Clinical Case Study: Kennedy Class IV Restorative Treatment Intraoral and Extraoral Observations1
 |  |
Clinical Presentation and Visual Analysis
Patient History and Case Description
A 68-year-old male presented for a routine appointment. His primary complaint was an inability to chew effectively, and he requested information regarding restorative treatment options. The patient noted that his last dental visit was “a long time ago.”
Medical and Social History
- Medical Conditions: Hypertension, hypercholesterolaemia, ischaemic heart disease, osteoarthritis, and skin cancers.
- Social History:
- Non-smoker for 30 years.
- Alcohol consumption: Average of 1–2 drinks per week.
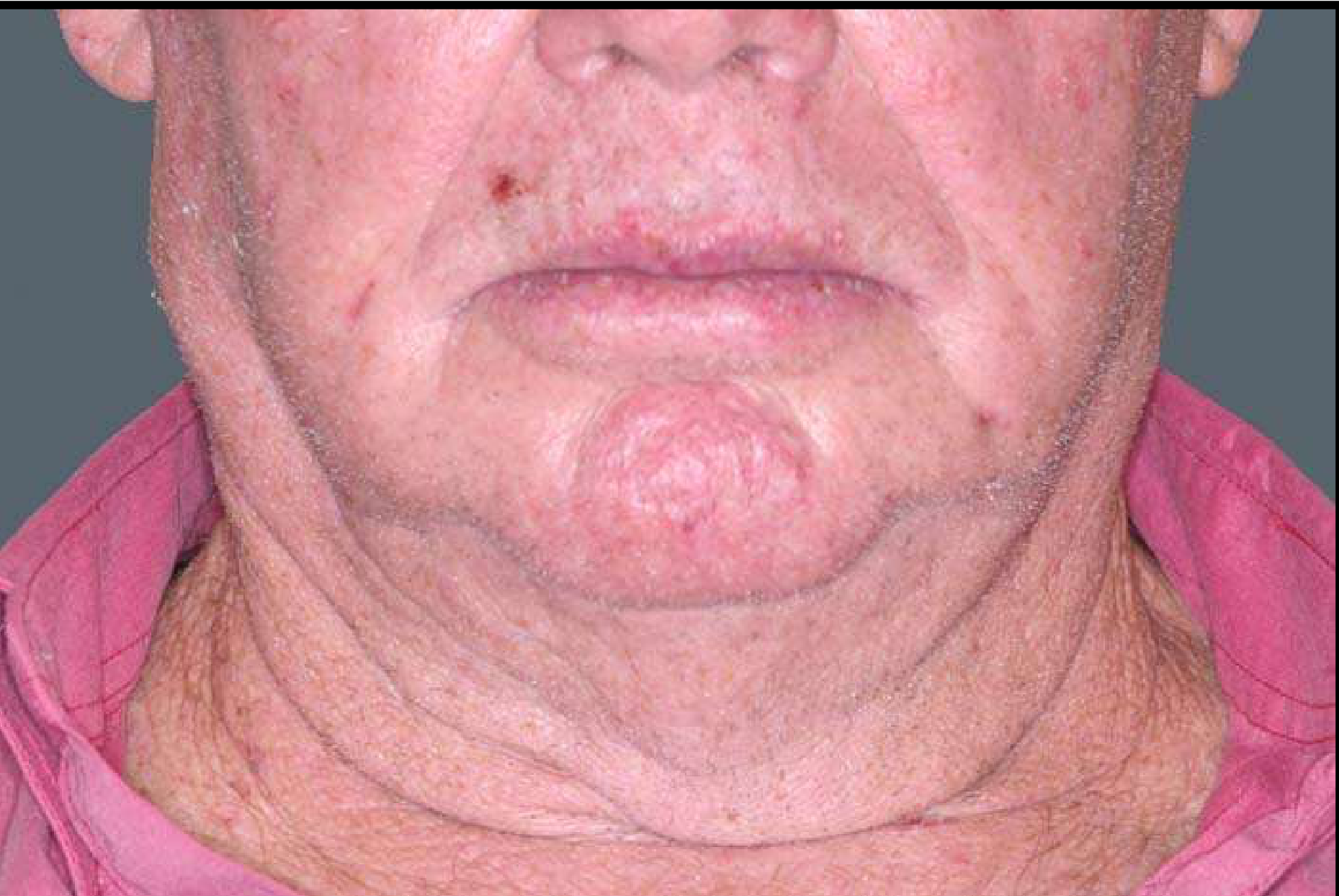
Identify the pathosis and describe the clinical features.
Extra orally
- Asymmetric lesion
- The patient presents with visible facial/neck asymmetry.
- palpate the area
- feels soft, doesn’tfeel different from other tissue
- Feels hard:
- need to know if its mobile or fixed! (Assessment is required to determine if the lump is fixed to the skin or underlying structures).
- need to know if its painful
- ==Definition: Assessment of whether the lesion is well-defined.==
- ==Sensation: Check for any changes in sensation in the affected area.==
- ==Size: A lump larger than one centimeter is a clinical concern.==
What is the differential diagnosis?
Lump/Asymmetry Extra orally
- Lipoma (if soft lump) — typically expected to feel like a soft lump.
- Lymphoadenopathy
- looking for source of infection
- lymph nodes up to 1 cm shouldn’t be worried about , afterwards its likely to be reactive
- ==Reactive Lymph Node: Often associated with a source of infection; typically a concern if larger than 1cm.==
- Metastatic deposit in the lymph node
- ==Neoplastic Deposit: A metastatic deposit within the lymph node (nodes can enlarge due to infection or malignancy).==
- ==Parotid Region Swelling: Potential benign swellings or tumors related to the parotid gland.==
- ==Cysts: Including dermoid cysts.==
- ==Cellulitis: Though less likely if the presentation is a localized hard lump without other specific inflammatory markers.==
Neck Lumps
Never ignore patients with neck lumps, particularly if they are hard
- you need to always follow up
What are the relevant clinical investigations?
Extra orla lump
- Fine needle aspiration/ biopsy
- Necessary to provide a definitive diagnosis of the tissue.
- CT of the head and the neck
- If it is a metastatic deposit we need to know where its from
- Used as a primary screening tool to look for a possible source/primary lesion. It allows for the evaluation of both bone and soft tissue and is relatively inexpensive and fast.
- Results show that its a metastatic deposit of a squamous cell carcinoma but CT doesn’t show anything?
- this is an example of an unknown primary !
- ==MRI: Better for looking at soft tissue detail compared to bone, though more expensive.==
- ==Ultrasound: Can be used to assist in diagnosis.==
Percentage of head and neck cancers with unknown primary cancer
- between 1-4% of head and neck cancers have an unknown primary
- Immune system dealt with the primary, or it lost blood supply
- in this patients case he might have had a skin cancer removed but the lesion may have spread
What is the diagnosis?
- ==Metastatic Squamous Cell Carcinoma: The biopsy confirmed a metastatic deposit of squamous cell carcinoma.==
- ==Unknown Primary: In this specific case, the primary source was not found on the scans. This occurs in 1% to 4% of head and neck cancers.==
- ==Potential reasons for unknown primary: The immune system may have dealt with the primary lesion, the primary outgrew its blood supply and disappeared, or (most likely in this case) it originated from a previously removed skin cancer that had already spread.==
How would you manage this patient?
- ==Follow-up: Never ignore neck lumps, particularly hard ones, even if they are asymptomatic.==
- ==Multidisciplinary Team (MDT): The patient should be referred to a multidisciplinary team for further management.==
Footnotes
-
Original PDF page 1: 10. Epithelial Pathosis II, p.1 ↩