Viral, Bacterial, Fungal Infections of the Oral Cavity1
Dr Lalima Tiwari
BDSc (UWA), DClinDent (OralMed) (UWA), MRACDS (OralMed), FOMAA
Oral Medicine Specialist | Adjunct Senior Lecturer
Learning Outcomes
Core Knowledge Requirements2
Develop a comprehensive knowledge of viral, bacterial, and fungal infections affecting the oral soft tissues, specifically:
Career Context
- Understand that these infections are common and will frequently be encountered in a dental career
- Be aware of how to identify and diagnose these conditions appropriately
- Viral Infections
- Herpes simplex infection
- Varicella zoster infection
- Hand foot and mouth disease
- Bacterial Infections
- Syphilis
- Gonorrhoea
- Tuberculosis
- Fungal Infections
- Oral candidiasis The oral mucosa is a common site for primary viral infections, particularly HHV and HPV
- HPV has strong oncogenic associations with oropharyngeal cancers
- Other viruses manifesting in oral cavity include HIV and HCV
**Clinical Competencies and Outcomes **
- Discuss the clinical features, histopathology, investigation, and management of common and important infections that:
- Are primary or reactivated infections of oral soft tissues.
- Have oral soft tissue manifestations but also involve other parts of the body.
- Describe the clinical features of infections in immunocompromised patients.
- Describe appropriate measures to reduce risks of infection spread.
Viral Infections
Outcomes to know for viral infections
- Key clinical features of a viral infection
- what are some ways to investigate a suspected viral infection
- Are there any special considerations for an adult with severe viral infection?
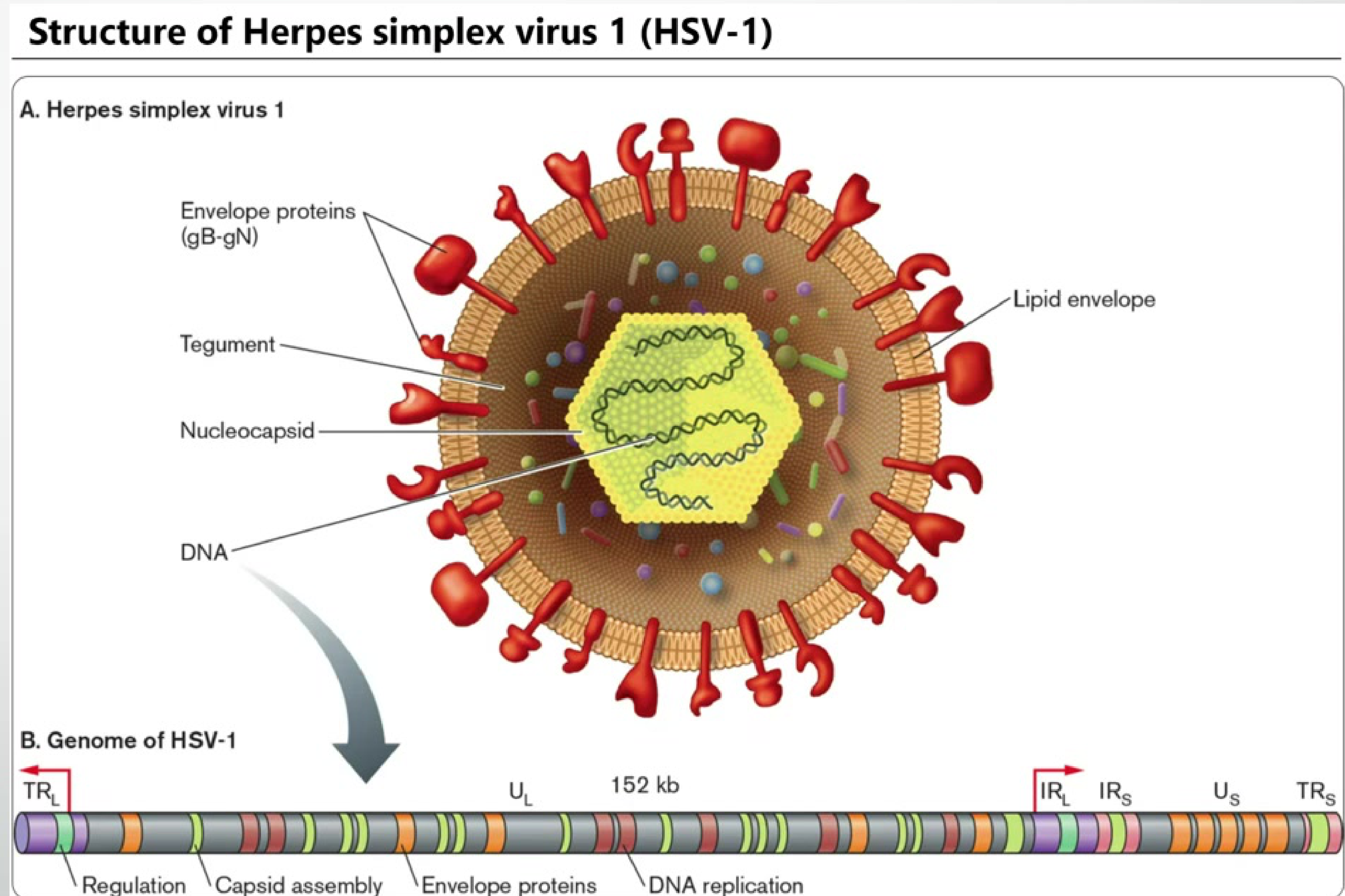
Herpes Simplex Virus34
Background
- Part of the Human Herpesvirus (HHV) family
- DNA virus
- -herpevirinae virus
- Short reproductive cycle
- Characterized by irreversible destruction of infected cells, followed by maintenance of latent infection in the sensorial neural ganglion
- Includes HSV-1, HSV-2, and VZV

Herpes Simplex Infection
“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 985
Clinical Features
“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 985
Primary HSV-1 Infection
- Demographics: Most common in young patients (6 months to 5 years)
- Onset: 1-2 weeks after exposure
- Symptoms: Malaise, fever, lethargy, widespread ulcerations across oral mucosa and gingiva
- Gingiva becomes swollen and erythematous (often mistaken for ANUG)
- Bilateral cervical lymphadenopathy due to immune response
- Duration: 7-10 days
- Complications: Dehydration (most common), HSV Encephalitis (medical emergency)



Clinical Features5
Primary HSV-1
- affects any orla mucosal surface
- Arises 1-2 weeks of acquisition of the virus
- Non specific features: Malaise, pyrexia, lethargy
- Eruption of widespread ulceration of oral mucosa and gingiva
- superficial small, spherical ulcers that can coelsce to large size, irregular outlined ulcers
- Free/attached gingiva becomes swollen, erythematous, ulcerated; can mimic ANUG
- Symptomps: pain, dysphagia, dysarthria, possibly drooling
- Bilateral cervical lymphadenopathy, macular cutaneous rash
- Resolve within 7 -10 days
- Can be severe and prolonged in immunocompromised individuals
- **Primary Herpetic Gingivostomatitis most common clinical presentation **
- Children aged 6 months - 5 years
- **Dehydration most common complication **
- lethargy, drowsiness or focal neurology and altered behaviors may indicate HSV encephalitis
Primary HSV-2 Infection
- Similar clinical picture to HSV-1
- Illness may be less severe
- Not as prolonged as that caused by HSV-1
- Location: Most commonly affects the hard and soft palate, primarily due to orogenital contact
Secondary HSV-1 Infection67
- Reactivated HSV-1 infection
- Affects about 30% of patients with a history of primary infection
- Typically affects the vermillion of the lips (herpes labialis/cold sores)
- Can also affect perioral or perinasal skin
- Sole intra-oral involvement is a rare manifestation
- Clinical progression: Paraesthesia erythema vesiculation pustule formation superficial ulceration eventual spontaneous healing
- Duration: Approximately 5–7 days
Precipitating Factors of secondary HSV-1 infection
- Concomitant illness
- Exposure to sunlight or UV radiation
- Phases of the menstrual cycle
- Pregnancy
- Stress
- Immunosuppression (can lead to severe, prolonged herpes labialis involving intra-oral sites)
- Recurs at exact same site each time
- this corresponds to the residency of herpes simplex virus iwthin the trigeminal gnaglion
- Can act as a precipitant of erythema multiforme minor
- Herpetic Whitlow: A complication of primary oral or genital herpes caused by inoculation of the virus through a break in the skin barrier
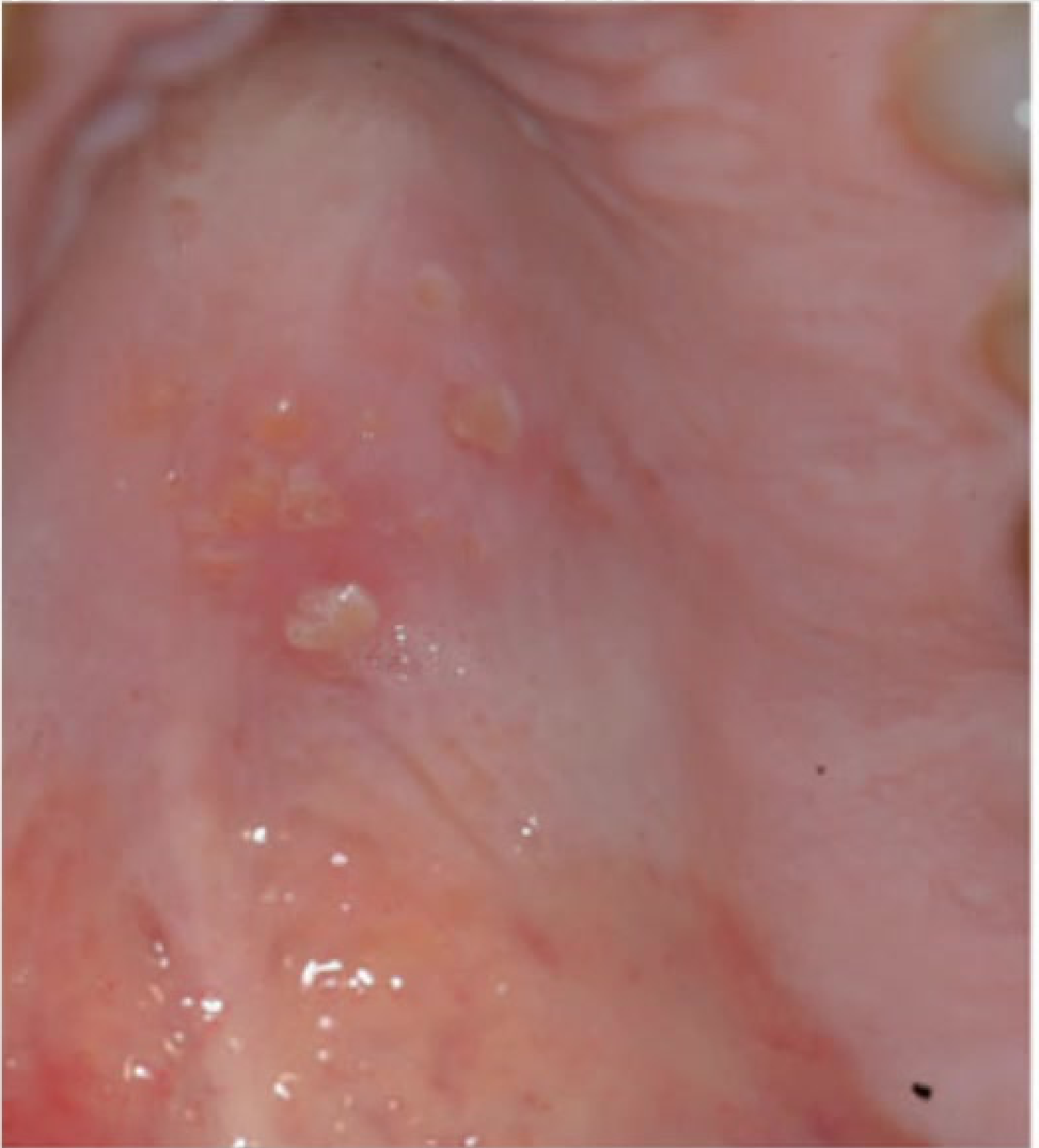
Case Study: Primary Herpetic Gingivostomatitis
Presentation: Classic presentation of primary HSV infected patient, typically a young child Observations: Multiple ulcerations in oral cavity, erythematous and swollen gingiva, significant pain with fever Diagnosis: Primary herpetic gingivostomatitis he exact same site each time due to the location of residency of the virus within the trigeminal ganglion
Case Study: Herpes Labialis
Presentation: Classic presentation of herpes labialis Observations: Vesicle formation, ulceration, and separation. Lesion crusts up and spontaneously heals History: Patient reports lesion recurs in same spot every time, activated by stress or sunlight




** Herpes Simplex infection In Immunocompromised Patients**
Clinical Features
Presents as more severe disease and complications
- Symptoms include severe pharyngitis, oral exudative and ulcerative lesions, fever, malaise, myalgia, and cervical lymphadenopathy
- Chronic mucocutaneous herpes simplex infection may extend into deeper cutaneous layers, leading to tissue necrosis
- Frequent recurrences
- Diagnostic Clue: If patient resembles primary herpetic gingivostomatitis but is an adult, question underlying immune issues
- Rare Complications: Encephalitis or keratitis
Risk Factors for Increased Severity
- HIV Infection: Lesions can occur anywhere (skin, oral, perianal); HSV can affect HIV viral replication, and frequent mucosal reactivation is associated with higher levels of plasma HIV RNA
- Malignancy
- Organ Transplantation: Reactivation rates of 60–80% in patients previously infected with HSV-1
- Malnutrition
- Pregnancy
- Advanced age

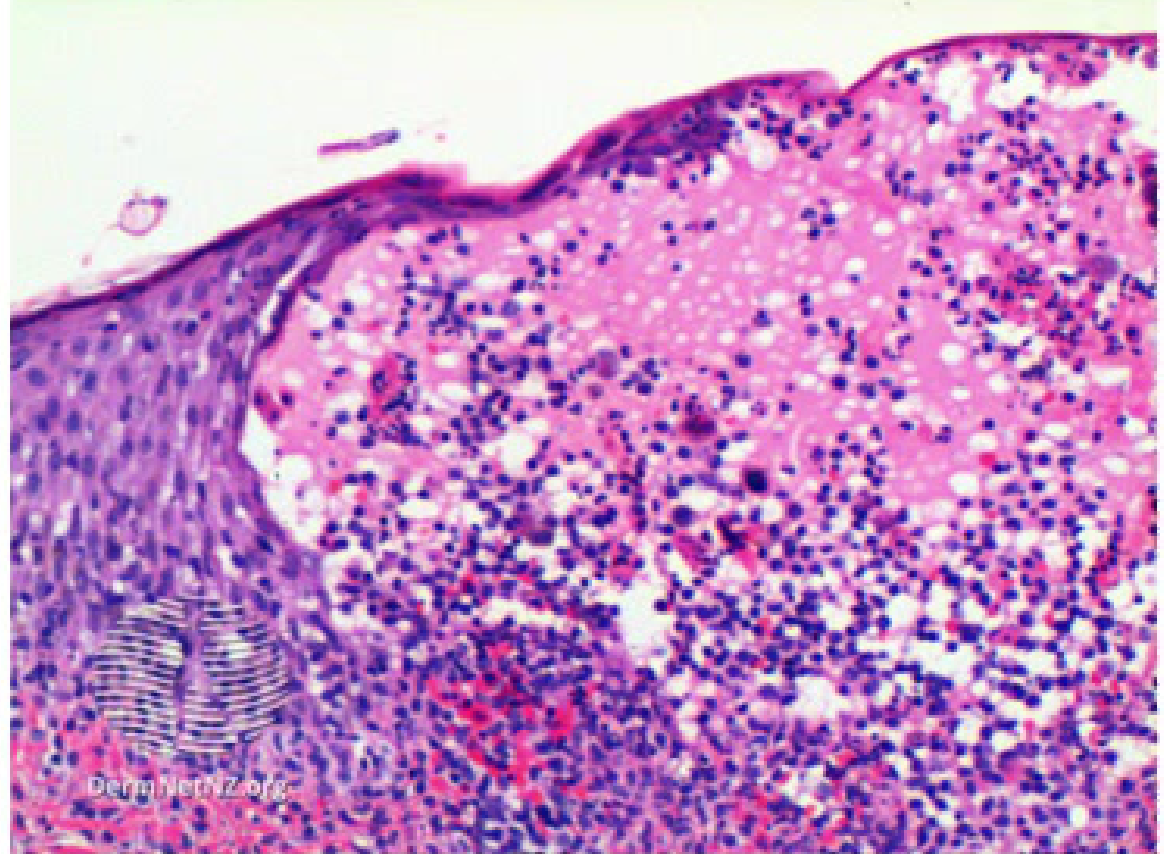
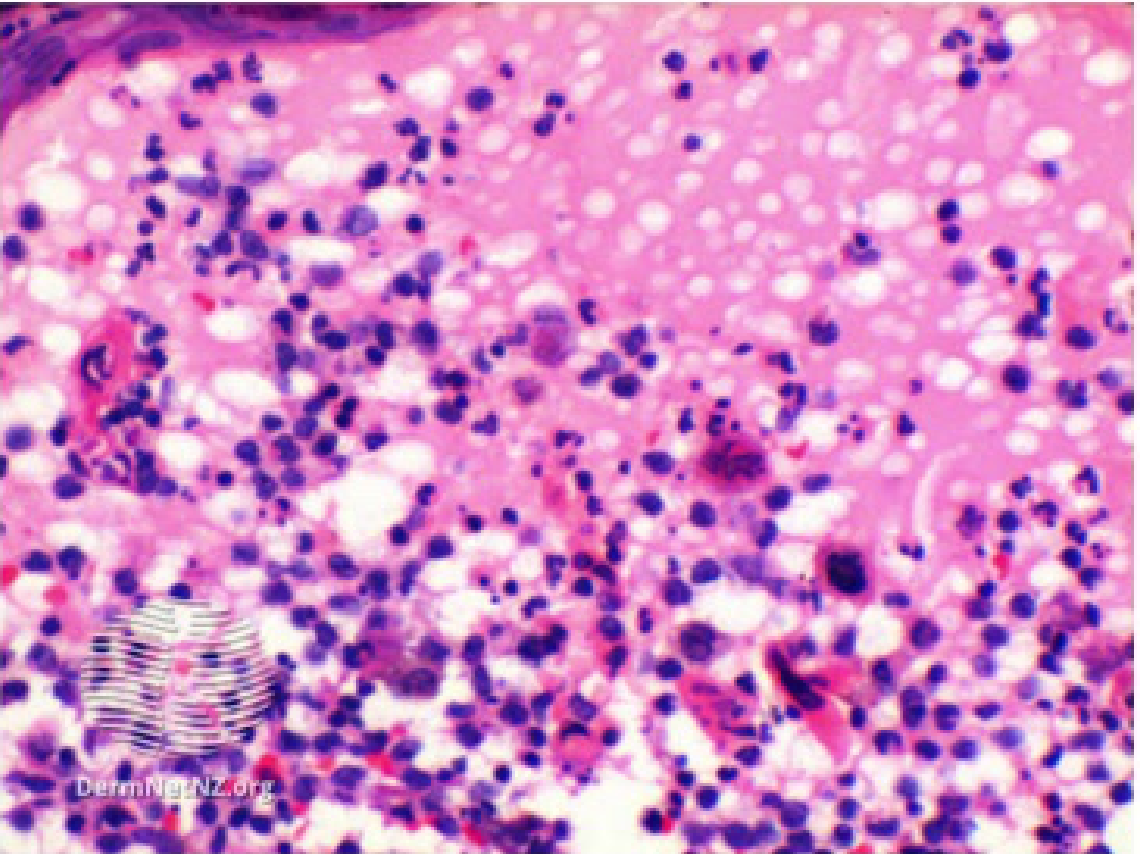
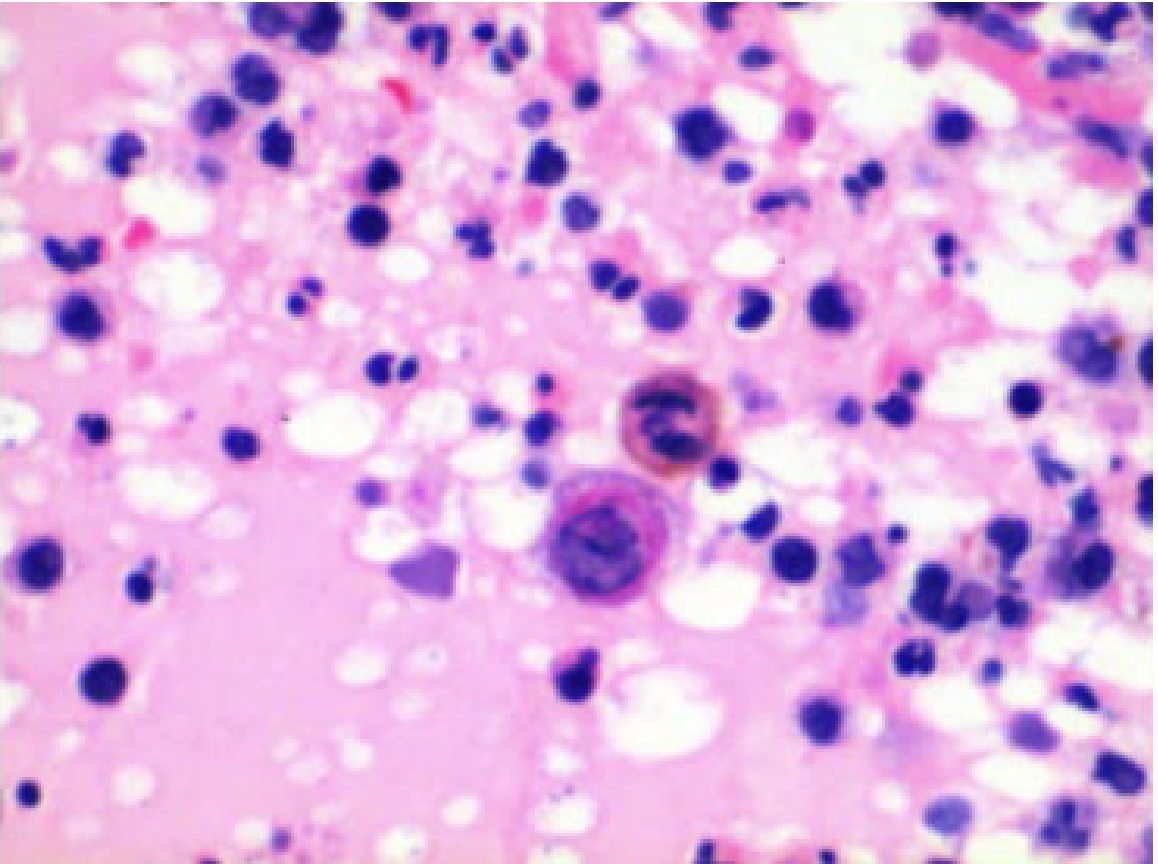
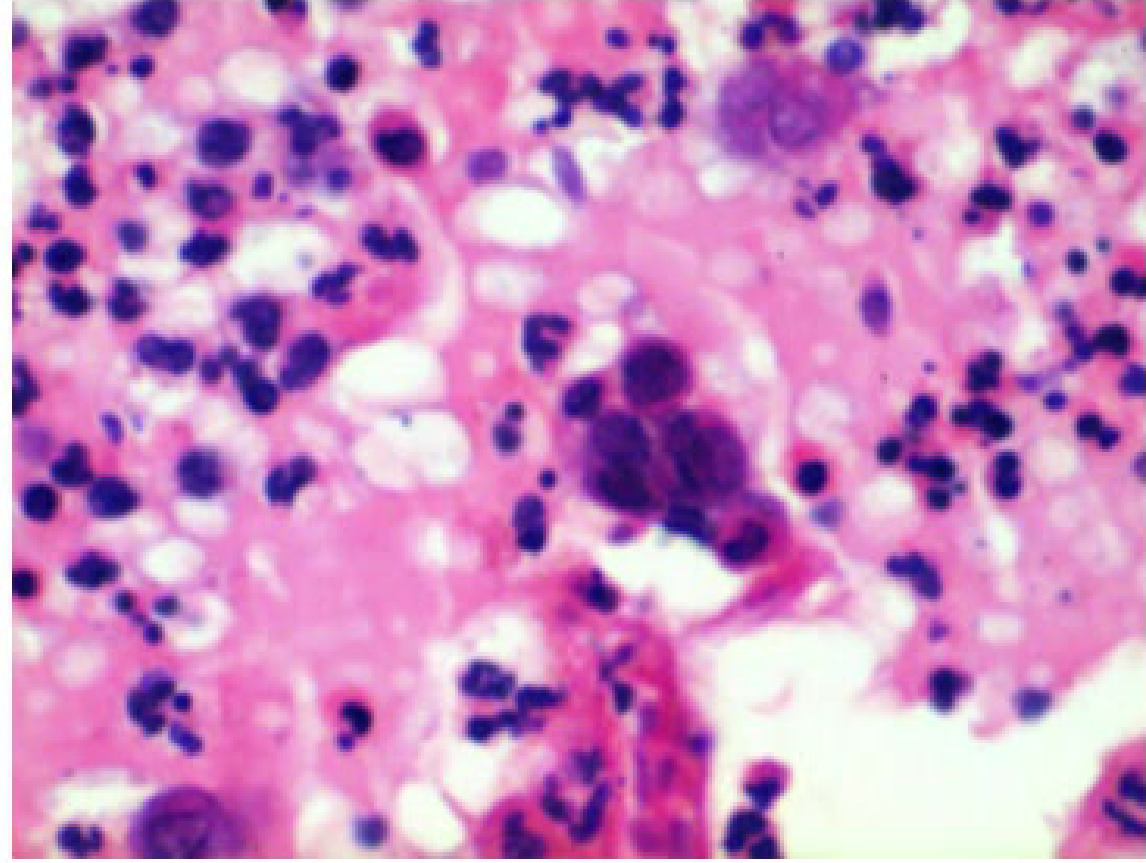
Histopathology of HSV-1 Infection8
- Ballooning degeneration of infected epithelial cells
- Presence of inclusion bodies
- Formation of multinucleated giant epithelial cells
- Acantholysis
- Formation of Tzanck cells
Investigations9
“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 987
- Molecular: PCR testing for identification of HSV DNA
- Viral Culture: Vesicular fluid is removed with a sterile cotton swab and placed in viral medium to determine the presence of HSV-1, HSV-2, or other herpes viruses
- Serology: A greater than four-fold rise in HSV-1 specific IgG antibodies between the acute (ulcerative) and convalescent phases provides a retrospective diagnosis of primary HSV-1
- Full Blood Count (FBC): Should be obtained for adults with primary HSV to rule out underlying causes of immunosuppression
- Immunofluorescence Staining: Examination for herpes antigens via immunofluorescence microscopy
- Clinical Diagnosis: Herpes labialis is primarily a clinical diagnosis
Management10
(“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 987) (pdf)
- Primary HSV-1 Management:
- Topical anti-inflammatory: Benzidamine hydrochloride spray or mouthwash (Difflam)
- Topical anesthetics: Lignocaine gels or mouth rinses
- Systemic analgesia and antipyretics: Ibuprofen or paracetamol to reduce fever
- Hydration: Absolutely key to prevent dehydration
- Antivirals: Acyclovir 200mg tablets or suspension five times daily for 7 days (if severe, immunocompromised, or early presentation)
- Herpes Labialis Management:
- Topical antivirals: 5% acyclovir cream or 1% penciclovir cream
- Timing: Must be applied at prodromal stage (tingling, irritation, itching); not effective once blistering occurs
Direct contact
All patients with primary or secondary HSV should avoid direct contact with other individuals to lessen risk of transmission of the causitive virus

Varicella Zoster Infection
“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 988
Clinical Features11
- Caused by VZV (HHV-3)
- Primary infection: Chicken Pox
- Secondary infection: Shingles (Herpes Zoster)
- Transmission: Via droplets or close contact with lesions
- Chicken Pox
- Commonly seen in preschool children
- Presentation: Maculopapular cutaneous rash evolving into vesicles, then pustulates and scabs
- Systemic: Fever, malaise, reduced appetite, headaches
- Duration: 7-14 days
- Oral Lesions: Can occur before cutaneous rashes; vesicles rupture into multiple small pinpoint ulcerations
- Prevalence: At least 90% of world population infected by age 15
- Complications uncommon: secondary infection of skin lesions can cause:
- impetigo
- cutaneous abscesses, cellulitis
- Rare complications include pulmonary or neurological diseases
Herpes Zoster12
Clinical Features1314
- Also known as Shingles
- Caused by reactivation of VZV in the ganglia of cranial nerves or dorsal roots
- Occurs when cellular immunity to VZV is impaired (e.g., immunosuppression, HIV disease, malignancy)
- Typically occurs later in life
- Affects thoracic dermatomes via reactivation within spinal ganglia
- Characterized by painful eruptions of vesicles, ulceration, and prolonged erythema of skin supplied by one or more dermatomes on one side of the thorax or upper abdomen
- Pain: Intense, sharp pain; may mimic toothache when oral ulcers commence
- Trigeminal Nerve Involvement: Can affect any branch (Ophthalmic > Maxillary > Mandibular) on one side
- Distribution: Unilateral distribution with minor crossover in the midline; bilateral involvement is rare
- the site affected depends on the affected branched of the trigeminal nerv e
-
- Oral Lesions: Similar to HSV-1; superficial ulcers that coalesce into large, irregular ulcers
- Duration: Lasts 5–10 days in immunocompetent hosts; longer in the immunocompromised
- mimics a toothached
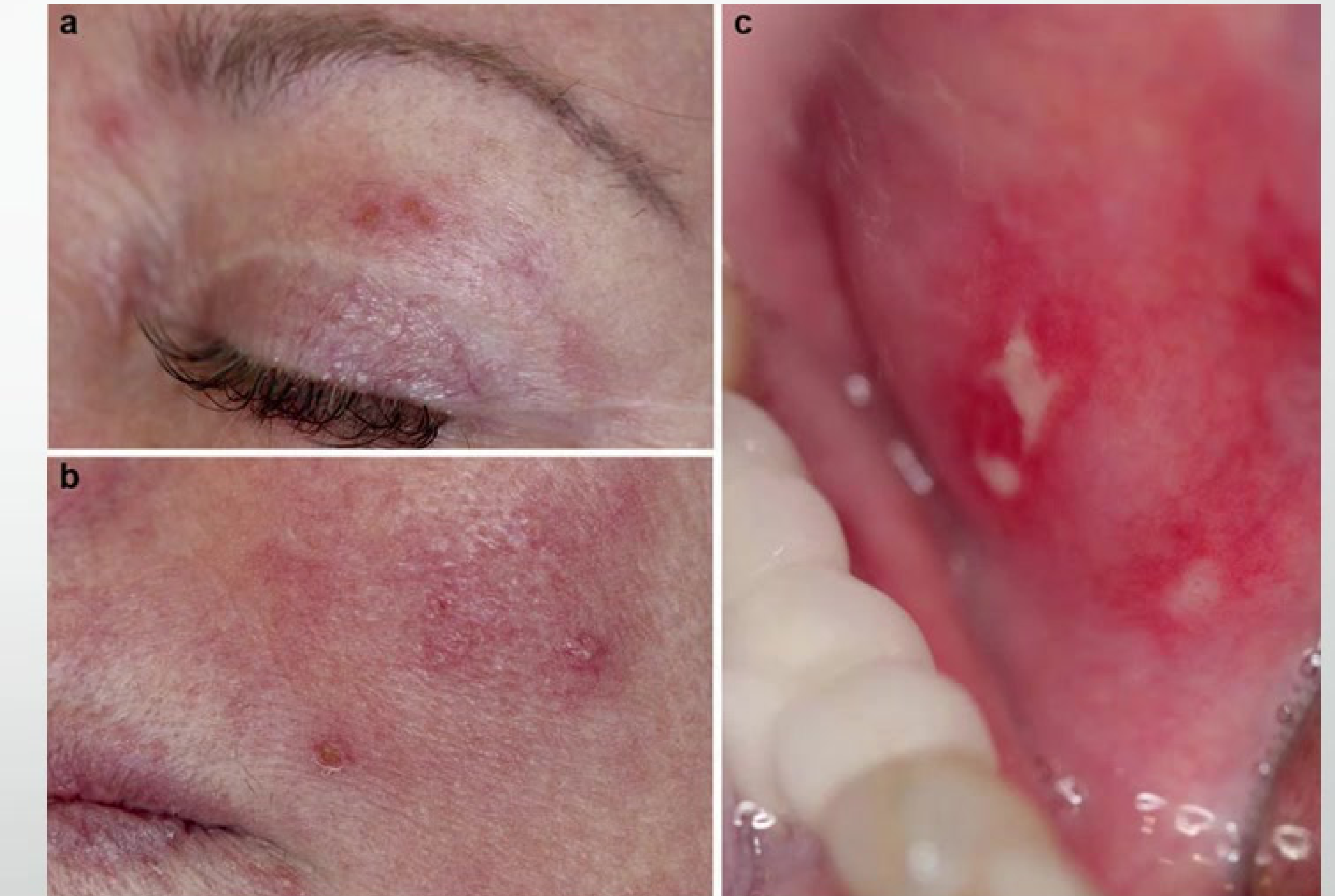
Case Study: Orofacial Shingles
Presentation: Clinical photo showing skin involvement including lip, nose, and zygoma area Observations: Vesicles, erythema, and oral ulcerations following maxillary branch of trigeminal nerve, unilateral distribution Significance: Classic picture of orofacial shingles; important for dentists to detect as it can mimic toothache



**Complications of orofacial shingles
- Post-herpetic neuralgia (PHN): Pain persisting for 3 or more months after the shingles rash has healed
- Stages: Prodromal (<1 week) → Acute Herpetic Neuralgia (rash heals in 2-4 weeks) → Subacute → Post-Herpetic Neuralgia (>3 months)
- Cause: Dysfunction of nerve secondary to viral infection
- Meningoencephalitis
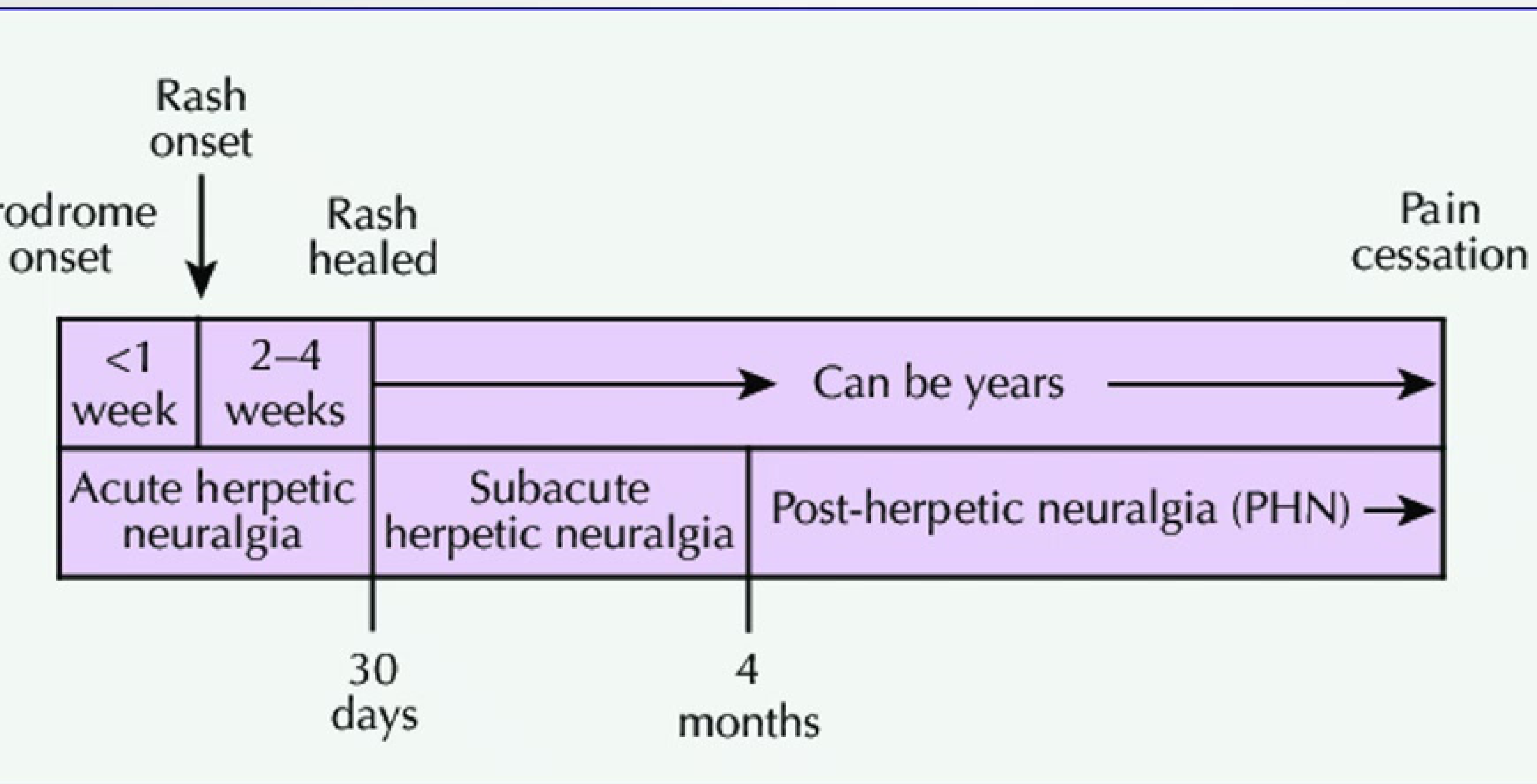 ####### Pain Classification Timeline
####### Pain Classification Timeline
- Acute herpetic neuralgia: From prodrome onset through the first 30 days
- Subacute herpetic neuralgia: From 30 days to 4 months
- Post-herpetic neuralgia (PHN): Pain persisting beyond 4 months
Ramsay Hunt Syndrome15
- A rare manifestation of shingles caused by VZV reactivation within the geniculate ganglion
- Clinical Presentation:
- Otitis externa
- Unilateral lower motor neuron palsy of the facial nerve
- Ulceration of the anterior 2/3 of the tongue and soft palate (ipsilateral to the palsy)
- Assessment: When suspecting orofacial shingles, assess intraorally (soft palate, tongue) and inside ears for vesicles/blistering

Histopathology of varicella zoster
- Histopathology is identical to Herpes Simplex Virus
- Requires clinical correlation, immunohistochemistry, viral culture, or PCR to differentiate between viral types
Investigations for varicella zoster 16
- Diagnosis of chicken pox is primarily based on clinical history and presentation
- Identification of VZV DNA via PCR
- Retrospective serological confirmation (4-fold or more rise in specific antibodies between acute and convalescent phases)
- Prudent to assess Full Blood Count (FBC) for evidence of neutropenia, leukemia, or white blood cell dyscrasias
Management
- Primary (Chickenpox):
- Symptomatic relief (condition runs its course)
- Calamine for itchiness
- Warm baths with sodium bicarbonate or potassium permanganate
- Antivirals not routinely indicated
- Orofacial Shingles:
- Antiviral Therapy: 800mg oral acyclovir five times daily for 7 days (almost always warranted)
- Ophthalmic Involvement: Refer to specialist ophthalmology immediately if ophthalmic division suspected
- Prevention of Spread: Avoid contact with household members (especially older or immunocompromised); isolation important
- Topical antivirals are not beneficial
- Vaccination:
- Chickenpox immunizations available for children (National Immunisation Program)
- Zoster Vaccine: Adults 60+ who have not previously received it; Adults 70-79 receive free; Adults 50+ who are immunocompromised eligible
Hand Foot and Mouth Disease
Clinical Features17
-
Systemic Symptoms: Fever, reduced appetite, sore throat, and malaise
-
Oral Lesions: Numerous vesicles and ulcers (2–7 mm) appearing on day 1–2; typically affects buccal mucosa, labial mucosa, and tongue; disappears after 1 week
-
Cutaneous Lesions: Palms of hands and soles of feet are affected after oral lesions; presents as vesicles or small blisters on the distal flexor aspect of fingers or toes
-
Demographics: Typically affects infants and children between 3-10 years of age
-
Etiology: Most common virus is Coxsackievirus A16 (others include A5, A7, A9, A10)
-
Epidemiology: Outbreaks most frequent in summertime; common in schools, nurseries, daycare; can affect parents, carers, teachers
-
Transmission: Fecal-oral contact, inhalation of respiratory droplets, or direct interaction with cutaneous lesions
-
Incubation: 3-7 days; most contagious in first week; virus present in feces for 6-8 weeks and respiratory system for 1 week
-
Prognosis: No notable long-lasting consequences

Histopathology18
- Rarely biopsied
- Lymphocytic infiltration of the epithelium
- Keratinocyte apoptosis
- Intraepithelial/intraepidermal vesiculation resulting from epidermal oedema
Investigations19
- Diagnosis: Typically based on clinical presentation
- Laboratory Tests:
- Viral culture
- Immunoassay from cutaneous lesions, mucosal lesions, or stool samples (oral specimens have the highest isolation rate)
- Biopsy of atypical lesions
- Raised white cell count and atypical lymphocytes
- Raised serum C-reactive protein (CRP)
Management
- Supportive Care: Hydration, topical or systemic analgesia, antipyretics (paracetamol or ibuprofen)
Bacterial Infections
- Bacterial infections are divided into odontogenic (most common) and non-odontogenic.
- Non-odontogenic infections (Syphilis, Gonorrhea, Tuberculosis) pose serious health concerns and diagnostic challenges.
- There has been a worldwide resurgence of these conditions.
Syphilis is a systemic infection with the following characteristics:
Syphilis20
- Caused by Treponema pallidum.
- Anaerobic filamentous spirochete capable of invading any organ of the human body.
- Known as the "great imitator" due to non-specific manifestations and ability to mimic other diseases.
- Organism evades immune system, enabling survival for decades.
- Estimated global prevalence of 0.5% (15-49 year olds).
- Sexually transmitted infection.
- Acquired (sexual) or congenital (vertical) transmission.
- 50% likelihood of transmission after exposure to infectious lesions.
- Indirect transmission via blood transfusions (less frequent).
- Easily transmissible by kissing or close contact with infectious lesions.
- Major global health resurgence; the rate of Syphilis doubled in Western Australia between 2016 – 2020.
Communities at Risk21
Specific groups identified as being at higher risk in Western Australia include:
- Historically: Aboriginal communities in remote areas, Men who have sex with men.
- People experiencing homelessness.
- People who use methamphetamine and/or inject drugs.
- Culturally and linguistically diverse (CALD) people.
- People who are 16 – 35 years old.
- Aboriginal people 16 – 39 years old (Goldfields, Kimberley, Pilbara).
- Women of childbearing age.
- 30% of syphilis infections in Perth accounted for by women of childbearing age.
Clinical Features
- Acquired syphilis can be divided into:
- Primary
- Secondary
- Latent
- Tertiary
- Non specific presentation and remarkable ability to mimic other diseases
Primary Syphilis
Clinical Presentation of the Primary Stage
Clinical Features
- Characteristic Chancre: A highly infectious lesion occurring at the site of inoculation.
- Incubation period: 3 – 90 days.
- Lesion appearance: Large, painless ulcer with an indurated margin.
- Lymphadenopathy: Painless swelling of lymph nodes occurs in 80% of cases after the chancre develops.
- Common Sites: Intrarectal, perianal, and oral (4-12%).
- Oral Sites: Tongue, gingiva, palate, and lips.
- Resolution: Chancres can heal without treatment within 8 weeks, typically without scarring.
- Systemic dissemination: Can occur even if the local lesion heals.
- Diagnostic Challenge: There is a low rate of diagnosis due to the infection often going unnoticed in the primary stage.
Chancre

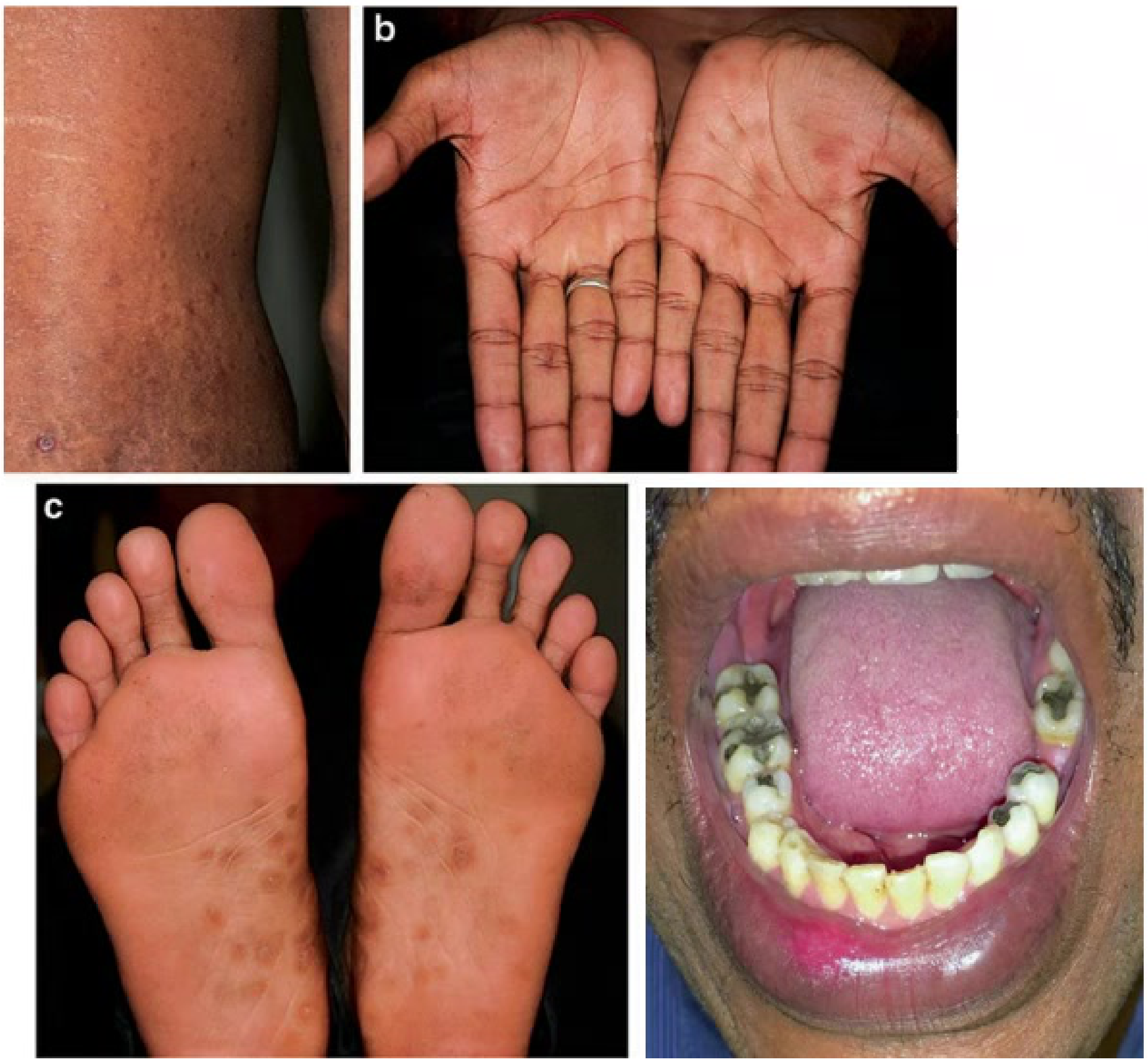
Secondary Syphilis
Clinical Presentation of the Secondary Stage
Clinical Features
- Timing: Occurs 2 – 12 weeks after contact with T. pallidum.
- Dermatological Features: Localised or generalised skin rash, specifically maculopapular lesions on palms and soles. These can mimic eczema, psoriasis, drug eruption, or lichen planus.
- Systemic Symptoms:
- Alopecia, malaise, sore throat, and headache.
- Weight loss and low-grade fever.
- Generalised lymphadenopathy and muscle aches.
- Organ Involvement: Renal, ophthalmologic, hepatic, bone, joint, and CNS involvement may occur.
- Oral Manifestations: Seen in 30% of individuals.
- Mucous patches: Highly infectious, slightly elevated plaques that may be ulcerated.
- Multiple lesions may coalesce to form serpiginous (snail-track) lesions.
- Duration: Lasts for weeks or months, with potential relapses.
Latent Syphilis
Clinical Presentation of the Latent Stage
Clinical Features
- Follows the untreated secondary stage.
- Characterized by an absence of clinical signs of primary or secondary disease.
- Only detectable through serologic testing.
- Sexual transmission is unlikely during this stage.
- Potential for progression to Tertiary Syphilis, involving neurological and cardiovascular complications.
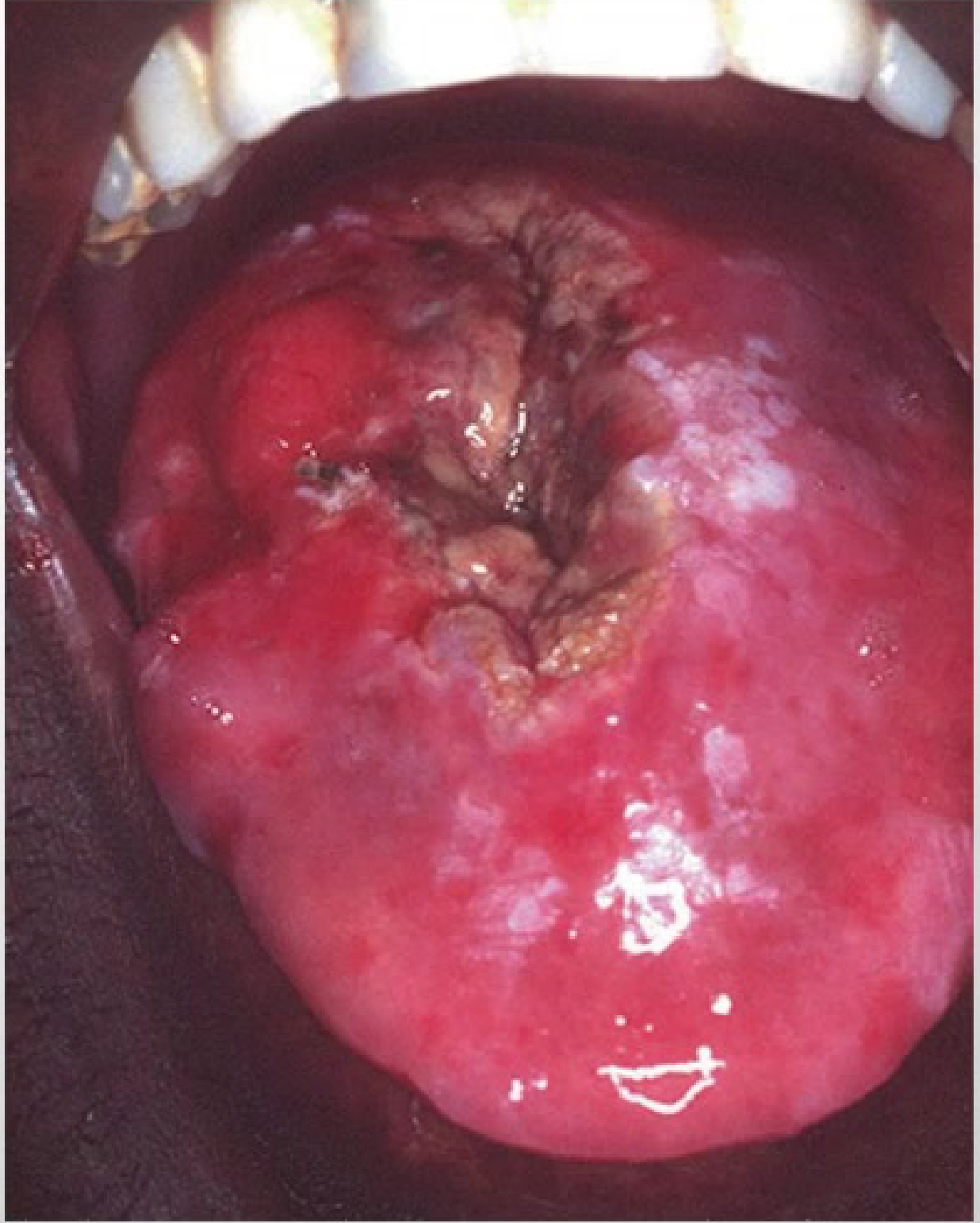
Tertiary Syphilis
Clinical Presentation of the Tertiary Stage
Clinical Features
- Timing: Can manifest 1 year after initial infection or decades later.
- Develops in one-third of untreated patients.
- Transmission unlikely due to low bacterial numbers.
- The Gumma: A characteristic nodular, ulcerative lesion.
- Systemic Involvement: Affects skin, mucous membranes, CNS, liver, spleen, bones, and other organs.
- Cardiovascular Complications: Aortitis, aneurysm, and aortic regurgitation.
- CNS Manifestations: General paralysis and neurological decline.
- Oral Cavity Involvement:
- Affects the palate, tongue, tonsils, lips, and bone.
- Symptoms include pain, swelling, oronasal fistula, and osteonecrosis.
- Associated conditions: Atrophic glossitis, syphilitic leukoplakia, and parotid gland involvement.
Case Study: Tertiary Syphilis Gumma
Presentation: Gumma on the dorsal tongue. Observations: Nodular ulcerative lesion affecting palate, tongue, tonsils, lips, and bone. Significance: Defines the tertiary stage; can cause osteonecrosis and fistulas.
Congenital Syphilis
Clinical Presentation of Congenital Syphilis
Clinical Features
- Transmission: Occurs in utero or during delivery via contact with contagious genital lesions.
- Outcomes: 25 – 50% of cases result in miscarriage; the risk of vertical transmission is 70 – 100%.
- Neonatal Symptoms: Infected infants may show symptoms at birth, including generalized lymphadenopathy, maculopapular rash, hepatosplenomegaly, and glomerulonephritis.
- Progression: Majority of untreated children surviving the first 6 – 12 months will progress to latent and tertiary syphilis.
- Physical Alterations: Saddle nose, high arched palate, frontal bossing of the skull, and mental retardation.
- Oral Manifestations: Peg-shaped incisors (Hutchinson’s teeth), defective molars (mulberry molars), atrophic glossitis, and skin fissures (rhagades).

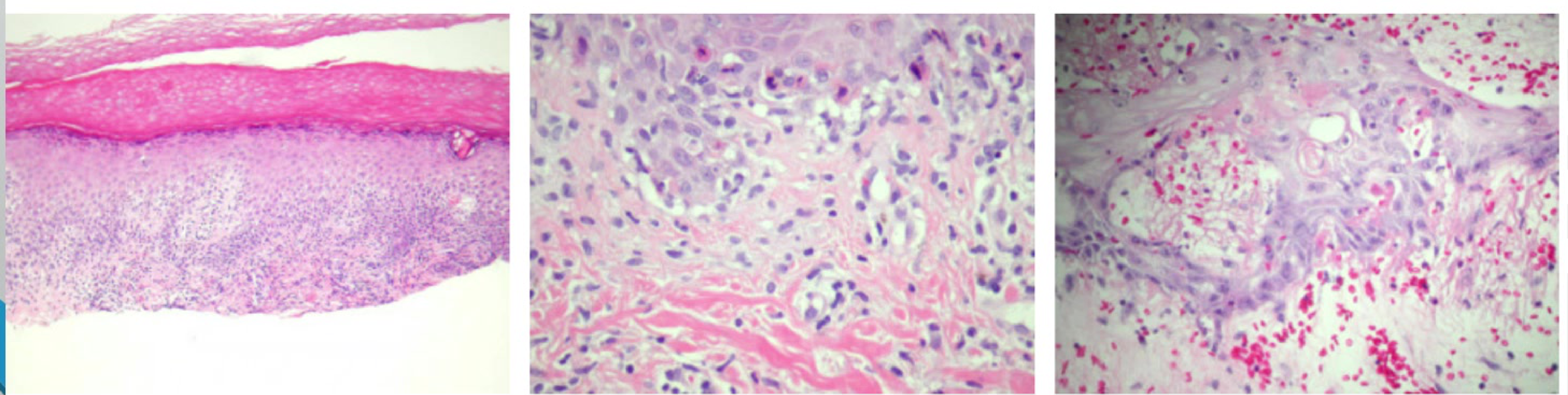
Histopathology
Microscopic Characteristics
- Cellular Infiltrate: Plasma cell infiltration, lymphocytes, and macrophages found in a perivascular distribution or band-like infiltrate in the lamina propria.
- Vascular Changes: Proliferative endarteritis.
- Tertiary Stage Features:
- Absence of epithelial lamina with peripheral pseudoepitheliomatous hyperplasia.
- Lamina propria contains foci of granulomatous inflammation with a large central zone of acellular necrosis.
- Well-circumscribed collections of histiocytes and multinucleated giant cells.
- Identification: Spirochetes can be demonstrated in some lesions using silver stains.
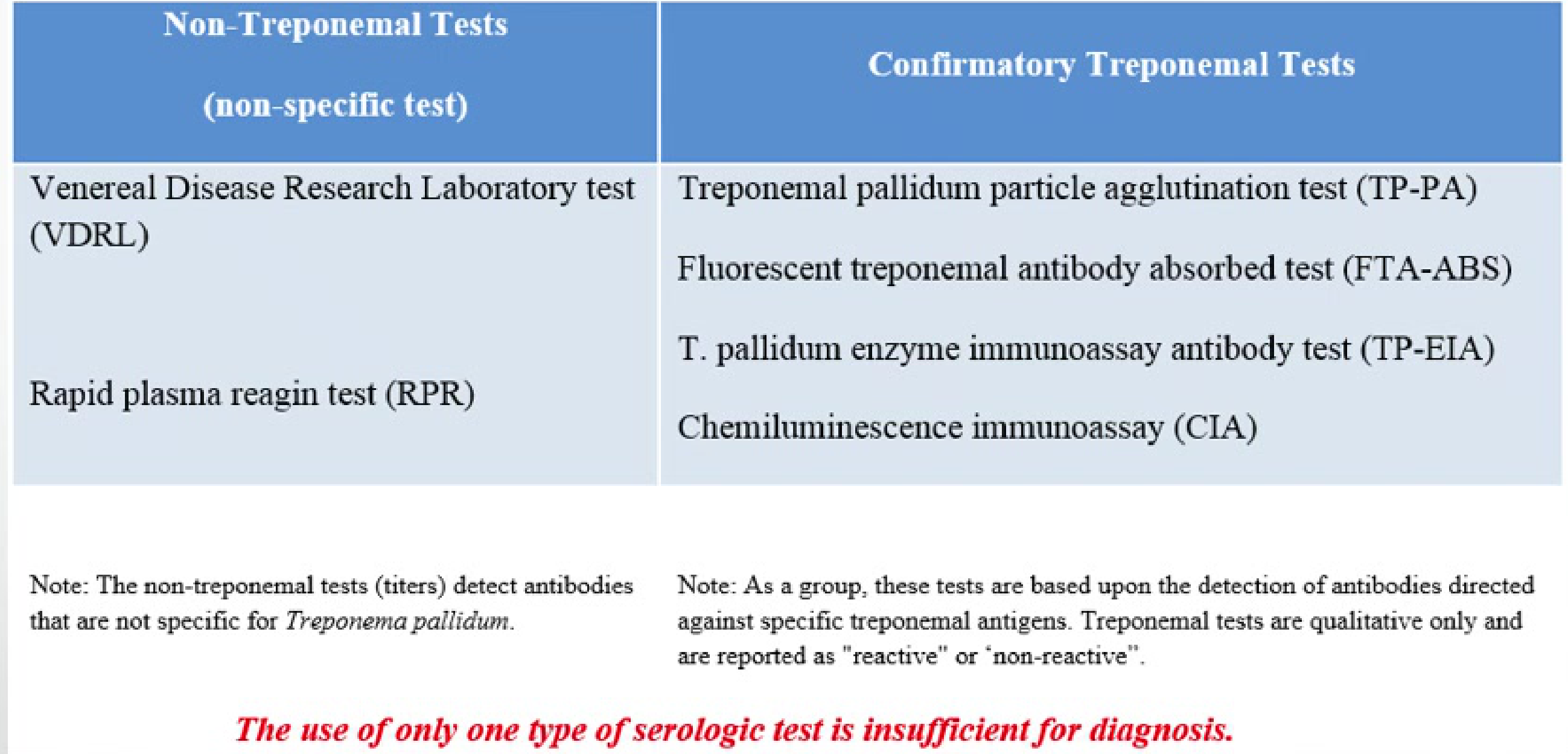
Investigations
Diagnostic Procedures
Diagnosis is based on clinical and serological findings. Biopsy may be used to rule out other pathologies.
-
Nontreponemal Tests (Screening)
- Detect IgM and IgG antibodies to lipoidal material from damaged cells.
- Become positive 1–4 weeks after the primary lesion appears (6 weeks post-exposure).
- Examples: Venereal Disease Research Laboratory (VDRL) and Rapid Plasma Reagin (RPR).
- Note: These are non-specific and may be negative in some latent or tertiary cases. Titers are used to monitor treatment.
-
Treponemal Tests (Diagnostic Confirmation)
- Detect antibodies against specific treponemal antigens.
- Examples: Fluorescent Treponemal Antibody Absorption (FTA-ABS), T. pallidum Particle Agglutination (TP-PA), Enzyme Immunoassay (TP-EIA), and Chemiluminescence Immunoassay (CIA).
- Note: These are qualitative (reactive/non-reactive). Once positive, patients usually remain positive for life.
-
Molecular Testing: Syphilis PCR test.
The use of only one type of serologic test is insufficient for diagnosis.
Syphillis Management
- Treponema pallidum maintains a high sensitivity to penicillin, which remains the primary treatment.
Treatment Protocols by Stage
- Primary, Secondary, Early Latent:
- Benzathine Penicillin: 2.5 million units IM single dose (Adults).
- Children: 50,000 units per kg IM single dose.
- Follow-up: Clinical and serologic evaluation 6-12 months after treatment.
- Late Latent and Late Syphilis:
- Benzathine penicillin 7.2 million units (3 doses of 2.4 million units IM at 1 week intervals).
- Children: 50,000 units per kg IM up to 2.4 million units at three doses in 1 week intervals for children
- Non-treponemal serological tests repeated at 6, 12, and 24 months.
- Tertiary Syphilis:
- Dependent on CSF examination.
- No Neurosyphilis: Benzathine penicillin G 7.2 million units total at 1 week intervals (3 doses)
- Neurosyphilis: Crystalline Penicillin (IV) 18-2million units per day, as 3-4 million units IV every 4h or continuous infusion for 10-14 days,
- usually requiring hospitalization.
Management Protocols
- Co-infection Screening: All patients should be tested for HIV infection.
- Partner Notification: Management and screening of sexual partners are essential.
- Dental Considerations:
- If oral lesions are present, elective dental care should be deferred.
- Normal treatment can recommence once oral lesions are successfully treated.
- Prevention: Focused on education, reduction of sexual partners, and consistent use of barrier protection.
Gonorrhoea
- Sexually transmitted infection
- Caused by *Neisseria gonorrhoeae
- One of the most common STIs
- Can develop and retain antimicrobial resistance
- oral mucosa usually resistant to gonococcal infection as organism cannot invade intact epithelium, but infection can occur when integrity of barrier is compromised
- Needs moist environment to remain viable
Systemic Clinical Features
-
Urogenital: Urethritis in men, cervicitis in women (pain while urinating, purulent/mucopurulent discharge).
-
Children: Can be asymptomatic.
-
Women: Can contribute towards infertility.
-
Eyes: Purulent conjunctivitis (can lead to corneal ulceration).
-
Joints: Rarely affects TMJ (gonococcal arthritis).
-
Global prevalence: 0.6% in men and 0.8% in women.
-
Oral mucosa and skin are generally resistant (cannot invade intact squamous epithelium).
-
Infection requires compromised barrier integrity and a moist environment.
Oropharyngeal and oral Manifestations of Gonorrhoea22
Oropharyngeal involvement
- Prevalence: Oropharyngeal involvement occurs in 20 – 25% of cases.
- Clinical Signs:
- Diffuse oropharyngeal erythema.
- Presence of small pustules.
- Submandibular or cervical lymphadenopathy.
- Gonococcal Tonsillitis.
- Systemic Signs: Fever is infrequent in localized oropharyngeal infection.
- Often asymptomatic and non-specific.
- Can range from slight erythema to severe ulcerations with white pseudomembrane.
- Mimics: Aphthous stomatitis, oral lichen planus, or primary herpetic gingivostomatitis.
- Other symptoms: Parotid gland involvement, oral burning, xerostomia, hypersalivation, dysgeusia, halitosis.

Oral involvement:
- May not be symptomatic
- non-specific
- Ranges from slight erythema to sever ulcertaion with white pseudomembrante
- Apthous stomatitis, oral lichen planus, primary herpetic gingivostomatitis
- occurs within 1 week of exposure
- oral burning, xerostomia, hypersalivation, dysgeusia, halitosis
- involvement of parotid glands can occur in secondary infections
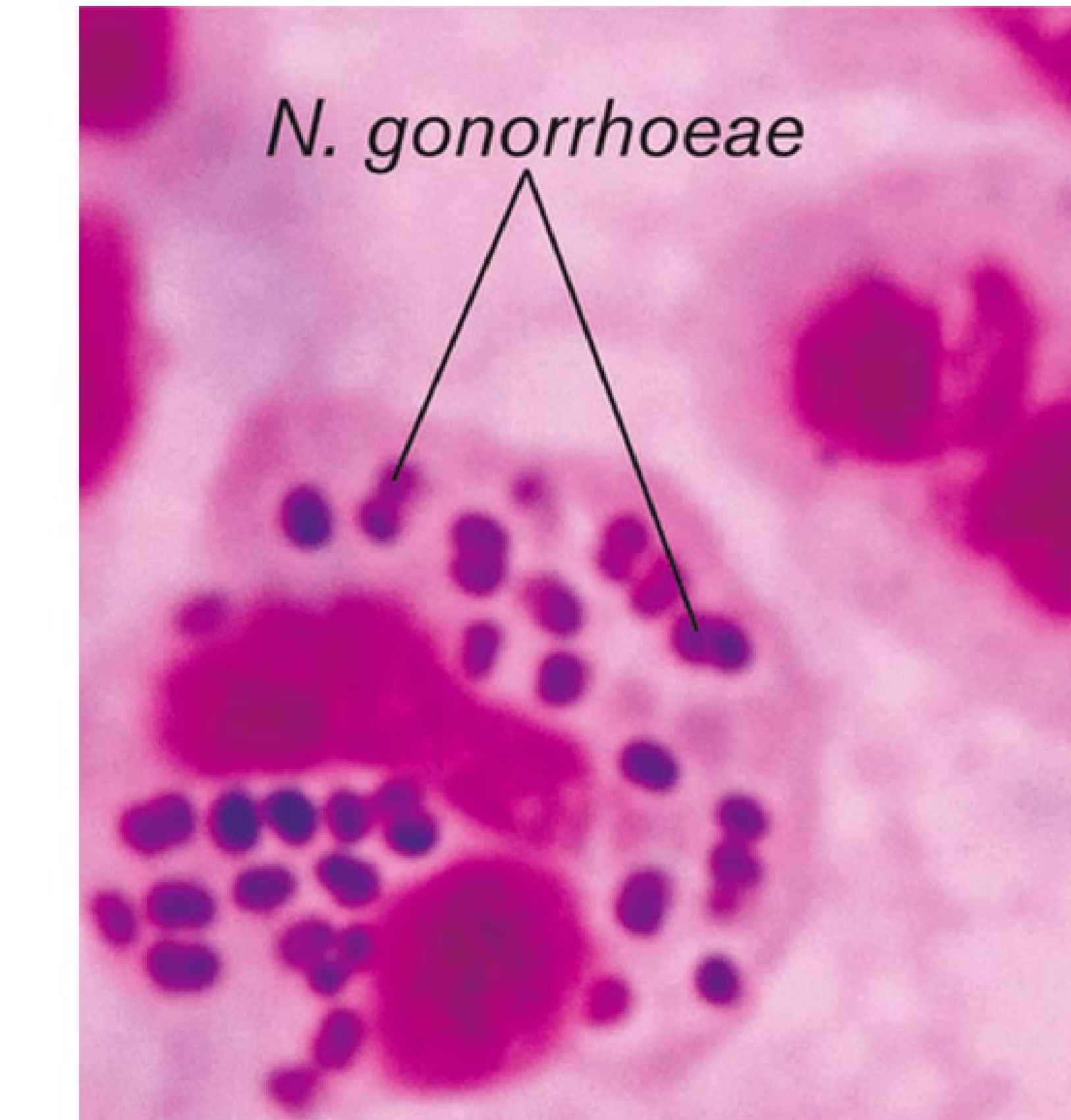
Histopathology
Microscopic Examination
- Gram Stain: Tests for characteristic Gram-negative diplococci within polymorphonuclear leukocytes (PMNLs).
- Limitations: Sensitivity and specificity vary; Gram-staining is not considered suitable for the definitive diagnosis of N. gonorrhoeae from pharyngeal specimens.
- Alternative: Methylene blue staining can be used as an alternative method to Gram stain.
Investigations
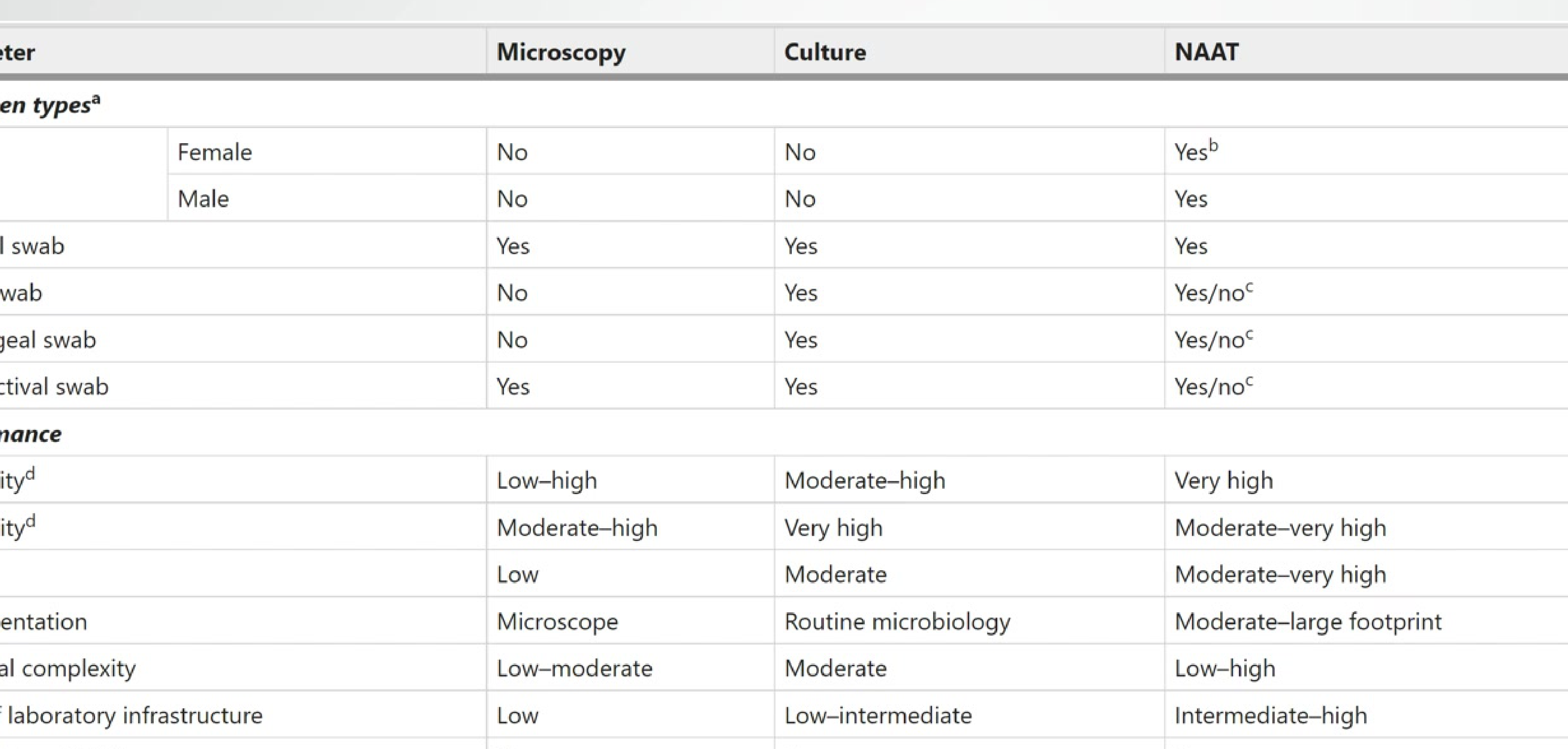
L5 Guide on testing Methods for syphillis
Diagnostic Parameters for Gonorrhoea
Parameter Microscopy Culture NAAT (Nucleic Acid Amplification) Specimen Types Urine Female: No / Male: No No Yes (Lower sensitivity in females) Urethral swab Yes Yes Yes Rectal swab No Yes Yes/No (Platform dependent) Pharyngeal swab No Yes Yes/No (Platform dependent) Conjunctival swab Yes Yes Yes/No (Platform dependent) Performance Sensitivity Low–high Moderate–high Very high Specificity Moderate–high Very high Moderate–very high Cost Low Moderate Moderate–very high Complexity Low–moderate Moderate Low–high POCT Potential Yes No Yes Note: NAAT is the most sensitive method, though culture is required for antibiotic susceptibility testing.
Link to original
Management
Treatment and Management
- Dual Antimicrobial Therapy: Recommended to address potential resistance and co-infection.
- Standard Regimen (Uncomplicated infections of cervix, urethra, rectum, pharynx):
- Ceftriaxone: 250 mg IM as a single dose.
- Azithromycin: 1 g orally as a single dose.
- Contact Tracing: Patients must be counselled to refer any sexual contacts from the preceding 60 days for screening.
- Co-infections: Always check for other sexually transmitted infections.
Tuberculosis
Etiology and Transmission23
Background
-
Following inhalation, bacilli are ingested by alveolar macrophages where they multiply and manipulate macrophage maturation.
-
Notifiable Disease: Substantial impact on public health.
-
Pathogen: Mycobacterium tuberculosis, an aerobic, acid-fast, non-motile, non-encapsulated, and non-spore forming bacillus.
-
Transmission: Respiratory droplets (coughing, sneezing, talking).
-
Risk Factors:
- Mortality exceeds 50% if untreated.
- Immunocompromised individuals are at the greatest risk.
- HIV-positive individuals are 20–40 times more likely to develop active disease; TB is a leading cause of death in this group and accelerates HIV progression. as well as impacts the efficacy of HIV treatment
Clinical Features
Disease Manifestations
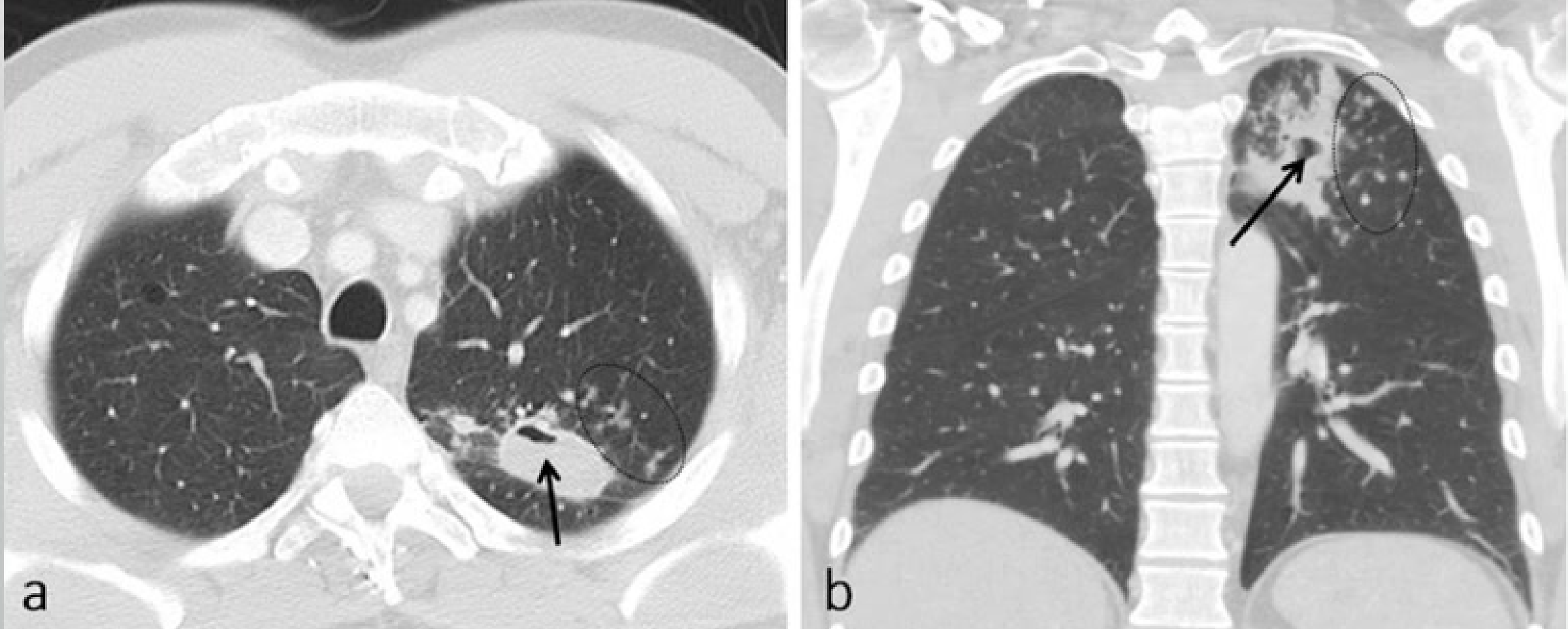
Pulmonary and Extrapulmonary Manifestations
- Pulmonary TB: Accounts for 85% of clinical presentations.
- Extra-pulmonary TB: Occurs in 15 – 25% of cases. Common sites include:
- Lymph nodes (Scrofula): Painful, firm, and non-mobile.
- Pleura, bones, meninges, and genitourinary tract.
- Systemic Symptoms: Night sweats, fever, weight loss, persistent cough, haemoptysis (coughing blood), and pleuritic pain.
- Neurological: Tuberculous meningitis can follow CNS involvement.
Oral Manifestations
Oral Presentation of Tuberculosis
- Prevalence: Uncommon (0.1 – 0.5% of cases).
- Demographics: More common in men; can be primary or secondary to systemic disease.
- Primary Oral TB: More frequently seen in younger individuals.
- Common Features:
- Most common on the tongue, but can affect any oral site.
- Oral ulceration: Indurated, ill-defined margins, with a hard necrotic base or grayish-yellow slough.
- Lesion resembles oral malignancy.
- May present as patches, papillomatous lesions, or indurated soft tissue masses.
- Bone and Glands:
- Tuberculous osteomyelitis: Involves the maxilla or mandible with bone sequestration and pain.
- Rare involvement of the parotid gland.

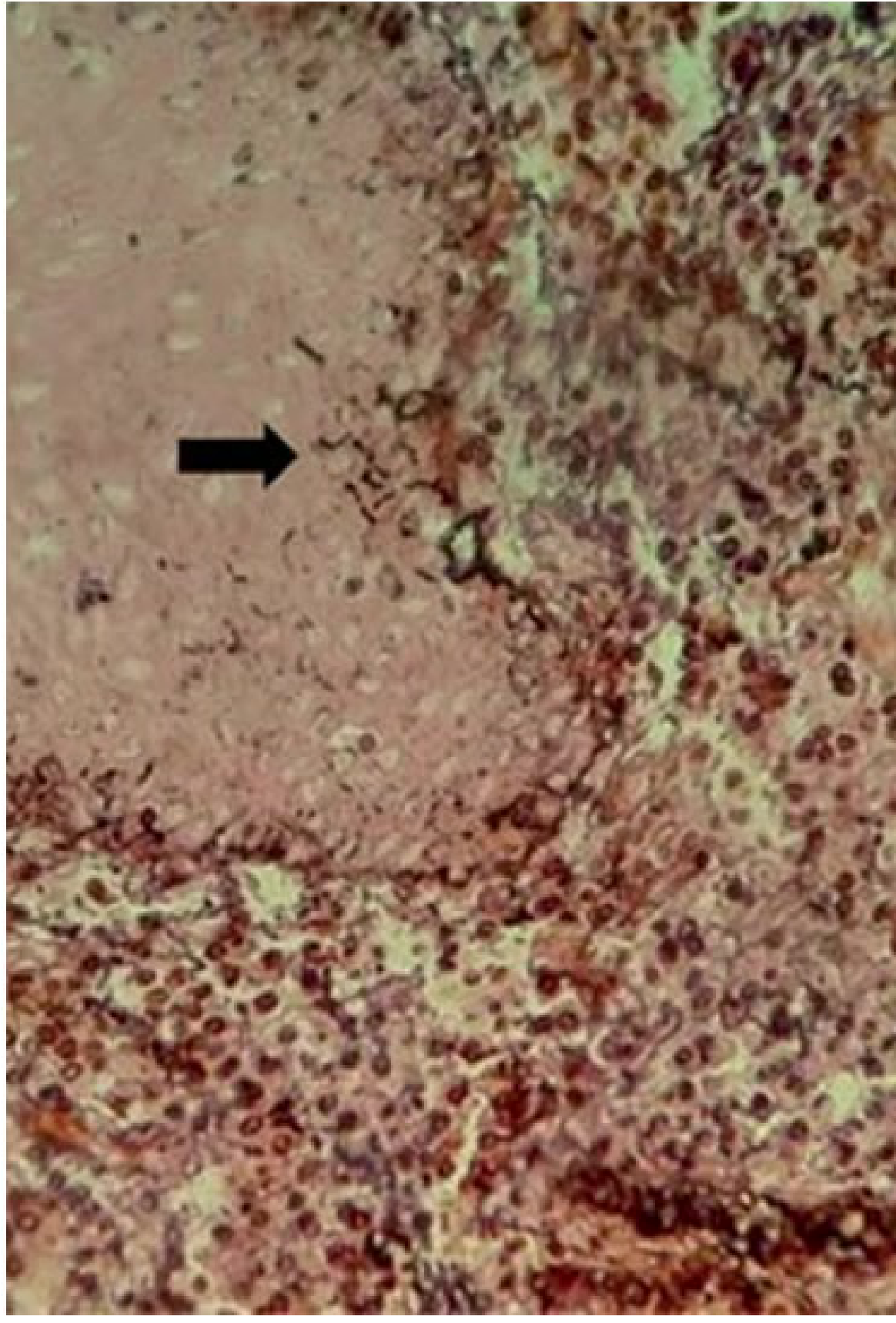
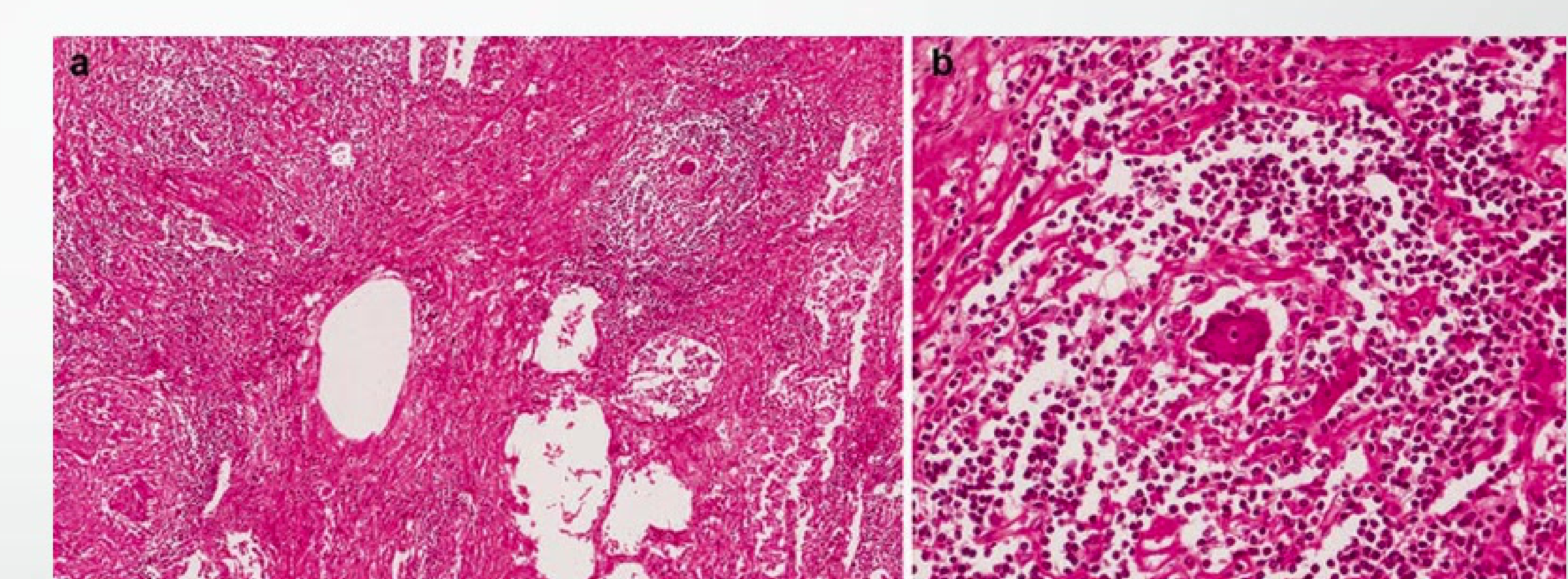
Histopathology
Histopathological Features
- Granuloma Structure:
- Central area of caseous (cheese-like) necrosis.
- Presence of epithelioid macrophages and Langerhans giant cells.
- Outer zone containing lymphocytes, plasma cells, and immature macrophages.
- Peripheral fibrosis.
- Special Stains: Ziehl–Neelsen stain is used to identify the acid-fast bacilli.
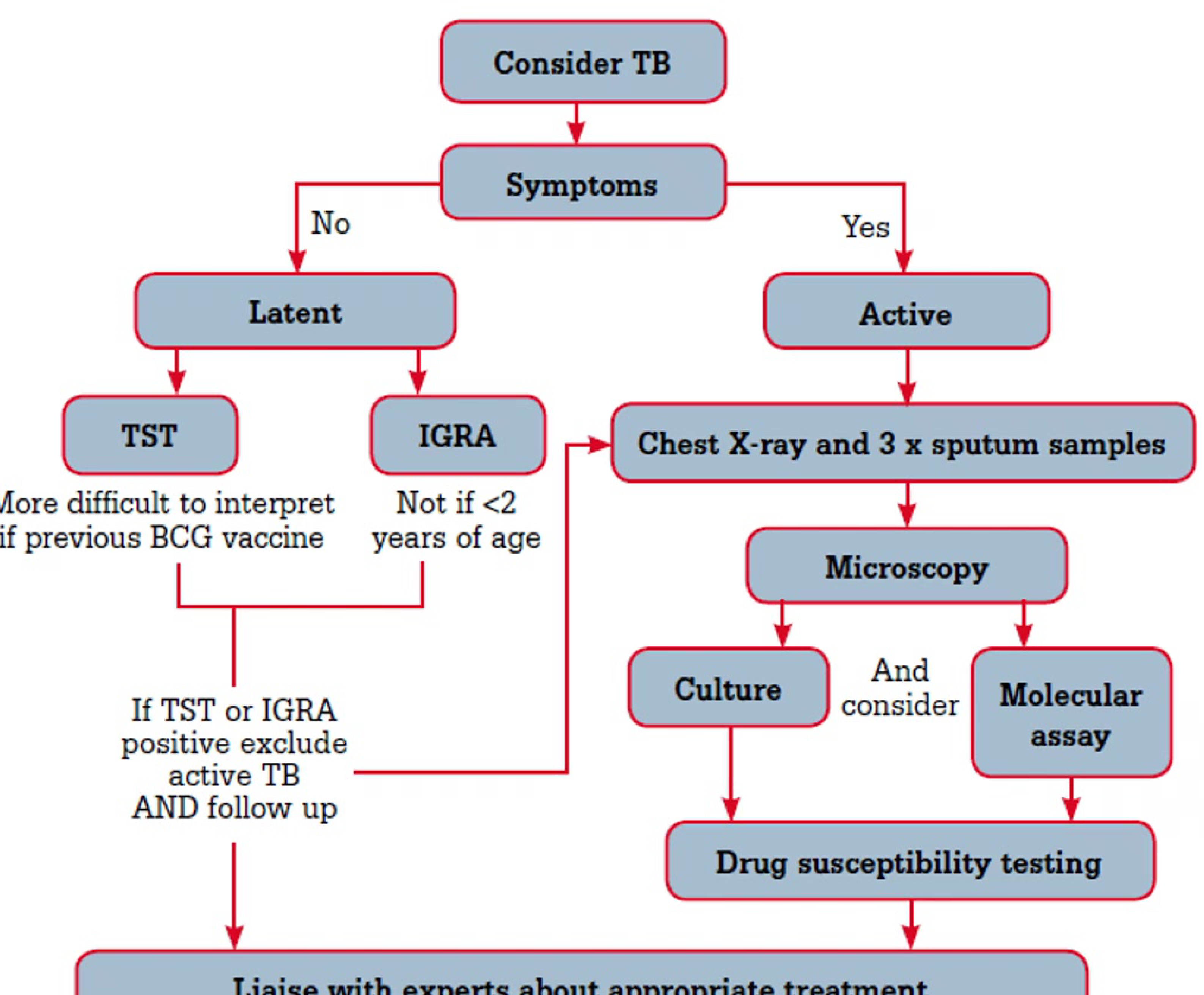
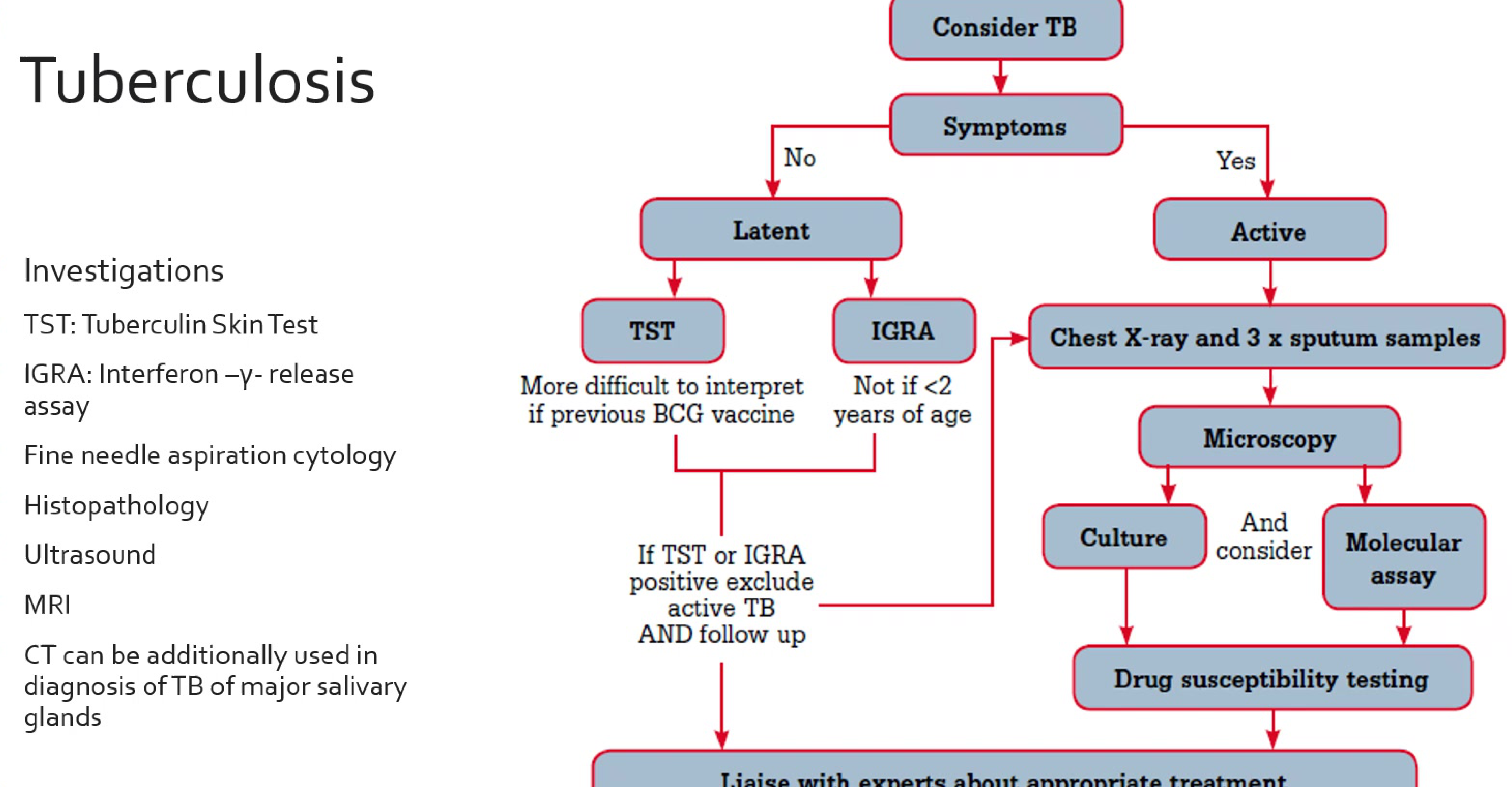
Investigations
Diagnostic Investigations
- Screening Tests:
- TST (Tuberculin Skin Test): Can be difficult to interpret if the patient had a previous BCG vaccine.
- IGRA (Interferon-gamma Release Assay): Preferred if the patient is over 2 years of age.
- Active Disease Protocol: Chest X-ray and 3x sputum samples (Microscopy, Culture, and Molecular assay).
- Culture: May take 4-8 weeks for results.
- Antimicrobial susceptibility testing important (WHO recommends line probe assays for second-line drug resistance).
- Imaging: Ultrasound, MRI, and CT (specifically for major salivary gland involvement).
- Biopsy: Fine needle aspiration cytology or formal histopathology.
- Drug Susceptibility: Essential to test for antibiotic resistance and liaise with experts for treatment.
Management
Treatment Regimen
- Antibiotic Resistance: A significant concern requiring specific susceptibility testing.
- Standard Adult Course:
- Initial Phase (2 months): Combination of isoniazid, rifampin, pyrazinamide, and ethambutol.
- Continuation Phase (4 months): Combination of isoniazid and rifampicin.
- Monitoring: Sputum specimens for acid-fast bacilli and culture should be obtained at monthly intervals to ensure clearance.
Prevention
Preventive Measures and Public Health
- Occupational Safety: Healthcare workers must follow universal infection control policies, including appropriate ventilation, aerosol control, and high-quality face masks.
- Well-recognized risk for healthcare workers (including dental).
- Infection Control: Vaccination, ventilation, filtration, air circulation control, good quality face masks.
- Regulatory: Tuberculosis is a notifiable disease.
- BCG Vaccine: Recommended in Australia for high-risk groups:
- Aboriginal and Torres Strait Islander neonates.
- Specific healthcare workers and travelers.
- Australian-born children of migrants from high-prevalence areas.
- Household contacts of individuals with leprosy.

Recap on Bacterial Infections
Review Questions24
- What are the stages of acquired syphilis?
- What are some manifestations of oral/oropharyngeal gonorrhoea?
- What tests are required if you suspect active TB?
Recap and questions for Candidiosis
- Name some predisposing factors that increase chances of candidiasis
- Are there any special considerations neded for a patient who presents with pseudomembranous candidiasis
- what investigations would you request for persistent angular cheilitis
Fungal Infections
Overview25
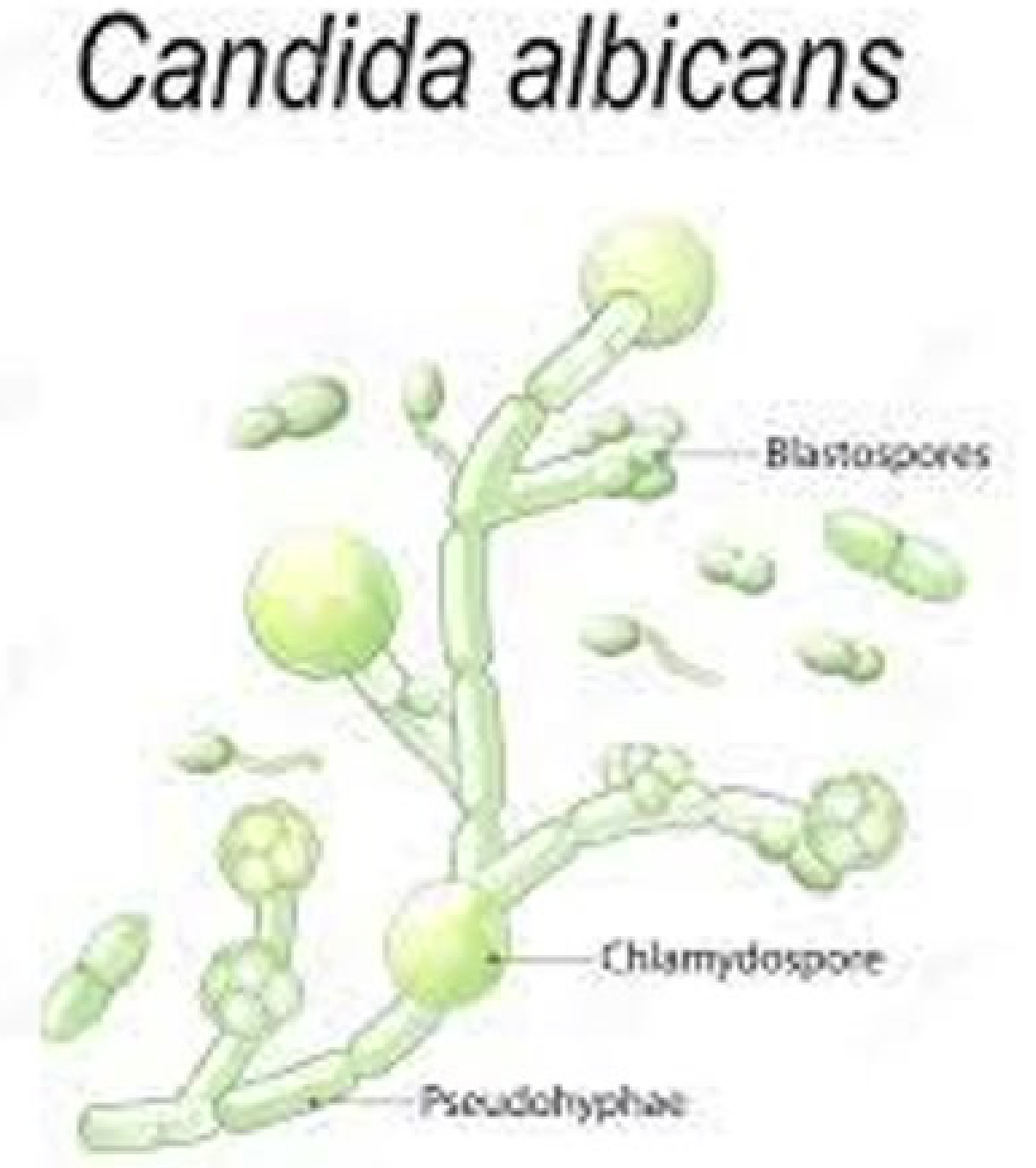
- Also known as Thrush.
- Caused by Candida albicans; an opportunistic pathogen.
- Colonizes mucocutaneous surfaces which can serve as portals of entry into deeper tissues when host defenses are compromised.
- It is a dimorphic fungus, existing in both yeast and hyphal phases.
- Host factors play a more important role than organism virulence attributes in the pathogenesis of oral candidiasis.
- Infection arises from an imbalance between fungal virulence factors and host defense.
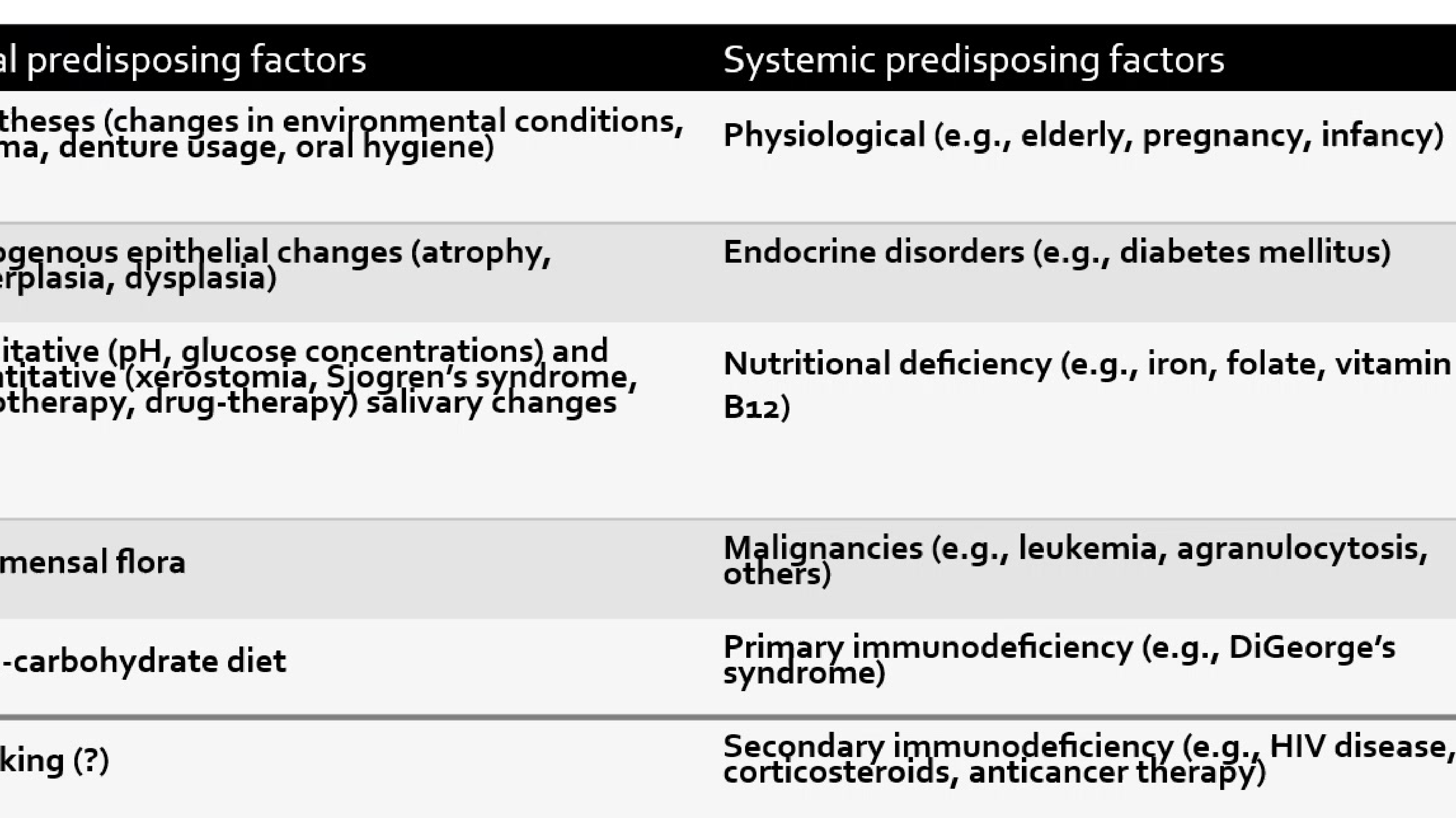
Predisposing Factors
Local Predisposing Factors
- Prostheses: Changes in environmental conditions, trauma, denture usage, and oral hygiene.
- Endogenous epithelial changes: Atrophy, hyperplasia, and dysplasia.
- Salivary changes: Qualitative (pH, glucose concentrations) and quantitative (xerostomia, Sjogren’s syndrome, radiotherapy, drug therapy) changes.
- Commensal flora: Alterations in the oral microbial balance.
- Diet: High-carbohydrate diet.
- Smoking: Potential contributing factor.
Systemic Predisposing Factors
- Physiological: Elderly, pregnancy, and infancy.
- Endocrine disorders: e.g., Diabetes mellitus.
- Nutritional deficiency: e.g., Iron, folate, and vitamin B12.
- Malignancies: e.g., Leukemia, agranulocytosis, and others.
- Primary immunodeficiency: e.g., DiGeorge’s syndrome.
- Secondary immunodeficiency: e.g., HIV disease, corticosteroids, and anticancer therapy.
Classification of Oral Candidosis
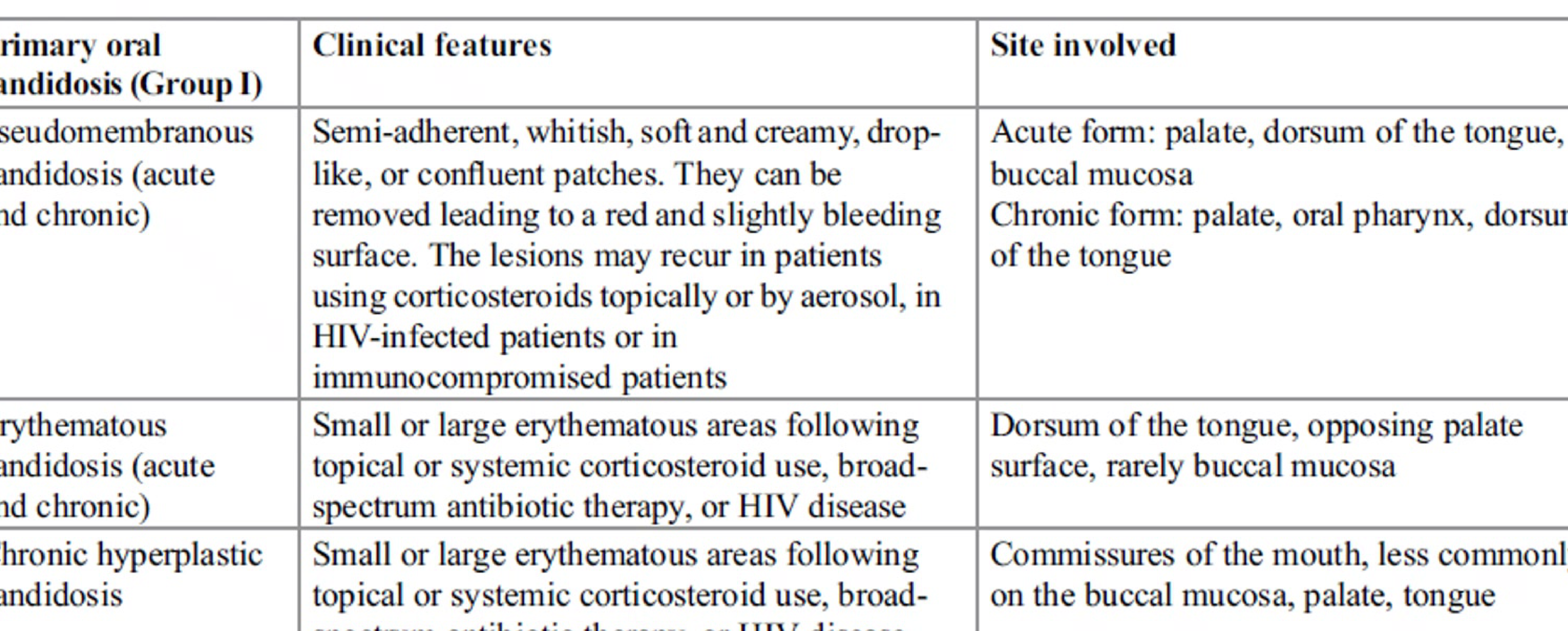
Clinical Classification (Group I: Primary Oral Candidosis)
-
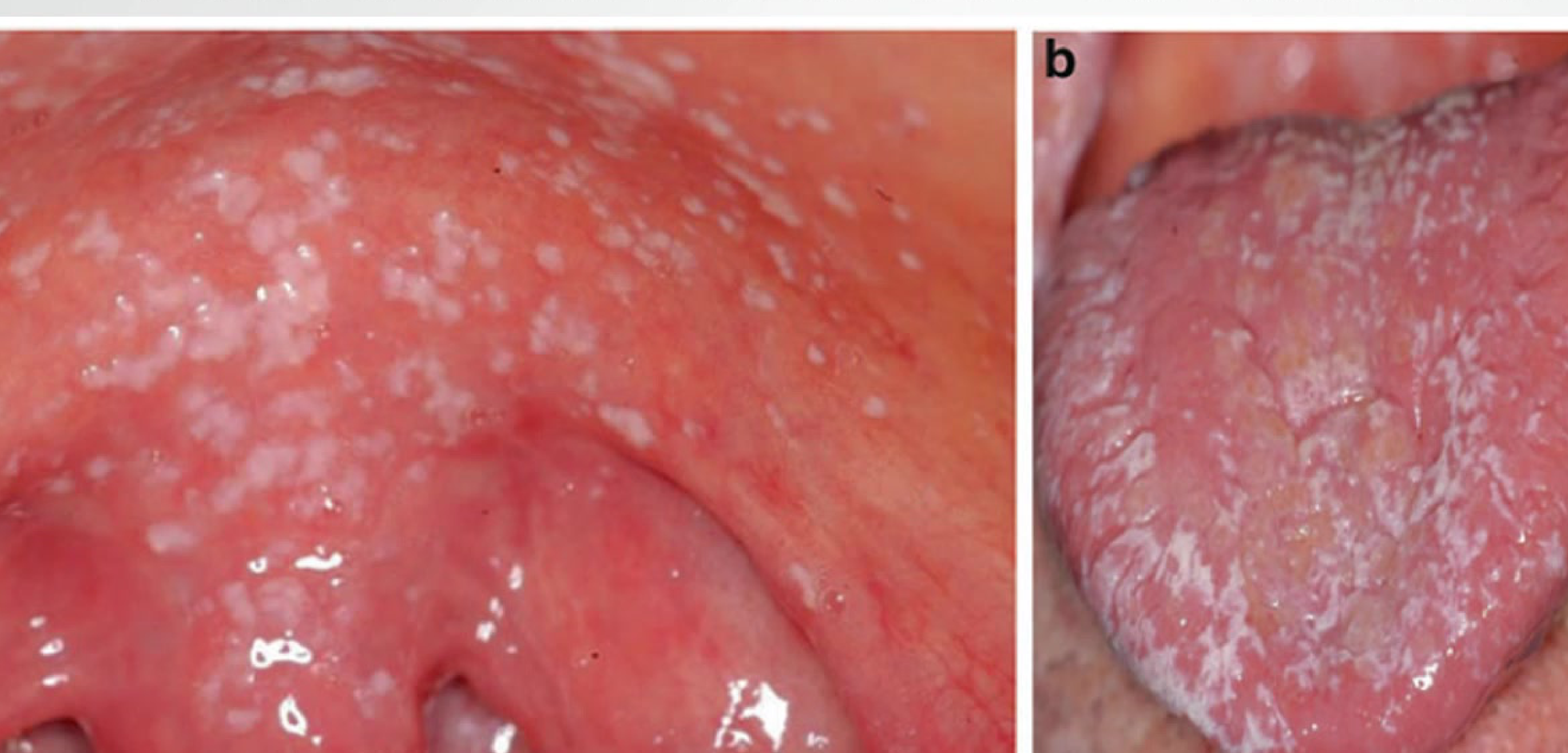
Pseudomembranous Candidosis (Acute and Chronic)
- Clinical features: Semi-adherent, whitish, soft and creamy, drop-like, or confluent patches. They can be removed, leading to a red and slightly bleeding surface. Lesions may recur in patients using topical or aerosol corticosteroids, HIV-infected patients, or immunocompromised patients.
- Demographics: Most commonly presented in patients with poor immune system function (immunocompromised)
- Presentation: Classic oral thrush with several generalized white creamy plaques that can be wiped off with gauze, revealing underlying erythema
- Site involved:
- Acute form: Palate, dorsum of the tongue, buccal mucosa.
- Chronic form: Palate, oral pharynx, dorsum of the tongue.
-
Erythematous Candidosis (Acute and Chronic)
- Clinical features: Small or large erythematous areas following topical or systemic corticosteroid use, broad-spectrum antibiotic therapy, or HIV disease.
- Site involved: Dorsum of the tongue, opposing palate surface, rarely buccal mucosa
- Pathology: Patient has more atrophy of the epithelium (lost initial layer), appearing red, erythematous, and inflamed
- Can cause erythema on hard and soft palate (Kissing Lesions via tongue transfer)
- Causes: Steroid puffers or antibiotic treatment (local change in microbiome)
- Symptoms: Quite painful. Requires antifungal therapy and correction of underlying factors.
- Presents as erythematous areas on the dorsum of the tongue.
- May occur simultaneously on the palate and tongue (referred to as “kissing lesions”).
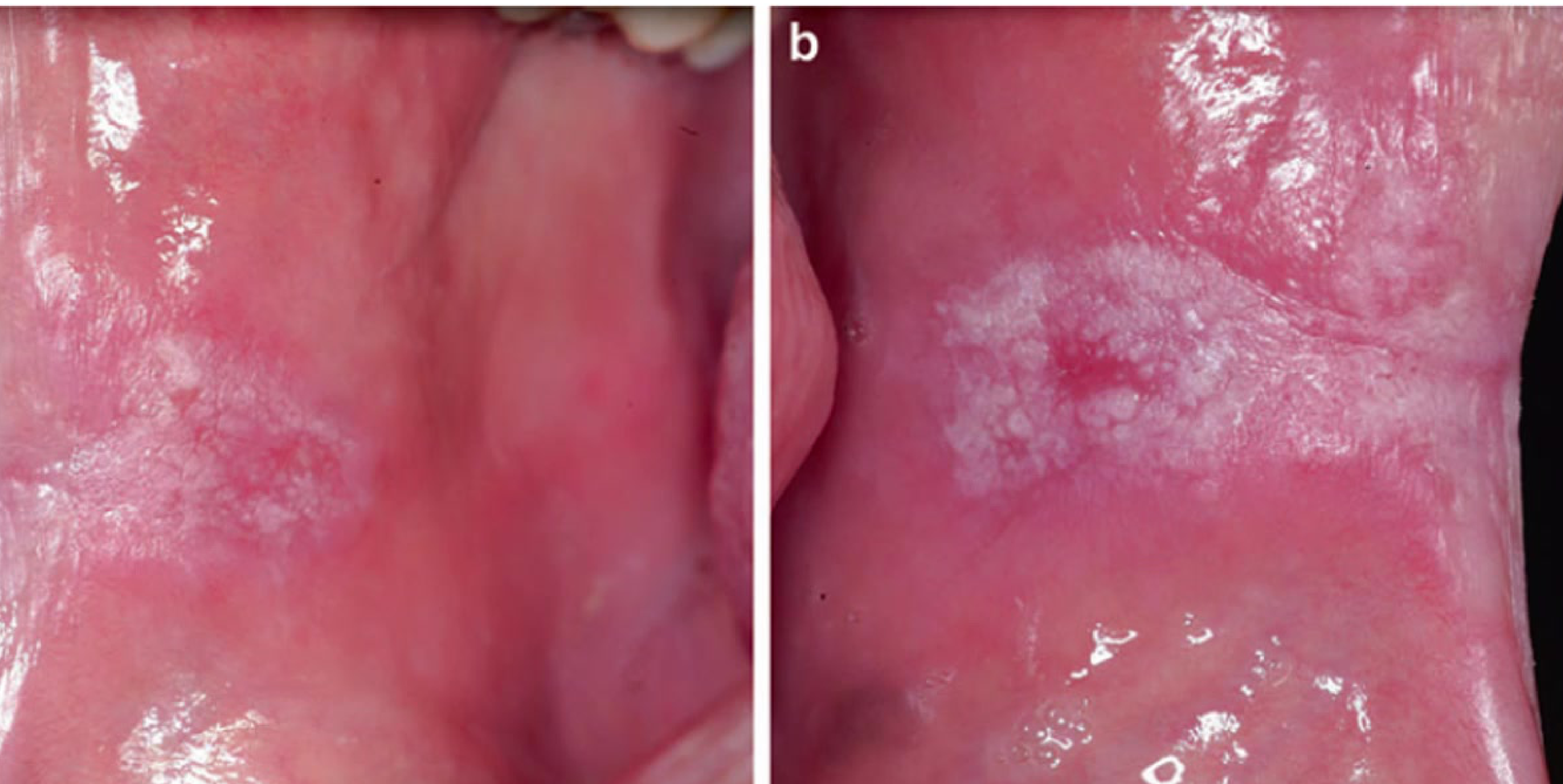
- Chronic Hyperplastic Candidosis
- Clinical features: Small or large erythematous areas following topical or systemic corticosteroid use, broad-spectrum antibiotic therapy, or HIV disease.
- Site involved: Commissures of the mouth, less commonly on the buccal mucosa, palate, tongue
- Sites: Bilateral anterior buccal commissures (symmetrical)
- Appearance: Rough, non-homogeneous white patches or plaques with underlying erythema
- Malignancy Risk: WHO does not currently consider it an oral potentially malignant disorder, but past cases reported associated dysplasia and malignancy
- Diagnosis: Biopsy required to rule out underlying dysplasia.
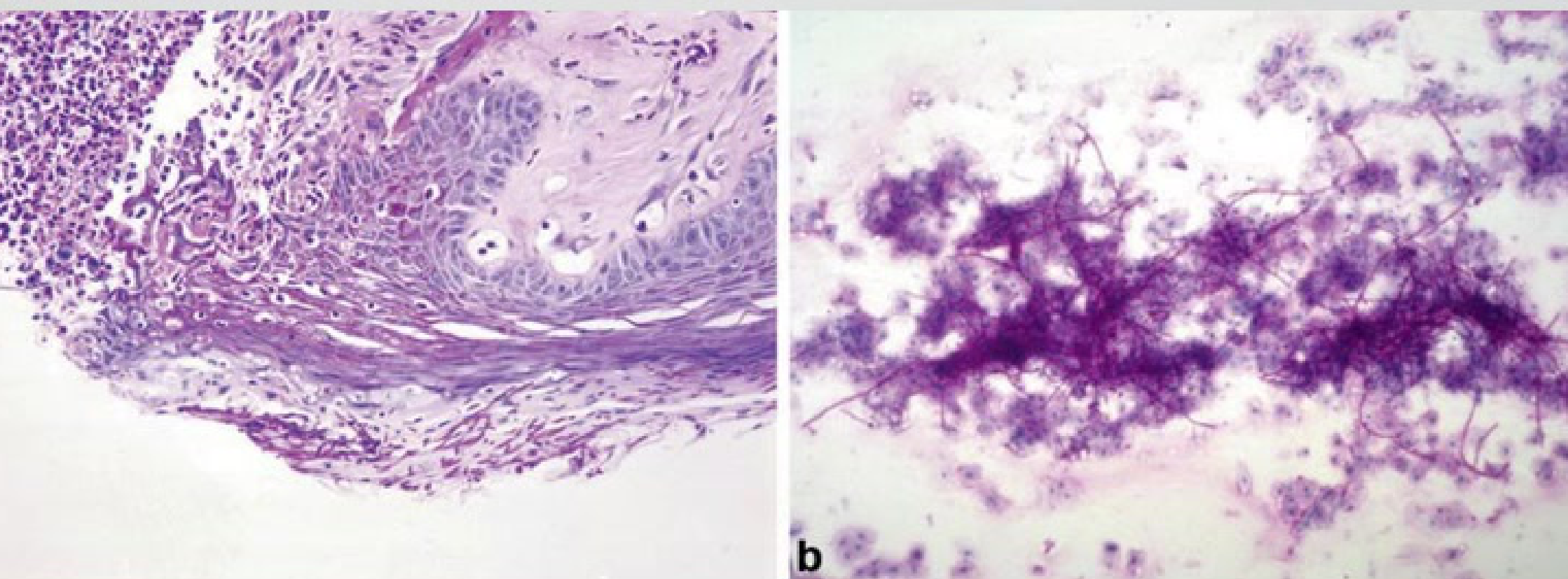
Histopathology
Microscopic Features of Pseudomembranous Candidiasis
- Hyphae penetrate the epithelium up to the spinous cell layer.
- Presence of edema.
- Micro-abscesses containing polymorphonuclear leukocytes within the outer layers of the epithelium.
- Deeper parts of the epithelium show acanthosis and inflammatory infiltrate.
Erythematous Candidiasis
Microscopic Features of Erythematous Candidiasis
- Histopathology is similar to Pseudomembranous Candidiasis.
- Pseudo-hyphae penetrate and extend to the superficial layers of the epithelium.
- Inflammatory reaction is observed in both the epithelium and connective tissue.


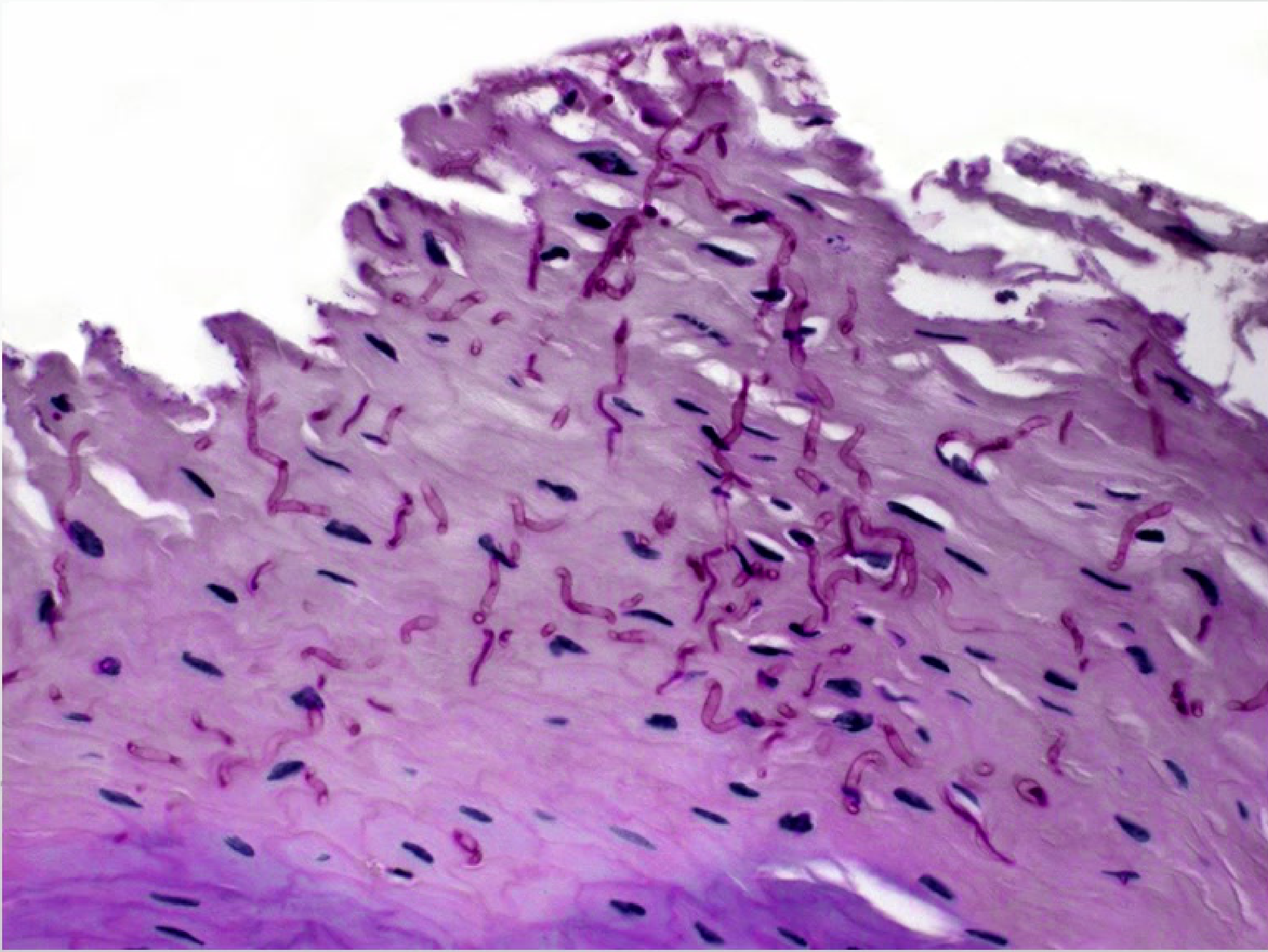
Chronic Hyperplastic Candidiasis
Microscopic Features of Chronic Hyperplastic Candidiasis
- Parakeratosis: Presence of nuclei in the stratum corneum.
- Hyperplastic epithelium: Increased thickness of the epithelial layer.
- Inflammatory infiltrate: Presence of inflammatory cells in the tissue.
- Candida hyphae invasion: Fungal hyphae penetrate the upper layers of the epithelium.
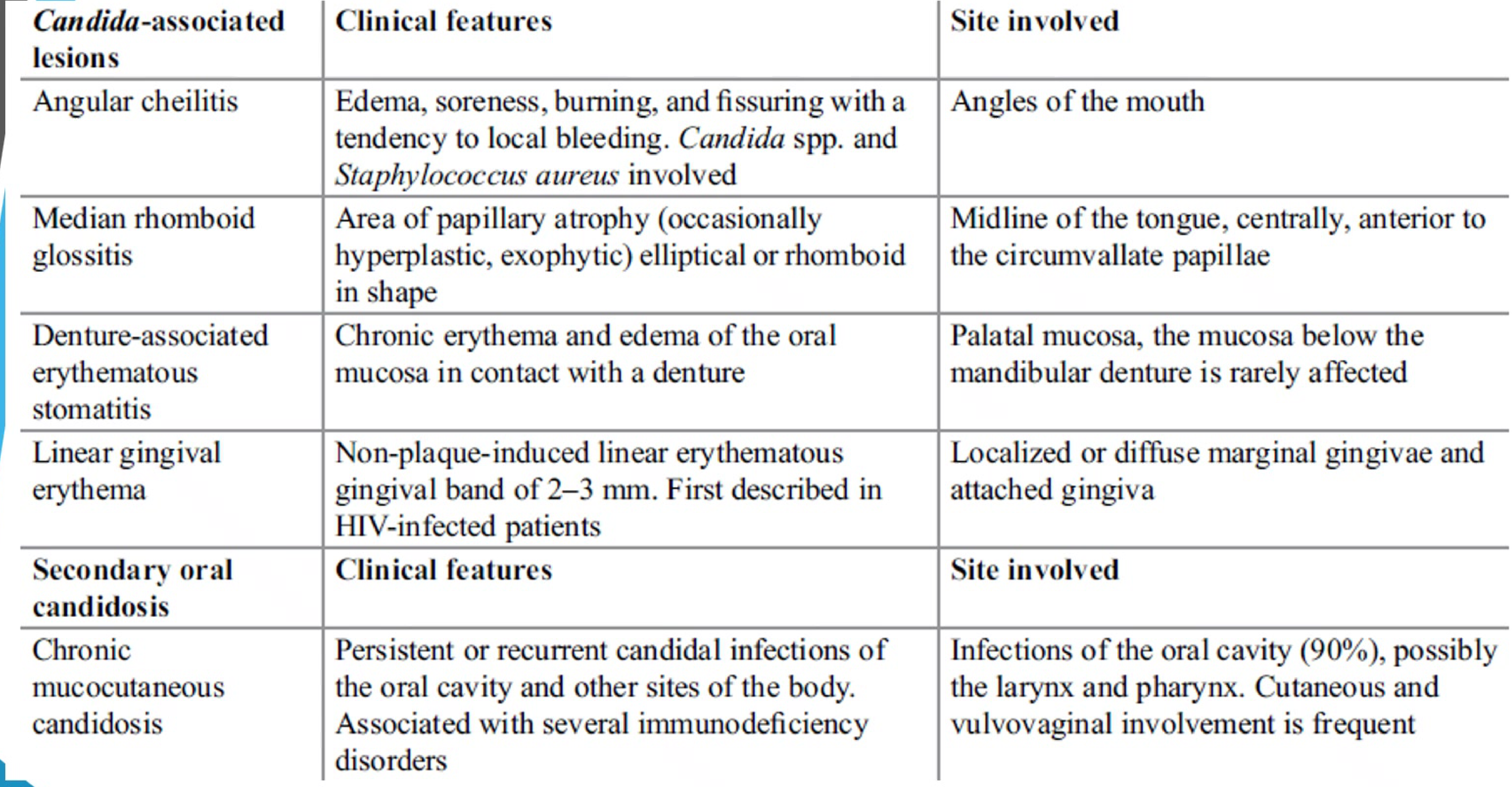
Candida-Associated Lesions
- Angular Cheilitis
- Clinical features: Edema, soreness, burning, and fissuring with a tendency to local bleeding. Involves Candida spp. and Staphylococcus aureus.
- Site: Angles of the mouth
Case Study: Angular Cheilitis
- Presentation: Classic clinical photo of a patient with angular cheilitis
- Observations: Fissuring and inflammation at the corners of the mouth
- Significance: Indicates need to investigate for underlying contributing factors like anaemia or immune issues

-
Predisposing Factors: Anaemia, Vitamin B12 deficiencies, impaired immunities, hyposalivation. Often associated with intraoral candidosis
-
Management: Investigate underlying factors (anaemia, haematinics). Treat angles of lips and intraorally.
-
Median Rhomboid Glossitis
- Clinical features: Area of papillary atrophy (occasionally hyperplastic or exophytic) elliptical or rhomboid in shape.
- Site: Midline of the tongue, centrally, anterior to the circumvallate papillae.

-
Denture-Associated Erythematous Stomatitis
- Clinical features: Chronic erythema and edema of the oral mucosa in contact with a denture.
- Site: Palatal mucosa; the mucosa below the mandibular denture is rarely affected
Case Study: Denture Associated Erythematous Stomatitis
- Presentation: Chronic erythema and oedema of oral mucosa in contact with the denture
- Classification:
- Localized inflammation or pinpoint hyperemia
- Diffuse erythema (part or entire denture covered mucosa)
- Inflammatory Papillary Hyperplasia: Granular or papillary type inflammation involving central hard palate and alveolar ridges
- Management: Denture hygiene is critical (avoid nocturnal use, clean/dry environment, mechanical cleaning, disinfecting)


.
- Linear Gingival Erythema
- Clinical features: Non-plaque-induced linear erythematous gingival band of 2–3 mm. First described in HIV-infected patients.
- Site: Localized or diffuse marginal gingivae and attached gingiva
- Association: Often associated with underlying HIV infected patients (prevalence 2-38%), but can occur in non-HIV patients
- Diagnosis: Reserved for lesions resistant to plaque removal after multiple treatments. Does not respond to scale and clean alone.

Secondary Oral Candidosis
- Chronic Mucocutaneous Candidosis
- Clinical features: Persistent or recurrent candidal infections of the oral cavity and other body sites. Associated with several immunodeficiency disorders.
- Site: Oral cavity (90%), possibly the larynx and pharynx. Cutaneous and vulvovaginal involvement is frequent.
Investigations
Diagnostic Procedures for Oral candidiasis
- Several clinical and laboratory techniques are used to confirm a provisional diagnosis.
- Cytology Smear: Presence of Candida hyphae confirmed with Periodic Acid-Schiff (PAS) staining of a pseudomembrane smear.
- Cultures: Swabs taken from mucosal tissues and the under-surface of dentures are useful, particularly in erythematous candidosis.
- Quantitative Determination: Fungal burden acts as a marker of infection.
- Infected individuals typically show counts ranging from 4,000 to 20,000 CFU/ml.
- Hematologic Investigations: Performed to check for underlying immunosuppression or nutritional deficiencies.
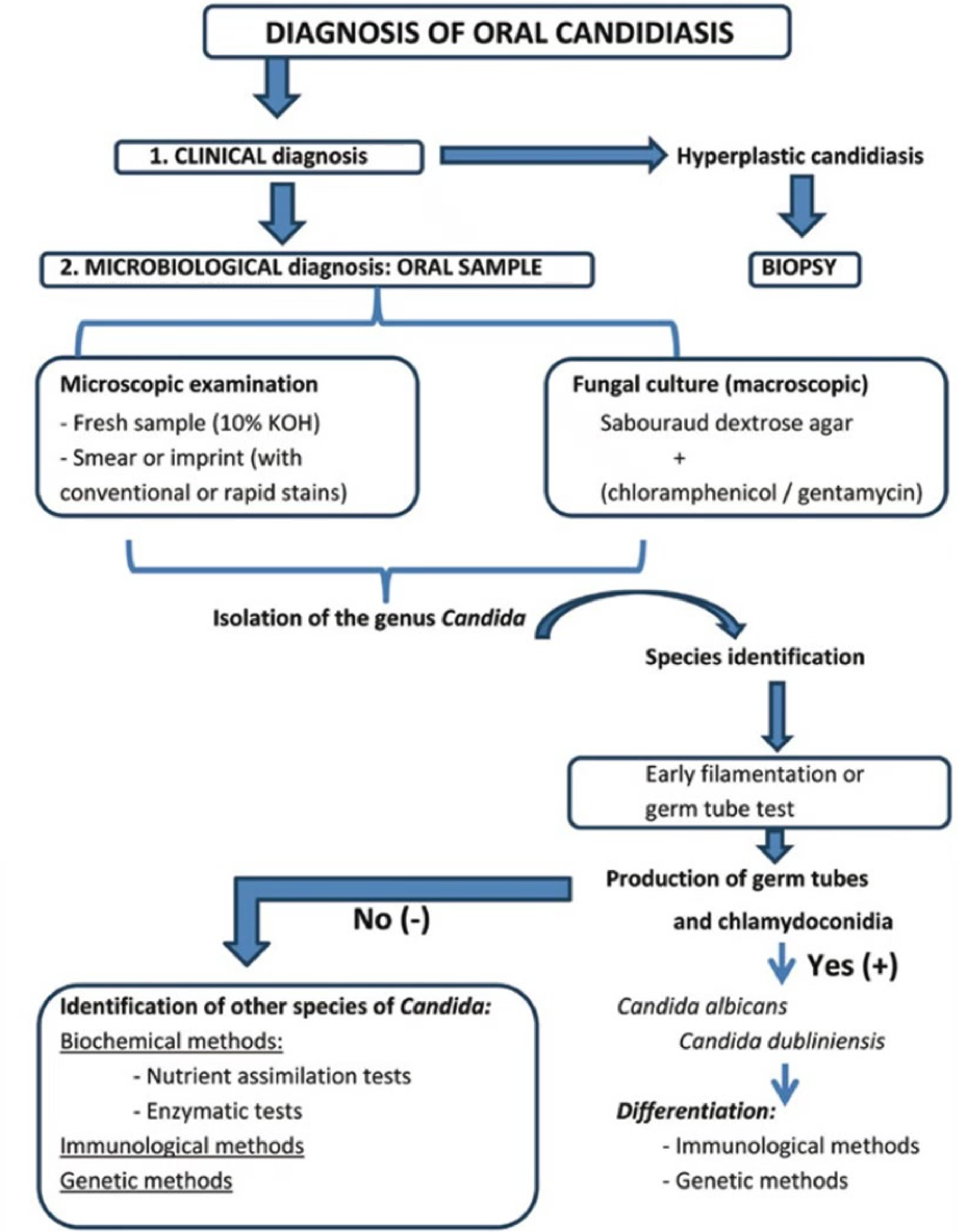
Diagnostic Flowchart for Oral Candidiasis
-
Clinical Diagnosis
- May lead directly to a diagnosis of Hyperplastic Candidiasis or require further sampling.
-
Microbiological Diagnosis
- Oral Sample / Biopsy:
- Microscopic Examination: Fresh sample (10% KOH) or Smear/Imprint (conventional or rapid stains).
- Fungal Culture: Sabouraud dextrose agar (with chloramphenicol/gentamycin).
- Oral Sample / Biopsy:
-
**Species Identification
- Species Differentiation: Immunohistochemical techniques (mainly for immunocompromised or treatment failure). Germ tube testing, genetic/biochemical methods
- Biopsy: Required for suspected hypoplastic candidiasis to rule out dysplasia**
- Isolation of the genus Candida.
- Germ Tube Test:
- Positive (+): Candida albicans or Candida dubliniensis (Differentiated via immunological or genetic methods).
- Negative (-): Identification of other Candida species using:
- Biochemical methods (Nutrient assimilation or enzymatic tests).
- Immunological methods.
- Genetic methods.
Management
Therapeutic Approach
- Identify and Correct Factors: Address underlying predisposing factors, such as anemia.
- Pharmacologic Treatment: Choice of agent is determined by the patient’s immunological status.
- Polyenes: Nystatin, Amphotericin B
- Nystatin: Used if drug interactions prevent others.
- Azoles: Miconazole, Clotrimazole, Ketoconazole, Itraconazole, Fluconazole.
- Echinocandins: Caspofungin, Micafungin, Anidulafungin.
- Polyenes: Nystatin, Amphotericin B
- Adjunctive Therapy: Use of chlorhexidine.
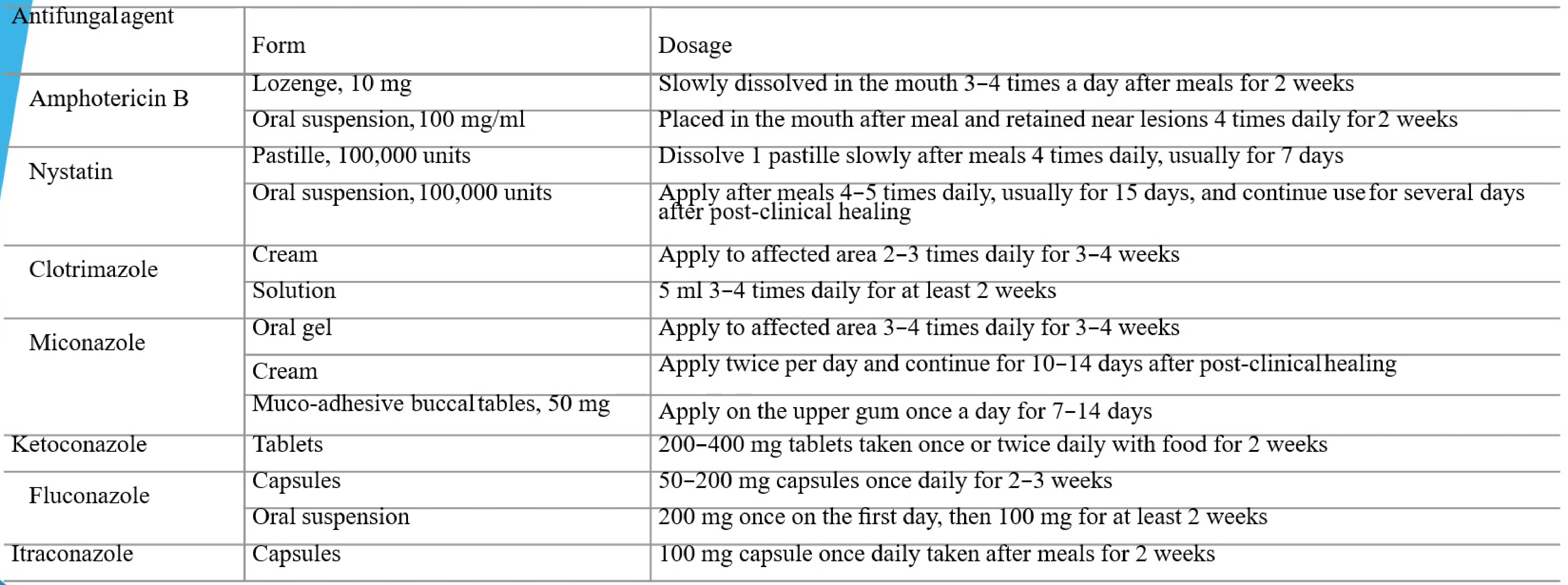
Antifungal Dosage and Administration
| Antifungal Agent | Form | Dosage |
|---|---|---|
| Amphotericin B | Lozenge (10 mg) | Dissolve slowly 3-4 times daily after meals for 2 weeks. |
| Oral suspension (100 mg/ml) | Retain in mouth near lesions 4 times daily after meals for 2 weeks. | |
| Nystatin | Pastille (100,000 units) | Dissolve 1 pastille slowly 4 times daily after meals for 7 days. |
| Oral suspension (100,000 units) | Apply 4-5 times daily after meals for 15 days; continue for several days after healing. | |
| Clotrimazole | Cream | Apply to affected area 2-3 times daily for 3-4 weeks. |
| Solution | 5 ml 3-4 times daily for at least 2 weeks. | |
| Miconazole | Oral gel | Apply to affected area 3-4 times daily for 3-4 weeks. |
| Cream | Apply twice daily; continue for 10-14 days after clinical healing. | |
| Muco-adhesive buccal tablets (50 mg) | Apply to upper gum once daily for 7-14 days. | |
| Ketoconazole | Tablets | 200-400 mg once or twice daily with food for 2 weeks. |
| Fluconazole | Capsules | 50-200 mg once daily for 2-3 weeks. |
| Oral suspension | 200 mg on day one, then 100 mg for at least 2 weeks. | |
| Itraconazole | Capsules | 100 mg once daily after meals for 2 weeks. |
Note: Always check for drug interactions.
Drug Interactions
- Miconazole interacts with Warfarin and Statins (contraindicated)
- Use Amphotericin B or Nystatin instead if patient is on these medications
Denture Care and Hygiene
- Avoid nocturnal (overnight) use of dentures.
- Clean dentures and keep them in a DRY environment when not in use.
- Mechanical Cleaning: Use a soft toothbrush and soap twice daily to remove biofilm from denture material.
- Disinfection: Soak twice weekly in:
- White vinegar (diluted 1:20)
- 0.1% Hypochlorite (diluted 1:10)
- Chlorhexidine
- Topical Application: If appropriate, apply miconazole gel to the denture-bearing surface 4 times daily for 4 weeks.
Footnotes
-
Original PDF page 1: L5 Bacterial, Fungal and Viral Infections slides, p.1 ↩
-
Original PDF page 2: L5 Bacterial, Fungal and Viral Infections slides, p.2 ↩
-
Original PDF page 4: L5 Bacterial, Fungal and Viral Infections slides, p.4 ↩
-
Original PDF page 5: L5 Bacterial, Fungal and Viral Infections slides, p.5 ↩
-
Original PDF page 7: L5 Bacterial, Fungal and Viral Infections slides, p.7 ↩
-
Original PDF page 8: L5 Bacterial, Fungal and Viral Infections slides, p.8 ↩
-
Original PDF page 10: L5 Bacterial, Fungal and Viral Infections slides, p.10 ↩
-
Original PDF page 12: L5 Bacterial, Fungal and Viral Infections slides, p.12 ↩
-
Original PDF page 13: L5 Bacterial, Fungal and Viral Infections slides, p.13 ↩
-
Original PDF page 14: L5 Bacterial, Fungal and Viral Infections slides, p.14 ↩
-
Original PDF page 15: L5 Bacterial, Fungal and Viral Infections slides, p.15 ↩
-
Original PDF page 17: L5 Bacterial, Fungal and Viral Infections slides, p.17 ↩
-
Original PDF page 16: L5 Bacterial, Fungal and Viral Infections slides, p.16 ↩
-
Original PDF page 18: L5 Bacterial, Fungal and Viral Infections slides, p.18 ↩
-
Original PDF page 20: L5 Bacterial, Fungal and Viral Infections slides, p.20 ↩
-
Original PDF page 21: L5 Bacterial, Fungal and Viral Infections slides, p.21 ↩
-
Original PDF page 22: L5 Bacterial, Fungal and Viral Infections slides, p.22 ↩
-
Original PDF page 23: L5 Bacterial, Fungal and Viral Infections slides, p.23 ↩
-
Original PDF page 24: L5 Bacterial, Fungal and Viral Infections slides, p.24 ↩
-
Original PDF page 25: L5 Bacterial, Fungal and Viral Infections slides, p.25 ↩
-
Original PDF page 26: L5 Bacterial, Fungal and Viral Infections slides, p.26 ↩
-
Original PDF page 36: L5 Bacterial, Fungal and Viral Infections slides, p.36 ↩
-
Original PDF page 40: L5 Bacterial, Fungal and Viral Infections slides, p.40 ↩
-
Original PDF page 47: L5 Bacterial, Fungal and Viral Infections slides, p.47 ↩
-
Original PDF page 48: L5 Bacterial, Fungal and Viral Infections slides, p.48 ↩