Benign Epithelial Pathosis1
Dr Agnieszka Frydrych
Introduction23
Clinical Significance4
- Common problems encountered in practice
- Importance of accurate recognition and appropriate management
Visual representation of patient anxiety and clinical presentation (inflamed tonsils) related to benign epithelial pathosis.
- Patient Anxiety: Misidentifying a benign lesion as potentially concerning can create unnecessary anxiety for the patient.
- Triage and Referral: Proper identification allows for correct triage. Patients with benign lesions should not be referred as urgent cases.
- Management: Recognizing benign conditions ensures that patients are managed appropriately, often requiring only reassurance rather than invasive intervention.
Leukoedema5
 |  |  |
 |  |  |
 |
Aetiology and Pathogenesis
- Generalized mild opacification of the oral mucosa.
- This is a common condition.
- Considered a normal variant rather than a pathological condition.
- Contributory factors may include smoking, alcohol use, and salivary alterations.
Clinical Features
- Typically an incidental finding during examination.
- Asymptomatic and symmetrically distributed.
- Appearance: Patients present with symmetric, gray-white surface alterations.
- Location: Generally affects the buccal mucosa.
- Demographics: More apparent in non-white individuals.
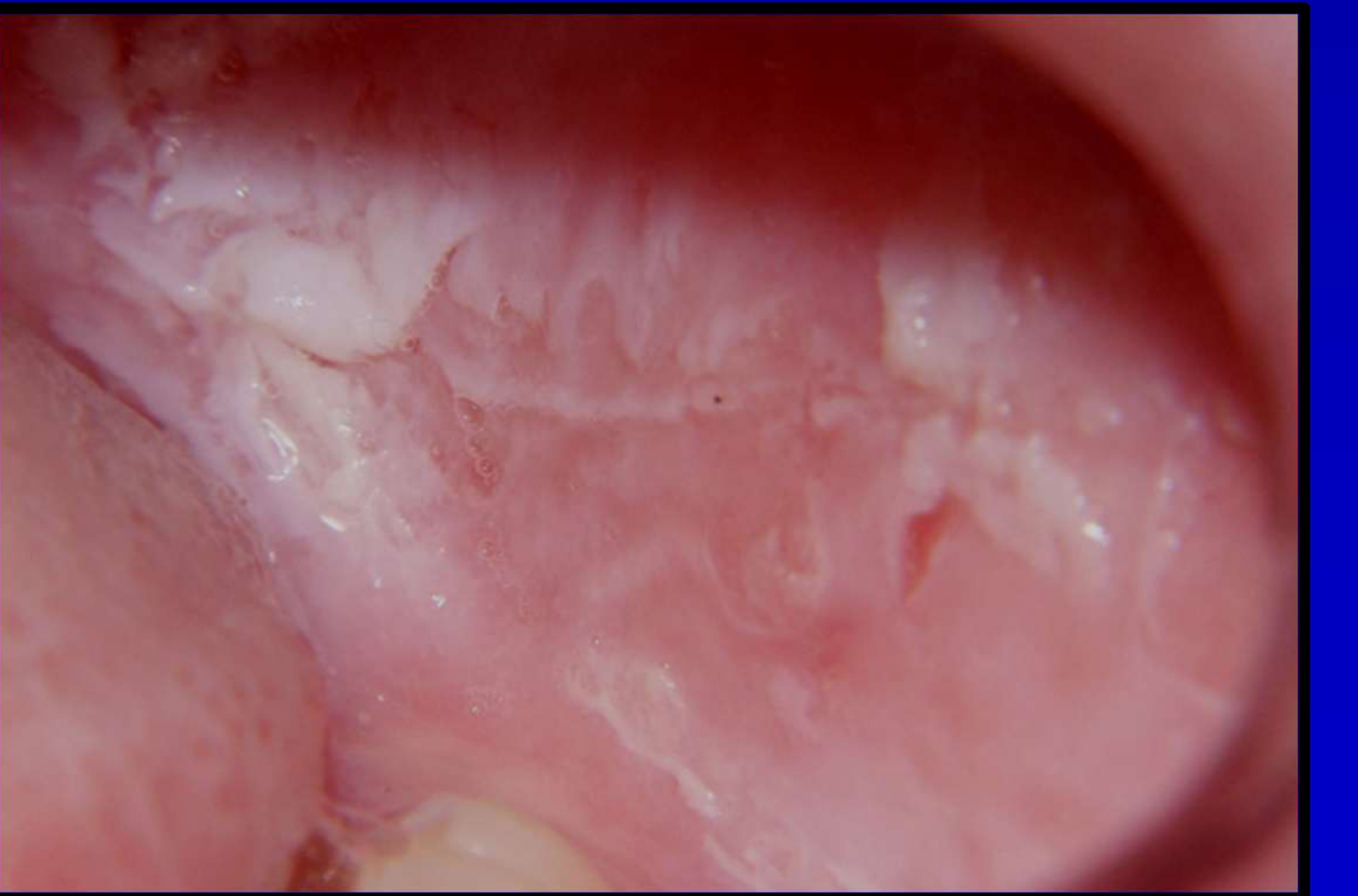
Clinical photographic documentation of Leukoedema (Photos courtesy of Dr. JE Bouquot).
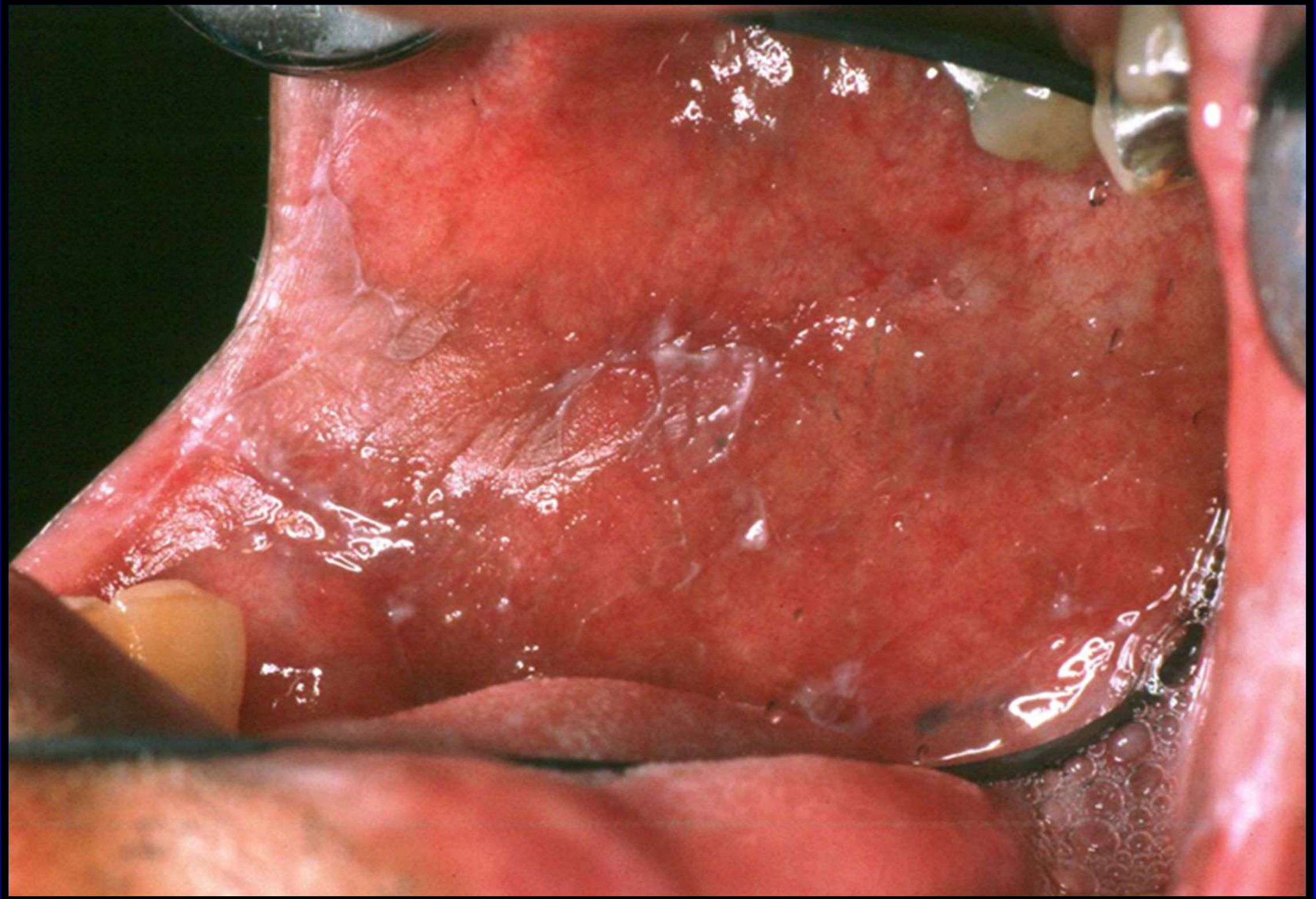
Case Study: Leukoedema Presentation
- Observation: A clinical example demonstrates obvious leukoedema affecting the buccal mucosa.
- Feature: The lesion presents as a gray-white opacification that is symmetric.
- Confirmation: Upon stretching the tissue during examination, the white appearance vanishes, distinguishing it from other white lesions.
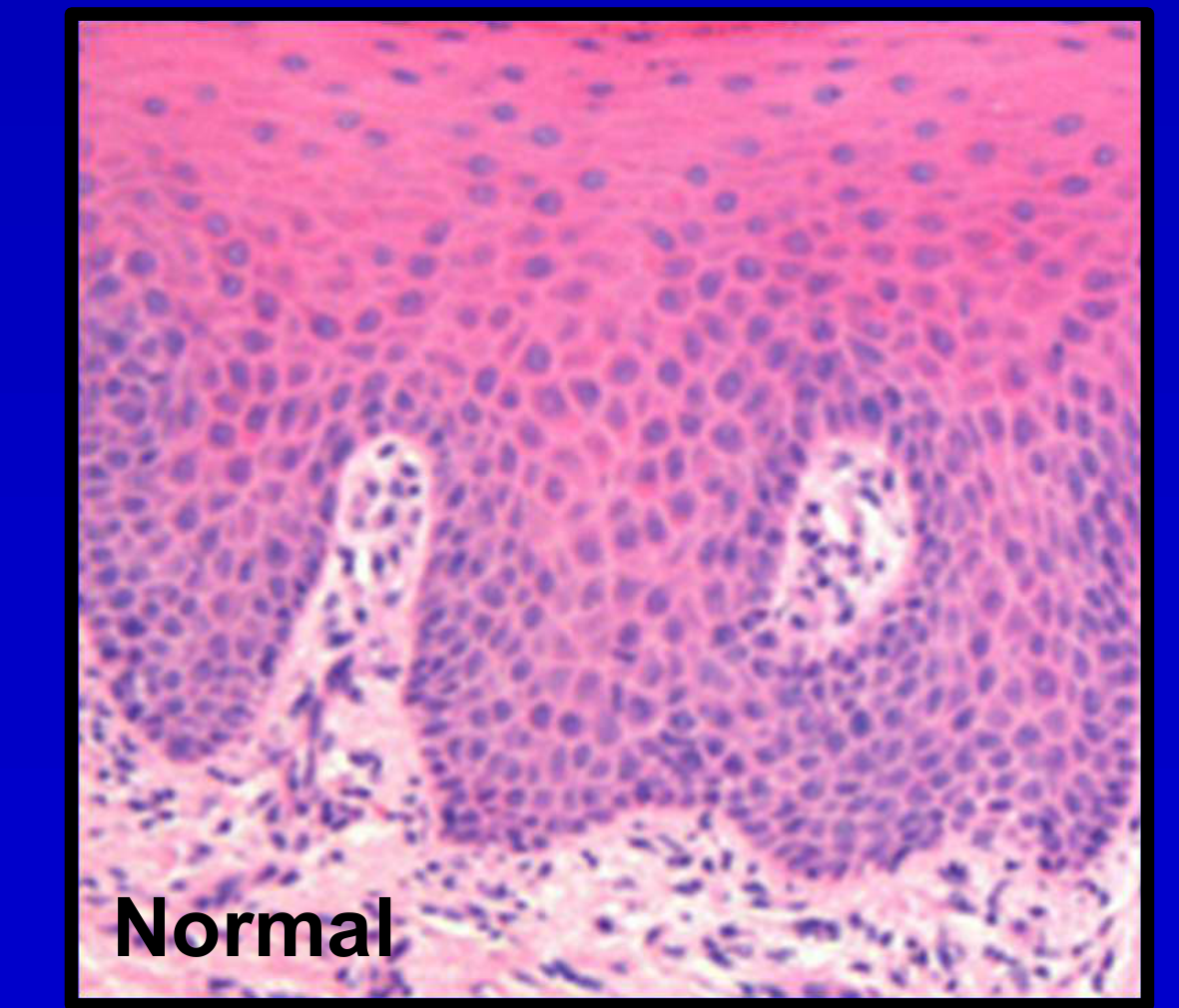
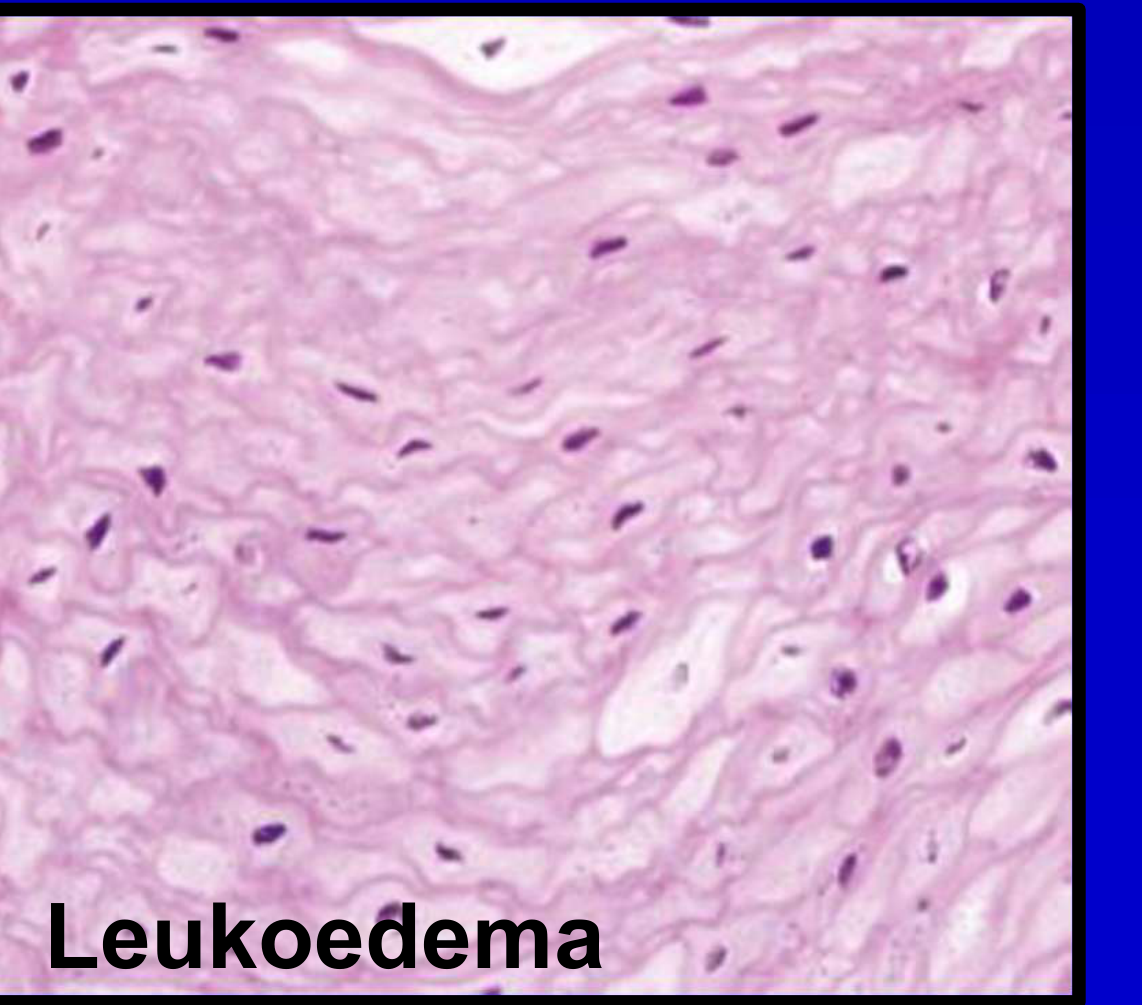
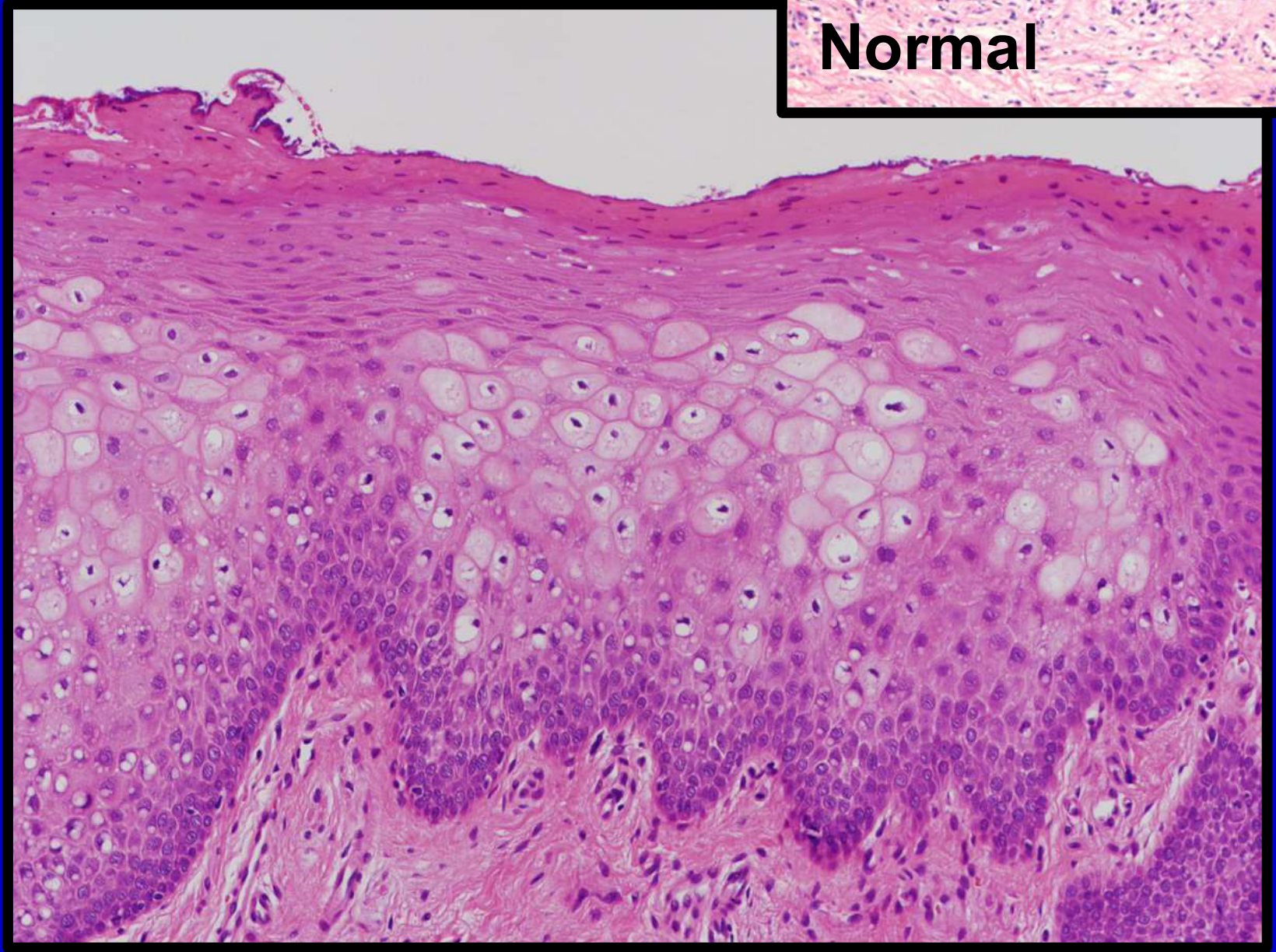
Histopathology
- The epithelium exhibits parakeratosis and acanthosis.
- Presence of intracellular oedema.
- Observation of pyknotic nuclei.
- Epithelial Cells: Enlarged epithelial cells possess small, pyknotic nuclei.
- Cytoplasm: The cytoplasm appears optically clear.
- Cell Type: There is marked intracellular oedema of the spinous cells.
Clinical Identification and Comparisons6
-
Differential Diagnosis Considerations:
- White sponge nevus
- Frictional keratosis
- Oral lichen planus
- Other similar leukoplakic lesions
-
Diagnostic Feature:
- A distinguishing characteristic is that Leukoedema disappears when the mucosa is stretched.
Definition of Differential Diagnosis7
Differential diagnosis is the process of comparing the patient’s status with the known signs, symptoms, and other features of the diseases that are possible causes of the patient’s condition or lesion
- Logical Grouping: Conditions listed must make sense together (e.g., orange and mandarin vs. bananas and oranges).
- Academic Expectations: DMD level students provide three conditions; DCD level requires a more extensive list.. exam
White Sponge Nevus8
 |  |  |
 |  |
Etiology and Pathogenesis9
- Autosomal dominant condition
- Caused by point mutations in genes coding for Keratin 4 and/or Keratin 13
Clinical Features
- Appear early in life
- White, thickened, spongy lesions
- Usually bilateral and symmetric
- Asymptomatic
- Lesions can also affect the mucosa of the esophagus, anus, vulva, and vagina
Clinical presentation typically involves diffuse white plaques across the oral mucosa.
White Sponge Nevus Presentation
- Observation: Clinical examples show white, thick, and spongy bilateral lesions
- Location: Affecting the buccal mucosa
- Characteristics: Distinctively spongy texture and symmetric distribution
Histopathology
- Thickened epithelium
- Spongiosis, acanthosis, and parakeratosis
- Perinuclear condensation of cytoplasm
- Within the prickle cell layer, there is marked hydropic vacuolar cell change
Differential Diagnosis
- Leukoedema
- Oral lichen planus
- Frictional keratosis
- Other hereditary or reactive keratoses
- Leukoedema is distinguished by the fact that it disappears on stretching
Treatment
- None required
- A biopsy may be required to confirm the diagnosis
- Patients are reassured regarding the benign nature of the pathosis
Squamous Papilloma
 |  |  |
 |  |
Aetiology and Pathogenesis
- Benign lesions caused by the Human Papillomavirus (HPV), specifically Types 6 and 11.
- Demographics: Typically affects adults
- Multiplicity: Can be single or multiple; numerous lesions may indicate immunodeficiency (e.g., HIV)
Clinical Features
- Distinctive exophytic lesions
- Cauliflower-like or finger-like processes
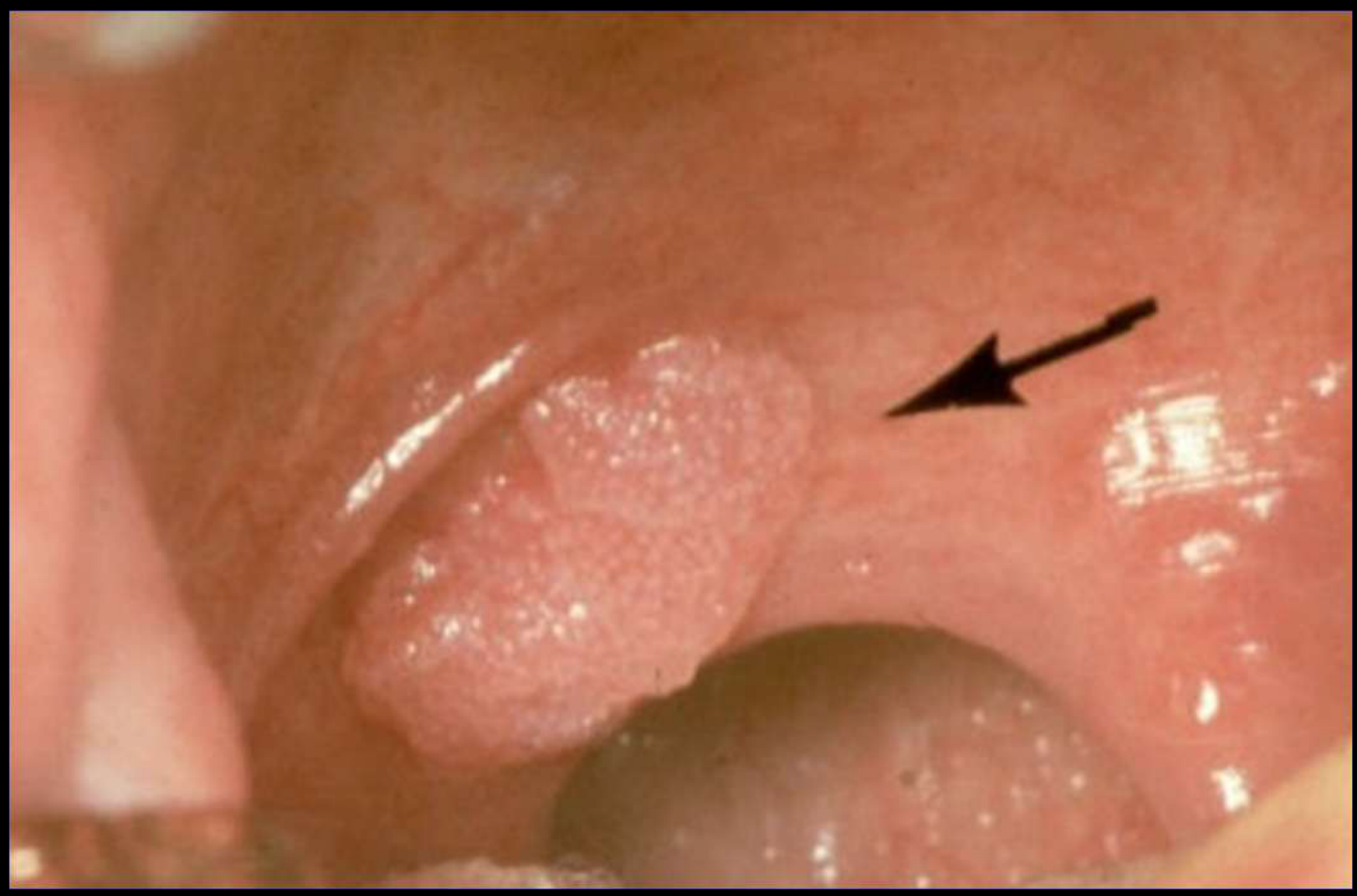
Clinical Presentation
- Intra-oral presentation typically appears as a small, cauliflower-like, exophytic lesion. Common sites include the buccal mucosa near the molar teeth.
Case Study: Squamous Papilloma Presentation
- Observation: Example displays squamous papilloma with distinct finger-like projections
- Appearance: Lesion exhibits classic cauliflower-like morphology associated with HPV-induced epithelial proliferation
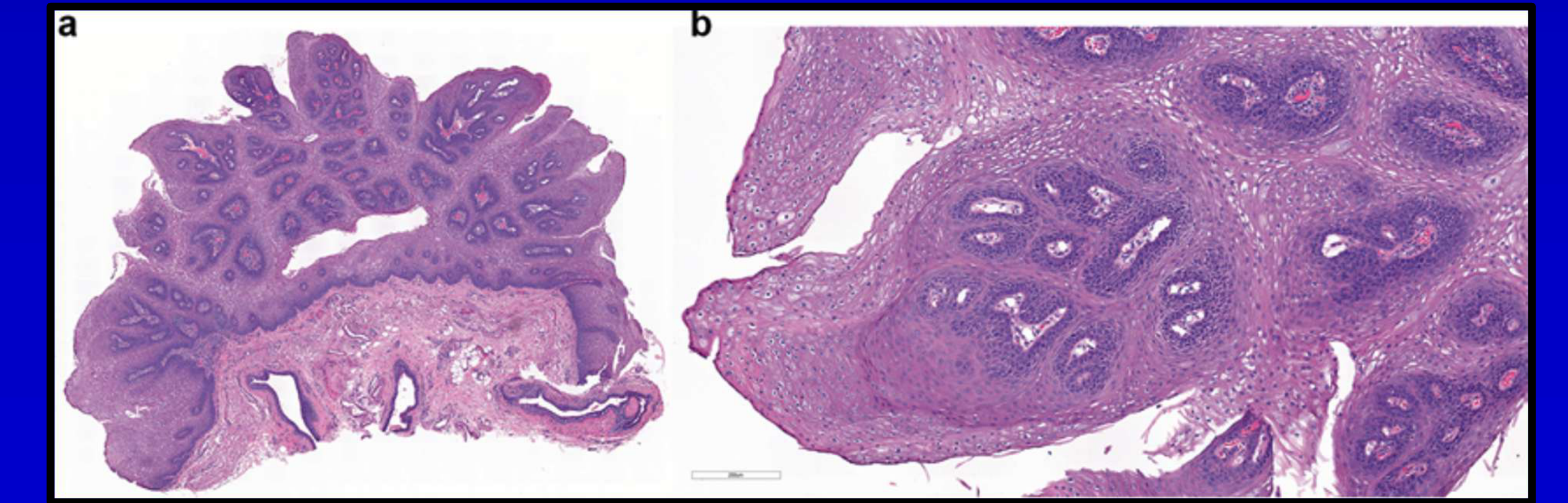
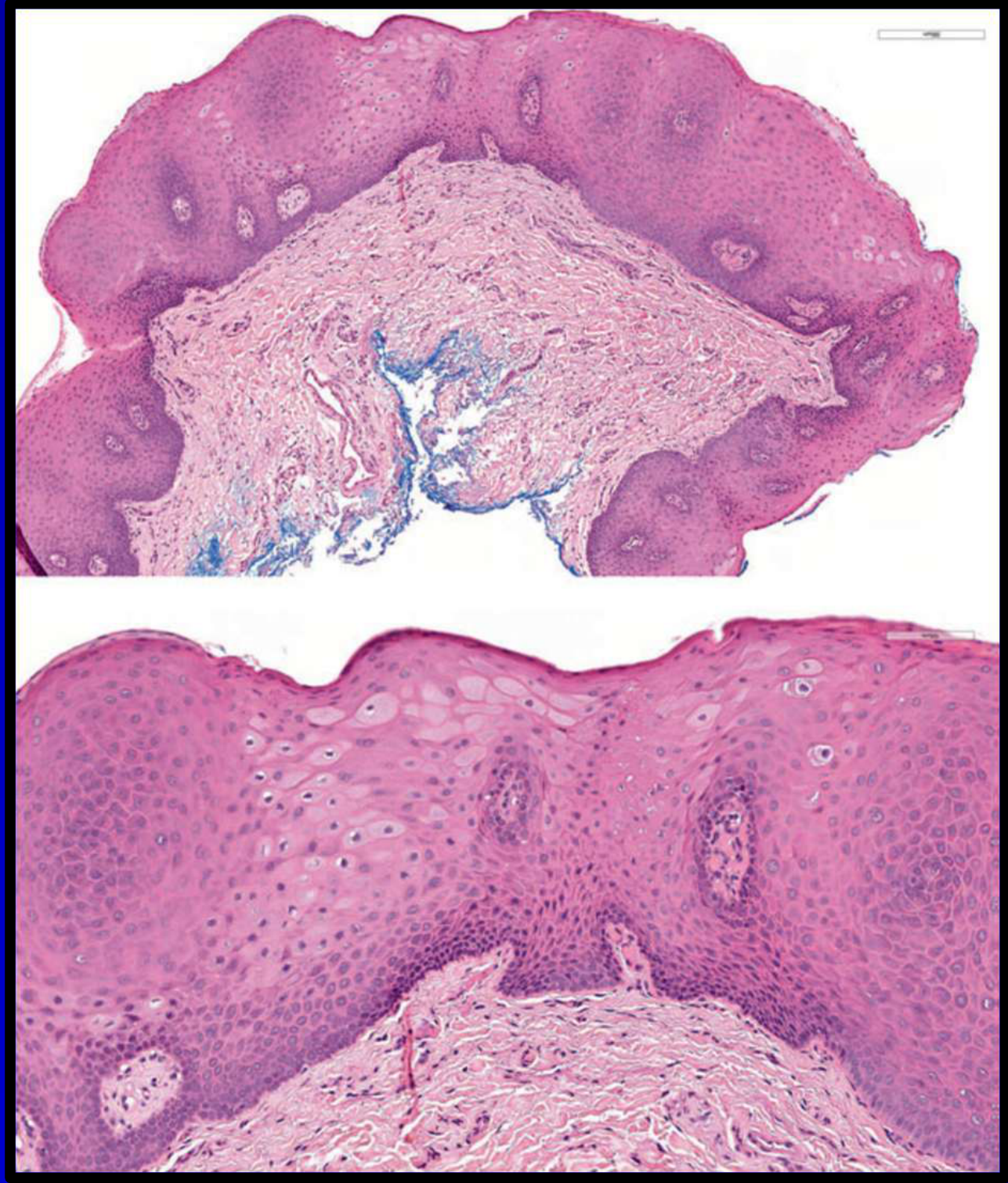
Histopathology
- Proliferation of stratified squamous epithelium supported by a vascular connective tissue core.
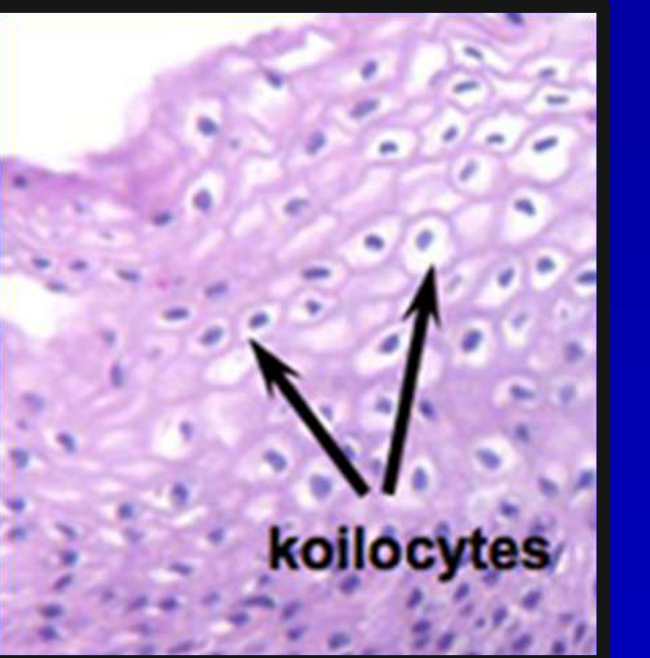
- Koilocytes (cells showing HPV-related cytopathic changes) may be observed within the epithelium.
- Koilocyte Appearance: Cells with crumpled nuclei, condensation of cytoplasm, and clear perinuclear halo
- Neoplastic Debate: Argument exists that some papillomas may be true benign neoplasms despite limited growth potential
Diagnosis and Treatment
- Diagnosis: Primarily based on clinical presentation.
- Treatment: Surgical excision is considered curative.
Verruca Vulgaris
 |  |
 |
Aetiology and Pathogenesis
- Benign lesions caused by the Human Papillomavirus (HPV)
- Associated with HPV Types 1 and 57, as well as Types 6 and 11
- Common Name: Infective warts
- Demographics: Commonly seen in children
- Transmission: May be caused by autoinoculation from warts on other sites
Clinical Presentation
- Similar appearance to squamous papilloma
- Lesions may be more round in shape or only slightly raised from the surface
- Lesions can be indistinguishable from squamous papilloma or condyloma acuminatum
Case Study: Verruca Vulgaris Presentation
Observation: Clinical pictures show lesions that are round or slightly raised Comparison: While similar to squamous papilloma, the morphology may be less finger-like and more rounded, consistent with cutaneous wart variants found in children
Histopathology
- Histological features are consistent with those of squamous papilloma
- Characterized by the presence of larger koilocytes
Diagnosis and Treatment
-
Diagnosis: Primarily based on clinical presentation
-
Treatment: Surgical excision is curative
-
This determines whether the lesion appears as a red lesion or a white lesion.
Condyloma Acuminatum
 |  |
 |  |
Aetiology and Pathogenesis
- Benign lesions caused by the Human Papillomavirus (HPV), specifically Types 2, 6, and 11.
- Classified as a sexually transmitted disease.
Clinical Presentation
- Characterized by numerous pink nodules.
- These nodules tend to grow and coalesce over time, often forming larger, cauliflower-like masses.
- In some cases, lesions can be indistinguishable from verruca vulgaris or squamous papilloma.
Histopathology
- Presence of papillary projections.
- Epithelium may be keratinized or non-keratinized.
- Presence of koilocytosis (cells with perinuclear halos and nuclear atypia, indicative of HPV infection).
Diagnosis and Treatment
- Diagnosis: Primarily clinical based on appearance and history.
- Treatment: Surgical excision is considered curative.
Clinical Considerations10
- What is the significance of these lesions when identified in children?
Significance in Children and Mandatory Reporting11
-
Identification of these lesions in children raises significant concerns regarding child welfare.
-
In accordance with the Government of Western Australia Department for Child Protection guidelines:
- Mandatory reporting of child sexual abuse is required.
- Healthcare providers must follow child protection protocols and “make the call” to report suspected abuse.
-
Clinicians must be careful because condyloma acuminatum, squamous papilloma, and verruca vulgaris can be clinically indistinguishable.
-
It is important not to focus on a single lesion but to look at the bigger picture, including the child's behavior and other physical signs.
Physiologic Pigmentation12
 |  |  |
 |
Aetiology and Pathogenesis
- Caused by increased melanin production.
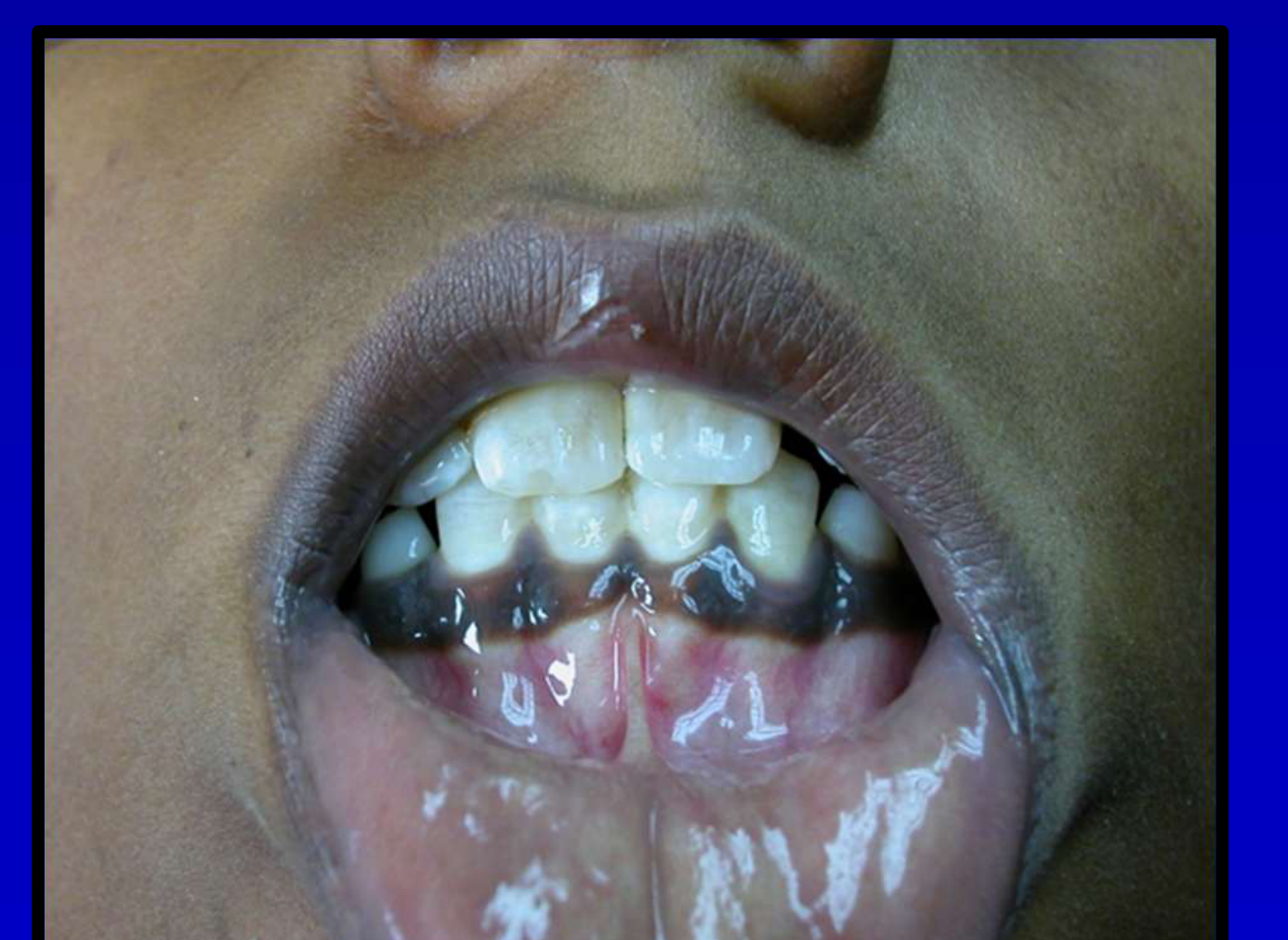
Physiologic (racial) pigmentation can present as dark spots or patches on the surface of the tongue and other oral mucosal sites.
- Mechanism involves increased melanin production, not increased numbers of melanocytes
- Benign condition
Clinical Presentation
-
Symmetric distribution
-
No alteration of tissue architecture
-
Can occur at any age
-
Degree of oral pigmentation may not correspond to the degree of cutaneous pigmentation
-
No gender predilection
-
Can occur in any intraoral location
-
Gingiva is the most commonly affected site
Case Study: Physiologic Pigmentation on the Tongue
- Observation: Examples show physiologic pigmentation affecting the tongue
- Feature: The pigmentation is symmetric and persistent, maintaining normal mucosal architecture
Histopathology
- Characterized by increased melanin production
- Melanin is found within the basal keratinocytes and subjacent connective tissue macrophages
- Normal numbers of melanocytes
- Melanin incontinence: Melanin spilled and picked up by macrophages in adjacent connective tissue
Differential Diagnosis
- Smoking-associated melanosis
- Addison’s disease
- Peutz-Jeghers syndrome
- Melanoma
Differential Diagnosis Details
- Addison's Disease: Primary adrenocorticoid insufficiency
- Mechanism: Reduced cortisol leads to increased ACTH and MSH, stimulating melanocytes
- Systemic Signs: Weakness, weight loss, nausea, vomiting, hypertension
- Peutz-Jeghers Syndrome: Autosomal dominant condition with melanotic macules and intestinal polyps
Diagnostic Considerations
- Biopsy may be required if atypical clinical features are present.
- Differentiate between localized physiologic pigmentation and systemic causes such as Addison's disease or genetic syndromes
Treatment
- No treatment is required.
Oral Melanotic Macules131415
 |  |  |
 |  |  |
 |  |  |
 |  |
Aetiology and Pathogenesis
Oral melanotic macules are focal pigmented lesions that may represent several different conditions:
- Intraoral freckle: A localized area of increased pigment.
- Post-inflammatory pigmentation: Darkening of the tissue following an inflammatory process.
- Systemic disease: Pigmentation as a manifestation of an underlying systemic condition.
Clinical Presentation
- Nature: Benign in character.
- Location: May affect any oral mucosal surface.
- Most commonly affected sites include the gingiva and the vermilion border of the lips.
- Symptoms: Typically asymptomatic.
Systemic Associations16
Generalized pigmentation due to Addison disease.
- Melanotic macules can also be associated with Peutz-Jeghers syndrome.
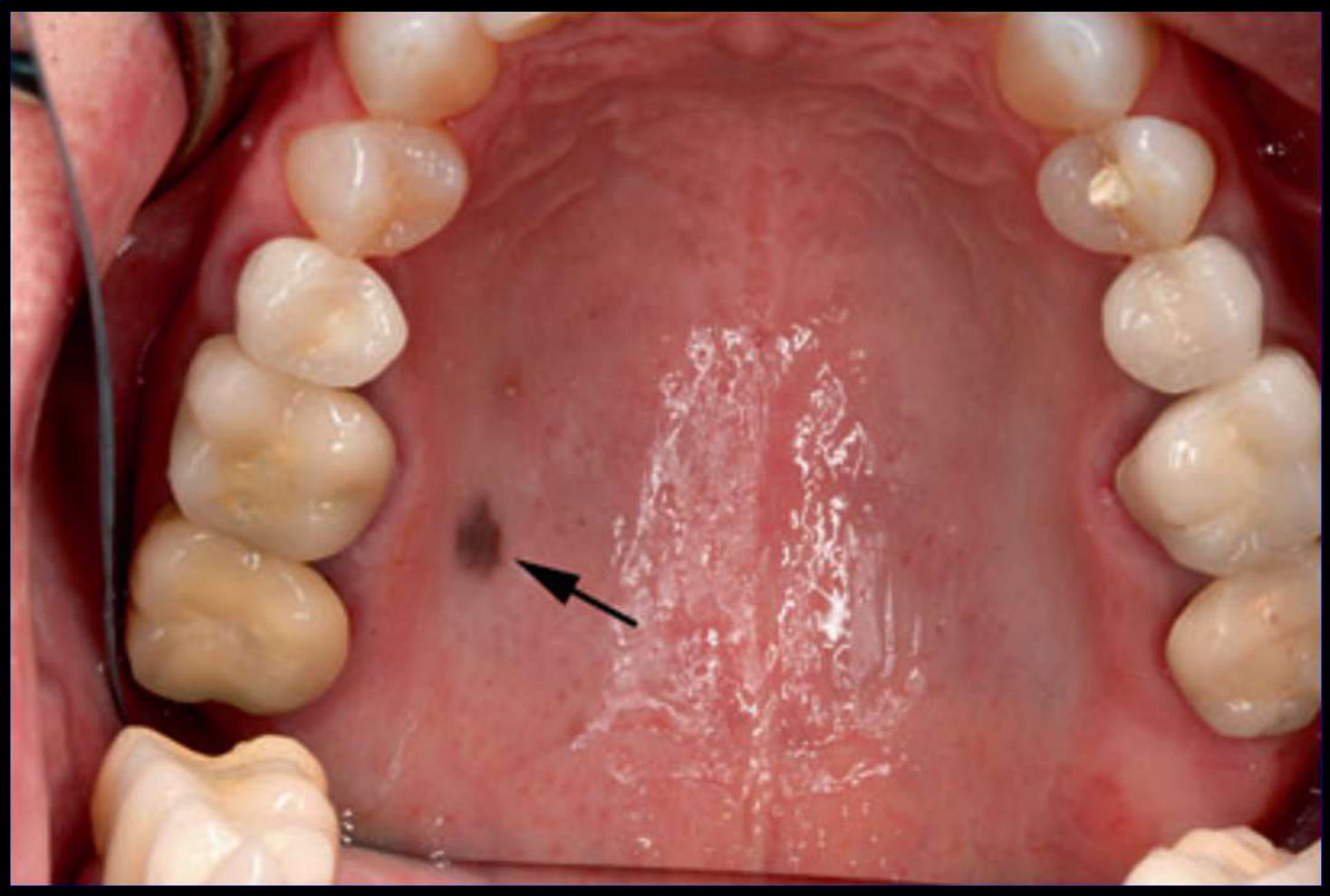
Case Studies: Oral Melanotic Macules
Case 1: Solitary Melanotic Macule
- Presentation: Solitary macule on gingiva
- Management: Biopsy undertaken to confirm diagnosis Case 2: Post-Inflammatory Pigmentation
- Presentation: Pigmentation on buccal mucosa following inflammation Case 3: Peutz-Jeghers Syndrome
- Presentation: Multiple melanotic macules
- Systemic Features: Autosomal dominant, intestinal polyps (hamartomas)
- Symptoms: Abdominal pain, rectal bleeding, diarrhea Case 4: Addison’s Disease
- Presentation: Diffuse pigmentation, not confined to oral mucosa
- Extra-oral Signs: Increased skin pigmentation
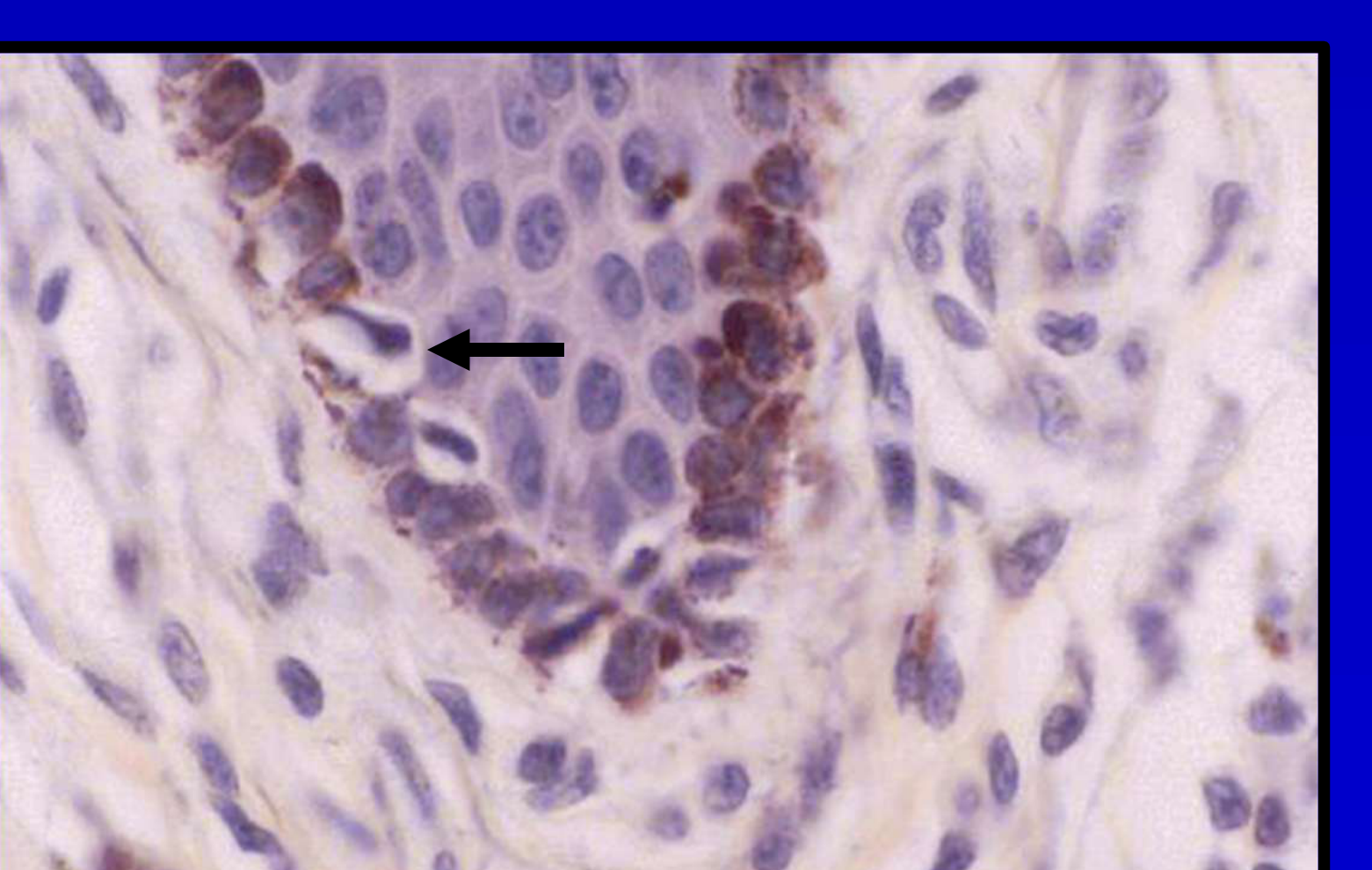
Histopathology
- Melanin accumulation: Increased pigment is observed within the basal keratinocytes.
- Melanocyte count: There are normal numbers of melanocytes present.
- Histopathology is exactly the same as physiologic pigmentation.
Differential Diagnosis
- Amalgam tattoos
- Nevi
- Malignant melanoma
Treatment and Management17
- Diagnosis: A biopsy may be required to establish a definitive diagnosis and rule out other pigmented lesions.
- Intervention: No specific treatment is required once a benign diagnosis is confirmed.
- Biopsy may be needed as shown in the gingival lesion example to rule out melanoma.
Melanocytic Nevus
 |  |  |
 |  |
Aetiology and Pathogenesis
- Consists of collections of nevus cells.
- These cells are found in the epithelium, the supporting connective tissue, or both.
- The condition is considered rare.
- It may present at any age.
- Nature: Benign neoplasms
- Onset: May present at birth (congenital)
Clinical Presentation
- Appears as small elevated papules or nodules.
- Lesions may be non-pigmented.
- May be non-pigmented (approx. 10% of cases)
- The palate is the most common intraoral site.
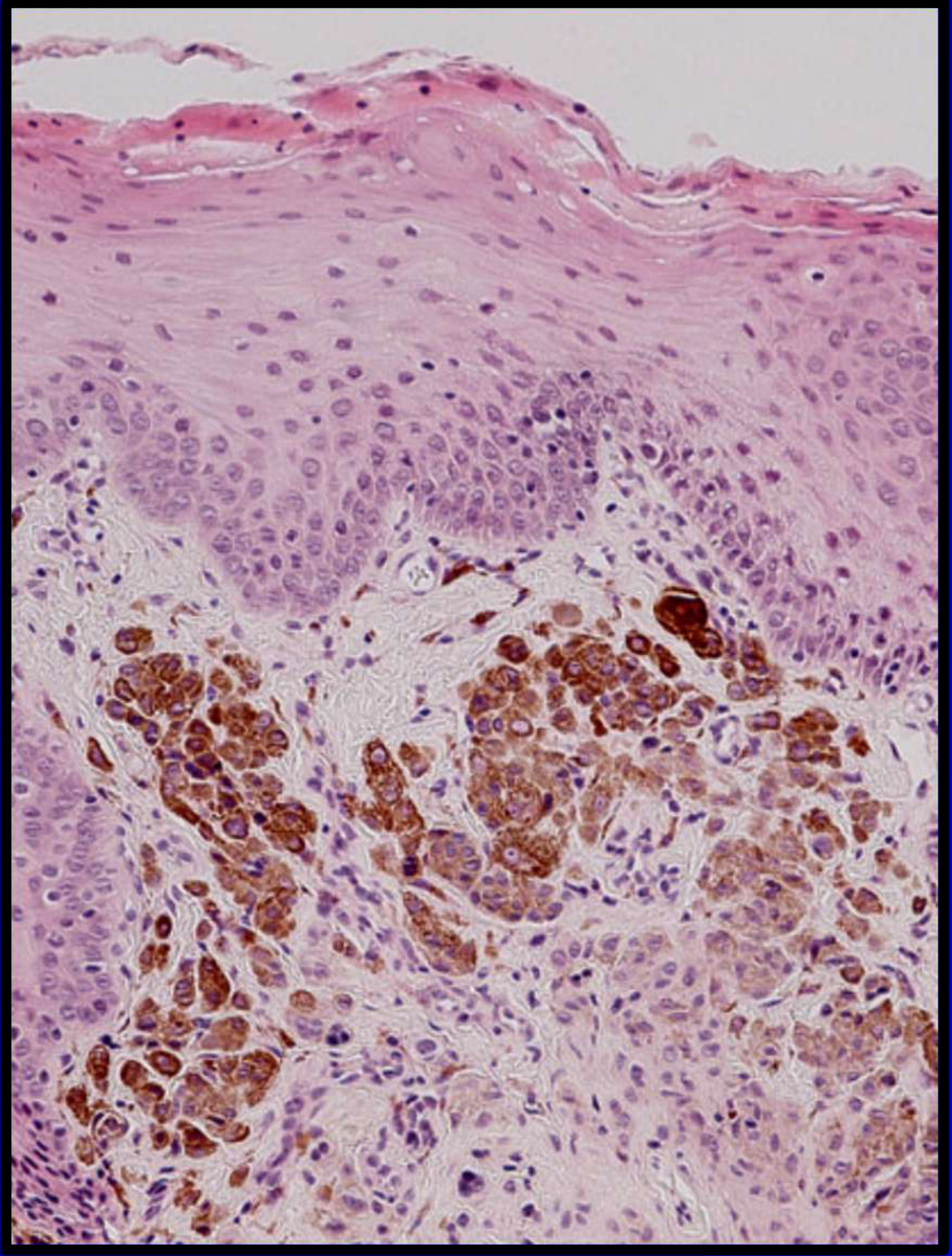
Case Study: Melanocytic Nevus Presentation
- Observation: An example shows a melanocytic nevus presenting as a raised lesion
- Clinical Concern: Because these lesions can mimic melanoma, excision is generally recommended to ensure accurate diagnosis
Histopathology
- Categorized into several subtypes based on the specific location of the nevus cells.
- Characterized by nests of pigmented nevus cells.
- Junctional Nevus: Cells located in the epithelium-connective tissue interface
- Intramucosal Nevus: Cells located in the connective tissue below the epithelium
- Compound Nevus: Cells located in both zones
- Blue Nevus: Cells found deep in the connective tissue
- Malignant Potential: Malignant transformation of oral melanocytic nevi is highly unlikely
Differential Diagnosis
- Melanotic macule
- Amalgam tattoo
- Melanoma
- Diagnostic Note: A biopsy is often required to establish an accurate diagnosis
Treatment
- Surgical excision is the indicated treatment.
- Management: Excision is generally recommended to ensure accurate diagnosis and rule out melanoma
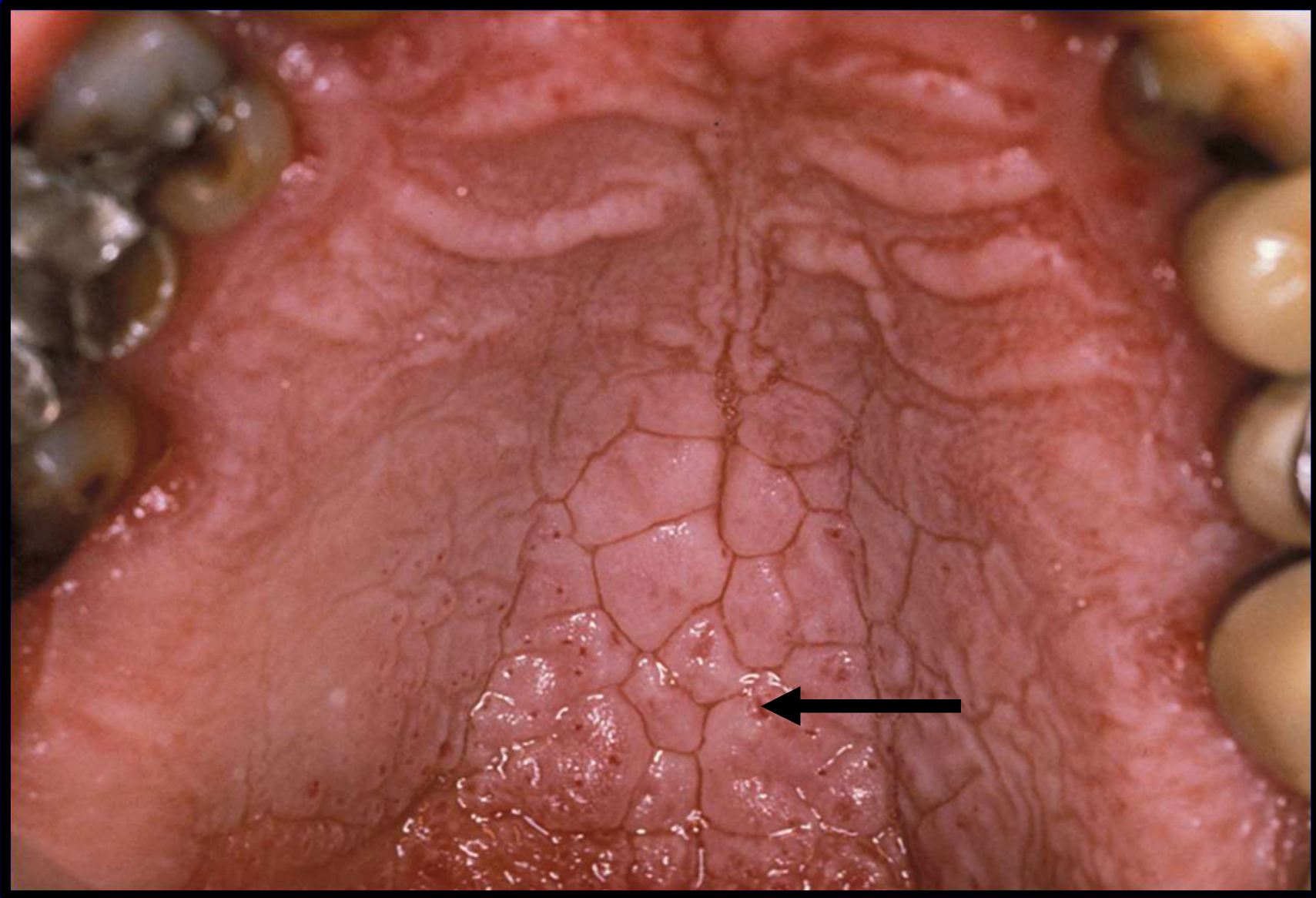
Nicotine Stomatitis
 |  |
 |  |
Aetiology and Pathogenesis
- Tobacco-related form of hyperkeratosis
- Prevalence: Very common lesions in smokers
- Progression: Palatal mucosa initially responds with erythematous change, followed by keratinization, then red dots surrounded by white keratotic rings appear
- Pathology of Dots: Represent inflammation surrounding the minor salivary gland excretory ducts
Clinical Presentation
- Hyperkeratosis
- Inflamed salivary duct orifices
Case Study: Nicotine Stomatitis Presentation
- Observation: Clinical images show the characteristic red dots surrounded by white keratotic rings on the palate
- Context: The patient is a smoker, and the lesions serve as a visible indicator of tobacco use
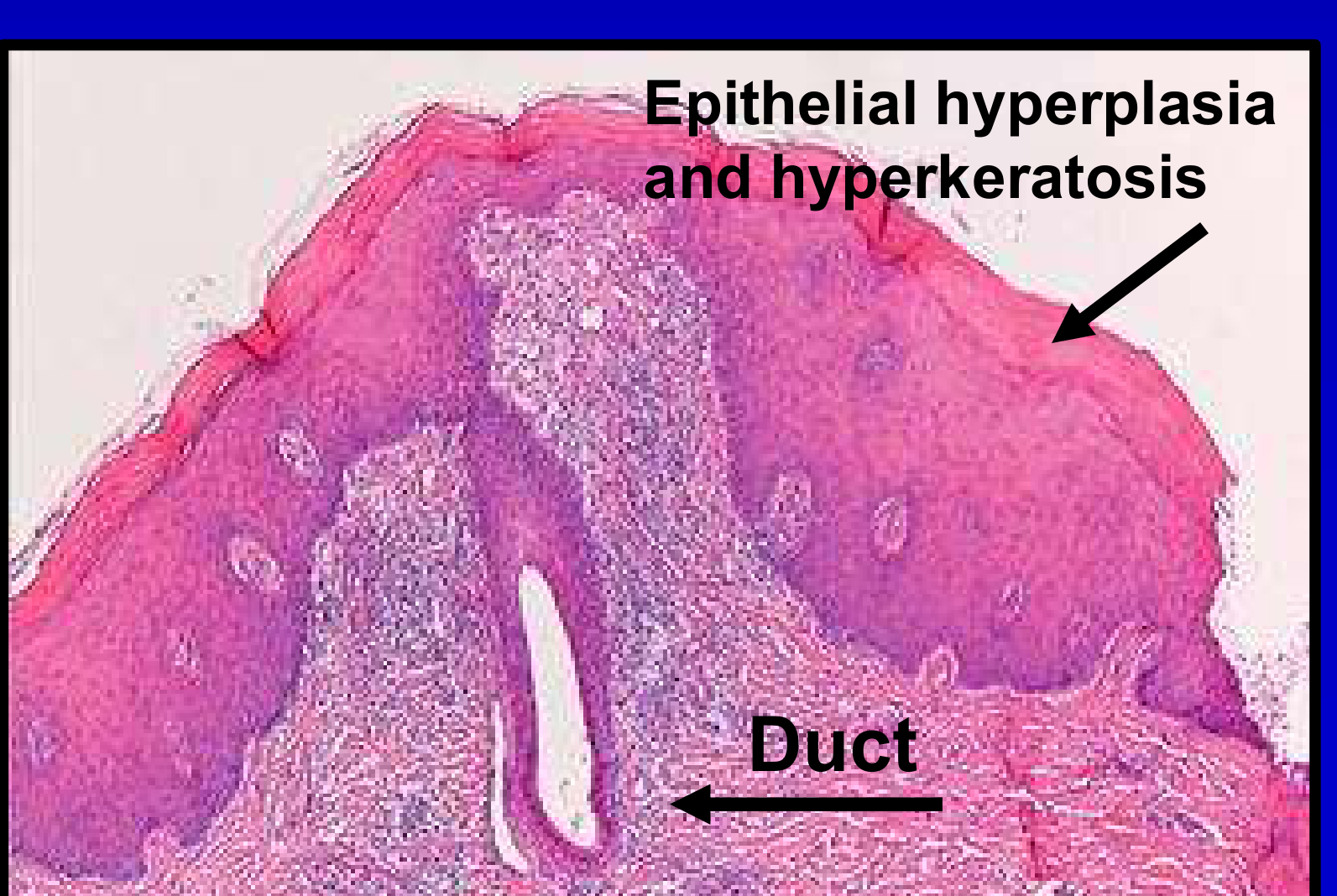
Histopathology
- Epithelial hyperplasia and hyperkeratosis
- Salivary glands show inflammatory salivary squamous metaplasia of excretory ducts
Treatment and Prognosis18
- Malignant transformation is rare
- Condition serves as an indicator of tobacco use
- Education: It serves as a valuable education point when discussing smoking cessation. Clinicians can point out the lesions to show patients the harm smoking is doing to their oral tissues
Hairy Tongue
 |  |
Aetiology and Pathogenesis
- Filiform papillary overgrowth
- Numerous predisposing factors
- Alteration in microbial flora
- Use of broad-spectrum antibiotics
- Steroid use
- Use of oxygenating mouthwashes
- Radiation therapy to the head and neck region
- Hematopoietic stem cell transplants
- Mechanism: Alteration of microbial flora with proliferation of fungi and chromogenic bacteria
- Alteration in microbial flora
Clinical Presentation19
- Enlarged filiform papillae appearing as dense and hairlike
- Asymptomatic
- Primarily a cosmetic problem
- Color ranges from white to brown to black
- Depends on diet, oral hygiene, and composition of bacteria
Case Study: Hairy Tongue Presentation
- Observation: Examples show elongated filiform papillae with surface contamination
- Appearance: Tongue appears "hairy" with discoloration ranging from white to black
- Factors: Post-radiation or antibiotic use
Histopathology
- Elongated filiform papillae
- Surface contamination by clusters of micro-organisms and fungi
- Underlying lamina propria is mildly inflamed
Diagnosis
- Clinical diagnosis
- Based on the characteristic appearance of the dorsal tongue surface
Treatment and Management20
- Identify the underlying cause
- Gentle scraping of the tongue
- Use of sodium bicarbonate
- Successful treatment dependent on identifying cause and discontinuing offending agent
- Treatment in post-radiation therapy patients is particularly difficult
Summary
Key Principles of Benign Epithelial Pathosis21
- Common problems occur commonly!
- It is important to recognize benign pathosis for what they are to avoid unnecessary concern or intervention.
- Ensure appropriate referral pathways are followed when clinical findings require specialist evaluation.
- Patients with benign pathosis should not be referred as urgent cases
- Incorrect triage delays care of truly urgent cases and creates unnecessary anxiety
Footnotes
-
Original PDF page 1: L9 Benign Epithelial Pathosis, p.1 ↩
-
Original PDF page 3: L9 Benign Epithelial Pathosis, p.3 ↩
-
Original PDF page 4: L9 Benign Epithelial Pathosis, p.4 ↩
-
Original PDF page 2: L9 Benign Epithelial Pathosis, p.2 ↩
-
Original PDF page 7: L9 Benign Epithelial Pathosis, p.7 ↩
-
Original PDF page 9: L9 Benign Epithelial Pathosis, p.9 ↩
-
Original PDF page 10: L9 Benign Epithelial Pathosis, p.10 ↩
-
Original PDF page 17: L9 Benign Epithelial Pathosis, p.17 ↩
-
Original PDF page 15: L9 Benign Epithelial Pathosis, p.15 ↩
-
Original PDF page 34: L9 Benign Epithelial Pathosis, p.34 ↩
-
Original PDF page 35: L9 Benign Epithelial Pathosis, p.35 ↩
-
Original PDF page 37: L9 Benign Epithelial Pathosis, p.37 ↩
-
Original PDF page 44: L9 Benign Epithelial Pathosis, p.44 ↩
-
Original PDF page 45: L9 Benign Epithelial Pathosis, p.45 ↩
-
Original PDF page 46: L9 Benign Epithelial Pathosis, p.46 ↩
-
Original PDF page 47: L9 Benign Epithelial Pathosis, p.47 ↩
-
Original PDF page 50: L9 Benign Epithelial Pathosis, p.50 ↩
-
Original PDF page 59: L9 Benign Epithelial Pathosis, p.59 ↩
-
Original PDF page 23: L9 Benign Epithelial Pathosis, p.23 ↩
-
Original PDF page 64: L9 Benign Epithelial Pathosis, p.64 ↩
-
Original PDF page 65: L9 Benign Epithelial Pathosis, p.65 ↩