Clinical Case Discussion Of Asymptomatic Oral Lesion
Patient Presentation and History1
A 48-year-old female presented with an asymptomatic oral lesion. The patient has been aware of the lesion’s presence for approximately two months.
Key Patient Factors:
- Medical History: Non-contributory.
- Social History: Non-smoker; does not consume alcohol.



Clinical Assessment And Diagnostic Activity
Clinical Assessment Activity
1. Identify the pathosis and describe the clinical features.
- ==Pathosis: The lesion is a mucocele, specifically a mucous retention cyst.==
- What can cause obstruction?
- infection, inflammation, scarring (from trauma) , sialolith, neoplasm
- ==Clinical Features:==
- ==Appearance: Described as a fluid-filled lesion.==
- ==Location: Associated with the submandibular gland duct.==
- ==Symptoms: Asymptomatic; present for approximately two months.==
- ==Palpation: Small mucoceles often feel “nice and soft” and perfectly round. Irregularity or tenderness may indicate a need for removal.==
2. What is the differential diagnosis?
- Salivary gland neoplasm
- ==Malignant Salivary Gland Tumor: Considered because the lesion is in a “high-risk area” in a female non-smoker/non-drinker.==
- ==Mucoepidermoid Carcinoma: Mentioned as a possibility where fluid retention is part of the tumor pathology.==
- SCC - could be blocking the duct
- Though the lesion does not look like a typical SCC, it is noted as a theoretical consideration for a lesion in a high-risk area.
- ==Mucous Extravasation Phenomenon: Distinguished from retention by the lack of an epithelial lining and the presence of an inflammatory response.==
3. What are the relevant clinical investigations?
- YOU DON’T NEED AN INVESTIGATION
- this looks like a mucocele and you don’t have to do imaging
- If you mucocele is small you can watch it, sometimes it can even resolve
- Most you should do is a sialogram or a CT sialogram
- ==Imaging Details:==
- ==Occlusal Radiograph: Used to look for sialoliths (salivary stones). However, its effectiveness is limited by the degree of calcification of the stone.==
- ==Sialogram / CT: A CT scan is advantageous to determine if there is a single stone or multiple stones along the duct.==
- ==Imaging Details:==
- ==Biopsy:==
- ==Incisional Biopsy: Not recommended as it may cause further injury to the duct or simply drain the fluid without providing a definitive specimen.==
- ==Excisional Biopsy: Preferred to confirm the diagnosis and ensure no other pathology is present.==
- ==Note on Palpation: While not a formal “investigation” in a lab sense, palpation for irregularity or tenderness is a key clinical assessment step.==
4. What is the diagnosis?
- mucocele in the submanddibular gland duct - the most common cause is a sialolith
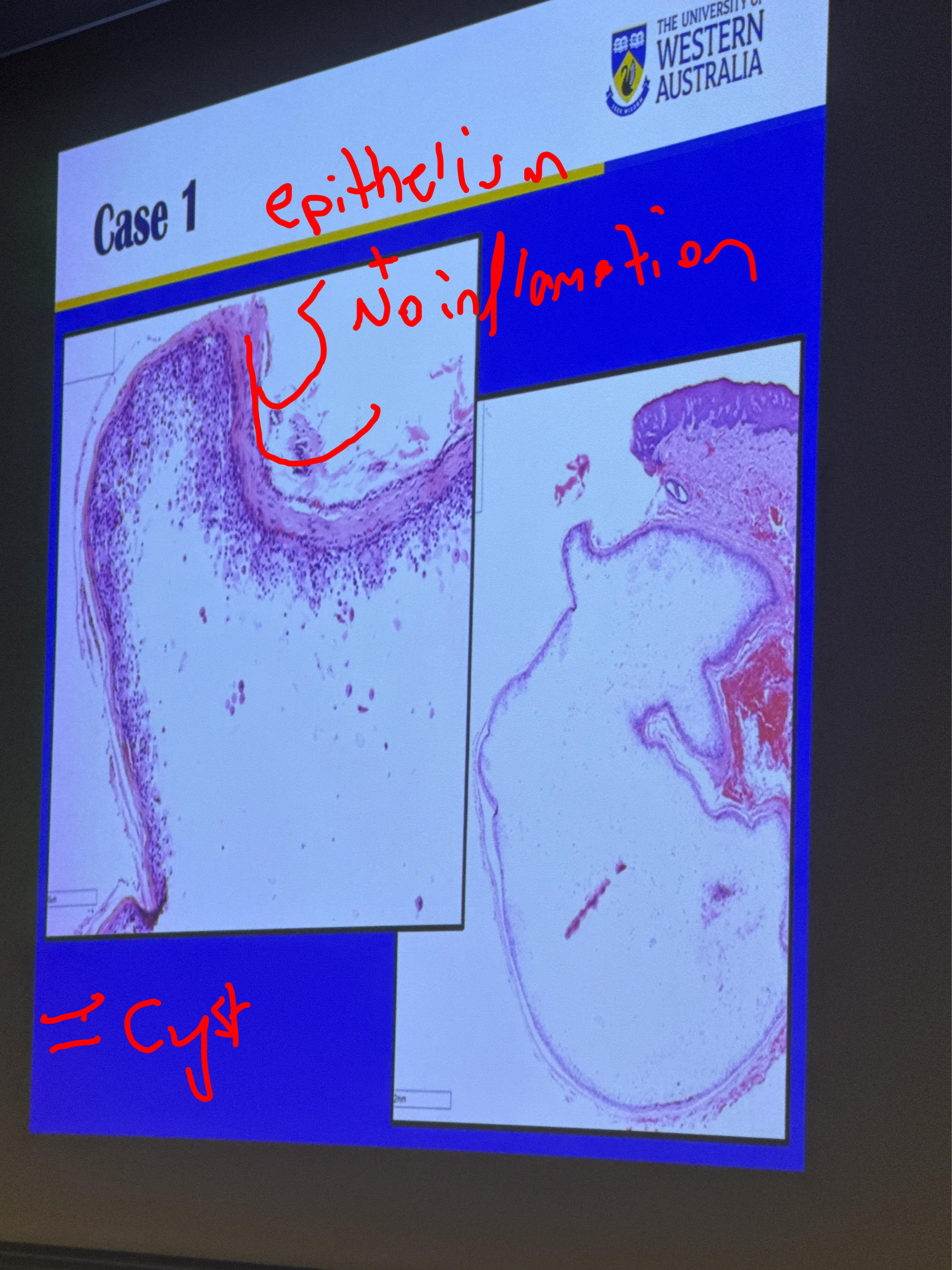
- ==Specific Diagnosis: Mucous Retention Cyst.==
- ==Histopathology:==
- ==Characterized by an epithelial-lined cavity.==
- The mucus is contained within the extended duct; there is no spillage into the surrounding connective tissue.
- ==Absence of inflammation: Unlike extravasation, there are typically no chronic inflammatory cells or macrophages in the surrounding soft tissue because the saliva (an irritant) is contained.==
- ==Etiology (Causes of Obstruction):==
- ==Mucus plugs or Sialoliths (most common).==
- ==Trauma leading to scarring or strictures.==
- ==Infection (e.g., Sialadenitis).==
- ==Compression by an adjacent neoplasm.==
5. How would you manage this patient?
- these lesions should actually be removed to make sure that there isn’t anythign else there
- ==Observation: If the mucocele is very small, soft, and asymptomatic, it can be monitored as some may resolve spontaneously.==
- ==Surgical Excision:==
- Recommended if the lesion has persisted (e.g., over two months) or if it feels irregular/tender.
- ==Risks: Patients must be warned about the risk of scarring due to ductal injury and a high recurrence rate (approximately 10%).==
- ==Recurrence Factors: High recurrence is often due to surgical scarring or the patient’s saliva having a higher mineral content.==
Extra:
- risk of recurrence is 10 percent
- due to scarring from excision
- ==Comparison of Mucocele Types:==
- ==Extravasation: Caused by severance of the duct; lacks an epithelial lining (pseudocyst); triggers an inflammatory response (macrophages) because saliva enters the connective tissue.==
- ==Retention: Caused by obstruction; possesses an epithelial lining; no inflammatory response in the surrounding tissue.==
Footnotes
-
Original PDF page 1: 13. Salivary gland disease case 1, p.1 ↩