Clinical Case Discussion Of Asymptomatic Mucosal Swelling
Patient Presentation and History1
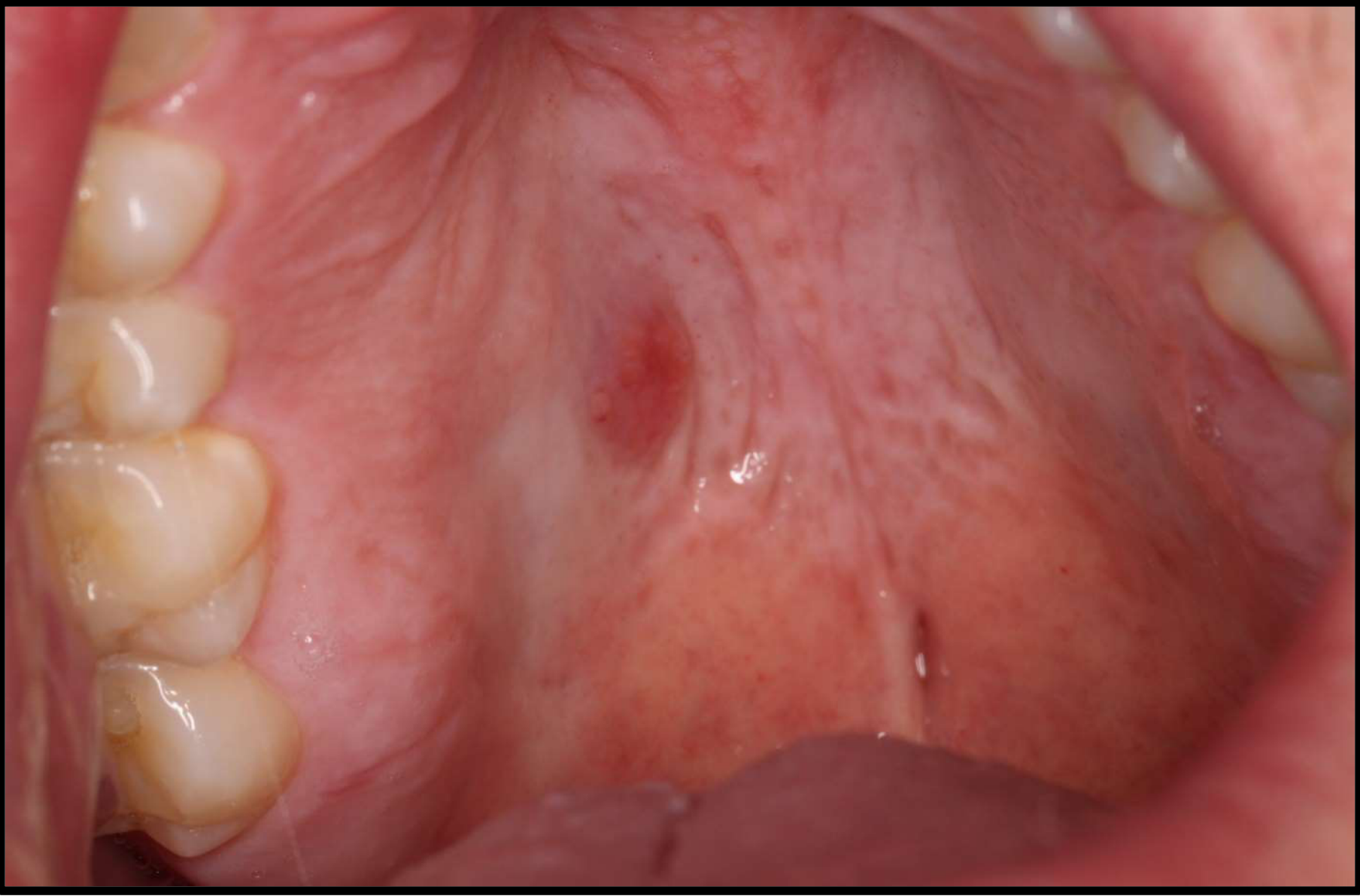
A 40-year-old male presented with an asymptomatic mucosal swelling. The patient was unaware of the lesion’s presence; it was discovered coincidentally during a routine dental examination.
- Medical History: Non-contributory.
- Social History:
- Smoker for 10 years (15 cigarettes per day).
- Consumes 2 alcoholic drinks per day.


Case Description and Patient History
Clinical Case Activity
1. Identify the pathosis and describe the clinical features.
==Identification:==
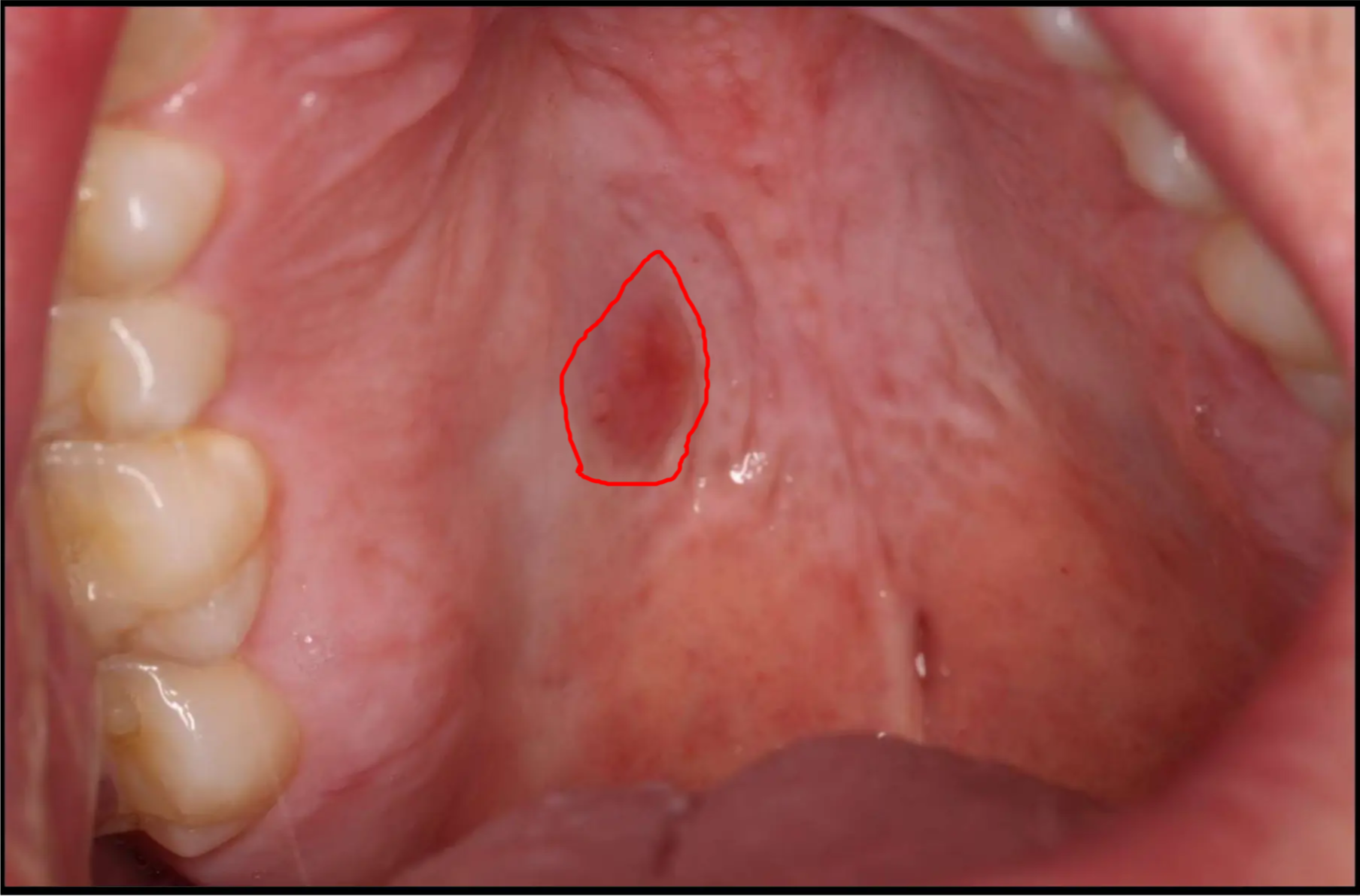
- The lesion is a red abnormality located on the palate.
- It is a solitary, asymptomatic lesion.
==Clinical Description:==
- ==Elevation: It is a raised, slightly elevated lesion (a lump).==
- ==Consistency: It is a solid lesion rather than fluid-filled.==
- ==Margins: It is well-defined.==
- ==Symptoms: The patient was unaware of it; it is asymptomatic with no ulceration.==
- ==Location Context: There are many minor salivary glands under the palatal mucosa in this area.==
2. What is the differential diagnosis?
- Salivary Gland tumour such as pleomorphic adenoma or mucoepidermal carcinoma
- Minor salivary gland tumors (e.g., Pleomorphic adenoma).
- Warthin tumor (though noted as less common in this presentation).
- Malignant salivary gland tumor (noting that these can be misleadingly well-defined and slow-growing).
- pyogenic granuloma
- Fibroepithelial polyp
- Note: Though the lesion is not pedunculated.
- Squamous cell carcinoma
- ==Vascular/Red Lesions:==
- Erythroplakia (less likely because erythroplakia is a red patch, whereas this is a raised lump).
- ==Reactive/Inflammatory Lesions:==
- Thermal burn (less likely as there is no edema or pain).
==Excluded Diagnoses:==
- ==Lichen Planus: Ruled out because lichen planus presents as reticular or “cobblestone” patterns and is not typically a raised lump.==
- ==Mucocele: Ruled out because the lesion is solid, whereas a mucocele is fluid-filled.==
3. What are the relevant clinical investigations?
most common locations for salivary gland tumours are upper lip and palate:
- we want to do an incisional biopsy because:
- a benign salivary gland tumour has a very different excision than a malignant one
- This is the preferred investigation to determine if the lesion is benign or malignant, as this dictates the surgical approach.
- histology:
- cellular pleomorphism
- hyperchromatism , dark staining
- mucin collections
- mucoepidermal tumour characteristics
- Examination for duct-like structures and cystic spaces containing mucin.
- Special staining to differentiate cell types.
- low grade:
- theres more mucin, which means its still well-differentiated
- Assessment for invasion of bone or other structures.
4. What is the diagnosis?
- ==Mucoepidermoid Carcinoma:==
- The lesion is identified as a malignant salivary gland tumor.
- ==Histological features: Presence of cystic components, epithelial cells, and mucin.==
- ==Grading: Can range from low-grade (better prognosis, more mucin) to high-grade (poor prognosis, less differentiation).==
5. How would you manage this patient?
- ==Surgery: The primary treatment is surgical excision.==
- ==Surgical Planning: The extent of the excision depends on whether the biopsy shows a benign or malignant process.==
- ==Adjunctive Therapy: Post-operative radiation may be used for more advanced cases, such as those with bone invasion or tumor spread.==
Footnotes
-
Original PDF page 1: 14. Salivary gland disease case 2, p.1 ↩