Dry Mouth
Clinical Presentation and Overview1
Dry mouth, clinically known as xerostomia, is a condition characterized by a lack of sufficient saliva to keep the mouth moist. This condition can significantly impact oral health and quality of life.
Clinical Significance
Dry mouth is one of the most underappreciated, underdiagnosed, and undermanaged oral health conditions. It presents both as a subjective symptom and an objective clinical sign, affecting daily functions such as eating, swallowing, speaking, and sleeping.
Key Characteristics
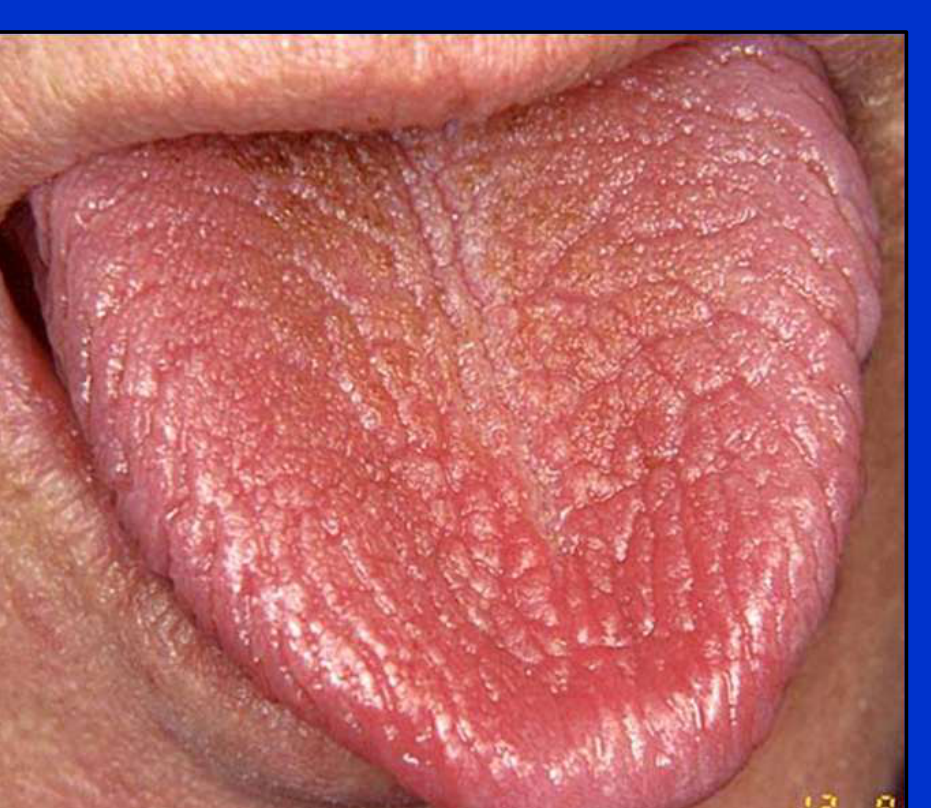
- Physical manifestations often include a dry, cracked appearance of the tongue.
- Complexity: Saliva is more than the sum of its parts; its components have multiple interacting functions.
- Persistence: Persistent dryness leads to a decline in general well-being.
- Diagnostic Difficulty: There is still much to learn about why individuals perceive dryness, which makes current treatment options sometimes unsatisfactory.
- It is a common clinical concern addressed within dental and oral medicine specialties.
Academic Affiliation
This information is presented by Dr. Agnieszka Frydrych from The University of Western Australia.
Lecture Outline2345
The following topics will be covered in this lecture:
- The physiology of saliva
- The distinction between xerostomia and hyposalivation
- Etiology including medications, disease, and radiation
- Diagnostic tools and multi-modal management strategies
Clinical Significance of Saliva6
Why talk about dry mouth?
“Saliva is not one of the popular body fluids. It lacks the drama of blood, the sincerity of sweat and the emotional appeal of tears…”
— Mandel ID, 1990
Function of Saliva
Saliva is essential for oral comfort and the maintenance of hard and soft tissues. Its absence is often only fully appreciated when functions are adversely affected.

Saliva Physiology and Function7
The salivary glands, like other secreting apparatus, are liable, per se, to become sluggish in their function. Knowing as we do the necessity of saliva, we at least are bound to employ the shortest, surest and easiest method for restoring a secretion, which in the animal system is indispensable to bodily health and energy.
— Wright S, 1842
Composition and Daily Production89
Salivary Constituents10
Saliva is composed of 99.5% water, supplemented by various inorganic and organic components.
-
Inorganic Components
- Sodium
- Potassium
- Calcium
- Magnesium
- Chloride
- Bicarbonate
- Phosphate
- Thiocyanate
- Iodide
- Fluoride
-
Organic Components
- Secretory IgA
- MUC5B and MUC7
- MUC5B specifically provides the slimy, viscoelastic coating necessary for lubrication
- Amylase
- Lysozyme
- Lactoferrin
- Lactoperoxidase for antimicrobial defense
- Statherin
- Albumin
- Glucose
- Lactate
- Lipids
- Amino Acids
- Urea and Ammonia
 | 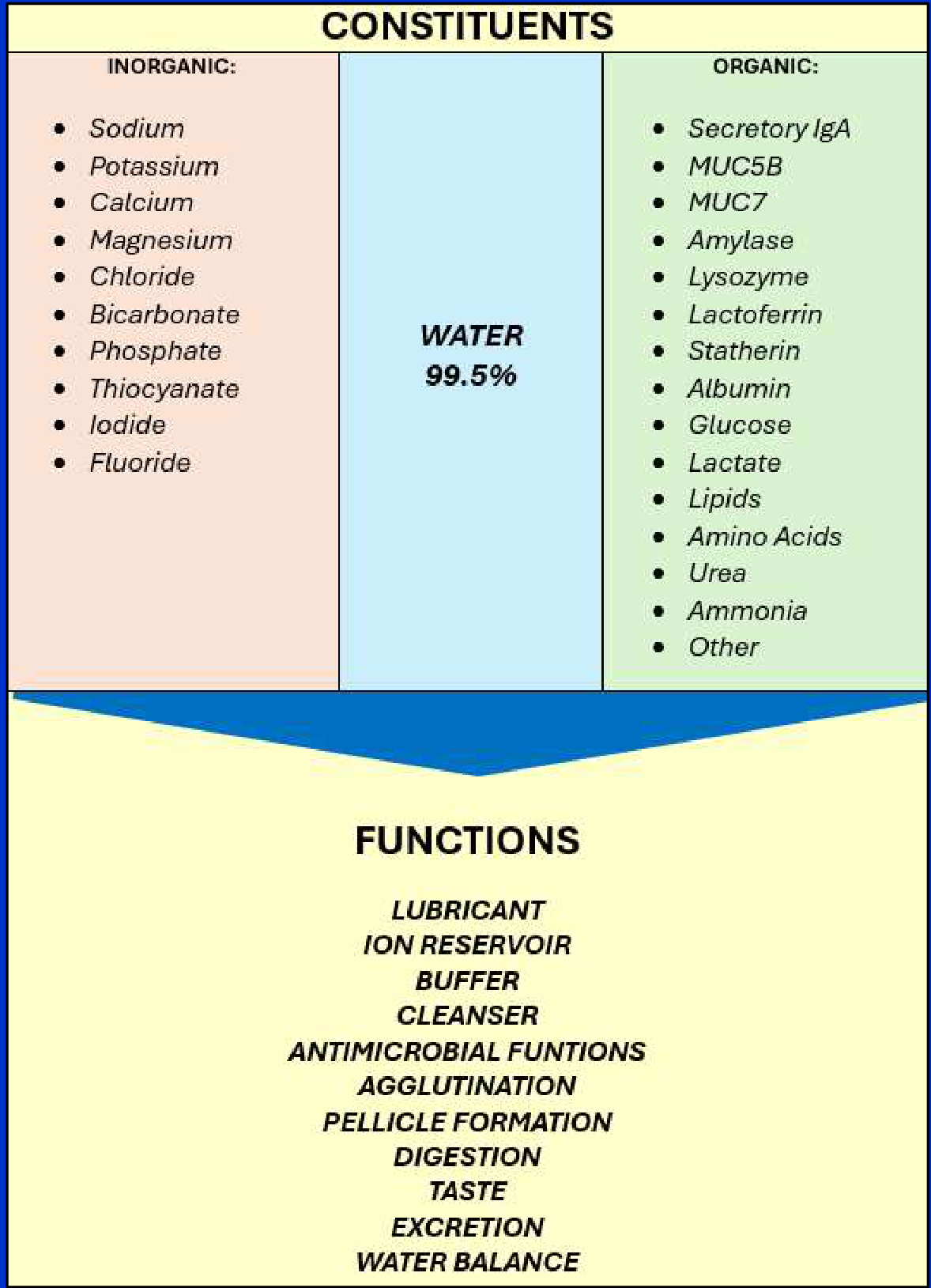 |
Salivary Functions
Saliva serves multiple critical roles in oral and systemic health:
-
Protection and Maintenance: Lubricant, Ion reservoir, Buffer, Cleanser, Pellicle formation.
-
Biological Defense: Antimicrobial functions, Agglutination.
-
Sensory and Digestive: Digestion, Taste.
-
Systemic Regulation: Excretion, Water balance.
-
Approximately 600ml of saliva is produced in a 24-hour period.
-
Stimulated saliva contributes up to 80-90% of the total daily volume.
-
Unstimulated saliva is the most important factor for maintaining oral comfort.
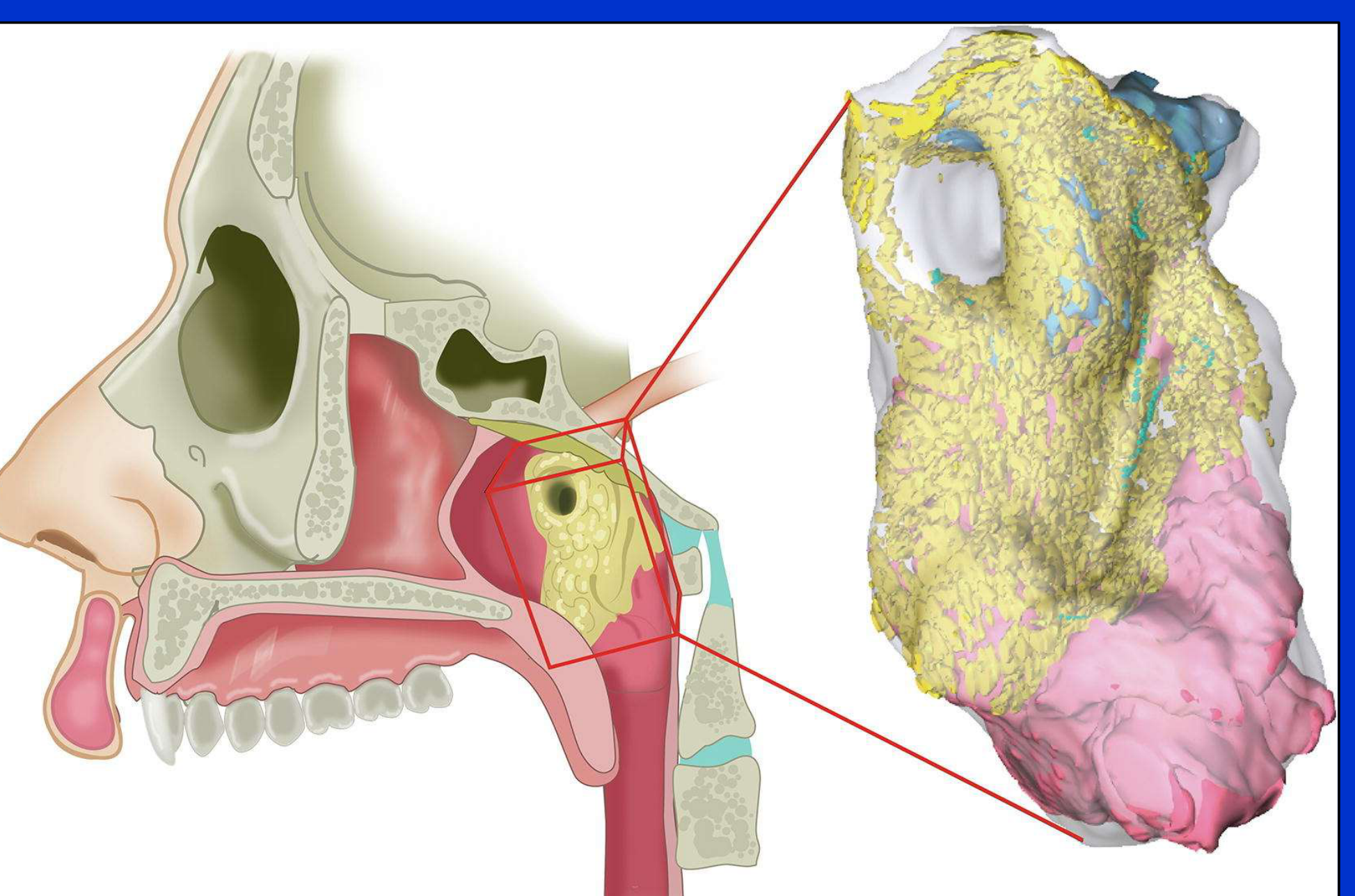
Tubarial Salivary Glands11
Recent anatomical research identifies the presence of tubarial salivary glands.
Clinical Significance
There is ongoing debate whether these are a "fourth major gland" or a conglomerate of minor glands, but they are critical for nasopharyngeal lubrication, especially in patients undergoing radiation therapy.
— Valstar MH et al, 2021
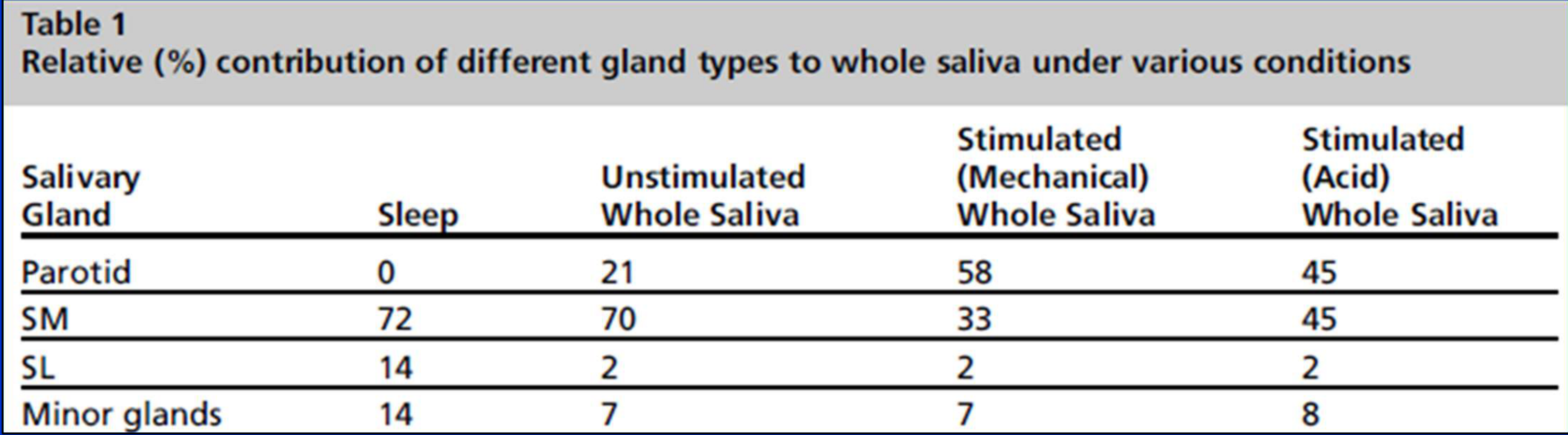
Percentage Contribution by Gland Type12
| Salivary Gland | Sleep (%) | Unstimulated Whole Saliva (%) | Stimulated (Mechanical) (%) | Stimulated (Acid) (%) |
|---|---|---|---|---|
| Parotid | 0 | 21 | 58 | 45 |
| Submandibular (SM) | 72 | 70 | 33 | 45 |
| Sublingual (SL) | 14 | 2 | 2 | 2 |
| Minor glands | 14 | 7 | 7 | 8 |
- The Parotid gland is primarily active during stimulation and does not produce mucins.
- The Submandibular and Sublingual glands are the main contributors at rest and night, producing essential mucins. — Jensen SB et al, 2014
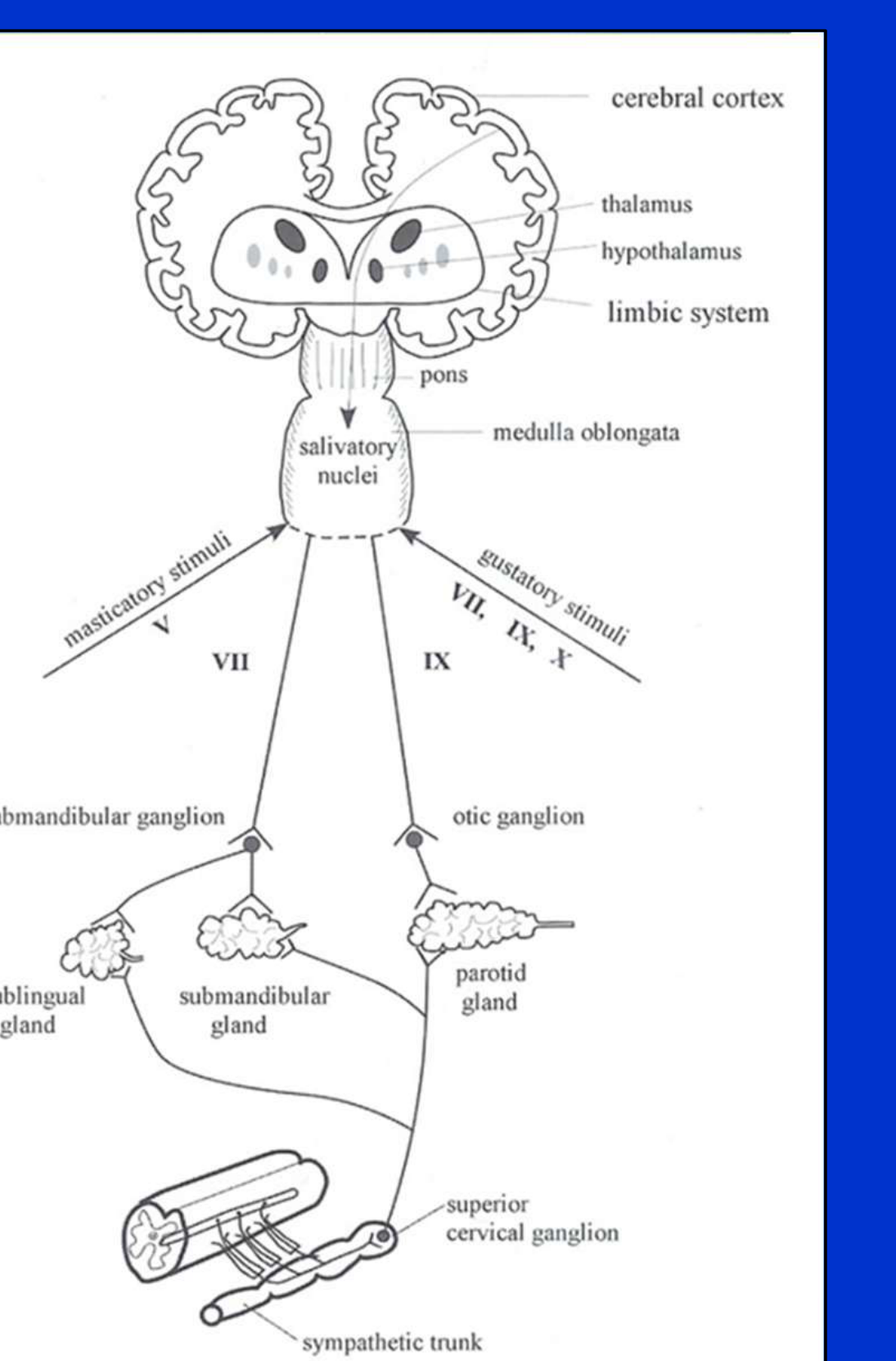
Neural Regulation of Secretion13
The secretion of saliva is regulated by reflexes involving the autonomic nervous system. This complex pathway involves:
- Central Control: Cerebral cortex, thalamus, hypothalamus, and limbic system.
- Brainstem Integration: Pons, medulla oblongata, and salivatory nuclei.
- Peripheral Pathways: Cranial nerves V, VII, IX, and X; submandibular and otic ganglia; superior cervical ganglion and sympathetic trunk.
Minor Salivary Gland Innervation14
- Primarily parasympathetic innervation.
- Characterized by little or no sympathetic innervation.
Minor Salivary Gland Innervation and Output15
- Primarily parasympathetic innervation.
- Little or no sympathetic innervation.
- Responsible for approximately 70% of MUC5B secretion.
- Because they are driven by parasympathetic signals, they are the primary source of the lubricating glycoprotein MUC5B.
Autonomic Effects on Secretion16
- Parasympathetic Stimulation: Generates abundant saliva with low protein concentration.
- Sympathetic Stimulation: Produces a small volume of saliva with high protein concentration and high viscosity
- Sympathetic stimulation produces very little mucin, leading to the characteristic "dry" feeling during stress.
Factors Influencing Salivary Flow Rates17
Salivary flow rates are dynamic and influenced by a wide variety of physiological and environmental factors.
Primary Influencing Factors1819
- Circannual rhythm
- Circadian rhythm
- Degree of hydration
- Emotional state
- Exposure to light
- Body position
- Mechanical stimuli
- Vomiting
- Gustatory and olfactory stimuli
- Gland size
In addition to flow rates, the chemical and organic composition of saliva will also vary based on these influencing factors.
 |  |
Clinical Significance of Salivary Assessment20
 |  |
 |
Challenges in Salivary Evaluation21
Assessing salivary function presents several clinical challenges regarding the interpretation of data:
- Value of Single-Point Assessments: There is limited diagnostic value in a single point-in-time assessment, as salivary flow can fluctuate.
- A patient might appear dry simply due to dental appointment anxiety or temporary dehydration.
- Need for Standardization: Salivary flow rate measurements require standardized protocols to ensure accuracy and reproducibility across different clinical settings.
Defining Normal Parameters22
A primary concern in clinical assessment is establishing a baseline for healthy function:
- Determining Normalcy: Defining what constitutes a “normal” salivary flow rate is complex due to individual biological variation.
- It is more important to identify a change from a patient's baseline than to rely on a universal average, as "normal" for one person may be "low" for another.
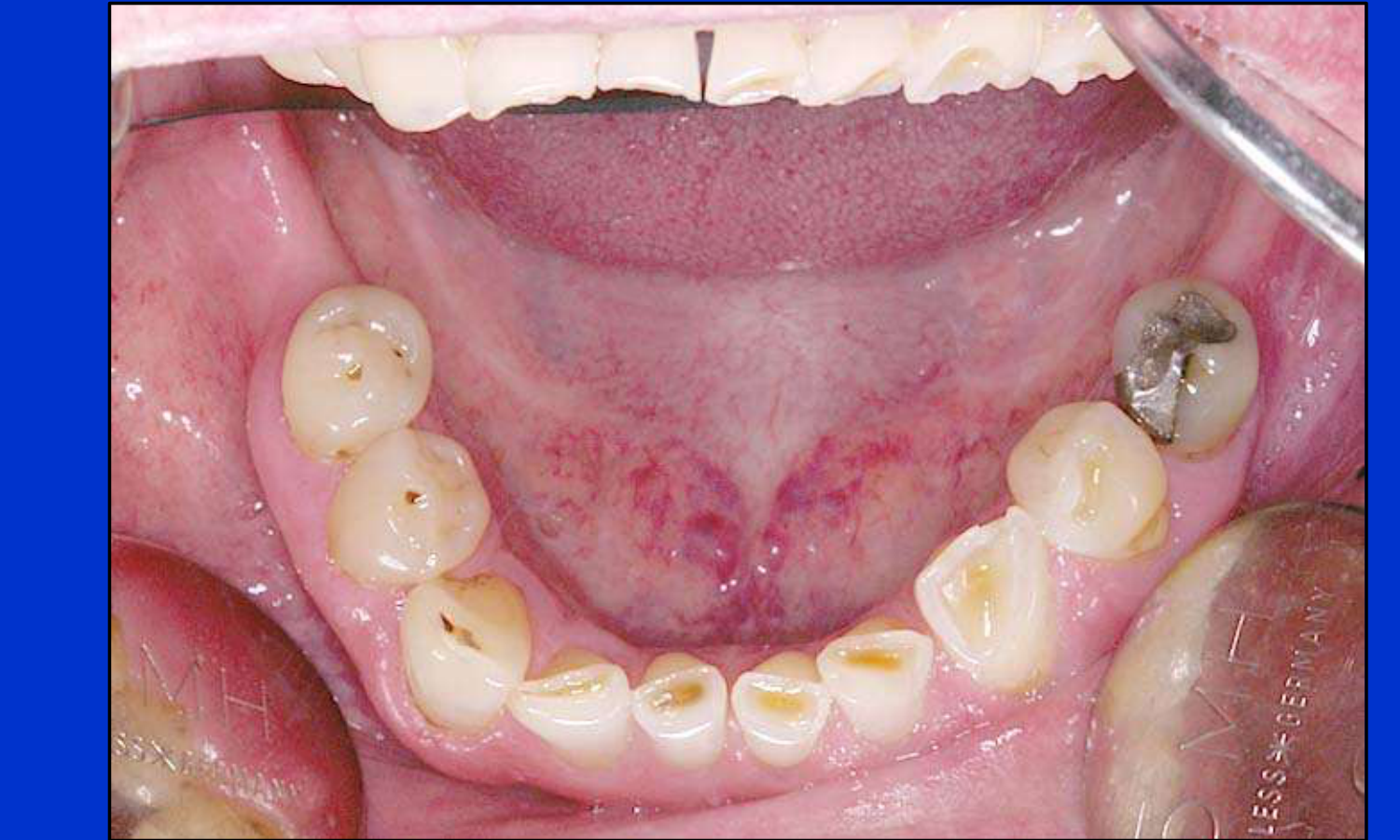
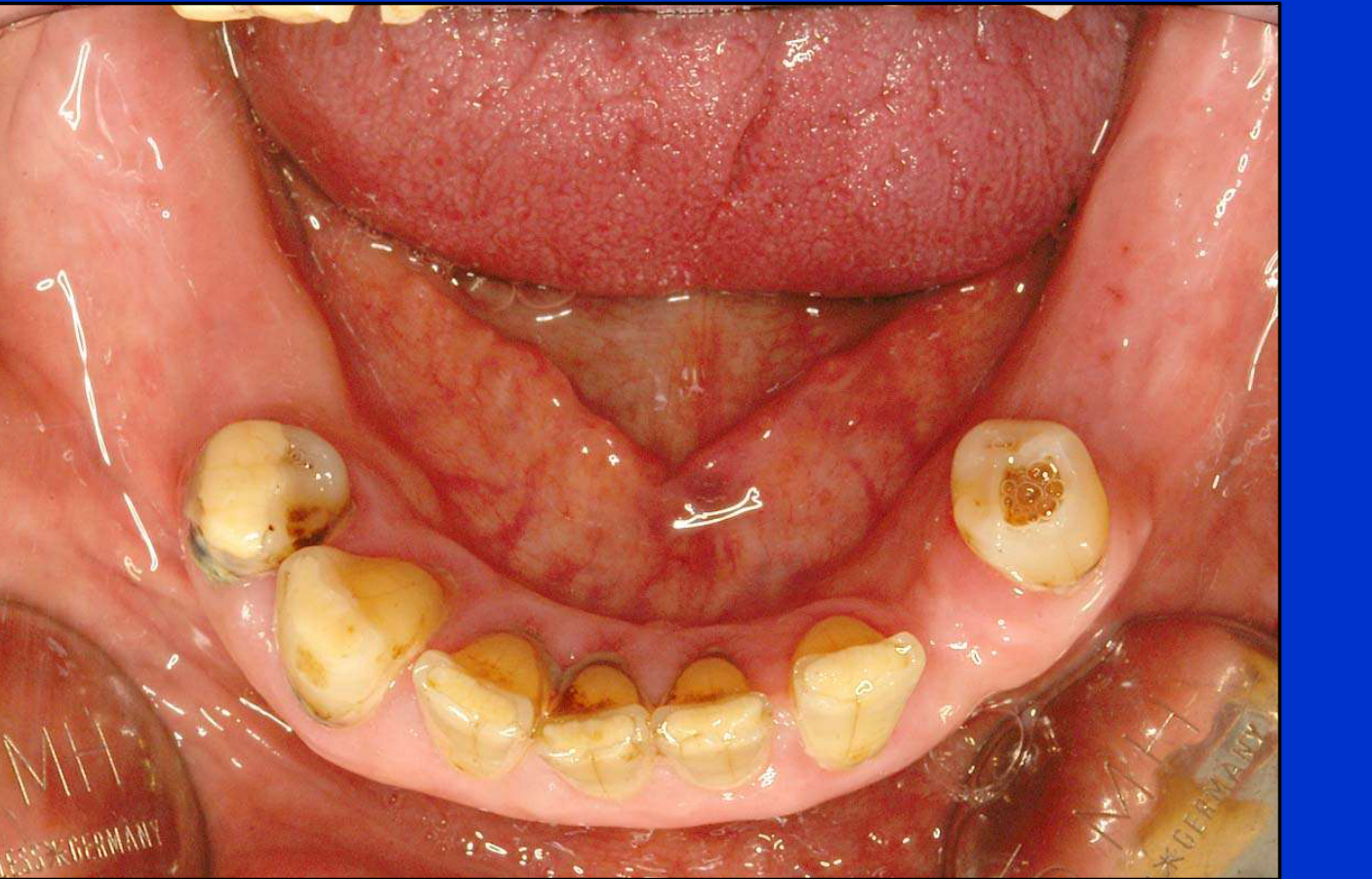
- Clinical Presentation: Observations of dental health, including the presence of restorations and the progression of decay, serve as indicators of the long-term impact of salivary flow on oral health.
 |  |
 |
Definitions and Prevalence23
Dry mouth is a complex condition that can be categorized into three distinct clinical observations:
- Xerostomia
- Salivary gland hypofunction
- Hyposalivation
Xerostomia vs Hypofunction
Subjective Experience24
- Xerostomia: The subjective experience or symptom of oral dryness as reported by the patient
Info
Xerostomia is like a headache; it is a subjective feeling that cannot be seen by the clinician, so the patient must report it. .
Objective Measures of Hypofunction25
Salivary gland hypofunction refers to diminished salivary flow and is based on objective measures of saliva production. Clinical thresholds include:
- Unstimulated whole saliva: 0.1–0.3 ml/min (Normal is >0.3 ml/min)
- Stimulated whole saliva: 0.7–1.0 ml/min (Normal is >1.0 ml/min)
Pathologically Low Flow26
Hyposalivation represents the low end of salivary gland hypofunction, characterized by pathologically low flow rates:
- Unstimulated whole saliva: ≤0.1 ml/min (Normal is >0.3 ml/min)
- Stimulated whole saliva: ≤0.5–0.7 ml/min (Normal is >1.0 ml/min)
Individual Variability27
- Salivary flow rates necessary for maintaining oral health are specific to the individual.
- A change in flow rate for a specific patient may be more clinically significant than the absolute volume.
- Some healthy individuals have naturally low flow without symptoms, while others feel dry despite having "normal" flow rates.
Clinical Relationship28
When evaluating the relationship between salivary gland hypofunction, hyposalivation, and xerostomia, it is important to note that the condition is not just a question of volume.
- The relationship is non-linear; symptoms usually only appear after a 50% drop from an individual's baseline flow.
Diagnostic Distinction29
Salivary gland hypofunction (SGH) and hyposalivation are not equivalent to xerostomia. One is an objective finding, while the other is a subjective symptom.
Prevalence and Patient Profiles
General Prevalence Rates30
- Prevalence of hyposalivation: 20%
- Prevalence of xerostomia: 23%
Statistical Overlap31
- Prevalence of hyposalivation: 20%
- Prevalence of xerostomia: 23%
- Combined hyposalivation and xerostomia: 2–6%
Patient Profile: Combined Presentation32
This patient profile includes individuals experiencing both objective hyposalivation and the subjective symptom of xerostomia.
- Example: Post-radiation therapy patients who both measure low and feel extremely dry.
Patient Profile: Objective Only33
This profile describes patients with objective hyposalivation who do not report the subjective feeling of xerostomia.
[!example] Case Study: Samantha
A 16-year-old girl born with salivary gland aplasia (missing major glands). She had pathologically low flow but did not complain of xerostomia because she had never known what a "wet" mouth felt like. Her primary issue was a high caries rate.

Patient Profile: Subjective Only34
This profile describes patients who report the subjective symptom of xerostomia but do not demonstrate objective hyposalivation.

Etiology of Hyposalivation and Xerostomia3536
An analysis of the underlying causes and etiologies associated with both hyposalivation (objective reduced flow) and xerostomia (subjective dryness).
The development of hyposalivation and xerostomia is typically attributed to several primary factors:
- Medications
- Systemic diseases
- Radiation therapy to the head and neck
- Other physiological or environmental factors
 |  |
 |
Medications and Polypharmacy
Pharmacological Influences37
Medication use is a leading cause of dry mouth. Specific drug classes associated with these symptoms include:
- Anticholinergics: These interfere with the parasympathetic signals required for saliva production.
- Sympathomimetics
- Other various drug classes
Polypharmacy Considerations
It is critical to note the impact of polypharmacy. The risk and severity of hyposalivation often increase significantly with the number of concurrent medications a patient is taking.
Polypharmacy in the Elderly
While a single drug might not cause dryness, the interaction of multiple drugs (common in the elderly) often results in a xerogenic effect.
Systemic Diseases and Conditions
Autoimmune and Chronic Inflammatory Diseases38
- Sjögren’s syndrome
- Systemic lupus erythematosus
- Rheumatoid arthritis
- Systemic sclerosis (scleroderma)
- Mixed connective tissue disease
- Primary biliary cirrhosis
- Sarcoidosis
- Graft versus host disease
- Inflammatory bowel disease
Endocrine and Metabolic Disorders
- Diabetes mellitus (Type I and II)
- Uncontrolled diabetes is a major cause.
- Diabetes insipidus
- Hypothyroidism
- End-stage renal disease
- Eating disorders
- Malnutrition
- Alcohol abuse
Neurological, Behavioural, and Psychiatric Disorders
- Cerebral palsy
- Parkinson’s disease
- Alzheimer’s disease
- Anxiety
- Depression
Genetic Conditions
- Salivary gland aplasia
- Ectodermal dysplasia
- Cystic fibrosis
Case Study: Samantha
Samantha presented with salivary gland aplasia, a rare genetic condition where the salivary glands fail to develop, leading to chronic hyposalivation.
Infectious Diseases
- HIV / AIDS
- Hepatitis C Virus (HCV)
- Epstein-Barr Virus (EBV) / Cytomegalovirus (CMV)
Other Systemic Conditions
- Gastroesophageal reflux disease (GERD)
- Hypertension
- Amyloidosis
Radiation Therapy and Aging
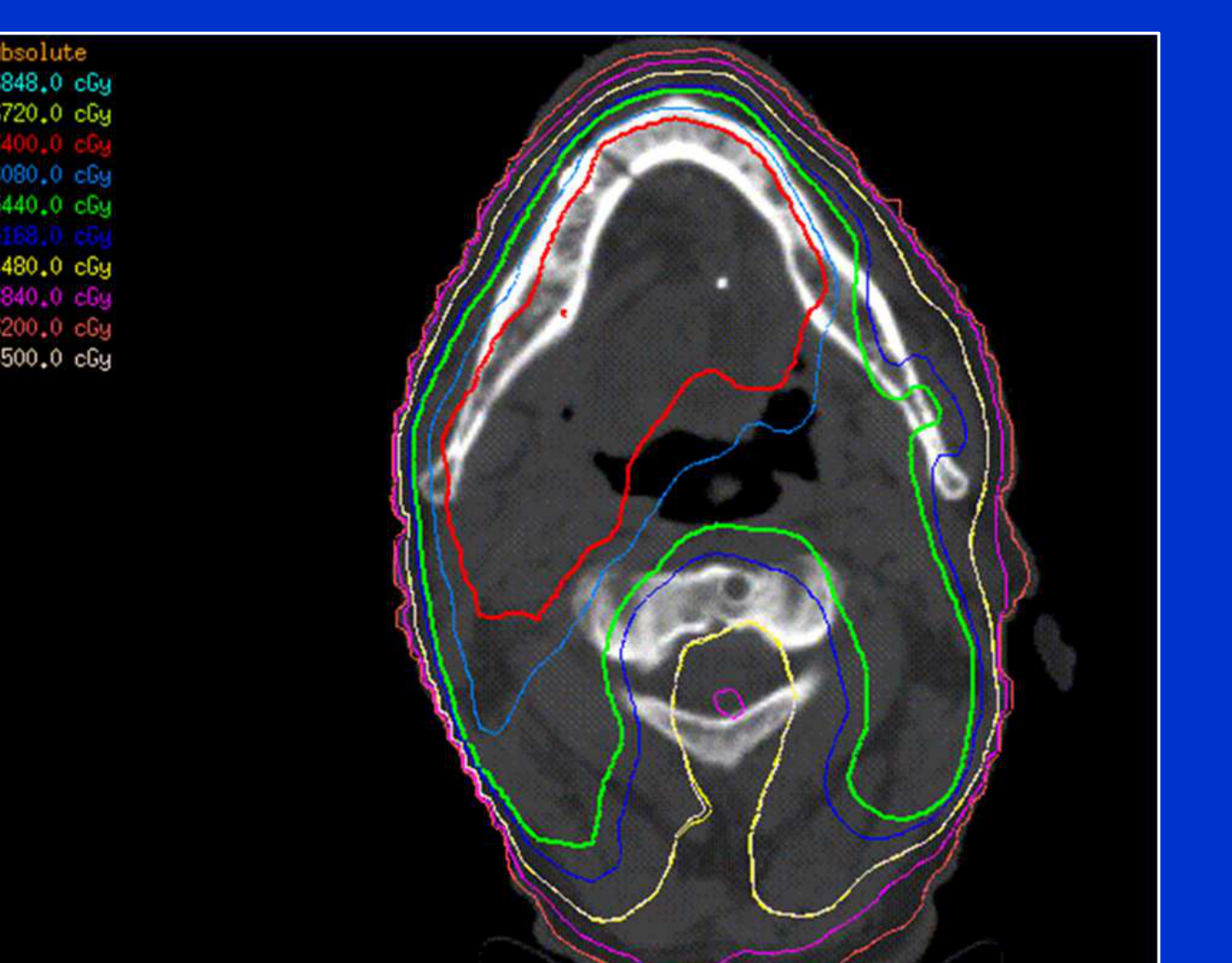
Radiation Exposure39
Direct damage to salivary gland tissue can occur through medical treatments involving radiation:
- Radiation therapy targeted to the head and neck region
- Radioactive iodine therapy
Menopause and Hormonal Changes40
Post-menopausal women frequently report symptoms of xerostomia. These complaints are often linked to:
- Changes in salivary flow rates
- Alterations in salivary composition
Hormone Replacement Therapy (HRT) may provide improvement for xerostomia in this population.
Age-Related Changes41
The aging process can lead to various alterations in salivary function, including:
- Structural changes within the salivary glands
- By age 75, acinar cells (secreting cells) decrease by 30–40%, replaced by fat.
- Salivary modifications:
- Reduced flow rates
- Changes in chemical composition
Aging and Xerostomia
Aging alone usually does not cause dry mouth unless it is compounded by systemic disease or medication.
Clinical Implications and Complications42
Hyposalivation and xerostomia lead to a variety of clinical challenges that affect daily function and comfort:
- Generalized oral discomfort
- Difficulty tolerating dentures
- Dysphonia (difficulty speaking)
- Dysphagia (difficulty swallowing)
- Dysgeusia (impaired sense of taste)
- Sleep disturbances
Oral and Systemic Effects
Impact on Oral Tissues and Breath43
The reduction in salivary flow contributes significantly to the following conditions:
- Halitosis: Chronic bad breath resulting from the lack of salivary cleansing action.
- Mucosal disease: Increased vulnerability of the oral soft tissues to inflammation and infection
- ==Mucositis and Ulceration: Lack of lubrication leads to tissue trauma==
- ==Candidosis: Fungal infections are very common in dry mouth patients due to the loss of antimicrobial salivary proteins==.
 |  |
Inflammatory and Gastric Complications44
- Sialadenitis: Inflammation of the salivary glands, often due to reduced flow and subsequent infection.
- GORD: Gastro-oesophageal reflux disease, which can be exacerbated by the lack of acid-neutralizing saliva
- ==Esophageal Injury: Without the buffering capacity of saliva, the risk of esophageal damage from stomach acid increases significantly==.
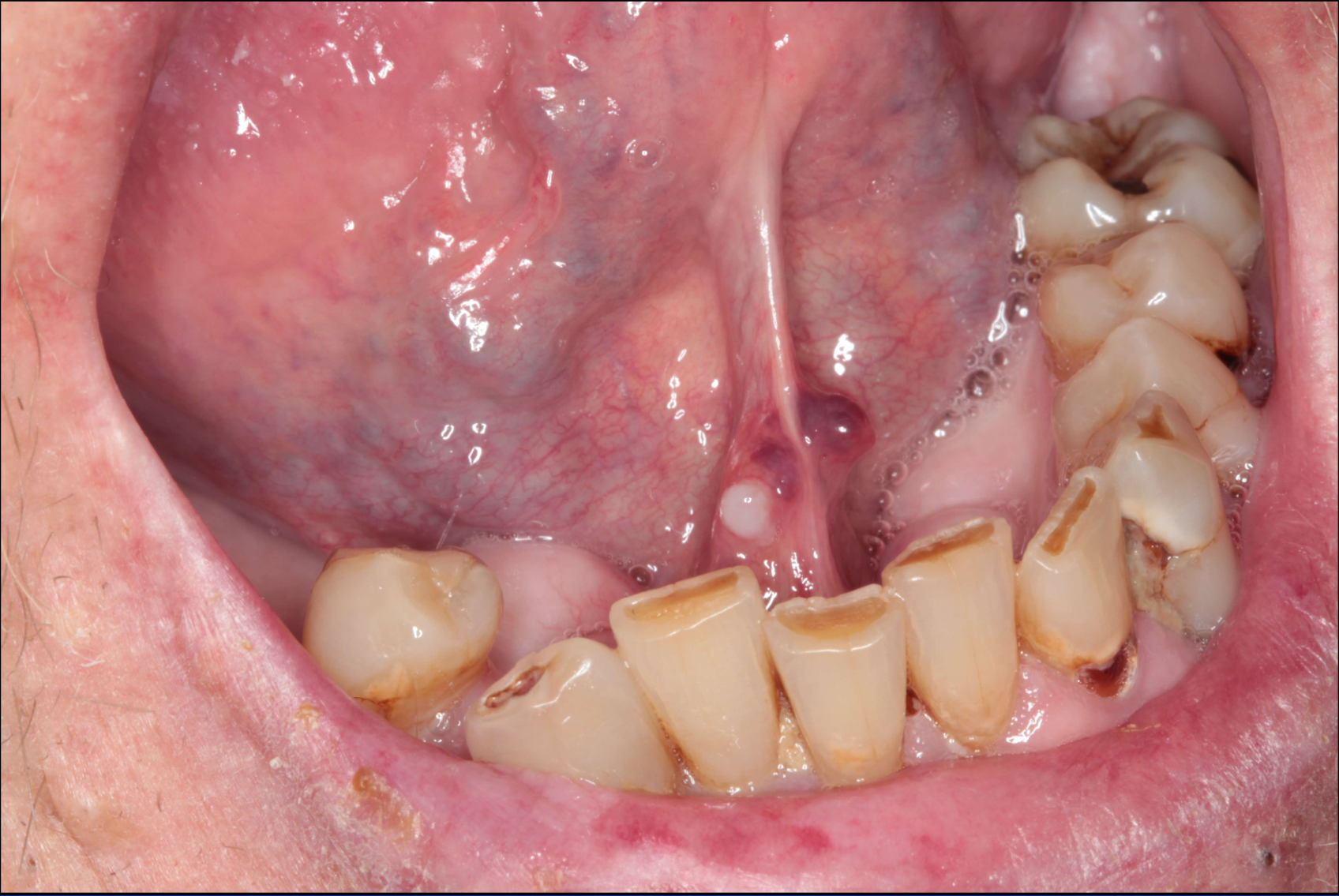
Dental and Periodontal Health45
Saliva plays a critical role in protecting the hard tissues of the mouth. Its absence leads to:
- Dental caries and non-carious tooth loss: Increased risk of decay and tooth wear (erosion/attrition) due to the loss of remineralization and buffering capacity
- ==Rampant Decay: Caries in hyposalivation patients often progresses rapidly and aggressively==.
- Periodontal disease: Greater susceptibility to gum disease and supporting tissue loss
- ==Complex Pathogen Link: While reduced clearance increases risk, lower pH and lack of calculus may sometimes be “protective” against specific periodontal pathogens==.
 |  |
Systemic and Psychosocial Impact46
The consequences of dry mouth extend beyond the oral cavity, affecting overall well-being and mental health:
- Impaired nutrition: Difficulty in chewing and swallowing can lead to poor dietary intake
- ==Dietary Shifts: Patients often compensate by shifting to soft, carbohydrate-rich foods, which can further exacerbate dental decay==.
- Depression and withdrawal: Social anxiety and psychological distress resulting from oral discomfort and communication difficulties.
- Decreased life quality: A cumulative reduction in the patient’s overall standard of living and daily satisfaction.
Diagnosis and Clinical Assessment47
The diagnostic process for dry mouth involves a comprehensive review of the patient’s status through several key stages:
- Medical history
- Dental history
- Clinical examination
Clinical Examination and Investigations
Visual Assessment of Oral Tissues48
Clinical examination includes a close-up inspection of the oral cavity, focusing on the uvula, surrounding soft tissues, and the condition of existing dental restorations.

Physical Examination Techniques49
Standard clinical examination procedures utilize:
- Dental mirrors to reflect and inspect the inner cheek and buccal mucosa.
- Dental probes to examine the gum line and the integrity of the teeth and surrounding tissues.
- Standardized flow rate measurements (draining method for unstimulated; paraffin wax chewing for stimulated).
 |  |
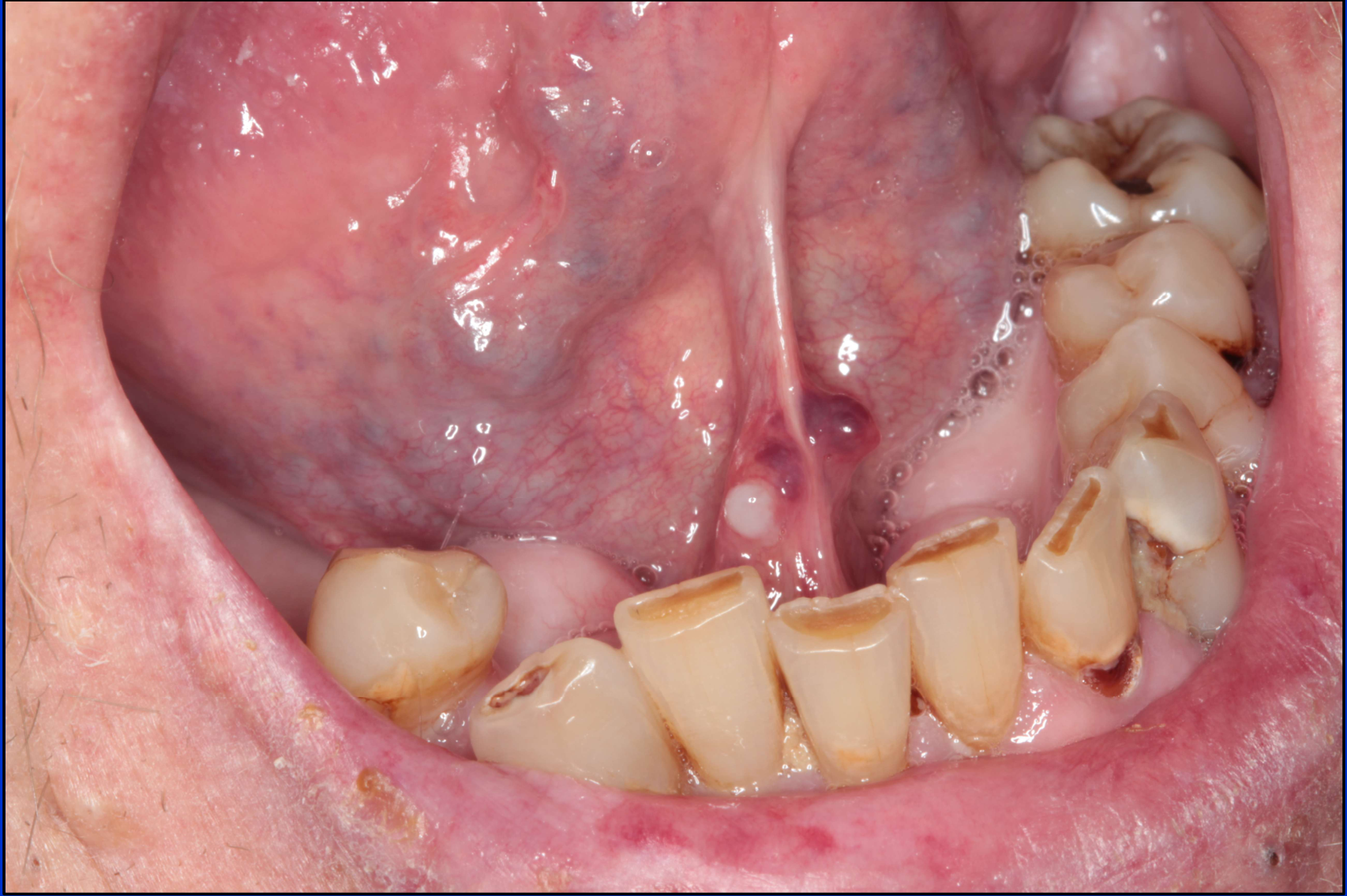
Mucosal Observations50
Examination focuses on identifying clinical signs of dryness or inflammation, such as:
- Red, inflamed tissue near the gum line.
- The appearance and hydration of the tongue and lower oral mucosa.
- Presence of candidosis or atypical caries patterns.
 |  |
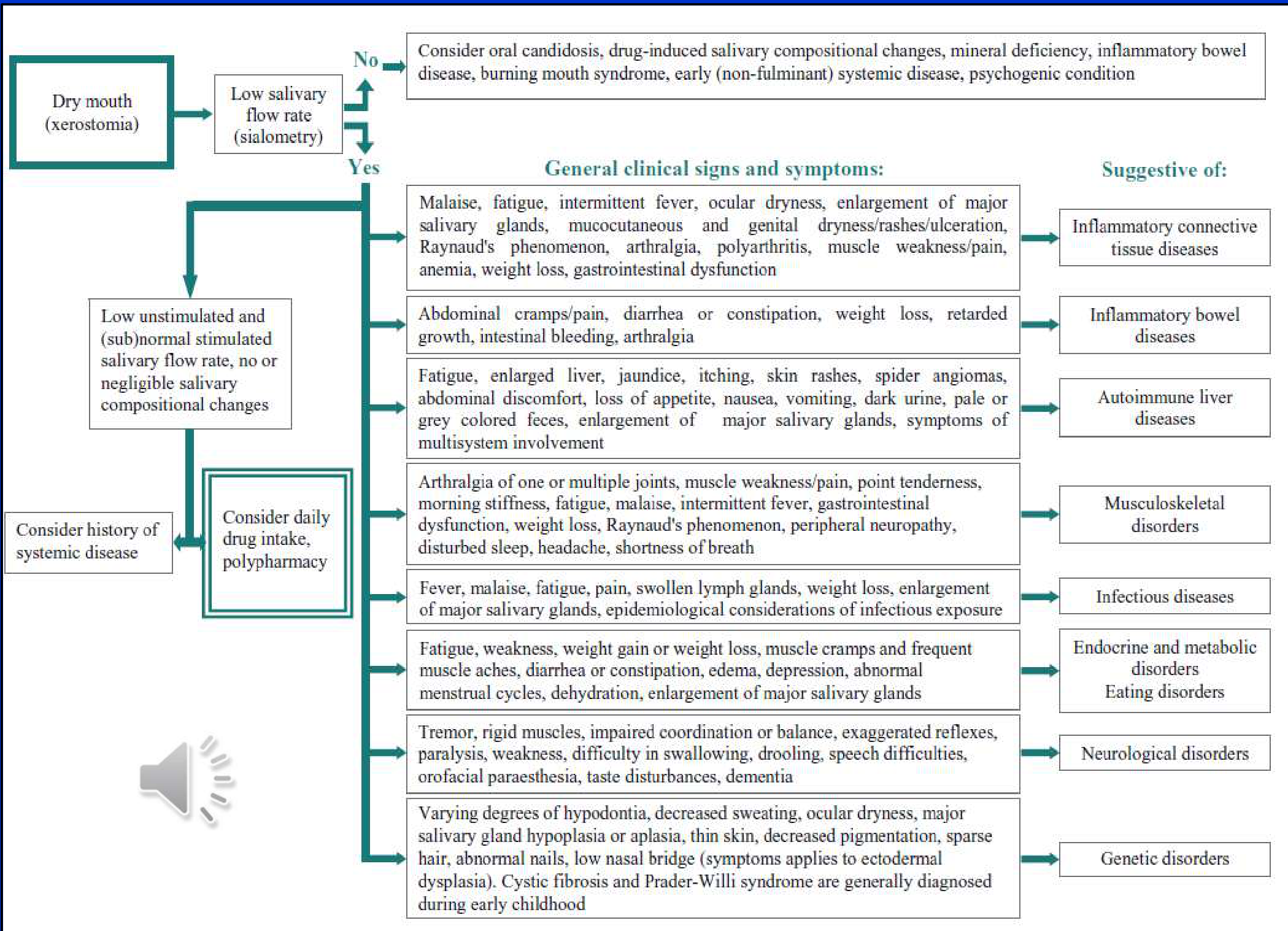
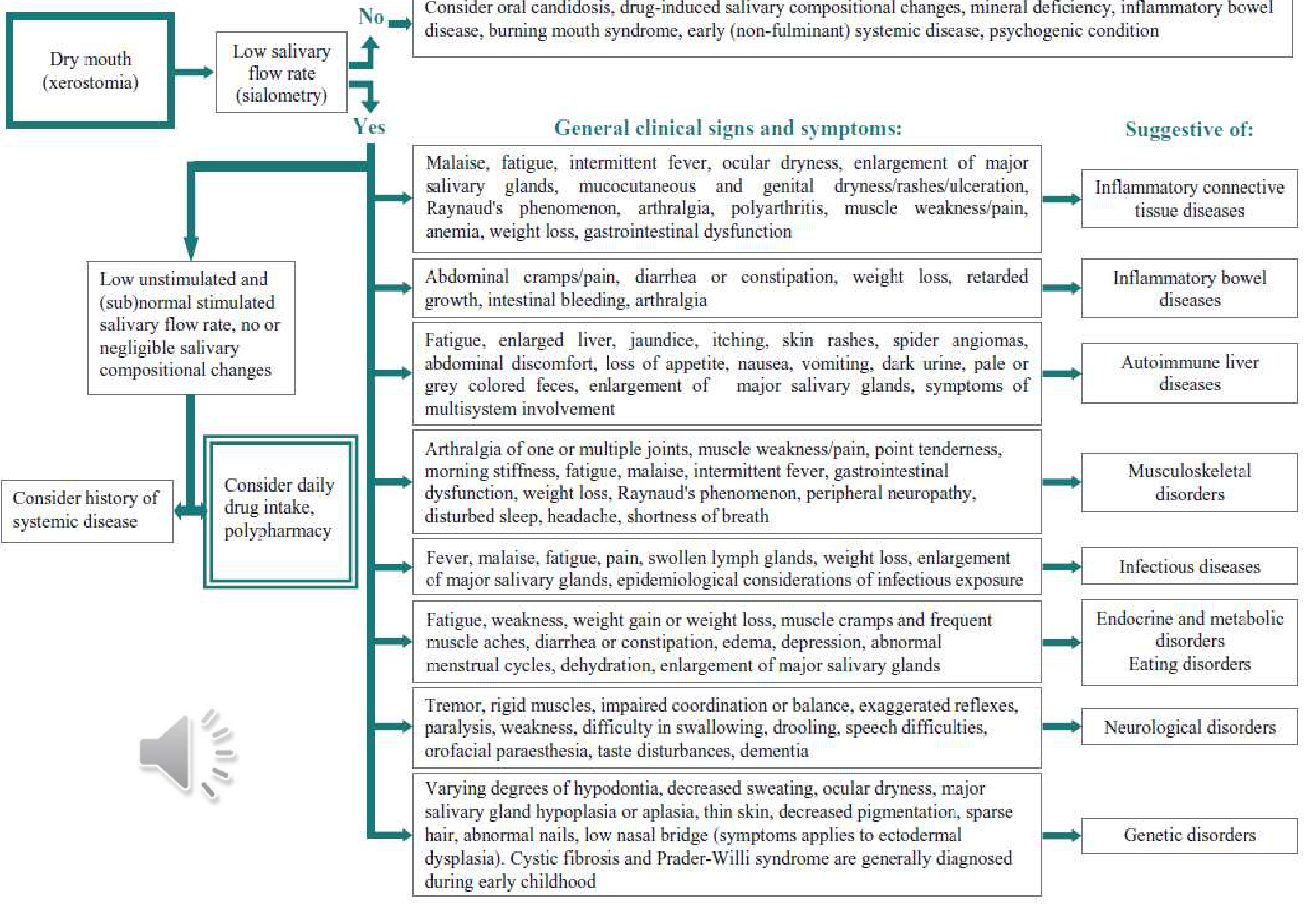
Diagnostic Flowchart for Dry Mouth (Xerostomia)51
Diagnosis When evaluating a patient for dry mouth, clinicians must determine if there is a low salivary flow rate (sialometry) and consider various underlying causes.
Scenario A: No Low Salivary Flow Rate If xerostomia is present but flow rates are normal, consider:
- Oral candidosis
- Drug-induced salivary compositional changes
- Mineral deficiency
- Inflammatory bowel disease
- Burning mouth syndrome
- Early (non-fulminant) systemic disease
- Psychogenic conditions
Scenario B: Low Unstimulated and (Sub)normal Stimulated Flow Rate If flow rates are low with negligible compositional changes, consider:
- History of systemic disease
- Daily drug intake or polypharmacy
 |  |
 |
Systemic Disease Indicators
| General Clinical Signs and Symptoms | Suggestive Systemic Condition |
|---|---|
| Malaise, fatigue, intermittent fever, ocular dryness, major salivary gland enlargement, mucocutaneous/genital dryness, Raynaud’s phenomenon, arthralgia, anemia | Inflammatory connective tissue diseases |
| Abdominal cramps, diarrhea/constipation, weight loss, retarded growth, intestinal bleeding, arthralgia | Inflammatory bowel diseases |
| Fatigue, enlarged liver, jaundice, itching, skin rashes, spider angiomas, nausea, dark urine, pale feces, multisystem involvement | Autoimmune liver diseases |
| Joint arthralgia, muscle weakness/pain, morning stiffness, peripheral neuropathy, disturbed sleep, shortness of breath | Musculoskeletal disorders |
| Fever, malaise, fatigue, swollen lymph glands, weight loss, salivary gland enlargement, infectious exposure history | Infectious diseases |
| Fatigue, weight fluctuations, muscle cramps, edema, depression, abnormal menstrual cycles, dehydration | Endocrine, metabolic, or eating disorders |
| Tremor, rigid muscles, impaired coordination, paralysis, swallowing difficulty, drooling, orofacial paraesthesia, taste disturbances | Neurological disorders |
| Hypodontia, decreased sweating, salivary gland hypoplasia, thin skin, sparse hair, abnormal nails (e.g., ectodermal dysplasia) | Genetic disorders |
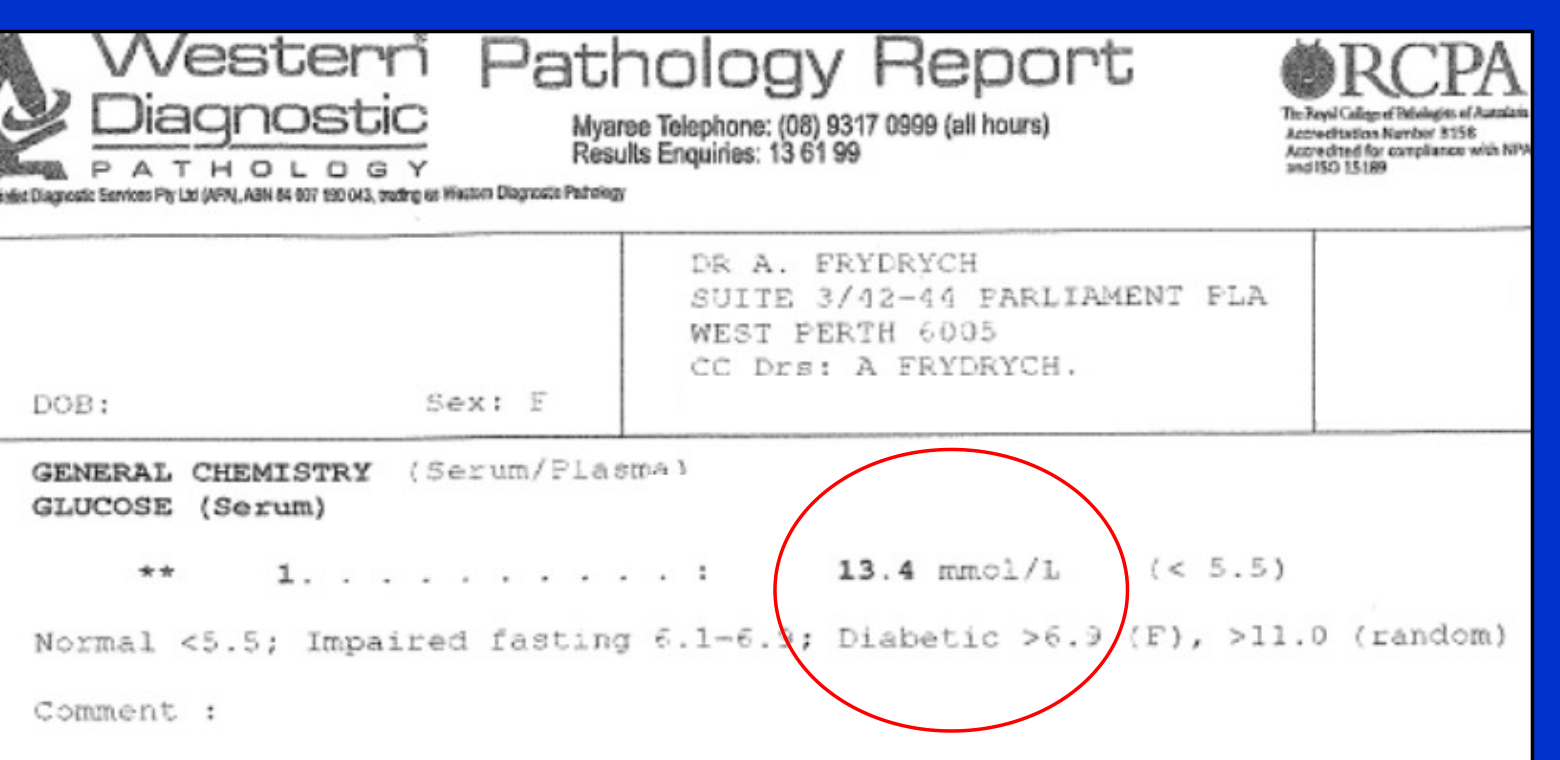
Case Study: Undiagnosed Diabetic
An overweight patient with a family history of diabetes presented with dry mouth, burning sensation, and poor healing. Investigations revealed she was an undiagnosed diabetic; treating the diabetes resolved her oral symptoms.
Laboratory Investigations52
Clinical findings such as tongue redness and swelling may necessitate pathology testing.
Case Example: General Chemistry (Serum/Plasma)
- Glucose (Serum): 13.4 mmol/L (Reference: < 5.5)
- Interpretation:
- Normal: < 5.5
- Impaired fasting: 6.1–6.9
- Diabetic: > 6.9 (Fasting), > 11.0 (Random)
 |  |
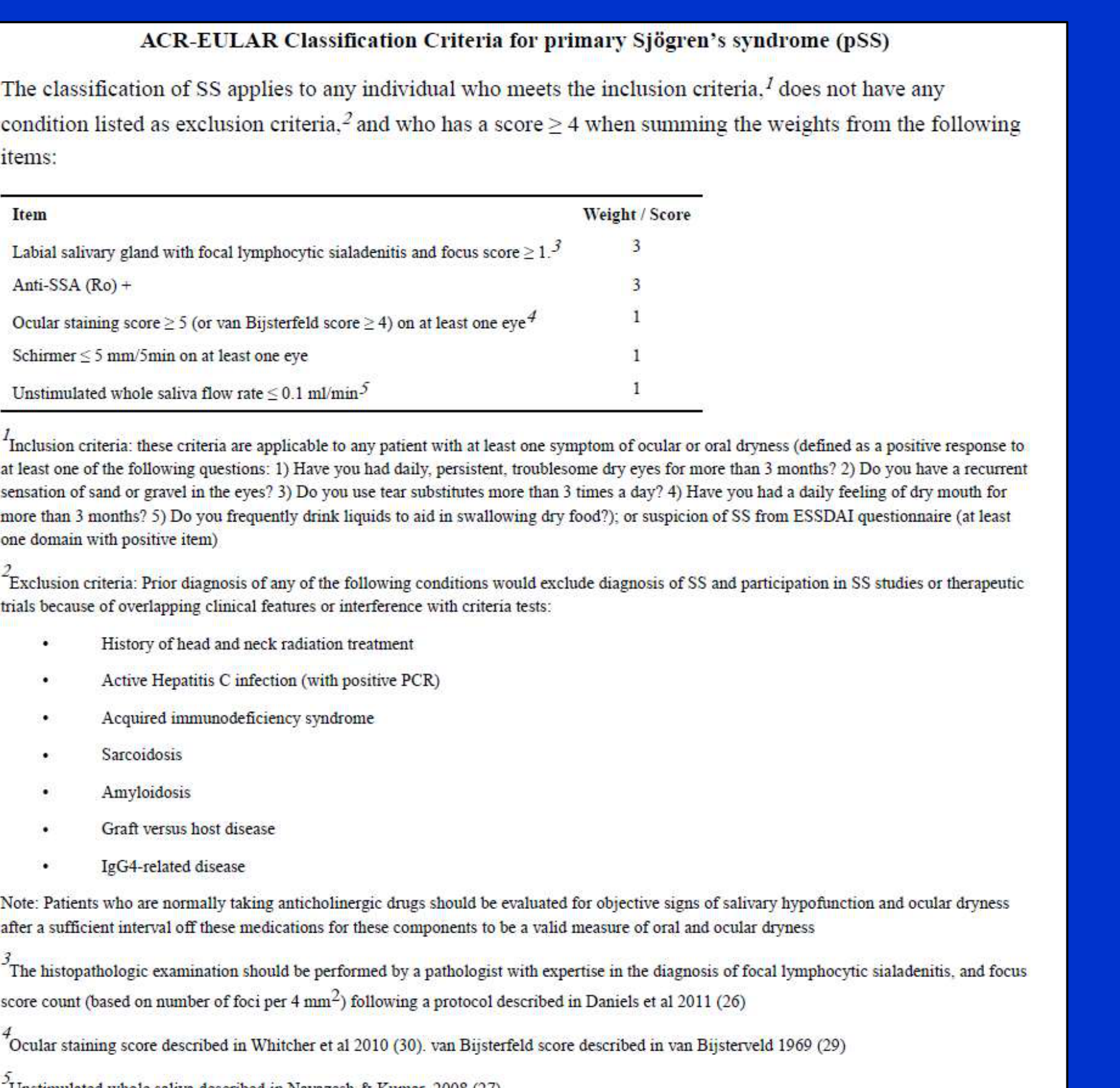
Sjogren’s Syndrome Classification Criteria53
The ACR-EULAR classification applies to individuals meeting inclusion criteria (symptoms of ocular or oral dryness for >3 months or positive ESSDAI questionnaire) and lacking exclusion criteria (e.g., radiation history, Hepatitis C, AIDS, Sarcoidosis, Amyloidosis, GVHD, IgG4-related disease).
A score of ≥ 4 is required for classification:
| Item | Weight / Score |
|---|---|
| Labial salivary gland with focal lymphocytic sialadenitis and focus score ≥ 1 | 3 |
| Anti-SSA (Ro) positive | 3 |
| Ocular staining score ≥ 5 (or van Bijsterfeld score ≥ 4) on at least one eye | 1 |
| Schirmer test ≤ 5 mm/5min on at least one eye | 1 |
| Unstimulated whole saliva flow rate ≤ 0.1 ml/min | 1 |
Clinical Notes:
- Patients on anticholinergic drugs should be evaluated after a sufficient interval off medication.
- Histopathologic examination requires expertise in focal lymphocytic sialadenitis focus scoring (per 4 mm²).
Subjective and Objective Measurement Tools
Distinguishing Subjective and Objective Symptoms54
Assessment must differentiate between:
- Xerostomia: The subjective sensation of dry mouth.
- Salivary gland hypofunction / hyposalivation: The objective reduction in salivary secretion.

Subjective Screening55
A primary screening question for xerostomia is:
- “Does your mouth usually feel dry?”
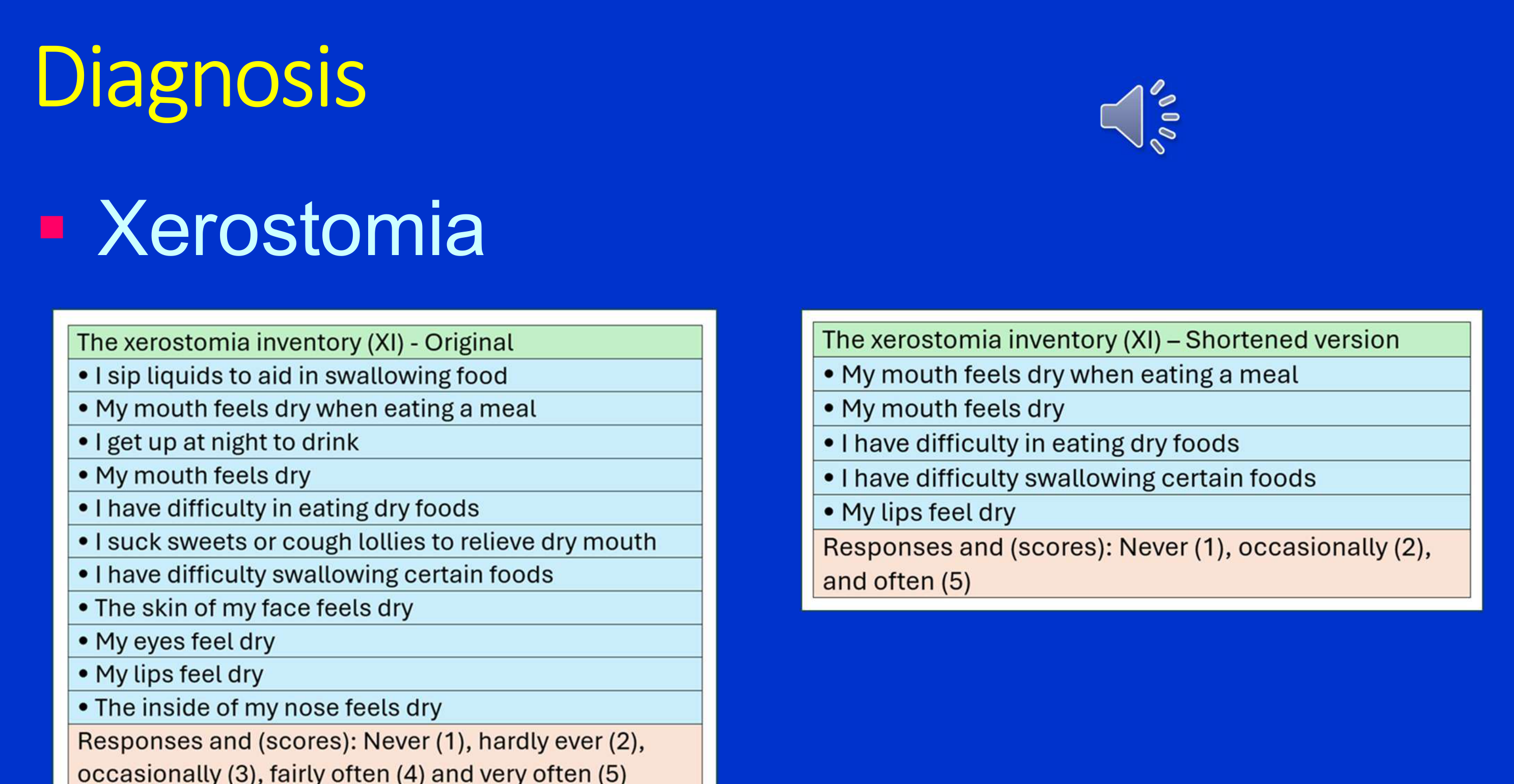
The Xerostomia Inventory (XI)56
Original Version (11 items)
- I sip liquids to aid in swallowing food
- My mouth feels dry when eating a meal
- I get up at night to drink
- My mouth feels dry
- I have difficulty in eating dry foods
- I suck sweets or cough lollies to relieve dry mouth
- I have difficulty swallowing certain foods
- The skin of my face feels dry
- My eyes feel dry
- My lips feel dry
- The inside of my nose feels dry
Scoring: Never (1), hardly ever (2), occasionally (3), fairly often (4), and very often (5).
Shortened Version (5 items)
- My mouth feels dry when eating a meal
- My mouth feels dry
- I have difficulty in eating dry foods
- I have difficulty swallowing certain foods
- My lips feel dry
Scoring: Never (1), occasionally (2), and often (5).
Objective Assessment57
Evaluation of salivary gland hypofunction and hyposalivation involves clinical measurements of saliva production.
- Flow rates should be measured for 5 minutes after the patient has avoided food/smoking for one hour.
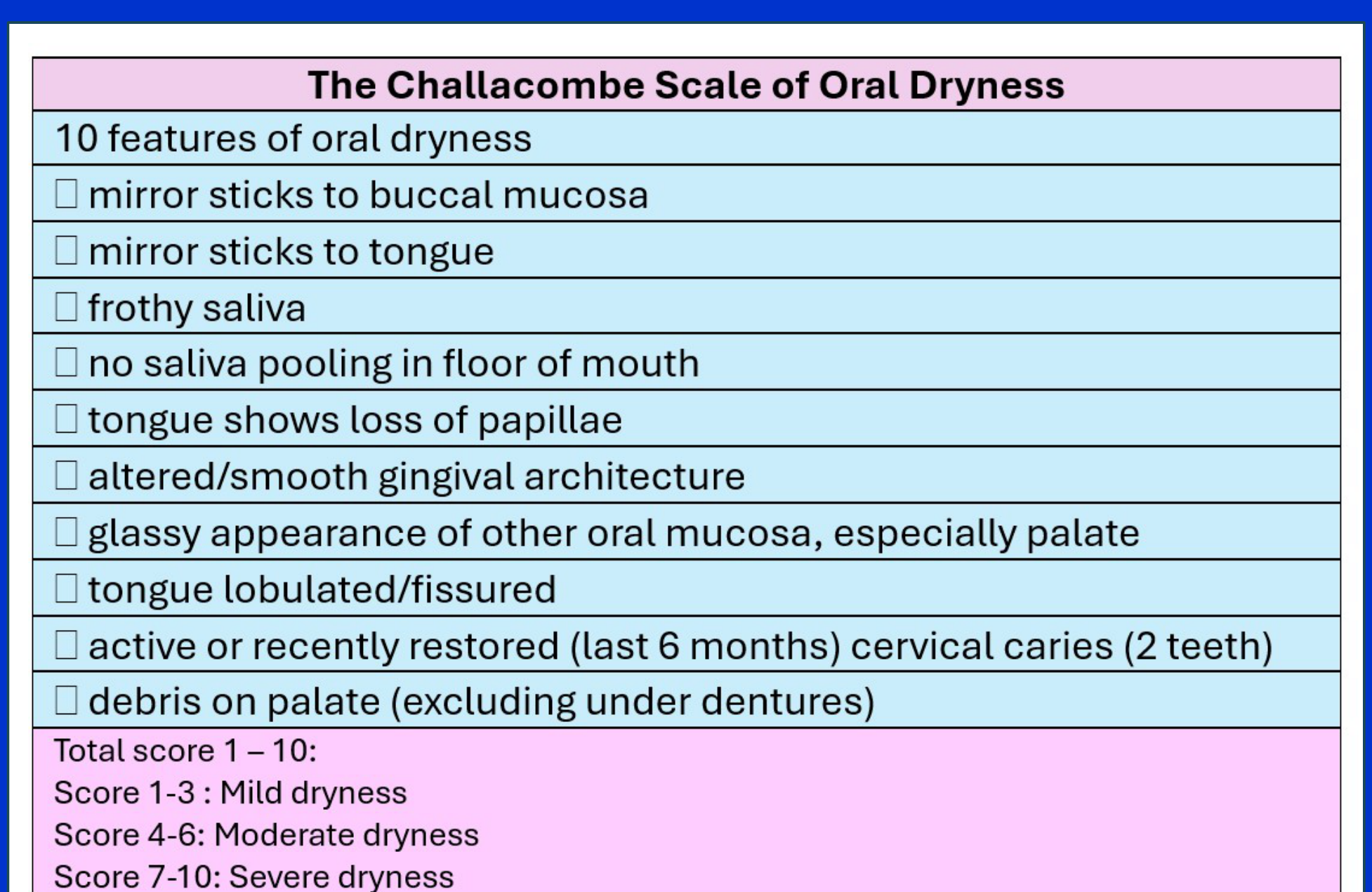
The Challacombe Scale of Oral Dryness58
This scale uses 10 clinical features to assess the severity of hyposalivation:
- Mirror sticks to buccal mucosa
- Mirror sticks to tongue
- Frothy saliva
- No saliva pooling in floor of mouth
- Tongue shows loss of papillae
- Altered/smooth gingival architecture
- Glassy appearance of other oral mucosa (especially palate)
- Tongue lobulated/fissured
- Active or recently restored (last 6 months) cervical caries (2 teeth)
- Debris on palate (excluding under dentures)
Severity Scoring:
- 1–3: Mild dryness
- 4–6: Moderate dryness
- 7–10: Severe dryness
Management Strategies59
The management of dry mouth addresses three clinical presentations:
- Xerostomia
- Hyposalivation
- Combined Xerostomia and hyposalivation
 |  |
 |
Core Management Pillars60
- Understand the nature of the problem
- Address the underlying cause or contributing factors
- Utilize symptomatic treatments and commercial saliva substitutes
- Implement stimulation of salivary glands (gustatory, pharmaceutical, or mechanical)
- Explore other therapeutic modalities
- Manage associated clinical complications
Symptomatic Treatments and Substitutes
Hydration61
- Water
- Crucial for preventing systemic dehydration.
- Note: Frequent consumption may paradoxically increase dry mouth symptoms in some contexts.
- Excessive water sipping can actually wash away the remaining protective mucus coating.

Natural Oils62
- Oil Application
- Example: Olive oil can be used as a topical lubricant.
- Olive oil is a cheap, effective lubricant with mild anti-inflammatory properties.
- Example: Olive oil can be used as a topical lubricant.
Composition of Commercial Salivary Substitutes63
| Agent Category | Examples and Components |
|---|---|
| Saliva Stimulant | Citric acid, malic acid, tartaric acid and their salts |
| Buffering Agent | Potassium hydroxide; Phosphate buffers (e.g., disodium phosphate) |
| Thickening Agent | Hydrocolloids (xanthan, guar gum); Glycerine; Water-soluble polymers (HA, PAA, CMC); Sugar alcohols (xylitol, erythritol, sorbitol) |
| Moisturizing Agent | Glycerine; Water-soluble polymers (guar gum, HA, PAA, CMC); Sugar alcohols |
| Adhesive Agent | Natural polysaccharides (guar gum, HA); Semisynthetic polymers (CMC); Synthetic polymers (PAA); Thiolated polymers |
| Lubricating Agent | Mucin; Glycerine; Polyethylene glycol (PEG); Cellulose-based polymers; Carrageenan, xanthan gum |
| Biological Effect | Xylitol (caries reduction); Fluoride (anti-cariogenic); Lactoferrin (anti-inflammatory) |
| Optional Agents | Sweeteners (sorbitol); Cooling agents (l-menthol); Surfactants; Colorants; Preservatives |
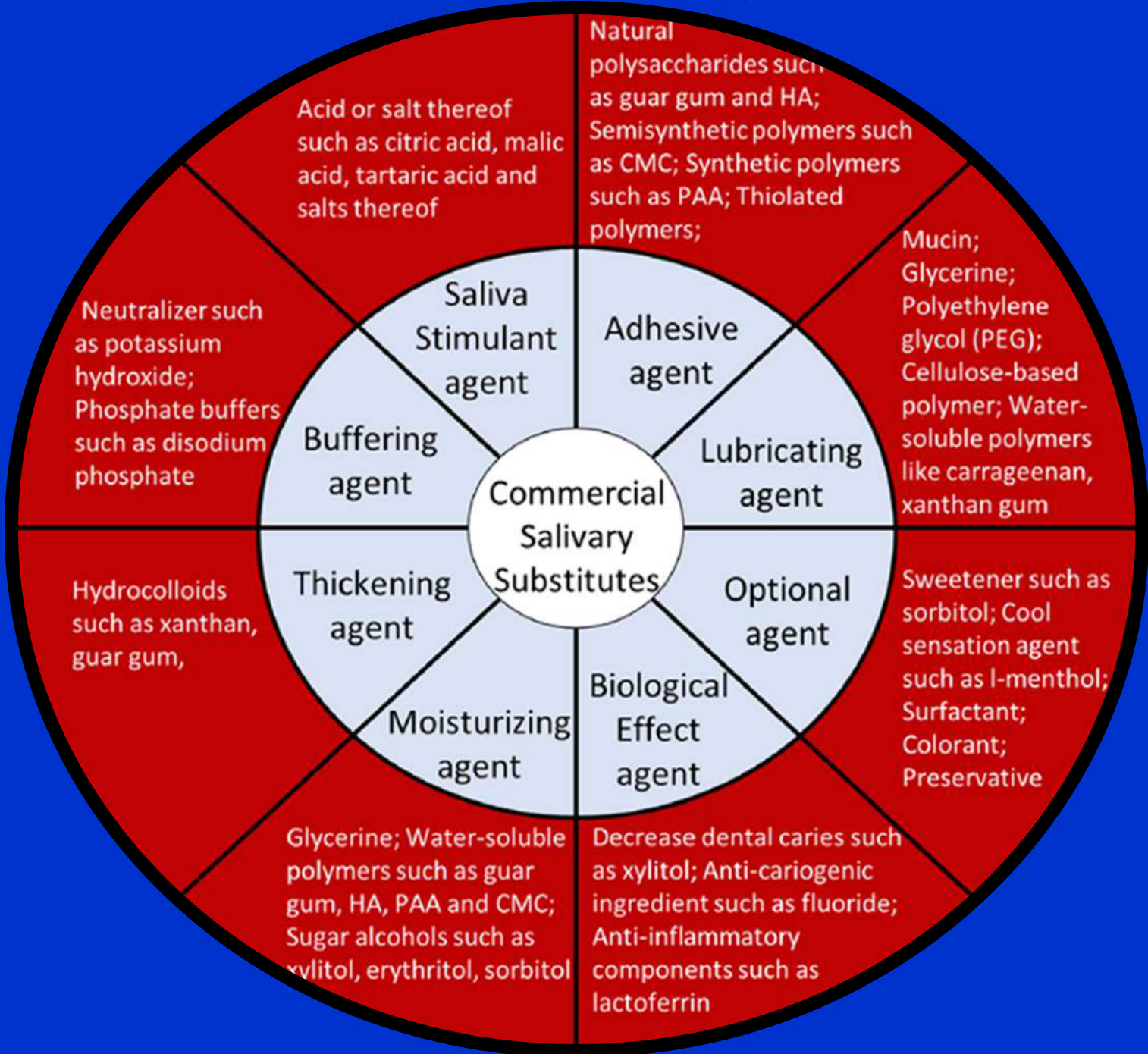
Functional Components of Substitutes64
-
Stimulants and Buffers: Acids (citric/malic) to prompt flow and neutralizers (potassium hydroxide/phosphates) to maintain pH.
-
Textural Agents: Hydrocolloids like xanthan and guar gum provide necessary thickness.
-
Protective Agents:
- Biological ingredients such as fluoride for anti-caries and lactoferrin for inflammation.
- Adhesives like CMC and PAA to ensure tissue coating.
-
Sensory/Stability Agents: Menthol for cooling sensations and various preservatives/colorants for product stability.
-
Thickening Agents
- Used to increase product viscosity.
- Example: Hydroxyethyl cellulose.
-
Lubricating Agents
- Designed to protect mucosal surfaces.
- Examples: Animal-derived mucin, glycerine, and polyethylene glycol.
- Mucin-based products are considered the most effective for lubrication.
-
Adhesive Agents
- Facilitate the formation of a protective coating to shield oral tissues from irritation.
- Types: Natural, semi-synthetic, and synthetic polymers.
-
Moisturising Agents
- Example: Carboxymethyl cellulose (CMC).
Supplemental Additives65
- Antimicrobial Proteins: Lysozyme, lactoferrin, and lactoperoxidase.
- Buffering Agents: To stabilize oral pH.
- Anti-cariogenic Agents: To prevent tooth decay.
- Salivary Stimulants: Integrated agents to encourage natural flow.
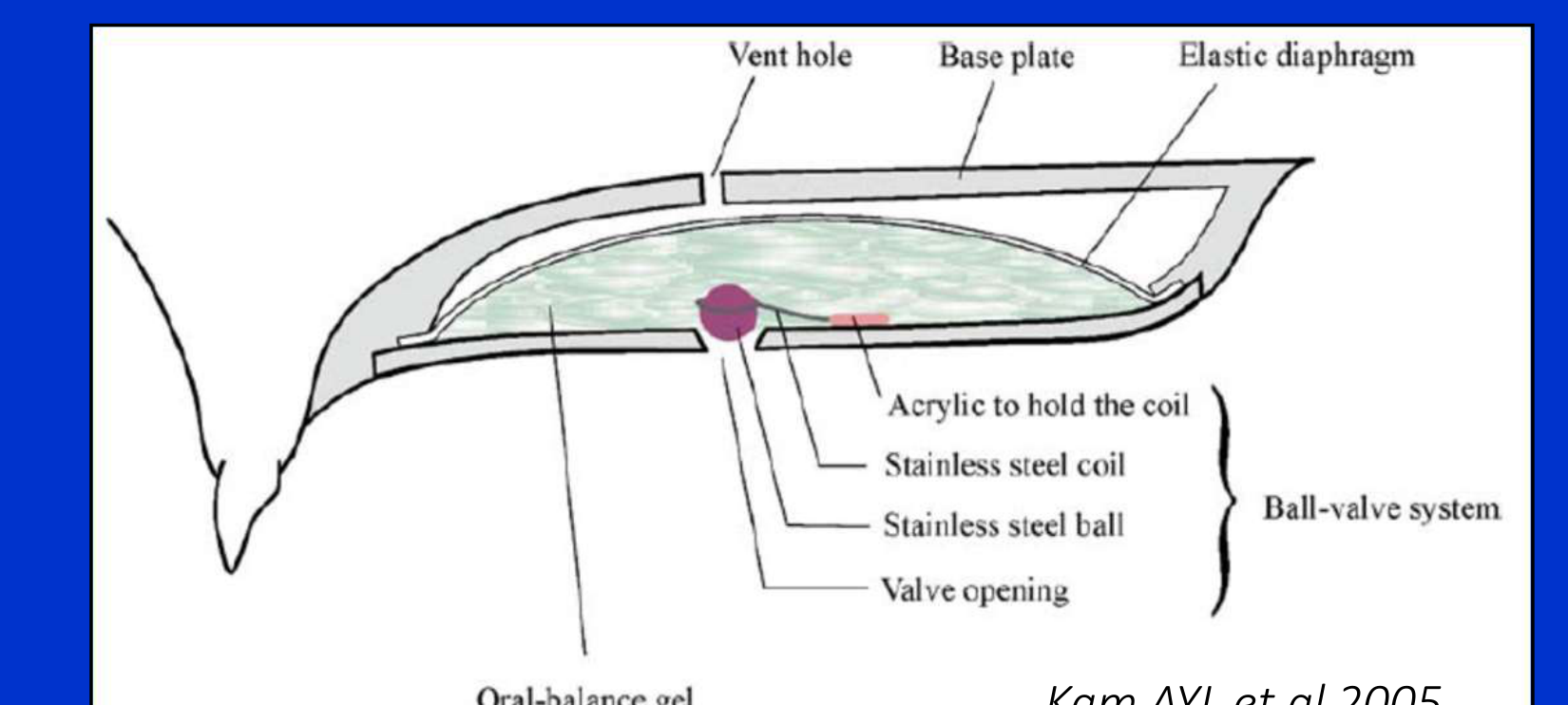
Mechanical Delivery Systems66
Research has explored specialized devices for delivering salivary substitutes, such as intraoral reservoirs featuring:
- Ball-valve systems (stainless steel ball and coil)
- Elastic diaphragms and vent holes
- Integration with oral-balance gels
- These devices can be bulky and increase the risk of oral candidosis.
 |  |
Limitations of Substitutes67
- Limited duration of action (requires frequent reapplication)
- Performance dependency on specific environmental conditions
- Financial cost to the patient
- Substitutes lack the complex macromolecular structure of real saliva.
Clinical Summary68
- There is currently limited evidence that salivary substitutes provide significant objective benefit.
- Despite limited evidence, they should still be offered as a management option for patient comfort.
- Substitutes are particularly recommended for cancer patients.
Salivary Stimulation and Secretogogues
Info
Stimulation is only effective if there is residual functioning gland tissue.
Mechanical Stimulation69
- Chewing Sugar-Free Gum
- Can effectively increase the unstimulated salivary flow rate.
- Provides symptomatic relief from xerostomia.
Gustatory Stimulation70
- Sugar-Free Confections
- Literature regarding efficacy is limited.
- Different sugar substitutes (sorbitol vs. mannitol) have varying properties.
- Caution: Many products contain added acids for flavor, which increases the risk of dental erosion
- Avoid acidic flavors like lemon; xylitol-based lollies are preferred.
Pharmacological Secretogogues71
- Pilocarpine: A cholinergic parasympathomimetic agent that acts as a non-selective muscarinic agonist
- Side effects include sweating, tearing, and urinary frequency.
- Contraindicated in patients with asthma or COPD.
- Cevimeline: An alternative muscarinic agonist
- More selective for M3 receptors with fewer side effects, but availability varies by region (e.g., unavailable in Australia).
- Other emerging pharmaceutical agents.
Neuro-electrostimulation and Other Approaches
Electrical Stimulation Modalities72
- TENS: Transcutaneous Electric Nerve Stimulation
- Uses external electrodes placed on the skin.
- Intraoral Electrostimulators:
- Removable devices.
- Fixed (Implant-supported) devices.
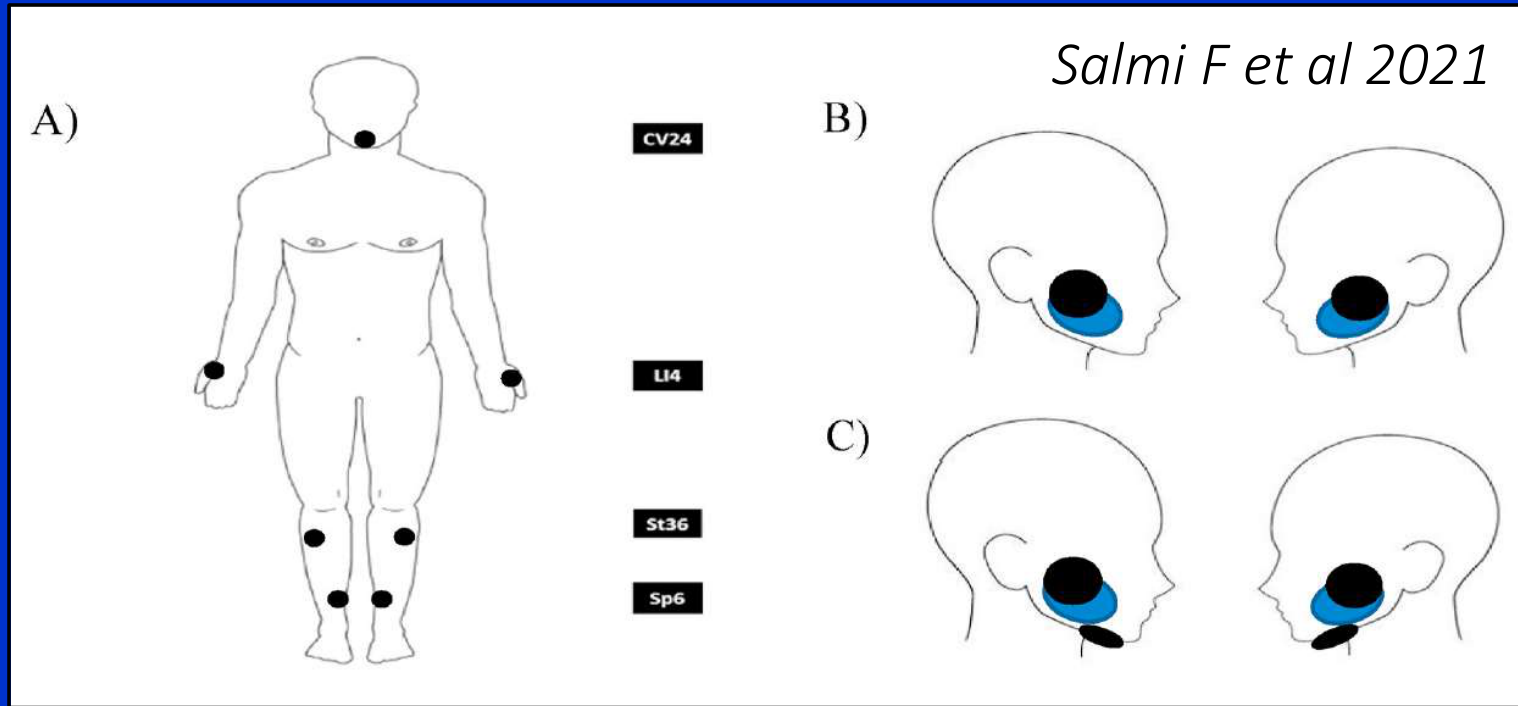
Advanced Nerve Stimulation73
- ALTENS (Acupuncture-like TENS): Combines electrical stimulation with acupuncture principles.
- Target Points: Stimulation often targets body points (CV24, LI4, St36, Sp6) and specific head points.
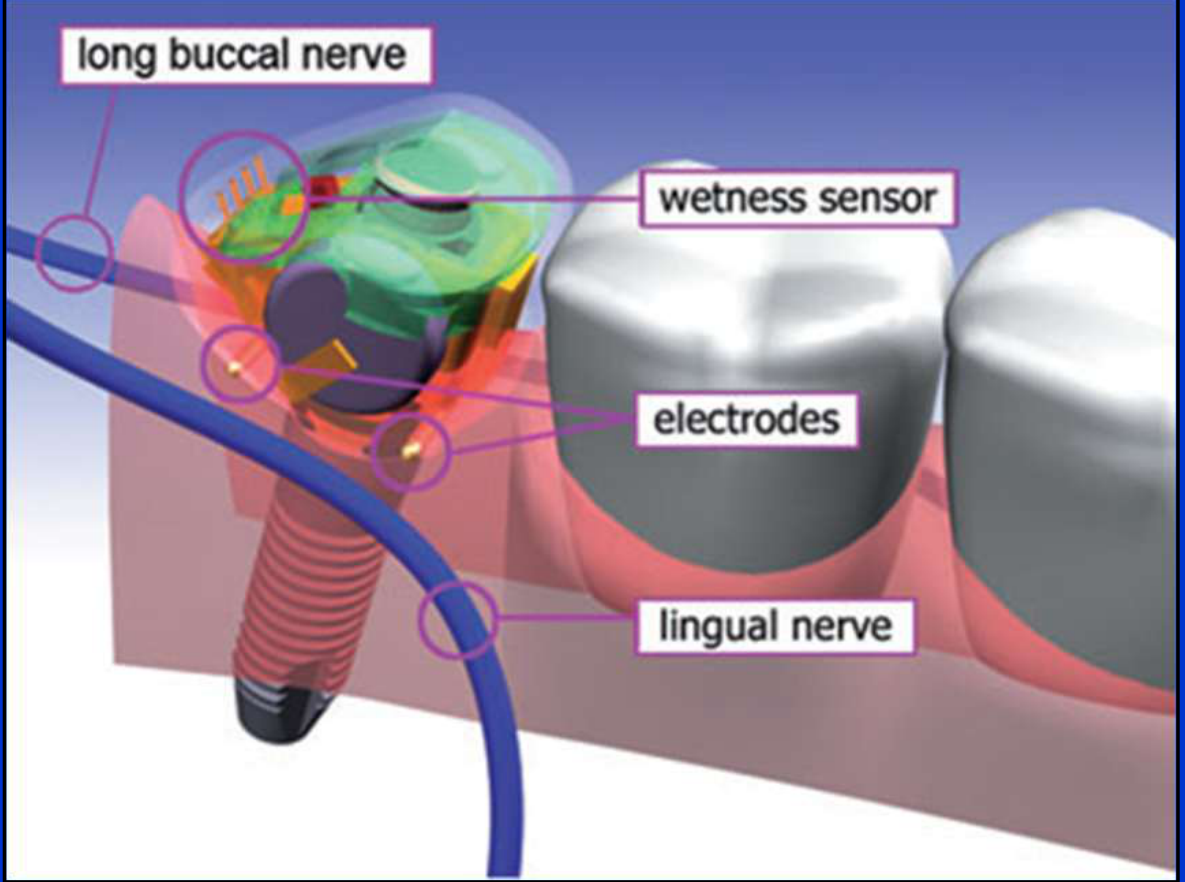
Specific Intraoral Devices74757677
- Removable Options:
- GenNarino
- SaliPen
- Implant-Supported Options:
- Saliwell Crown
- MICROSAL
Neuro-electrostimulation continues to be evaluated as a method for inducing salivary flow through neural pathways.
- Devices like Saliwell or Sallipen use electrodes to stimulate the lingual nerve and salivary reflex.
Salivary neuro-electrostimulation involves the application of electrical currents to stimulate the nerves responsible for salivary gland function.
The application of neuro-electrostimulation is a specialized approach in the management of salivary dysfunction.
 |  |  |
 |  |  |
 |
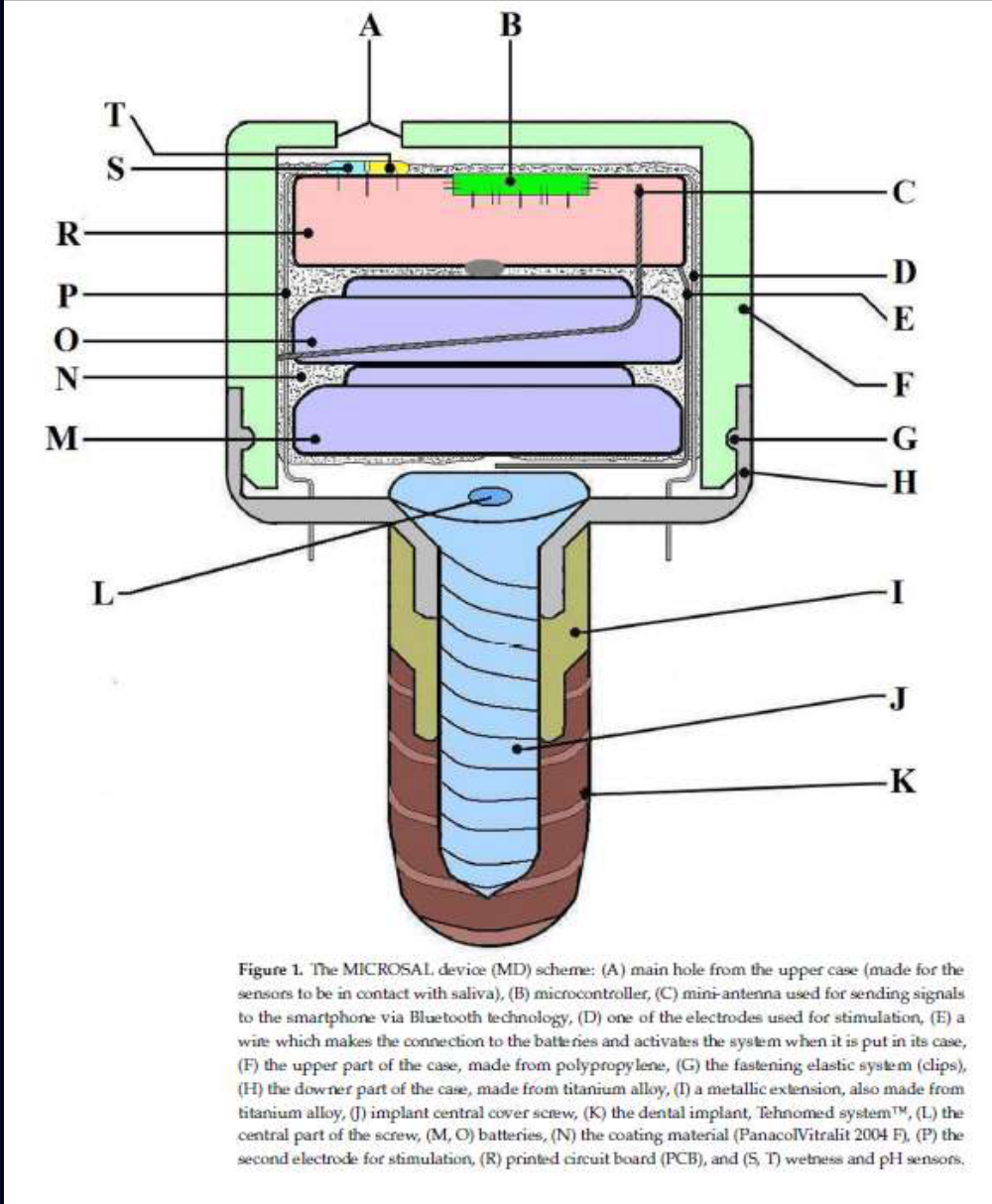
The MICROSAL Device (MD)78
The MICROSAL system is an integrated dental implant stimulation device featuring:
- Sensors: Wetness and pH sensors (S, T) in contact with saliva via a main hole (A).
- Electronics: Microcontroller (B), printed circuit board (R), and batteries (M, O).
- Communication: Mini-antenna (C) for Bluetooth connection to smartphones.
- Stimulation: Dual electrodes (D, P) for active stimulation.
- Housing: Titanium alloy lower case (H) and polypropylene upper case (F) secured by an elastic fastening system (G).
- Integration: Attached to a dental implant (K) via a central cover screw (J) and metallic extension (I).
- The device is a novel Romanian invention that communicates with smartphones to self-regulate stimulation.
 |  |
 |
Summary of Evidence79
There is currently limited evidence to definitively determine the effects of electrostimulation devices on either subjective dry mouth symptoms or objective saliva production. - Emerging evidence shows potential specifically for Sjogren’s syndrome and radiation patients.
Acupuncture80
- Evidence remains limited regarding the use of acupuncture for the management of hyposalivation and xerostomia.
Photobiomodulation81
- Radiation Therapy Parameters:
- Wavelength: 630–830 nm
- Radiant exposure: 2–10 J/cm²
- Frequency: 1–3 times per week
- May protect glands during radiation and improve flow in diabetic or medication-induced cases.
Experimental Approaches and Complication Management
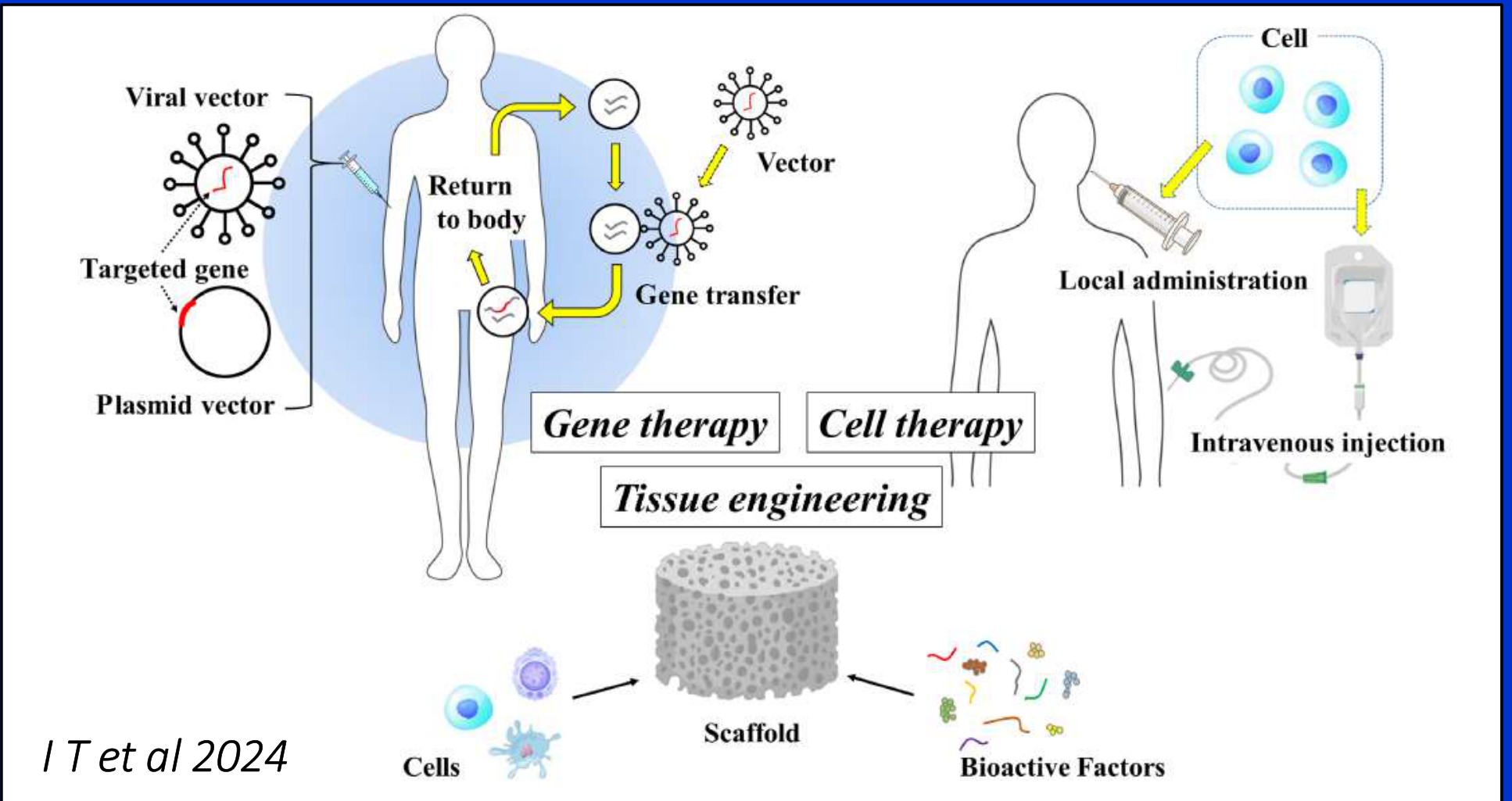
Experimental Therapeutic Approaches82
Research is currently investigating advanced biological interventions:
- Gene Therapy: Modifying cellular function to restore secretion.
- Cell Therapy: Utilizing stem cells or specialized cells to regenerate gland tissue.
- Tissue Engineering: Creating functional salivary gland constructs.
Managing Dental Caries Risk83
Patients with dry mouth require intensive preventive care due to increased caries risk:
- Dietary Modification: Reducing fermentable carbohydrates.
- Oral Hygiene: Enhanced plaque control.
- Fluoride: High-concentration topical applications.
- Re-mineralizing Agents: Products to support enamel integrity.
- Antimicrobial Agents: To manage oral flora.
- Regular Dental Care: Frequent professional monitoring
- Patients often crave cariogenic "soft" foods, necessitating constant dietary monitoring.
Management of Oral Complications84
- Mucosal Disease: Treatment of mucositis and oral candidiasis (fungal infections).
- Sialadenitis: Management of salivary gland inflammation.
- Halitosis: Addressing breath odor resulting from reduced flow and microbial changes
- Mucositis: Avoid irritants such as alcohol and spicy foods.
Prevention and Summary
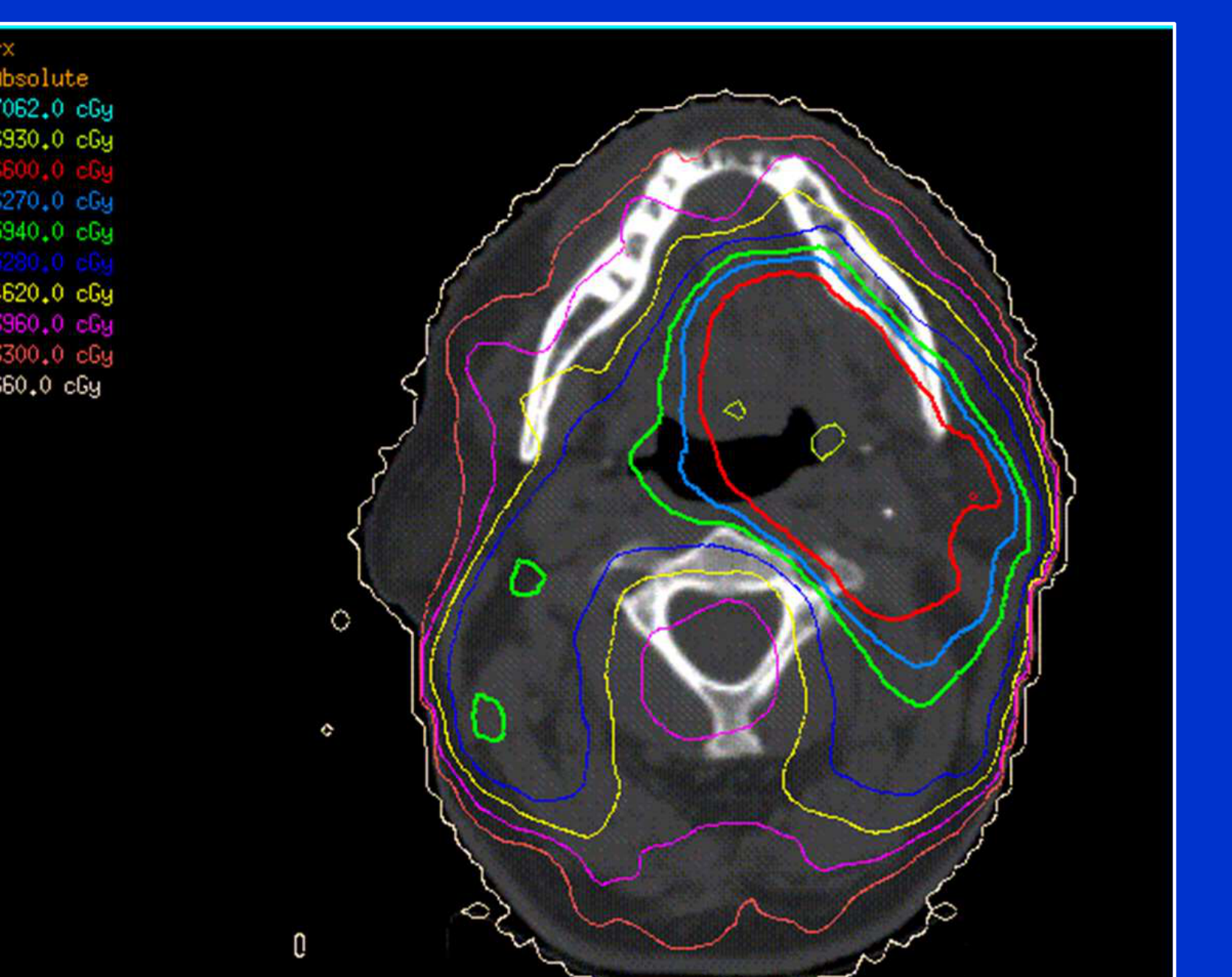
Preventive Focus Areas85
Prevention strategies are particularly critical for high-risk populations:
- Head and neck cancer patients (undergoing radiation/chemotherapy)
- Use IMRT (Intensity-Modulated Radiation Therapy) to limit doses to salivary glands.
- Patients with Sjögren’s Syndrome
- Use disease-modifying agents early in the disease course.
Summary of Dry Mouth Management86
- Clinical Context: Dry mouth is a common, complex, and growing problem requiring correct diagnosis.
- The prevalence is increasing specifically due to the aging population.
- Management Strategy:
- Address the underlying cause whenever possible.
- Provide symptomatic management for comfort.
- Utilize salivary stimulation techniques.
- Proactively manage secondary complications.
Footnotes
-
Original PDF page 1: L16 Dry Mouth, p.1 ↩
-
Original PDF page 2: L16 Dry Mouth, p.2 ↩
-
Original PDF page 3: L16 Dry Mouth, p.3 ↩
-
Original PDF page 4: L16 Dry Mouth, p.4 ↩
-
Original PDF page 5: L16 Dry Mouth, p.5 ↩
-
Original PDF page 6: L16 Dry Mouth, p.6 ↩
-
Original PDF page 7: L16 Dry Mouth, p.7 ↩
-
Original PDF page 9: L16 Dry Mouth, p.9 ↩
-
Original PDF page 11: L16 Dry Mouth, p.11 ↩
-
Original PDF page 8: L16 Dry Mouth, p.8 ↩
-
Original PDF page 10: L16 Dry Mouth, p.10 ↩
-
Original PDF page 12: L16 Dry Mouth, p.12 ↩
-
Original PDF page 13: L16 Dry Mouth, p.13 ↩
-
Original PDF page 14: L16 Dry Mouth, p.14 ↩
-
Original PDF page 15: L16 Dry Mouth, p.15 ↩
-
Original PDF page 16: L16 Dry Mouth, p.16 ↩
-
Original PDF page 17: L16 Dry Mouth, p.17 ↩
-
Original PDF page 18: L16 Dry Mouth, p.18 ↩
-
Original PDF page 19: L16 Dry Mouth, p.19 ↩
-
Original PDF page 29: L16 Dry Mouth, p.29 ↩
-
Original PDF page 27: L16 Dry Mouth, p.27 ↩
-
Original PDF page 28: L16 Dry Mouth, p.28 ↩
-
Original PDF page 30: L16 Dry Mouth, p.30 ↩
-
Original PDF page 31: L16 Dry Mouth, p.31 ↩
-
Original PDF page 32: L16 Dry Mouth, p.32 ↩
-
Original PDF page 33: L16 Dry Mouth, p.33 ↩
-
Original PDF page 34: L16 Dry Mouth, p.34 ↩
-
Original PDF page 35: L16 Dry Mouth, p.35 ↩
-
Original PDF page 36: L16 Dry Mouth, p.36 ↩
-
Original PDF page 37: L16 Dry Mouth, p.37 ↩
-
Original PDF page 38: L16 Dry Mouth, p.38 ↩
-
Original PDF page 39: L16 Dry Mouth, p.39 ↩
-
Original PDF page 40: L16 Dry Mouth, p.40 ↩
-
Original PDF page 41: L16 Dry Mouth, p.41 ↩
-
Original PDF page 42: L16 Dry Mouth, p.42 ↩
-
Original PDF page 43: L16 Dry Mouth, p.43 ↩
-
Original PDF page 44: L16 Dry Mouth, p.44 ↩
-
Original PDF page 45: L16 Dry Mouth, p.45 ↩
-
Original PDF page 46: L16 Dry Mouth, p.46 ↩
-
Original PDF page 47: L16 Dry Mouth, p.47 ↩
-
Original PDF page 48: L16 Dry Mouth, p.48 ↩
-
Original PDF page 49: L16 Dry Mouth, p.49 ↩
-
Original PDF page 50: L16 Dry Mouth, p.50 ↩
-
Original PDF page 51: L16 Dry Mouth, p.51 ↩
-
Original PDF page 52: L16 Dry Mouth, p.52 ↩
-
Original PDF page 53: L16 Dry Mouth, p.53 ↩
-
Original PDF page 54: L16 Dry Mouth, p.54 ↩
-
Original PDF page 55: L16 Dry Mouth, p.55 ↩
-
Original PDF page 56: L16 Dry Mouth, p.56 ↩
-
Original PDF page 57: L16 Dry Mouth, p.57 ↩
-
Original PDF page 58: L16 Dry Mouth, p.58 ↩
-
Original PDF page 59: L16 Dry Mouth, p.59 ↩
-
Original PDF page 60: L16 Dry Mouth, p.60 ↩
-
Original PDF page 61: L16 Dry Mouth, p.61 ↩
-
Original PDF page 62: L16 Dry Mouth, p.62 ↩
-
Original PDF page 63: L16 Dry Mouth, p.63 ↩
-
Original PDF page 64: L16 Dry Mouth, p.64 ↩
-
Original PDF page 65: L16 Dry Mouth, p.65 ↩
-
Original PDF page 66: L16 Dry Mouth, p.66 ↩
-
Original PDF page 67: L16 Dry Mouth, p.67 ↩
-
Original PDF page 68: L16 Dry Mouth, p.68 ↩
-
Original PDF page 69: L16 Dry Mouth, p.69 ↩
-
Original PDF page 70: L16 Dry Mouth, p.70 ↩
-
Original PDF page 71: L16 Dry Mouth, p.71 ↩
-
Original PDF page 74: L16 Dry Mouth, p.74 ↩
-
Original PDF page 75: L16 Dry Mouth, p.75 ↩
-
Original PDF page 76: L16 Dry Mouth, p.76 ↩
-
Original PDF page 77: L16 Dry Mouth, p.77 ↩
-
Original PDF page 78: L16 Dry Mouth, p.78 ↩
-
Original PDF page 79: L16 Dry Mouth, p.79 ↩
-
Original PDF page 80: L16 Dry Mouth, p.80 ↩
-
Original PDF page 81: L16 Dry Mouth, p.81 ↩
-
Original PDF page 82: L16 Dry Mouth, p.82 ↩
-
Original PDF page 83: L16 Dry Mouth, p.83 ↩
-
Original PDF page 84: L16 Dry Mouth, p.84 ↩
-
Original PDF page 85: L16 Dry Mouth, p.85 ↩
-
Original PDF page 86: L16 Dry Mouth, p.86 ↩
-
Original PDF page 87: L16 Dry Mouth, p.87 ↩
-
Original PDF page 88: L16 Dry Mouth, p.88 ↩
-
Original PDF page 89: L16 Dry Mouth, p.89 ↩
-
Original PDF page 90: L16 Dry Mouth, p.90 ↩
-
Original PDF page 91: L16 Dry Mouth, p.91 ↩
-
Original PDF page 92: L16 Dry Mouth, p.92 ↩
-
Original PDF page 93: L16 Dry Mouth, p.93 ↩
-
Original PDF page 94: L16 Dry Mouth, p.94 ↩
-
Original PDF page 95: L16 Dry Mouth, p.95 ↩