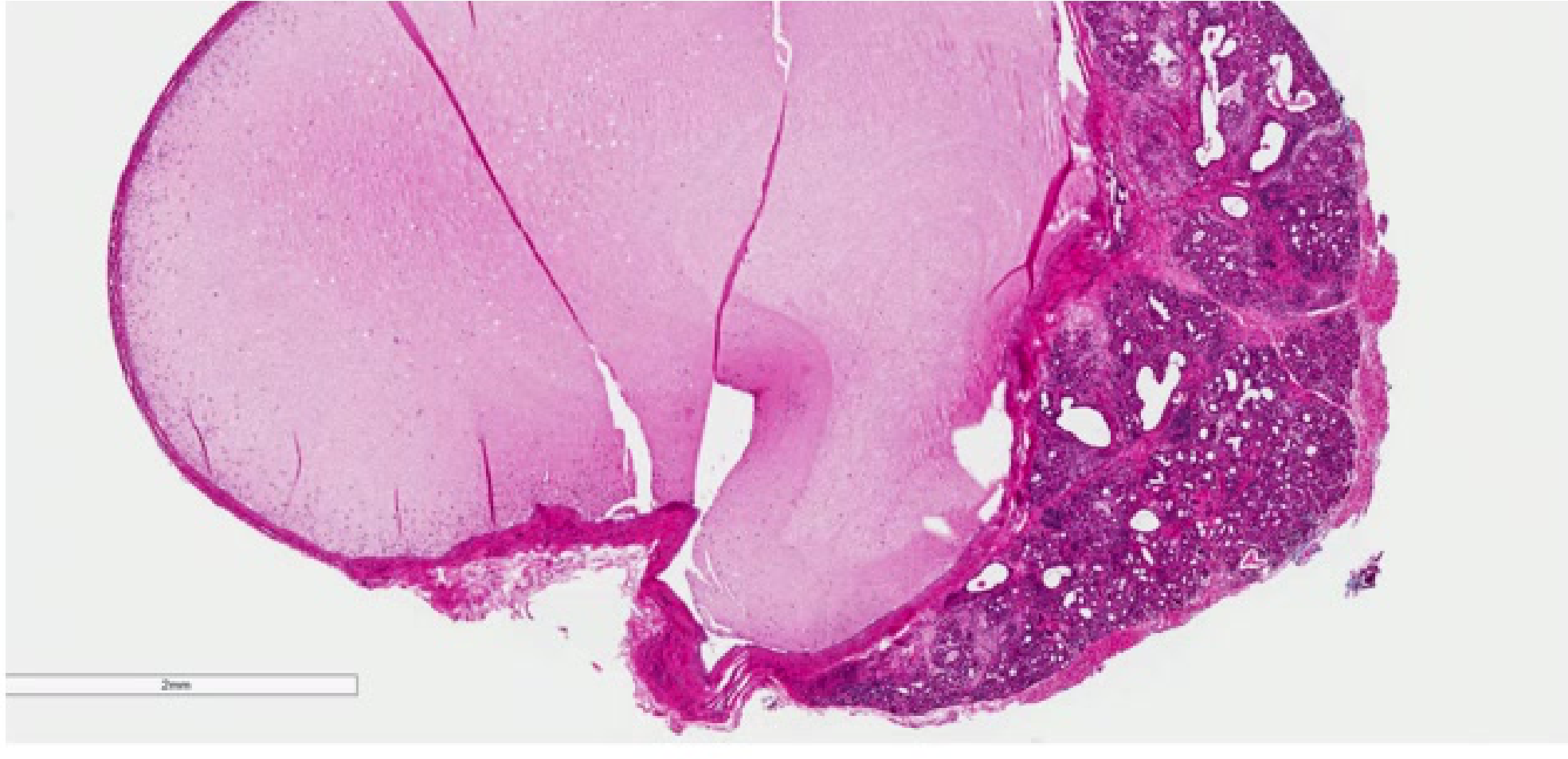
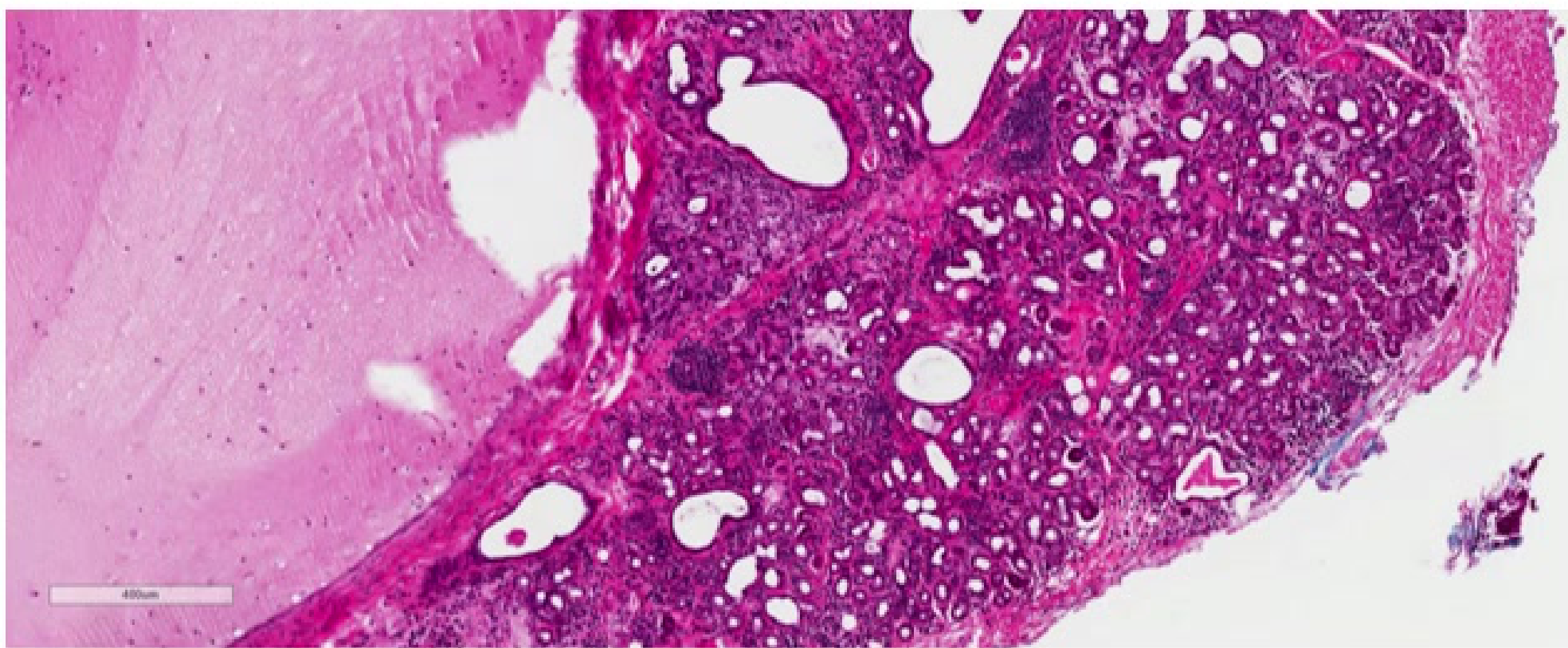
Histopathology15
-
Intact Lesions:
- Pseudocystic cavity containing mucus.
- Presence of numerous foamy epithelial histiocytes (muciphages), neutrophils, and granulation tissue.
- No epithelial cystic lining; superficial oral mucosa may show variable atrophy in superficial mucoceles.
-
Ruptured Lesions:
- Fragments of granulation tissue containing muciphages and neutrophils.
- Visible mucinous material.
- Associated salivary gland parenchyma may show obstructive changes, including acinar atrophy, ductal dilatation with periductal hyalinization, interstitial lymphoplasmacytic infiltration, and late-stage fibrosis.
-
Additional Features:
- A ruptured feeder salivary duct with squamous metaplasia may be observed.
- Chronic lesions may organize into fibrosis resembling a fibroepithelial polyp.
 |  |
Diagnosis16
- Patient history
- Clinical examination
- Biopsy
Management
- Surgical Excision: Complete excision of the lesion without rupture, including the removal of the associated minor salivary gland, is curative.
- Complications: Damage to adjacent glands during surgery may cause new lesions; patients should be warned of this and the risk of sensory nerve damage.
- Cryotherapy: An alternative curative method involving the deliberate destruction of the mucocele and underlying gland tissue. Note: This method does not provide a specimen for histopathologic review, making accurate clinical diagnosis essential.
Sialolithiasis
Sialolithiasis refers to the formation of salivary calculus or salivary stones.
Epidemiology17
- A very common disease of the salivary glands.
- Distribution:
-
80% occur in the submandibular gland or its duct (Wharton’s duct).
- 6% occur in the parotid gland.
- 2% occur in the sublingual or minor salivary glands.
-
- Demographics: More frequent in men than women, with a peak incidence between 30 and 60 years of age.
Etiology and Pathogenesis18
- The exact etiology is unknown, but contributing factors include duct system irregularities, inflammation, or local irritants.
- The submandibular gland is more prone to stones due to:
- Stagnation of calcium-rich, alkaline saliva, which promotes the calcification of the calculus within the duct.
- More alkaline, viscous, and mucous-rich saliva.
- Higher percentage of calcium phosphates.
- The long, sinuous path of Wharton’s duct, which contributes to stasis.
Clinical Presentation
- Recurrent swelling and pain in the involved gland, often exacerbated by eating (mealtime syndrome).
- Some cases remain asymptomatic.
Mealtime Syndrome
Pain and swelling are characteristically triggered or exacerbated by the thought, sight, or smell of food.
- Sialoliths are the most common cause of acute and chronic salivary gland infections.
- Size is usually less than 1 cm.
- Palpable stones feel like hard, small pebbles.
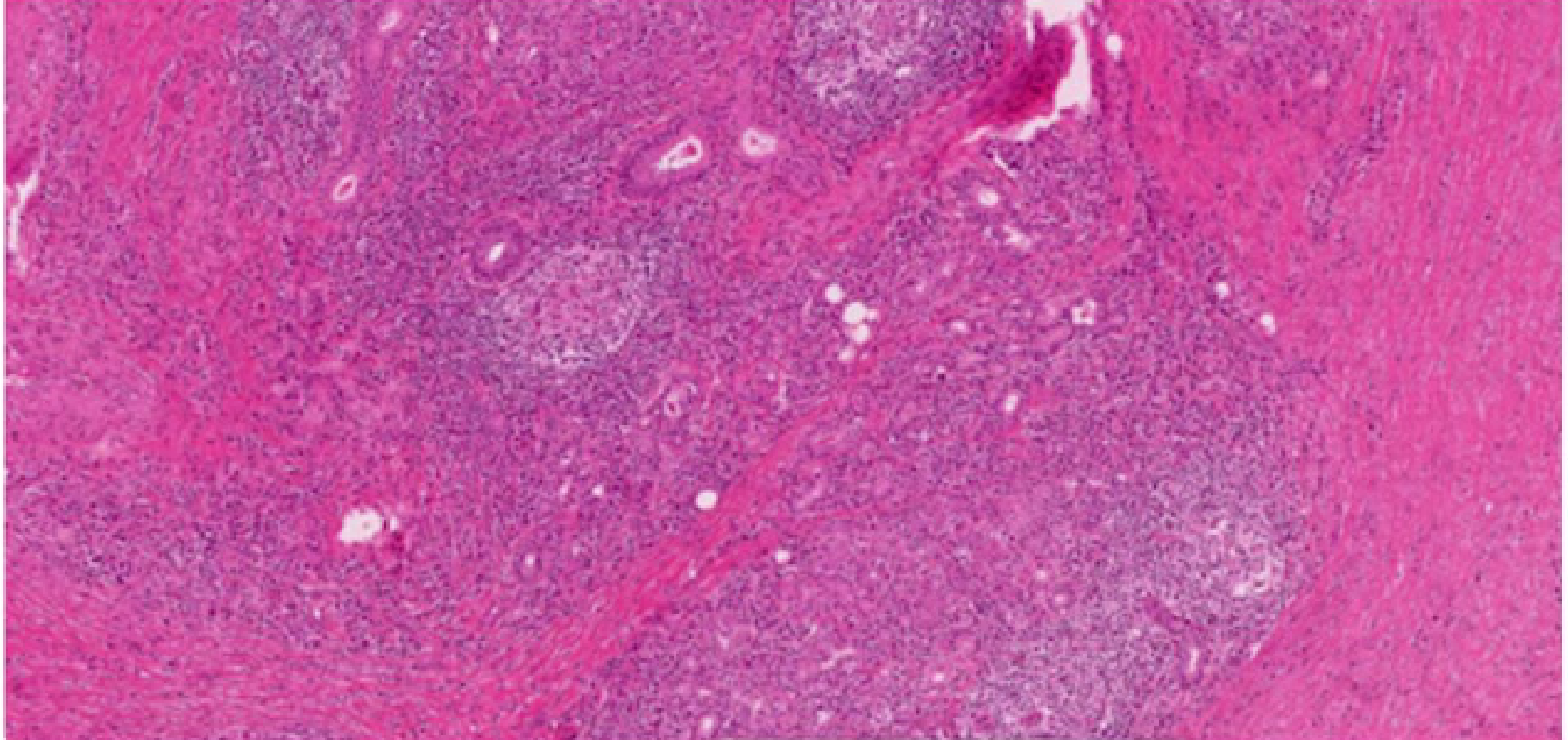
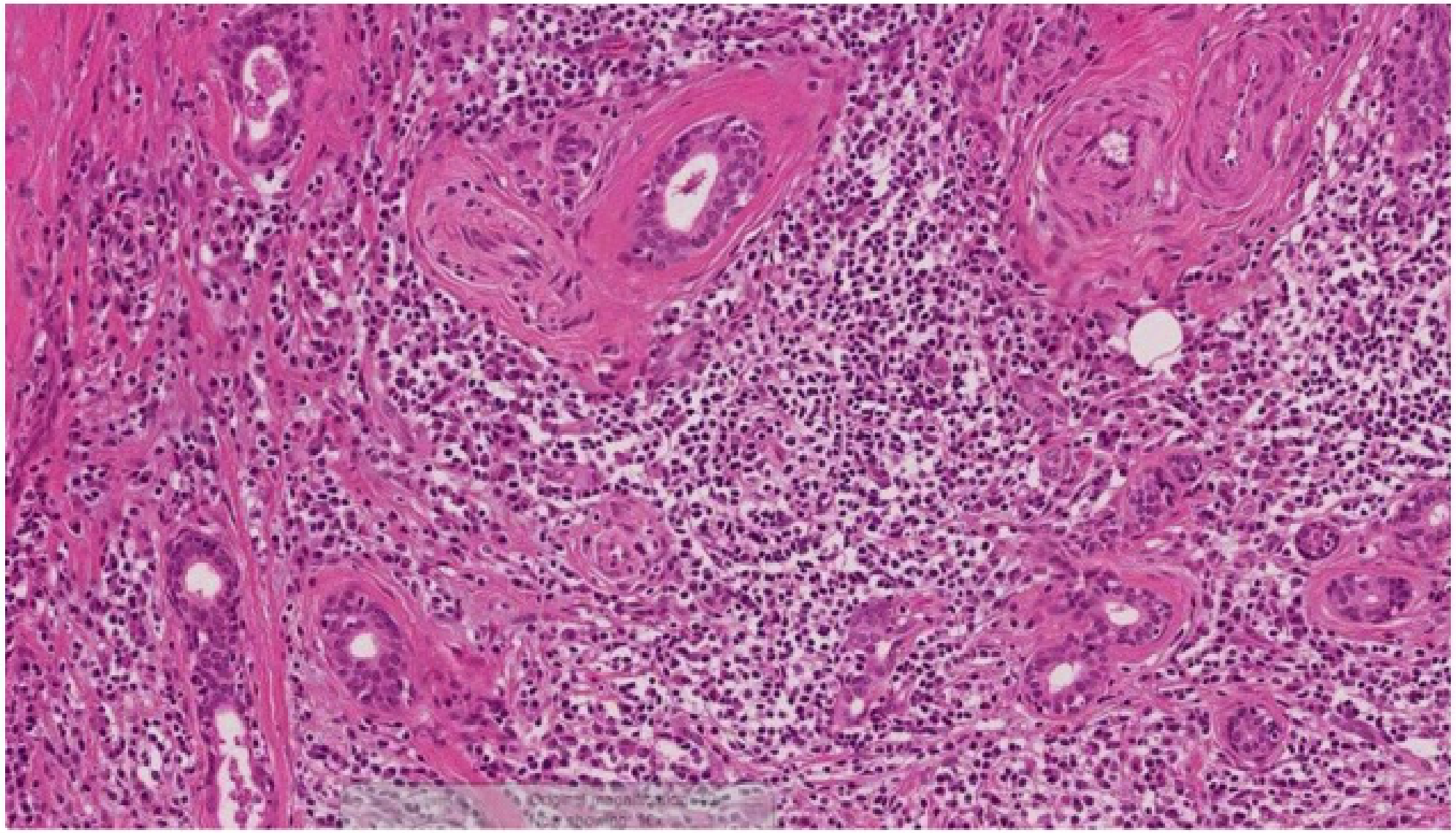
Histopathology19
- Glandular Changes: Varying degrees of acinar destruction, fibrosis, and chronic inflammation.
- Lymphoid Response: Presence of lymphoid aggregates containing prominent germinal centers.
- Ductal Changes: Ducts may undergo squamous and mucous metaplasia.
- Architecture: The lobular arrangement of the gland is generally maintained.
- Microliths: Small calcifications may be visible within the tissue.
 |  |
Diagnosis20
- Clinical Examination: May reveal swelling and absence of saliva secretion upon ductal blockage.
- Imaging:
- Intraoral occlusal radiographs, OPG, or CBCT.
- Note: 60-70% of calcified sialoliths are not detected by conventional radiography; non-contrast CT is the preferred indicator.
 |  |
 |
Management
- Minor Glands: Excision of the stone along with the associated gland.
- Major Glands:
- Palpable stones may be removed via an intraoral or sialoendoscopic approach, sparing the gland.
- If endoscopic removal is not possible, the associated gland may require removal.
- Conservative Measures: For small sialoliths, management includes salivary gland massage, irrigation, a sour diet, and sialogogues to stimulate flow.
Sialadenitis
Sialadenitis is an inflammation of the salivary glands. Bacterial forms can be either acute or chronic and often affect elderly patients with salivary hypofunction.
Etiology and Predisposing Factors21
- Primary Factor: Decreased saliva flow rate, allowing retrograde microbial colonization of the duct.
- Obstruction: Can be caused by calculi (stones), mucus plugs, tumor growth, or trauma.
- Microbiology: Staphylococcus aureus is the most common pathogen isolated in purulent cases.
Clinical Presentation22
- Acute Sialadenitis:
- Painful swelling of a single gland (commonly the parotid).
- Purulent discharge may be expressed from the duct orifice.
- Overlying skin may be red; abscess formation may occur.
- Risk of sepsis in immunocompromised individuals.
- Chronic Sialadenitis:
- May follow acute episodes.
- Characterized by repeated cycles of pain and inflammation.

Histopathology23
- Acute Suppurative Sialadenitis: Characterized by edema, hyperemia, and acute inflammatory cell infiltration.
- Viral Sialadenitis: Shows diffuse interstitial edema, intense hyperemia, and a dense lymphohistiocytic infiltrate.
Note: Diagnosis is usually clinical; biopsies are rarely performed for these conditions.
Diagnosis24
- Primarily based on clinical presentation.
- Chronic cases should be evaluated with imaging (e.g., ultrasound or CT) to identify underlying pathology like calculi or ductal strictures.
Management
- Infection Control: Empiric antimicrobial therapy, often starting with amoxicillin-clavulanate.
- Flow Promotion:
- Application of warm compresses.
- Administration of sialogogues.
- The use of sour drops is a common method to stimulate salivary flow.
- Salivary gland massage.
- Predisposing Factors: Addressing the underlying cause of decreased flow or obstruction.
Sjogren Syndrome
Sjogren’s Syndrome is an autoimmune systemic rheumatic disease characterized by progressive focal lymphocytic infiltration and destruction of exocrine glands.
Epidemiology25
- Predominantly affects females (9:1 female-to-male ratio).
- Median age of presentation is approximately 50 years, though it can occur at any age.
Pathogenesis
- Triggered by environmental factors interacting with genetic susceptibility.
- Results in chronic inflammation of exocrine glands (primarily salivary and lacrimal) and eventual loss of physiological function.
Clinical Manifestations26
Sjogren’s Syndrome is a slowly progressing disease with highly variable manifestations, ranging from organ-specific to systemic involvement.
- Sicca Symptoms: Dryness of the eyes (xerophthalmia) and mouth (xerostomia).
- Oral Signs:
- Dry, erythematous, sticky mucosa.
- Fissured tongue.
- Accelerated dental caries and oral candidosis.
- Parotid gland swelling (observed in 1/3 of patients).
- Ocular Signs:
- Red appearance and conjunctival inflammation.
- Other Dryness: Can affect the nose, respiratory tract, oropharynx, and vagina.
Systemic Features27
-
General Symptoms:
- Fatigue (80%)
- Chronic pain
- Low-grade fever (5%)
- Weight loss and Lymphadenopathy (15%)
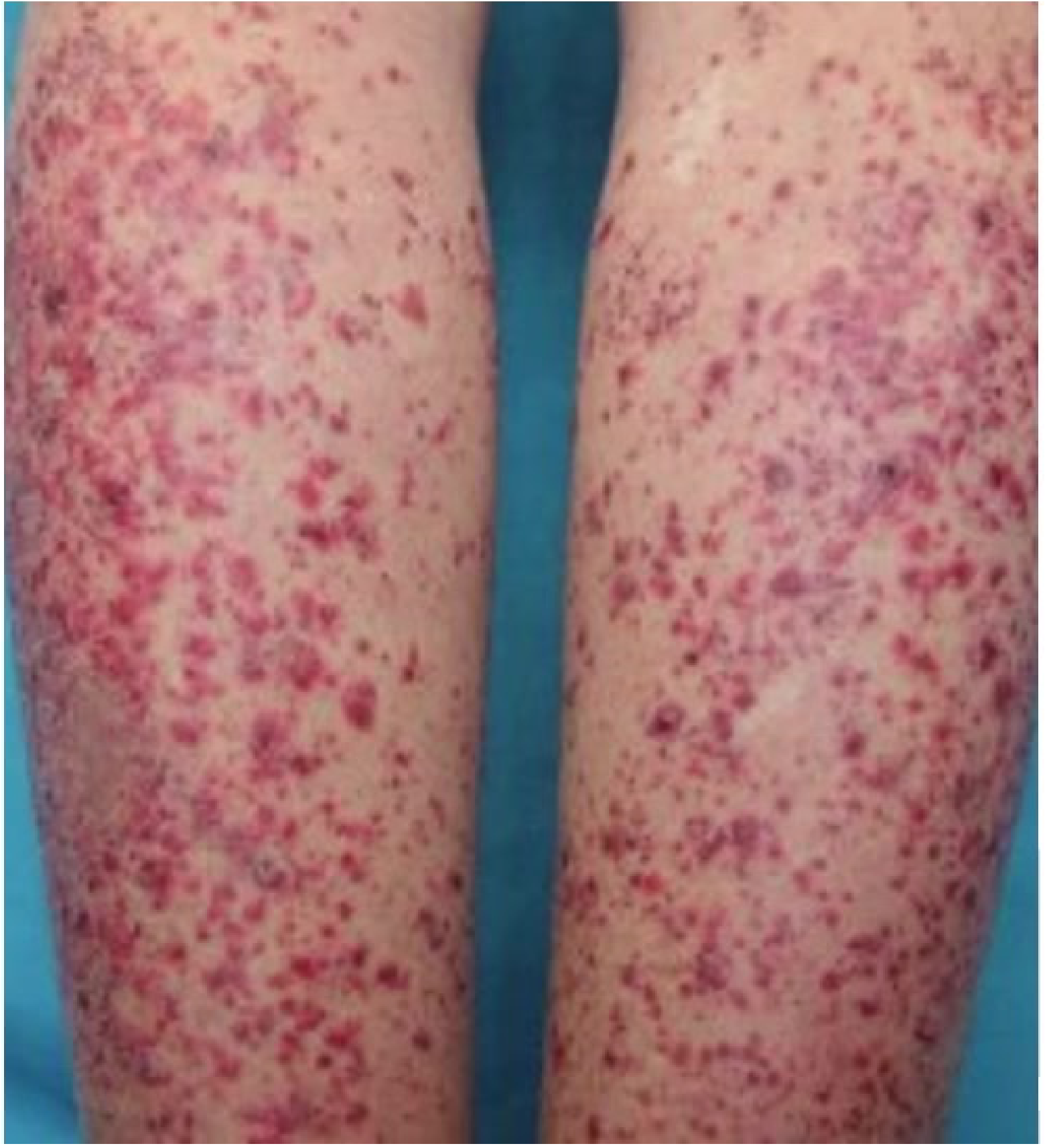
-
Cutaneous Features:
- Abnormally dry skin (23-68%)
- Cutaneous vasculitis (10%), purpura, and ulcers
- Annular erythema (9%)
-
Articular and Muscle Features:
- Arthralgia (60-70%)
- Myalgias (20-40%)
- Subclinical synovitis (20-30%) and non-erosive arthritis
Internal Organ Complications28
- Pulmonary (25%): Chronic obstructive lung disease, bronchiectasis, interstitial lung diseases, and pleuritis.
- Cardiovascular: Raynaud phenomenon (13%), pericarditis, pulmonary arterial hypertension, dysautonomia, and cryoglobulinaemic vasculitis.
- Nephro-urological:
- Renal tubular acidosis (9%) and glomerulonephritis (4%).
- Interstitial cystitis, osteomalacia, and renal stones.
- Hypokalaemic paralysis.
Neurological and Haematologic Complications29
- Peripheral Nervous System (10%): Mixed polyneuropathy, axon sensory/sensorimotor polyneuropathy, trigeminal or cranial neuropathies, and small-fibre neuropathy.
- Central Nervous System (2%): White matter lesions (MS-like), neuromyelitis optica, and recurrent aseptic meningitis.
- Haematologic Features:
- Unexplained leukopenia, lymphopenia, or neutropenia.
- Thrombocytopenia (2%) and Evans syndrome.
- Monoclonal gammopathy.
- B-cell lymphoma (5%): A significant long-term risk.
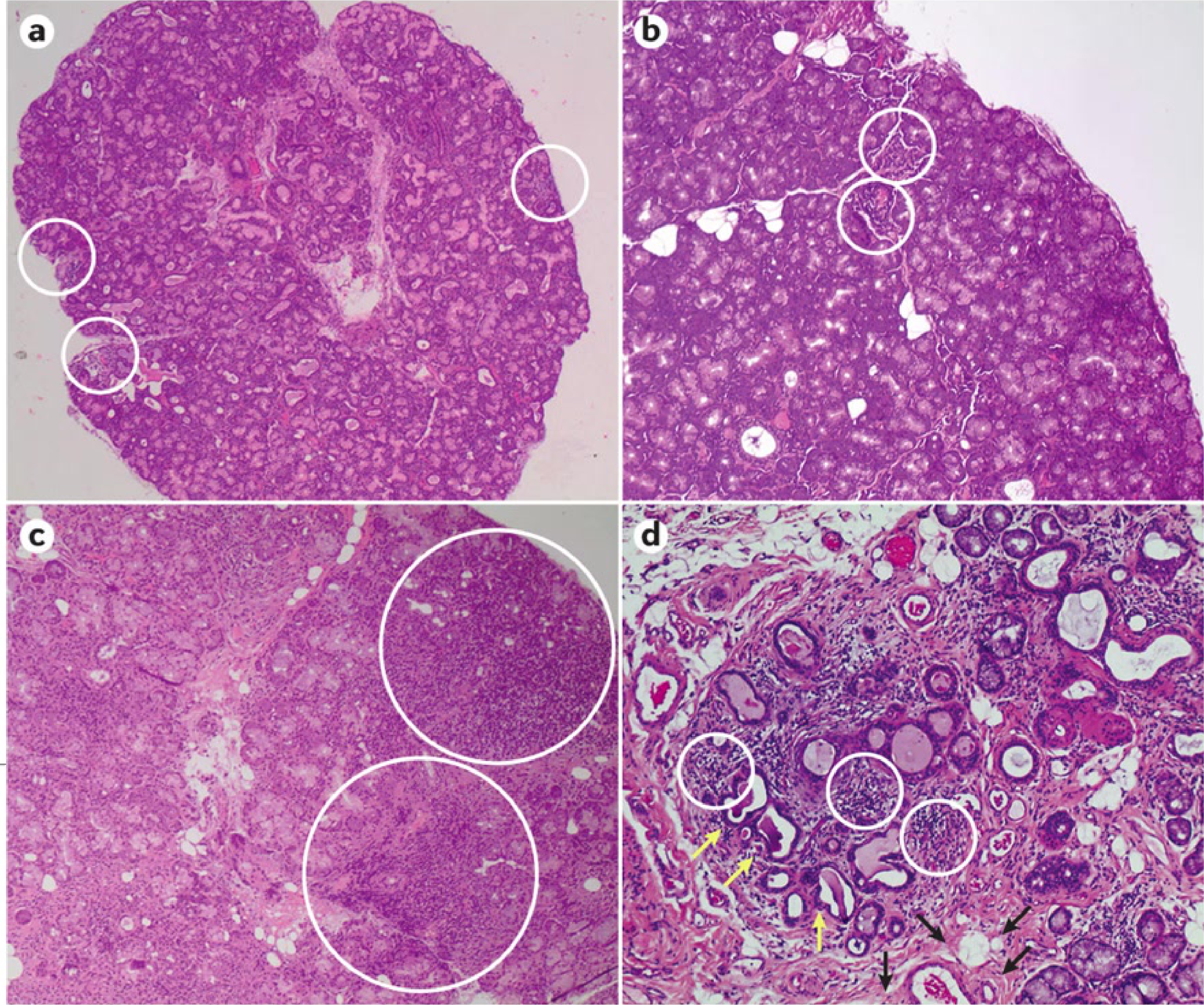
Histopathology: Labial Salivary Gland Biopsy3031
- Requirements: Accurate evaluation requires an adequate sample size (3–5 glands).
- Focus Score: Defined as the number of lymphocytic aggregates (foci) per 4 mm² of glandular surface.
- A focus is specifically defined as an aggregate of 50 or more lymphocytes.
- Diagnostic Threshold: A focus score of ≥1 foci/4 mm² is indicative of the disease.
- Key Feature: Focal lymphocytic sialadenitis is the hallmark histopathological feature of Sjogren’s Syndrome.
Histopathological analysis of salivary glands in Sjogren’s Syndrome scenarios typically demonstrates the characteristic focal lymphocytic sialadenitis required for classification and diagnosis.
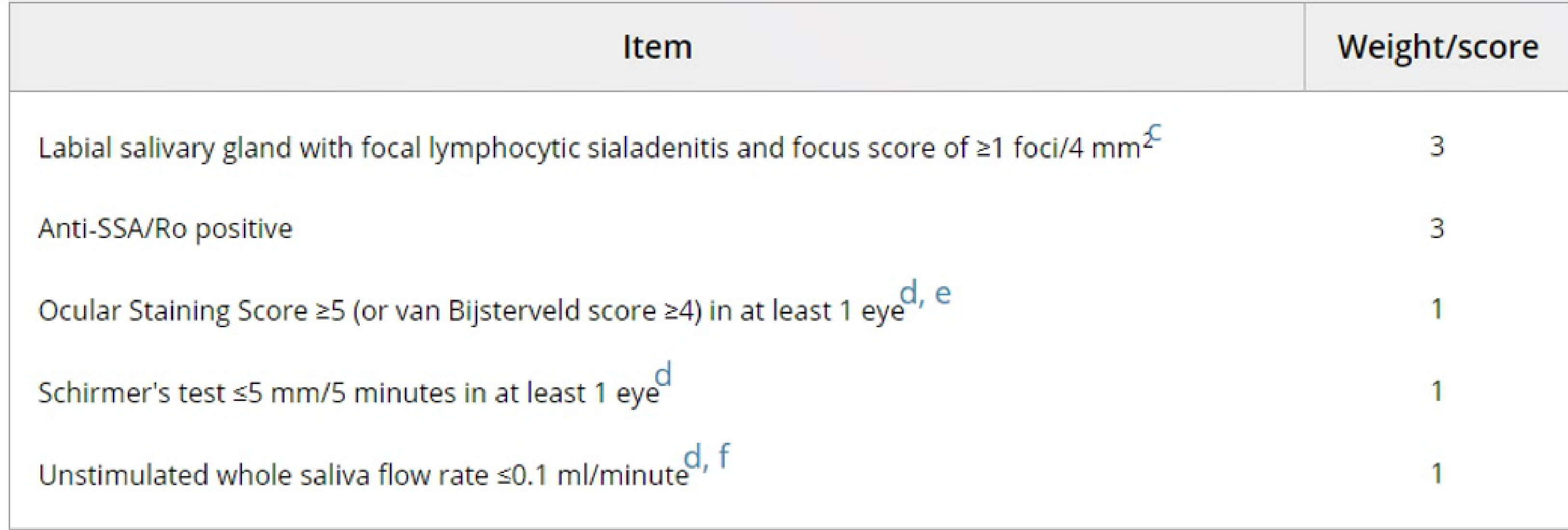
Classification Criteria (ACR/EULAR 2016)32
Primary Sjogren’s Syndrome is classified if a patient scores ≥4 based on the following weighted items: #DiagnosticClassifications
| Item | Weight/Score |
|---|---|
| Labial salivary gland with focal lymphocytic sialadenitis (focus score ≥1/4 mm²) | 3 |
| Anti-SSA/Ro positive | 3 |
| Ocular Staining Score ≥5 (or van Bijsterveld score ≥4) in at least 1 eye | 1 |
| Schirmer’s test ≤5 mm/5 minutes in at least 1 eye | 1 |
| Unstimulated whole saliva flow rate ≤0.1 ml/minute | 1 |
Management and Monitoring
- Lymphoma Risk: 5-10% of patients develop mucosa-associated lymphoid tissue (MALT) lymphoma, often in the parotid glands; periodic review is mandatory.
- Symptom Management: Use of saliva stimulants and moisturizing agents.
- Prevention: Reinforcement of strict caries prevention protocols.
Sialadenosis
Sialadenosis (or sialosis) is an uncommon, benign, non-inflammatory, and non-neoplastic enlargement of the salivary glands, typically presenting as bilaterally symmetrical and painless swelling.
Epidemiology33
- Usually begins between ages 20 and 60 years.
- Condition may persist for over 20 years.
- Most commonly affects the parotid glands.
Etiology
- Often associated with autonomic neuropathy.
- Linked Conditions:
- Endocrine disorders (Diabetes mellitus, hypothyroidism).
- Alcohol abuse and nutritional disorders.
- Medication-induced (psychotropic or antihypertensive drugs).
- Eating disorders, specifically bulimia, are also a recognized linked condition.
Clinical Presentation34
- Slowly progressing bilateral swelling of the parotid glands.
- Patients are often asymptomatic, though some may complain of reduced salivary flow.
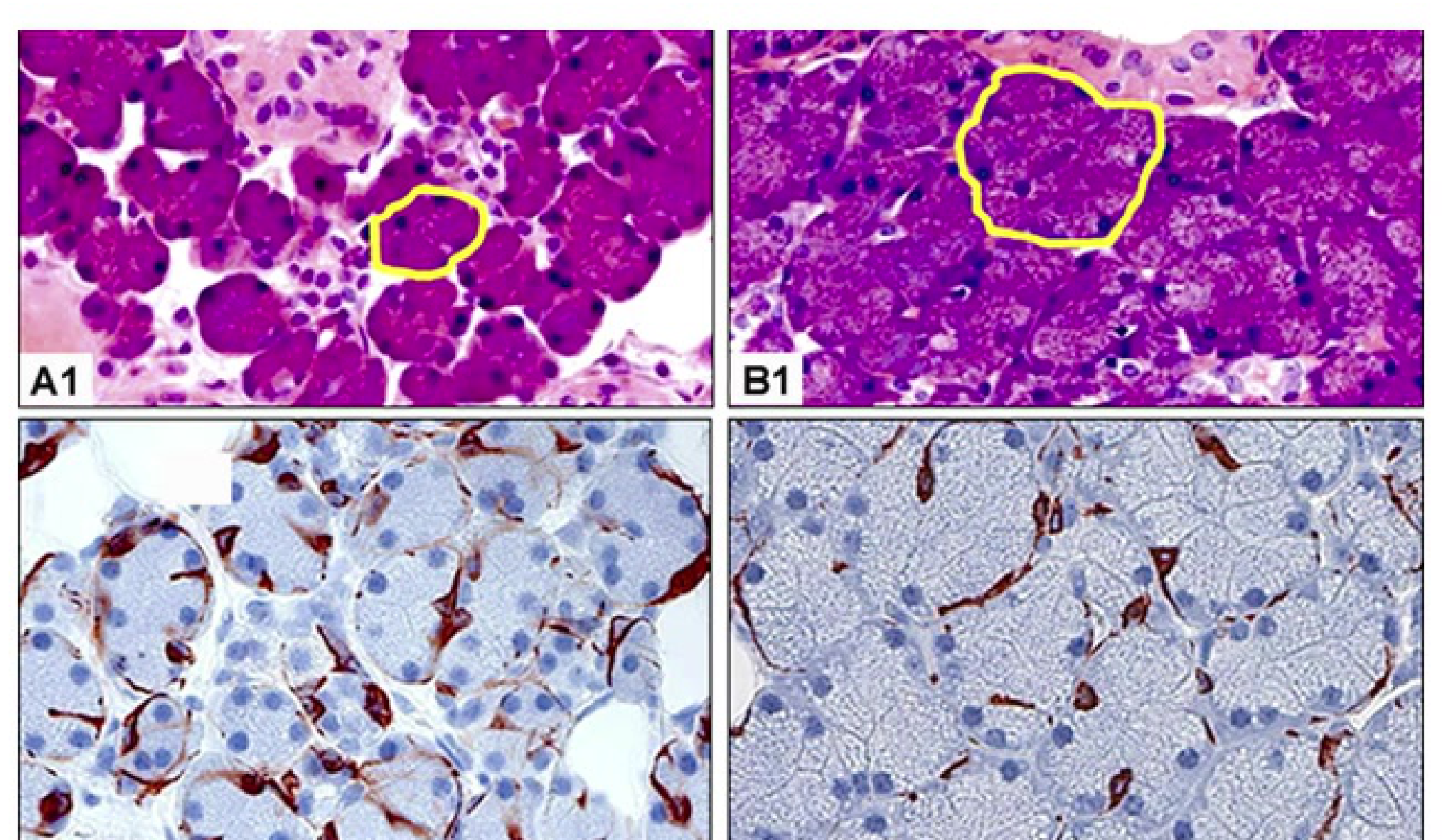 |  |
Histopathology
- Acinar Changes: Significant acinar enlargement (2-3 times normal diameter).
- Cellular Features: Basally situated nuclei and cytoplasm packed with granules.
- Inflammation: Inflammatory cells are typically absent.
- Progression: Long-standing disease may eventually lead to acinar atrophy and fatty replacement.
- Note: There is no correlation between specific clinical types and histologic appearance.
Diagnosis35
- Primarily a diagnosis of exclusion based on history and clinical examination.
- Investigations: May include blood tests, ultrasound, or sialography.
- Biopsy: Rarely required.
Management
- No specific treatment is available.
- Sialadenosis may resolve if the underlying systemic cause (e.g., endocrine disorder or medication) is successfully managed.
Necrotizing Sialometaplasia
Necrotizing sialometaplasia is a benign, inflammatory disorder of the salivary glands.
Etiology36
- The exact etiology is unknown, but ischemic necrosis of minor salivary gland tissue is the primary causative factor.
- Associated Triggers:
- Smoking
- Local trauma or pressure from dentures
- Local anesthetic injections or surgical procedures
- Immune response to an unknown allergen
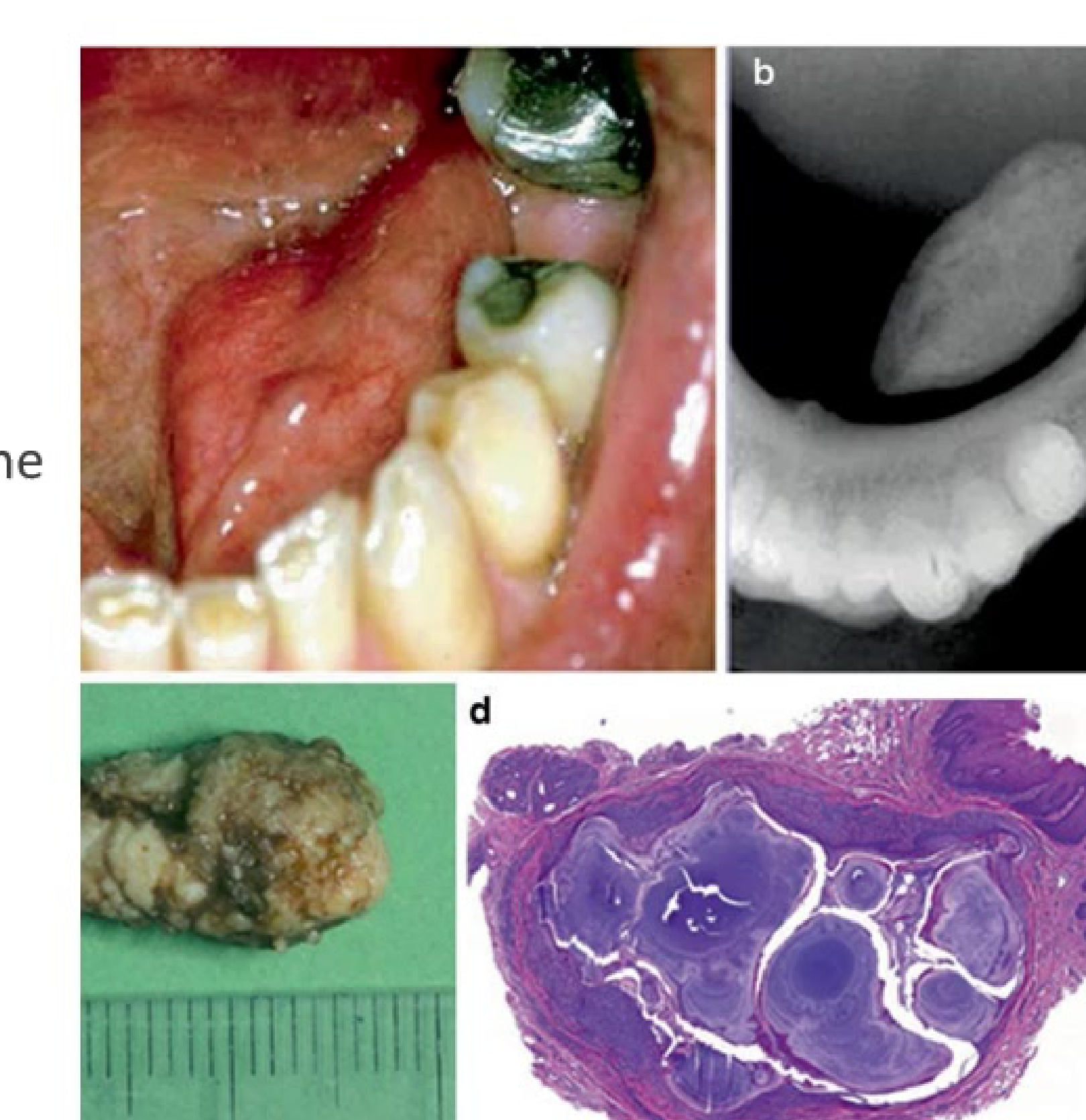
Clinical Presentation37
- Most commonly located in the posterior region of the hard palate.
- Presents as a chronic, “punched-out” ulcer.
- Clinical appearance can resemble malignancy (e.g., squamous cell carcinoma).
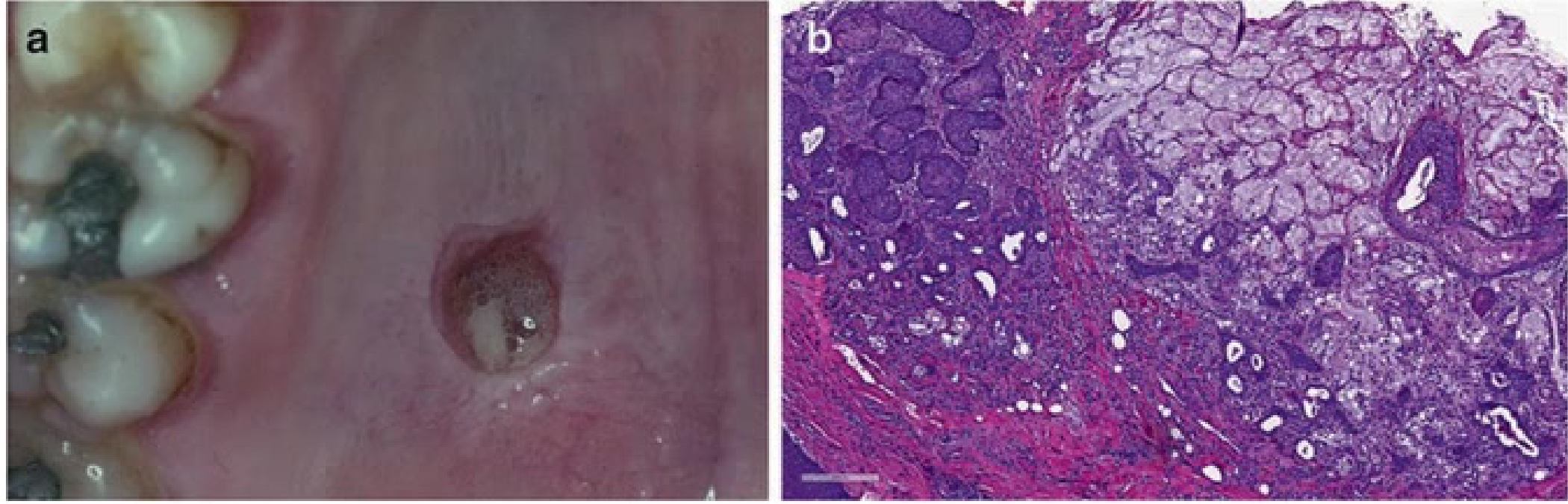 |  |
Histopathology
- Ductal Changes: Lobular arrangement is preserved, but the central ductal system shows squamous cell metaplasia.
- Cellular Features: Islands of squamous cells may show hyperplasia.
- Necrosis: Necrotic acini and inflammatory cells are present at the periphery.
- Infiltrate: Diffuse mixed inflammatory infiltrate consisting of lymphocytes, plasma cells, neutrophils, macrophages, and occasional eosinophils.
Diagnosis38
- Clinical examination
- Biopsy (essential to rule out malignancy)
Management
- Natural Course: The condition is self-limiting.
- Resolution: Typically resolves spontaneously within 3 to 10 weeks.
- Symptomatic Treatment: Analgesics and 0.12% Chlorhexidine (Chx) mouthwash.
- Intervention: Surgical intervention is not required.
Learning Outcomes39
Discuss the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of the following salivary gland neoplasms:
- Pleomorphic adenoma
- Warthin’s tumour
- Oncocytoma
- Mucoepidermoid carcinoma
- Acinic cell carcinoma
- Adenoid cystic carcinoma
- Polymorphous low grade adenocarcinoma
Discuss the aetiology, clinical features, diagnosis, and management of dry mouth.
Salivary Gland Neoplasms40
Pleomorphic Adenoma
Introduction41
- Other names: Benign mixed tumour.
- Prevalence: Most common benign neoplasm of the major and minor salivary glands, accounting for up to 80% of benign salivary gland tumours
Diagnostic Note
Warthin's tumours are known to show high uptake (appear "hot") on PET scans, which can sometimes be confused with malignancy if not correlated clinically. .
- Malignancy: Malignant transformation may occur in long-standing lesions.
Epidemiology
- Age: Wide age range; found in children and adults, but most common in the 3rd to 6th decades of life.
- Gender: Female predominance (2:1).
Aetiopathogenesis42
- Aetiology: Unknown.
- Radiation: Incidence has been reported to increase 15-20 years after exposure to radiation.
Clinical Presentation
- Growth: Slow-growing, painless submucosal mass; may remain undiagnosed for years.
- Mobility: May be fixed or mobile.
- Symptoms: Depend on the site of involvement; may include pain, facial nerve palsy, skin fixation, and epistaxis.
- Major Salivary Glands: Most common site is the superficial lobe of the parotid gland. Less commonly occurs in submandibular and sublingual glands.
- Often presents as a firm mass upon palpation.
- Minor Salivary Glands: Most common sites are the palate and upper lip, but can occur at any oral site, the nose, paranasal sinuses, and larynx.
- Warning Signs: Rapid enlargement of a tumour nodule should raise suspicion of malignant transformation.
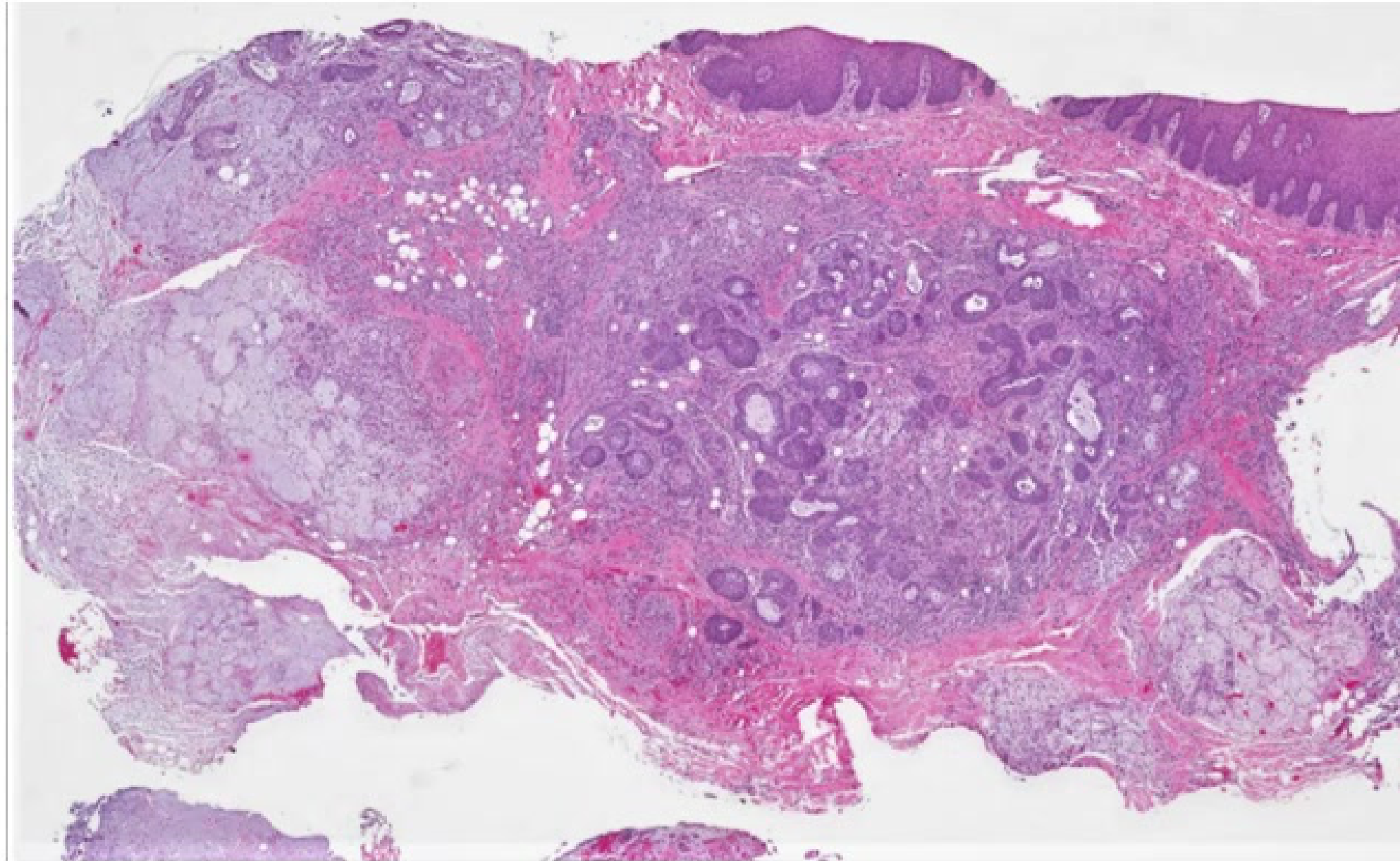
Histopathology43
- Gross Features: Bosselated outer surface, often with tongue-like protrusions (pseudopods).
- Primary Components:
- Epithelial (ductal): Forms the inner layer of cysts and tubules.
- Myoepithelial cells: Forms the outer layer of cysts and tubules; also scattered within the myxoid stroma. Cytology can be plasmacytoid, spindled, epithelioid, clear, or stellate shaped.
- Stromal component: Typically myxoid, chondroid, or myxochondroid; can also be hyalinized or fibrotic.
- Metaplastic Changes: May include adipose, osseous, squamous (sometimes with keratinization), sebaceous, and mucinous metaplasia.
- Vascular Involvement: Intravascular permeation has been reported in a small percentage of cases and does not increase the risk of recurrence or distant metastasis.
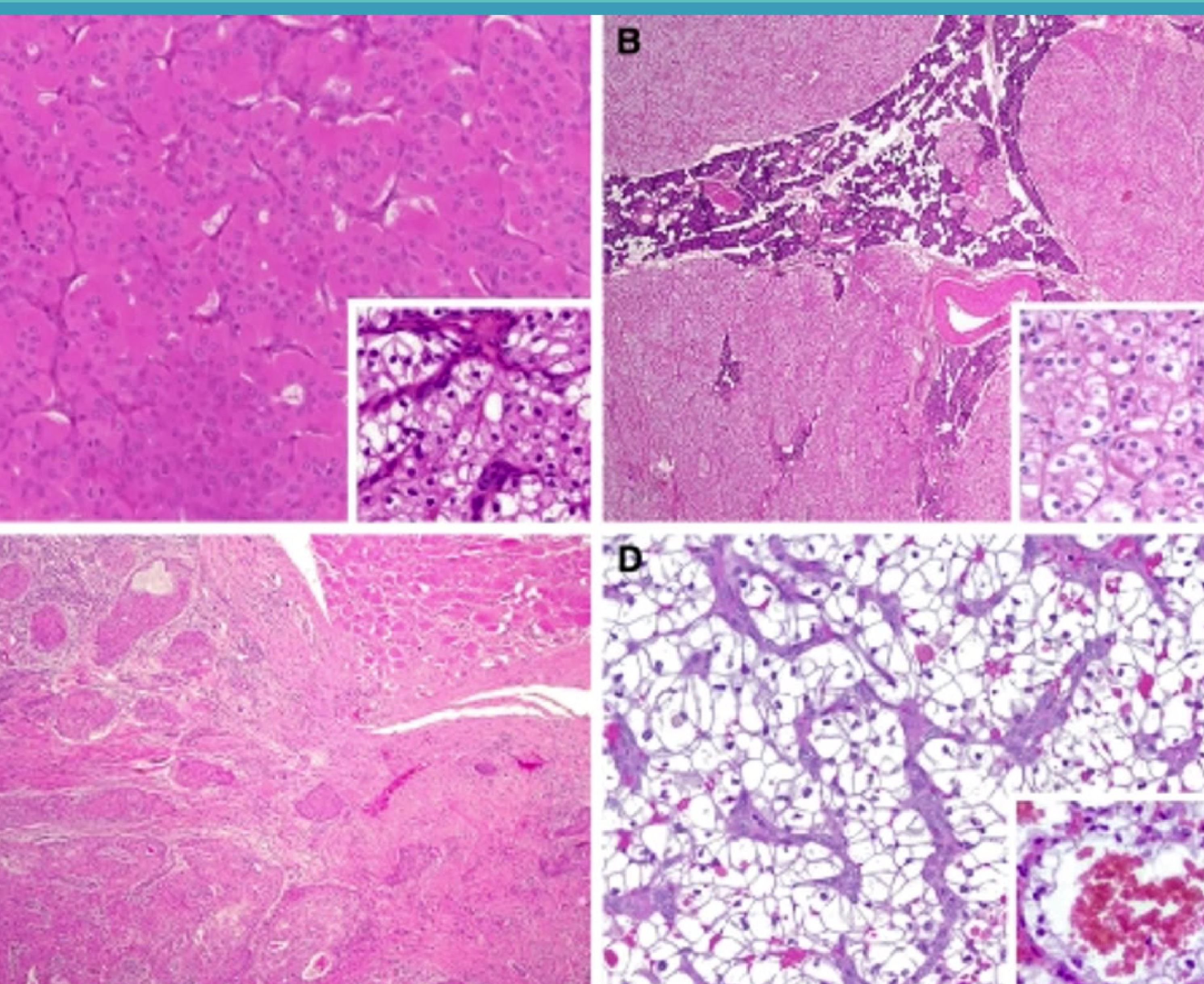
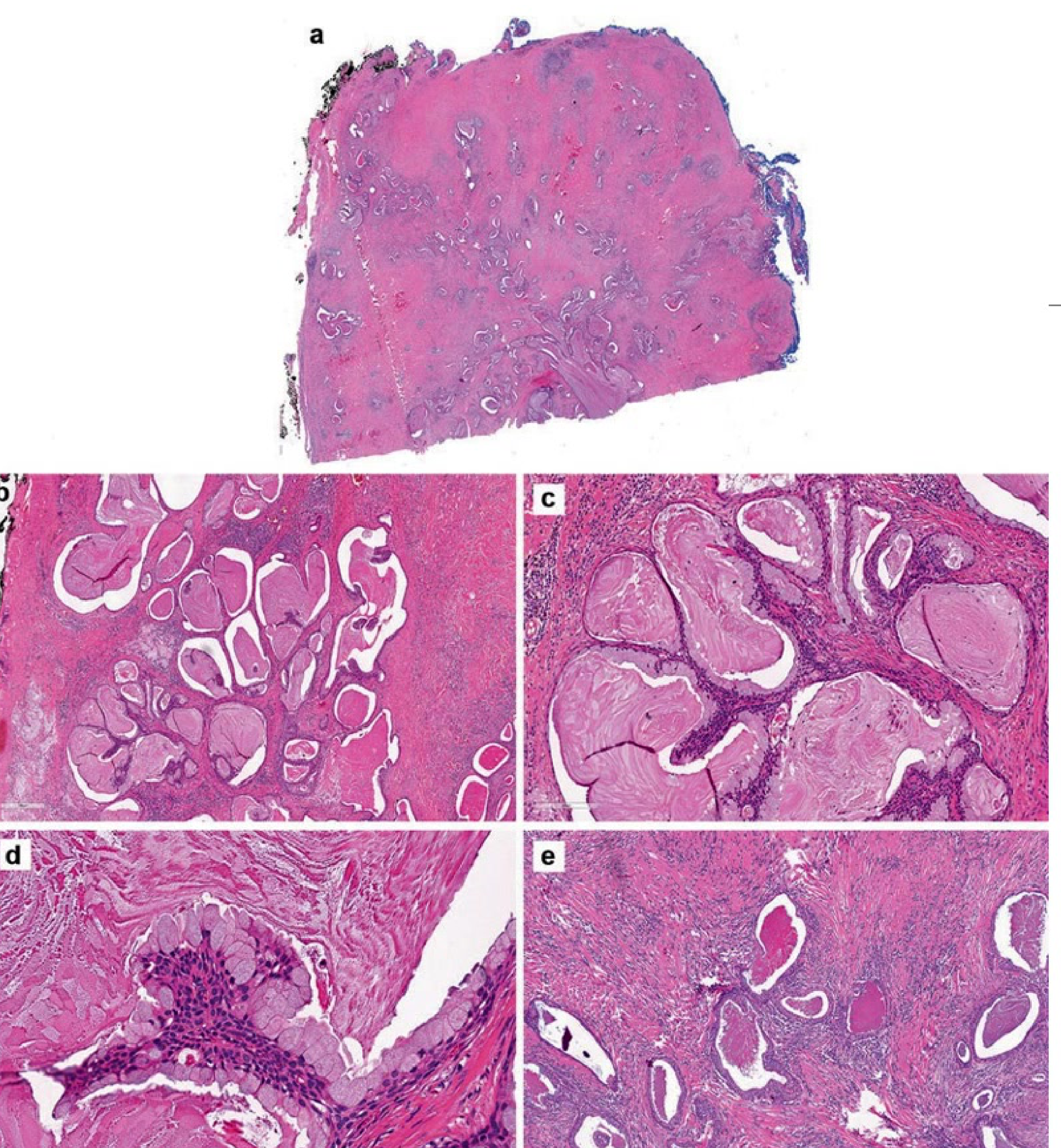
Microscopic Illustrations44
Visual documentation of Pleomorphic Adenoma features (Contemporary Oral Medicine, 2019) demonstrating the diverse epithelial and stromal arrangements characteristic of the “mixed” tumour.
 |  |
 |  |
Diagnosis45
- History and Clinical Examination
- Investigations:
- Imaging: Ultrasound, CT, MRI.
- Biopsy: Small incisional biopsies or fine needle aspirates (FNA) can complicate diagnosis as they may not be representative of the entire lesion.
Management and Prognosis
- Treatment: Excision of the tumour with clear margins.
- Prognosis: Excellent after surgical resection in most cases.
- Recurrence Factors: Related to incomplete encapsulation, extracapsular tumour extension, and intraoperative tumour rupture/spillage.
- Malignant Transformation: Progression into Carcinoma ex pleomorphic adenoma occurs in up to 7% of cases.
Warthin’s Tumour
Introduction46
- Other names: Adenolymphoma, papillary cystadenoma lymphomatosum, cystadenolymphoma.
- Definition: A benign salivary gland tumour composed of oncocytic epithelial cells lining ductal, papillary, and cystic structures within a lymphoid stroma.
- Prevalence: Second most common salivary gland neoplasm, accounting for up to 15% of all salivary gland tumours.
- Malignancy: Malignant transformation has been reported.
Epidemiology
- Age: Most commonly diagnosed in the 6th to 7th decade of life.
- Gender: Slight male predominance.
Risk Factors: Smoking47
- Association: Reported since the 1980s; numerous studies note a strong correlation.
- Risk Level: Smoking habit carries a 4 to 8-fold greater risk of developing Warthin’s tumour (WT) compared to non-smokers.
- Research (Kotwall C. 1992):
- Case-control study (1980–1989) comparing WT (28 cases) vs. Pleomorphic Adenoma (69 cases).
- Positive smoking history defined as 10 pack-years.
- Found an 8 times higher risk for WT in smokers.
Risk Factors: Autoimmune Diseases48
- Research (Gallo et al. 1997):
- Retrospective analysis of 140 WT patients vs. 380 Pleomorphic Adenoma (PA) patients over 25 years.
- WT patients showed a significantly higher incidence of autoimmune disorders (23% vs. 3%; p<0.001).
- Significant smoking history in WT group (87% vs. 38%; p<0.001).
- Pathogenesis Hypothesis: Supports an immune-mediated pathogenesis; smoking may facilitate these immune reactions.
Risk Factors: EBV Infection49
- Research (Santucci et al. 1993):
- First reported detection of the EBV genome in Warthin’s tumour.
- Frequently noted in neoplastic cells of multiple or bilateral WT (86.7%).
- Occasionally noted in solitary WT (16.7%).
- Significance: Suggests a strong association between EBV infection of cells and the development of multiple or bilateral lesions.
Pathogenesis50
- Nature of Process: Controversial; debated as a neoplastic process versus a metaplastic process with secondary lymphoid reaction.
- Accepted Theory:
- Neoplasm arising from heterotopic salivary ducts located within pre-existing intra-parotid or para-parotid lymphoid tissue.
- Immunohistochemistry (IHC) Support: Luminal and basal epithelial cells of WT are similar to striated duct cells and basal cells of the excretory duct (Ellis & Auclair 1996).
- Other Factors: Nitrous Oxide has been associated with WT development, though its specific role in pathogenesis is not yet established.
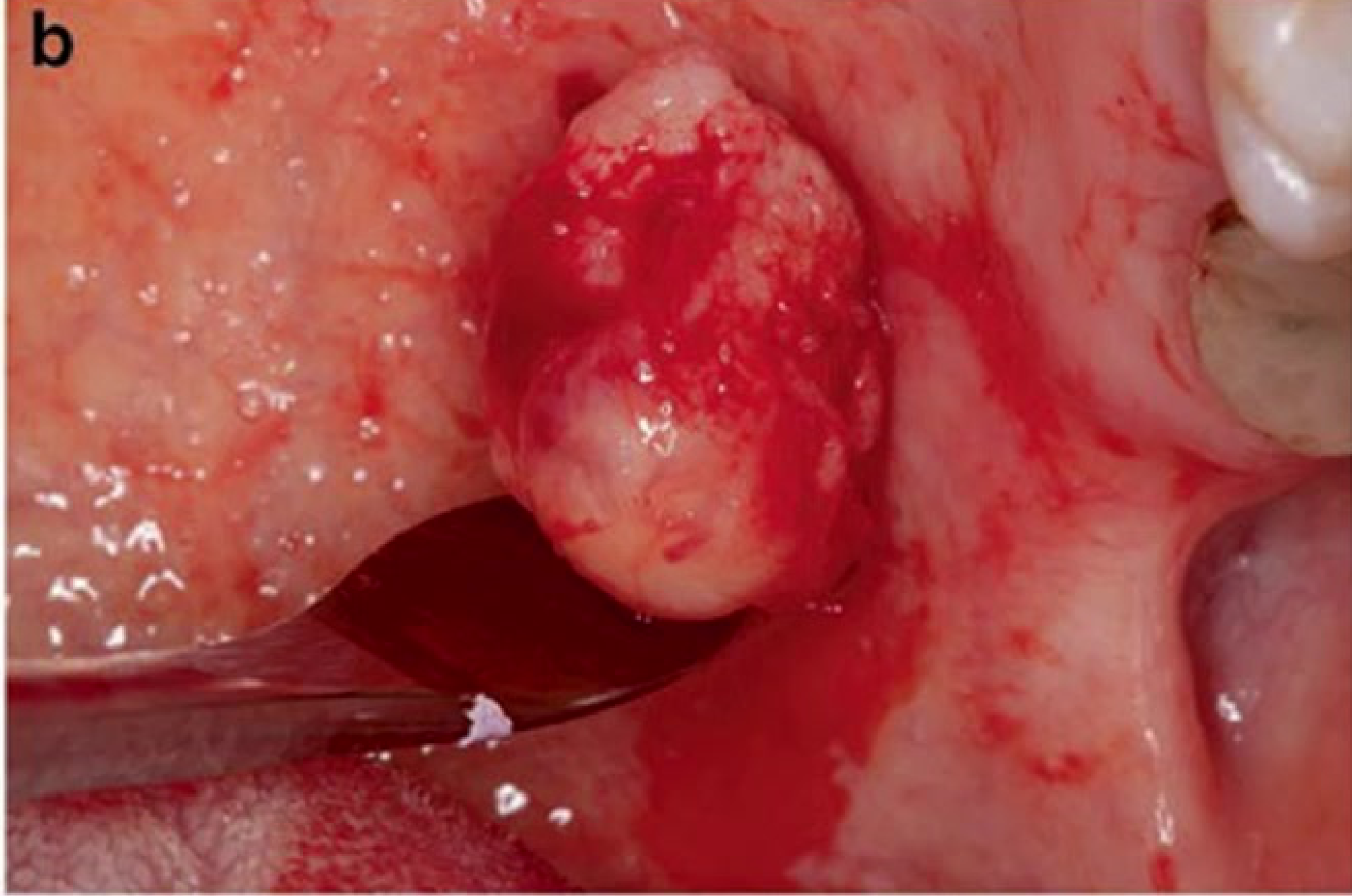
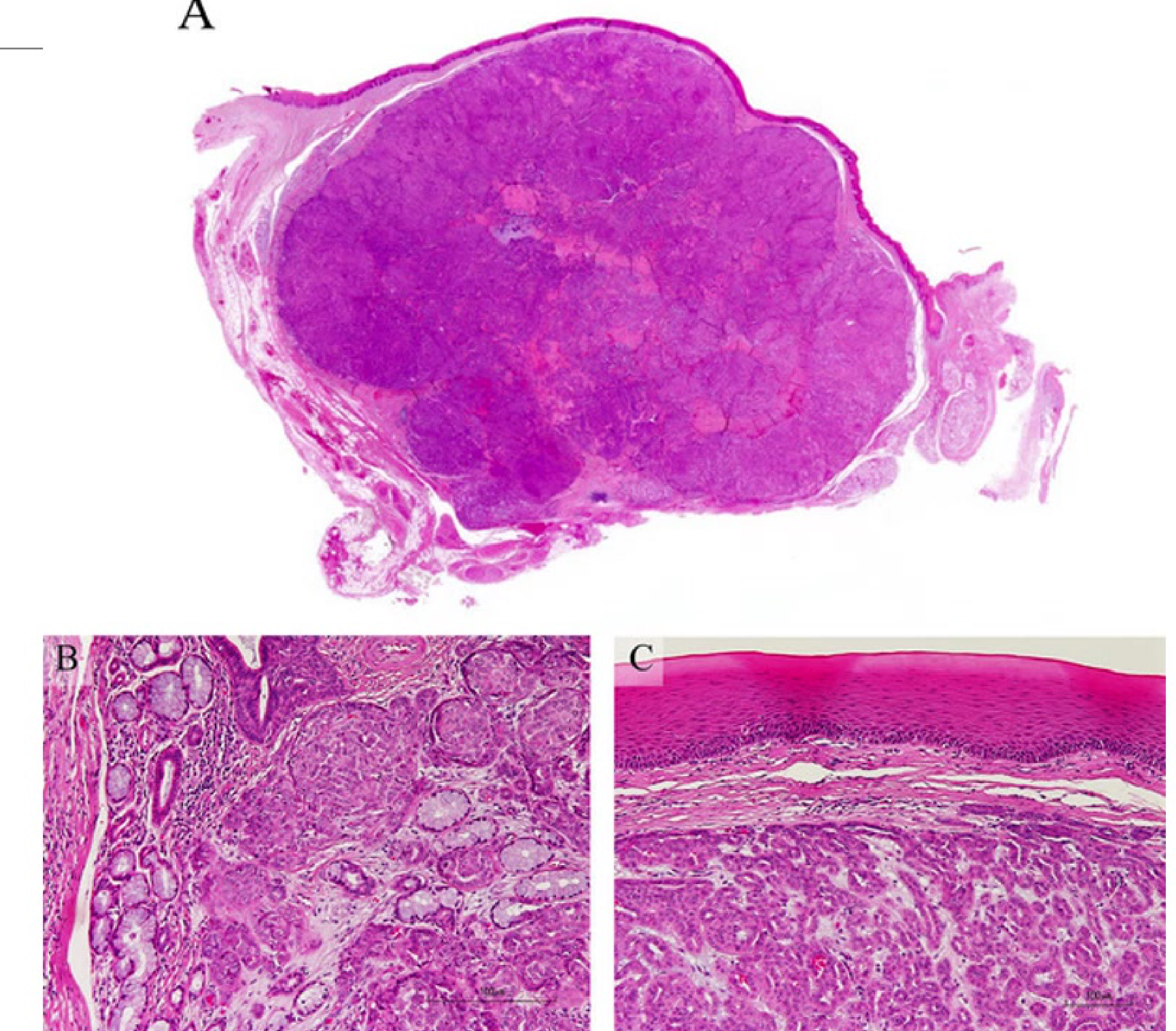
Clinical Presentation51
- Symptoms: Painless, discrete, slow-growing lump.
- Location: Almost exclusively involves the parotid glands; often presents as a mass/swelling in the upper neck or angle of the mandible
- Typically located in the inferior pole of the parotid gland.
- Distribution: May be unilateral or bilateral; multifocal lesions may occur.
- Complications: May present with facial nerve palsy if the nerve is involved.
 |  |
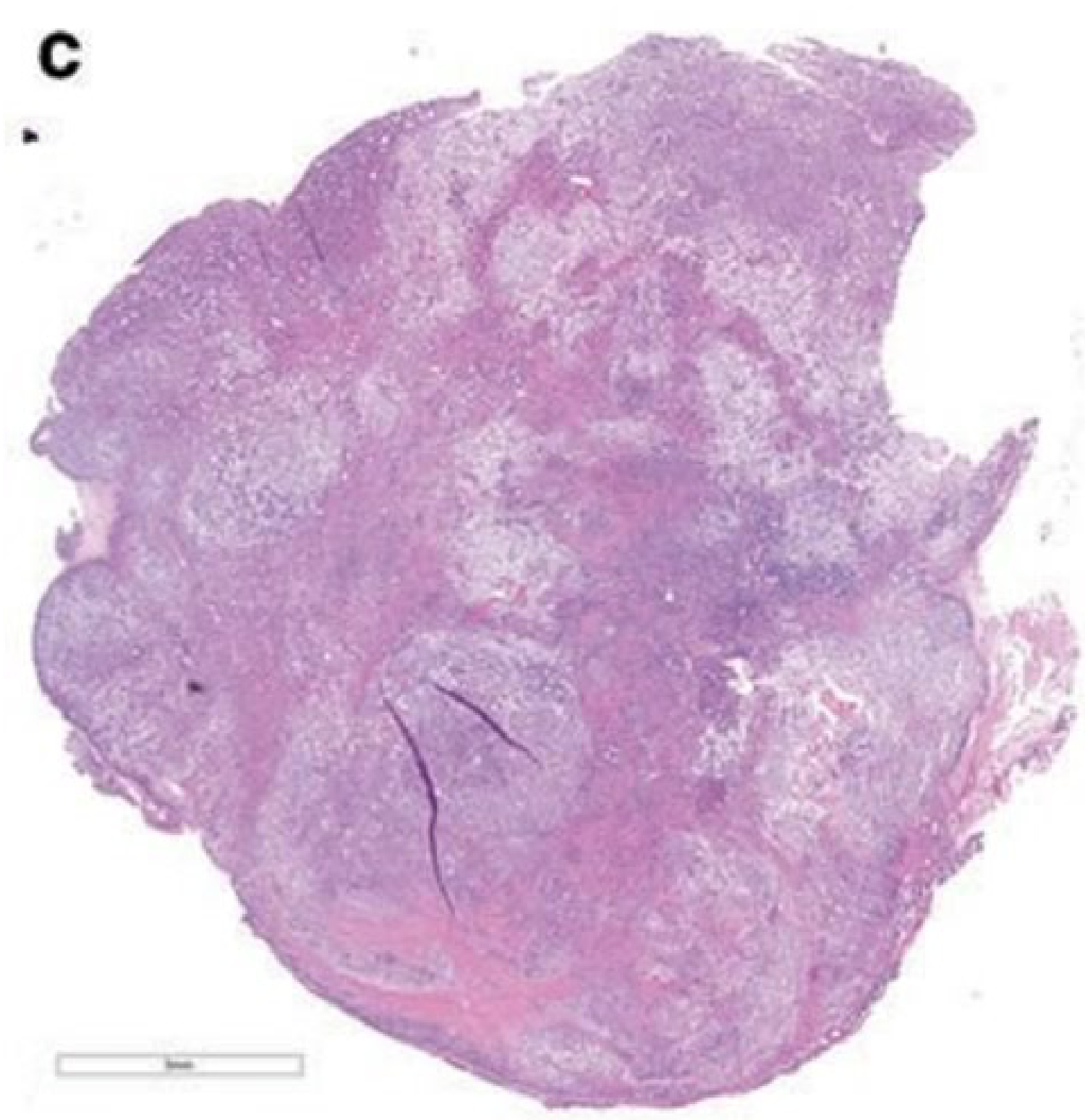
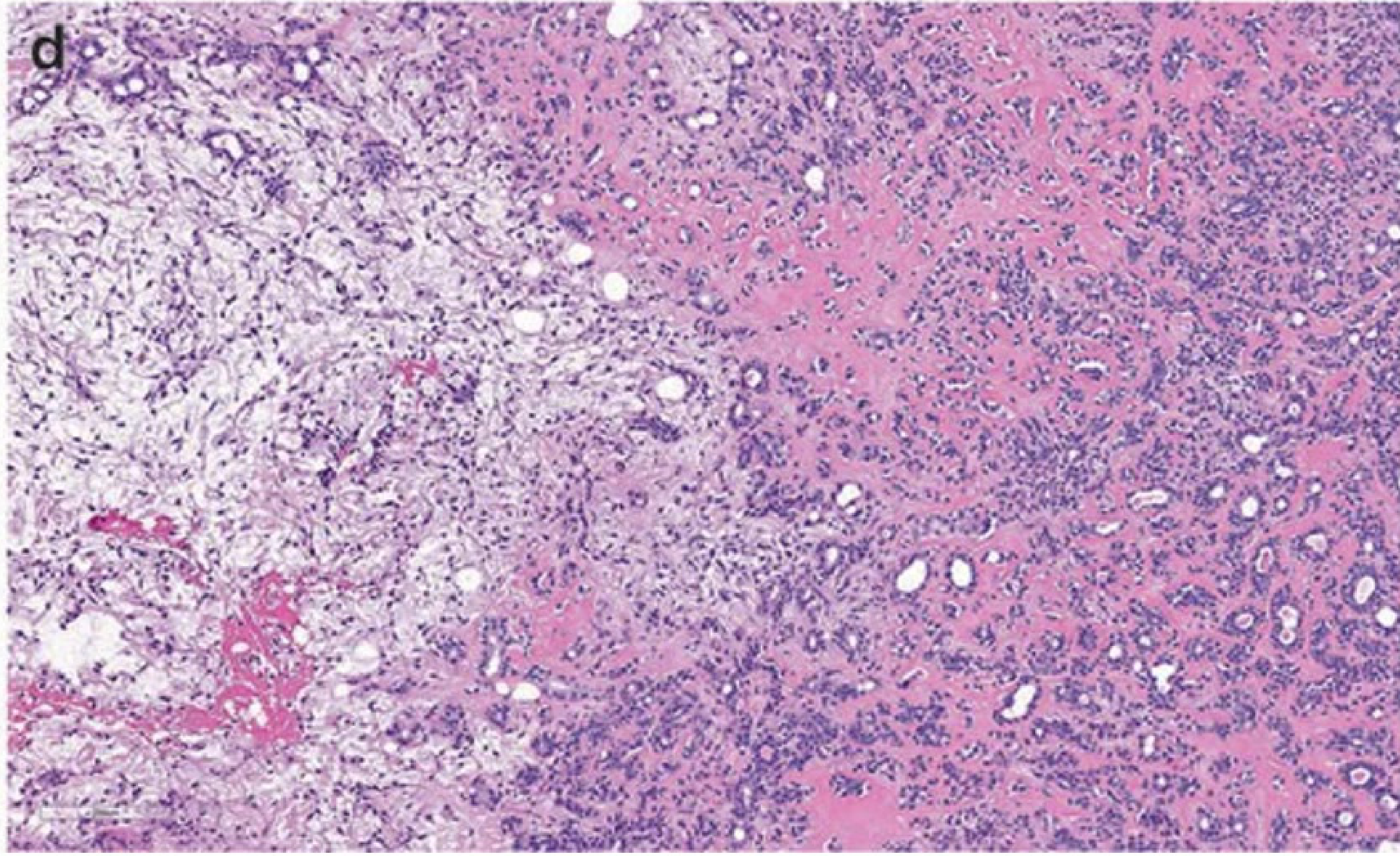
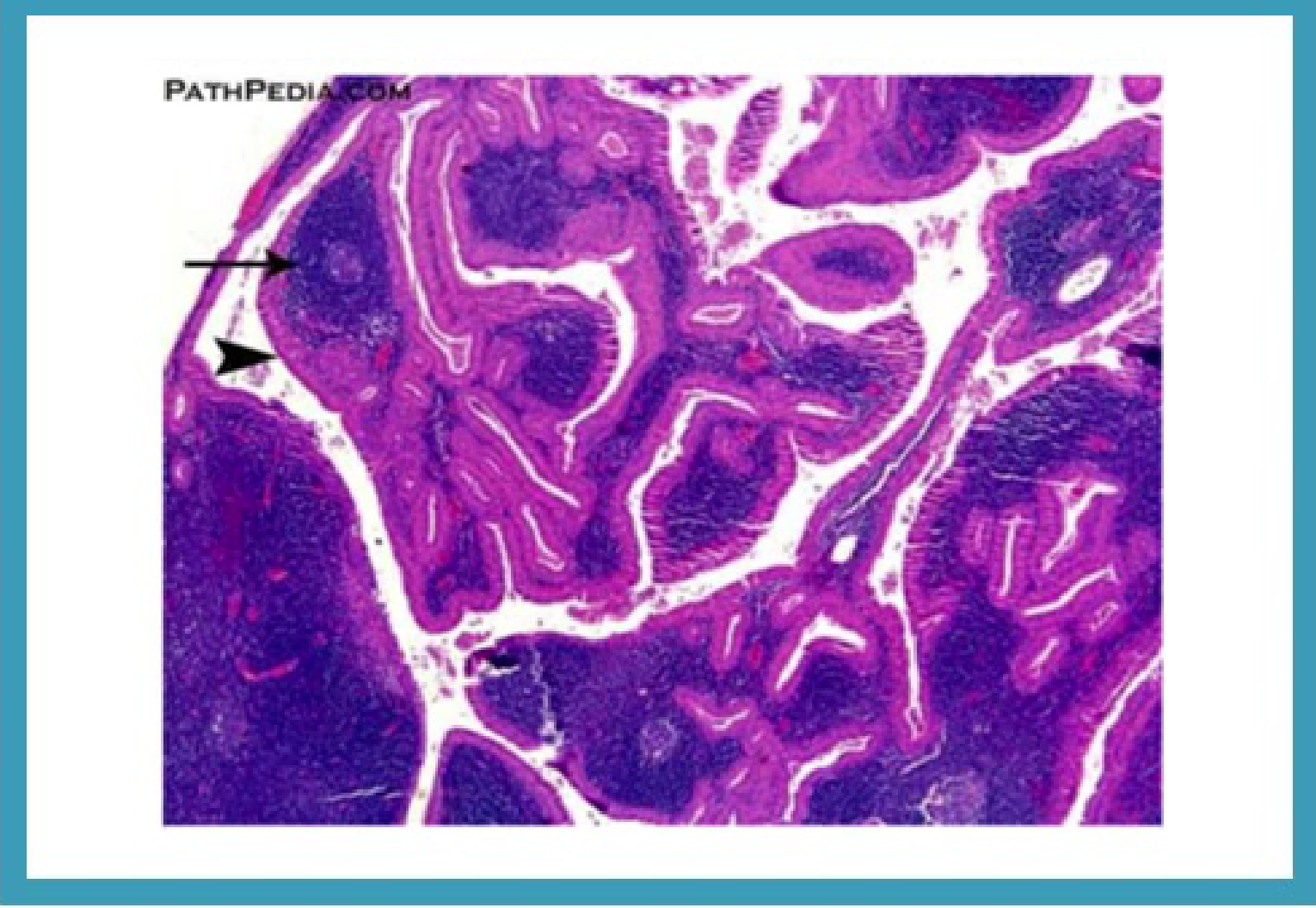
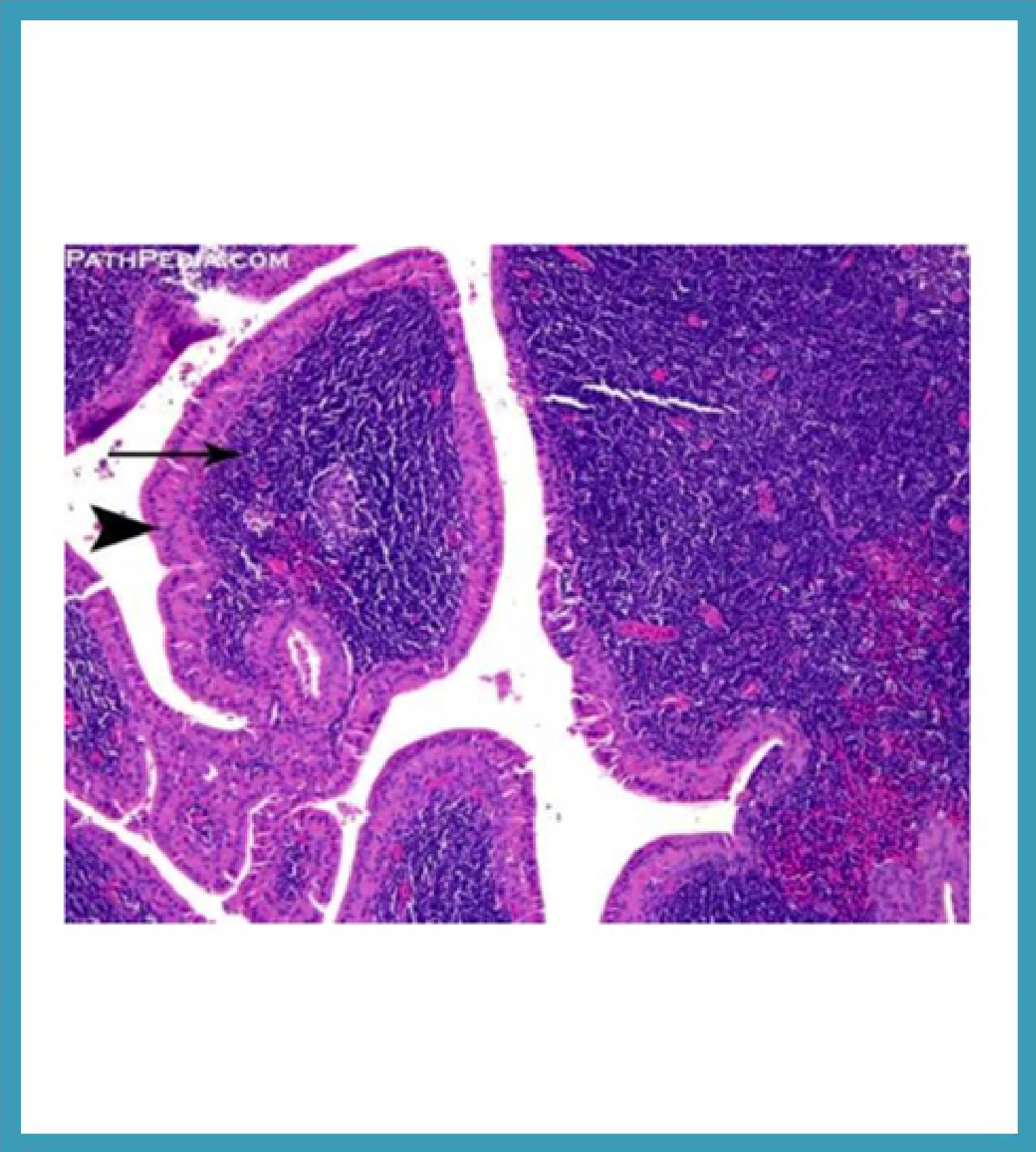
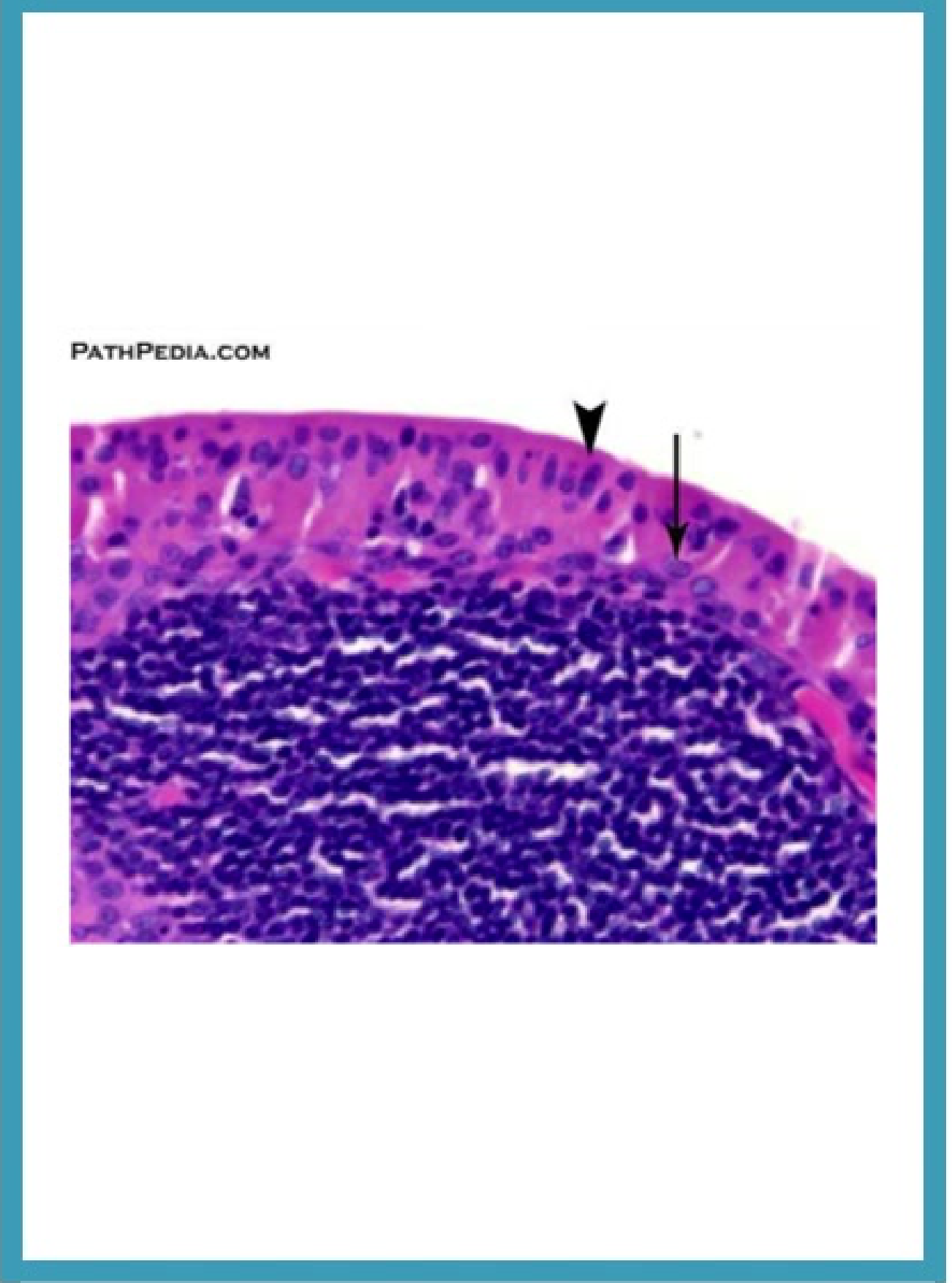
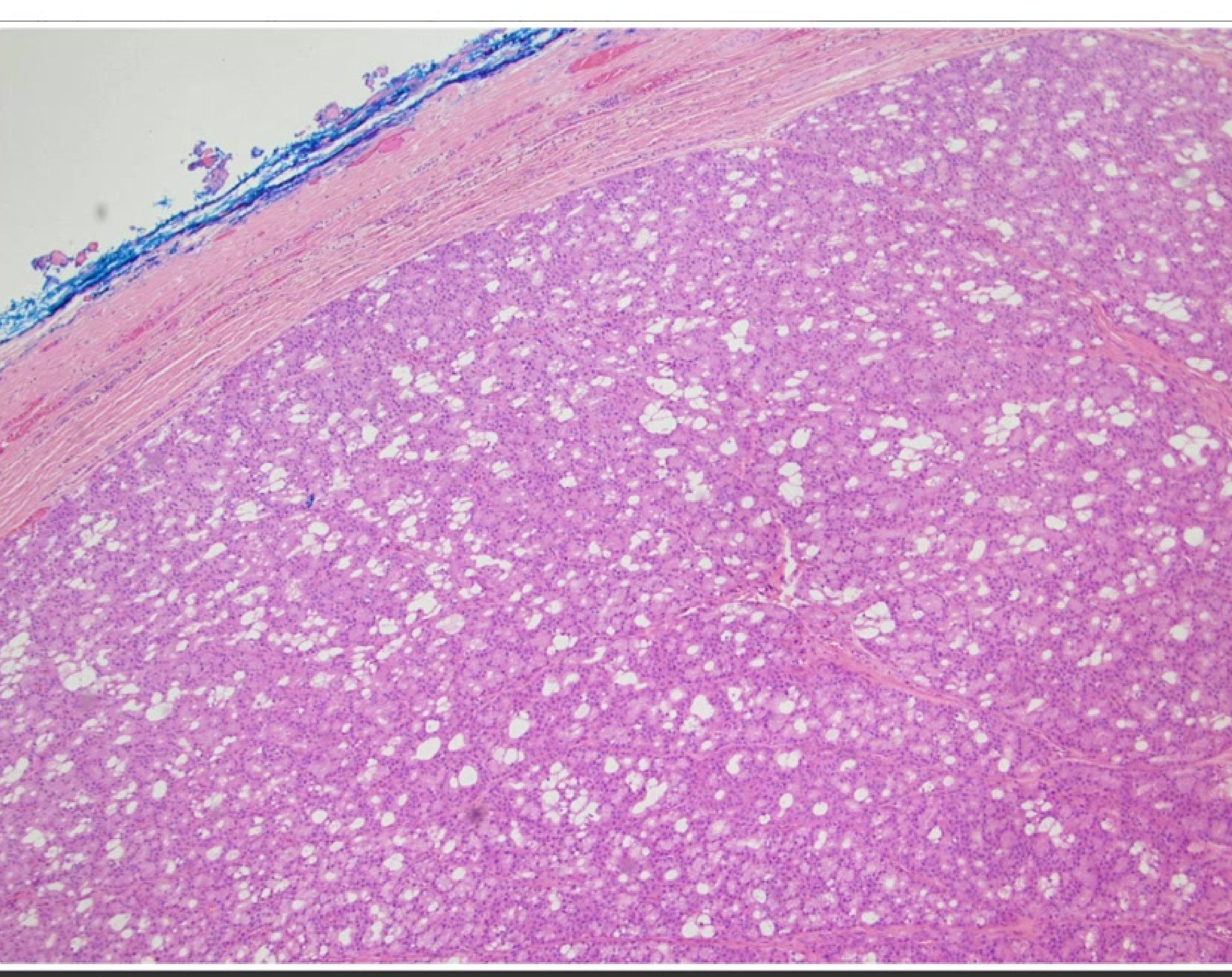
Histopathology52
- Architecture: Papillary-cystic structures.
- Stroma: Lymphoid stroma with germinal centres.
- Epithelial Component: Lined by oncocytic epithelial cells arranged in two layers:
- Inner columnar cells.
- Outer cuboidal cells.
- Secondary Features: Granulomatous reaction with Langhans-type giant cells may occur.
Histopathology (Continued)53
- Key Features:
- Papillary-cystic structures.
- Oncocytic epithelial cell lining.
- Lymphoid stroma with germinal centres.
- Cellular Detail:
- Inner columnar epithelial cells.
- Outer cuboidal epithelial cells.
- Potential for granulomatous reaction with Langhans-type giant cells.
Histopathology Summary54
- Structural Patterns: Papillary-cystic formations.
- Cellular Lining: Oncocytic epithelial cells (inner columnar and outer cuboidal).
- Background: Lymphoid stroma containing germinal centres.
- Inflammatory Response: Possible granulomatous reaction with Langhans-type giant cells.
Clinical Evaluation and Imaging55
- Clinical Evaluation:
- History and physical examination, including Head and Neck (H&N) exam.
- Assessment of risk factors, specifically smoking history.
- Role of Imaging:
- The necessity of imaging for clinically benign, superficial parotid tumours is unclear.
- Warthin’s tumours appear hypermetabolic on PET scans.
Management and Outcomes56
- Surgical Management: Complete excision with an adequate margin.
- Superficial Parotidectomy Risks: Facial nerve damage, Frey’s syndrome, haematoma.
- Prognosis:
- Low recurrence rate.
- Malignant transformation is rare (approximately 0.3%).
- Conservative Management: Observation is considered controversial.
Oncocytoma57
Introduction58
- Other names: Oncocytic adenoma, oxyphilic adenoma.
- Definition: An uncommon benign salivary gland neoplasm predominantly composed of large eosinophilic epithelial cells called oncocytes.
Epidemiology
- Prevalence: Uncommon (up to 2% of all salivary gland neoplasms).
- Age: Most common in the 6th to 8th decades of life.
- Gender: No gender predilection.
Histopathology59
- Cellular Morphology: Monotonous large polygonal cells with well-defined cell borders, deeply eosinophilic granular cytoplasm (or clear cell/glycogen change), and small round nuclei.
- Growth Patterns: Sheets, trabeculae, acini, or follicular patterns.
- Stroma and Inclusions:
- Vascular stroma.
- Background of oncocytic nodular hyperplasia.
- Psammoma bodies and tyrosine-rich crystals may be present.
- Exclusions: No mitotic figures and no elastosis.
Diagnosis60
- Clinical Assessment: History and physical examination.
- Investigations:
- Imaging: Ultrasound, CT, MRI.
- Cytology.
- Scintigraphy: Technetium 99-m pertechnetate scintigraphy; oncocytomas present as “hot” lesions.
Management
- Treatment: Surgical excision.
- Prognosis: Recurrences are rare, though additional oncocytomas may arise in the residual salivary gland tissue.
Mucoepidermoid Carcinoma
Introduction61
- Other names: Mucoepidermoid tumour.
- Definition: A salivary gland malignancy composed of mucinous, intermediate (clear-cell), and squamoid/epidermoid tumour cells forming cystic and solid patterns.
- Prevalence: Most common malignant salivary gland tumour in children and young adults.
Epidemiology and Aetiology
- Age: Wide age range, with a peak incidence in the second decade of life.
- Risk Factors: May develop secondary to radiation or chemotherapy during childhood (median latency period of 8 years).
Clinical Presentation62
- General Features: Varies by site, size, and grade; generally presents as a slow-growing mass.
- Specific Presentations:
- Cystic intraoral MEC can resemble a mucocele.
- Mucinous MEC may fluctuate in size due to cyst rupture.
- Common Sites: Parotid gland (most common), followed by the palate, submandibular gland, and other intraoral minor salivary glands.
- Rare Sites: Primary intraosseous (central) MECs.

Histopathology63
- Architecture: Numerous mucin-filled cysts of varying shapes and sizes and cribriform structures set within a dense desmoplastic stroma.
- Cell Types: Cystic spaces are lined by a combination of:
- Mucocytes: Pale cytoplasm and peripherally displaced nuclei.
- Intermediate cells.
- Epidermoid cells: Polygonal with central, mildly pleomorphic nuclei and abundant cytoplasm (no definite keratinization).
- Stroma: Extensive sclerosis and a prominent peritumoral inflammatory infiltrate (lymphocytes, plasma cells, and lymphoid aggregates with reactive germinal centers).
Diagnosis and Management64
- Diagnosis: History, clinical examination, imaging (ultrasound, CT, MRI), cytology, and biopsy.
- Management:
- Surgical excision with clear margins.
- Radiotherapy may be used for local control in specific cases.
- Prognosis:
- Low- and intermediate-grade MECs are generally less aggressive.
- 10-year survival rates:
- Low-grade: 90%
- Intermediate-grade: 70%
- High-grade: 25%
Acinic Cell Carcinoma
Introduction65
- Other names: Acinic cell adenocarcinoma, acinar cell carcinoma.
- Definition: A malignant salivary gland neoplasm composed of cancer cells with acinar features.
- Prevalence: Second most common salivary gland malignancy in children.
Epidemiology and Aetiology
- Age: Wide range (including children); most patients are aged 50 years and above.
- Gender: Female predominance (1.5:1).
- Aetiology: Unknown; previous radiation exposure is a known risk factor.
Clinical Presentation66
- Mass Characteristics: Slow-growing, solitary, unfixed masses; some may be multinodular or fixed to the skin.
- Location: Over 90% occur in the parotid glands; can also occur in intraoral minor salivary glands.
- Symptoms:
- Pain occurs in approximately one-third of patients.
- Facial paralysis may develop if there is neural involvement.

Histopathology67
- Cellular Diversity: Multiple cell types including serous acinar, intercalated ductal, vacuolated, nonspecific glandular, and clear cells.
- Acinar Cell Features: Large and polyhedral with basophilic granular cytoplasm and eccentric nuclei. Focal diastase-resistant PAS positive reaction may be present.
- Morphologic Patterns: Solid, microcystic, papillary cystic, and follicular.
- Stroma: Prominent lymphoid infiltrate (tumour-associated lymphoid proliferation) ranging from patchy collections to dense infiltrates with follicles.
- Exclusions: Mitosis, necrosis, and significant pleomorphism are usually absent.
Diagnosis and Management68
- Diagnosis: History, clinical examination, imaging, cytology, and biopsy (noting wide variation in histomorphology).
- Management:
- Surgical excision.
- Radiotherapy may be indicated in some cases.
- Prognosis:
- Recurrence rates up to 35%.
- Metastasis can occur to regional lymph nodes and lungs.
- Good 10-year survival rate of approximately 90%.
Adenoid Cystic Carcinoma
Introduction69
- Definition: A slow-growing but relentless salivary gland malignancy composed of epithelial and myoepithelial neoplastic cells.
- Architecture: Forms various patterns including tubular and cribriform structures with variably solid components.
- Prevalence: Accounts for less than 10% of all salivary gland neoplasms.
Epidemiology
- Incidence: Annual incidence of 2 cases per 100,000 population.
- Age: Median age of 57 years.
- Gender: Female predominance (1.5:1).
- Ethnicity: No ethnic predilection.
Aetiology and Clinical Presentation70
- Aetiology: Unknown.
- Symptoms:
- Mass/swelling.
- Perineural Invasion: Neurological signs such as numbness, paraesthesia, pain, or facial/tongue weakness.
- Location: Most frequent in major salivary glands; over 30% occur in minor glands (oral cavity, sinonasal tract).
- Metastasis:
- Lymph node involvement is uncommon.
- Distant metastasis reported in over 50% of cases (lungs, bone, liver, brain).

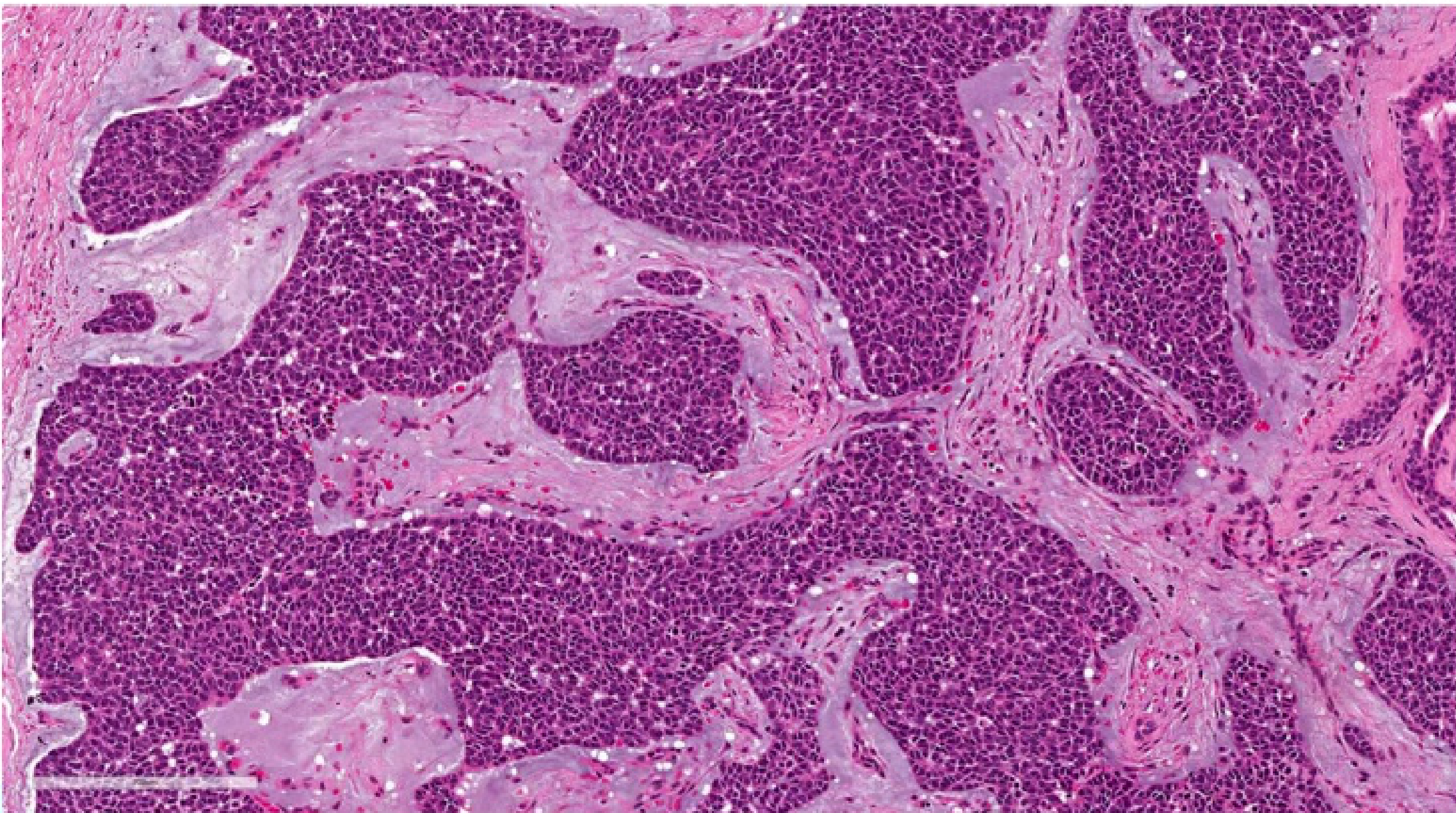
Histopathology71
- Cell Types: Biphasic tumor composed of ductal cells (cuboidal, eosinophilic cytoplasm) and myoepithelial cells (dark angulated nuclei, scanty cytoplasm, basaloid appearance).
- Architectural Patterns:
- Tubular: Simple tubules with inner ductal and outer myoepithelial cells.
- Cribriform: Predominantly myoepithelial cells with myxoid or hyalinized globules; scattered ductal elements
- The cribriform pattern is often described as having a "Swiss cheese" appearance.
- Solid: Nests and sheets of basaloid cells
- The solid architectural pattern is associated with the worst clinical prognosis.
- Invasion: Perineural invasion is frequent.
- High-Grade Transformation: Characterized by comedo-type necrosis, frequent mitoses (>10 per 10 HPF), and marked nuclear atypia. Associated with higher risk of metastasis and death.
Histopathologic Patterns72
- Tubular Pattern: Composed of inner ductal and outer myoepithelial cells.
- Cribriform Pattern: Composed predominantly of myoepithelial cells admixed with hyalinized or myxoid globules.
- Solid Pattern: Tumour cells forming solid sheets and nests.
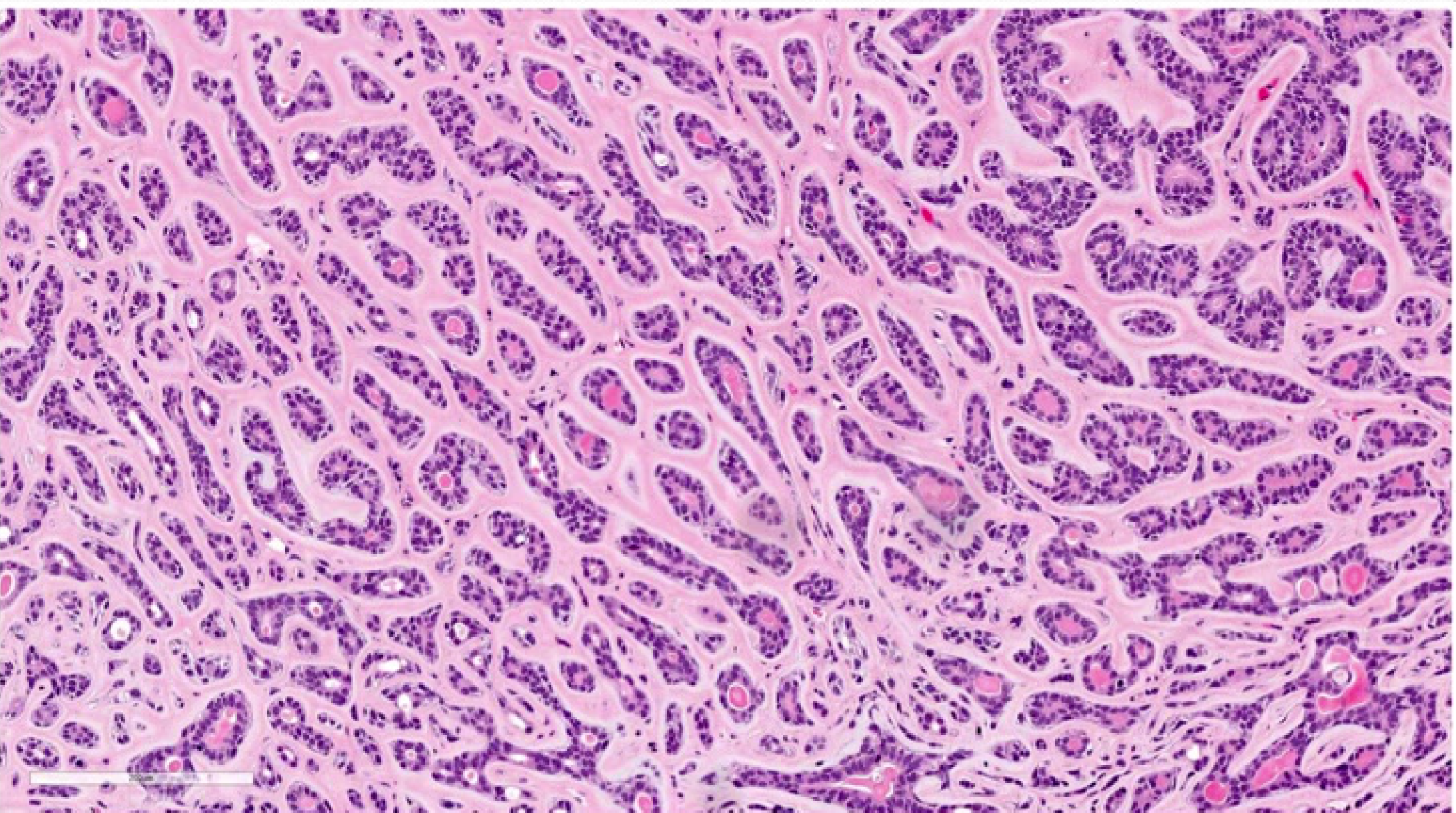 | 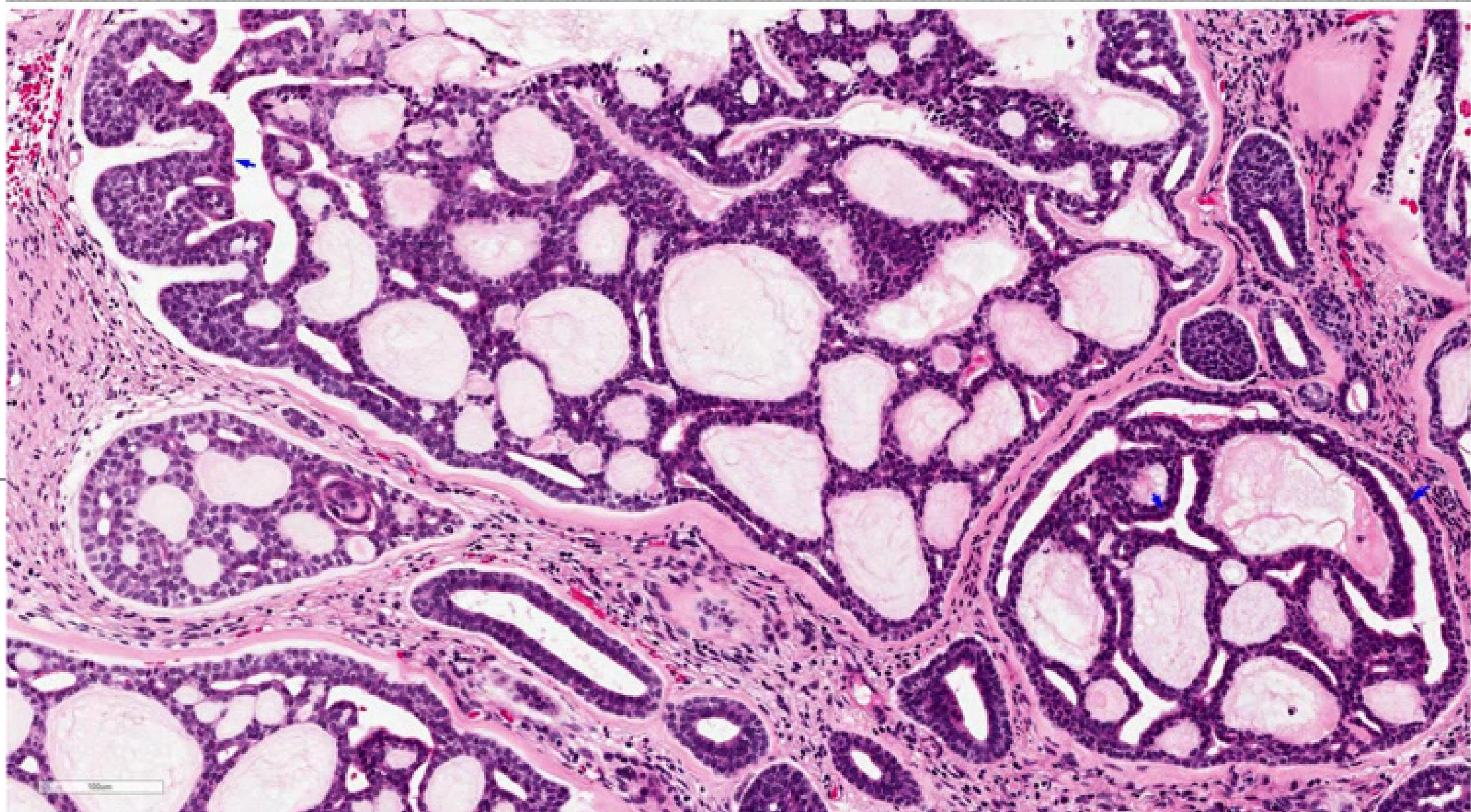 |
 |
Diagnosis and Management73
- Diagnosis: History, clinical examination, imaging, cytology, and biopsy.
- Management:
- Surgery: Wide excision with clear margins.
- Radiotherapy: Improves local control in cases of microscopic residual disease.
- Prognosis:
- Local recurrence rate is highly variable.
- Limited success with radiotherapy/chemotherapy for recurrent or metastatic disease.
- 10-year survival rate: 50-70%.
Polymorphous Low Grade Adenocarcinoma74
Introduction75
- Other names: Terminal duct carcinoma, lobular carcinoma, cribriform adenocarcinoma of tongue/minor salivary glands.
- Definition: A malignant salivary gland tumour (PAC) characterised by cytological uniformity, histomorphological diversity, and an infiltrative growth pattern.
- Prevalence: Second most common intraoral malignant salivary gland neoplasm.
Epidemiology and Aetiology
- Age: Wide range; most commonly diagnosed in patients over 50 years of age.
- Gender: Female predominance (2:1).
- Aetiology: Unknown.
Clinical Presentation76
- Symptoms: Painless mass of variable duration (weeks to years); may show bleeding, telangiectasia, or ulceration.
- Location: Most common site is the palate (hard > soft), followed by lips, buccal mucosa, and alveolar mucosa. Less common in major glands, nasopharynx, and nasal cavity.
- Behaviour: Aggressive; may invade soft tissue and bone.
- Invasion: Frequent perineural involvement.
- Metastasis: Nodal metastasis in up to 15% of cases.

Histopathology77
- Cytologic Uniformity: Monotonous tumor cells with pale nuclei and marked chromatin clearing (resembling papillary thyroid carcinoma).
- Architectural Diversity: Highly variable patterns including:
- Single filing arrangement
- Trabecular, tubular, and reticular
- Papillary, solid, and cribriform
- Growth Features: Targetoid arrangement and streaming of tumor cells/nests around nerves and vessels are common.
Diagnosis and Management78
- Diagnosis: History, clinical examination, imaging, and cytology.
- Biopsy Challenges: Difficulties with small samples; neoplastic cells may appear deceptively bland.
- Management:
- Surgical excision with clear margins.
- Radiotherapy may be appropriate in select cases.
- Prognosis:
- Overall survival is generally good.
- Local recurrence rates up to 33% are reported; approximately half occur within 5 years.
This section discusses the aetiology, clinical features, diagnosis, and management of dry mouth.
Dry Mouth and Xerostomia
Clinical Definitions and Impact
Terminology and Diagnostic Thresholds79
- Salivary gland hypofunction: Decreased saliva flow rate.
- Hyposalivation: Pathological low saliva flow rate.
- Unstimulated whole saliva flow rate: ≤ 0.1 ml/min
- Stimulated whole saliva flow rate: ≤ 0.5–0.7 ml/min
- Xerostomia: The subjective feeling of oral dryness.
Clinical Significance in Dentistry80
Dry mouth has a significant negative impact on quality of life, including:
- Functional limitations: Difficulty chewing and swallowing.
- Physical symptoms: Physical pain and taste changes.
- Psychological impact: Physical disability and psychological discomfort.
- Oral health risks: Increased susceptibility to dental diseases.
 |  |
 |
Clinical Assessment and Examination
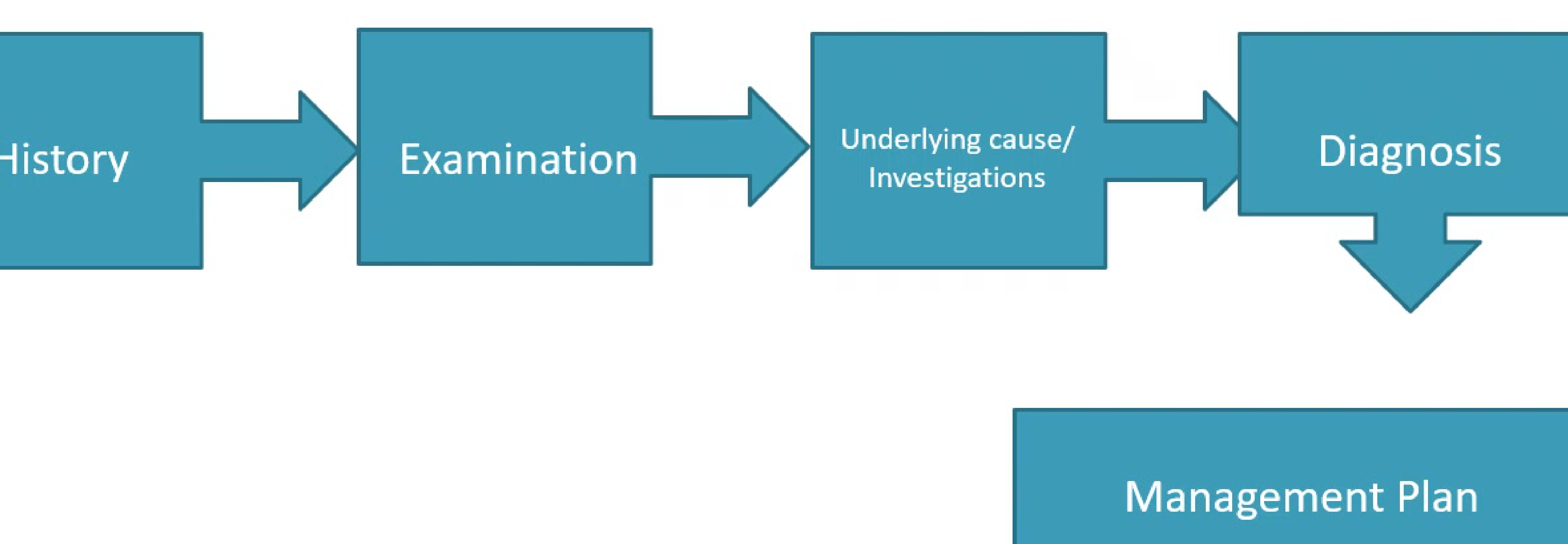
Clinical Pathway81
- History
- Examination
- Underlying cause / Investigations
- Diagnosis
- Management Plan
Patient History and Subjective Assessment82
-
Subjective symptoms
- Complaints of xerostomia throughout the oral cavity or localized to specific parts.
- Behavioral indicators: Carrying water bottles or keeping a glass of water beside the bed.
- Noted changes in saliva consistency.
-
Xerostomia Assessment (Fox et al. 1987)
- Does the amount of saliva in your mouth seem to be too little, too much, or do you not notice it?
- Do you have any difficulty in swallowing?
- Does your mouth feel dry when eating a meal?
- Do you sip liquids to aid in swallowing dry food?
-
Medical and Lifestyle Factors
- Review of medical history and current medications.
- Assessment of behaviors: Water intake, caffeine intake, alcohol consumption, and smoking.
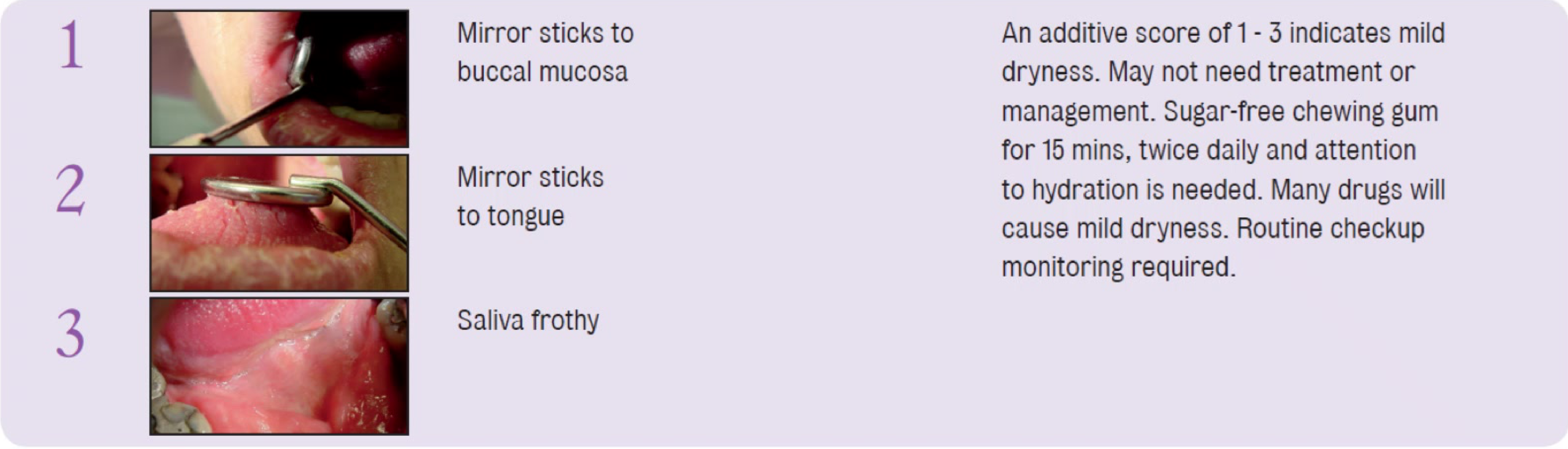
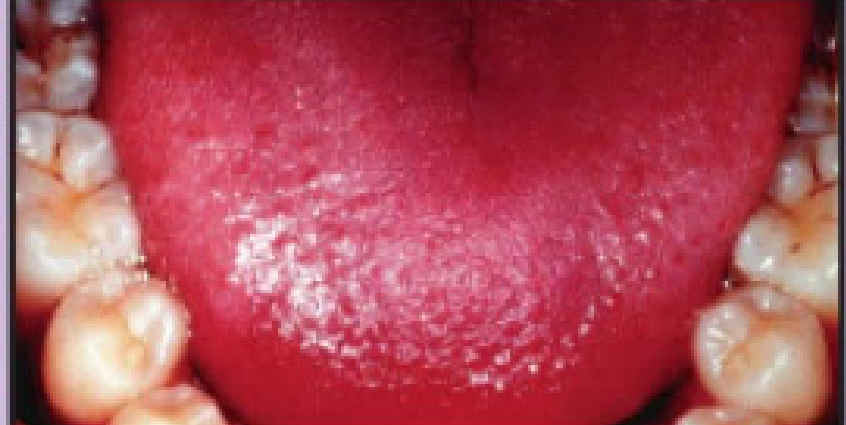
The Challacombe Scale: Mild Dryness83
An additive score of 1 - 3 indicates mild dryness.
-
Clinical Signs:
- Mirror sticks to buccal mucosa
- Mirror sticks to tongue
- Saliva appears frothy
-
Management:
- May not require intensive treatment.
- Use sugar-free chewing gum for 15 minutes, twice daily.
- Maintain proper hydration.
- Monitor during routine checkups, as many drugs cause mild dryness.
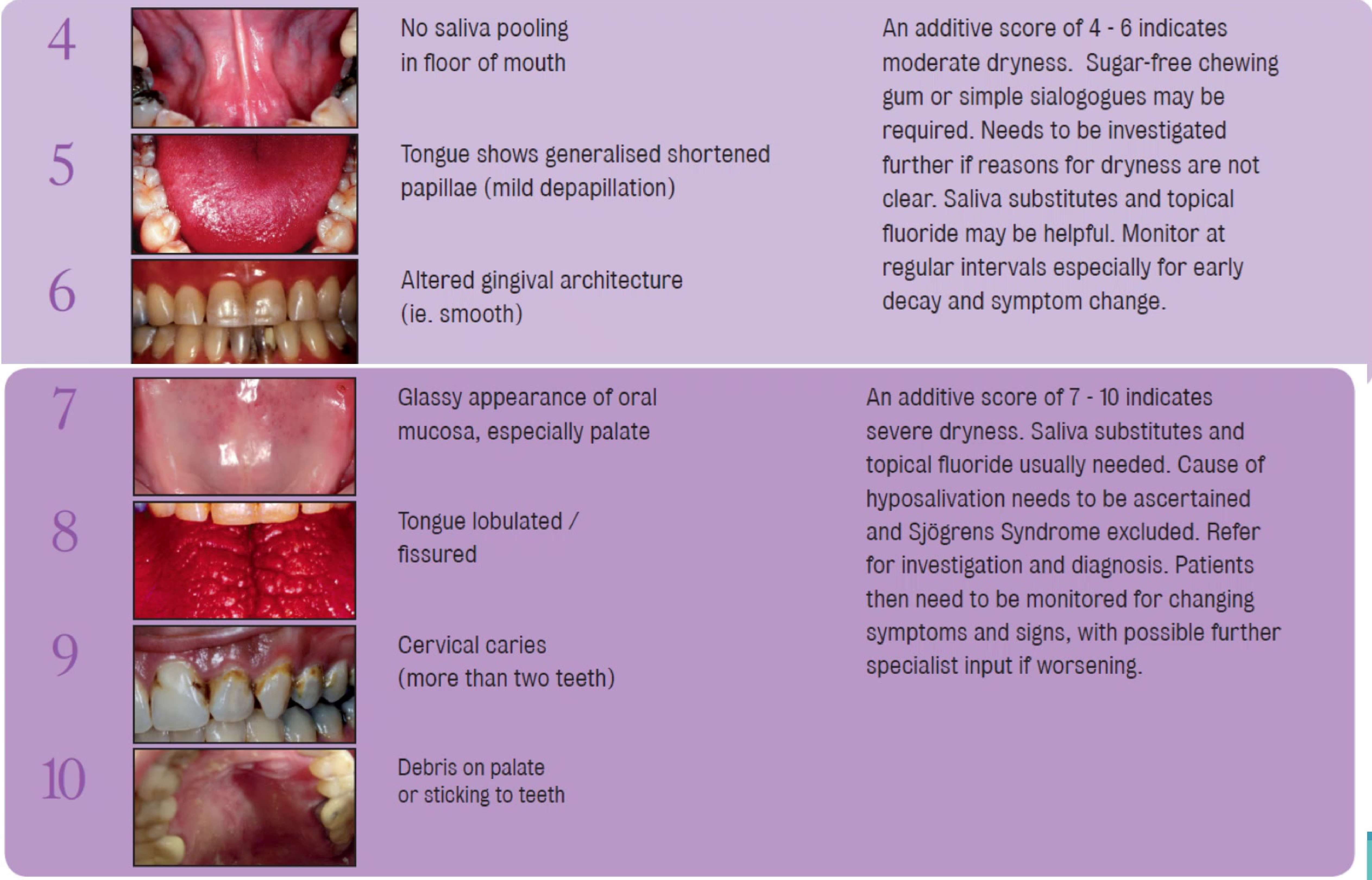
The Challacombe Scale: Moderate Dryness84
An additive score of 4 - 6 indicates moderate dryness.
-
Clinical Signs: 4. No saliva pooling in the floor of the mouth 5. Tongue shows generalized shortened papillae (mild depapillation) 6. Altered gingival architecture (e.g., smooth appearance)
-
Management:
- Sugar-free chewing gum or simple sialogogues may be required.
- Further investigation is needed if the cause is unclear.
- Saliva substitutes and topical fluoride may be helpful.
- Regular monitoring for early decay and symptom changes.
 |  |
 |
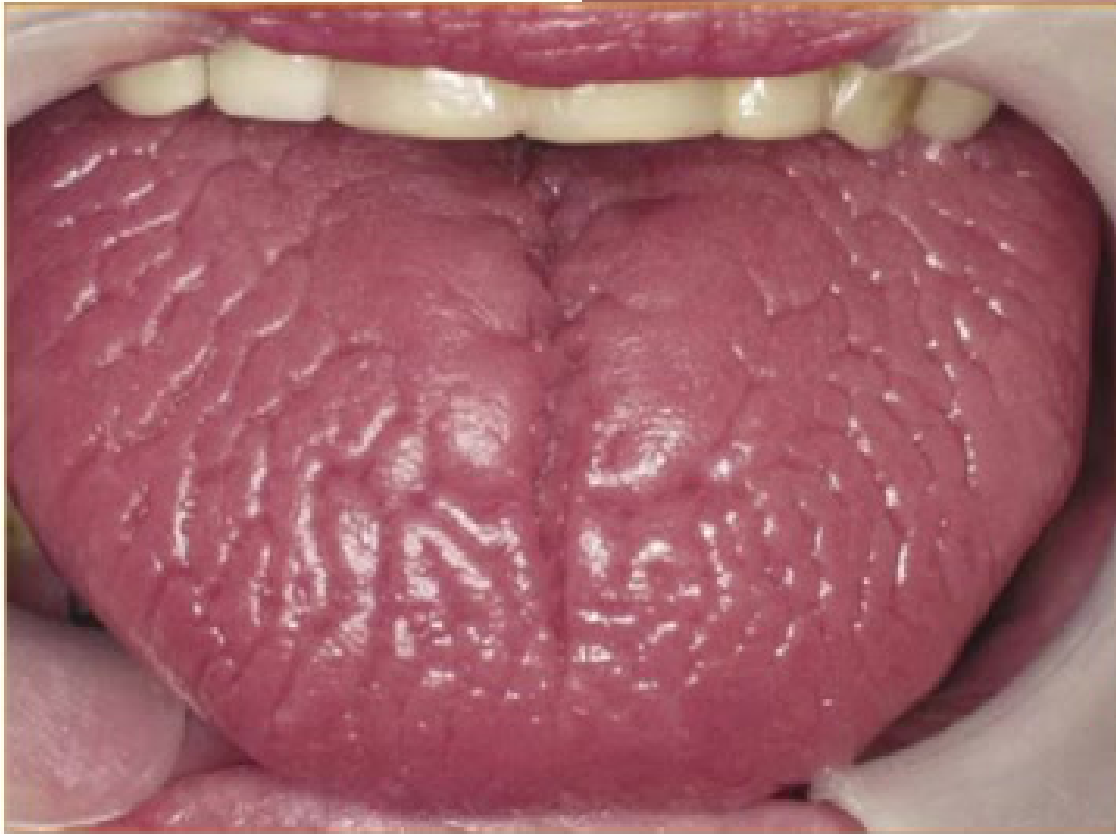
The Challacombe Scale: Severe Dryness85
An additive score of 7 - 10 indicates severe dryness.
-
Clinical Signs: 7. Glassy appearance of oral mucosa, especially the palate 8. Tongue is lobulated or fissured 9. Cervical caries (affecting more than two teeth) 10. Debris on the palate or sticking to teeth
-
Management:
- Saliva substitutes and topical fluoride are usually necessary.
- The cause of hyposalivation must be determined; Sjögren’s Syndrome should be excluded.
- Refer for specialist investigation and diagnosis.
- Continuous monitoring for worsening signs and symptoms.
Underlying Causes and Investigations
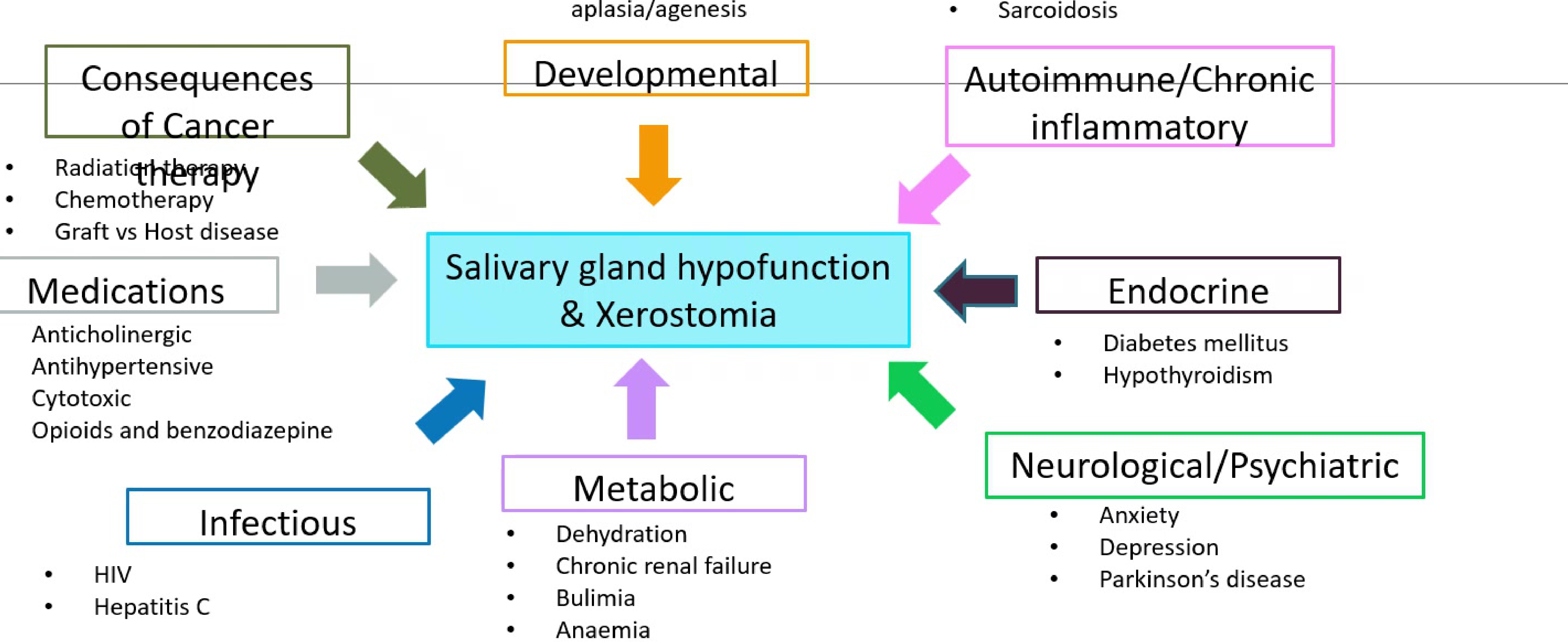
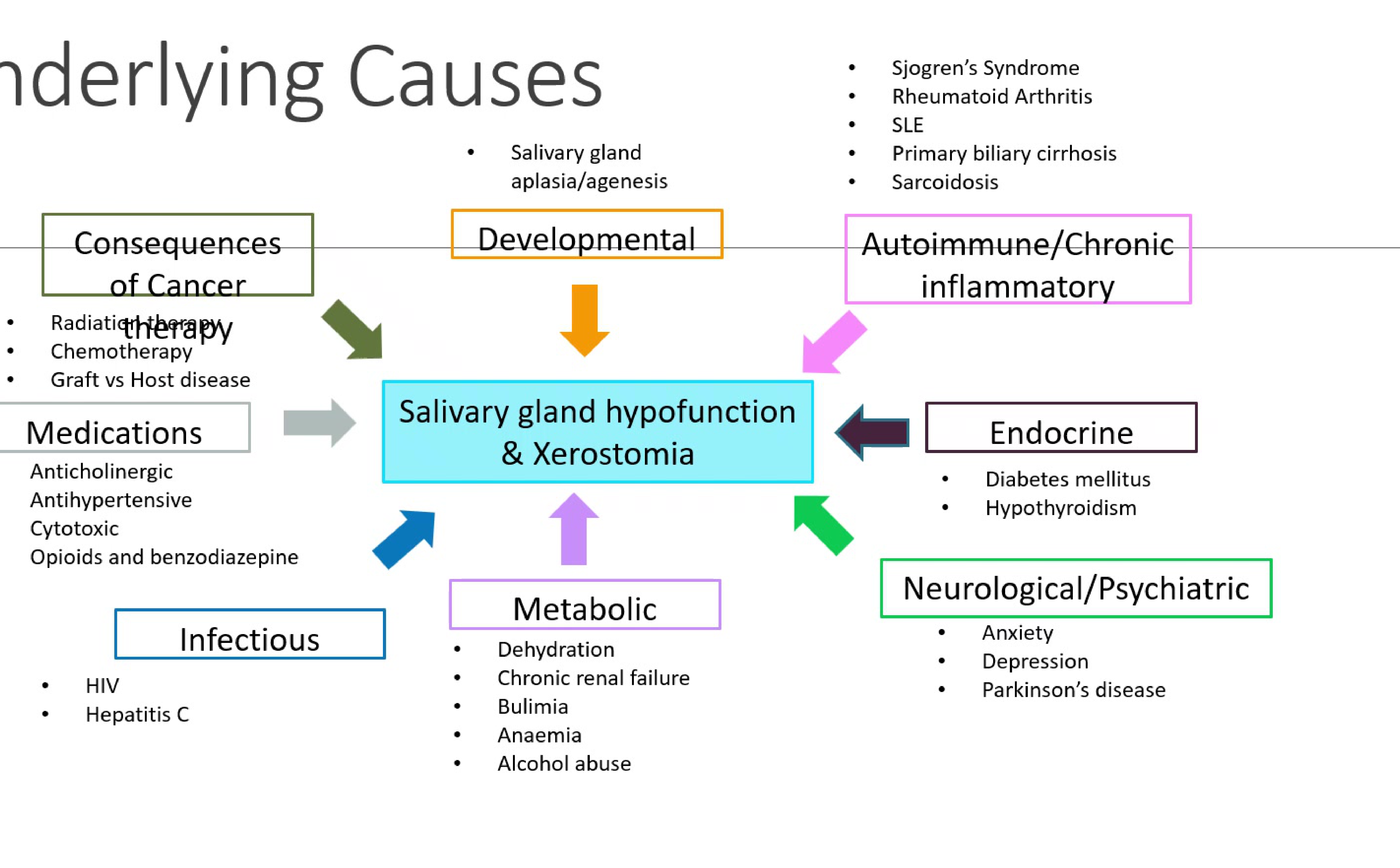
Etiology of Salivary Gland Hypofunction and Xerostomia86
Identification of the underlying cause is essential for the management of salivary gland hypofunction and the subjective feeling of xerostomia.
Categorization of Underlying Causes87
-
Consequences of Cancer Therapy
- Radiation therapy
- Chemotherapy
- Graft vs. Host disease
-
Medications
- Anticholinergics
- Antihypertensives
- Cytotoxic drugs
- Opioids and benzodiazepines
-
Infectious Diseases
- HIV
- Hepatitis C
-
Developmental Disorders
- Salivary gland aplasia or agenesis
-
Autoimmune and Chronic Inflammatory Conditions
- Sjögren’s Syndrome
- Rheumatoid Arthritis
- Systemic Lupus Erythematosus (SLE)
- Primary biliary cirrhosis
- Sarcoidosis
-
Endocrine Disorders
- Diabetes mellitus
- Hypothyroidism
-
Neurological and Psychiatric Factors
- Anxiety
- Depression
- Parkinson’s disease
-
Metabolic and Other Factors
- Dehydration
- Chronic renal failure
- Bulimia
- Anaemia
- Alcohol abuse
 |  |
Diagnostic Investigations88
- Saliva Testing: Unstimulated or stimulated whole saliva flow rate tests.
- Serology: Testing for SS-A, SS-B, ds-DNA, fasting glucose/HbA1c, and thyroid function.
- Imaging: Ultrasound, CT, or MRI imaging.
- Biopsy: Salivary gland biopsy.
- Ophthalmology: Schirmer’s test to assess tear production.
Management Strategies
Salivary Stimulation Techniques89
- Mechanical Stimulation: Chewing sugar-free gum to aid in caries prevention.
- Pharmacological Intervention: Use of sialogogues such as Pilocarpine
- Pilocarpine is a pharmacological stimulant, but note that side effects include excessive sweating and it is contraindicated in patients with cardiovascular disease.
- Electro-stimulation: Devices like the Saliwell device, which augment the salivary reflex and stimulate motor neural pathways of the submandibular and sublingual glands.
 |  |
Management of Complications90
-
Mucosal Care
- Antifungal therapy for secondary infections.
- Reduction of irritants: Avoid alcohol, smoking, and hot or spicy foods.
- Ensure proper fit and hygiene of dentures.
-
Caries Prevention Protocol
- Strict oral hygiene maintenance.
- Regular use of topical fluorides (e.g., high-fluoride toothpaste).
- Frequent dental recalls are recommended for monitoring and prevention.
- Antifungal therapy should be considered for the management of candidosis.
- Dietary modifications to reduce sugar intake (e.g., use of Xylitol).

Contact Information
Congratulations on completing the module.
Academic Inquiries91
If you have any questions regarding the material covered in this presentation, please direct your correspondence to:
- Email: Lalima.Tiwari@uwa.edu.au
Footnotes
-
Original PDF page 1: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.1 ↩
-
Original PDF page 2: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.2 ↩
-
Original PDF page 4: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.4 ↩
-
Original PDF page 5: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.5 ↩
-
Original PDF page 6: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.6 ↩
-
Original PDF page 7: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.7 ↩
-
Original PDF page 9: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.9 ↩
-
Original PDF page 8: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.8 ↩
-
Original PDF page 11: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.11 ↩
-
Original PDF page 10: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.10 ↩
-
Original PDF page 13: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.13 ↩
-
Original PDF page 12: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.12 ↩
-
Original PDF page 14: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.14 ↩
-
Original PDF page 15: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.15 ↩
-
Original PDF page 16: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.16 ↩
-
Original PDF page 17: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.17 ↩
-
Original PDF page 18: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.18 ↩
-
Original PDF page 19: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.19 ↩
-
Original PDF page 20: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.20 ↩
-
Original PDF page 21: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.21 ↩
-
Original PDF page 22: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.22 ↩
-
Original PDF page 23: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.23 ↩
-
Original PDF page 24: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.24 ↩
-
Original PDF page 25: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.25 ↩
-
Original PDF page 26: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.26 ↩
-
Original PDF page 27: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.27 ↩
-
Original PDF page 28: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.28 ↩
-
Original PDF page 29: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.29 ↩
-
Original PDF page 30: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.30 ↩
-
Original PDF page 31: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.31 ↩
-
Original PDF page 32: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.32 ↩
-
Original PDF page 33: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.33 ↩
-
Original PDF page 34: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.34 ↩
-
Original PDF page 35: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.35 ↩
-
Original PDF page 36: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.36 ↩
-
Original PDF page 37: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.37 ↩
-
Original PDF page 38: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.38 ↩
-
Original PDF page 39: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.39 ↩
-
Original PDF page 40: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.40 ↩
-
Original PDF page 3: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.3 ↩
-
Original PDF page 41: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.41 ↩
-
Original PDF page 42: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.42 ↩
-
Original PDF page 43: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.43 ↩
-
Original PDF page 44: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.44 ↩
-
Original PDF page 45: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.45 ↩
-
Original PDF page 46: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.46 ↩
-
Original PDF page 47: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.47 ↩
-
Original PDF page 48: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.48 ↩
-
Original PDF page 49: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.49 ↩
-
Original PDF page 50: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.50 ↩
-
Original PDF page 51: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.51 ↩
-
Original PDF page 52: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.52 ↩
-
Original PDF page 53: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.53 ↩
-
Original PDF page 54: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.54 ↩
-
Original PDF page 55: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.55 ↩
-
Original PDF page 56: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.56 ↩
-
Original PDF page 59: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.59 ↩
-
Original PDF page 57: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.57 ↩
-
Original PDF page 58: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.58 ↩
-
Original PDF page 60: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.60 ↩
-
Original PDF page 61: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.61 ↩
-
Original PDF page 62: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.62 ↩
-
Original PDF page 63: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.63 ↩
-
Original PDF page 64: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.64 ↩
-
Original PDF page 65: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.65 ↩
-
Original PDF page 66: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.66 ↩
-
Original PDF page 67: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.67 ↩
-
Original PDF page 68: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.68 ↩
-
Original PDF page 69: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.69 ↩
-
Original PDF page 70: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.70 ↩
-
Original PDF page 71: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.71 ↩
-
Original PDF page 72: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.72 ↩
-
Original PDF page 73: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.73 ↩
-
Original PDF page 78: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.78 ↩
-
Original PDF page 74: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.74 ↩
-
Original PDF page 75: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.75 ↩
-
Original PDF page 76: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.76 ↩
-
Original PDF page 77: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.77 ↩
-
Original PDF page 79: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.79 ↩
-
Original PDF page 80: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.80 ↩
-
Original PDF page 81: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.81 ↩
-
Original PDF page 82: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.82 ↩
-
Original PDF page 83: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.83 ↩
-
Original PDF page 84: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.84 ↩
-
Original PDF page 85: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.85 ↩
-
Original PDF page 86: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.86 ↩
-
Original PDF page 87: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.87 ↩
-
Original PDF page 88: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.88 ↩
-
Original PDF page 89: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.89 ↩
-
Original PDF page 90: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.90 ↩
-
Original PDF page 91: L15 Non neoplastic and neoplastic salivary gland diseases slides, p.91 ↩