
CASE 2
CASE DISCUSSION
Case description: 66-year-old male presented for a routine dental examination. He was not aware of any oral mucosal problems, having been asymptomatic. His medical history is significant for hypertension, hypercholesterolaemia, sleep apnoea, GORD, NIDDM. He currently takes Diaformin, Norvasc, Mizart, Lorstat and Acimax. He reported smoking 30 cigarettes per day, having stared smoking at the age of 16, and reported consuming one bottle of wine per day.
Activity:
- Identify the pathosis and describe the clinical features
- What is the differential diagnosis?
- What are the relevant clinical investigations?
- What is the diagnosis?
- How would you manage this patient?
1. Identify the pathosis and describe the clinical features
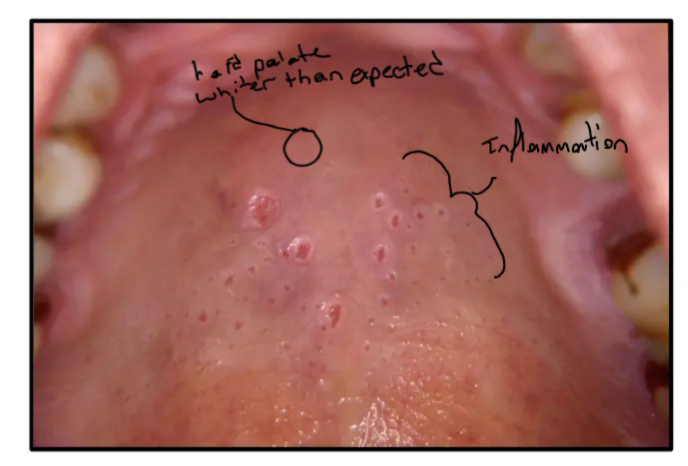
a. white palate harder than expected b. Inflammation in the hard palate
- The palate appears white/keratotic (hyperkeratosis) and may show brownish discoloration
- Multiple small, circular, raised papules with red, inflamed dots in the center
- The red dots represent the inflamed openings of the minor salivary gland ducts, not ulcers
- Pathophysiology involves metaplastic changes (metaplasia) of the ductal epithelium due to chronic heat and chemical irritation
2. What is the differential diagnosis?
White hard palate
- Smokers keratosis
Inflamed areas in hard palate
- OSCC
- Minor Salivary Gland tumors
- Thermal Injury: Chronic burn from hot foods or liquids
- Squamous Cell Carcinoma (SCC): Especially if the surface is irregular or persistent in heavy smokers/drinkers
- Note: Aphthous ulcers are ruled out as these lesions are papular and inflamed, not ulcerated
- Nicotinic Stomatitis: Primary clinical suspicion given the white background with red dots - Nicotinic Stomatitis: Primary clinical suspicion given the white background with red dots
3. What are the relevant clinical investigations?
Red inflamed lesions
- Clinical Photography: Used to document the baseline for monitoring and as an educational tool for the patient.
- Biopsy: Not initially required for classic nicotinic stomatitis. However, if a specific area looks suspicious (e.g., cauliflower appearance, persistent after smoking cessation), a biopsy is the only way to rule out SCC.
If we determine its nicotinic stomatitis that doesn’t reduce
-
Blood tests:
- Coagulation profile
- likely with this patent drinking it means the liver enzymes are going to be abnormal
- Liver Function Tests (LFTs): Relevant to assess the liver's ability to produce clotting factors and metabolize medications if surgical intervention is required.
- Coagulation profile
-
HbA1C
- the patient is a diabetic
- Diabetes is relevant due to delayed healing.
- HbA1c Tells us Glycemic control of 3 months
- Fasting Glucose: Not ideal for assessing overall control as it only provides a "snapshot" in time and can fluctuate.
- the patient is a diabetic
-
Glucose tolerance test
- We would not do this test its only used to diagnose diabetes
4. what is the diagnosis
Red inflamed lesions
- Nicotinic stomatitis
Clinical Presentation
Nicotinic Stomatitis (Smoker's Palate) is characterized by the white keratotic change of the palate with red dots representing the inflamed orifices of minor salivary gland ducts.
5. How would you manage this patient?
Nictonic Stomatitis
- If the patient stops smoking then we would expect resolution
- Patient Education: Use the oral findings as a "window" into the patient's systemic health. Explain that if the oral mucosa is showing these changes, the respiratory tract is likely also damaged, increasing risk for asthma and lung cancer.
- Monitoring/Follow-up: Re-evaluate the patient after a period of smoking cessation (e.g., 6 months).
- Referral: Provide resources for smoking cessation programs.
What if the lesions don’t resolve?
- needs further investigation, the only way is to biopsy the lesion
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.