 |  |
 |  |
Summary
- Nicotinic stomatitis (smoker’s palate) is a reactive palatal lesion caused by chronic heat exposure—most often tobacco smoke (pipe/cigar/reverse smoking), but also reported with habitual very hot beverages; heat, not nicotine, is the driver. (Source: Contemporary OM; Chem Injuries)
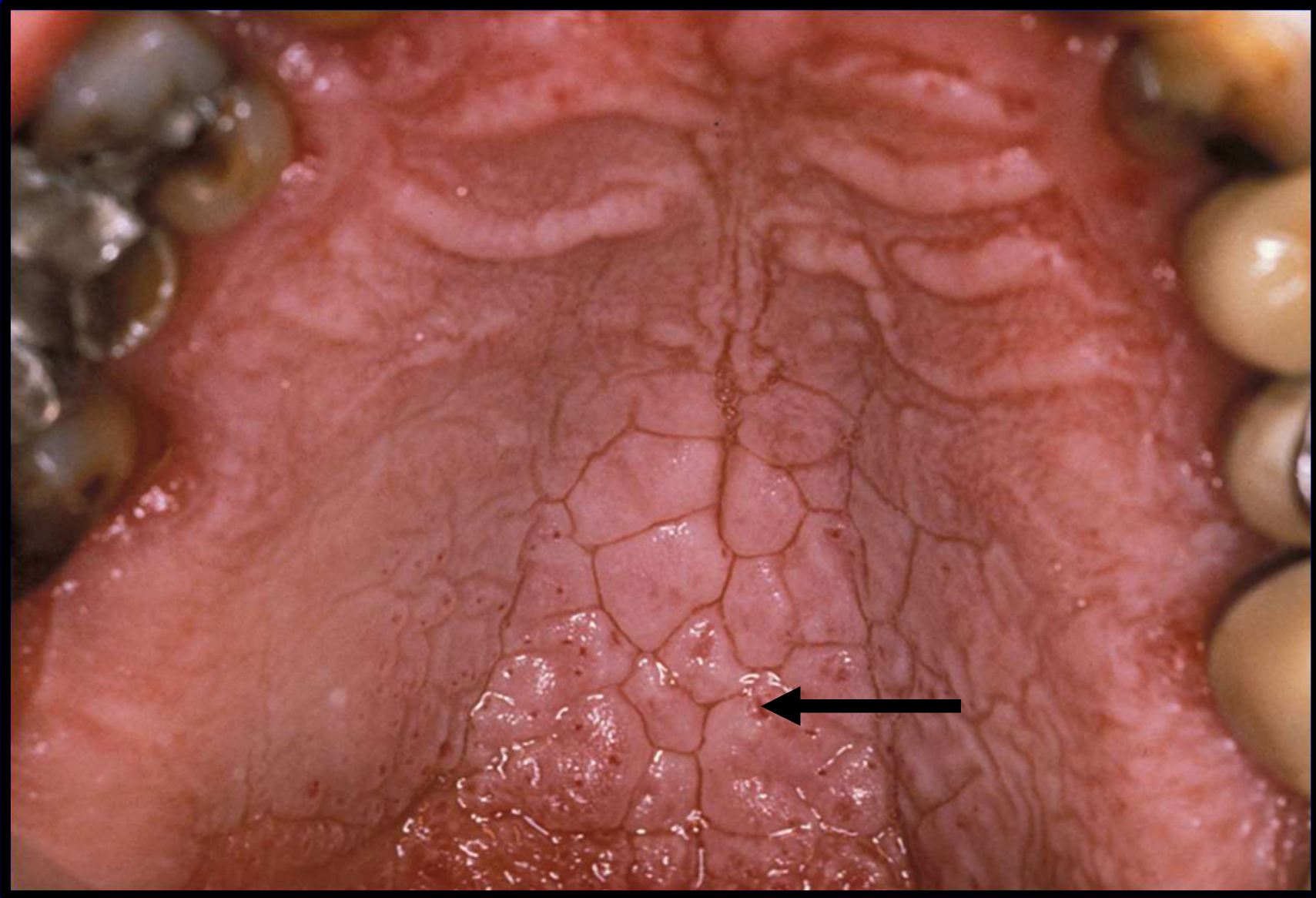
- Typical presentation is diffuse palatal hyperkeratosis/whitening with scattered red punctate papules (inflamed minor salivary duct orifices) and a cobblestone/“dried mud” surface; patients are usually asymptomatic. (Source: Contemporary OM; Chem Injuries; Source: L9 Benign Epithelial Pathosis)
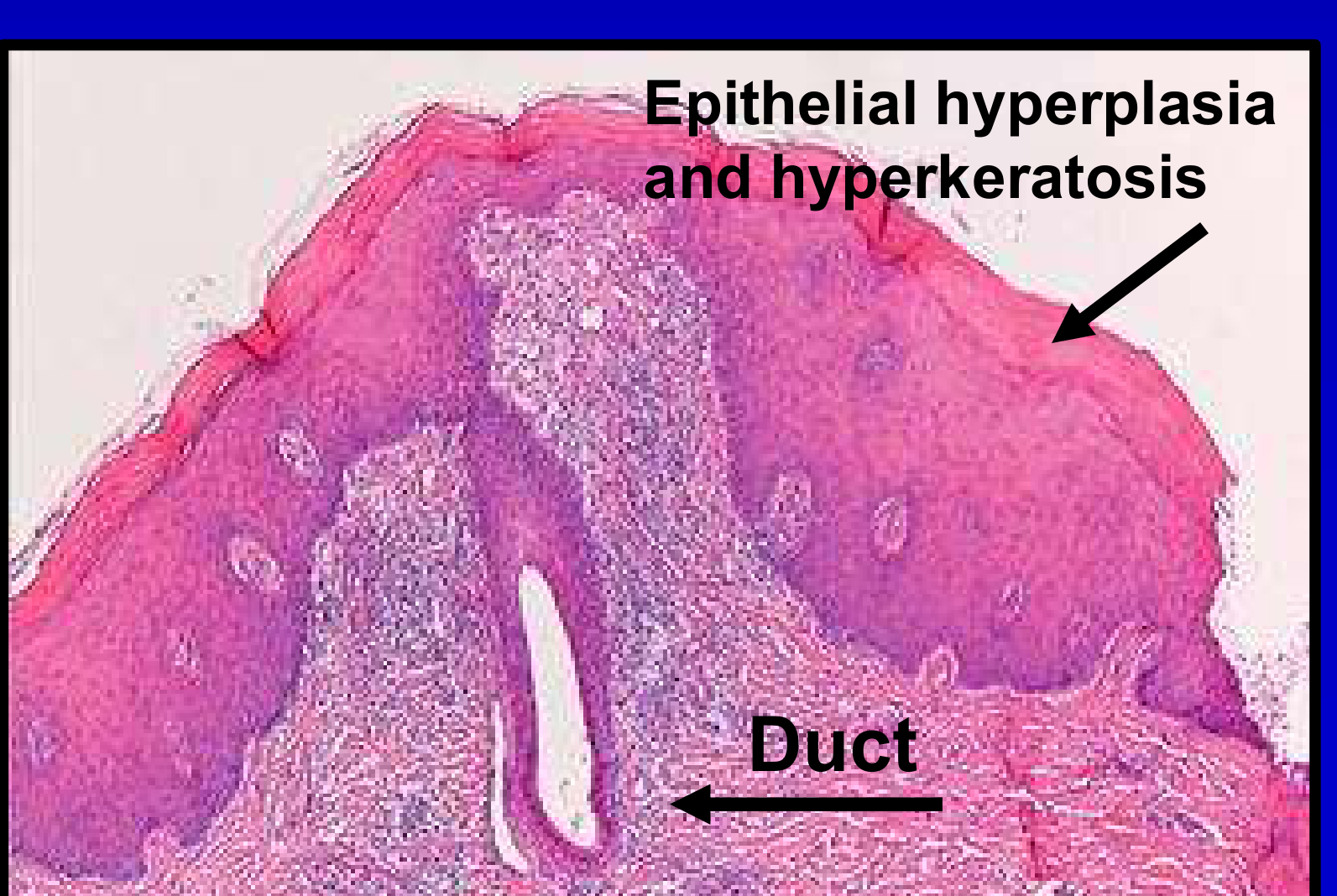
- Histology shows epithelial hyperplasia/hyperkeratosis with inflammatory squamous metaplasia of minor salivary gland ducts. (Source: L9 Benign Epithelial Pathosis)
- Lesions persist with continued smoking but regress after cessation; management centers on cessation and follow‑up. (Chem Injuries; Source: Benign Epithelial Pathosis Tutorial)
- Malignant transformation is rare, but suspicious focal raised/warty/fleshy areas or persistence after cessation require biopsy and closer follow‑up, especially in reverse smokers. (Source: L9 Benign Epithelial Pathosis; Source: Contemporary OM; Source: Benign Epithelial Pathosis Tutorial)
Etiology and Pathophysiology
- Heat injury from tobacco smoke (pipe/cigar/reverse smoking) is the primary driver; “nicotinic” is a misnomer because heat—not nicotine—is responsible. (Source: Contemporary OM; Chem Injuries)
- Chronic heat leads to palatal hyperkeratosis and thickening with inflammation of minor salivary duct orifices (red dots). (Source: Contemporary OM; Chem Injuries; Source: L9 Benign Epithelial Pathosis)
- Progression often follows erythema → keratinization → red dots surrounded by white keratotic rings. (Source: L9 Benign Epithelial Pathosis)
- Reverse smoking produces the most severe form of the lesion. (Source: Contemporary OM)
Contributory factors :
- Pipe, cigar, or reverse smoking. (Source: Contemporary OM)
- Chronic exposure of the palate to smoke and heat from burning tobacco products. (Chem Injuries)
- Habitual consumption of very hot beverages. (Source: Contemporary OM)
Prevalence
- Very common among smokers. (Source: L9 Benign Epithelial Pathosis)
- More common in males in the fifth decade and older; typically asymptomatic. (Source: Contemporary OM)
Histological Features
- Epithelial hyperplasia and hyperkeratosis. (Source: L9 Benign Epithelial Pathosis)
- Inflammatory squamous metaplasia of minor salivary gland excretory ducts. (Source: L9 Benign Epithelial Pathosis)
Clinical Features
Location
- Hard and soft palate. (Chem Injuries)
Appearance
- Thick white plaque/diffuse whitening of the palatal mucosa (hyperkeratosis). (Chem Injuries; Source: Contemporary OM)
- Established lesions may be fissured with a cobblestone or “dried mud” surface. (Source: Contemporary OM)
- Scattered 1–3 mm red punctate papules/dots represent inflamed minor salivary duct orifices. (Source: Contemporary OM; Chem Injuries)
- Red dots may be surrounded by white keratotic rings. (Source: L9 Benign Epithelial Pathosis)
- Usually asymptomatic. (Source: Contemporary OM)
Differential Diagnoses
- Squamous cell carcinoma (especially if irregular or persistent in heavy smokers/drinkers). (Source: Benign Epithelial Pathosis Tutorial)
- Minor salivary gland tumors. (Source: Benign Epithelial Pathosis Tutorial)
- Thermal injury (chronic burn from hot foods or liquids). (Source: Benign Epithelial Pathosis Tutorial)
Relevant Clinical Investigations
- Clinical photography to document baseline appearance for monitoring and patient education. (Source: Benign Epithelial Pathosis Tutorial)
- Biopsy is not initially required for classic cases, but is indicated for suspicious focal areas (raised/warty/fleshy or “cauliflower”-like) or persistence after smoking cessation to rule out SCC. (Source: Benign Epithelial Pathosis Tutorial; Source: Contemporary OM)
- Case‑based labs (e.g., coagulation profile/LFTs or HbA1c) may be considered when systemic comorbidities or planned procedures warrant assessment. (Source: Benign Epithelial Pathosis Tutorial)
Patient Management
- Smoking/habit cessation is primary; lesions persist with continued smoking and regress after cessation. (Chem Injuries; Source: Benign Epithelial Pathosis Tutorial)
- Patient education: use the lesion as a visible indicator of tobacco harm and provide cessation resources. (Source: L9 Benign Epithelial Pathosis; Source: Benign Epithelial Pathosis Tutorial)
- Re‑evaluate after cessation (e.g., 6 months) and monitor regularly; reverse smokers warrant closer follow‑up. (Source: Benign Epithelial Pathosis Tutorial; Source: Contemporary OM)
- Biopsy any persistent or suspicious focal change to exclude SCC. (Source: Benign Epithelial Pathosis Tutorial; Source: Contemporary OM)
- Malignant transformation is rare, but vigilance is required. (Source: L9 Benign Epithelial Pathosis)