Unit A: Diagnostic Procedures
DMD Level 2 Orthodontic Seminar1
This unit covers the fundamental aspects of malocclusion, divided into the following primary areas of study:
- Part 1. Malocclusion: what is it and why should we treat it?
- Part 2. The etiology of malocclusion
Malocclusion: Definition and Treatment Rationale
Learning Objectives2
Ideal Occlusion and Angle Classification3456789
- Describe ideal occlusion in terms of the relationship of the teeth to the line of occlusion.
- Describe ideal occlusion in terms of the occlusal relationship of the teeth in all three planes of space (transverse, antero-posterior and vertical).
- List the dental characteristics on which the Angle classification is based.
- Discuss the advantages of the Angle system for classification.
- Describe the functional, health and psychosocial reasons for orthodontic treatment, and place them in perspective in terms of their relative importance.
- Describe realistic goals for orthodontic treatment, and indicate the way they have changed as modern dentistry developed.
- Discuss how need for orthodontic treatment compares with demand in the US at present and how demand is likely to change in the near future.
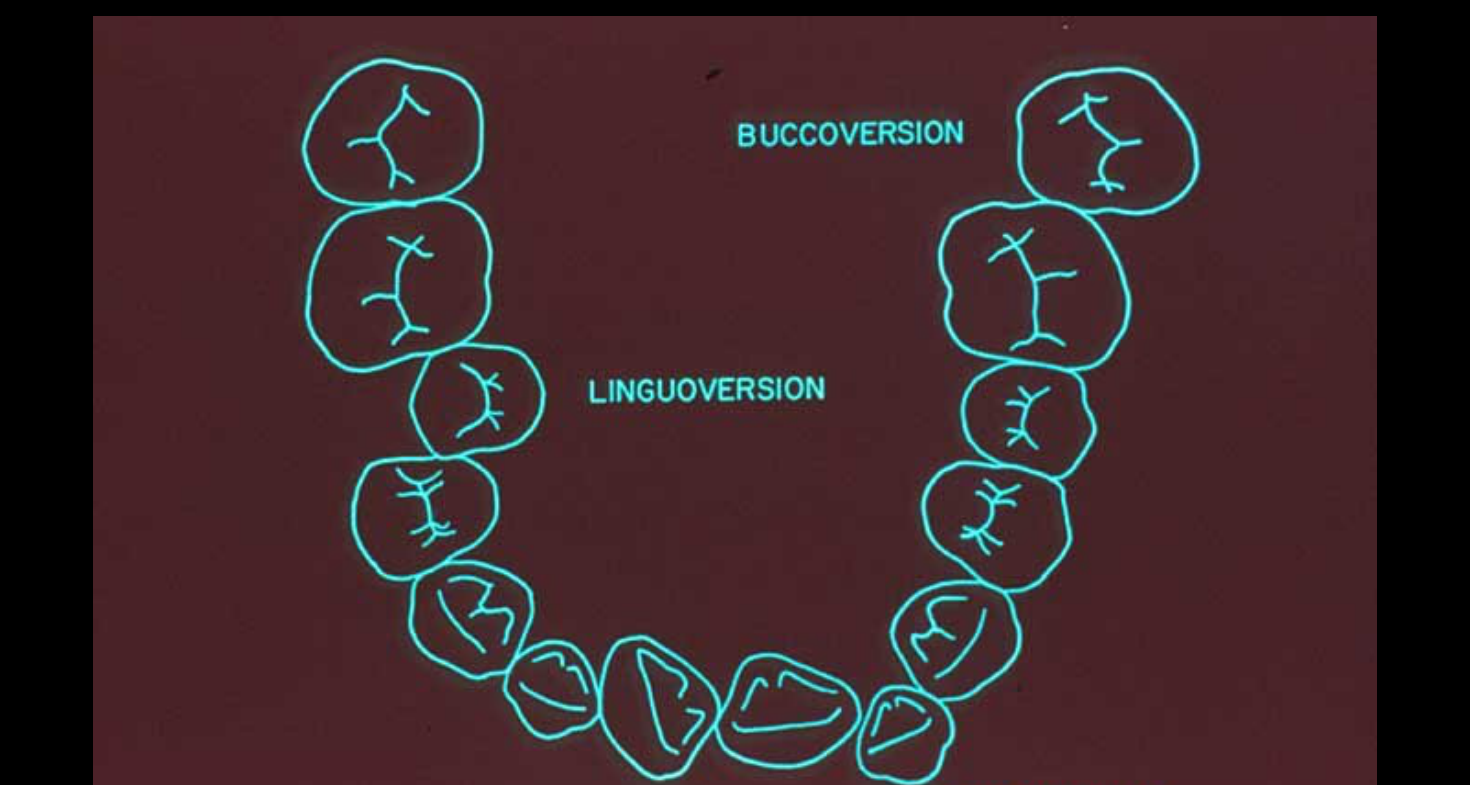
Angle described deviations from the line of occlusion.
- Angle used specific suffixes to identify tooth positions: Buccal-version (buccal), Lingual-version (lingual), Labial-version (labial), and Torsional-version (rotation).
- Limitations of Angle’s Method: It is criticized for being subjective and lacking quantification (e.g., no measurements in millimeters) and does not consider transverse/vertical planes or soft tissue.
- Despite its age, the system remains in use for simple clinical communication of general malocclusion groups.
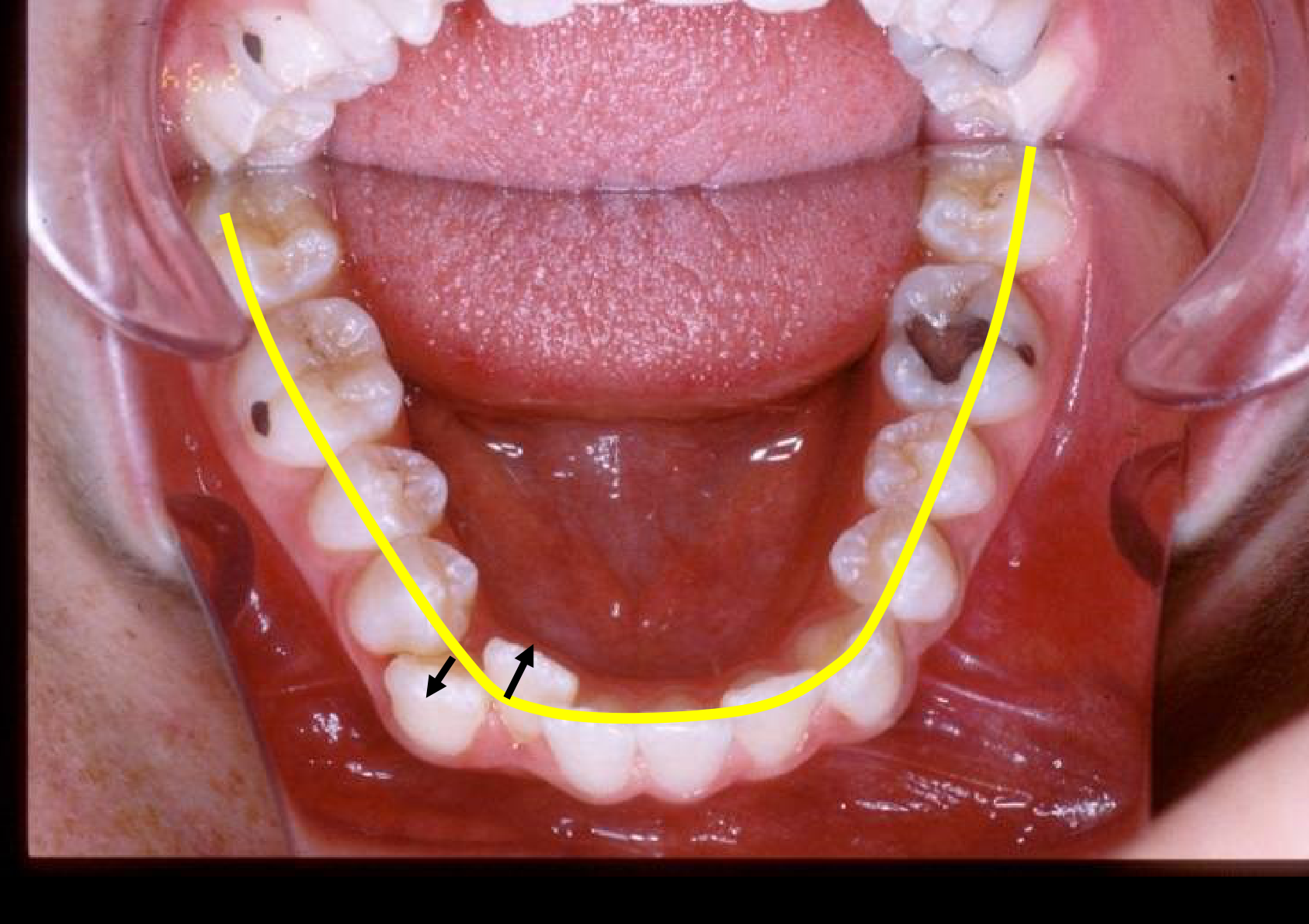
The Line of Occlusion
In the upper and lower arches, this line represents the engagement between the arches, sitting on approximately 138 occlusal contact points.
OR IS IT RANGE WHERE VALUES DICTATE THE CUT-OFF?
Describe ideal occlusion in terms of the occlusal relationship of the teeth in all three planes of space (transverse, antero-posterior and vertical).
 |  |  |
 |  |  |
 |  |
Historical Context10
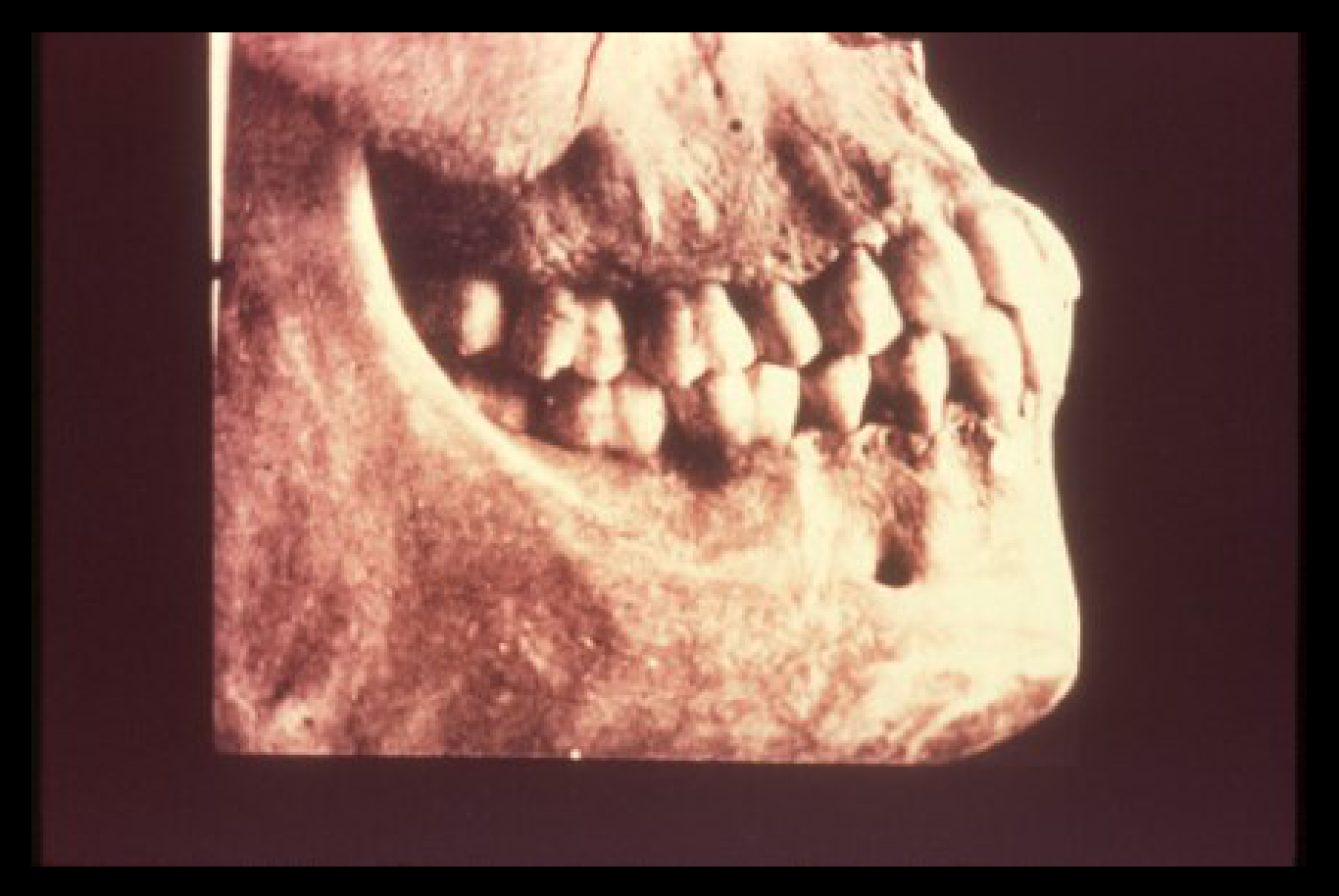
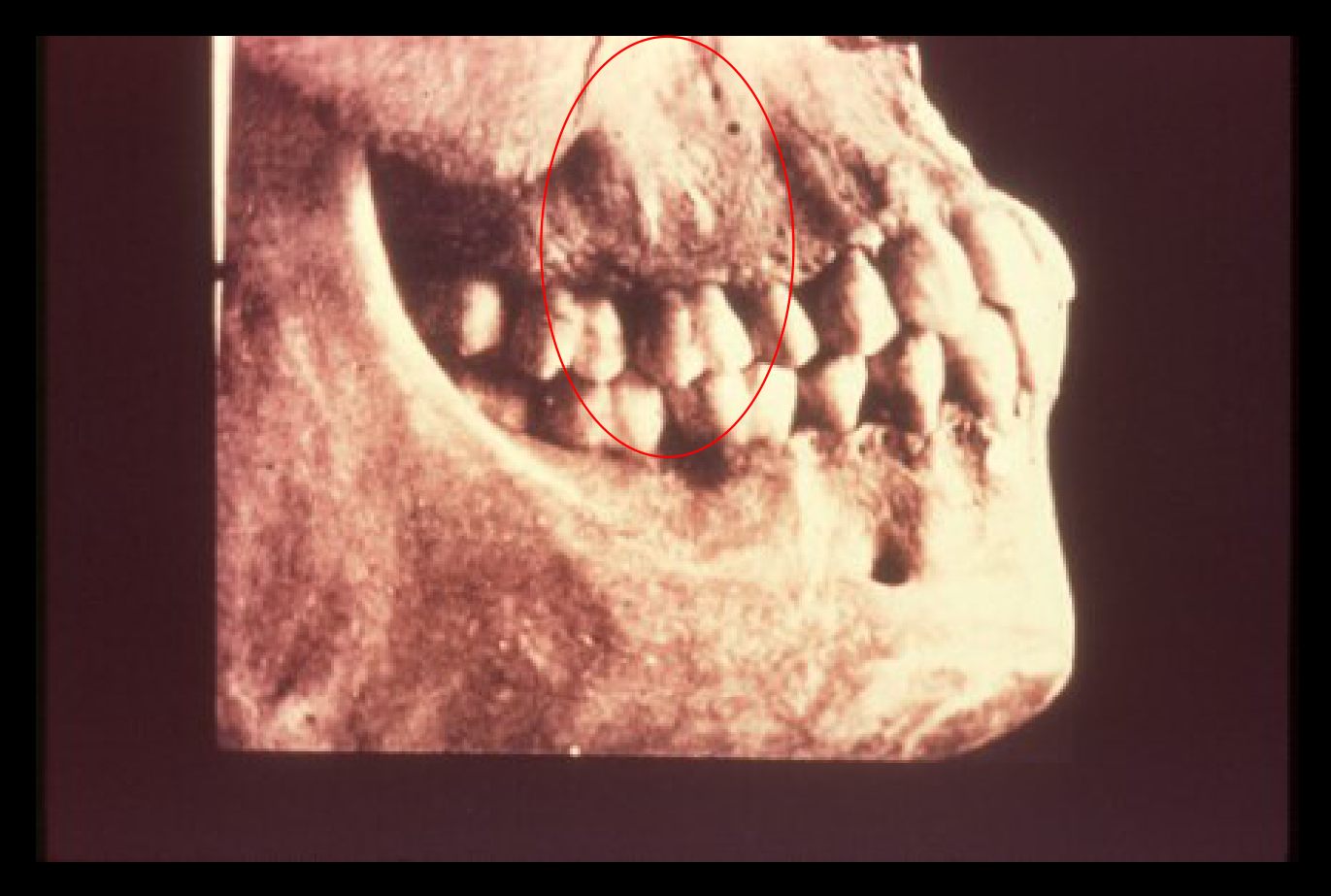
Dr. Edward H. Angle described ideal occlusion in detail as found in an American Indian skull.
 |  |
Class 1 Normal1112
- List the dental characteristics on which the Angle classification is based.
- Molar Relationship: The mesiobuccal cusp of the upper first molar should sit in the buccal groove of the lower first molar; the distobuccal cusp sits in the embrasure between the lower 6 and 7.
- Palatal Cusp: The upper palatal cusp should sit in the main fossa of the lower first molar.
- Class I Malocclusion: Defined as cases where molars are in the correct Class I relationship, but other teeth exhibit versions or drift from the line of occlusion.
 |  |
Historical Documentation131415
Dr. Edward H. Angle described ideal occlusion in detail as found in an American Indian skull. Documentation includes portraits of Dr. Angle and skull diagrams showing the zygomatic arch and teeth alignment.
Angle classified the occlusal relationships of the teeth into four parts:
-
Normal occlusion
-
Class I malocclusion
-
Class II malocclusion
-
Class III malocclusion
-
Discuss the advantages of the Angle system for classification.
 |  |
 |
Rationale for Orthodontic Treatment16
- Describe the functional, health and psychosocial reasons for orthodontic treatment, and place them in perspective in terms of their relative importance.
Primary Objectives of Orthodontics17
- Reduce psychosocial handicap
- Particularly relevant for Class II patients with large overjets who may experience social impacts like bullying.
- Improve oral function
- Includes preventing instabilities or amending conditions related to the Temporomandibular Joint (TMJ).
- Adjunct to disease control (not to treat disease)
- While malocclusion (like anterior crossbites) doesn't cause caries, it makes cleaning harder, making patients more prone to lesions without meticulous hygiene.
Treatment Goals and Paradigms18
- Describe realistic goals for orthodontic treatment, and indicate the way they have changed as modern dentistry developed.
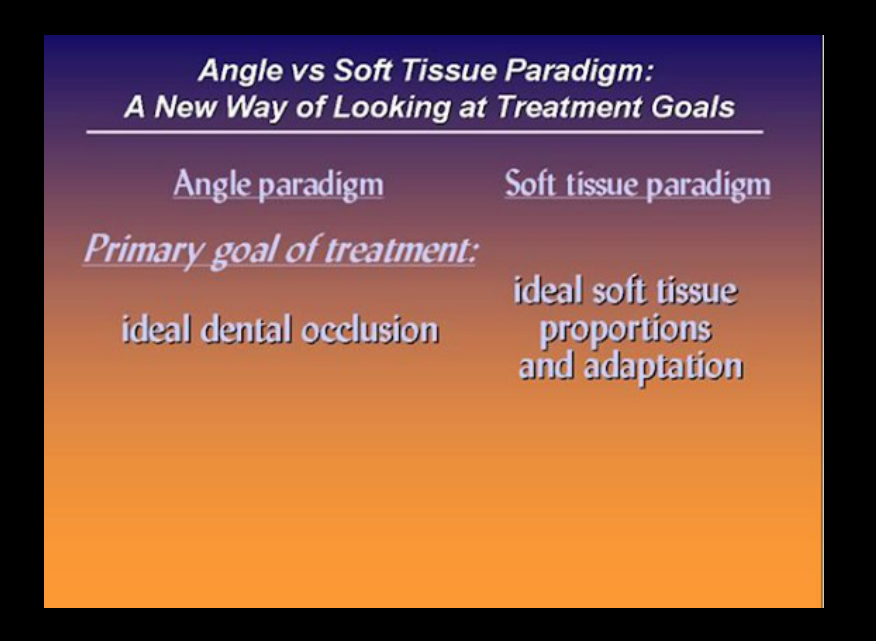
Angle vs Soft Tissue Paradigm: A New Way of Looking at Treatment Goals19
| Feature | Angle Paradigm | Soft Tissue Paradigm |
|---|---|---|
| Primary goal of treatment | Ideal dental occlusion | Ideal soft tissue proportions and adaptation |
| Secondary goal of treatment | Jaw relationships | Functional occlusion |
| Hard vs soft tissue relationship | Ideal skeletal/dental produces ideal soft tissue | Ideal soft tissue defines ideal skeletal/dental |
| Diagnostic emphasis | Dental casts, cephalometric x-rays | Clinical examination of soft tissues |
| Treatment approach | Obtain ideal dental and skeletal relationships, and the soft tissues will be OK | Determine ideal soft tissue relationships, and then place the jaws and teeth as needed to obtain them |
Modern Patient Perception
Patients often identify themselves by their profile in the mirror rather than molar relationships. Modern standards favor fuller profiles (e.g., the "Angelina Jolie era") over the straight or concave profiles favored in the past.
 |  |
 |  |
Treatment Demand and Patient Demographics20
Discuss how need for orthodontic treatment compares with demand in the US at present and how demand is likely to change in the near future.
Treatment Categories21
- Normal
- Malocclusion - no treatment
- Malocclusion - treatment

Socioeconomic Factors: Median Family Income Comparison22
2010 Data
- All other races: $59,914
- Hispanic origin: $36,771
2010-2012 Data
- All other races: $55,626
- Hispanic origin: $37,035

Who seeks orthodontic treatment?232425
- 65% of the population have malocclusion.
- Dentists feel that 55% need treatment.
- Patients feel that 35% need treatment.
Distribution includes Class I, Class II, Class III, and Normal Occlusion.
Do lay people not recognize problems OR do they place different values on the benefits of treatment?
Lay people can discriminate between good and bad teeth. It is simply that they place different value on the treatment to address the problem.

Treatment Utilization26
- Range: 5-40% get treatment.
- Socioeconomic Factors: In certain areas like Oahu, up to 75% of treatment may be government-funded.
- Compliance Issues: 100% free treatment risks low patient compliance; poor hygiene can lead to white spot lesions around brackets for which the clinician may be held responsible.
- Many factors influence this decision, including socioeconomic status.
Increasing Adult Demands27
- Job advancement
- Need to “trade up”
Perception of Treatment Benefit28
- Dentists: 55%
- Lay people: 35%
- Would accept if no cost: 50%

Treatment Acceptance Rates29
- 55% Need treatment
- 50% Accept treatment at no cost
- 5% Wouldn’t accept treatment even if it was free
Summary30
- Malocclusion is defined as a deviation of the line of occlusion or a deviation in the way the teeth relate.
- Malocclusion is more prevalent than normal occlusion.
- Most malocclusion consists of dental crowding, but 15% have a skeletal problem.
The Etiology of Malocclusion
Learning Objectives31
- Describe known causes of malocclusion in terms of major categories, and put the known causes in perspective relative to the total number of patients with malocclusion.
- Indicate the two types of malocclusion most likely to be due to inherited jaw proportions, and describe the evidence to support your categorization.
- Indicate the mechanism by which trauma to the mandible can affect its future growth.
- Identify the magnitude of force needed to cause movement of a tooth, and relate this to the observed threshold for tooth movement.
- Identify the duration of force needed to cause movement of a tooth, and relate this to the impact of habits like thumb sucking on the dentition.
- Describe the maturation of oral function from infancy to adult life, with particular emphasis on the pattern of swallow.
- Discuss myofunctional therapy for tongue thrusting as a potential therapy for anterior open bite in children, with emphasis on its underlying assumptions and their validity.
- Describe the possible role of nasal obstruction in the etiology of malocclusion, and indicate the probable mechanism by which it would have an effect.
Major Categories of Malocclusion Causes
Primary Etiological Categories32
- Hereditary factors
- Interference with normal development
- Trauma
- Disturbance with normal function
Classification of Causes33
- Facial form and congenital anomalies
- Postnatal Growth Disturbances
- Inherited Facial Disproportions
- Environmental Causes
Prevalence of Known Causes34
- 5% Known
- The rest (95%) Unknown
 |  |
Inherited Facial Disproportions3536
- Class II trends show similar genetic patterns in patients with deficient chins and large overjets. Indicate the two types of malocclusion most likely to be due to inherited jaw proportions, and describe the evidence to support your categorization.
 |  |
 |
Research Methodologies37
- Twin studies
- Family studies
- Dog studies
The Habsburg Dynasty
The Habsburg Dynasty (Spain/Europe) maintained a "protrusive Class III" jaw for over 200 years due to inbreeding to keep power within the family, demonstrating that genetic influence is very strong in Class III patients and often visible across generations.
 |  |
Trauma and Postnatal Growth Disturbances38394041
Indicate the mechanism by which trauma to the mandible can affect its future growth.
 |  |
 |
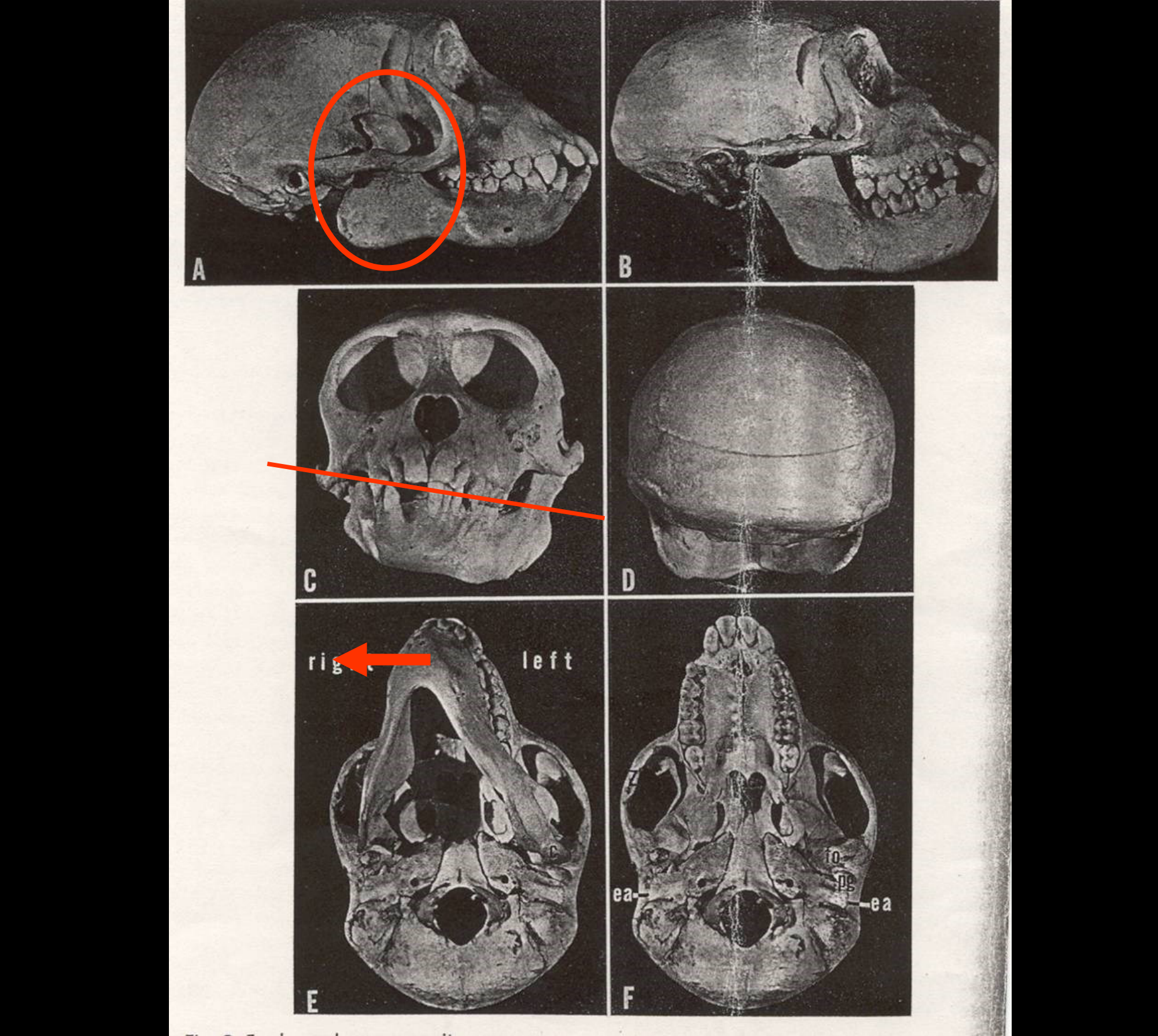
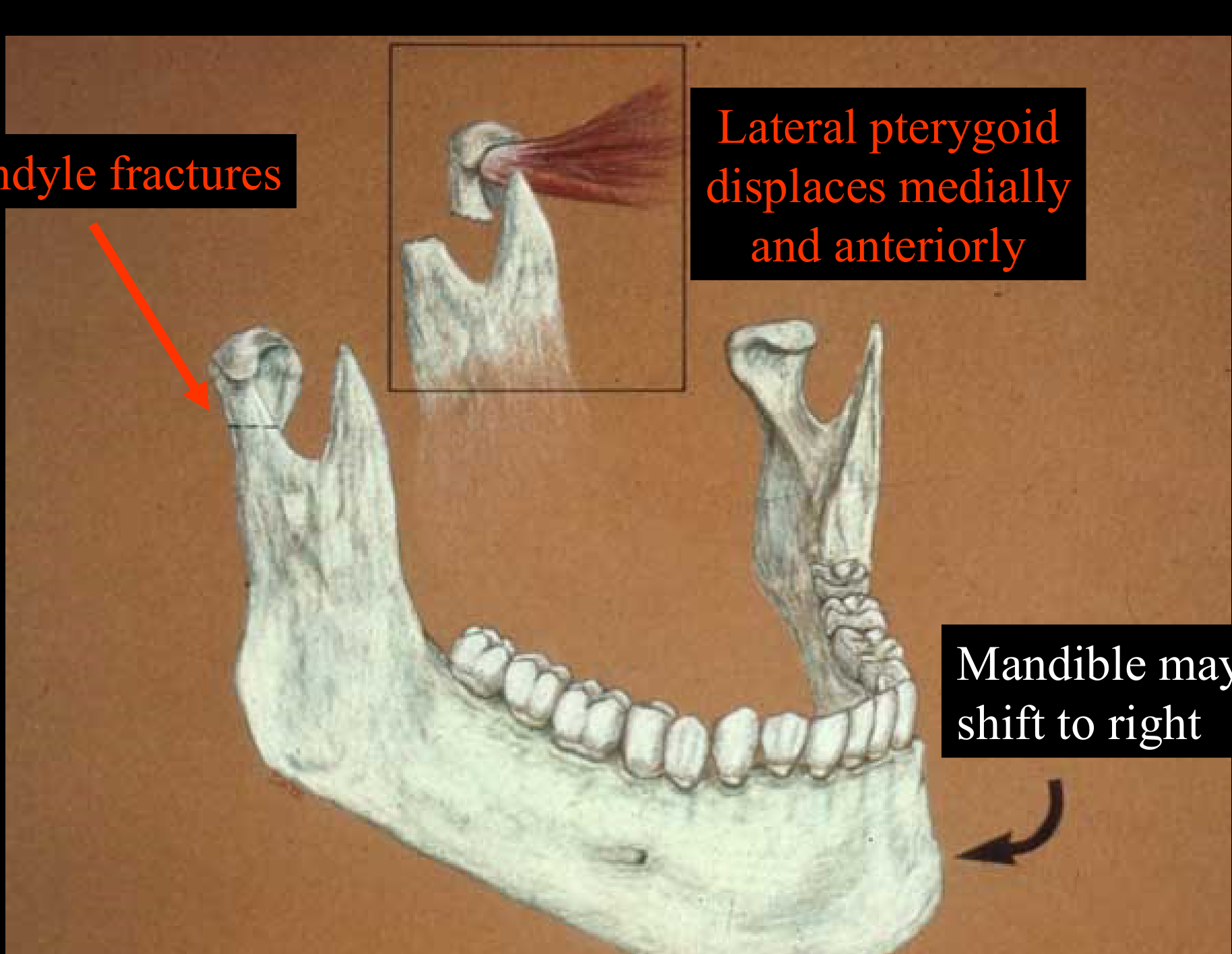
Condyle Fractures42
- Lateral pterygoid displaces medially and anteriorly
- Mandible may shift to the right
Research Methodology (Monkeys)
Researchers performed condylectomies on one side in monkeys to simulate unilateral fractures. The monkeys developed a shift in the mandible toward the side of the fracture and an occlusal cant.
Effect of Fracture of Mandibular Condyle in Children43
- 75% - Condyle regenerates: No growth deficit
- 25% - Partial regeneration: Growth deficit occurs
Mandibular Translation44
In order to grow properly, the mandible must be able to translate. Opening on a hinge is not enough.
-
Ankylosis of mandible leads to fusion across the Temporomandibular joint.
-
This fusion restricts motion.
-
Restricted motion inhibits growth.
- Clinical Signs of Ankylosis/Fracture:
- Mandible shifts to the same side as the fracture because the condyle is no longer under the traction of the lateral pterygoid muscle.
- Occlusal Cant: As the mandible shifts, compensatory extrusion occurs on the opposite side to maintain contact.
- Retrusive Chin: Because the mandible cannot grow anteroposteriorly, the patient develops a deficient chin.
- Clinical Signs of Ankylosis/Fracture:

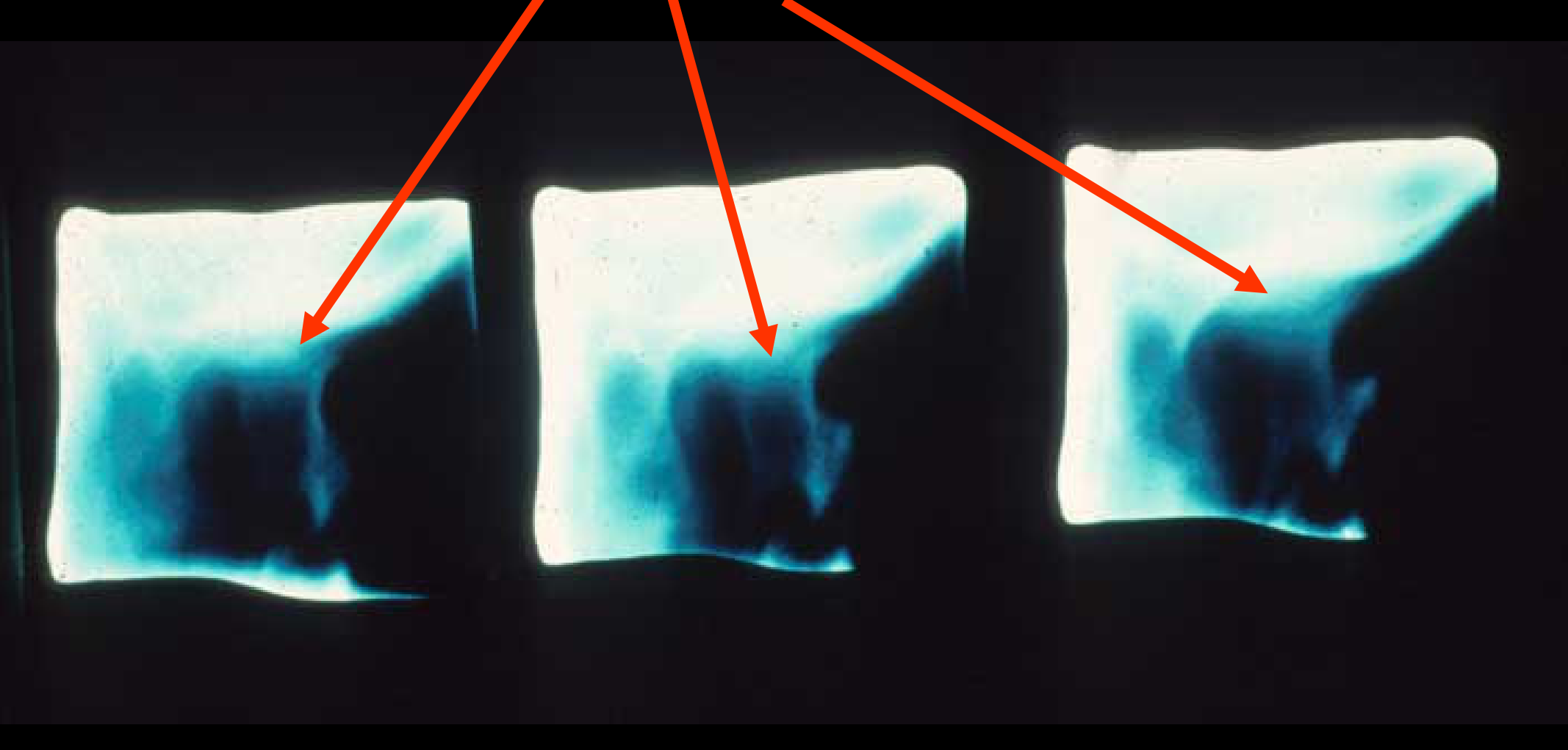
Early Childhood Fractures4546
Fractures of the condyle in early childhood.
 |  |
Ankylosis47
Ankylosis resulting from scarring.
Surgical Intervention48
Remove ankylosed joint.

Joint Replacement495051
Replace with something which grows at the same rate. - Costochondral Graft: The joint is often replaced with a piece of the patient's rib because it is a “growth site” that grows via endochondral ossification at a rate similar to the condyle.
 |  |
 |
Environmental Causes and Tooth Movement Forces52535455
Identifying the magnitude of force needed to cause movement of a tooth, and relating this to the observed threshold for tooth movement.
Identify the duration of force needed to cause movement of a tooth, and relate this to the impact of habits like thumb sucking on the dentition.
 |  |
Force and Eruption Data5657
- Force: 3 Gms.
- Intervals: 1 Sec to 3 Secs.
Eruption (Microns) over Time (Hours):
- 1.0 Hour: Force On
- 2.0 Hours: Force Off
- 3.0 Hours: Force On
- 4.0 Hours: Force Off
- 5.0 Hours
Figure showing eruption (microns) over time (hours) with On/Off force cycles and error bars.
Experiment on Force Levels
- Force A (Below eruption level): No change; the tooth continues to erupt.
- Force B (Equal to eruption level): Eruption is blocked while force is applied, but resumes once removed.
- Force C (Beyond eruption level): Achieves intrusion. Once removed, a "catch-up" eruption occurs, ending at the same point as Level B.
 |  |
Conclusions on Intermittent Force5859
Intermittent light force affects the eruption of the rabbit incisor based on duration:
- 50% Time: Similar to continuous force
- 25% Time: Intermediate effect (individual variation)
- 10% Time: Little or no effect
- Habit Duration: If a habit (like thumb sucking) is practiced for 12 hours a day (50% of the time), it has the same clinical effect as if it were practiced for 24 hours.
- Open Bite: A significant open bite (e.g., 7mm) is usually the result of a high-pressure thumb-sucking habit rather than just tongue posture.
 |  |
Maturation of Oral Function and Habits6061
Describe the maturation of oral function from infancy to adult life, with particular emphasis on the pattern of swallow.
Lip Posture62
- A: Relaxed Lip Closure
- B: Forced Lip Closure
Discuss myofunctional therapy for tongue thrusting as a potential therapy for anterior open bite in children, with emphasis on its underlying assumptions and their validity.
- Tongue Posture Training: Training a patient to “hold the tongue back” is generally ineffective because the instinct for an anterior seal is physiological.
- Treatment (Crib): A "crib" is used to block the tongue. Success depends on the patient having enough vertical growth to close the bite; otherwise, it becomes a surgical case.

Nasal Obstruction and Respiratory Mode6364
Describe the possible role of nasal obstruction in the etiology of malocclusion, and indicate the probable mechanism by which it would have an effect.
 |  |
Evidence Sources6566
- Linder-Aronson experiments
- Vig experiments
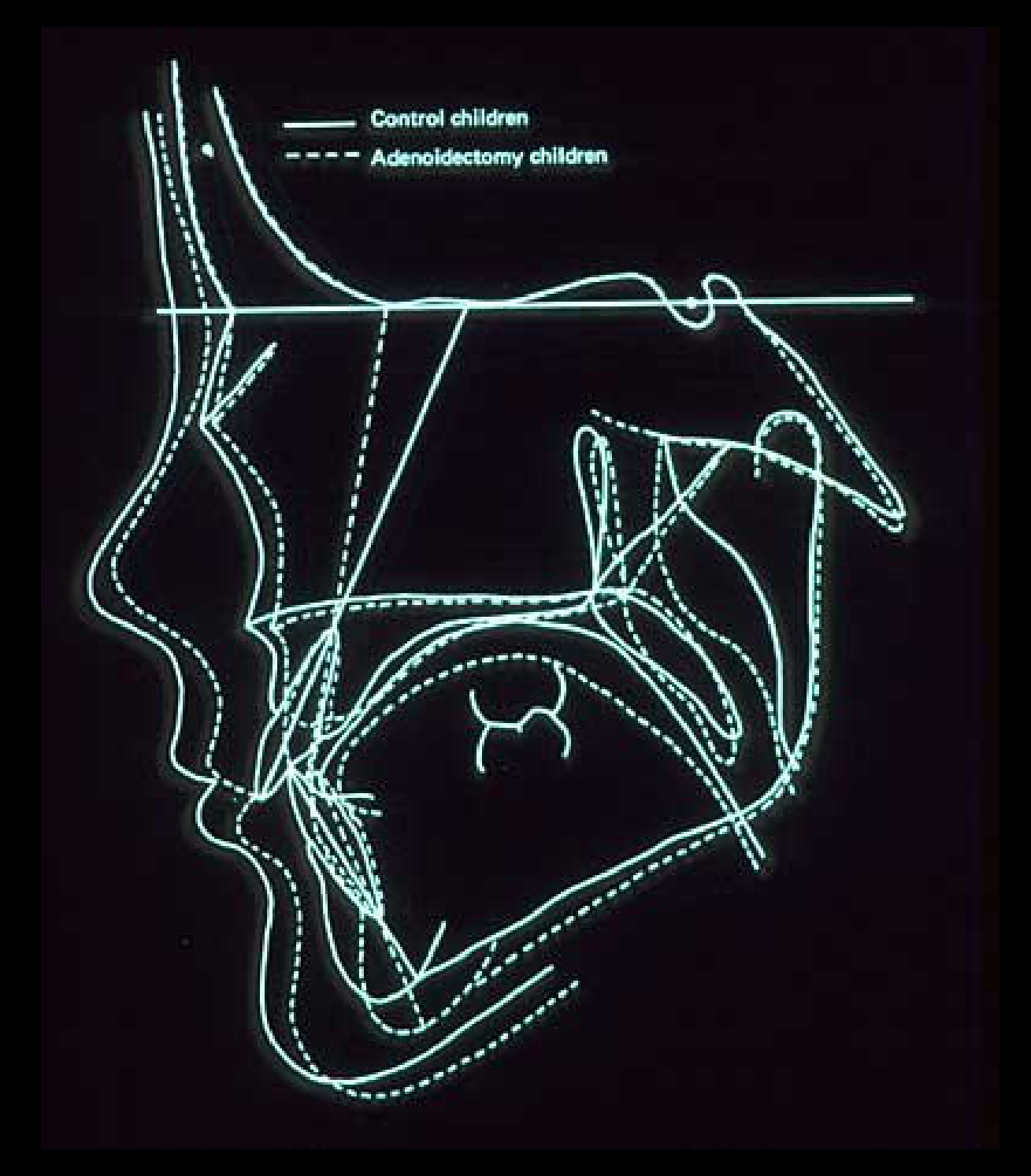
Conclusion67
Partial nasal obstruction in humans tends to increase face height.
Mechanism Concept68
Mode of respiration makes a difference as it alters postural relationships, leading to a change in resting pressures.
- Long Face Syndrome: Postural changes from nasal obstruction create a muscle/tongue imbalance, resulting in an atresic upper arch and a long face.
Evidence69
- Linder-Aronson experiments
- Vig experiments
- Adenoidectomy Studies: Removing obstructions shifted patients to nasal breathing, leading to enlargement of the nasopharyngeal cavity and upper arch (molar region), and protrusion of incisors due to new tongue posture.
- Head Position (DIG Experiment): Total nasal blockage causes a reflex where the patient moves their head back to keep the mouth open.
Footnotes
-
Original PDF page 1: DMD Level II Unit A(2), p.1 ↩
-
Original PDF page 2: DMD Level II Unit A(2), p.2 ↩
-
Original PDF page 3: DMD Level II Unit A(2), p.3 ↩
-
Original PDF page 4: DMD Level II Unit A(2), p.4 ↩
-
Original PDF page 5: DMD Level II Unit A(2), p.5 ↩
-
Original PDF page 6: DMD Level II Unit A(2), p.6 ↩
-
Original PDF page 7: DMD Level II Unit A(2), p.7 ↩
-
Original PDF page 8: DMD Level II Unit A(2), p.8 ↩
-
Original PDF page 9: DMD Level II Unit A(2), p.9 ↩
-
Original PDF page 10: DMD Level II Unit A(2), p.10 ↩
-
Original PDF page 11: DMD Level II Unit A(2), p.11 ↩
-
Original PDF page 12: DMD Level II Unit A(2), p.12 ↩
-
Original PDF page 13: DMD Level II Unit A(2), p.13 ↩
-
Original PDF page 14: DMD Level II Unit A(2), p.14 ↩
-
Original PDF page 15: DMD Level II Unit A(2), p.15 ↩
-
Original PDF page 16: DMD Level II Unit A(2), p.16 ↩
-
Original PDF page 17: DMD Level II Unit A(2), p.17 ↩
-
Original PDF page 18: DMD Level II Unit A(2), p.18 ↩
-
Original PDF page 19: DMD Level II Unit A(2), p.19 ↩
-
Original PDF page 20: DMD Level II Unit A(2), p.20 ↩
-
Original PDF page 21: DMD Level II Unit A(2), p.21 ↩
-
Original PDF page 22: DMD Level II Unit A(2), p.22 ↩
-
Original PDF page 23: DMD Level II Unit A(2), p.23 ↩
-
Original PDF page 24: DMD Level II Unit A(2), p.24 ↩
-
Original PDF page 25: DMD Level II Unit A(2), p.25 ↩
-
Original PDF page 26: DMD Level II Unit A(2), p.26 ↩
-
Original PDF page 27: DMD Level II Unit A(2), p.27 ↩
-
Original PDF page 28: DMD Level II Unit A(2), p.28 ↩
-
Original PDF page 29: DMD Level II Unit A(2), p.29 ↩
-
Original PDF page 30: DMD Level II Unit A(2), p.30 ↩
-
Original PDF page 31: DMD Level II Unit A(2), p.31 ↩
-
Original PDF page 32: DMD Level II Unit A(2), p.32 ↩
-
Original PDF page 33: DMD Level II Unit A(2), p.33 ↩
-
Original PDF page 34: DMD Level II Unit A(2), p.34 ↩
-
Original PDF page 35: DMD Level II Unit A(2), p.35 ↩
-
Original PDF page 36: DMD Level II Unit A(2), p.36 ↩
-
Original PDF page 37: DMD Level II Unit A(2), p.37 ↩
-
Original PDF page 38: DMD Level II Unit A(2), p.38 ↩
-
Original PDF page 39: DMD Level II Unit A(2), p.39 ↩
-
Original PDF page 40: DMD Level II Unit A(2), p.40 ↩
-
Original PDF page 41: DMD Level II Unit A(2), p.41 ↩
-
Original PDF page 42: DMD Level II Unit A(2), p.42 ↩
-
Original PDF page 43: DMD Level II Unit A(2), p.43 ↩
-
Original PDF page 44: DMD Level II Unit A(2), p.44 ↩
-
Original PDF page 45: DMD Level II Unit A(2), p.45 ↩
-
Original PDF page 46: DMD Level II Unit A(2), p.46 ↩
-
Original PDF page 47: DMD Level II Unit A(2), p.47 ↩
-
Original PDF page 48: DMD Level II Unit A(2), p.48 ↩
-
Original PDF page 49: DMD Level II Unit A(2), p.49 ↩
-
Original PDF page 50: DMD Level II Unit A(2), p.50 ↩
-
Original PDF page 51: DMD Level II Unit A(2), p.51 ↩
-
Original PDF page 52: DMD Level II Unit A(2), p.52 ↩
-
Original PDF page 53: DMD Level II Unit A(2), p.53 ↩
-
Original PDF page 54: DMD Level II Unit A(2), p.54 ↩
-
Original PDF page 55: DMD Level II Unit A(2), p.55 ↩
-
Original PDF page 56: DMD Level II Unit A(2), p.56 ↩
-
Original PDF page 57: DMD Level II Unit A(2), p.57 ↩
-
Original PDF page 58: DMD Level II Unit A(2), p.58 ↩
-
Original PDF page 59: DMD Level II Unit A(2), p.59 ↩
-
Original PDF page 60: DMD Level II Unit A(2), p.60 ↩
-
Original PDF page 62: DMD Level II Unit A(2), p.62 ↩
-
Original PDF page 61: DMD Level II Unit A(2), p.61 ↩
-
Original PDF page 63: DMD Level II Unit A(2), p.63 ↩
-
Original PDF page 64: DMD Level II Unit A(2), p.64 ↩
-
Original PDF page 65: DMD Level II Unit A(2), p.65 ↩
-
Original PDF page 66: DMD Level II Unit A(2), p.66 ↩
-
Original PDF page 67: DMD Level II Unit A(2), p.67 ↩
-
Original PDF page 68: DMD Level II Unit A(2), p.68 ↩
-
Original PDF page 69: DMD Level II Unit A(2), p.69 ↩