- Physical and chemical Injuries July 11, 2025 4:39 PM
Physical and Chemical Injuries of the Oral Cavity
Cell injuries
This section serves as a review of general pathology concepts related to cell injury, which is foundational to understanding specific oral lesions.
Types of Injuries (aetiology)
- Physical (e.g., surgical trauma)
- Chemical (e.g., exposure to caustic substances)
- Thermal (e.g., burns)
- Infectious (e.g., microorganisms)
- Clinically, the patient’s chief complaint includes a painful area or a “lump”.
Aetiology of Physical and Chemical Injuries
- Traumatic occlusion
- Sharp occlusal anatomy
- Thermal injury
- Radiation induced
- Head and neck radiation therapy can cause severe oral mucositis, which can compromise a patient’s ability to eat, swallow, and continue cancer therapy.
- Acidic and alkaline compounds
- For example, acid etch used in dentistry can damage soft and hard tissues if not applied correctly.
- Medications
- A common example is an aspirin burn, which occurs when a patient places an aspirin tablet directly on the mucosa near a painful tooth, causing a chemical burn due to its acidic nature.
Types of cell injuries (biological response)
Cellular responses to injury are categorized based on their potential for recovery, which is determined by the severity and duration of the injurious stimulus.
Reversible
If the stimulus is removed, the cell can return to its normal state. Reversible changes often manifest as cellular adaptations, which can be morphological changes at the cellular and tissue level. These include:
- Hyperplasia
- Hypertrophy
- Atrophy
- Metaplasia
- Metaplasia can often be seen in salivary gland and duct diseases
- Dysplasia
- Intracellular pigments

L2 Physical and chemical injuries, p.8
Irreversible
If the injury is too severe or prolonged, the cell passes a point of no return and undergoes cell death. Irreversible changes include:
- Necrosis
- Ischemia
- Apoptosis
- Free radical damage
- Pathologic calcification
- Cell ageing
Definitions
- Hyperplasia is an increase in the size of an organ or tissue due to an increase in the number of cells (physiologic or pathologic)
- Hypertrophy is an increase in size of a tissue or body part due to the increase in the size of individual cells (physiologic or pathologic).
- Atrophy refers to decrease in size of cells, organs, tissues, or body parts because of disease, hormonal alteration, injury, or lack of use (physiologic or pathologic).
- Metaplasia is caused by a stimulus that changes one cell type into another. A classic example is the respiratory epithelium in smokers changing to a more robust stratified squamous epithelium. In the oral cavity, trauma can induce squamous metaplasia or, if the epithelium is already squamous, an increase in thickness (acanthosis).
- Dysplasia is defined as lack of proper maturation of a tissue. When cells are unable to mature, the tissue cannot properly develop.
- It is often a precursor to malignancy and represents an advanced response to persistent injury (e.g., from tobacco or alcohol) where cells lose their normal organization.
Table: Types of Cellular Adaptations — Physiologic vs. Pathologic
| Physiologic | Pathologic | |
|---|---|---|
| Normal cells | ||
| Hyperplasia | A. Kidney regeneration | B. Gum hyperplasia |
| Hypertrophy | C. Pregnancy (uterine enlargement) | D. Cardiac hypertrophy in infant |
| Atrophy | E. Arm in sling (disuse atrophy) | F. Tongue muscle atrophy |
| An oral example of pathologic atrophy is the thinning of the oral mucosa due to nutritional deficiencies. The mucosa appears red (erythematous) because the underlying blood vessels are more visible. | |
Endogenous Intracellular Pigments
- Melanin is produced by melanocytes located in the basal layer of the epithelium. The number of melanocytes is consistent among all humans; skin and mucosal color is determined by the activity of these cells and the amount of melanin they produce. It can be seen in the skin following lacerations and chronic inflammatory disorders as oral lichen planus.
- Hemosiderin is a pigment derived from hemoglobin of red blood cells. It is composed of ferric oxide. A localized deposit of hemosiderin is seen after bruising when the red blood cells break down and the hemoglobin is released into the surrounding tissues
Definitions
- Ischemia is a restriction in blood supply generally due to damaged blood vessels. The result is damage, dysfunction, or death of tissue supplied by that blood vessel, called infarction.
- Necrosis is the death of cells and tissues that fail to adapt to environmental changes. Pathologic necrosis occurs when normal cell functions cannot be sustained due to infection, toxins, trauma, or lack of oxygen.
- Apoptosis is the process of programmed or planned cell death (tumours and inflammatory disorders). This contrasts with cell death due to injury.
- Free radical damage : Free radicals inflict damage when they react with cell membranes or cellular DNA via peroxidation of membrane lipids, a process that has been implicated in some diseases and ageing.
- Pathologic calcification : abnormal deposition of calcium and may be dystrophic or metastatic. Dystrophic calcification can be observed in both vital and necrotic pulp tissues. Causes include irritation, injury, and reaction to the caries process.
Inflammation
Table 2.2 Types of Inflammation
| Acute | Chronic | Granulomatous | |
|---|---|---|---|
| Onset | Sudden | Gradual | Gradual |
| Duration | Short | Long-standing | Long-standing |
| Predominant cell type(s) | Neutrophils, macrophages | Lymphocytes, plasma cells, macrophages | Epithelioid histiocytes, multinucleated giant cells, lymphocytes |
| Clinical characteristics | Pain, erythema, and edema; fever | Loss of function | Nonpainful enlargement; nodules |
| Outcome | Abscess; resolution; progression to chronic inflammation | Fibrosis; tissue destruction | Medical or surgical intervention |
Physical and chemical injuries
Leukoedema
L2 Physical and chemical injuries, p.14
This term should only be reserved for clinical presentation; the histopathologic feature is keratinocyte edema.
- Clinical Findings
- This is present in up to 90% of the population and is more readily discerned in dark-skinned individuals.
- Delicate lacy, grey-white lines are present on the buccal mucosa or tongue (nonkeratinized sites) that disappear with stretching
- Microscopic Features: Thickened epithelium (acanthosis) with swollen epithelial cells filled with fluid ( Histological images of epithelial tissue.
[[L2 Physical and chemical injuries.pdf#page=16&selection=19,0,21,19&color=yellow|Contact Desquamation]]
- superficial injury to the mucosa caused by direct contact with a mild- to-moderately irritating or caustic toothpaste or mouthwash
- Strips of desquamated keratinocytes appear eosinophilic and degenerated or coagulated, and generally lie on the surface of the otherwise intact mucosa
Frictional Keratosis
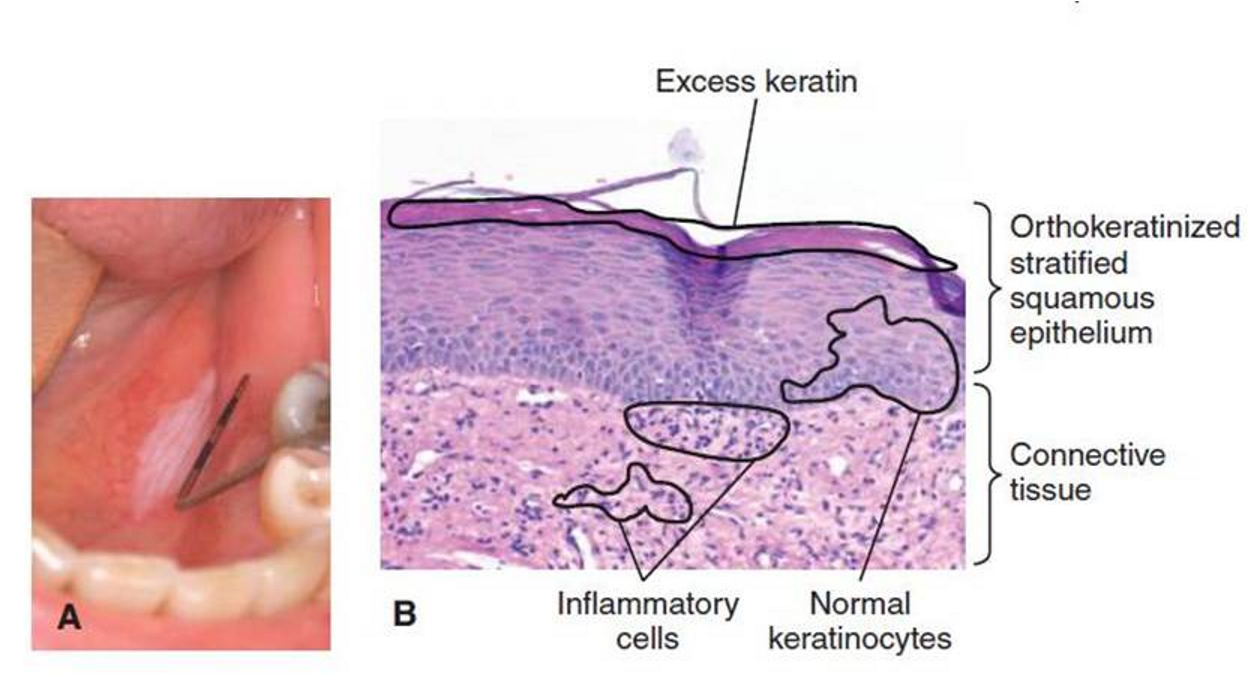
- Frictional Keratosis: benign reactive phenomenon occurs when the mucous membranes are repeatedly irritated over a prolonged period.
- It represents a protective mechanism that increases the thickness of the surface epithelium to protect the underlying tissues from persistent irritation. It is commonly seen on edentulous alveolar ridges under dentures. - Microscopic Features: Hyperkeratosis (increased thickness of the surface keratin layer), acanthosis (increased thickness of the spinous layer), and often, bacterial colonies on the keratin surface. Histological images of epithelial tissue with acanthosis and spongiosis.
Linea alba
- Linea alba (“white line”) is a specific form of frictional keratosis seen as athin, slightly raised white keratotic line along the occlusal plane on the buccal mucosa, and it is often bilateral.
- Linea alba is a variation of normal anatomy but may become prominent in some individuals.
Morsicatio buccarum
-Morsicatio buccarum, linguarum, and labiorum, are forms of frictional keratosis caused by habitual chewing or nibbling of the cheek (morsicatio buccarum), tongue (morsicatio linguarum), and lip (morsicatio labiorum).
- Extra surface keratin builds up (hyperkeratosis) to minimise damage to the deeper tissues. The surface appears white and somewhat shredded. Cessation of the habit usually leads to regression of the lesion.
- Microscopic Features: Similar to frictional keratosis with hyperkeratosis and acanthosis, but the surface is typically more irregular and may show swollen superficial cells and surface bacterial colonization.
Snuff dippers keratosis
- Snuff dippers keratosis is seen in users of smokeless tobacco. White plaques develop in the vestibule where the tobacco directly touches the tissues. These lesions are characterised by thickened white mucosa that is typically wrinkled or corrugated.
- Theclinical presentation may vary from an ill-defined area of white wrinkled thickening to deeply folded tissue with red patches. In addition to mucosal changes, gingival recession around the teeth may be pronounced. Extrinsic staining of teeth is also common. - Microscopic Features: Shows acanthosis with a remarkable increase in the thickness of the superficial epithelial layer, where cells appear swollen and enlarged.
Black hairy tongue
- Coated tongue is retention keratosis caused by dehydration with reduced watery and increased mucous saliva, and poor diet low in fresh fruits and vegetables, leading to retention of keratin rather than normal shedding.
- It is very commonly seen in inpatients in the hospital.
- Antibiotics have been associated with black hairy tongue but they are not a direct effect of the antibiotic. The patient is ill and required antibiotic therapy and is likely dehydrated and not eating normally.
- Microscopic Features: Extreme elongation of filiform papillae with hyperkeratosis. Bacterial colonies are present within the elongated keratin spires. Histological images of skin tissue under a microscope, showing hair follicles and layers of the epidermis and dermis.
Amalgam tattoo
- Amalgam tattoos result from accidental implantation of dental amalgam within the oral tissues.
- Amalgam can be introduced into oral mucosa in several ways:
- During placement or removal of amalgam restorations or during crown preparation.
- Fracture of dental amalgams via trauma or tooth extraction may also leave residual amalgam within soft tissues.
- Endodontic treatment that involved placing amalgam at the apex of the tooth
- Diagnosis is confirmed by x-ray. However, if the lesion cannot be confirmed radiographically, a biopsy is often necessary to rule out melanoma, which is a critical differential diagnosis, especially in high-risk populations.
Post-inflammatory pigmentation
- Inflammation releases prostaglandins and other inflammatory products that stimulate melanocytes to increase synthesis of melanin.
- Melanin becomes trapped by macrophages, called melanophages .
- More common in individuals with darker skin.
- Lesions disappear shortly after the inflammatory process resolves.
- Hypermelanosis may present for many years
- These lesions cause concern because they may resemble early melanoma.
Smoker melanosis
- Smoker’s melanosis is a condition of excessive melanin pigmentation found in the gingiva of about 20% of smokers and seen more frequently in females.
- Melanin deposition is considered a protective mechanism.
- Melanosis is thought to be an attempt by the body to protect itself from toxins and heat produced by smoking tobacco.
- Any mucosal surface can be affected, but melanosis is most commonly seen in the facial anterior gingiva and rarely in the molar areas It must be distinguished from racial melanosis (physiologic pigmentation in individuals with darker skin) and other pigmented lesions like melanoma.
Traumatic ulcer
- Ulcer: the loss of surface epithelium with exposure of the underlying connective tissues.
- Ulcers are one of the most common injuries to the human body.
- Traumatic ulcers are almost always of acute onset, immediately following the traumatic event.
- The lateral border of the tongue and labial mucosa are the most common locations.
- Lesions will appear as round to ovoid depressions with yellow necrotic centers and erythematous irregular borders.
- Patients complain of pain that slowly subsides as the lesion heals over 7 to 10 days.
- Microscopic Features: The ulcer shows a discontinuity of the surface epithelium, covered by a layer of fibrinous exudate. The underlying connective tissue contains a heavy acute inflammatory infiltrate(predominantly neutrophils) and granulation tissue (proliferating new blood vessels and fibroblasts) at the base. Traumatic ulcer
Anesthetic necrosis
- Anesthetic necrosis is an unusual traumatic ulceration typically seen in patients who receive an injection in the greater palatine foramen for dental procedures on the maxillary teeth. It is believed that the epinephrine in the local anesthetic causes mild ischemia, leading to localized necrosis.
- Anesthetic necrosis appears as a well-defined tender-to-painful lesion at the injection site. While necrosis is an irreversible injury to individual cells, the tissue can heal. The anesthetic causes a localized, self-limiting injury. Once the drug is metabolized and the ischemia resolves, the body’s healing mechanisms repair the defect.
- The lesion heals without treatment in 7 to 10 days. The occurrence is idiosyncratic and not every injection causes this, but larger lesions will take longer to heal.
Burns
- Burns to the oral mucous membranes destroy surface epithelium and are usually very painful.
- Burns can be thermal or chemical and are of acute onset following exposure to the source.
- Thermal burns can be induced by contact with hot foods or liquids. Hot foods that contact the lips or oral cavity mucosa may result in acute tissue destruction.
- Palatal burns from eating hot pizza are a common example. Occasionally, accidental contact with live electrical wires can cause deep burns to the face and/or oral cavity.
- Electrical burns of the lips and commissures can be seen in young children who accidentally chew or bite into electrical cords. Electrical burns to the lips are often severe, involving extensive tissue damage and requiring special reconstruction by a plastic surgeon.
Chemical Burns
- Chemical burns can result when caustic agents contact the oral mucosa. Chemical burns may appear as thick, rough hyperkeratotic plaques with a corrugated or cratered surface and/or areas of ulceration.
- Patients may misuse acidic medications, such as aspirin tablets or powders that contain acetylsalicylic acid.
- Aspirin may cause a significant burn if placed adjacent to or over a painful tooth, rather than being swallowed.
- Patients may use strong agents, such as hypochlorite (bleach), to clean or disinfect Dental materials such as sodium hypochlorite (used in endodontics) and hydrogen peroxide (used in teeth whitening) can also cause significant tissue damage if they contact the mucosa, highlighting the importance of proper isolation (e.g., with a rubber dam).
Nicotinic stomatitis
- Nicotine stomatitis occurs in smokers and results from exposure of the palate to the smoke and heat of burning tobacco products.
- It generally appears as a thick, white plaque of the hard and soft palate, containing scattered, tiny, raised red (erythematous) dots. The erythematous dots represent irritated minor salivary gland ducts. The lesion is a response to chronic heat, which causes irritation and inflammation of these ducts.
- Nicotine stomatitis persists as long as the individual continues smoking. The lesion itself is benign and will regress upon smoking cessation. Histological image of glandular skin structures with dermal and epidermal layers.
**[[2. Physical and Chemical Injuries of the Oral Cavity#pyogenic-granuloma-| Pyogenic granuloma]]
**
- Pyogenic granulomas are exophytic lesions composed of an exuberant overgrowth of granulation tissue in response to minor chronic irritation.
- The name is inaccurate because it is not due to pyogenic (pus-producing) bacteria and is not granulomas.
- Microscopic Features: The lesion is composed of a highly vascular proliferation of granulation tissue with a mixed inflammatory infiltrate. The surface is usually ulcerated.
Traumatic fibroma
- Traumatic (irritation) fibromas are benign lesions with dense, highly fibrous connective tissue, like a scar.
- They are more appropriately called focal fibrous hyperplasia to denote a reactive rather than neoplastic origin.
- They occur anywhere that persistent chronic tissue irritation occurs, most often along the line of occlusion, where repetitive trauma from biting may occur.
- They may be sessile or pedunculated with a pink smooth surface
- Management: Simple surgical excision.
Drug-induced gingival hyperplasia
- Drug-induced gingival overgrowth is considered a reactive phenomenon seen in patients taking medications that stimulate collagen growth or prevent its breakdown.
- It is well documented that phenytoin (Dilantin), cyclosporine, nifedipine, and other calcium channel blockers may lead to gingival overgrowth.
- Clinically, the lesions are similar and do not differ based on type of drug.
Flowchart: Management of Suspected Reactive Lesion
A systematic approach is essential for diagnosis: 1. Patient History: Take a thorough history to identify any potential sources of trauma or irritation. 2. Identify and Remove Cause: If an irritating factor (e.g., a sharp cusp or overhanging restoration) is found, remove it. 3. Review and Observe: Re-evaluate the patient after a period (e.g., 2 weeks). A true reactive lesion should resolve or significantly improve once the stimulus is gone. 4. Biopsy: If the lesion persists after removing the suspected cause, a biopsy is mandatory to establish a definitive diagnosis and rule out more serious conditions like malignancy.
- Lesion suspected to be reactive
- ↓
-
- Look for source of irritation
- ↓
- ├──> Suspected source identified and removed or relieved
- │ ↓
- │ - Patient returns in 2—3 weeks
- │ ↓
- │ ├──> Lesion gone: continue observation
- │ └──> Lesion still present: try again to remove suspected source
- │ ↓
- │ - Patient returns in another 2—3 weeks: lesion still present
- │ ↓
- │ → Biopsy
- ↓
- └──> No source identified or suspected: source cannot be removed or relieved
- ↓
- → Biopsy